PEDIATRIC ONCOLOGY 0031-3955/97 $0.00 + .20 HODGKIN’S DISEASE Melissa M. Hudson, MD, and Sarah S. Donaldson, MD Despite incomplete understanding of the pathology of Hodgkin’s disease, its cell of origin, and the molecular events that induce its malignant transforma- tion, most children diagnosed with Hodgkin’s disease will be long-term survi- vors. Many controversies still exist regarding the optimal staging and treatment of children, which has evolved over the past 30 years owing to the pioneering efforts of pediatric investigators to reduce late treatment sequelae. Today, most institutional protocols prescribe multiagent chemotherapy, either alone or in conjunction with low-dose involved-field radiation therapy for children in whom growth and development is still an issue. Recent studies indicate that ”risk- adapted” combined modality regimens of involved-field radiotherapy and three to four cycles of chemotherapy produce cure rates comparable with those using similar radiotherapy and six cycles, with fewer acute and late treatment sequelae in children with localized disease. Identification of patients at risk for treatment failure who may benefit from intensification of therapy remains a challenge for the future. Similarly, better understanding of the pathogenesis of Hodgkin’s disease may provide the basis for novel therapies that improve cure rates and reduce treatment toxicity. EPIDEMIOLOGY AND CAUSE The incidence of Hodgkin’s disease exhibits a characteristic bimodal distri- bution in regard to age.z3 In the United States and other industrialized countries, the early peak occurs in the mid to late 20s and the second peak after the age of 50. In developing countries, the early peak occurs before adolescence. Epidemiologicstudies demonstrate three distinct forms of Hodgkin’s disease, the characteristics of which suggest different causes: a childhood form, in patients 14 years or younger; a young adult form, in patients 15 to 34 years; and an older From the Department of Hematology-Oncology, St. Jude Children’s Research Hospital; the Department of Pediatrics, University of Tennessee, Memphis, College of Medicine, Memphis, Tennessee (MMH); and the Department of Radiation Oncology, Stanford Medical Center, Stanford, California (SSD) PEDIATRIC CLINICS OF NORTH AMERICA ~~ ~ VOLUME 44 * NUMBER 4 AUGUST 1997 891
Transcript
PEDIATRIC ONCOLOGY 0031-3955/97 $0.00 + .20
HODGKIN’S DISEASE Melissa M. Hudson, MD, and Sarah S. Donaldson, MD
Despite incomplete understanding of the pathology of Hodgkin’s disease, its cell of origin, and the molecular events that induce its malignant transforma- tion, most children diagnosed with Hodgkin’s disease will be long-term survi- vors. Many controversies still exist regarding the optimal staging and treatment of children, which has evolved over the past 30 years owing to the pioneering efforts of pediatric investigators to reduce late treatment sequelae. Today, most institutional protocols prescribe multiagent chemotherapy, either alone or in conjunction with low-dose involved-field radiation therapy for children in whom growth and development is still an issue. Recent studies indicate that ”risk- adapted” combined modality regimens of involved-field radiotherapy and three to four cycles of chemotherapy produce cure rates comparable with those using similar radiotherapy and six cycles, with fewer acute and late treatment sequelae in children with localized disease. Identification of patients at risk for treatment failure who may benefit from intensification of therapy remains a challenge for the future. Similarly, better understanding of the pathogenesis of Hodgkin’s disease may provide the basis for novel therapies that improve cure rates and reduce treatment toxicity.
EPIDEMIOLOGY AND CAUSE
The incidence of Hodgkin’s disease exhibits a characteristic bimodal distri- bution in regard to age.z3 In the United States and other industrialized countries, the early peak occurs in the mid to late 20s and the second peak after the age of 50. In developing countries, the early peak occurs before adolescence. Epidemiologic studies demonstrate three distinct forms of Hodgkin’s disease, the characteristics of which suggest different causes: a childhood form, in patients 14 years or younger; a young adult form, in patients 15 to 34 years; and an older
From the Department of Hematology-Oncology, St. Jude Children’s Research Hospital; the Department of Pediatrics, University of Tennessee, Memphis, College of Medicine, Memphis, Tennessee (MMH); and the Department of Radiation Oncology, Stanford Medical Center, Stanford, California (SSD)
PEDIATRIC CLINICS OF NORTH AMERICA ~~ ~
VOLUME 44 * NUMBER 4 AUGUST 1997 891
892 HUDSON & DONALDSON
adult form, in patients 55 to 74 yearsz3 Hodgkin’s disease is rarely diagnosed in children younger than 5 years of age in industrialized countries. Its incidence reveals a slight male predominance, which is most marked in patients younger than 10 years of age, whereas in adolescents, the incidence in males and females is roughly The association between Hodgkin’s disease and young pa- tients from higher socioeconomic status, a pattern similar to that seen with paralytic poliomyelitis 50 years ago, has led some investigators to attribute pathogenesis to an infectious agent.
Clustering of Hodgkin’s cases within families or races has been attributed to genetic predisposition to the disease, or to common exposure to a causal agent. Studies of familial Hodgkin’s disease have indicated increased association with specific human leukocyte antigens (HLAS).~~ Many investigators have ob- served concordance of Hodgkin’s disease in first-degree relatives, including sibling and parent-child pairs.z3 In families in which twins are concordant, an elevated risk of Hodgkin’s disease ranges from threefold among first-degree relatives to sevenfold in siblings.43 Hodgkin’s disease is also diagnosed more frequently in individuals with congenital or acquired immune system abnormali- ties, and this fact may reflect the slight increase in familial in~idence .~~
Several epidemiologic studies have suggested that infectious agents, includ- ing herpes virus 6, cytomegalovirus, and Epstein-Barr virus (EBV), may be involved in the transmission of Hodgkin’s disease. Enhanced activation of EBV, suggested by the high EBV antibody titers observed in many patients, and in situ hybridization evidence of EBV genomes in Reed-Stemberg cells,6” support the hypothesis that EBV may play a role in the pathogenesis of Hodgkin’s disease. A number of EBV-associated antigens have been detected in Hodgkin’s specimens.” Expression of the EBV latent membrane protein (LMP) varies among the histologic subtypes and is found in up to 96% of mixed cellularity cases, 34% of nodular sclerosing cases, and 10% of lymphocyte predominance cases. Both Reed-Stemberg cells and their variants consistently express Epstein- Barr nuclear antigen (EBNA)-1, but EBNA-2, viral capsid antigen (VCA), early antigen, and membrane antigen have not been found.24 These data suggest that EBV, either alone or with other carcinogens, may play a direct role in the pathogenesis of Hodgkin’s disease.
CELL OF ORIGIN
The histology of Hodgkin’s disease is unusual because of the reactive infiltrate of normal lymphocytes, plasma cells, and eosinophils that accompanies the malignant Reed-Sternberg cells. The cellular origin of the Reed-Stemberg cell remains controversial, and its immunophenotype varies with the histologic subtype of Hodgkin’s disease. Recent investigations of Hodgkin’s and Reed- Sternberg cells have documented the expression of surface markers consistent with a T- or B-lymphocyte Hodgkin’s specimens usually do not express myeloid or monocytic antigenic markers with the exception of CD15 (Leu-Ml), which is found in a high proportion of cases with nodular sclerosing, mixed cellularity, or lymphocyte-depleted histology. Conversely, nodular lymphocyte- predominant Hodgkin’s disease expresses the leukocyte common antigen and B- cell-specific J chain but is negative for CD15, consistent with a B-cell malignancy.
