David Alain Wohl, MD Associate Professor of Medicine School of Medicine Site Leader, AIDS Clinical Trials Unit- Chapel Hill University of North Carolina at Chapel Hill Director, North Carolina AIDS Training and Education Center Chapel Hill, North Carolina Co-Director for HIV Services North Carolina Department of Correction Raleigh, North Carolina HIV and Cardiovascular Disease: How Worried Should We Be? Supported by educational grants from AbbVie, Bristol- Myers Squibb, Gilead Sciences, Janssen, Merck, and ViiV.
Transcript
David Alain Wohl, MDAssociate Professor of Medicine School of MedicineSite Leader, AIDS Clinical Trials Unit-Chapel HillUniversity of North Carolina at Chapel HillDirector, North Carolina AIDS Training and Education CenterChapel Hill, North CarolinaCo-Director for HIV ServicesNorth Carolina Department of CorrectionRaleigh, North Carolina
HIV and Cardiovascular Disease:How Worried Should We Be?
Supported by educational grants from AbbVie, Bristol-Myers Squibb, Gilead Sciences, Janssen, Merck, and ViiV.
clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
About These Slides
Users are encouraged to use these slides in their own noncommercial presentations, but we ask that content and attribution not be changed. Users are asked to honor this intent
These slides may not be published or posted online without permission from Clinical Care Options (email [email protected])
DisclaimerThe materials published on the Clinical Care Options Web site reflect the views of the authors of the CCO material, not those of Clinical Care Options, LLC, the CME providers, or the companies providing educational grants. The materials may discuss uses and dosages for therapeutic products that have not been approved by the United States Food and Drug Administration. A qualified healthcare professional should be consulted before using any therapeutic product discussed. Readers should verify all information and data before treating patients or using any therapies described in these materials.
clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
Disclosures
David A. Wohl, MD, has disclosed that he has received consulting fees from Gilead Sciences and Janssen and funds for research support from Merck.
clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
Outline
There are data suggesting increased risk of comorbidities, including CVD, in people with HIV
CVD is clearly more common in people with HIV
What is unclear is why
– Possibilities
– More risk factors (smoking, sedentariness, stress, depression)
– HIV (via immune and inflammatory mechanisms, microbial translocation, CMV)
– ART
Assessing risk
Approaches to prevention
clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
Outline
There are data suggesting increased risk of comorbidities, including CVD, in people with HIV
CVD is clearly more common in people with HIV
What is unclear is why
– Possibilities
– More risk factors (smoking, sedentariness, stress, depression)
– HIV (via immune and inflammatory mechanisms, microbial translocation, CMV)
– ART
Assessing risk
Approaches to prevention
clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
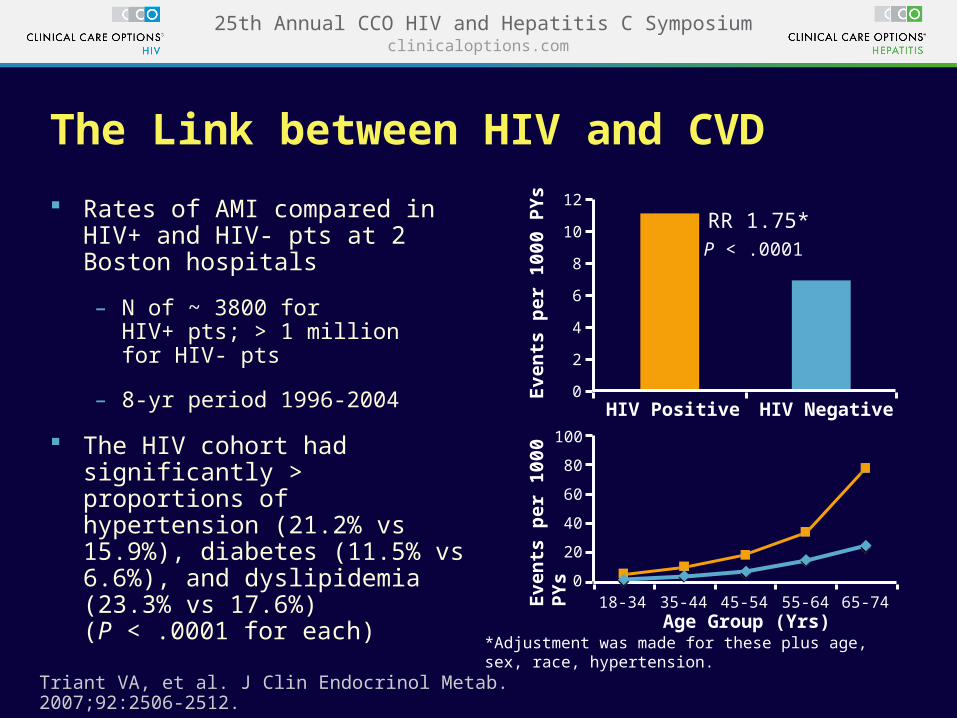
The Link between HIV and CVD
Rates of AMI compared in HIV+ and HIV- pts at 2 Boston hospitals
– N of ~ 3800 for HIV+ pts; > 1 million for HIV- pts
– 8-yr period 1996-2004
The HIV cohort had significantly > proportions of hypertension (21.2% vs 15.9%), diabetes (11.5% vs 6.6%), and dyslipidemia (23.3% vs 17.6%) (P < .0001 for each)
Triant VA, et al. J Clin Endocrinol Metab. 2007;92:2506-2512.
