38
HIV/AIDS CHALLENGE IN UGANDA A REPORT AND PROPOSAL BY A MEDICAL STUDENT FROM MAKERERE UNIVERSITY UGANDA EAST AFRICA Willington Amutuhaire

HIV/AIDS CHALLENGE IN UGANDA
A REPORT AND PROPOSAL BY A MEDICAL STUDENT FROM MAKERERE UNIVERSITY
UGANDAEAST AFRICA
Willington Amutuhaire
Talk outline• Background• Evolution of the epidemic• History of HIV in Uganda• Epidemiological trends• Routes of transmission• National response• Impact of HIV• Prevention of HIV• HIV testing• HIV treatment• Challenges• Proposal• My Research project
BACKGROUNDGEOGRAPHICAL
LOCATION OF UGANDAUganda lies in sub-
Saharan Africa.It is a land locked
country in east Africa bordering Kenya to the east, Tanzania and Rwanda to the south, Democratic Republic of Congo to west and Sudan to the north.

Background Covers an area of
236,036 km2 with an estimated population of 30 million people and an average population growth rate of 3.2% (population secretariat Uganda 2007).
Majority of Ugandans (88%) live in rural areas where subsistence agriculture is the source of food and income.
Ugandan women preparing a meal (above) and men transporting matooke (plantain) to the market (below)

Africa carries 25% of the world’s disease burden; However she has 3% of the world’s health workers and 1% of the world’s economic resources.
(Robinson M, Clarke P Lancet 2008)
Patients with liver disease
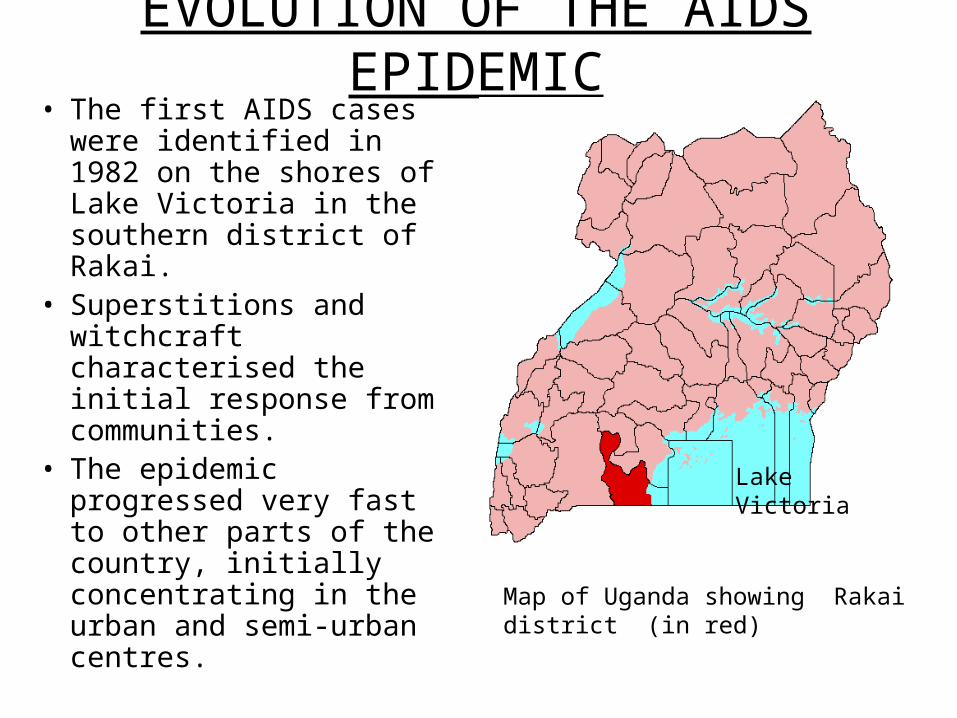
EVOLUTION OF THE AIDS EPIDEMIC• The first AIDS cases were
identified in 1982 on the shores of Lake Victoria in the southern district of Rakai.
• Superstitions and witchcraft characterised the initial response from communities.
• The epidemic progressed very fast to other parts of the country, initially concentrating in the urban and semi-urban centres.
Map of Uganda showing Rakai district (in red)
Lake Victoria
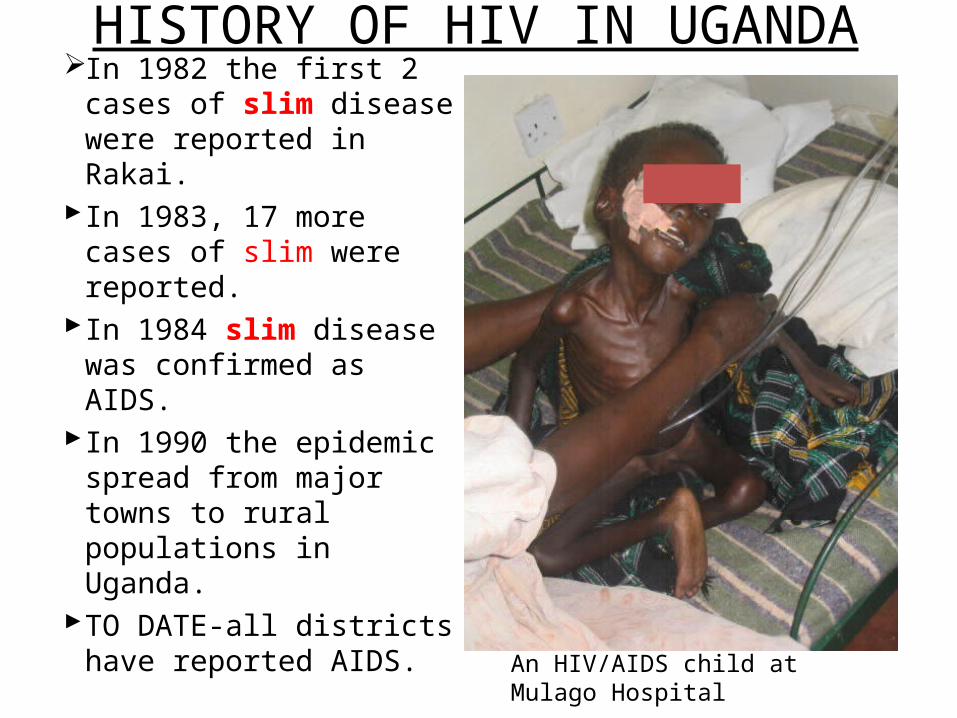
HISTORY OF HIV IN UGANDAIn 1982 the first 2 cases
of slim disease were reported in Rakai.
In 1983, 17 more cases of slim were reported.
In 1984 slim disease was confirmed as AIDS.
In 1990 the epidemic spread from major towns to rural populations in Uganda.
TO DATE-all districts have reported AIDS. An HIV/AIDS child at Mulago
Hospital
HIV/AIDS EPIDEMIOLOGICAL TRENDS IN UGANDA
• Sub-Saharan Africa accounts for 68% of those living with HIV/AIDS globally (UNAIDS 2007).
• Uganda was among the first hard hit countries with a prevalence rate of 9% from 1987 to 1988.
• In 1992 the prevalence rate was 18.3% in rural areas and 30% in the towns.
• From 1993-2002 prevalence rate was 6%.• The current prevalence rate is 6-8%. Women
8% and 5% in men.

