59
© 2020 PYA, P.C. WE ARE AN INDEPENDENT MEMBER OF HLB—THE GLOBAL ADVISORY AND ACCOUNTING NETWORK Holiday Cheer – 2021 Medicare Final Rules December 17, 2020
Page 0
© 2020 PYA, P.C.
WE ARE AN INDEPENDENT MEMBER OF HLB—THE GLOBAL ADVISORY AND ACCOUNTING NETWORK
Holiday Cheer – 2021 Medicare Final RulesDecember 17, 2020
Page 1
Introductions
Valerie RockCHC, CPC
Principal, Healthcare [email protected]
Kathy ReepMBA
Principal, Healthcare [email protected]
Angie CaldwellMBA, CPA
Principal, Healthcare [email protected]
Martie RossJD
Principal, Healthcare [email protected]
Lori FoleyCMA, CHC, PHR, SHRM-CP
Principal, Healthcare [email protected]
Page 2
Agenda
Key Provisions of the 2021 OPPS Final Rule and Most Favored Nation Model
Changes to Evaluation & Management Services and the New G-Code for Complex Visits
Conversion Factor Reduction and Physician Compensation
Care Management and Remote Patient Monitoring
Telehealth and Virtual Services
1
2
3
4
5
Page 3
1. Key Provisions of the 2021 OPPS Final Rule and Most Favored Nation Model
Page 4
• Conversion factor of $82.797 for CY2021• Compared to $80.7841 for CY2020 (2.4 percent increase)
• Increase in outlier threshold from $5,075 (CY2020) to $5,300 for CY2021• Payment for 340B drugs at ASP minus 22.5 percent
• Proposed at ASP minus 28.7 percent
• Payment policy not applicable to rural sole community hospitals, children’s hospitals, or PPS-exempt cancer hospitals
• Site neutral payment for clinic visits in grandfathered off-campus provider-based departments• Continues payment at 40 percent of OPPS rate
CY2021 Outpatient PPS Final Rule
Page 5
CY2021 Outpatient PPS Final Rule (cont’d)
• Elimination over three years of inpatient-only list• Inpatient/outpatient decision moves to the hands of physicians
• Moves approximately 300 musculoskeletal-related services from IPO list for CY2021
• Indefinite* exemption from certain medical review activities • Exempt from site-of-service claim denials
• Exempt from BFCC-QIO referrals to RACs for non-compliance with the two-midnight rule
• Exempt from RAC reviews for patient status
• Still subject to billing in compliance with two-midnight rule and subject to review for education purposes
• Defining “indefinite”
Page 6
• Adds additional 278 procedures to ASC CPL in CY2021• Including total hip arthroplasty
• Increases services requiring prior authorization (DOS on or after July 2021)
• Cervical fusion with disc removal
• Implanted spinal neurostimulators
• Changes level of supervision for certain outpatient therapeutic services• Applies to non-surgical extended duration therapeutic services
• Example: Infusion services
• Changes the minimum default level of supervision to general for the entire service
• Previously required direct supervision at the initiation of service
CY2021 Outpatient PPS Final Rule (cont’d)
Page 7
CMS Most Favored Nation Model
• Interim final rule issued November 20• Program begins nationally January 1, 2021
• Comments due on IFR January 26, 2021
• Provides for mandatory innovation model • Effective 2021 – 2027
• Mandatory for most Part B providers receiving separate payment for included drugs• Excludes children’s hospitals, PPS-exempt cancer hospitals, CAHs, IHS facilities, FQHCs, RHCs, etc.
• Focuses on top 50 drugs based on updated annual Medicare Part B spending• Selected drugs represent 75 percent of Part B drug spending
Page 8
• Reimbursement will move from ASP + 6 percent to rates based on the lowest price in other developed countries (MFN price)• MFN price phase-in (unless accelerated):