Eve
nts
per
10
00 P
Ys
Eve
nts
per
10
00 P
Ys
18-34 35-44 45-54 55-64 65-74Age Group (Yrs)
0
20
40
80
100
60
0
2
4
10
12
8
6
RR 1.75*P < .0001
HIV Positive HIV Negative
*Adjustment was made for these plus age, sex, race, hypertension.
clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
100
80
60
40
20
0
Post WS, et al. Ann Intern Med. 2014;160:458-467.
HIV Infection and Subclinical Coronary Atherosclerosis
+ - + - + - + - + - + -40-4453 26
45-49124 45
50-54118 88
55-5991 60
60-6450 54
65+14 36Men in Each Group, n
HIV StatusAge, yrs
Pre
vale
nce
of
No
nca
lcif
ied
Pla
qu
e (%
)
clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
Outline
There are data suggesting increased risk of comorbidities, including CVD, in people with HIV
CVD is clearly more common in people with HIV
What is unclear is why
– Possibilities
– More risk factors (smoking, sedentariness, stress, depression)
– HIV (via immune and inflammatory mechanisms, microbial translocation, CMV)
– ART
Assessing risk
Approaches to prevention
clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
Outline
There are data suggesting increased risk of comorbidities, including CVD, in people with HIV
CVD is clearly more common in people with HIV
What is unclear is why
– Possibilities
– More risk factors (smoking, sedentariness, stress, depression)
– HIV (via immune and inflammatory mechanisms, microbial translocation, CMV)
– ART
Assessing risk
Approaches to prevention
clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
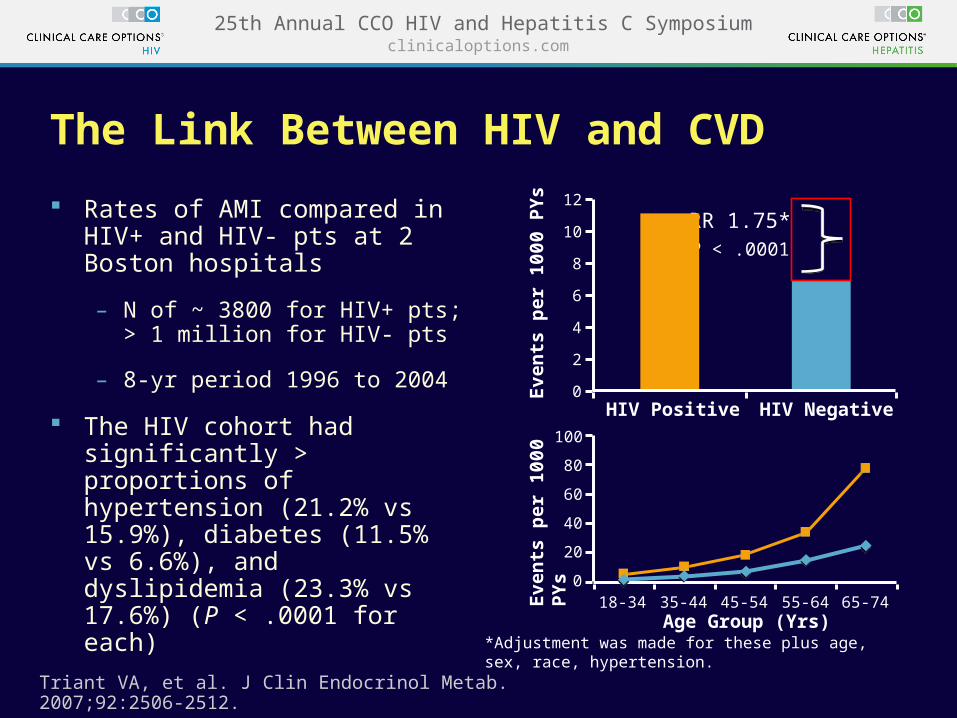
The Link Between HIV and CVD
Rates of AMI compared in HIV+ and HIV- pts at 2 Boston hospitals
– N of ~ 3800 for HIV+ pts; > 1 million for HIV- pts
– 8-yr period 1996 to 2004
The HIV cohort had significantly > proportions of hypertension (21.2% vs 15.9%), diabetes (11.5% vs 6.6%), and dyslipidemia (23.3% vs 17.6%) (P < .0001 for each)
Triant VA, et al. J Clin Endocrinol Metab. 2007;92:2506-2512.
