Optimizing therapy for locally advanced larynx cancer: techniques, advances and trials of RT-based therapy Yong Chan Ahn, MD, PhD Dept. of Radiation Oncology Samsung Medical Center Sungkyunkwan University School of Medicine
Transcript
Optimizing therapy for locally advanced larynx cancer:
techniques, advances and trials of RT-based therapy
Yong Chan Ahn, MD, PhD Dept. of Radiation Oncology
Samsung Medical Center
Sungkyunkwan University School of Medicine
2007, Green
Goals in HNC Management
• Early stage disease (stage I/II):
– 40% of patients.
– Single modality (surgery or RT alone) is
recommended.
– Two modalities result in similar LC and OS.
• Locally advanced disease (stage III/IV):
– 60% of patients.
– Combined modality is recommended.
2007, Green
EBM and RT technique
• 3-D CRT remains minimal standard of RT
technique.
• Whenever possible, IMRT should be
implemented.
2007, Green
EBM for CRT
• Level 1 evidence showed in favor of CCRT
in advanced HNSCC.
• DM rate remains high (15%~20% at 5 years),
which might be reduced by Ind CTx + CCRT.
• Ind CTx + CCRT is not supported by level 1
evidence and should remain investigational.
• RT alone remains alternative to CCRT to unfit
patients to CCRT (>70 years, heavy
comorbidities).
2007, Green
2007, Green
2007, Green
2006, JCO
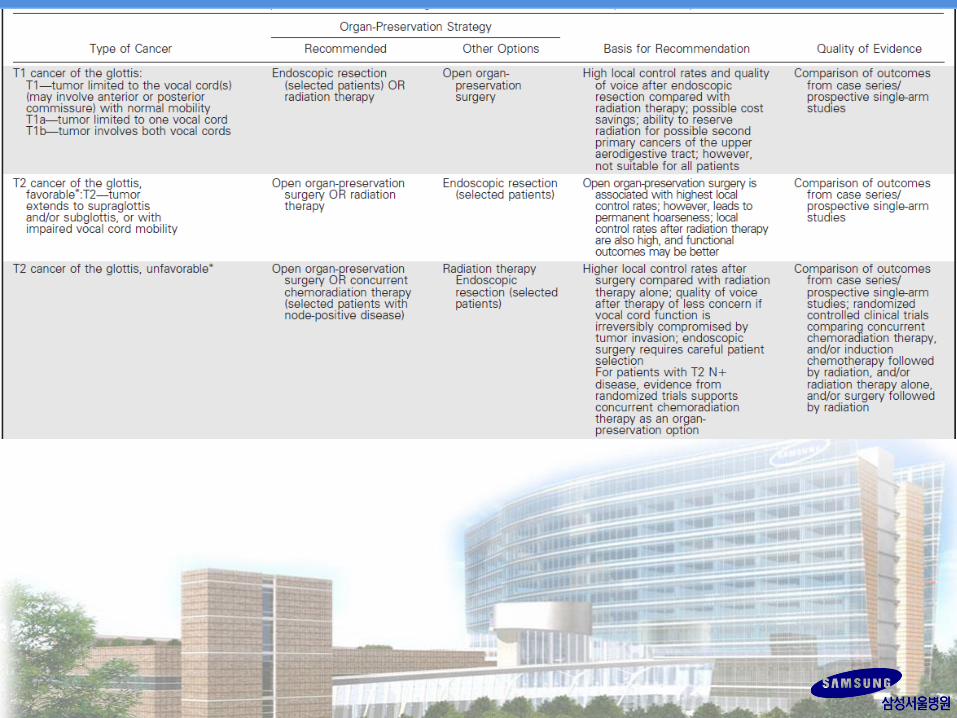
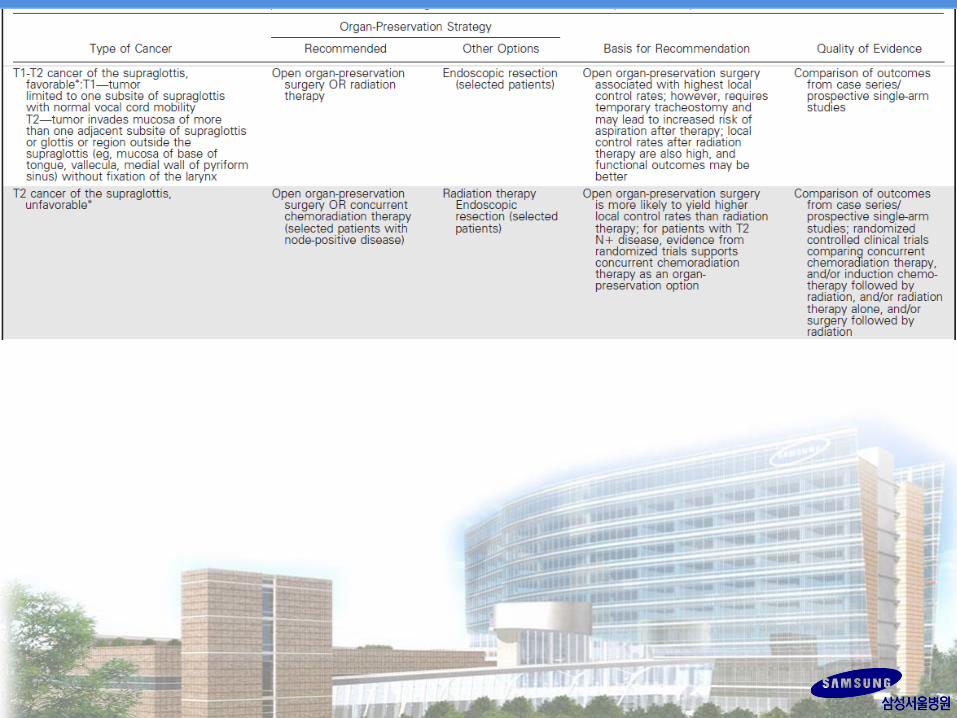
Summary of ASCO Panel (2006)
• All patients with T1-2 laryngeal cancer, with rare
exception, should be treated initially with intent to
preserve larynx.
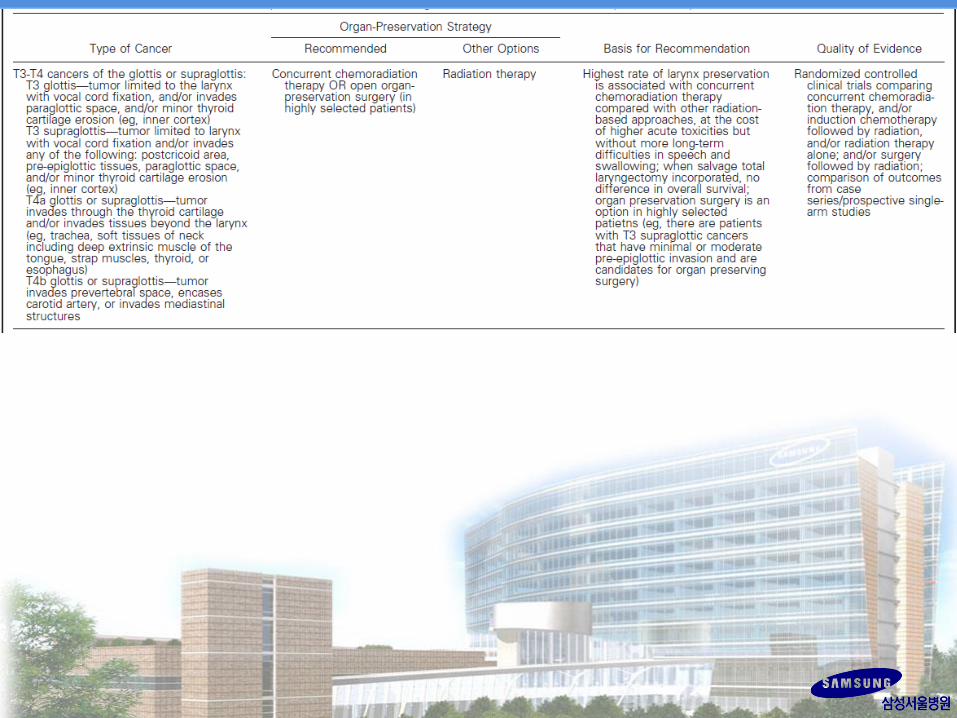
• For most patients with T3-4 disease without tumor
invasion through cartilage into soft tissues, LP approach
is appropriate, standard treatment option, and CCRT is
most widely applicable approach.