• Year 1: 25 percent MFN, 75 percent ASP + 6
• Years 2 – 3: Moves to 50 percent MFN/50 percent ASP +6, then 75 percent MFN/25 percent ASP + 6
• Years 4 – 7: 100 percent MFN
• New add-on payment ($148.73) for each does of MFN model eligible drug (HCPCS M1145)
• IFR includes some level of billing guidance
• Significant impact on hospital drug reimbursement when fully phased-in
CMS Most Favored Nation Model (cont’d)
Page 9
2. Changes to E/M Services and the New G-Code for Complex Visits
Page 10
• Fee schedule payments established under Section 1848 of the Social Security Act• Relative value for the service
• Work
• Practice expense
• Malpractice expense
• Geographic adjustment factor • Reflects variation in practice costs between metropolitan and non-metropolitan areas between
and regions
• Conversion factor (RVU x CF = national payment rate)• Dollar amount based on statutory cap on MPFS spending
• Sustainable Growth Rate replaced in 2015 by MACRA annual adjustment factor
Medicare Physician Fee Schedule
Page 11
• 2021 MPFS proposed rule published August 17, 2020 (572 pages + related downloads)• Telehealth, care management services, MSSP, QPP, OUD
services, FQHC PPS, NCDs, infusion therapy, Part B drugs, MDPP
• Comment period closed October 5
• 2021 MPFS final rule published December 1, 2020 (2,165 pages + related downloads)• Effective January 1, 2021
Rulemaking
Page 12
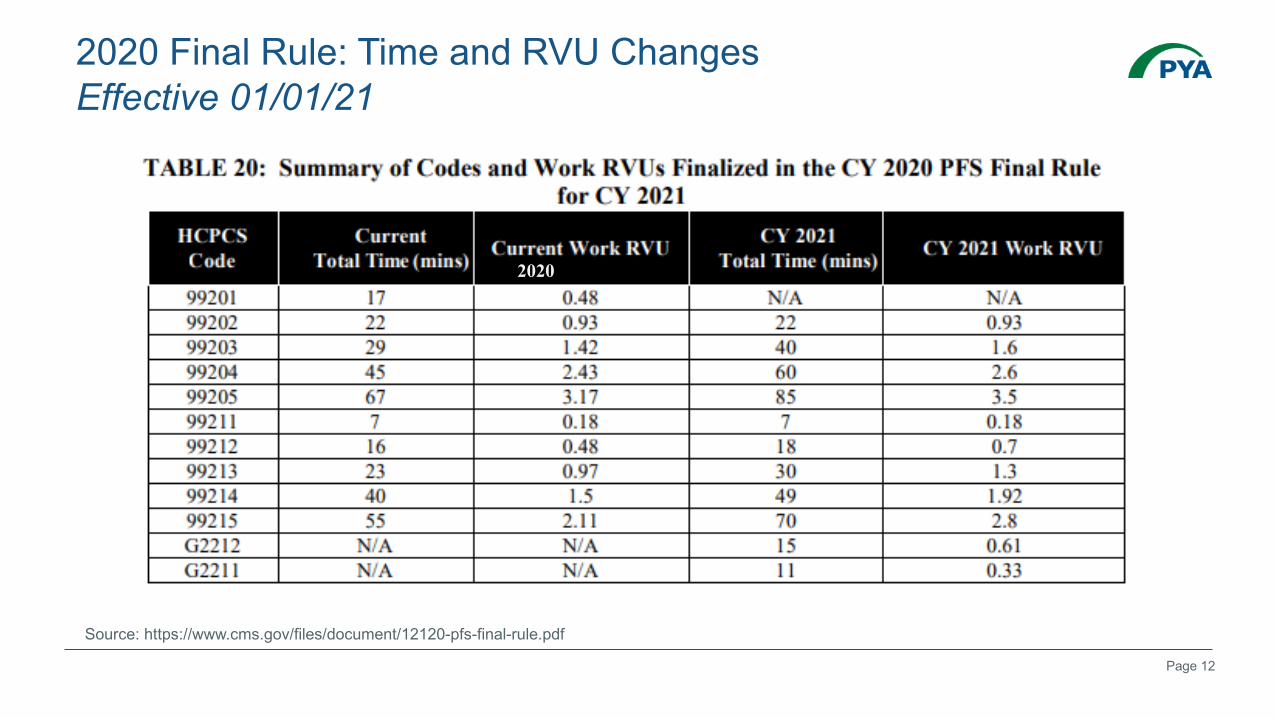
2020 Final Rule: Time and RVU ChangesEffective 01/01/21
Source: https://www.cms.gov/files/document/12120-pfs-final-rule.pdf
2020
Page 13
1. G2211: Add-on code for established patient outpatient E/M to account for complexity inherent to those services (0.33 wRVU)
2. 99417: Prolonged outpatient E/M beyond the total time of the primary procedure; each 15 minutes (starts at low end of range) (0.61 wRVU)
3. G2212: Medicare Prolonged outpatient E/M, beyond the top end of the range of total time.
2021 Final Rule: New CodesEffective 01/01/21
New codes relating to outpatient E/M
Page 14
• No offset to reduce redistributive impact of outpatient E/M changes
• Conversion factor impact • 2019 to 2020: 5¢ increase ($36.04 to $36.09) = 0.14% increase
• 2020 to 2021: $3.68 reduction ($36.09 to $32.41) = 10.20% reduction• If performed same number of RVUs in 2020 and 2021, would receive 10.20% less in reimbursement
in 2021
2021 Final Rule
Page 15
• “As these office/outpatient E/M visit codes make up around 20 percent of total PFS expenditures, we understand… the magnitude of the redistributive adjustment necessary to budget neutralize the increased values.”• Paying more to manage beneficiaries means paying less to do things to beneficiaries
• Physicians who primarily perform office visits will generate more revenue; physicians who are hospital-based or who primarily perform procedures will generate less
• H.R.8702 – Holding Providers Harmless From Medicare Cuts During COVID-19 Act of 2020• Currently under consideration
“Redistributive Impact”
Source:
Page 16
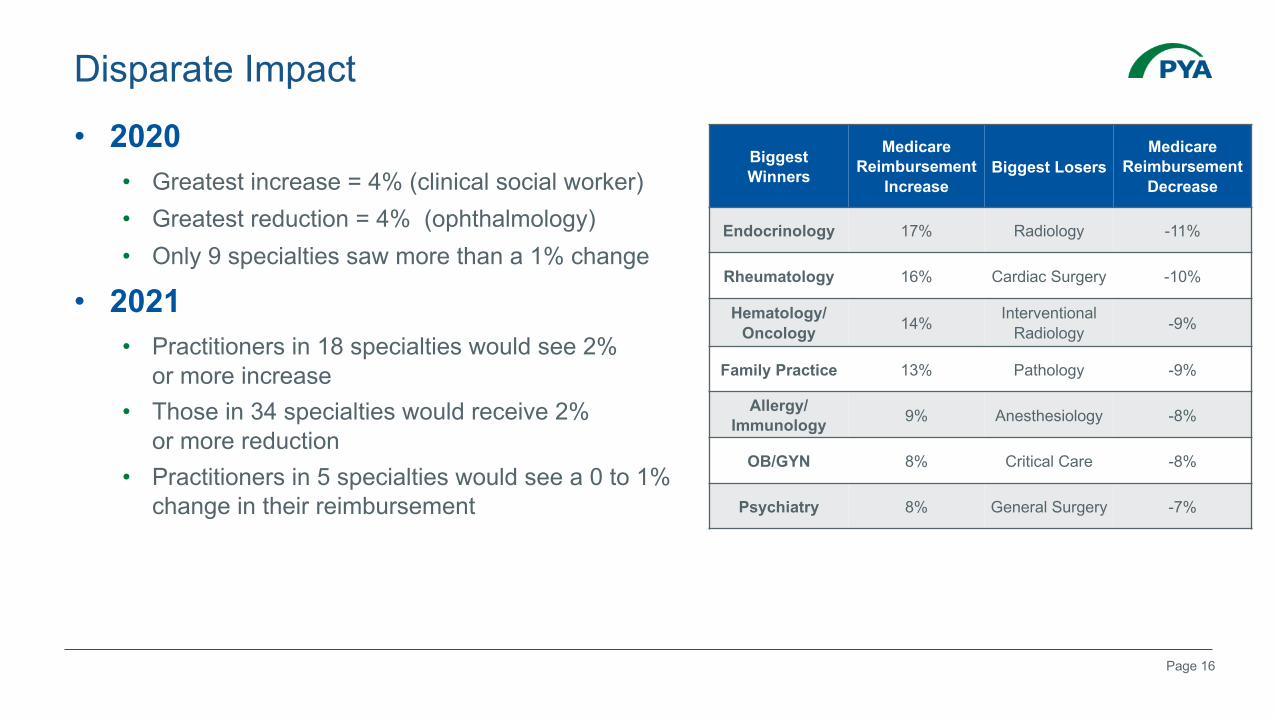
Biggest Winners
Medicare Reimbursement
IncreaseBiggest Losers
Medicare Reimbursement
Decrease
Endocrinology 17% Radiology -11%
Rheumatology 16% Cardiac Surgery -10%
Hematology/Oncology 14% Interventional
Radiology -9%
Family Practice 13% Pathology -9%
Allergy/Immunology 9% Anesthesiology -8%
OB/GYN 8% Critical Care -8%
Psychiatry 8% General Surgery -7%
• 2020• Greatest increase = 4% (clinical social worker) • Greatest reduction = 4% (ophthalmology)• Only 9 specialties saw more than a 1% change