Eve
nts
per
10
00 P
Ys
Eve
nts
per
10
00 P
Ys
18-34 35-44 45-54 55-64 65-74Age Group (Yrs)
0
20
40
80
100
60
0
2
4
10
12
8
6
RR 1.75*P < .0001
HIV Positive HIV Negative
*Adjustment was made for these plus age, sex, race, hypertension.
clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
How Big Is the Contribution of HIV and HIV-Related Factors to CVD and Other Conditions Associated With Aging?
Traditional Factors
clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
0.14 (0.02 to 0.25)0.19 (0.05 to 0.33)0.16 (0.03 to 0.29)0.15 (-0.05 to 0.35)-0.02 (-0.21 to 0.17)
.65
.023
.009
.015
.133.83
0.03 (-0.34 to 0.29)
0.11 (-0.01 to 0.22)0.13 (-0.01 to 0.27)0.15 (0.02 to 0.29)0.16 (-0.04 to 0.36)-0.07 (-0.27 to 0.12)
.88
.075
.062
.026
.109.46
*Adjusted for age, race, CT scanning center, cohort (before vs after 2001).†Adjusted for age, race, CT scanning center, cohort, and CAD risk factors (systolic blood pressure, antihypertensive medication use, diabetes medication use, fasting glucose level, total and high-density lipoprotein cholesterol levels, use of lipid-lowering medications, body mass index, and pack-yrs of smoking).‡Ratio of HIV-infected to HIV-uninfected men.§Analyses (in natural log scale) include men with plaque present (plaque score >0).ǁHIV-infected minus HIV-uninfected men.
P Value Mean Difference (95% CI)ǁ P Value
clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
1. Klein DB, et al. CROI 2014. Abstract 737. 2. Klein DB, et al. Clin Infect Dis. 2015;60:1278-1280. 3. Marcus JL, et al. CROI 2014. Abstract 741. 4. Marcus JL, et al. AIDS. 2014;28:1911-1919.
[3,4]
The reduced MI incidence rates for HIV+ in recent yrs is likely a result of:
– CVD risk factor reduction
– Use of more lipid-friendly ART
– Reduced immunodeficiency
Yr
200
150
100
50
1996-1999
2000-2003
2004-2007
2008-2009
2010-2011
250
0
Stroke Rates by HIV Status and Yr[3,4]
Ca
se
s p
er
10
0,0
00
PY
s
HIV+HIV-
400
MIs
pe
r 1
00
,00
0 P
Ys
300
200
100
0
1996-992000-03
2004-072008-09
2010-11
HIV+HIV-
MI Rates Over Time by HIV Status[1,2]
clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
Hanna D, et al. CROI 2015. Abstract 729.
2001-2012 mortality data NYC
The NYC HIV Surveillance Registry and Vital Statistics Registry
National Death Index
145,000 HIV+ people
– 29,000 deaths
Over time, as HIV+ persons were less likely to die of HIV-related causes, the proportion succumbing to CVD increased
General population, menGeneral population, womenHIV diagnosed, menHIV diagnosed, women
Leading Underlying Causes of Death for HIV-Diagnosed New Yorkers, by Proportion
Age-Standardized CVD Mortality Rate, by HIV Diagnosis Status and Sex
clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
Risk Factors for CVD Events in HIV+ Pts
Risk ratios for PI and boosted PI were estimated per additional yr, TC and HDL cholesterol per mmol/L higher, and systolic BP per 10 mmHg higher.
Friis-Moller N, et al. European J of CV Prevention and Rehab. 2010;17:491-501.