ROUTES OF TRANSMISSION OF HIV IN UGANDA
• Heterosexual transmission accounts for 84%.• Mother to child transmission accounts for
14%.• Contaminated blood/blood products, use of
un-sterilised needles and syringes, and use of un-sterilised instruments all account for 2%.

HIV/AIDS FUNDING IN UGaNDA• U.S Presidential Emergency plan for AIDS
Relief(PEPFAR) contributes 75%• The Global fund to fight Malaria,HIV and
Tuberculosis set up by G8 in 2002• International non governmental organisations 20%• Government of uganda allocates 5% ($ 30 m) for
HIV/AIDS• $ 1 is sufficient to buy antiretroviral therapy for
one patient per day but unfortunately majority of Ugandans can’t afford a dollar per day.
NATIONAL RESPONSE TO HIV/AIDS• Response confined to Ministry of Health 1982-
1984. • Disease viewed as witchcraft and later the
disease of the immoral.• In 1985, the national committee for the
prevention of AIDS was established.• In the same year, the first AIDS control program
in the country was established.• In 1987, HIV/AIDS was declared a public health
problem and also a socio-economic disaster that called for interventions from all sectors.
• AIDS control projects started in 12 ministries.
UGANDA AIDS COMMISSION• Established in 1992 with the following
objectives;-prevention of HIV with a focus on
children, youth and gender issues (gender based violence,).
-mitigating the health and socio-economic impact of AIDS.
-a national information base for HIV/AIDS.-capacity building and research in
HIV/AIDS.-planning, monitoring and evaluation
National HIV/AIDS programmes.
The AIDS support organisation(TASO)• Founded in 1986 by Noerine Kaleeba and 15 colleagues
most of whom have died. With the following objectives 1. Fight discrimination and stigma.2. Provide counselling services for HIV/AIDS patients and
their families.3. Complement available medical services (antiretroviral
therapy)4. Sensitise the public and promote positive attitudes
towards people with HIV/AIDS and their families.5. Provide material support to clients and their families e.g
food.6. Build and support community-based efforts initiated to
respond to the AIDS epidemic.