• 2021• Practitioners in 18 specialties would see 2%
or more increase • Those in 34 specialties would receive 2%
or more reduction• Practitioners in 5 specialties would see a 0 to 1%
change in their reimbursement
Disparate Impact
Page 17
• CMS’ and the AMA’s collaboration has resulted in:• Revised Outpatient E/M code descriptions in the 2021 CPT Manual (99202-99215)
• 2021 E/M Guidelines published in 2021 CPT Manual effective January 1, 2021• MDM and Time redefined
• Omission of CPT Code 99201
• Revised Work Relative Value Units (wRVUs)
• No other E/M code set guidelines have been changed at this time; however, some other ranges’ values have been proposed to increase.
• Since the change is in CPT, impact will be industry-wide.
2021 E/M Guidelines History: How Did We Get Here?
Page 18
2021 E/M Changes: Key Elements
Eliminated history and physical
exam as elements for code selection
Modified MDM criteria with focus on tasks affecting management of
patient conditions
Allows providers to choose to select code
based on MDM or Total Time
Page 19
• The 2020 MPFS Final Rule adopted an add-on G-code to indicate E/M complexity of primary care and specialty care of ongoing complex conditions.
• The 2021 MPFS Proposed Rule requests comment to help clarify the definition of this code and has now been finalized as G2211.• G2211: Visit complexity inherent to E/M associated with medical care services that serve
as the continuing focal point for all needed health care services and/or with medical care services that are part of ongoing care related to a patient’s single, serious, or complex chronic condition. • Add-on code, list separately in addition to office/outpatient evaluation and management visit, new
or established
• Not restricted to a specialty
• Distinct from preventive and care management services
CMS G-Code
Page 20
CMS G-Code (cont’d)
“…we believe HCPCS add-on code GPC1X reflects thetime, intensity, and PE when practitioners furnish servicesthat enable them to build longitudinal relationships with allpatients (that is, not only those patients who have achronic condition or single high-risk disease) and toaddress the majority of patients’ health care needs withconsistency and continuity over longer periods of time.”
Source: 85 Fed. Reg. 50,138 (Aug. 17, 2020)
Page 21
2021 E/M Changes: Preparation Be aware of malpractice liability• Providers should continue to carefully document services being rendered to mitigate
malpractice implications.
Guard against fraud and abuse• Health systems should continue to perform monitoring and auditing to address refund
obligations from over-coding.
• Coding auditors should update audit tools to match guidelines.
Update compliance plan• Compliance officers should update current policies and procedures and include these codes
in the audit workplan.• Note: Do not eliminate references to 1995/1997 guidelines still in effect for other code ranges.
Evaluate EHR• Administrators should confirm EHR schedule and plans for implementing E/M code
changes, if any.
Page 22
2021 E/M Changes: Preparation (cont’d) Assess financial impact• Perform gap analyses to determine whether any financial impact will result from
code level selection changes per the new guidelines and the value changes by CMS.
• Consider provider compensation impacts relevant to wRVU and code utilization changes.
Confirm other payer requirements• Be aware of specific self-funded plan, other governmental, and commercial payer
requirements above and beyond the CMS changes and interpretations of the guidelines.
