36
HODGKIN LYMPHOMA DR. AMRIT KAHLON HEMATOLOGIST, BC CANCER – ABBOTSFORD CENTER FEBRUARY 18, 2021
HODGKINLYMPHOMADR.AMRITKAHLON
HEMATOLOGIST, BCCANCER– ABBOTSFORDCENTERFEBRUARY18, 2021

CONFLICTOFINTERESTDISCLOSUREIhavereceivededucationalgrantfundingfromJanssen
IhavereceivedspeakersfeesandadvisoryboardhonorariafromJanssen,CelgeneandSanofiGenzyme

OBJECTIVES
ReviewepidemiologyandpathogenesisofHodgkinlymphomaReviewclinicalpresentationofHodgkinlymphoma
RecognizediagnosticcriteriaSummarizekeytherapeuticoptions
Reviewpost-treatmentfollow-uprecommendations

MYQUESTIONSDoyoutakecareofHodgkinlymphomapatientsinyourpractice?
1. Yes
2. No

MYQUESTIONSWhattypeofcaredoyouprovide?
1. Makingthediagnosis
2. Discussingthediagnosis
3. Managingacutesideeffectsofchemotherapy
4. Post-treatmentfollowupcare
5. 1or2or4
6. Alloftheabove

EPIDEMIOLOGY
Overallincidenceislow◦ AnnualageadjustedincidenceinpopulationsofEuropeanancestry~2-3%per100,000
◦ HLisoneofthemostcommoncancersinyoungadults
90%10%

RISKFACTORSImmunosuppresion◦ IntheHIVpopulation,cHLisoneofthemostcommonnon-AIDSdefiningcancersandisalmostalwaysEBVpositive◦ Autoimmunedisorders
Geneticriskfactors◦ GenomewideassociationstudiesinpopulationsofEuropeanancestryhaveidentified18geneticriskvariantsprimarilyinimmunerelatedgenes
Familialrisk◦ 3-5greaterriskwithafamilyhistoryofHL◦ Veryhighincidenceinidenticaltwins(~100fold)comparedtofraternaltwins
Socioeconomicstatus◦ HighersocioeconomicstatusassociatedwithNSHLandyoungerageatdiagnosis◦ LowersocioeconomicstatusassociatedwithMCHLandLDHLandolderageatdiagnosis
EBV◦ Variesbyage,geographicregion,andimmuno-competence
Connors,JMetal.NatureReviewsDiseasePrimers.2020.6:61UpToDate.Hodgkinlymphoma:Epidemiologyandriskfactors.

EPIDEMIOLOGYTRIMODALAGESPECIFICPATTERN
• 15-35years• EBVnegativeNSHL• Associatedwithhigh
socioeconomicstatus,Europeanancestry,andslightlyhigherincidenceinfemalesex
• Twosmallerpeaksinage<15yrsandelderlyadults>50yrs• EBVpositiveMCHL• Associatedwithlow
socioeconomicstatus,non-Europeanethnicity,andmalesex
Connors,JMetal.NatureReviewsDiseasePrimers.2020.6:61

PATHOPHYSIOLOGY• HodgkinandReed-Sternbergcells
• DevelopfrommalignanttransformationofdevelopingBlymphocytes
• AberrantautocrineandparacrinesignalingbyHRScells• Attractsinflammatorytumor
micro-environment• Tumormicro-environment
• Inflammatorycellinfiltrate• Supportgrowthandsurvival
ofHRScells• Allowsimmuneevasionof
tumorcells
Connors,JMetal.NatureReviewsDiseasePrimers.2020.6:61UpToDate.PathogenesisofHodgkinlymphoma.

CLINICALPRESENTATIONLymphadenopathy◦ Supra-diaphragmaticlymphadenopathy
◦ Neck– 60-80%◦ Axillary– 30%◦ Inguinal– 10%
◦ Isolatedsub-diaphragmaticlymphadenopathyisuncommon(<10%)◦ Mediastinalmass
◦ Asymptomatic,cough,SOB,retrosternalchestpain,uncommonlypericardial/pleuraleffusionorsuperiorvenacavasyndrome
Constitutional(”B”)symptoms– 40%◦ Fevers(>38C),drenchingnightsweats,unexplainedweightlossof>/=10%ofbodyweightwithin6months◦ Pel-Ebsteinfever
◦ Uncommonbutcharacteristiccyclicriseandfallinfeverover1-2weeks
Pruritus– 10-15%
Alcoholinducedpain- <10%
Connors,JMetal.NatureReviewsDiseasePrimers.2020.6:61UpToDate:ClinicalpresentationanddiagnosisofclassicalHodgkinlymphomainadults