Immunophenotyping of Hodgkin’s and Reed-Stemberg cells has also indi- cated expression of a number of activation antigens, including the interleukin-2 (IL-2) receptor, Ki-1 (CD30), the transferrin receptor, and HLA DR epitopes.48, 59
Of these, the levels of soluble serum CD30 have been shown to correlate with
HODGKINS DISEASE 893
disease activity. High serum IL-2 levels also have been correlated with poor prognosis in children with Hodgkin’s disease?* Production of other cytokines by Hodgkin’s and Reed-Stemberg cells is thought to be responsible for many of the nonspecific clinical features in patients with Hodgkin’s disea~e.’~
PATHOLOGY
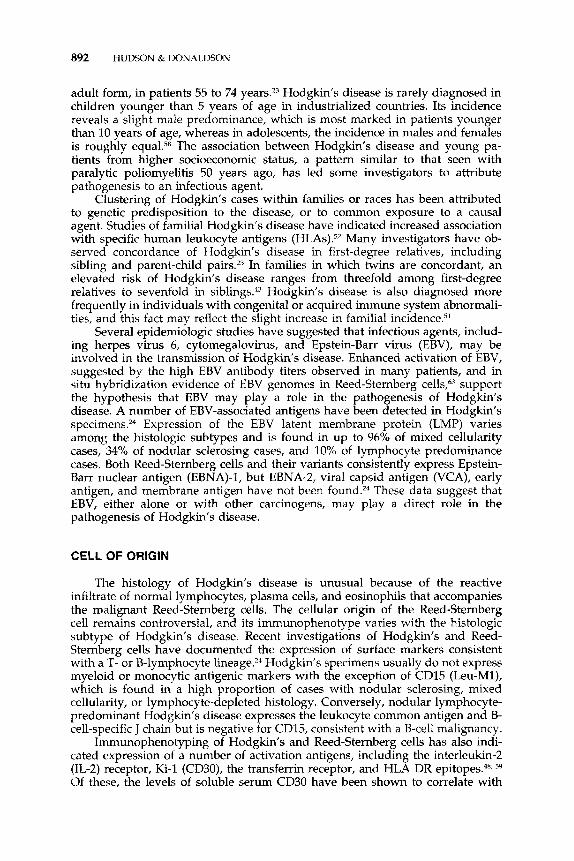
Reed-Sternberg cells are large (1545 pm in diameter), with abundant cyto- plasm and either multiple or multilobed nuclei. The nuclear membrane is usually intensely stained, and the delicate chromatin network within it typically gives way to a peculiar halolike clear zone around the nucleolus. The nucleoli are also large and prominent (Fig. 1). One variant of the Reed-Sternberg cell is the lacunar cell, characteristically seen in nodular sclerosing disease. This variant appears as a cell in a space due to the artifactual retraction of the abundant pale cytoplasm after formalin fixation. Another variant, the frequently seen Hodgkin’s cell, has the nuclear and nucleolar features of the Reed-Stemberg cell. In some biopsy specimens, Hodgkin’s cells are more pleomorphic and may be difficult to distinguish from anaplastic large cell lymphoma.41
Definition of Histologic Subtypes
The most universally accepted morphologic classification scheme, the Rye classification system, defines four histologic subtypes of Hodgkin’s disease: lymphocytic predominance (LP), mixed cellularity (MC), lymphocytic depletion (LD), and nodular sclerosis (NS).41 Historically, prognosis in the first three categories was correlated with the ratio of lymphocytes to abnormal cells.
Figure 1. Characteristic Reed-Sternberg cell and mononuclear variant of Hodgkin’s dis- ease. (Hernatoxylin and eosin; original magnification x 400.)
894 HUDSON & DONALDSON
However, histology now has less prognostic significance since the development of highly curative contemporary treatment regimens.
In LP Hodgkin’s disease, the lymph node architecture may be partially or completely destroyed. This subtype may be misinterpreted as reactive hyperpla- sia because of its characteristic cellular proliferation of benign-appearing lym- phocytes, and occasional histiocytes. Multiple tissue sections may be required before a diagnostic Reed-Stemberg cell is identified; fibrosis usually is not seen. LP Hodgkin’s disease affects 10% to 15% of children, is more common in boys and younger patients, and usually presents as clinically localized disease.
Reed-Stemberg cells and their variants are often numerous (5-15/high- power field) in specimens of MC Hodgkin’s disease. This subtype is character- ized by a diffusely effaced lymph node containing an inflammatory background of lymphocytes, plasma cells, eosinophils, histiocytes, and malignant reticular cells. Fine interstitial fibrosis may be seen, and focal necrosis may be present but usually is not marked. This subtype is observed in about 30% of patients and is more common in children 10 years or younger and those with human immunodeficiency virus (HN) infection. MC Hodgkin’s disease frequently pre- sents as advanced disease, with extranodal extension.16
The LD subtype of Hodgkin’s disease is rarely observed in children, and a significant proportion of previous cases designated as LD Hodgkin’s may actu- ally represent diffuse large cell lymphoma. The presence of numerous, bizarre, malignant reticular cells, many Reed-Sternberg cells, and few lymphocytes char- acterizes this subtype. Diffuse fibrosis and necrosis are common. Patients with LD Hodgkin‘s histology often present with widespread disease that involves the bones and bone marrow.
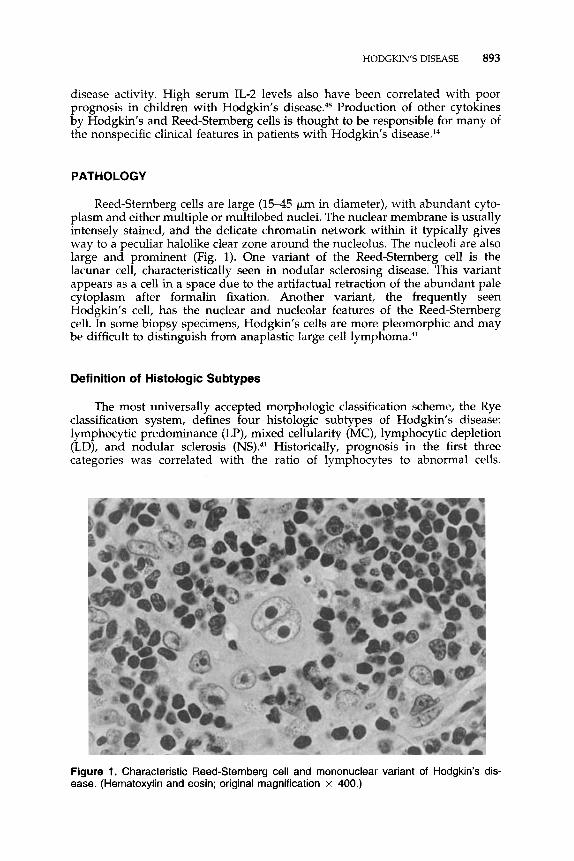
The NS subtype of Hodgkin’s disease is the most common one, affecting about 40% of younger patients and 70% of adolescents.16 This subtype is charac- terized by a thickened lymph node capsule comprised of orderly collagenous bands that divide the lymphoid tissue into circumscribed nodules (Fig. 2). NS Hodgkin’s disease has a striking propensity to involve the lower cervical, supraclavicular, and mediastinal lymph nodes. Because of the abundance of collagen, the radiographic appearance of these lesions (particularly in the medi- astinum) may only slowly return to normal, even when the patient is responding to therapy.