Page 23
3. Conversion Factor Reduction and Physician Compensation
Page 24
Impact: Independent Medical Specialists
• Direct impact to bottom line
• Increase in Medicare reimbursement if primarily an E/M practice• Potential increase in other payer reimbursement, if other payers utilize
reference pricing
• Additional reimbursement could help expand capacity for high risk and rising risk patients, thus increasing ability to participate in value-based models
Page 25
Impact: Independent Proceduralists
• Direct impact to bottom line
• Decrease in Medicare reimbursement• Potential decrease in other payer reimbursement, if other payers utilize
reference pricing
• 3 options:1. Do more procedures / grow market share
2. Reduce expenses
3. Pursue value-based payments
Page 26
Impact – Employed or Contracted Physicians
• Medical specialists• Increased Medicare reimbursement for the physician’s E/M services
• The same amount of work now will produce more wRVUs
• Employer will pay the physician more compensation for the same amount of work
• The incremental financial loss is limited to the amount the contracted conversion factor exceeds the actual reimbursement per wRVU received
Contractual conversion factor does not change(unless contract subsequently amended or renegotiated)
Page 27
• Proceduralists • Overall decreased Medicare reimbursement
• Some increase in total wRVUs due to increase in the RVUs for office/outpatient E/M codes (but far less than medical specialists who provide these services more regularly), with an overall net decrease in wRVUs (depending on E/M volume).
• Compensation would not be dramatically impacted
• Don’t forget anesthesia • Proposed conversion factor will decline from $22.20 per ASA unit to $20.05 per
ASA unit
• Impact to financial assistance subsidies caused by potentially lower collections
Impact – Employed or Contracted Physicians
Page 28
Contract Review Challenges
• Benchmark survey data tied to the compensation conversion factor will not fully reflect these impacts for another 2-3 years given normal timing lags in survey data and the varied rate with which contract modifications occur• It may be 2023 (based on 2022 data) before benchmark surveys have stabilized
from the impact.
• Documentation surrounding commercial reasonableness• Consider compensation structure alternatives
• Incentivize for managing high-risk and rising-risk patients
• Reduce healthcare costs
• Improve patient outcomes
Page 29
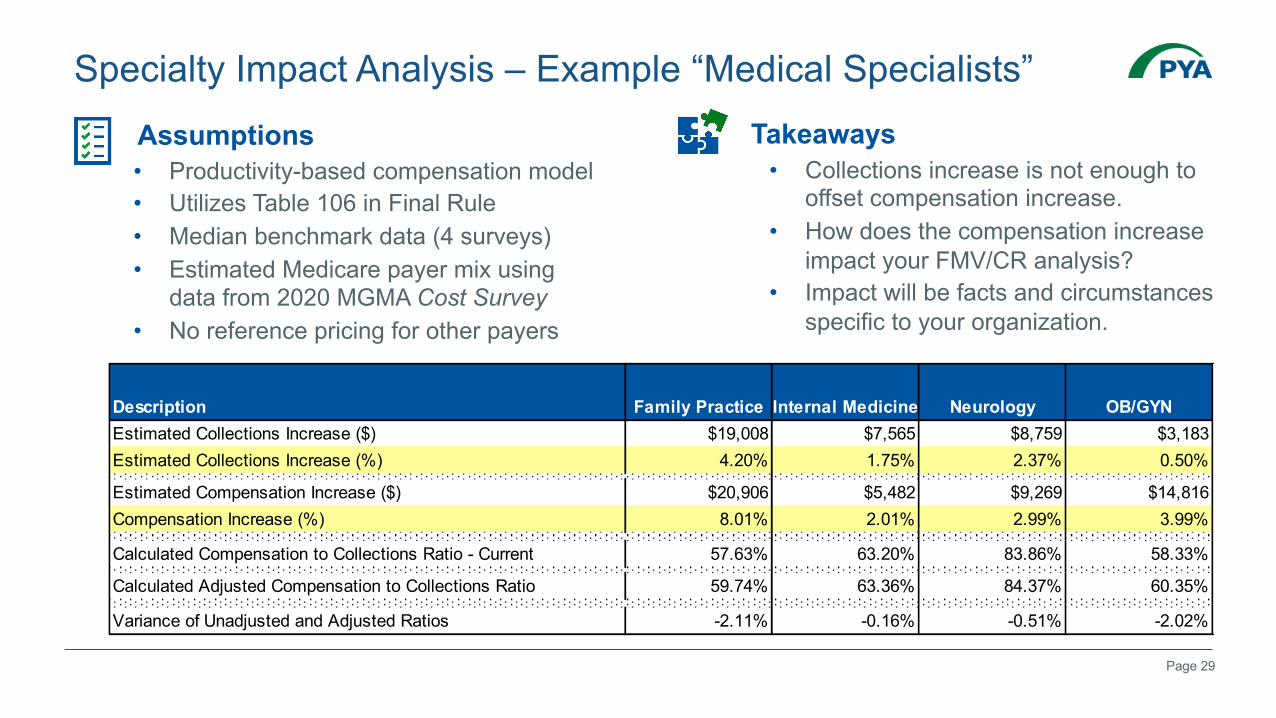
Specialty Impact Analysis – Example “Medical Specialists”Assumptions• Productivity-based compensation model• Utilizes Table 106 in Final Rule• Median benchmark data (4 surveys)• Estimated Medicare payer mix using
data from 2020 MGMA Cost Survey• No reference pricing for other payers
Takeaways• Collections increase is not enough to
offset compensation increase.• How does the compensation increase
impact your FMV/CR analysis?• Impact will be facts and circumstances
specific to your organization.