• To ensure optimum outcome, special expertise and
multidisciplinary team are necessary, and team should
fully discuss with patient advantages and disadvantages
of LP options compared with treatments that include TL.
2009, HN
2009, HN
Question 1
• Q1: Which patients are suitable for LP trials? Once
selected, what are stratification variables of highest
importance to obtain most valuable information from
randomized trials?
• A1: Trial population should include patients with
T2-3 laryngeal or hypopharyngeal squamous cell
carcinoma not considered for partial laryngectomy
and exclude those with laryngeal dysfunction or age
more than 70 years.
2009, HN
Question 2
• Q2: What are optimal assessments to conduct in
patients enrolled in LP trials to assess risks and
benefits of study treatment?
• A2: Functional assessments should include speech
and swallowing. Voice should be routinely assessed
with a simple, validated instrument.
2009, HN
Question 3
• Q3: What are optimal endpoints to use in LP trials?
How are these endpoints defined?
• A3: Primary endpoint should capture survival and
function. Panel created new endpoint: laryngo-esophageal
dysfunction-free survival. Events are death, local relapse,
total or partial laryngectomy, tracheotomy at 2 years or
later, or feeding tube at 2 years or later. Recommended
secondary endpoints are OS, PFS, LRC, time to
tracheotomy, time to laryngectomy, time to discontinuation
of feeding tube, and QoL/patient reported outcomes.
2009, HN
Question 4
• Q4: What are most promising translational research
opportunities that should be explored? What clinical
trial practices will foster translational research?