CLINICAL PRESENTATION
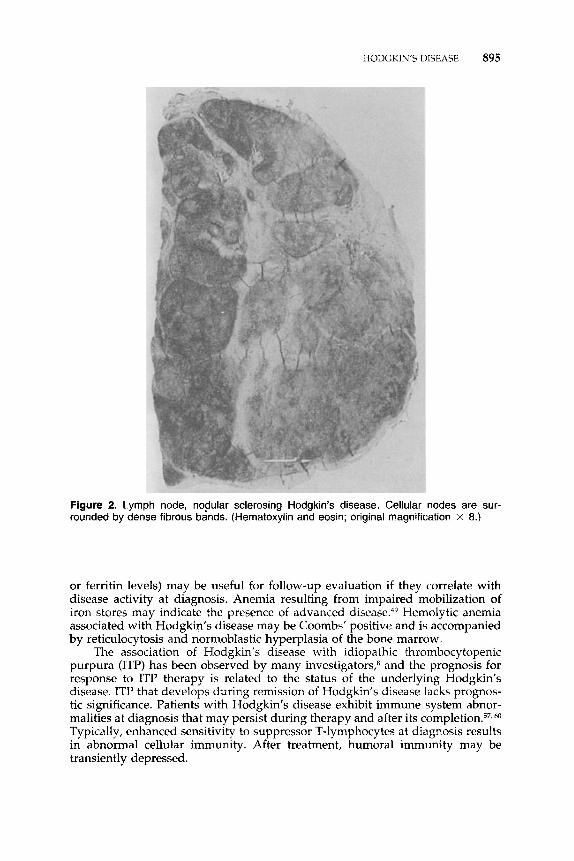
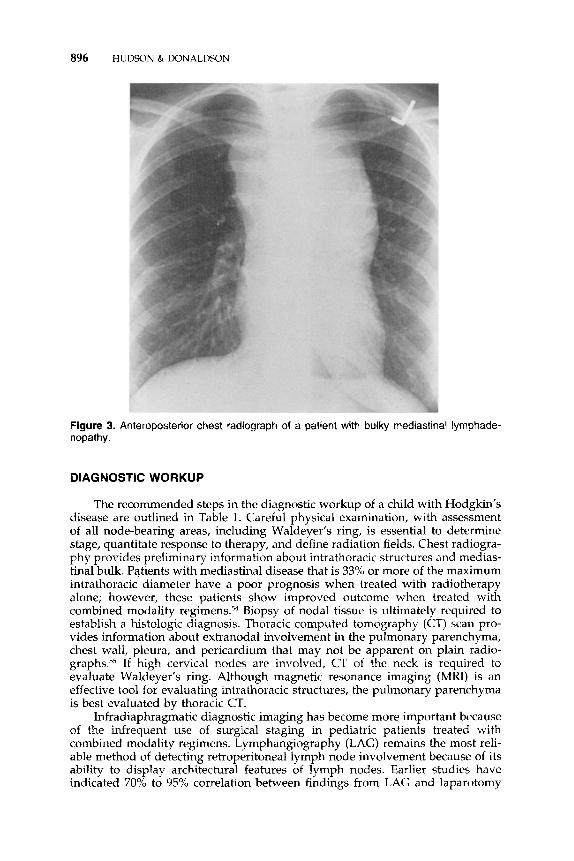
Asymptomatic cervical or supraclavicular lymphadenopathy, which may fluctuate over time, is the most common presentation of Hodgkin’s disease in children. Two thirds of patients will also have mediastinal adenopathy (Fig. 3), which may produce symptoms of tracheal or bronchial compression. Infre- quently, axillary or inguinal lymphadenopathy is the first presenting sign. Pri- mary disease presenting in a subdiaphragmatic site is rare, occurring in only about 3% of ca~es.3~ Constitutional symptoms, including fever, drenching night sweats, and weight loss, occur in 25% to 30% of children and negatively impact prognosis. Other symptoms such as pruritus and alcohol-induced pain are infrequent and do not influence outcome.
Laboratory abnormalities observed at diagnosis are relatively nonspecific and include neutrophilic leukocytosis, lymphopenia, eosinophilia, and mono- cytosis.61 Nonspecific laboratory test results that reflect activation of the reticulo- endothelial system (e.g., elevated erythrocyte sedimentation rate, serum copper,
HODGKIN’S DISEASE 895
Figure 2. Lymph node, nodular sclerosing Hodgkin’s disease. Cellular nodes are sur- rounded by dense fibrous bands. (Hernatoxylin and eosin; original magnification x 8.)
or ferritin levels) may be useful for follow-up evaluation if they correlate with disease activity at diagnosis. Anemia resulting from impaired mobilization of iron stores may indicate the presence of advanced disease.49 Hemolytic anemia associated with Hodgkin‘s disease may be Coombs’ positive and is accompanied by reticulocytosis and normoblastic hyperplasia of the bone marrow.
The association of Hodgkin’s disease with idiopathic thrombocytopenic purpura (ITP) has been observed by many investigators,8 and the prognosis for response to ITP therapy is related to the status of the underlying Hodgkin’s disease. ITP that develops during remission of Hodgkin’s disease lacks prognos- tic significance. Patients with Hodgkin’s disease exhibit immune system abnor- malities at diagnosis that may persist during therapy and after its completion.57, Typically, enhanced sensitivity to suppressor T-lymphocytes at diagnosis results in abnormal cellular immunity. After treatment, humoral immunity may be transiently depressed.
896 HUDSON & DONALDSON
Figure 3. Anteroposterior chest radiograph of a patient with bulky mediastinal lymphade- nopathy.
DIAGNOSTIC WORKUP
The recommended steps in the diagnostic workup of a child with Hodgkin’s disease are outlined in Table 1. Careful physical examination, with assessment of all node-bearing areas, including Waldeyer’s ring, is essential to determine stage, quantitate response to therapy, and define radiation fields. Chest radiogra- phy provides preliminary information about intrathoracic structures and medias- tinal bulk. Patients with mediastinal disease that is 33% or more of the maximum intrathoracic diameter have a poor prognosis when treated with radiotherapy alone; however, these patients show improved outcome when treated with combined modality regimens.54 Biopsy of nodal tissue is ultimately required to establish a histologic diagnosis. Thoracic computed tomography (CT) scan pro- vides information about extranodal involvement in the pulmonary parenchyma, chest wall, pleura, and pericardium that may not be apparent on plain radio- g r a p h ~ . ~ ~ If high cervical nodes are involved, CT of the neck is required to evaluate Waldeyer’s ring. Although magnetic resonance imaging (MRI) is an effective tool for evaluating intrathoracic structures, the pulmonary parenchyma is best evaluated by thoracic CT.