Description Family Practice Internal Medicine Neurology OB/GYNEstimated Collections Increase ($) $19,008 $7,565 $8,759 $3,183Estimated Collections Increase (%) 4.20% 1.75% 2.37% 0.50%
Estimated Compensation Increase ($) $20,906 $5,482 $9,269 $14,816Compensation Increase (%) 8.01% 2.01% 2.99% 3.99%
Calculated Compensation to Collections Ratio - Current 57.63% 63.20% 83.86% 58.33%
Calculated Adjusted Compensation to Collections Ratio 59.74% 63.36% 84.37% 60.35%
Variance of Unadjusted and Adjusted Ratios -2.11% -0.16% -0.51% -2.02%
Page 30
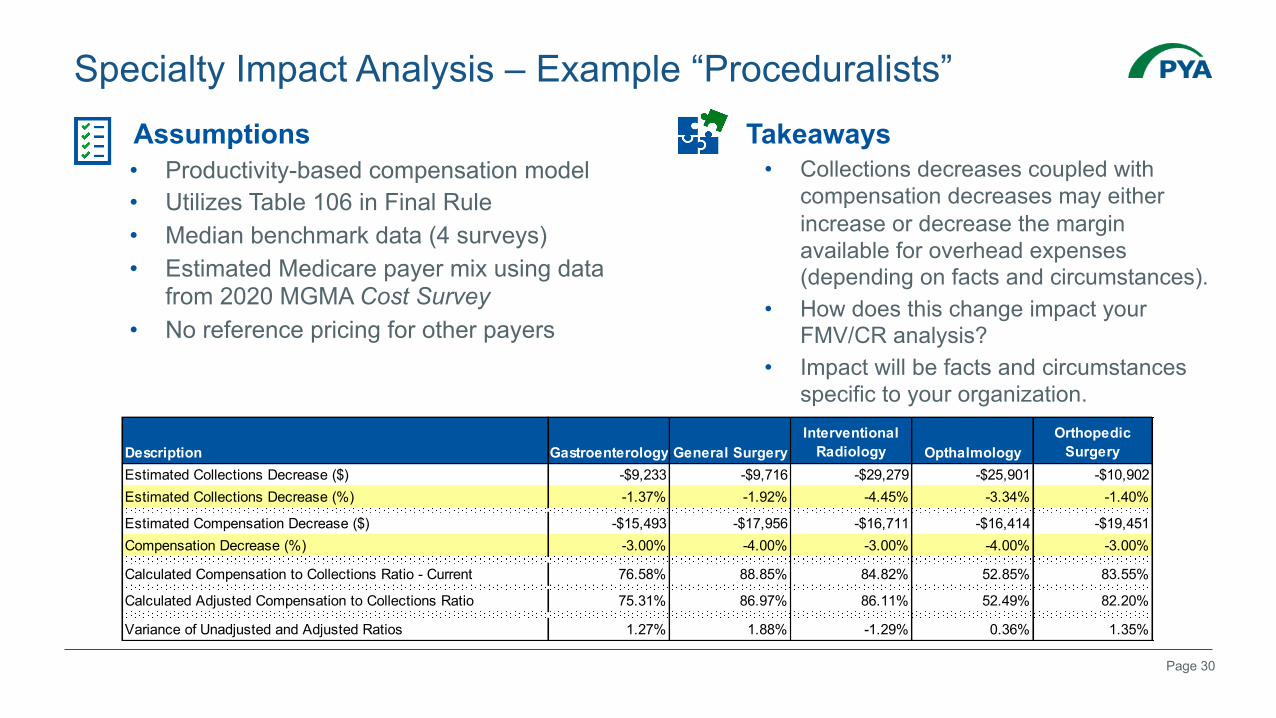
Specialty Impact Analysis – Example “Proceduralists”Assumptions• Productivity-based compensation model• Utilizes Table 106 in Final Rule• Median benchmark data (4 surveys)• Estimated Medicare payer mix using data
from 2020 MGMA Cost Survey• No reference pricing for other payers
Takeaways• Collections decreases coupled with
compensation decreases may either increase or decrease the margin available for overhead expenses (depending on facts and circumstances).
• How does this change impact your FMV/CR analysis?
• Impact will be facts and circumstances specific to your organization.
Description Gastroenterology General SurgeryInterventional
Radiology OpthalmologyOrthopedic
SurgeryEstimated Collections Decrease ($) -$9,233 -$9,716 -$29,279 -$25,901 -$10,902Estimated Collections Decrease (%) -1.37% -1.92% -4.45% -3.34% -1.40%
Estimated Compensation Decrease ($) -$15,493 -$17,956 -$16,711 -$16,414 -$19,451Compensation Decrease (%) -3.00% -4.00% -3.00% -4.00% -3.00%
Calculated Compensation to Collections Ratio - Current 76.58% 88.85% 84.82% 52.85% 83.55%
Calculated Adjusted Compensation to Collections Ratio 75.31% 86.97% 86.11% 52.49% 82.20%
Variance of Unadjusted and Adjusted Ratios 1.27% 1.88% -1.29% 0.36% 1.35%
Page 31
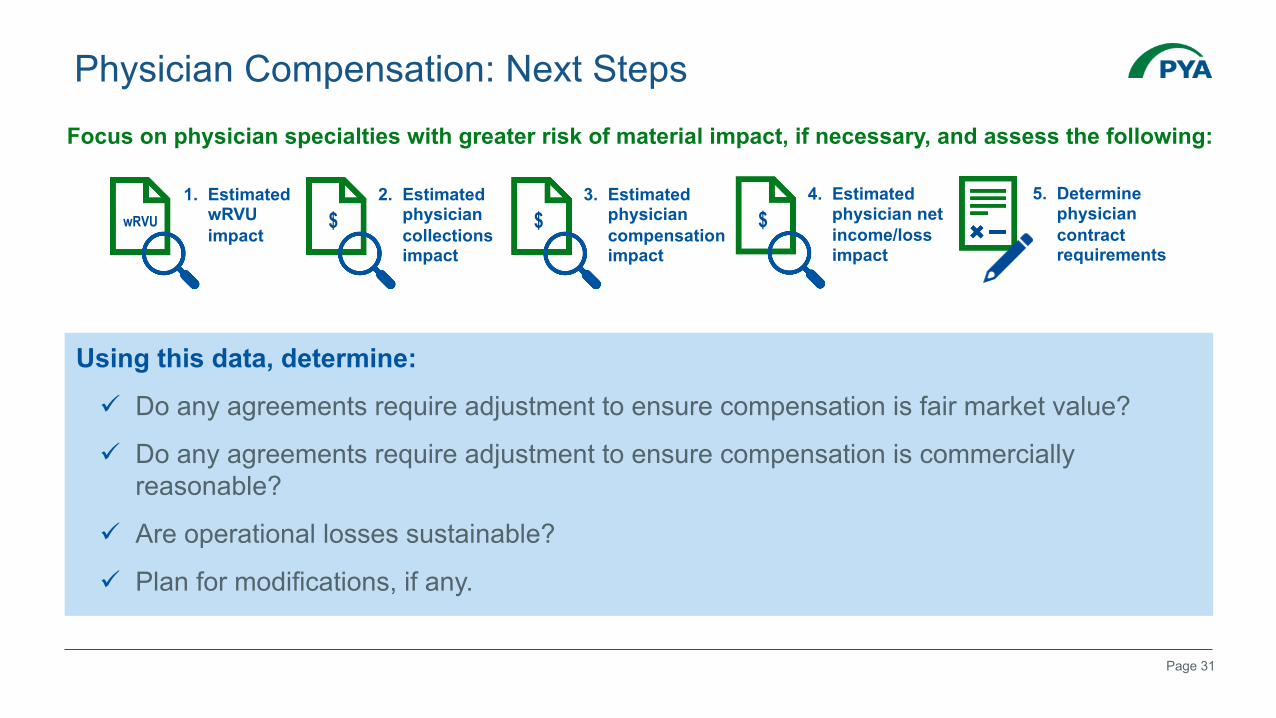
Physician Compensation: Next Steps
Using this data, determine:
ü Do any agreements require adjustment to ensure compensation is fair market value?
ü Do any agreements require adjustment to ensure compensation is commercially reasonable?