CLINICALPRESENTATIONSpreadiscontiguousvialymphaticchannelsbeforeinvolvingmoredistantornon-adjacentsites/organs◦ Spleen,bone/bonemarrow,lung,liver◦ Rare– GI,CNS,skin,nephroticsyndrome(minimalchangedisease)
Laboratoryabnormalities◦ Anemia◦ Hypercalcemia◦ Eosinophilia◦ Other– lymphopenia,hypoalbuminemia,thrombocytosis,leukocytosis
Diseasetempo◦ Slowbutcanbevariable
Connors,JMetal.NatureReviewsDiseasePrimers.2020.6:61UpToDate:ClinicalpresentationanddiagnosisofclassicalHodgkinlymphomainadults

DIAGNOSISLymphnodebiopsy
• Excisionalbiopsypreferredtocoreneedlebiopsy
• IdentificationofHRSorLPcellsintheproperhistologicalmicroenvironment• HRSvariants(mononuclearvariants,lacunar
cells,necroticforms,areusefulforidentifyingcHLsubtypes
• Immuno-histochemicalstaining:CD3,CD15,CD20,CD30,CD45,PAX-5,EBVbyEBERandLMP1• CD30positive,variableCD15positive,CD45
negative

DIAGNOSIS/CLASSIFICATION• CLASSICALHODGKINLYMPHOMA
(90%)• NodularsclerosingHL(NSHL)–
70%• MixedcellularityHL(MCHL)–
20-25%• LymphocyterichHL(LRHL)– 3-
5%• LymphocytedepletedHL(LDHL)
– rare• NON-CLASSICALHODGKIN
LYMPHOMA(10%)• Nodularlymphocytedepleted
HL(NLPHL)
Connors,JMetal.NatureReviewsDiseasePrimers.2020.6:61

STAGINGHistoryandphysical(lymphadenopathy,abdominalorganomegaly)
Laboratoryinvestigations:CBC,renal,calcium,albumin,liverfunctiontests,HIV,hepatitisBandhepatitisCserology
Imaging◦ CTneck,chest,abdomen,andpelvis◦ PETscan
◦ Upstages41%ofpatientsfromdetectionofextra-nodaldiseaseespeciallyboneandbonemarrowdisease◦ Downstages10%ofpatients
Bonemarrowbiopsy◦ NolongerroutinelydoneifPETscanstagingavailable◦ IfPETunavailable,bonemarrowdoneif
◦ Bsymptoms◦ WBC<4x10*9/L,HGB<120g/L(women),HGB<130g/L(men),PLT<125x10*9/L
BCCancer:CancerManagementGuidelines.HodgkinLymphoma

STAGING

MANAGEMENT– ABVDCHEMOTHERAPYOriginallydevelopedin1975◦ 4drugintravenousregimen(doxorubicin,vinblastine,bleomycin,dacarbazine)◦ Itisdeliveredasanoutpatientevery14daysin28daycycles
Alternativechemotherapyregimens◦ BEACOPPchemotherapy
◦ DevelopedbytheGermanHodgkin’sLymphomaStudyGroup(GHSG)◦ ConsistsoforalprednisoneandIVbleomycin,etoposide,doxorubicin,cyclophosphamide,vincristine,procarbazine◦ ComparedwithABVD,BEACOPPimprovesPFSbutdidnotdemonstrateaclearOSadvantage
◦ ABVDvs.BEACOPP:7yearPFS73%vs.85%(p=0.004),OS84%vs.89%(p=0.39)◦ IncreasedtoxicitywithBEACOPPcomparedtoABVD
◦ StanfordV◦ Notcommonlyused◦ Combinesabriefintensivechemotherapyregimenwithradiationtherapyusinglessdoxorubicinandbleomycin◦ NoPFSorOSdifferencecomparedtoABVD
BonadonnaGetal.Cancer1975;36(1):252.VivianiSetal.NEJM.2011;365(3):203.UpToDate.Initialtreatmentofadvanced(stageIII-IV)classicalHodgkinlymphoma