Makerere university HIV/AIDS projectsInfectious disease institute(IDI)
was opened in 2004 as a collaboration between Makerere University and Pfizer. It offers training, research, prevention, care and treatment services.
Makerere University Walter Reed Project. A collaboration between Makerere & Walter Reed institute of research (U.S Army) in HIV Vaccine development
Makerere - Mbarara Universities joint AIDS programme (MJAP) collaboration in Study of Effects of Antiretroviral therapy, teaching of service providers
IDI building (above) and Makerere main building (below)
• Joint clinical research centre (JCRC)Founded in 1990 as a joint project of the Ministries of Health, Defence and Makerere University.Early on, 70% of HIV patients received their Antiretroviral therapy from JCRC.
• Baylor College of Medicine Children foundation, cares for children infected or exposed to HIV, teaching and research
• Makerere-Johns Hopkins University research collaboration in Prevention of Mother to Child HIV Transmission
Baylor college of medicine (above) and JCRC ART clinic launch below

Trends in the prevalence of AIDS in Uganda3 phases:Phase 1: Rapid spread and increase
in prevalence from 1982-1991. Phase 2: Dramatic decline in
prevalence From 1992-2000 during which
period, HIV prevalence fell drastically from 15% in rural areas and over 30% in cities to around 5% in 2001.
Phase 3: Stabilisation of prevalence rate at 6-7% from 2002-2005.
Phase 4: HIV prevalence rate may be increasing again?
Reasons for Change in TrendsPhase 1 Lack of knowledge about the
disease Lack of treatmentPhase 2 Death Decline in new infections due to
behavioural change (ABC) and the sheer scale of HIV epidemic
Phase 3 Free HIV drugs.HIV is no longer
an immediate death sentencePhase 4: Economic crisis, NGOs have
cut funding and some HIV centres have closed
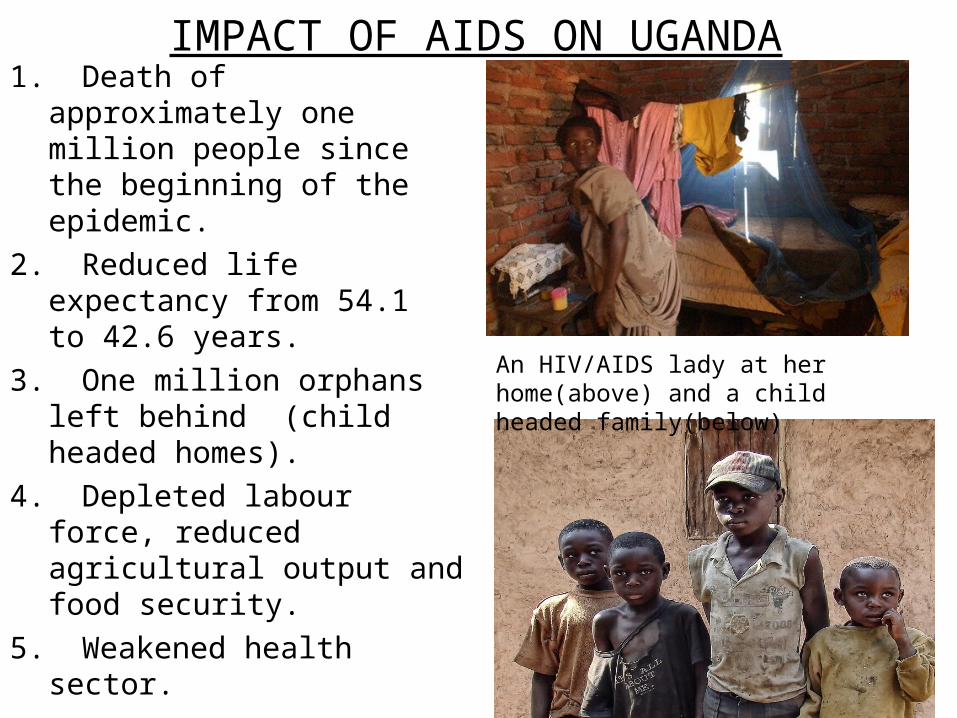
IMPACT OF AIDS ON UGANDA1. Death of approximately
one million people since the beginning of the epidemic.
2. Reduced life expectancy from 54.1 to 42.6 years.
3. One million orphans left behind (child headed homes).
4. Depleted labour force, reduced agricultural output and food security.
5. Weakened health sector.
An HIV/AIDS lady at her home(above) and a child headed family(below)
6. Increased poverty at the household level7. Stigma and discrimination at all levels of
society8. Increased school drop-outs due to lack of
school fees and also to care for the sick “If someone in Uganda tells you they have not
been affected by HIV/AIDS, then they are lying”
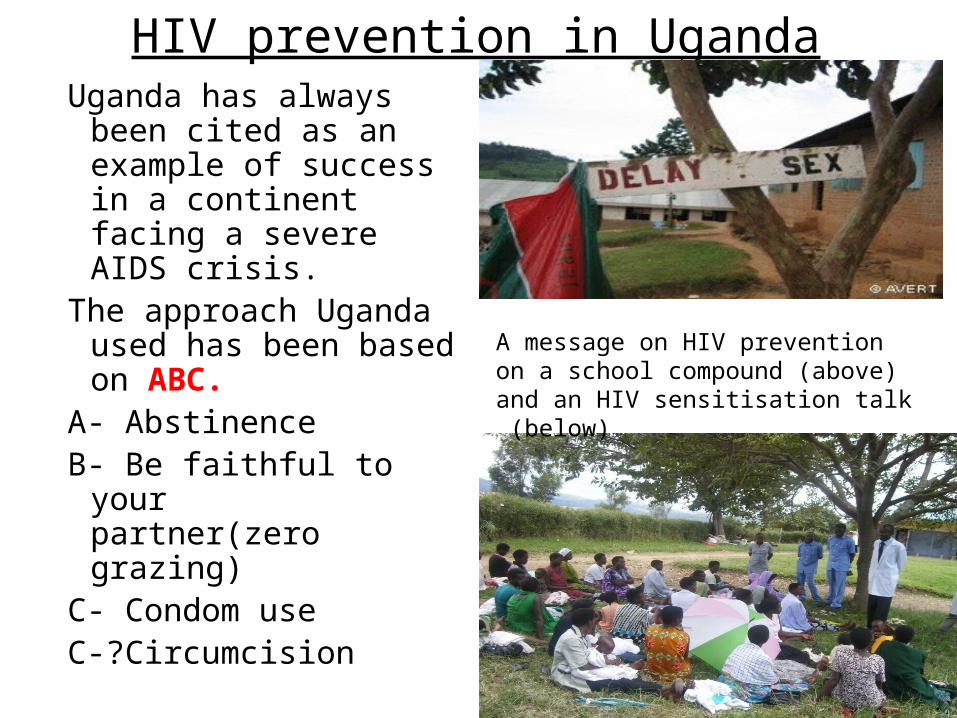
HIV prevention in UgandaUganda has always been
cited as an example of success in a continent facing a severe AIDS crisis.
The approach Uganda used has been based on ABC.
A- Abstinence B- Be faithful to your
partner(zero grazing)C- Condom useC-?Circumcision
A message on HIV prevention on a school compound (above) and an HIV sensitisation talk (below)