Infradiaphragmatic diagnostic imaging has become more important because of the infrequent use of surgical staging in pediatric patients treated with combined modality regimens. Lymphangiography (LAG) remains the most reli- able method of detecting retroperitoneal lymph node involvement because of its ability to display architectural features of lymph nodes. Earlier studies have indicated 70% to 95% correlation between findings from LAG and laparotomy
HODGKIN’S DISEASE 897
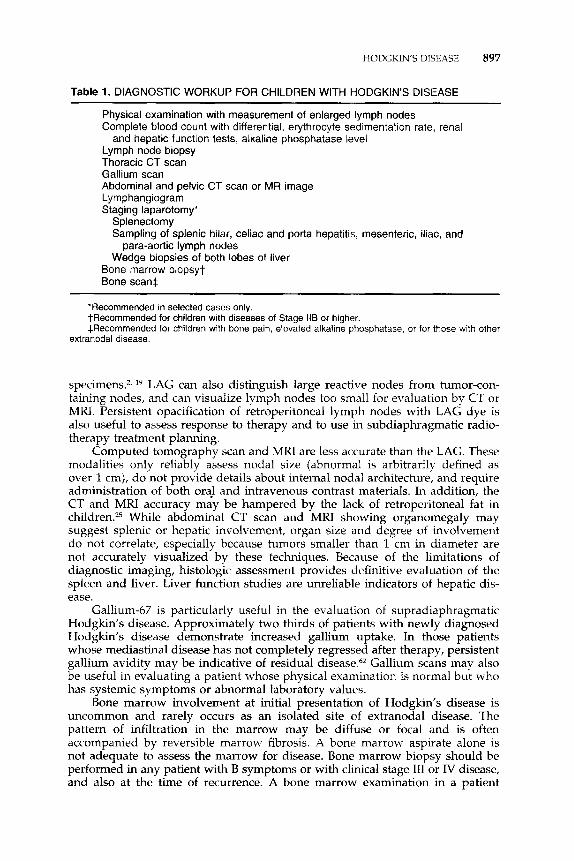
Table 1. DIAGNOSTIC WORKUP FOR CHILDREN WITH HODGKIN’S DISEASE ~ ~~
Physical examination with measurement of enlarged lymph nodes Complete blood count with differential, erythrocyte sedimentation rate, renal
Lymph node biopsy Thoracic CT scan Gallium scan Abdominal and pelvic CT scan or MR image Lymphangiogram Staging laparotomy*
Splenectomy Sampling of splenic hilar, celiac and porta hepatitis, mesenteric, iliac, and
Wedge biopsies of both lobes of liver
and hepatic function tests, alkaline phosphatase level
para-aortic lymph nodes
Bone marrow biopsyt Bone scant
‘Recommended in selected cases only. tRecommended for children with diseases of Stage llB or higher. *Recommended for children with bone pain, elevated alkaline phosphatase, or for those with other
extranodal disease.
specimens.2, l9 LAG can also distinguish large reactive nodes from tumor-con- taining nodes, and can visualize lymph nodes too small for evaluation by CT or MRI. Persistent opacification of retroperitoneal lymph nodes with LAG dye is also useful to assess response to therapy and to use in subdiaphragmatic radio- therapy treatment planning.
Computed tomography scan and MRI are less accurate than the LAG. These modalities only reliably assess nodal size (abnormal is arbitrarily defined as over 1 cm), do not provide details about internal nodal architecture, and require administration of both oral and intravenous contrast materials. In addition, the CT and MRI accuracy may be hampered by the lack of retroperitoneal fat in children.z5 While abdominal CT scan and MRI showing organomegaly may suggest splenic or hepatic involvement, organ size and degree of involvement do not correlate, especially because tumors smaller than 1 cm in diameter are not accurately visualized by these techniques. Because of the limitations of diagnostic imaging, histologic assessment provides definitive evaluation of the spleen and liver. Liver function studies are unreliable indicators of hepatic dis- ease.
Gallium-67 is particularly useful in the evaluation of supradiaphragmatic Hodgkin’s disease. Approximately two thirds of patients with newly diagnosed Hodgkin’s disease demonstrate increased gallium uptake. In those patients whose mediastinal disease has not completely regressed after therapy, persistent gallium avidity may be indicative of residual disease.6z Gallium scans may also be useful in evaluating a patient whose physical examination is normal but who has systemic symptoms or abnormal laboratory values.
Bone marrow involvement at initial presentation of Hodgkin’s disease is uncommon and rarely occurs as an isolated site of extranodal disease. The pattern of infiltration in the marrow may be diffuse or focal and is often accompanied by reversible marrow fibrosis. A bone marrow aspirate alone is not adequate to assess the marrow for disease. Bone marrow biopsy should be performed in any patient with B symptoms or with clinical stage 111 or IV disease, and also at the time of recurrence. A bone marrow examination in a patient
898 HUDSON & DONALDSON
with newly diagnosed clinical stage (CS) I-IIA disease is rarely abnormal, and thus is not indicated in this setting.
A technetium-99 bone scan with corresponding plain radiographs of abnor- mal areas aids in the assessment of skeletal metastases and should be reserved for the child who has bone pain, a serum alkaline phosphatase concentration that is elevated beyond that expected for age, or extranodal disease identified by other staging studies.
STAGING
Hodgkin’s disease spreads contiguously to adjacent lymph nodes until late in the course of the disease.32 The anatomically based Ann Arbor staging system, adopted in 1971 (Table 2),9 assigns stage based on the number of sites of lymph node involvement, the presence of extranodal disease, and a history of B symptoms. Patients are classified as A if asymptomatic and as B if symptoms of a temperature of over 38°C for 3 consecutive days, drenching night sweats, or an unexplained loss of 10% body weight or more over 6 months precede diagnosis. The anatomic locations of lymph node chains designated as ”regions” for the purpose of staging are illustrated in Figure 4.32 Substage E denotes extranodal disease; originally, this designation identified extranodal disease which could be appropriately treated by radi~therapy.~’
If the treatment plan prescribes radiation therapy only, precise anatomic staging is required for the design of radiation fields. However, if chemotherapy is planned, histologic confirmation of microscopic disease is less important. Surgical staging laparotomy should be considered only if the findings will significantly alter therapy.I0
TREATMENT
Optimal therapy planning for pediatric Hodgkin’s disease requires a multi- disciplinary approach from the time of diagnosis. Factors influencing treatment decisions are the age and physical maturity of the patient, the disease stage and bulk, and potential treatment sequelae. The therapy recommended should en-
Table 2. ANN ARBOR STAGING CLASSIFICATION FOR HODGKIN’S DISEASE
Stage I:
Stage II:
Involvement of a single lymph node region (I) or of a single extralymphatic
Involvement of two or more lymph node regions on the same side of the organ or site (IE).
diaphragm (11) or localized involvement of an extralymphatic organ or site and one or more lymph node regions on the same side of the diaphragm w.