ABVD– SIDEEFFECTSNeutropenia(34%),nausea/vomiting(13%),alopecia(34%)◦ Severeinfections(2%),anemia(5%)andthrombocytopenia(3%)arerare
Bleomycininducedpulmonarytoxicity(20-30%)◦ Developssubacutelywhileontherapyoruptosixmonthsposttreatment
◦ Mortalityrateof4.2%anddecreased5yearOS(63%vs.90%)
◦ Acutereactions:fever,hyperpyrexiasyndrome,anaphylactoidreactions◦ Latebleomycin-relatedpulmonarytoxicity– pulmonaryfibrosis
◦ Riskfactorsincludeage>40yrs,mediastinalradiation,useofGCSF,exposuretohighFiO2,cigarettesmoking◦ Symptomsincludedrycoughandshortnessofbreathonexertion◦ PulmonaryfunctiontestingcanshowasignificantdeclineinDLCO
Doxorubicinassociatedcardiomyopathy◦ Associatedwithtotaldose>400mg/m2(ABVD6cycles300mg/m2)◦ 7.8xhigherriskofmyocardialinfarctioncomparedtoageadjustednormalpopulation
Vinblastineassociatedperipheralneuropathy
Fertilityisgenerallypreserved◦ Moststudiesshowalowimpactonovarianreserveandfertility◦ Azoospermiaandoligospermiatendtorecovertonormalvaluesposttreatment◦ Fertilitypreservationshouldstillbediscussedinhigherriskpatients
.UpToDate.Initialtreatmentofadvanced(stageIII-IV)classicalHodgkinlymphoma

MANAGEMENT– TRADITIONALAPPROACH
Connors,JMetal.NatureReviewsDiseasePrimers.2020.6:61

PETADAPTEDAPPROACH• FDGavidPETisusedtomeasurethe
responseafterinitialbriefchemotherapytoidentifypatientswithahighqualityresponsetopermitde-escalatingintensityoftherapytoreducetoxicity• Omitradiation• De-intensifychemotherapy
• InterimFDGavidPETfollowing2cyclesofchemotherapyareusedinlimitedandadvancedstagedisease
• FDGavidPETisusedattheendoftreatmenttodistinguishbetweenfibronecroticdebrisandactivelymphomainresidualmasses
Connors,JMetal.NatureReviewsDiseasePrimers.2020.6:61

PETADAPTEDAPPROACHLIMITEDSTAGEDISEASE2cyclesABVD
PETpositive
Radiation
PETnegative
2cyclesAVD
InterimFDG-PET
• AdoptedbyBCCancerin2005
• Rationalewastominimizethelong-termtoxicityofradiationforpatientswithchemosensitivedisease
• RetrospectivereviewofBCdatafromJuly2005-April2016publishedDecember2018
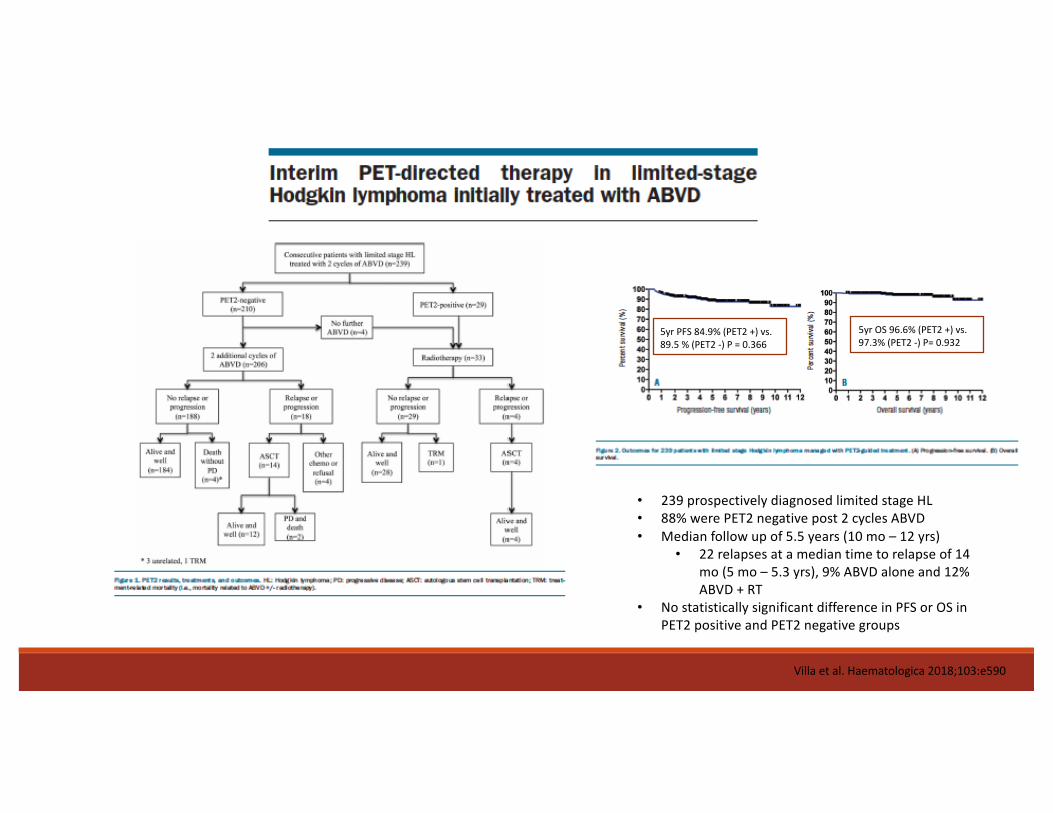
Villaetal.Haematologica2018;103:e590
• 239prospectivelydiagnosedlimitedstageHL• 88%werePET2negativepost2cyclesABVD• Medianfollowupof5.5years(10mo– 12yrs)
• 22relapsesatamediantimetorelapseof14mo(5mo– 5.3yrs),9%ABVDaloneand12%ABVD+RT
• NostatisticallysignificantdifferenceinPFSorOSinPET2positiveandPET2negativegroups
5yrPFS84.9%(PET2+)vs.89.5%(PET2-)P=0.366
5yrOS96.6%(PET2+)vs.97.3%(PET2-)P=0.932