• A4: Correlative biomarker studies for near-term
trials should include EGFR, ERCC-1, Ecadherin and
b-catenin, epiregulin and amphiregulin, and TP53
mutation.
2009, HN
Summary
• By focusing on 3 important treatment goals
(survival, disease control, and laryngeal-
esophageal function), clinical trials can more
effectively evaluate and quantify therapeutic
benefit of novel treatment options for locally-
advanced laryngeal and hypopharyngeal cancer.
2009, HN
2014, Green
2014, Green
2014, Green
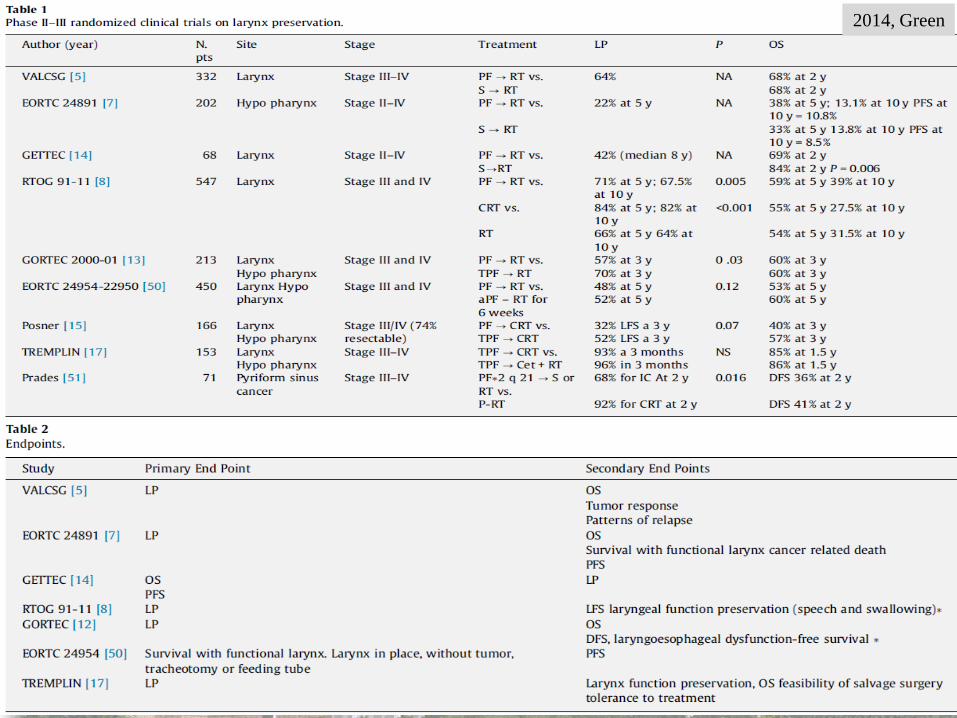
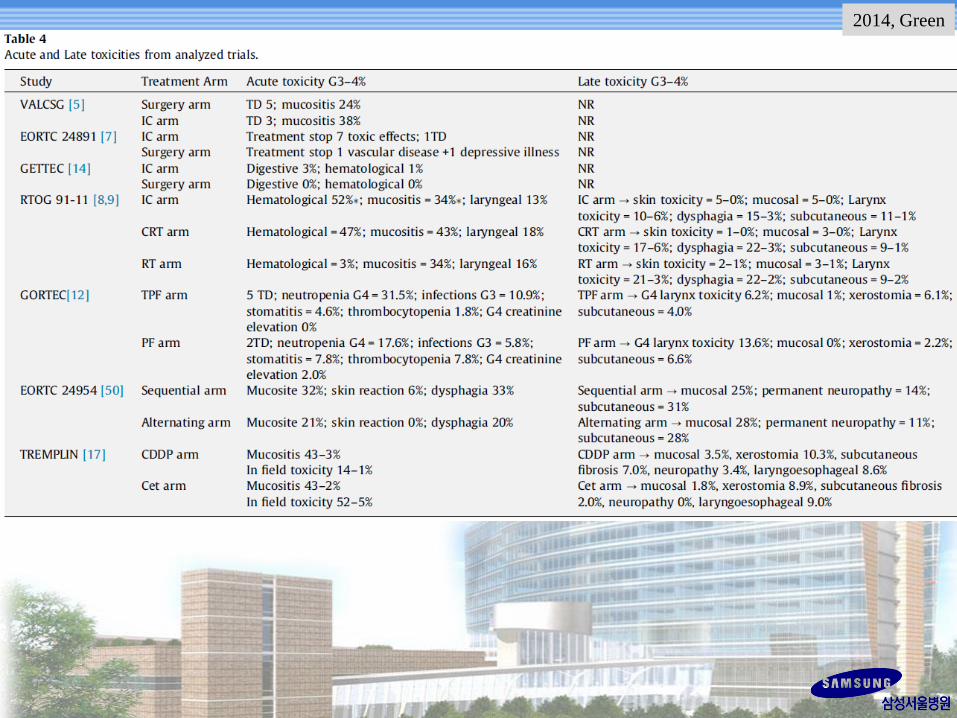
Conclusion
• LP is feasible by CCRT, alternating CRT and
Ind CTx followed by RT/CCRT.
• Still there is no one standard LP treatment
accepted worldwide.
• Heterogeneity exists both for population and
endpoints.
– LP endpoint – local cure vs. functional outcomes.
– Primary endpoint combining survival and function is
recommended.
2014, Green
Conclusion
• Optimal LP approach has yet to be determined
and clinical investigations are warranted.
• Next generation LP trials:
– should compare standard Tx (alternating CRT, CCRT,
Ind CTx + RT) with emerging approaches (Ind TPF +
RT, CCRT or Cetuximab-RT).
– should be conducted in accordance with recently
developed consensus guidelines.
2014, Green
2015, OL Clin NA
Larynx Function after RT
• Organ and function preservation are not
necessarily synonymous.
• Current evidence documents high rates of
locoregional control and reasonably good
swallowing and voice outcome after CRT.
• Newer techniques (IMRT, IGRT or proton
therapy) can minimize swallowing dysfunction
with promising results.