Stage 111: Involvement of lymph node regions on both sides of the diaphragm (Ill), which may be accompanied by involvement of the spleen (Ill,) or by localized involvement of an extralymphatic organ, site (IllE), or both ( I l l sE) .
Stage IV: Diffuse or disseminated involvement of one or more extralymphatic organs or tissues with or without lymph node involvement.
The absence or presence of a temperature of over 38°C for 3 consecutive days, drenching night sweats, or unexplained loss of 10% or more of body weight in the 6 months preceding admission are to be denoted in all cases by the suffix letters A or B, respectively.
Figure 4. Anatomic definition of separate lymph node regions used for staging purposes. (Adapted from Kaplan HS, Rosenberg SA: The treatment of Hodgkin's disease. Med Clin North Am 50:1591, 1966; with permission.)
sure the best opportunity of long-term, disease-free survival (DFS) balanced with the lowest risk of severe treatment toxicity. Today, most pediatric protocols prescribe multiagent chemotherapy alone, or in combination with low-dose, involved-field radiation therapy in growing children. The addition of radiation to combination chemotherapy improves DFS in patients with bulky disease and substage B-type symptoms, and allows for fewer cycles of less toxic chemother- apy. High-dose, extended-field radiation therapy alone is reserved for adoles- cents and fully grown patients with localized disease. The goals of current studies on clinically staging children with localized disease are to determine whether high cure rates can be maintained by using fewer cycles of chemother- apy and low-dose, involved-field radiation. Investigations into advanced-stage disease are also focused on maintaining treatment efficacy with the use of combined modality therapy, limiting doses of radiotherapy and cycles of poten- tially toxic chemotherapy, and avoiding staging laparotomy. Therapy options for the various stages are discussed in the following sections.
900 HUDSON & DONALDSON
Treatment Results
Early-Stage and Favorable Disease
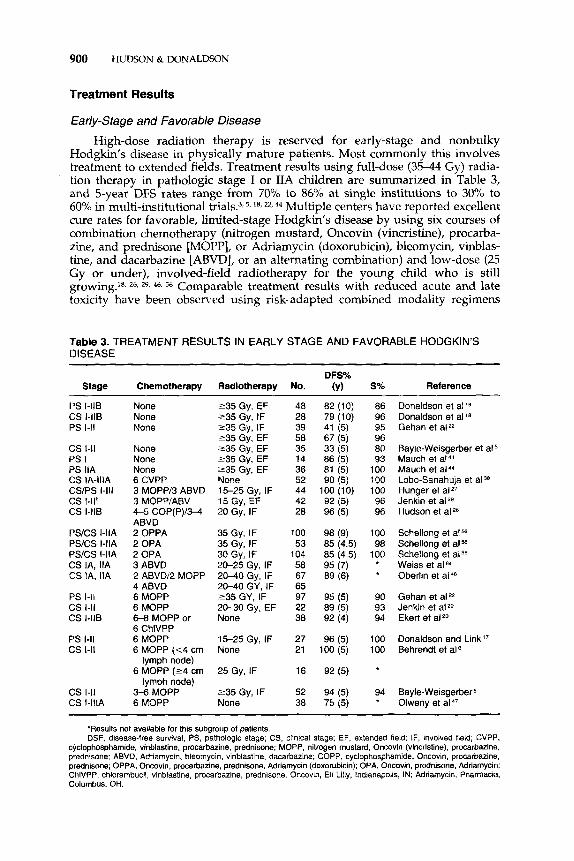
High-dose radiation therapy is reserved for early-stage and nonbulky Hodgkin's disease in physically mature patients. Most commonly this involves treatment to extended fields. Treatment results using full-dose (35-44 Gy) radia- tion therapy in pathologic stage I or IL4 children are summarized in Table 3, and 5-year DFS rates range from 70% to 86% at single institutions to 30% to 60% in multi-institutional trials.3Z5, 2z,44 Multiple centers have reported excellent cure rates for favorable, limited-stage Hodgkin's disease by using six courses of combination chemotherapy (nitrogen mustard, Oncovin (vincristine), procarba- zine, and prednisone [MOPP], or Adriamycin (doxorubicin), bleomycin, vinblas- tine, and dacarbazine [ABVD], or an alternating combination) and low-dose (25 Gy or under), involved-field radiotherapy for the young child who is still growing.1s, 26, 29, 46, 56 Comparable treatment results with reduced acute and late toxicity have been observed using risk-adapted combined modality regimens
Table 3. TREATMENT RESULTS IN EARLY STAGE AND FAVORABLE HODGKIN'S DISEASE
235 Gy, EF 235 Gy, IF 235 Gy, IF 235 Gy, EF 235 Gy, EF 235 Gy, EF 235 Gy, EF None 15-25 Gy, IF 15 Gy, EF 20 Gy, IF
35 Gy, IF 35 Gy, IF 30 Gy, IF 20-25 Gy, IF 20-40 Gy, IF 20-40 GY, IF 235 GY, IF 20-30 Gy, EF None
15-25 Gy, IF None
25 Gy, IF
235 Gy, IF None
48 28
58 39
35 14 36 52 44 42 2a
100 53
104
67 65 97 22
58
38
27 21
16
52 38
86 96 95 96
93 100 100 100 96 96
100 98
100
ao
90 93 94
100 100
94
Donaldson et alle Donaldson et al Gehan et aIz
Bayle-Weisgerber et a15 Mauch et atM Mauch et al 44
Lobo-Sanahuja et aIB Hunger et alz7 Jenkin et ,Iz8 Hudson et al 26
Schellong et a1% Schellong et aIM Schellong et a156 Weiss et al Oberlin et al 46
Gehan et aIz Jenkin et aIz9 Ekert et alZo
Donaldson and Link Behrendt et a16
Bayle-Weisgerber5 Olweny et aI4'
"Results not available for this subgroup of patients. DSF, disease-free survival; PS, pathologic stage; CS, clinical stage; EF, extended field, IF, involved lieid; CVPP,
prescribing low-dose, involved-field radiotherapy and fewer cycles of chemo- therapy.&, 61
Some groups have reported treatment results with chemotherapy alone using MOPP and similar therapies containing alkylating agents for early-stage Hodgkin's disease.28, 38 However, long-term disease-free status and treatment- related toxicities for these patients have not been evaluated. The potential advantages of chemotherapy-only regimens include the elimination of staging laparotomy and splenectomy, and of radiation-related late treatment sequelae. The disadvantages are exposure to higher doses of alkylating drugs (compared with those prescribed in combined modality regimens) and increased morbidity from myelosuppression, gonadal injury, and secondary leukemia.