PETADAPTEDAPPROACADVANCEDSTAGEDISEAE2cyclesABVD
PETpositive
4cyclesABVD
PETpositive-radiation
PETnegative– noradiation
PETnegative
4cyclesAVD
EndoftreatmentPET
InterimFDGPET• Rationalewastominimizelong-term
toxicityofbleomycinandradiationforpatientsdemonstratingchemosensitivedisease
• ApproachbasedonevidencefromResponseAdaptedTherapyinHodgkinLymphoma(RATHL)trial(2016)

Johnsonetal.NEJM2016;374:2419-29
• ProspectivetrialtotestaresponseadaptedapproachbasedonPET2after2cyclesABVDandmodifyingtreatmentbasedonresults
• 83.7%ofpatientshadanegativePET2
3yrPFSwas85.7%(ABVD)vs.84.4%(AVD)
3yrOSwas97.2%(ABVD)vs.97.6%(AVD)

PROGNOSISOverallapproximately90%ofpatientsintheagerangeof16-70yearscananticipatebeingcured◦ 50%ofrelapsingpatientswillbecuredwithHDT/ASCT
Limitedstagedisease◦ Cureratesare90-95%fornon-bulkystageIAorIIAdisease◦ Ariskstratificationmodelforlimitedstagediseaseisnotcommonlyused
Advancedstagedisease◦ Cureratesare70-80%foradvancedstagedisease◦ InternationalPrognosticScore(IPS)providesvalidatedestimatesofprobablePFSandOS
Connors,JMetal.NatureReviewsDiseasePrimers.2020.6:61

• IPSisthemostwidelyusedriskstratificationindexforHL• InitiallypublishedinNEJMin1998
• Isbasedonpatientstreatedbefore1992withavarietyofchemotherapyregimens+/- radiation
• Predicted5yrFFPandOSrangingfrom42%-84%and56%-89%respectively
• BCCancervalidatedthescoreinamorerecentlytreatedpatientpopulationandpublishedresultsin2012• Included740patientstreatedbetween1980to2010• TheIPSremainedprognosticforbothFFPandOS• 5yrFFPandOSrangedfrom62%-88%and67%-98%
respectively