2015, OL Clin NA
2015, OL Clin NA
2015, OL Clin NA
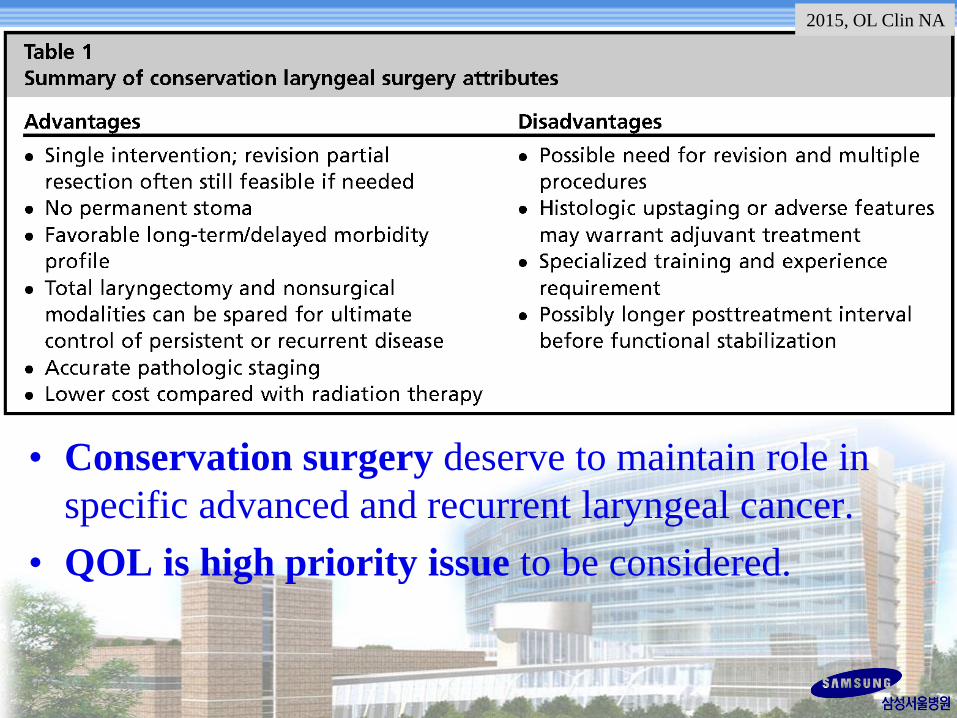
• Conservation surgery deserve to maintain role in
specific advanced and recurrent laryngeal cancer.
• QOL is high priority issue to be considered.
2015, OL Clin NA
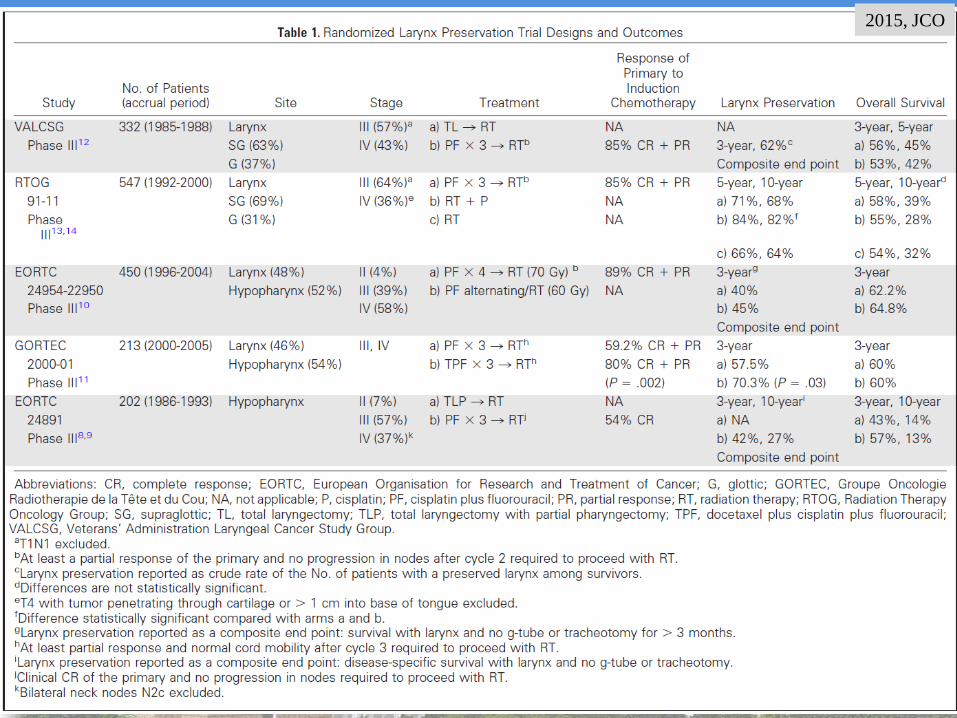
2015, JCO
2015, JCO
Locally advanced larynx cancer
• Requires experienced multidisciplinary team
evaluation and frank discussion of options and
expectations with patients.