Generally, because standard-dose radiation therapy, chemotherapy alone, and combined modality therapy offer excellent long-term DFS rates in most children with localized disease, the risk and severity of acute and late treatment toxicities most often influence the choice of therapy. However, because 50% or more of patients with bulky mediastinal adenopathy (mediastinal masses 33% or more of the maximal intrathoracic diameter) relapse after treatment with either radiation therapy or chemotherapy alone, a combined modality approach is recommended for these patients.4O In addition, many investigators also believe strongly that all children with B symptoms (particularly fever and weight loss) should receive combined modality therapy because of the poor prognostic impli- cations of these constitutional symptoms, even in the setting of clinically local- ized disease."
Advanced Stage and Unfavorable Disease
Patients with disease limited to the spleen, or the splenic hilar or porta hepatis nodes (stage IIIAJ, were historically thought to be good candidates for radiation therapy alone, in contrast to those with more extensive involvement in the retroperitoneal ,lymph nodes (stage IIIA2).I3 However, the distinction between stages IIIAl and IIIA2 is less important in growing children in whom the recommended treatment includes chemotherapy and low-dose radiation therapy. The cornerstone of therapy for advanced Hodgkin's disease is combina- tion chemotherapy, although some investigators believe that the addition of radiation therapy improves DFS. Pediatric protocols prescribing MOPP, ABVD, MOPP and ABVD, or similar hybrid combinations with or without low-dose radiotherapy have resulted in DFS rates of 70% to 90% in children with advanced disease (Table 4).* Treatment regimens using combination chemotherapy alone for advanced-staged cancer patients avoid sequelae of surgical staging and radiation; however, these regimens contain substantial doses of alkylating agents, which are associated with potential morbidity from myelosuppression, gonadal injury, and secondary leukemia?, 20, 28, 38, 47 Attempts to reduce late treatment side effects from alkylating agents by substituting other agents have resulted in inferior event-free survival rates in patients with advanced-stage disease.4', 56
More aggressive management approaches are clearly needed for some ad- vanced-stage cancer patients with extranodal disease; however, identification of patients at risk for treatment failure remains difficult. The impressive cure rates accomplished with more modern regimens stimulates consideration of earlier treatment with even more aggressive therapies, such as hematopoietic stem cell
CS 1116, IV 6 CVPP/6 EBO None 24 60 (5) 81 Lobo-Sanahuja et aIM CS/PS IV 3 MOPP/3 ABVD 15-25 Gy, IF 13 69 (10) 85 Hunger et alZ7 PS/CS llBE, 2 OPPN4 COPP 20-36 Gy, IF 65 82 (5) 94 Schellong et
cs lll/lV 4-5 COP(P)/34 20 Gy, IF 57 93 (5) 93 Hudson et alzE
CS 1118, IV 5 MOPP/5 ABVD 20-25 Gy, EF 38 60 r) * Weiss et alffl cs Ill 3 ABVD/3 MOPP 20-40 GY,EF 40 82 (6) * Oberlin et cs IV 3ABVD/3 MOPP 20-40 GY,EF 21 62 (6) * PS/CS llBE, 2 OPPN4 COPP 25 Gy, IF 50 88 (4.5) * Schellong et alM
PS/CS IIAE, 2 OPPN2 COPP 30 Gy, IF 53 94 (9) * Schellong et al=
PS 111, IV 4 MOPP/4 ABVD 21 Gy TN 62 77 (3) 95 Weiner et a162 cs IV 6 MOPP 25-35 Gy, EF 15 82 (5) 80 Jenkin et ,Iz9 PS 111, IV 12 ABVD 21 Gy, R 65 87 (3) 89 Fryer et aI2’ CS 1-11, Ill, IV 6-8 MOPP or 6 None 53 92 (4) 94 Ekert et ,Izo
PS Ill, IV 6 MOPP 15-25 Gy, IF 28 84 (5) 78 Donaldson and Link”
IIIAE, 1118, IV
ABVD
IIIAE, 1118, IV 2 OPN4 COMP 25 Gy, IF * 54 (4.5) 100
llB PS/CS IllA 2 OPN2 COMP 30 Gy, IF 55 (9) *
ChlVPP
‘Results not available for this subgroup of patients. DFS, disease-free survival; CS, clinical stage; CVPP, cyclophosphamide, vinblastine, procarbazine,
transplantation. More novel approaches are designed to test if early intensive chemotherapy will improve cure rates among high-risk patients. The MOPP/ ABV hybrid combinationw* 33 uses active agents that are non-cross-resistant to MOPP chemotherapy earlier than in the traditional alternating MOPP/ABVD regimens. Early treatment results indicate the feasibility and efficacy of this hybrid regimen in a clinically staged pediatric cohort.30 Similarly, the Stanford V program uses a shortened duration of dose-intensive and consolidative radiation therapy to sites of bulky disea~e.~ The advantages of these approaches include reduced duration of therapy and lower cumulative doses of individual drugs, which should decrease the risks of second malignancies and infertility. Contin- ued evaluation of these and similar treatment approaches will determine whether cure rates in children with advanced-stage cancer can be improved.
RELAPSED DISEASE
As many as 10% to 20% of children with localized disease and 30% to 40% of those with advanced disease will relapse, usually within the first 3 years of diagnosis. For patients who relapse after radiation therapy only, salvage rates range from 50% to 80% after retreatment with chemotherapy. Patients treated with conventional therapy who respond very poorly are those who (1) fail to
HODGKIN'S DISEASE 903
achieve a complete remission; (2) have a brief remission (lasting 12 months or less); or (3) develop multiple relapses. Hematopoietic stem cell transplantation provides DFS for approximately 20% to 30% of these patients.' Progression-free survival after salvage with conventional therapy in patients with longer (12 months or more) initial remissions ranges from 40% to 50% at 5 years. However, fatal treatment complications (especially second malignancies) reduce their long- term event-free survival to 25Y0.~~ Progression-free survival rates as high as 50% to 80% after myeloablative chemotherapy with hematopoietic stem cell transplantation now suggest that high-dose therapy may be even more effective than is conventional therapy.45, The risk of transplant-associated morbidity and mortality is related to the extent of previous therapy and the intensity of the conditioning regimen. Transplant-associated mortality (most commonly second- ary to infectious or cardiopulmonary complications) occurs in as many as 25% of patients (mean,
Novel therapeutic approaches for relapsed Hodgkin's disease currently under investigation include I3'I-labeled antibody directed against ferritin, a tu- mor-associated protein found in patients with Hodgkin's disea~e,"~ and the radionuclide yttrium-90, which deliver localized radiation directly to tumor- bearing areas.7 Innovative immunotherapy strategies under investigation are attempting to exploit the characteristic pattern of EBV gene expression in Reed- Sternberg and Hodgkin's cells" through vaccines that incorporate the highly immunogenic LMP-1 tumor antigen? 36 and through autologous EBV-specific cytotoxic T lymphocyte^.^^
COMPLICATIONS OF THERAPY
With improved cure rates, increasing attention is focused on minimizing the early and late complications of therapy.I5 Soft tissue and bone growth alterations are less common now that combined modality therapy with low- dose, involved-field radiation therapy is the preferred treatment for growing children. Similarly, the incidence of chemotherapy-related cardiopulmonary injury has been reduced because of restrictions of the cumulative doses of doxorubicin and bleomycin in contemporary 27 In fully grown pa- tients treated with radiation as a single modality, cardiopulmonary damage is presently uncommon due to improvements in radiation technology and shielding techniques, and reductions in daily fraction size. Continued monitor- ing of children and adolescents treated with regimens including lower cumula- tive doses of bleomycin, doxorubicin, and low-dose radiation therapy is required to determine if the collective use of these modalities will predispose these patients to late cardiopulmonary injury.