ü Are operational losses sustainable?
ü Plan for modifications, if any.
1. Estimated wRVU impact
wRVU
2. Estimated physician collections impact
$3. Estimated
physician compensation impact
$4. Estimated
physician net income/loss impact
$5. Determine
physician contract requirements
Focus on physician specialties with greater risk of material impact, if necessary, and assess the following:
Page 32
4. Care Management and Remote Patient Monitoring
Page 33
• 2018• CMS began reimbursing for CPT 99091
• Historically bundled into other services• Required 30 minutes of provider’s personal time, initiation during a face-to-face visit, patient consent
• 2019• CMS announced it would reimburse 3 new RPM codes
• CPT 99453: Remote monitoring of physiologic parameter(s) (e.g., weight, blood pressure, pulse oximetry, respiratory flow rate), initial; set-up and patient education on use of equipment.
• CPT 99454: Remote monitoring of physiologic parameter(s) (e.g., weight, blood pressure, pulse oximetry, respiratory flow rate), initial; each 30 days.
• CPT 99457: Remote physiologic monitoring treatment management services, 20 minutes or more of clinical staff/physician/other qualified health care professional time in a calendar month requiring interactive communication with the patient/caregiver during the month.• Note: clinical staff/physician/other qualified health care professional time
RPM: How did we get here?
Page 34
• 2020• CMS adopts revised code structure for 99457 and add-on code 99458
• CPT 99457: Remote physiologic monitoring treatment management services, clinical staff/physician/ other qualified health care professional time in a calendar month requiring interactive communication with the patient/caregiver during the month; initial 20 minutes.
• CPT 99458: Remote physiologic monitoring treatment management services, clinical staff/physician/ other qualified health care professional time in a calendar month requiring interactive communication with the patient/caregiver during the month; additional 20 minutes.