Prevention of Mother To Child Transmission (PMTCT)
Started in 2000 in a small number of Antenatal clinics. The programme includes;
1. Voluntary counselling and testing (VCT) for mothers attending ANC.
2. Treatment of mothers and children following positive diagnosis.
Currently 80% of pregnant mothers receive PMTCT.
A pregnant mother receiving PMTCT services at a health centre in Kampala, the capital city of Uganda
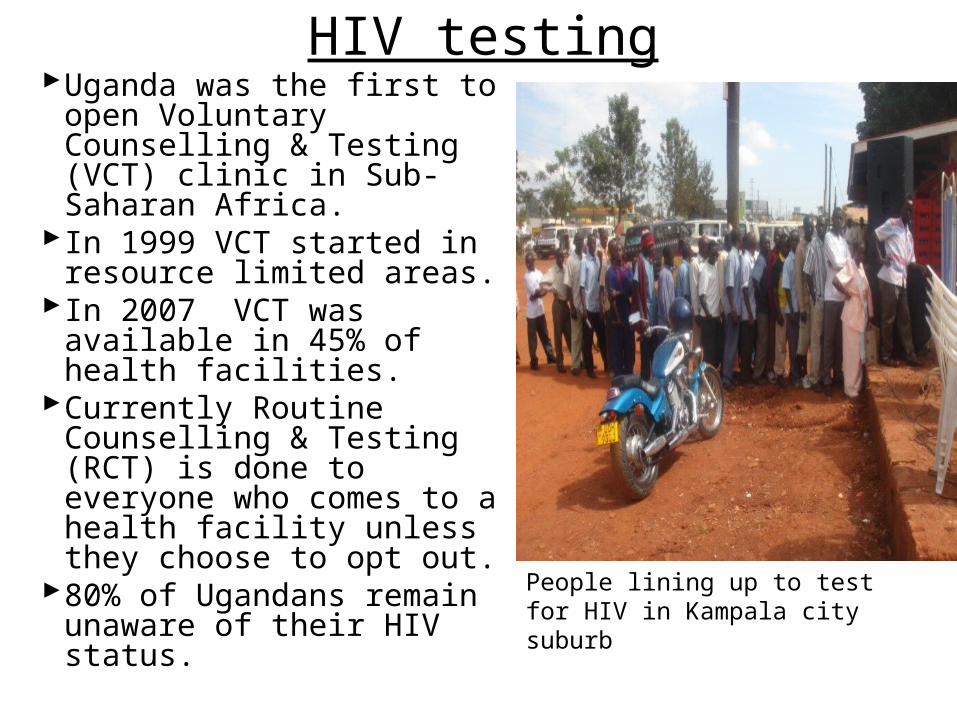
HIV testing
People lining up to test for HIV in Kampala city suburb
Uganda was the first to open Voluntary Counselling & Testing (VCT) clinic in Sub-Saharan Africa.
In 1999 VCT started in resource limited areas.
In 2007 VCT was available in 45% of health facilities.
Currently Routine Counselling & Testing (RCT) is done to everyone who comes to a health facility unless they choose to opt out.