• To achieve good function outcomes and
minimizing risk for recurrence and salvage
laryngectomy.
• Not only tumor extent and pretreatment
laryngeal function, but also expected tolerance
of treatment should be considered.
2015, JCO
Locally advanced larynx cancer
• Current level I evidence endorses
CCRT/CDDP for T2N+, T3, and selected low
volume T4 tumors.
• Carboplatin or cetuximab instead of CDDP
concurrent with RT could be considered.
• Induction TPF + RT (lower-level evidence).
• Induction chemo + CCRT (investigational).
2015, JCO
Locally advanced larynx cancer
• Endoscopic resection is as single modality for
early-stage larynx cancer, if likelihood of
positive margin is low.
• For more advanced disease, patients suitable
for endoscopic resection must be carefully
selected by skilled, experienced team.
2015, JCO
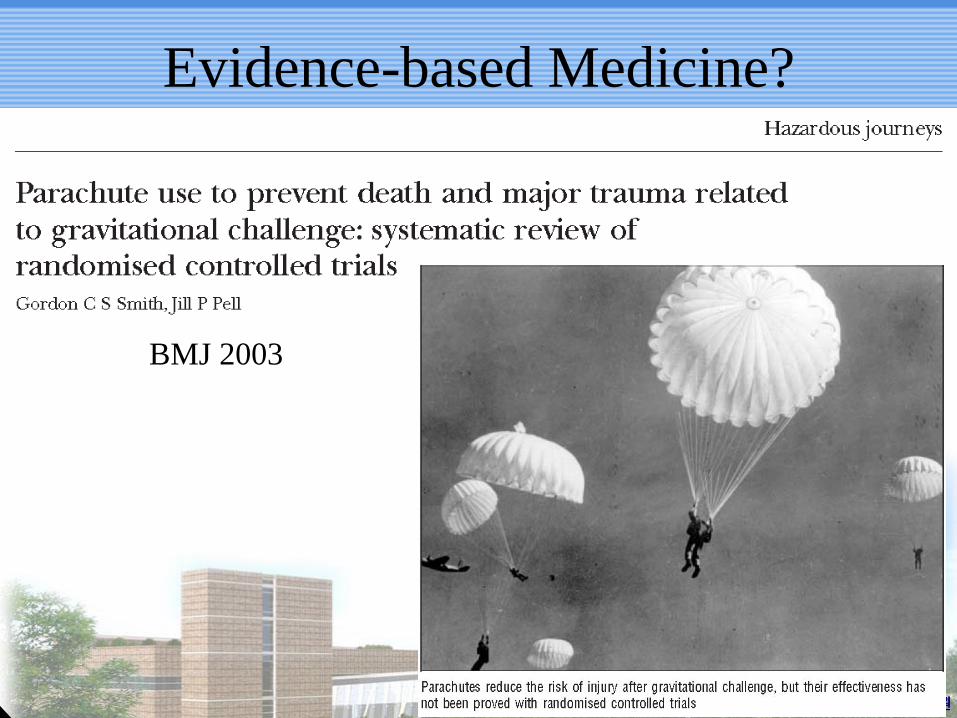
Evidence-based Medicine?