• No frequency limitation imposed
• Not available for RHC/FQHC billing
RPM: How did we get here? (cont’d)
Page 35
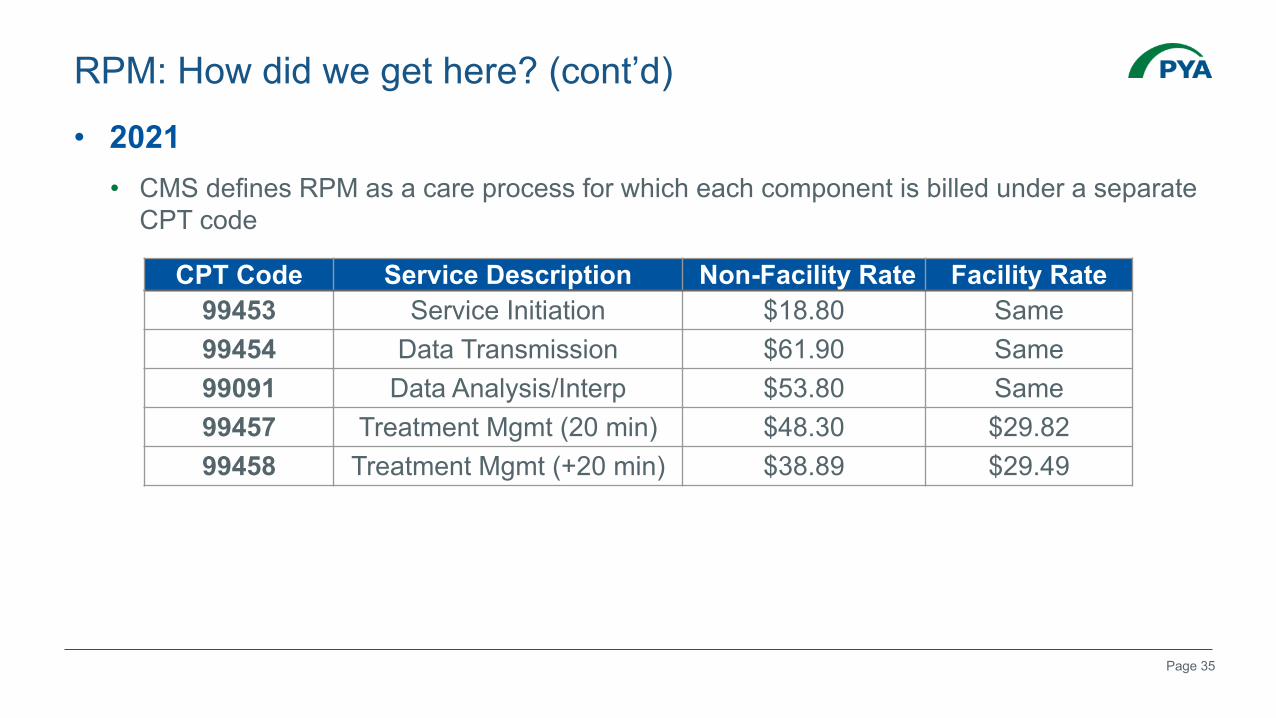
• 2021• CMS defines RPM as a care process for which each component is billed under a separate
CPT code
RPM: How did we get here? (cont’d)
CPT Code Service Description Non-Facility Rate Facility Rate99453 Service Initiation $18.80 Same99454 Data Transmission $61.90 Same99091 Data Analysis/Interp $53.80 Same99457 Treatment Mgmt (20 min) $48.30 $29.8299458 Treatment Mgmt (+20 min) $38.89 $29.49
Page 36
RPM: Ordering and Consent
• Ordering and billing must be done by eligible providers:ü Physicians and non-physician practitioners who are eligible to bill for E/M services
X Independent Diagnostic Testing Facilities
X Rural Health Clinics (RHCs)
X Federally Qualified Health Centers (FQHCs)
• Must have an established relationship with beneficiary, except that for duration of PHE, permitted for a new patient.
• Must obtain consent prior to or at the initiation of the service including acknowledgment of responsibility for co-payment or deductible; consent can be verbal but must be documented in the medical record.
Page 37
• Monitoring should: ü Relate to a chronic and/or acute illness or condition
ü Be reasonable, medically necessary, and “used to develop and manage a treatment plan related to a chronic and/or acute health illness or condition”
• Documentation of same should be included in patient’s medical record.
RPM: Medical Necessity
Page 38
• Device must:ü Meet the definition of “medical device” stated in section 201(h) of the Federal Food, Drug
and Cosmetic Act
ü Automatically upload patient physiologic data (i.e., data are not self-recorded and/or self-reported by the patient)
ü Be capable of generating and transmitting either (a) daily recordings of the beneficiary’s physiologic data, or (b) an alert if the beneficiary’s values fall outside pre-determined parameters.
ü Be reasonable and necessary for the diagnosis or treatment of the patient’s illness or injury or to improve the functioning of a malformed body member
ü Be used to collect and transmit reliable and valid physiologic data that allow an understanding of a patient’s health status in order to develop and manage a plan of treatment
RPM: Technology Requirements
Page 39
• Reimburse for practice expenses associated with furnishing RPM services including:• Cost associated with the monitoring device
• Its placement with the beneficiary
• Transmission of data to the billing practice
• No work Relative Value Unit assigned as no practitioner work – supervision or otherwise – is required.
CPT 99453 and 99454: What’s Included?
Page 40
• Report for device set-up and patient education
• Report for each episode of care which is defined by CPT Guidelines as “beginning when the remote monitoring physiologic service is initiated, and ends with attainment of targeted treatment goals” even if multiple devices are provided to the beneficiary.
• Should not be reported if monitoring is less than 16 days• During PHE, only 2 days of monitoring is required for patients with suspected or
confirmed cases of COVID-19.
CPT 99453: Service Initiation
Page 41
• Absent guidance by CMS, we recommend documenting:ü Practitioner order
ü Condition being monitored and medical necessity of the device
ü Beneficiary consent
ü Identification of the device
ü Date of the delivery to the patient
ü Date(s) training is provided
ü Place of service – location at which billing physician maintains his/her practice
ü Date of service – date on which the device records the 16th day of data in a 30-day period following initiation of the service (or the last date of that 30-day period)
CPT 99453: Documentation
Page 42
• Used to report the provision and programming of the device for daily recording or programmed alert transmissions over a 30-day period• Provided monitoring occurs during at least 16 days during the 30-day period
• Can only be billed once per 30-day period even if multiple devices are utilized
• Should not be reported if monitoring is less than 16 days• During PHE, only 2 days of monitoring is required for patients with suspected or
confirmed cases of COVID-19.
CPT 99454: Data Transmission
Page 43
• Absent guidance by CMS, we recommend ü Documentation sufficient to demonstrate monitoring occurred for at least 16 days in a 30-
day period.