80% of Ugandans remain unaware of their HIV status.
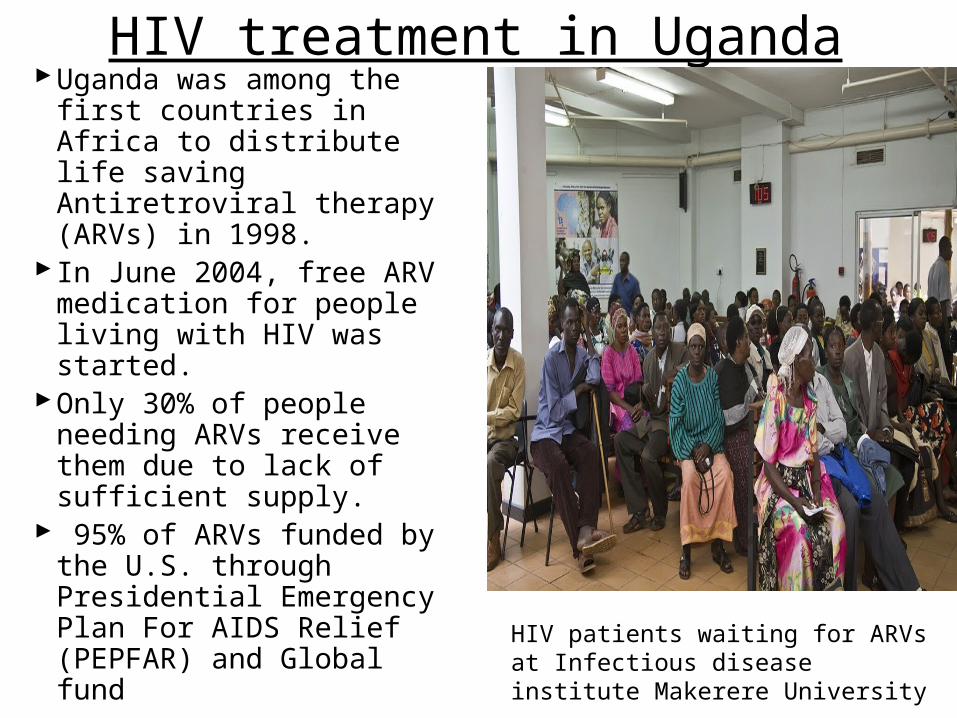
HIV treatment in UgandaUganda was among the first
countries in Africa to distribute life saving Antiretroviral therapy (ARVs) in 1998.
In June 2004, free ARV medication for people living with HIV was started.
Only 30% of people needing ARVs receive them due to lack of sufficient supply.
95% of ARVs funded by the U.S. through Presidential Emergency Plan For AIDS Relief (PEPFAR) and Global fund
HIV patients waiting for ARVs at Infectious disease institute Makerere University
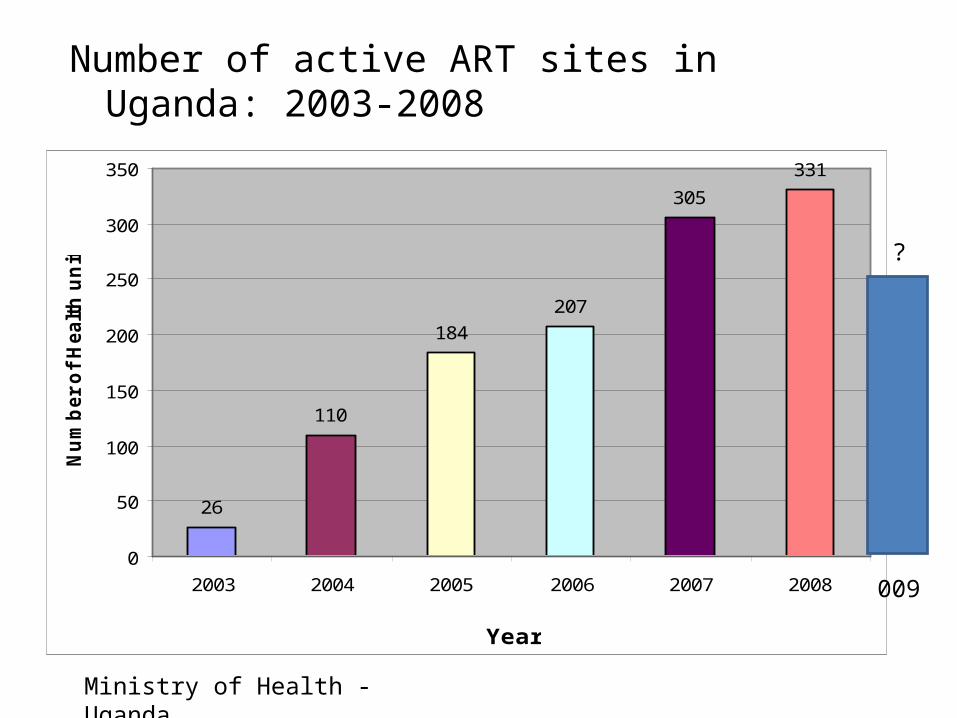
Number of active ART sites in Uganda: 2003-2008
26
110
184
207
305
331
0
50
100
150
200
250
300
350
2003 2004 2005 2006 2007 2008
Year
Nu
mb
er
of
Healt
h u
nit
s
Ministry of Health - Uganda
?
009