RELAPSEDHODGKINLYMPHOMAEligiblefor
ASCT
YES
Salvagechemotherapy
HDT/ASCT
MaintenanceBrentuximab
vedotin
NO
-SingleagentBrentuximabvedotin-Pembrolizumab/nivolumab-Radiotherapyforlocalizeddisease-Palliativechemotherapy(singleagentorcombination)-Clinicaltrial
AUTOLOGOUSSTEMCELLTRANSPLANTELIGIBLEHL• Salvageregimen(GDP,ICE,DHAP)
• Gemcitabine/dexamethasone/cisplatinmostcommonlyusedinBC
• Noheadtoheadtrialstoestablishsuperiorityofoneregimenoveranother
• 2-3cyclesdeliveredpriortoproceedingwithtransplanttodemonstratechemo-sensitivedisease
• MaintenanceBrentuximabvedotin• BrentuximabisgivenIVin3weekcyclesfor
16cycles• AETHERAtrial:maintenanceBrentuximab
postASCTcanpreventapproximately1/3ofrelapsesexpectedtooccurpostASCT
Connors,JMetal.NatureReviewsDiseasePrimers.2020.6:61Moskowitzetal.Blood.Dec2018.132(25),2639.

HIGHDOSETHERAPYANDAUTOLOGOUSSTEMCELLTRANSPLANT
• AnumberofHDTregimensareinuse• BEAM,CBV– nonehasemergedassuperior
• WithcurrentsupportivecareASCTrelatedmortalityisexpectedbe<5%
• Long-termtoxicities• Infertilityinwomen>25yearsandmenof
anyage• 5-10%riskofdevelopingsecondneoplasms• Hypothyroidism
• Fiveindependentfactorsassociatedwithoutcome• Timetorelapse<3mo,stageIVdiseaseat
relapse,performancestatus(ECOG>!),largestindividualtumor> 5cm,lackofCRtosecond-linechemotherapy
Connors,JMetal.NatureReviewsDiseasePrimers.2020.6:61

ANTIBODYDRUGCONJUGATESBRENTUXIMABVEDOITIN
• Approved2011forrelapsepostASCT• ORR75%andCR34%
• Maintenancetherapyposttransplant• AETHERAtrial
• Newer1stlinecombinationAVD-BvforstageIII/IVCHL• ECHELON-1trialdemonstrated
improved2yrPFSof82.1%(AVD-Bv)vs.77.2%(ABVD)
• GreatestbenefitforpatientswithstageIVor2ormoresitesofextra-nodalinvolvement
• Maintoxicities– peripheralneuropathy
Domingo-Domenech,EVAandAnnaSureda.JClinMed.2020May;9(5):1384.

IMMUNECHECKPOINTINHIBITORS• Nivolumabandpembrolizumabavailablefor
useinCanada• Pembrolizumabapprovedforuseupto
2years• Nivolumabapprovedforuseuntil
diseaseprogressionorunacceptabletoxicity
• Nivolumabbeingtrialedin1stlinetreatmentwithAVDandincombinationwithbrentuximabandAVDandincombinationwithbrentuximabaloneinrelapsed/elderlysetting
• Maintoxicities:autoimmunecomplications
Domingo-Domenech,EVAandAnnaSureda.JClinMed.2020May;9(5):1384.

ALLOGENEICSTEMCELLTRANSPLANTLimitedroleinHodgkinlymphoma◦ Highernon-relapseassociatedmortality(NRM)(>15%)
◦ Acuteandchronicgraftvs.hostdisease(GVHD)◦ SevereopportunisticinfectionsinthecontextofGVHD
Remainsareasonableoptionforselectedfitpatients◦ OnlycurativestrategyforpatientswithHLthatrelapseafterauto-SCT◦ Diseasestatusattransplantationplaysthemostimportantrole
◦ 4yrPFSandOSwas18%and41%intheglobalpopulation◦ 4yrPFSandOSimprovedto40%and60%respectivelyforpatientsallograftedwith
chemosensitivedisease
Neweragentssuchasbrentuximabvedotinandtheimmunecheckpointinhibitorshaveprovidednewoptionsforbridgingpatientstopotentiallycurativeallogeneicstemcelltransplant
Thetimingofallogeneictransplantafterbrentuximabvedotinandimmunecheckpointinhibitortherapyremainsatopicofdiscussion
Domingo-Domenech,EVAandAnnaSureda.JClinMed.2020May;9(5):1384.