ü Place of service – location at which billing physician maintains his/her practice
ü Date of service • If at least 16 days but less than 30 days:
• The last day the device records data and transmits it to the provider
• If more than 30 days:• The date of service for the first instance would be 30 days following the delivery of the device or completion
of training (whichever occurred later). The date of service for each instance thereafter would be 30 days from the prior date of billing, assuming at least 16 days monitoring occurred after prior date of service
CPT 99454: Documentation
Page 44
• Do not bill 99453 and 99454 when these services are including in other codes for the duration of time of the physiologic monitoring service.• Example: 95250 for continuous glucose monitoring requires a minimum of 72-hours of
monitoring
• CMS does not require practitioner to bill for 99091 or 99457 to bill for 99453 and 99454.
• CMS will not pay more than one practitioner for CPT 99453 for an episode of care or 99454 for a 30-day period, even if each is furnishing a distinct service.• No offered resolution for claims submitted by multiple practitioners
CPT 99453 and 99454: Billing Exceptions
Page 45
• “[A]fter the data collection period for CPT 99453 and 99454, the physiologic data that are collected and transmitted may be analyzed and interpreted as described in CPT 99091….”
• Performed by physician/NPP/clinical staff if “incident to” requirements are met• Requires direct supervision by the billing physician
• Due to PHE, direct supervision is permitted via interactive audio/visual real-time communications technology through December 31, 2021
• Agency will consider extension of this permission in 2022 rulemaking
CPT 99091: Data Analysis and Interpretation
Page 46
• Requires 30 minutes of services furnished over a 30-day period
• Valuation of the code includes 40 minutes of work, including:ü 5 minutes pre-service work (chart review), and
ü 5 minutes post-service work (chart documentation).
ü Therefore, these activities should not be counted toward 30-minutes.
• Appears to require at least 16 days of data except during PHE (2 days)
• CMS does not specifically address whether same technology requirements apply as for 99453 and 99454.
• Date of service – date on which 30 minutes accumulated or last day of the 30-day period
CPT 99091: Data Analysis and Interpretation (cont’d)
Page 47
• CPT 99457 – Initial 20 minutes
• CPT 99458 – Additional 20 minutes in the same calendar month• Requires “live interactive communication” with the patient during the month,
defined as “real-time synchronous, two-way audio interaction that is capable of being enhanced with video or other kinds of data transmission.”
• Requires general supervision• Must be billed under the NPI of the practitioner who supervises the clinical staff performing
the service
• No frequency limits imposed by CMS on CPT 99458
CPT 99457 and 99458: Treatment Management
Source: 85 Fed. Reg. 50,138 (Aug. 17, 2020)
Page 48
• CMS notes:• Codes may be reported during the same service period as chronic care management,
transitional care management and behavioral health integration services.• Do not count time for these services towards 99457 / 99458.
• Do not count any time on a day when the provider reports an E/M service including office or other outpatient services, domiciliary, rest home services or home services.
• Do not count time related to any other reported service.
CPT 99457 and 99458: Other Services
Page 49
• CMS provides the following guidance related to CCM and the same is assumed to apply:• Time spent on different days, or by different clinical staff members in the same calendar
month, can be aggregated to total 20 minutes.
• If two staff members are furnishing services at the same time (e.g., discussing the patient’s condition), the time can only be counted by one individual.
• Time less than 20 minutes cannot be rounded up; time cannot be carried forward to the next month.
CPT 99457 and 99458: Time Accumulation
Page 50
• Absent guidance by CMS, we recommend:ü The date and time spent providing the non-face-to-face services (including start and stop
times)
ü The name of the care team member providing services (with credentials)
ü A brief description of the services provided
ü Date of service (based on CCM) – 99457 - the date on which the 20th minute of work occurs or any date thereafter in the calendar month; 99458 - the date each subsequent 20 minutes occurs or any date thereafter in the calendar month
ü Place of service – location of billing physician’s practice
CPT 99457 and 99458: Documentation
Page 51
• CMS notes:• According to the CPT Codebook, CPT 99091 and 99457 cannot both be billed for the
same time period for the same beneficiary.
• However, CMS has determined that “in some instances when complex data are collected, more time devoted exclusively to data analysis and interpretation by a [practitioner] may be necessary such that the criteria could be met to bill for both CPT codes 99091 and 99457 within a 30-day period.” • CMS cautions, however, that one cannot use the same time to meet the criteria for both CPT
99091 and 99457.
CPT 99457 and 99091: Separate…but Together?
Page 52
• 2013• Finalized with 57 HCPCS that could not be billed concurrently
• 2020• Finalized “policy to allow concurrent billing of TCM services, when reasonable and
necessary, with 16 actively priced…codes during the 30-day period covered by TCM”
• 2021• Finalized removal of 14 additional codes (all ESRD) from the list of remaining codes that
could not be billed concurrently with TCM
• 2021• Finalized proposal to allow G2058 (CPT 99439) to also be billed concurrently
CPT 99495 and 99496: Transitional Care Management
Page 53
• G2214: (Initial or subsequent psychiatric collaborative care management, first 30 minutes in a month of behavioral health care manager activities, in consultation with a psychiatric consultant, and directed by the treating physician or other qualified healthcare professional)• Intended to capture 30 minutes of behavioral health care manager time
• Existing CoCM rules apply including general supervision
• CPT time rules apply consistent with 99492 – 99494
• Can be billed during same month as CCM and TCM
HCPCS G2214: Psychiatric Collaborative Care Model

Page 54
5. Telehealth and Virtual Services
Page 55
Source: https://www.cms.gov/newsroom/press-releases/trump-administration-finalizes-permanent-expansion-medicare-telehealth-services-and-improved-payment
Page 56
• Extend COVID-19 PHE telehealth flexibilities through December 31, 2021
• Details to come….
Emergency Coronavirus Relief Act of 2020
Page 57
How can we HELP?
Page 58
A national healthcare advisory services firm providing consulting, audit, and tax services

