PI
Boosted P
I
Male Sex
NRTI
Age (per 5
Yrs O
lder)
Current C
igare
tte
Smokin
g
Family
Histo
ry
of CVD
Exsmokin
g
Diabetes
Total
Cholestero
l HDL
Cholestero
l
Systolic
BP
Estimated Risk Ratio of CVD Events Among 22,625 HIV-Positive Pts
(D:A:D Study)
3.5
3.0
2.5
2.0
1.5
1.0
0.5
0
1.001.08
1.631.70
1.421.43
2.35
1.27
1.92
1.21
0.67
1.05
Est
imat
ed R
isk
Rat
io (
95%
CI)
Greater R
isk
clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
Chronic Inflammation Is Associated With Increased Risk for Comorbidities in HIV+ Pts
Deeks SG. Annu Rev Med. 2011;62:141-155.
Untreated HIV Infection
HIV replication
ART
Loss of immunoregulatory cellsLoss of gut mucosal integrity and microbial translocation
Decreased but persistent chronic inflammation, immune activation, elevated
coagulation markers, microbial translocation, and increased risk of coinfection
Increased incidence of comorbidities and clinical disease
Traditional comorbidity risk factors, such as dyslipidemia, smoking, lipodystrophy, HTN, obesity, substance use
clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
100
60
0
-40
80
40
-20
-60
20
*Adjusted for age, race, smoking, HCV infection, obesity, diabetes and MACS site. †Error bars represent 99.7% CIs, calculated with Bonferroni adjustment to maintain a family-wise error rate of 0.05. Filled markers represent statistical significance (P < .002).
Biomarkers of Inflammation Are Elevated in HIV+ Pts Even on ART
Wada NI, et al. AIDS. 2015;29:463-471.
Adjusted Percentage Differences in Biomarkers of Inflammation and Immune Activation in HIV-Positive Pts and Uninfected Individuals*†
(Multicenter AIDS Cohort Study, 1984-2009)
Dif
fere
nce
(%
)
CXCL10
sCD27
IL-1
0sI
L-2R
αIL
-2sT
NFR2IF
N-γCXCL1
3TNF-α
IL-1
2p70
sIL-
6RBAFFCCL2 IL
-6sC
D14G
M-C
SFCCL1
1CRPIL
-1β
sGP13
0IL
-8CCL1
3CCL1
7CCL4
HIV suppressed relative to ART naive
HIV suppressed relative to HIV uninfected
clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
Plasma IL-6 Levels Correlated With Incidence of Mortality SMART and ESPRIT
19,000 PYs of follow-up among 4304 PYs (median age: 42 yrs; median CD4: 526; 77% men)
– 157 all-cause deaths
– 117 non-AIDS deaths
– 101 progressions to AIDS
– 121 CVD
– 99 NADM
IL-6 (baseline) was found to be a stronger predictor of all cause mortality and many fatal non-AIDS events than the other 2 markers
Adjustment attenuated the associations but IL-6 remained significant including for CVD
Borges A, et al. CROI 2015. Abstract 761.
25
20
15
10
5
0
Cru
de
In
cid
ence
Ra
tes
per
10
00 P
YF
U (
95%
CI)
All-cause death
Non-AIDS/violent/
accidental death
AIDS CVD NADM
Crude Incidence Rates of Clinical Outcomes Across Biomarker Quartiles*
Events, n
IL-6
1st quartile2nd quartile3rd quartile4th quartile
1421
35
87
72
23
6
16
3624
1526
54
33
2113
42
2819
10
*Quartiles were defined differently in SMART and ESPRIT trials.
clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
Role of Monocytes in Atheromatous Plaque Development
HIV activates monocytes and endothelial cells (in conjunction with proatherogenic lipids)
– Increase monocyte transmigration
– Increase uptake of oxLDL
– Promote differentiation into foam cells
– And contribute to atherosclerotic plaque formation
Campbell J, et al AIDS. 2014;28:2175-2187.
clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
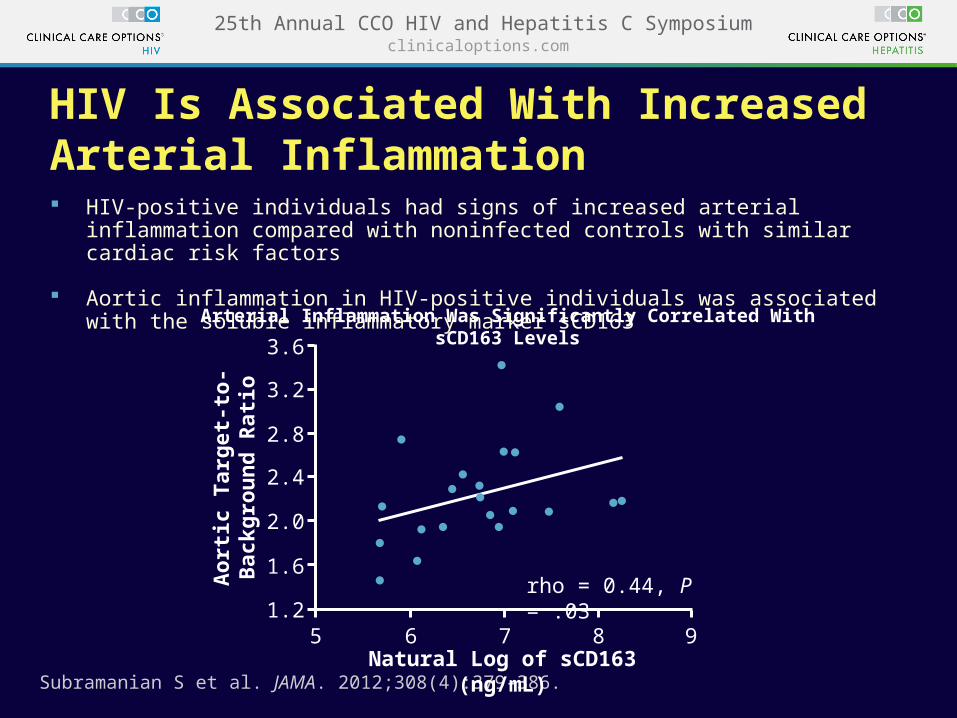
HIV Is Associated With Increased Arterial Inflammation HIV-positive individuals had signs of increased arterial inflammation compared with
noninfected controls with similar cardiac risk factors
Aortic inflammation in HIV-positive individuals was associated with the soluble inflammatory marker sCD163
Subramanian S et al. JAMA. 2012;308(4):379-386.
Arterial Inflammation Was Significantly Correlated With sCD163 Levels3.6
3.2
2.8
2.4
2.0
1.6
1.25 6 7 8 9
rho = 0.44, P = .03
Natural Log of sCD163 (ng/mL)
Ao
rtic
Tar
get
-to
-B
ackg
rou
nd
Rat
io
clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
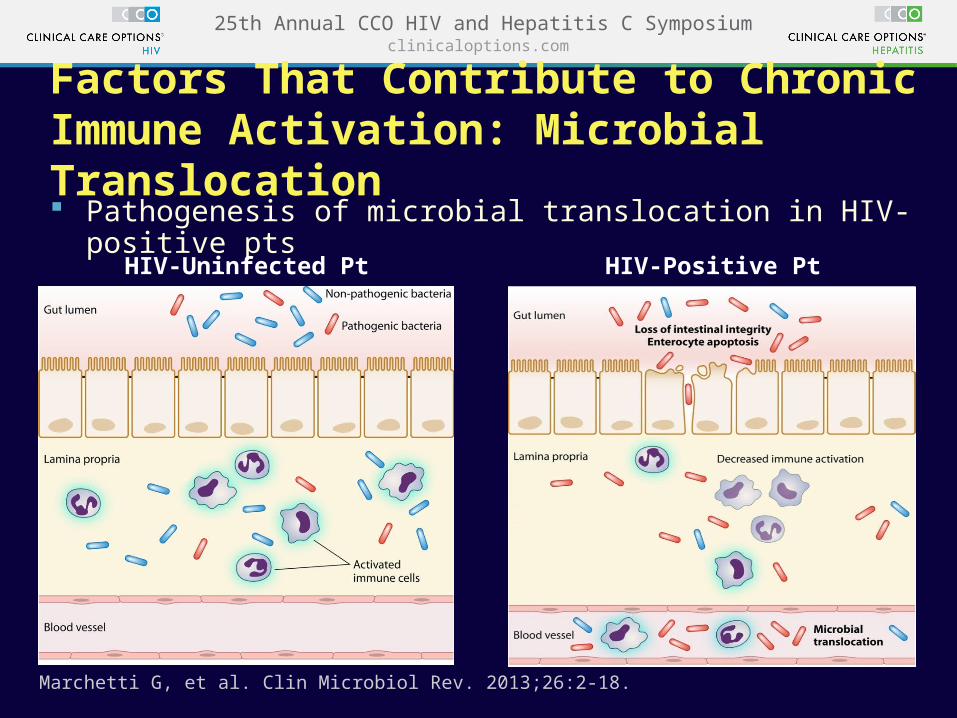
Pathogenesis of microbial translocation in HIV-positive pts
Factors That Contribute to Chronic Immune Activation: Microbial Translocation
Marchetti G, et al. Clin Microbiol Rev. 2013;26:2-18.