Common Opportunistic infections• TB. Uganda is 15th
among the 22 TB High Burden Countries (HBCs). High association of TB & HIV (40-50% TB are HIV+).
• Kaposi Sarcoma(48.9 of cancers in men and 17.9 in women)
• Cryptococcus Meningitis(10-30%)
• Pneumocysts Carinii neumonia(16.5%)
• Candidaisis(80-90%)Mulago Hospital
Cutaneous KS(above) and Oral Candidiasis(below)
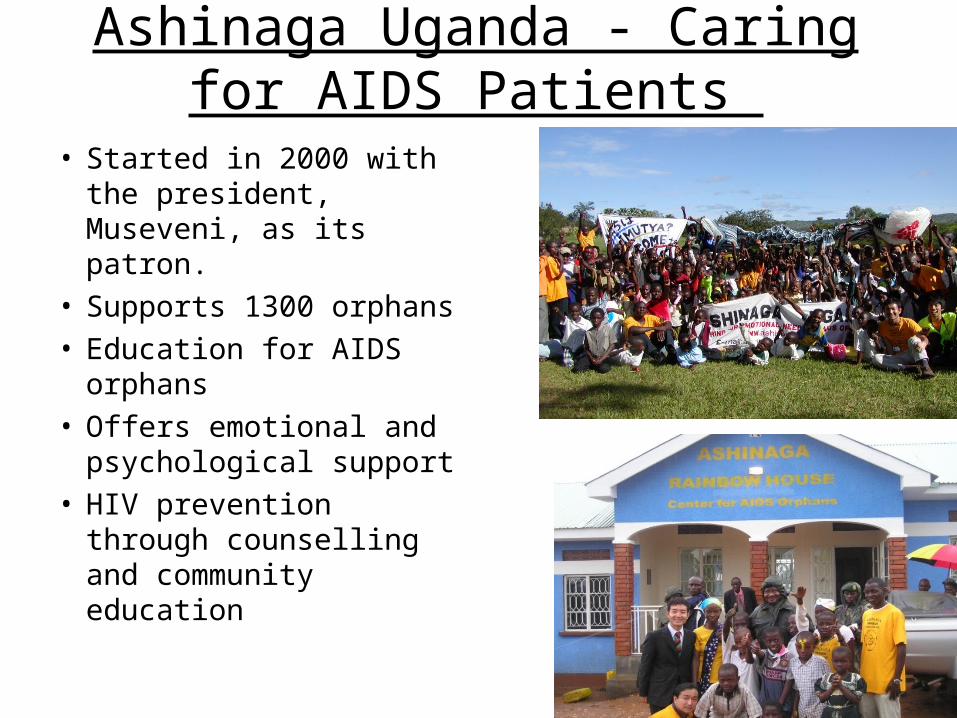
Ashinaga Uganda - Caring for AIDS Patients
• Started in 2000 with the president, Museveni, as its patron.
• Supports 1300 orphans• Education for AIDS
orphans• Offers emotional and
psychological support• HIV prevention through
counselling and community education