The reader is referred to the article herein, Long-Term Survivors of Child- hood Cancer, for a comprehensive overview of complications following malig- nant disease and its treatment in children.
References
1. Armitage 70, Biermxn PJ, Vose JM: Autologous bone marrow transplantation for Hodgkin's disease. Adv Oncol 10:25, 1994
2. Baker LL, Parker BR, Donaldson SS, et al: Staging of Hodgkin's disease in children: Comparison and CT and lymphography with laparotomy. AJR Am J Roentgenol 154:1251, 1990
904 HUDSON & DONALDSON
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
Barrett A, Crennan E, Barnes J, et a1 Treatment of clinical stage I Hodgkin’s disease by local radiation therapy alone. Cancer 66:670, 1990 Bartlett NL, Rosenberg SA, Hoppe RT, et al: Brief chemotherapy, Stanford V, and adjuvant radiotherapy for bulky or advanced-stage Hodgkin’s disease: A preliminary report. J Clin Oncol 13:1080, 1995 Bayle-Weisgerber C, Lemercier N, Teillet F, et al: Hodgkin’s disease in children: Results of therapy in a mixed group of 178 clinical and pathologically staged patients over 13 years. Cancer 54:215, 1984 Behrendt H, Van Bunningen FM, Van Leeuwen EF: Treatment of Hodgkin’s disease in children with or without radiotherapy. Cancer 59:1870, 1987 Bierman PJ, Vose JM, Leichner PK, et al: Yttrium 90-labeled antiferritin followed by high-dose chemotherapy and autologous bone marrow transplantation in poor-prog- nosis Hodgkin’s disease. J Clin Oncol 11:698, 1993 Bradley SJ, Hudson GV, Linch DC: Idiopathic thrombocytopenic purpura in Hodgkin’s disease: A report of eight cases. Clin Oncol 5:355, 1993 Carbone PP, Kaplan HS, Musshoff K, et al: Report of the committee on Hodgkin’s disease staging classification. Cancer Res 31:1860, 1971 Cohen IT, Higgins CR, Powars DR, Hays DM: Staging laparotomy for Hodgkin’s disease in children: Evaluation of the technique. Arch Surg 112:948, 1977 Cooper DL, DeVita VT: Hodglun’s disease: Current therapy and controversies. Adv Oncol 10:17, 1994 Desch CE, Lasala MR, Smith TJ, Hillner BE: The optimal timing of autologous bone marrow transplantation in Hodgkin’s disease patients after a chemotherapy relapse. J Clin Oncol 10200, 1992 Desser RK, Golomb HM, Ultmann JE, et al: Prognostic classification of Hodgkin‘s disease in pathologic stage 111, based on anatomic considerations. Blood 49:883, 1977 Diehl V, von Kalle C, Fonatsch C, et al: The cell of origin in Hodgkin’s disease. Semin Oncol 17:660, 1990 Donaldson SS, Kaplan HS: Complications of treatment of Hodgkin’s disease in chil- dren. Cancer Treatment Rep 66:977, 1982 Donaldson SS, Link MI? Childhood lymphomas: Hodgkin’s disease and non- Hodgkin’s lymphoma. In Moosa AR, Robson MC, Schimpff SC (eds): Comprehensive Textbook of Oncology. Baltimore, Williams & Wilkis, 1986, p 1161 Donaldson SS, Link MP: Cpmbined modality treatment with low-dose radiation and MOPP chemotherapy for children with Hodgkin’s disease. J Clin Oncol5:742, 1987 Donaldson SS, Whitaker SJ, Plowman PN, et al: Stage I-II pediatric Hodgkin’s disease: Long-term follow-up demonstrates equivalent survival rates following different man- agement schemes. J Clin Oncol8:1128, 1990 Dudgeon DL, Kelly M, Ghory MJ, et a1 The efficacy of lymphangiography in the staging of pediatric Hodgkin’s disease. J Pediatr Surg 21:233, 1986 Ekert H, Waters KD, Smith PJ, et al: Treatment with MOPP or ChlVPP chemotherapy only for all stages of childhood Hodgkin’s disease. J Clin Oncol6:1845, 1988 Fryer CJ, Hutchinson RJ, Krailo M, et al: Efficacy and toxicity of 12 courses of ABVD followed by low-dose regional radiation in advanced Hodgkin’s disease in children: A report from the Children’s Cancer Study Group. J Clin Oncol 8:1971, 1990
22. Gehan EA, Sullivan MP, Fuller LM, et al: The Inteigroup Hodgkin’s disease in children: A study of stages I and 11. Cancer 65:1429, 1990
24. Haluska FC, Brufsky AM, Canellos GP: The cellular biology of the Reed-Stemberg cell. Blood 84:1005, 1994
25. Hanna SL, Fletcher BD, Boulden TF, et al: MR imaging of infradiaphragmatic lymph- adenopathy in children and adolescents with Hodgkin disease: Comparison with lymphography and CT. Journal of Magnetic Resonance Imaging 3:461,1993
26. Hudson MM, Greenwald CG, Thompson E, et al: Efficacy and toxicity of multiagent chemotherapy and low-dose involved-field radiotherapy in chldren and adolescents with Hodgkin’s disease. J C l i Oncol 11:100, 1993
27. Hunger SP, Link MI‘, Donaldson SS: ABVD/MOPP and low-dose involved-field radio-
HODCKIN’S DISEASE 905
therapy in pediatric Hodgkin’s disease: The Stanford experience. J Clin Oncol 122160, 1994
28. Jacobs P, King HS, Karabus C, et al: Hodgkin’s disease in children: A ten-year experience in South Africa. Cancer 53:210, 1984
29. Jenkin D, Doyle J, Berry M, et al: Hodgkin’s disease in children: Treatment with MOPP and low-dose, extended field irradiation without laparotomy. Late results and toxicity. Med Ped Oncol 18:265,1990
30. Jenkin D, Greenberg M: Hodgkin’s disease in childhood. Early treatment results in clinically staged patients utilizing MOPP/ABV (3 cycles) and extended field radiation treatment (1500 cGy) [abstract]. Med Ped Oncol 23:542, 1994
31. Kaplan H S Hodgkin’s Disease, ed 2. Cambridge, MA, Harvard University Press, 1980 32. Kaplan HS, Rosenberg SA: The treatment of Hodgkin’s disease. Med Clin North Am
50:1591, 1966 33. Klimo P, Conners JM. MOPP/ABV hybrid program: Combination chemotherapy based
on early introduction of seven effective drugs for advanced stage Hodgkin’s disease. J Clin Oncol 3:1174, 1985
34. Khanna R, Burrows SR, Kurilla MG, et al: Localization of Epstein-Barr cytotoxic 7 cell epitopes using recombinant vaccinia: Implications for vaccine development. J Exp Med 176:169, 1992
35. Krikorian JG, Portlock CS, Mauch I’M: Hodgkin’s disease presenting below the dia- phragm: A review. J Clin Oncol4:1551, 1985