HIV-Uninfected Pt HIV-Positive Pt
clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
A Marker of Microbial Translocation Declines During Suppressive ART but Does Not Normalize
Progressors were chronically HIV-positive individuals and individuals with AIDS (< 200 CD4+ cells/mm3)
Each group contains combined pt data from 2 unique cohorts, grouped according to HIV status and study design.
Brenchley JM, et al. Nat Med. 2006;12:1365-1371.
ProgressorsUntreated
Progressors48 Wks ART
Uninfected
150
100
50
0
Pla
sma
LP
S (
pg
/mL
)
P = .0107 P = .0026
clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
7 clinical cohorts from NA-ACCORD (~ 20%)
All ART users except those on ABC at study entry
Only ART-naive persons observed to have initiated ART
Awaiting more comprehensive analysis using marginal structural model with time updated data (if capable of
doing with relatively small sample size)
ABC and CV Disease: NA-ACCORD
Palella F, et al. CROI 2015. Abstract 749LB.
D:A:D replication
Full Study Population
Restricted Study Population
0 1.00 2.00 3.00 4.00
Adjusted HR
clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
NA-ACCORD: Risk Factors Associated With MI
Palella F, et al. CROI 2015. Abstract 749LB.
Recent ABC use
Age < 40 (vs 50-59) yrs
Age 40-49 (vs 50-59) yrs
Age ≥ 60 (vs 50-59) yrs
Smoking
Hypertension
Diabetes
eGFR 30-59 (vs ≥ 60) mL/min/1.73m2
eGFR < 30 (vs ≥ 60) mL/min/1.73m2
High (≥ 240 vs < 240 mg/dL) total cholesterol
Statin use
High (≥ 300 vs < 300 mg/dL) triglycerides
0 8.006.004.002.00
Adjusted HR for MI
Restricted study population
Full study population
clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
D:A:D Renal Disease and CVD
Ryom L, et al. CROI 2015. Abstract 742.
25
20
15
10
5
0 12 24 36 48 60 720
Mos After Baseline24,605915598746
24,023890793739
22,376831383530
20,895768176026
18,979697764922
15,631598952413
13,0015134444
8
>90>60-≤60>30-≤60≤30
N Under Follow-up
Kapian-Meier Progression to CVD by Confirmed Baseline eGFR
Per
cen
tag
e W
ith
CV
D
Baseline (confirmed) eGFR ≤30 >30-≤60 >60-≤90 >90
clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
Toxic Effects of Stress
Helplessness and health
– More helplessness > risk of CVD, DM, and depression
Effects occur early and linger
– Early hardships continue to be associated with illness later in life despite SE ascendancy
Poverty by definition produces stress for which there are fewer resources to address problems
Stress leads to biological changes (hypercortisolism, increases in markers of inflammation)
– ? CNS changes such as reduced hippocampus volume?
clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
Take Homes
This is complex
Clear signals for role of discrimination in risk of CVD
There are underlying psychosocial, genetic, and sex differences in one’s susceptibility to exposure to discrimination
Depression is major co-occurrence
Discrimination is a factor that needs to be included in CVD research
Lewis T, et al. Annu Rev Clin Psychol. 2015;11:407-40.
clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
Chronic depressive symptoms Present AbsentHIV Status Infected Uninfected Race Black Hispanic Whites and othersBMI category Underweight or nomal BMI Overweight ObeseEducation Completed high school/GED Did not complete high schoolHousehold income level < $12,000/yr $12,000/yrUse of antidepressants Present AbsentIllicit drug use Present AbsentAlcohol use Present Absent
2.4 ± 0.60.1 ± 0.3
0.8 ± 0.3-0.4 ± 0.6
1.3 ± 0.4-0.5 ± 0.5-0.3 ± 0.7
0.2 ± 0.5-0.2 ± 0.61.5 ± 0.5
0.6 ± 0.40.4 ± 0.5
1.4 ± 0.4-0.4 ± 0.4
1.7 ± 0.50.2 ± 0.3
1.0 ± 0.60.4 ± 0.3
-1.4 ± 0.80.8 ± 0.3
< .01
.07
.01
.23
.7
< .01
.02
.41
< .01
1.3 ± 0.6-0.3 ± 0.4
0.3 ± 0.40.2 ± 0.6
0.9 ± 0.40.3 ± 0.60.2 ± 0.6
0.7 ± 0.50.02 ± 0.50.7 ± 0.5
0.4 ± 0.50.5 ± 0.5
0.6 ± 0.40.3 ± 0.5
0.6 ± 0.50.4 ± 0.4
1.0 ± 0.5-0.03 ± 0.5
-0.4 ± 0.61.3 ± 0.4
< .01
.52
.34
.37
.86
.51
.72
.07
< .01
VariableUnadjusted Estimated
FRS (Mean ± SE) P Value Adjusted* Estimated FRS P Value
*Adjusted for initial visit Framingham risk score in addition to factors displayed in the table.Note: Bold values denote P < .01
Chronic Depressive Symptoms and Framingham Coronary Risk in HIV-Infected and Uninfected Women
clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
Demographics, CVD Risk Factors, and Other Important
Covariates Models
HIV-Specific Factors Models
HR (95% CI) HR (95% CI)
Any depressive disorder
1.31 (1.03-1.67) 1.31 (1.03-1.67)
MDD 1.27 (0.98-1.64) 1.28 (0.99-1.65)
Dysthymic disorder
1.46 (1.07-1.99) 1.47 (1.08-2.01)
Association of Depressive Disorders With Incident AMI (separate models)
2.59
3.32 3.28
3.88
Unadjusted Incident AMI Rates per 1000 Person-Yrs by Depressive Disorder
5.0
4.0
3.0
2.0
1.0No
Depressive Disorder
Any Depressive
Disorder
MDD Dysthymic Disorder
Depressive Disorders Predicts Incident AMI in HIV+ Veterans: Veterans Aging Cohort Study
clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
Outline
There are data suggesting increased risk of comorbidities, including CVD, in people with HIV
CVD is clearly more common in people with HIV
What is unclear is why
– Possibilities
– More risk factors (smoking, sedentariness, stress, depression)