Challenges• HIV prevalence is high among the married, this
increases transmission to children.• Religious leaders preach against condom use.• Some religious groups discourage use of
antiretroviral therapy and encourage patients to concentrate on prayers.
• 95% of ART is donor funded.• Political instability especially in northern Uganda.• Limited resources for research about HIV in Uganda.• Corruption: Global fund suspended funding in 2005
due to financial mismanagemant.• Economic crisis. Reduced funding by international
organisationsS

ProposalCollaboration between Universities in Africa
and U.S.A both in research and student exchange programs is necessary, particularly in basic science research in HIV where little basic research has been done in Africa
To establish a basic HIV/AIDS research centre in Africa in future.
To accelerate basic reseach to deveop new and more effective antiretroviral drugs that are affordable to HIV/AIDS patients.

BACKGROUND: HIV –ASSOCIATED METABOLIC SYNDROME
The introduction of highly active antiretroviral therapy (HAART) has drastically improved the life expectancy of patients with acquired immunodeficiency syndrome (AIDS), by reducing infection-related mortality. There has, however, been an increasing adverse events,such as metabolic derangements, related to HAART, especially with regimens containing protease inhibitors. These metabolic complications include insulin resistance, diabetes mellitus, dyslipidemia and lipodystrophy. All of these complications are associated with increased risk for atherosclerosis and cardiovascular disease
Research Project
Background: A Role of Tat in HIV associated metabolic syndrome
The etiology of human immunodeficiency virus (HIV)-associated metabolic syndrome appears to be multifactorial. Other than the anti-viral drugs, HIV-1 infection itself, including virally encoded molecule, Tat (Transactivator of transcription), has been proposed as a major contributor to the development of these pathologic changes and/or the vulnerability of patients to the adverse effects of HAART.
The Human immunodeficiency virus type 1 (HIV 1) Tat protein is also a major viral transactivator required for HIV replication.
Nonetheless, neither the approach nor the management of the HIV patient with metabolic syndrome has been established

BACKGROUND: Sirt1 and Tat in HIV infectionSirt1 is NAD+-dependent deacetylase and the closest mammalian
homologue of the yeast longevity gene, Sir2 (silent information regulator 2). Sirt1 plays important roles in metabolism, as well as DNA repair, transcriptional regulation and apoptosis. Sirt1 deacetylates a variety of substrates, including p53, PPAR-γ, FOXOs and NF-κB. Importantly, activation of Sirt1 improves insulin sensitivity and ameliorates obesity-induced diabetes in mice. The clinical trial is under way to evaluate the efficacy and safety of Sirt1 activator in patients with type 2 diabetes.
A previous study has shown that Tat binds to the catalytic domain of Sirt1 and inhibits the deacetylase activity of Sirt1 and that Sirt1 deacetylates Tat and inhibits the function of Tat
Sirt1 Tat