BMJ 2003
Natural history of gravitational challenge
• Effectiveness needs to be judged:
– Intervention vs. non-intervention
• Natural history of free fall:
– Survival has been reported after gravitation
challenges of more than 10,000 meters.
– Use of parachutes is associated with morbidity and
mortality.
• Studies are required to calculate balance of
risks and benefits of parachute use.
Parachute and healthy cohort effect
• Possibility of selection and reporting bias:
– Jumping from aircraft without parachute -- likely to
have psychiatric morbidity
– Using parachutes – less likely to have psychiatric
morbidity
Apparent protective effect may be “healthy
cohort” effect.
Parachutes and military industrial complex
• Parachute industry has earned billions of
dollars.
• One would not be brave enough to test product
in randomized controlled trial, with vast
commercial concerns.
• Industry sponsored trials are more likely to
conclude in favor of commercial product, and it
is unclear whether results of such industry
sponsored trials are reliable.
Is preferred Tx evidence-based?
• Single modality with surgery or RT to stages
I/II (40% of patients).
• Combined modality treatment to stages III/IV
(60% of patients).
• No single therapeutic regimen offers clear-cut
superiority over others.
• Many different regimens yield little difference.
• More indicated options are not always
evidence-based.
The man jumped out without a
parachute over 7,600 m!
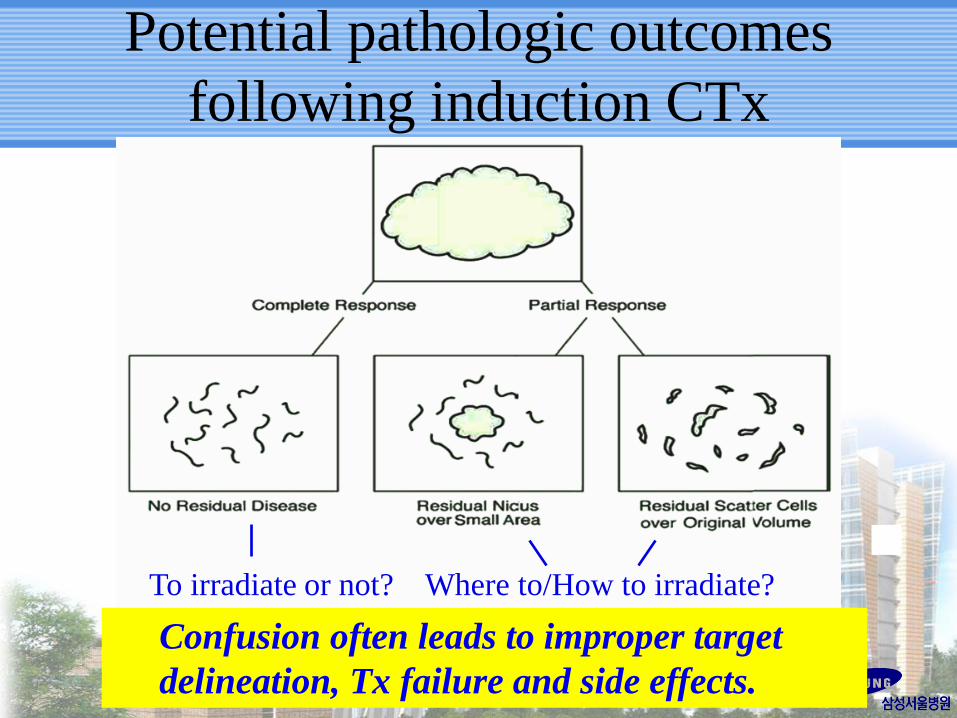
Potential pathologic outcomes
following induction CTx
To irradiate or not? Where to/How to irradiate?
Confusion often leads to improper target
delineation, Tx failure and side effects.
Summary or Personal Bias?
• For early stage disease, RT alone may be
sufficient.
• For loco-regionally advanced disease, CCRT
should be considered first (whenever possible).
– Satisfactory clinical outcomes (LC, DFS and OS)
without compromising functional impairment.
– Little confusion in target delineation as in induction