– HIV (via immune and inflammatory mechanisms, microbial translocation, CMV)
– ART
Assessing risk
Approaches to prevention
clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
CVD Risk Prediction Equations Developed for the General Population Consistently Underestimate CVD Risk in HIV Pts
An outpatient study cohort (n=2392) had similar findings of underestimated CVD risk (15% to 25%)[2]
1. Regan S, et al. CROI 2015. Abstract 751. 2. Thompson-Paul A, et al. CROI 2015. Abstract 747.
5-Yr Predicted Rate (%)
Framingham Risk Score
5-Y
r E
ven
t R
ate
(%
)
5-Y
r E
ven
t R
ate
(%
)
ACC/AHA CVD Risk Calculator
5-Yr Predicted Rate (%)
Observed
Predicted
Observed
Predicted
Observed vs Predicted 5-Yr CVD Outcomes in Partners Healthcare System HIV Longitudinal Cohort of 2270 HIV-Positive Pts[1]
clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
Outline
There are data suggesting increased risk of comorbidities, including CVD, in people with HIV
CVD is clearly more common in people with HIV
What is unclear is why
– Possibilities
– More risk factors (smoking, sedentariness, stress, depression)
– HIV (via immune and inflammatory mechanisms, microbial translocation, CMV)
– ART
Assessing risk
Approaches to prevention
clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
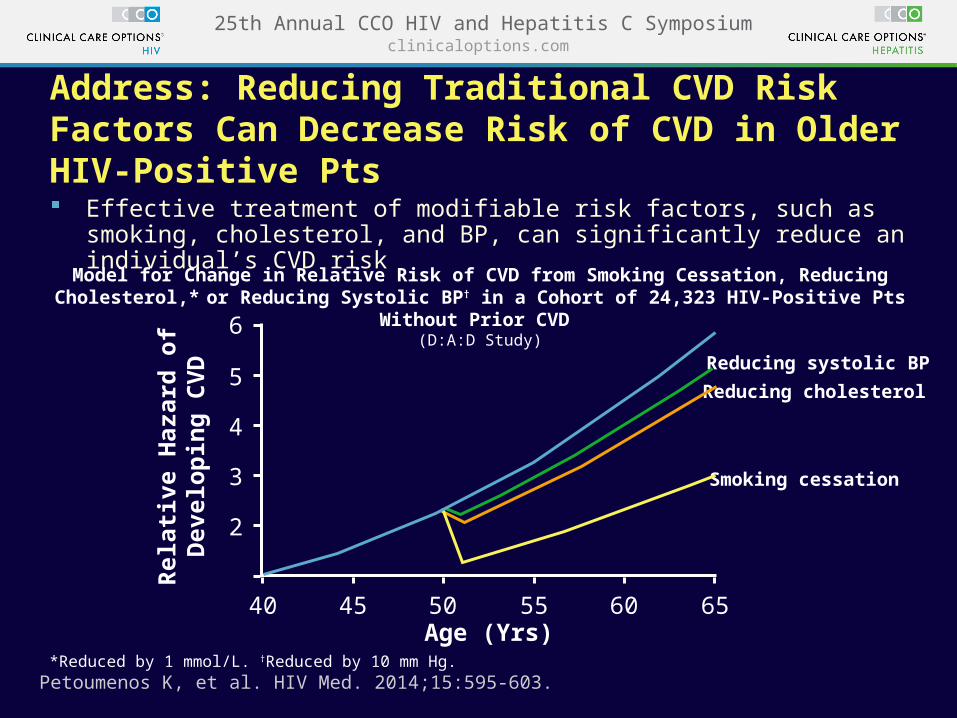
Address: Reducing Traditional CVD Risk Factors Can Decrease Risk of CVD in Older HIV-Positive Pts
Effective treatment of modifiable risk factors, such as smoking, cholesterol, and BP, can significantly reduce an individual’s CVD risk
Model for Change in Relative Risk of CVD from Smoking Cessation, Reducing Cholesterol,* or Reducing Systolic BP† in a Cohort of 24,323 HIV-Positive Pts Without Prior CVD
(D:A:D Study)
*Reduced by 1 mmol/L. †Reduced by 10 mm Hg. Petoumenos K, et al. HIV Med. 2014;15:595-603.
Reducing cholesterol
Reducing systolic BP
Smoking cessation
6
5
4
3
2
40 45 50 55 60 65Age (Yrs)
Rel
ativ
e H
azar
d o
f D
evel
op
ing
CV
D
clinicaloptions.com25th Annual CCO HIV and Hepatitis C Symposium
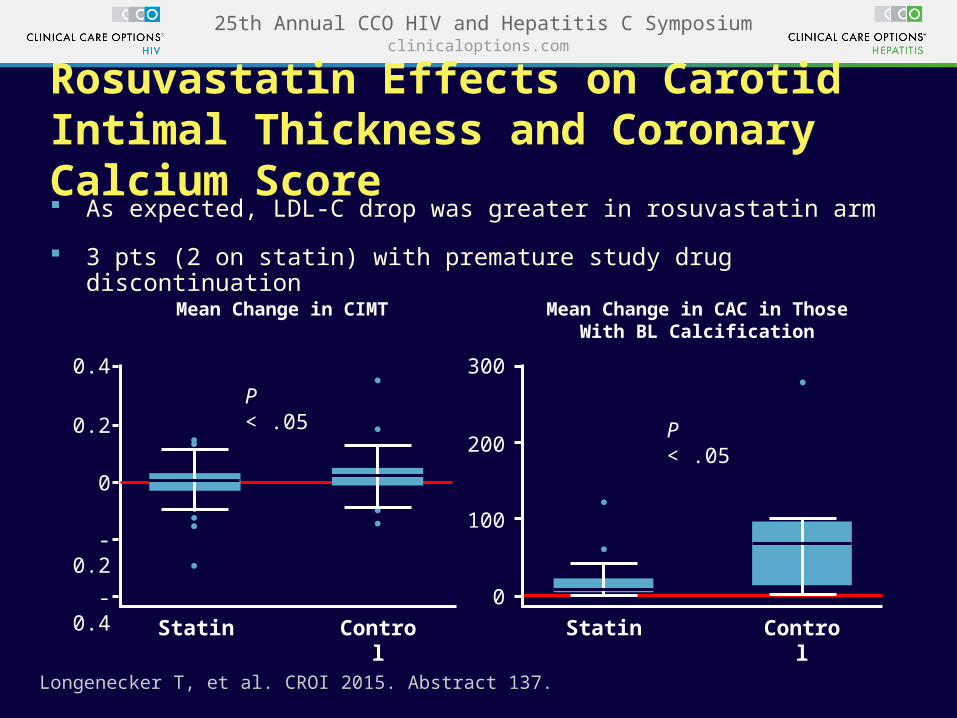
Rosuvastatin Effects on Carotid Intimal Thickness and Coronary Calcium Score