SURVIVORSHIPCARERELAPSESURVEILLANCE
MANAGEMENTOFLONGTERMCOMPLICATIONS

RELAPSESURVEILLANCERelapseSurveillance◦ 5yearriskofrelapsefromdiagnosisforallpatientsis18.1%
◦ 72%ofrelapsesoccurwithinthefirst2yearsofdiagnosis◦ Theriskofrelapsediminishesto5.6%at2yearsfromdiagnosis◦ Foradvancedstagepatientsremainingrelapsefreeat2years,the5yearriskofrelapse
is7.6%andforthreeyearspostdiagnosisiscomparabletolimitedstagepatientsat4.1%
◦ Patientsarenowbeingtransitionedtosurveillancefollowupthroughtheirprimarycareproviderat2yearspostcompletionoftreatment◦ Clinicvisitsevery6monthsforyear2-5posttreatmentandannuallyafteryear5
◦ History◦ Physicalexamincludinglymphnodeandspleenexam◦ Bloodtests(CBC,LFTs,creatinine,LDH,calcium,albumin)◦ Chestx-ray(forpatientswiththoracicdisease)everyvisitfor2yearsandthenevery
othervisit(BCrecommendation)
Hapgoodetal.JClinOncol.2016.34:2493-2500BCCancer.Cancermanagementguidelines.Hodgkinlymphoma

LATECOMPLICATIONSOFTHERAPYSecondarymalignancies– leadingcauseofdeathinsurvivorsofHodgkinlymphoma◦ Increasedriskofsolidtumorsappearsapproximately5yearsaftercompletingtherapyandcontinuestoriseforatleast20years◦ Lung,colonandbreastaremostcommonsecondarymalignancies◦ Skin,thyroid,esophagus,colon,andsarcomasoccurtypicallyintheareasofradiation◦ Solidtumorsaremorefrequentthanhematologicmalignancies
◦ TheriskofAMLpeaksat5-9yearsposttreatment◦ Screening
◦ Nogeneralconsensusregardingoptimalscreeningprogram◦ BCrecommendations
◦ “Although uncommon,certainsecondaryneoplasmsoccurwithincreasedfrequencyinpatientswhohavebeentreatedforHodgkinlymphoma.Theseincludeacutemyelogenousleukemia,thyroid,breast,lunganduppergastrointestinalcarcinomaandmelanomaandcervicalcarcinoma-in-situ.Itisappropriatetoscreenfortheseneoplasmsfortherestofthepatient'slifebecausetheymayhavealengthyinductionperiod.”
◦ Annually◦ TSHlevel(onlyifthyroidirradiated)◦ Mammographyforwomenbeginning10yearsafterdiagnosisofHodgkinlymphomaoratage40years,whichevercomesfirst◦ Papsmear
UpToDate.ApproachtotheadultsurvivorofclassicalHodgkinlymphoma.BCCancer.Cancermanagementguidelines.Hodgkinlymphoma

LATECOMPLICATIONSOFTHERAPYCardiovasculardisease– mostcommonnon-malignantcauseofdeath◦ Coronaryarterydisease,valvulardisease,pericardialdisease,arrhythmia,cardiomyopathy,andperipheralarterydisease
◦ Increasedriskemergessoonaftercompletionoftreatmentandremainselevatedforthesurvivorslifetime
◦ Riskfactors◦ Pre-existingheartdiseaseisthemostsignificantpredictorofpost-HLtherapycardiaccomplications◦ Others:chemotherapy(doxorubicin),radiationtherapy,traditionalcardiacriskfactors
◦ Screening◦ Cardiacexamandauscultationforheartmurmurs,carotidbruits◦ Screeningandmanagementofcardiacriskfactors
◦ Bloodpressuremonitoring,screeningfordiabetes,dyslipidemia◦ Smokingcessation◦ Nutritionalcounselling/obesitycontrol
◦ Counselpatientstoreportsymptomssuchasfatigue
UpToDate.ApproachtotheadultsurvivorofclassicalHodgkinlymphoma.

LATECOMPLICATIONSOFTHERAPY◦ Significantpsychosocialimpactwhichcanbepersistentandsevere◦ Cognitive◦ Emotionalfunctioning◦ Rolefunctioning◦ Socialfunctioning◦ Fatigue◦ Dyspnea◦ Sleepdisturbance◦ Financialproblems
◦ Impactcanbeinfluencedbybaselineimpactandage◦ Highertumorburdenatassociatedwithimpairedbaselinescores◦ Impactisindependentofchemotherapytype
◦ Moreliteratureisrequiredtobetterassessthelong-termpsychosocialimpactofcancertreatment
Kreissl,Setal.JCO.2020.38(25).2839.


