36. Lemas MV, Zhang H, Schaad HJ, et al: Strategies toward the development of a therapeutic vaccine for the treatment of EBV-associated Hodgkin’s disease [abstract]. I n Proceedings of the Cold Spring Harbor Meeting on Cancer Cells: Epstein-Barr Virus and Associated Disease. Cold Spring Harbor, New York, Cold Spring Harbor Laboratory, 1994, p 222
37. Lenhard RE Jr, Order SE, Spunberg JJ, et al: Isotopic immunoglobulin: A new systemic therapy for advanced Hodgkin’s disease. J Clin Oncol 3:1296, 1985
38. Lobo-Sanahuja F, Garcia I, Barrantes JC, et al: Pediatric Hodgkin’s disease in Costa Rica: Twelve years’ experience of primary treatment by chemotherapy alone, without staging laparotomy. Med Ped Oncol 22:398, 1994
39. Longo DL, Duffey PL, Young RC, et a1 Conventional-dose salvage combination chemo- therapy in patients relapsing with Hodgkin‘s disease after combination chemotherapy: The low probability of cure. J Clin Oncol 10:210, 1992
40. Longo DL, Glatstein E, Duffy PL, et al: Radiation therapy versus combination chemo- therapy in the treatment of early stage Hodgkin’s disease: Seven-year results of a prospective randomized trial. J Clin Oncol 9:906, 1991
41. Lukes RJ, Butler JJ: The pathology and nomenclature of Hodgkin’s disease. Cancer Res 26:1063, 1966
42. Link MP, Hudson M, Donaldson SS, et al: Treatment of children with unfavorable and advanced stage Hodgkin‘s disease with vinblastine, etoposide, prednisone and Adriamycin (VEPA) and low-dose, involved field irradiation [abstract]. Proc Am Soc Clin Oncol 13:392, 1994
43. Mack TM, Cozen W, Shibata DK, et al: Concordance for Hodgkin’s disease in identical twins suggesting genetic susceptibility to the young-adult form of the disease. N Engl J Med 332413, 1995
44. Mauch PM, Weinstein H, Botnick I., et al: An evaluation of long-term survival and treatment complications in children with Hodgkin’s disease. Cancer 51:925, 1983
45. Nademanee A, Sniecinski I, Schmidt GM, et a1 High-dose therapy followed by autolo- gous peripheral-blood stem-cell transplantation for patients with Hodgkin’s disease and non-Hodgkin’s lymphoma using unprimed and granulocyte colony-stimulating factor-mobilized peripheral-blood stem cells. J Clin Oncol 1221 76, 1994
46. Oberlin 0, Leverger G, Pacquement MA, et al: Low-dose radiation therapy and reduced chemotherapy in childhood Hodgkin’s disease: The experience of the French Society of Pediatric Oncology. J Clin Oncol 10:1602, 1992
47. Olweny CLM, Katongole-Mbidde E, Kiire C, et al: Childhood Hodgkin’s disease in Uganda: A ten year experience. Cancer 42:787, 1978
906 HUDSON & DONALDSON
48. Pui CH, Ip S, Thompson E, et al: High serum interleukin-2 levels correlate with a poor prognosis in children with Hodgkin’s disease. Leukemia 3:481, 1989
49. Ratkin GA, Presant CA, Weinerman €3, Reinhard E H Correlation of anemia with infradiaphragmatic involvement in Hodgkin’s disease and other malignant lympho- mas. Canadian Medical Association Journal 11 1:924, 1974
50. Reece DE, Conners JM, Spinelli JJ, et al: Intensive therapy with cyclophosphamide, carmustine, etoposide & cisplatin, and autologous bone marrow transplantation for Hodgkin’s disease in first relapse after combination chemotherapy. Blood 83:1193,1994
51. Riggs S, Hagemeister FB: Immunodeficiency states: A predisposition to lymphoma. In Fuller LM, et a1 (eds): Hodgkin’s Disease and Non-Hodgkin’s Lymphomas in Adults and Children. New York, Raven, 1988, p 451
52. Robertson SJ, Lowman JT, Grufferman S, et al: Familial Hodgkin’s disease. A clinical and laboratory investigation. Cancer 59:1314, 1987
53. Rooney CM, Smith CA, Ng C, et al: Use of viral-specific cytotoxic lymphocytes to control Epstein-Barr virus-related lymphoproliferation. Lancet 345:9, 1995
54. Roskos RR, Evans RC, Gilchrist GS, et al: Prognostic significance of mediastinal mass in childhood Hodgkin’s disease. Cancer Treatment Rep 66961, 1982
55. Rostock RA, Siegelman SS, Lenhard RE, et al: Thoracic CT scanning for mediastinal Hodgkin’s disease: Results and therapeutic implications. Int J Radiat Oncol Biol Phys 9:1451, 1983
56. Schellong G, Bramswig JH, Homig-Franz I Treatment of children with Hodgkin’s disease: Results of the German Pediatric Oncology Group. Ann Oncol 3:73, 1992
57. Slivnick DJ, Ellis TM, Nawrocki JF, Fisher RI: The impact of Hodgkin’s disease on the immune system. Semin Oncol 17673, 1990
58. Spitz MR, Sider JF, Johnson CC, et a1 Ethnic patterns of Hodgkin‘s disease incidence among children and adolescents in the United States, 1973-1982. J Natl Cancer Inst 76235, 1986
59. Stein H, Mason DY, Gerdes J, et al: The expression of the Hodgkin’s disease associated antigen Ki-1 in reactive and neoplastic lymphoid tissue: Evidence that Reed-Stemberg cells and histiocytic malignancies are derived from activated lymphoid cells. Blood 66:848, 1985
60. Tan CT, DeSousa M, Good RA: Distinguishing features of the immunology of Hodgkin’s disease in children. Cancer Treatment Rep 66:969, 1982
61. Vecchi V, Pileri S, Burnelli R, et al: Treatment of pediatric Hodgkin disease tailored to stage, mediastinal mass, and age. Cancer 72:2049, 1993
62. Weiner M, Leventhal B, Cantor A, et al: Gallium-67 scans as an adjunct to CT scans for the assessment of a residual mediastinal mass in pediatric patients with Hodgkin’s disease: A Pediatric Oncology Group Study. Cancer 68:2478, 1991
63. Weiner MA, Leventhal BG, Marcus R, et al: Intensive chemotherapy (MOPP plus ABVD) and low dose radiotherapy for the treatment of advanced stage Hodgkin’s disease in pediatric patients: A Pediatric Oncology Group Study. J Clin Oncol 9:1591, 1991
64. Weiss L, Movahed LA, Wamke RA, et al: Detection of Epstein-Barr viral genomes in Reed-Stemberg cells of Hodgkin‘s disease. N Engl J Med 320:502, 1989
Address reprint requests to Melissa M. Hudson, MD
Department of Hematology/Oncology St. Jude Children’s Research Hospital