In HIV1 Infection:
A Novel Drug candidate Compound A can block the inhibition of Sirt1 by Tat and can inhibit Tat activity by enhancing Sirt1 –mediated deacetylation of Tat.
Sirt1 activity
Tat
Insulin resistance Promotion of HIV replication, aggravation of HIV related symptoms
Sirt1 activityTat
activity
Compound A

AIM: To identify a compound which can block the binding of Tat to Sirt1
METHODS: Cos-7 cells were co-transfected with HA-Tat and Flag-Sirt1; the cells were then treated with different concentrations of compound A
Protein expression of Sirt1 and Tat was assayed by western blotting using Anti-Flag antibody and Anti-HA antibody
The effect of Compound A on Sirt1 activity and Sirt1-Tat interaction was determined by western blotting using Anti-acetyl lysine antibody and immunoprecipitation using Anti-flag antibody respectively

Immunoprecipitation with Anti-Flag antibody of cell-lysate co transfected with Sirt1-Flag and Tat-HA
IgG heavy chain
IgG light chain
HA-Tat

RESULTS:Western blotting witha) Anti-Flag antibody
Flag-Sirt1
b) Ant-HA antibody
HA-Tat
1 2 3 4
1 2 3 4
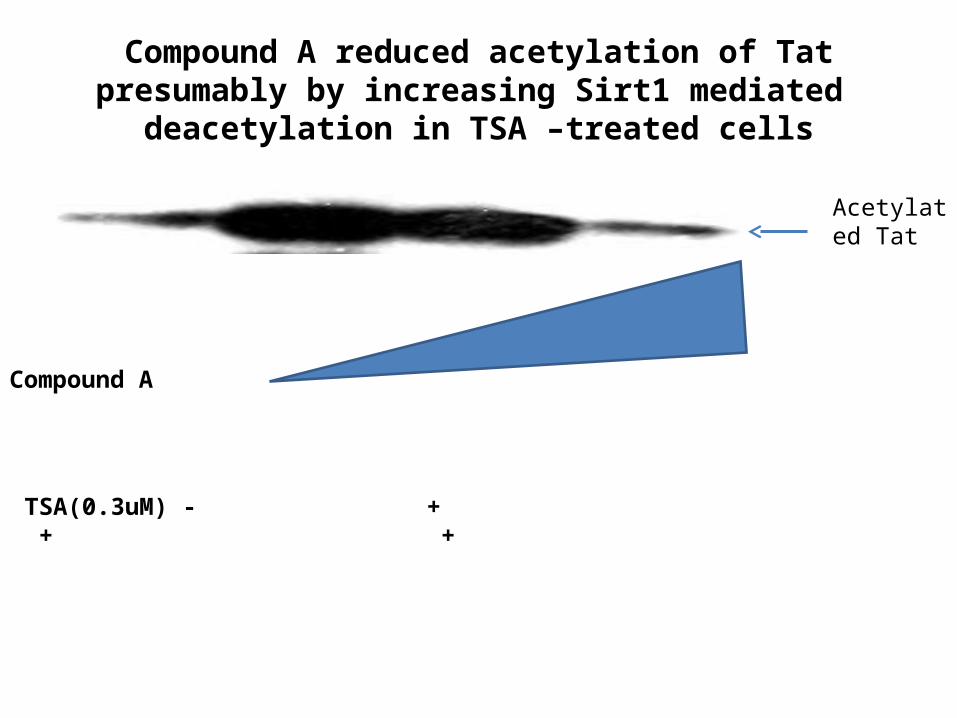
Compound A reduced acetylation of Tat presumably by increasing Sirt1 mediated deacetylation in TSA –treated cells
Compound A
TSA(0.3uM) - + + +
Acetylated Tat
KEY FINDINGS:1.Compound A decreased Tat acetylation in a
dose dependent manner in TSA treated cells.2.Compound A blocked the binding of Tat to
sirt1.DISCUSSION: Compound A and its derivatives which
can block the binding of of Tat to Sirt1 while reducing the acetylation of Tat may be a potential drug candidate to prevent and/ treat HIV infection and HIV –related metabolic syndrome by inhibiting Tat activity while activating Sirt1.

Acknowlegement1.Endocrine society for the sponsorship2.My mentor: Prof Masao Kaneki3.Faculty of Medicine Makerere University
Thank you for listening
Welcome to Kampala, Capital city of Uganda

















