Homeless Children: Homeless Children: What Every Health Care Provider Should Know What Every Health Care Provider Should Know Catherine Karr, Catherine Karr, MD MD Joining Hands. Healing Joining Hands. Healing Lives. Lives. Health Care for the Homeless Health Care for the Homeless Clinicians’ Network Clinicians’ Network
Transcript
Homeless Children:Homeless Children:What Every Health Care Provider Should KnowWhat Every Health Care Provider Should Know
Catherine Karr, MDCatherine Karr, MD
Joining Hands. Healing Lives.Joining Hands. Healing Lives.Health Care for the Homeless Clinicians’ Health Care for the Homeless Clinicians’ NetworkNetwork
Acknowledgements
Prepared in collaboration with the Health Care for the Homeless Clinicians Network - Pediatric Work Group
Work space provided by the Harborview Injury and Prevention Research Center
Did you know?
The number of homeless families with children is increasing
The number of unaccompanied homeless adolescents is increasing
Homelessness is an important risk factor for a number of health issues
If you care for children….
You are likely to care for children who are homeless or at risk of becoming homeless
Contents
Recognizing homelessnessUnderstanding the specific health problems of homeless childrenInfectious disease, injury, lead, mental health & behavior problems, nutrition and growth, anemia, dental health, immunizations, asthma, vision, child abuse
Modifying health care plans and prevention strategiesFinding resources for your homeless patients and their families
This presentation is designed as a primer.
The goals are to help you:
Recognize homelessness and the risks of homelessness in families with childrenUnderstand the specific health problems of homeless childrenModify health care plans and prevention strategies appropriatelyKnow how to find resources for your homeless patients and their families
Recognizing homelessness and the risks of becoming homeless in families with children
A legal definition
Stewart B. McKinney Act, 42 U.S.C. § 11301, et seq. (1994)
a person who "lacks a fixed, regular, and adequate night-time residence and ... has a primary night time residency that is: (A) a supervised publicly or privately operated shelter designed to provide temporary living accommodations... (B) an institution that provides a temporary residence for individuals intended to be institutionalized, or (C) a public or private place not designed for, or ordinarily used as, a regular sleeping accommodation for human beings." 42 U.S.C. § 11302(a) The term "'homeless individual' does not include any individual imprisoned or otherwise detained pursuant to an Act of Congress or a state law." 42 U.S.C. § 11302.
An operational definitionHomelessness includes:
Camping with no permanent home to return to
Doubling-up temporarily with another family
Having no permanent place to return to after hospitalizationLiving out of a carLiving in an emergency or transitional shelter
Who is homeless?
40%
4%14%
40%
2%Families with ChildrenUnaccompanied minorsSingle WomenSingle MenNot specified
U.S. Conference of Mayors. A Status Report on Hunger and Homelessness in America’s Cities: a 27-city survey. December 2001.
What about homeless children?
41% are under age 5 1
85% are in families headed by single mothers 2
1. The Institute for Children and Poverty. Homeless in America: A Children’s Story. Part One. New York. 1999.2. The Better Homes Fund. Homeless Children: America’s New Outcasts. 1999.
How many childrenare homeless in the United States?
0
200,000
400,000
600,000
800,000
1,000,000
1,200,000
1,400,000
Estimates of Annual Number ofHomeless Children
U.S. Department ofEducation (1989)
General AccountingOffice (1989)
National Coalition for theHomeless (1990)
Urban Institute (2000)
National Coalition for theHomeless (2001)
Modified from Bassuk EL Homeless Families. Scientific American 265:66-74 (1991).
Recent estimates suggestthat 2% of American children are homeless in the course of one year.
Urban Institute. America’s Homeless II: Population & Services. February 2000.
Families with children are among the fastest growing segment of people experiencing homelessness
What are the trends?Nationwide, city officials predict:
Requests for emergency shelter by homeless families will increase (Request for shelter by homeless families 2000 - 01 - 22%)
The nation’s weak economy will mean that the number of homeless people will increase
U.S. Conference of Mayors. A Status Report on Hunger and Homelessness in America’s Cities: a 27-city survey. December 2001.
How can I identifyfamilies & children at risk?
Know the important risk factors for homelessness
Know how to ask sensitively about homelessness—homelessness carries a stigma
An overview of riskand protective factors that influence family homelessness
Bassuk EL et al. Homelessness in female-headed families: childhood and adult risk and protective factors. AJPH 87:242-248 (1997).
Public Sector Assistance forLow-Income Families
Precipitating Risk orProtective Factors
Childhood/DistalRisk Factors
BackgroundFactors
Proximal Risk Factors
Gender
Parental Socioeconomic Status
Race/Ethnicity
Events & conditionsin childhood
1. Monetary Resources2. Social Resources3. Non-cash Benefits4. Current Health Status5. Current Substance Use6. Primary Tenancy7. Pregnancy8. Dependent Children9. Partner Violence
Housing & Job Market Conditions
Homelessness
1. Work History2. Mental Health Status3. Chronic Health Conditions4. Educational Attainment5. Victimization6. Drug & Alcohol Use
Causes of homelessness:
Lack of affordable housingLow paying jobsSubstance abuse and lack of needed servicesMental illness and lack of needed servicesDomestic violenceUnemploymentPovertyPrison releaseChange/cuts in public assistance
U.S. Conference of Mayors. A Status Report on Hunger and Homelessness in America’s Cities: a 27-city survey. December 2001.
Lack of affordable housing:
The gap between the number of affordable housing units and the number of people who need them is the largest on record — 5.4 million units
National Coalition for the Homeless. NCH Fact sheet #1. Why Are People Homeless?June 1999.
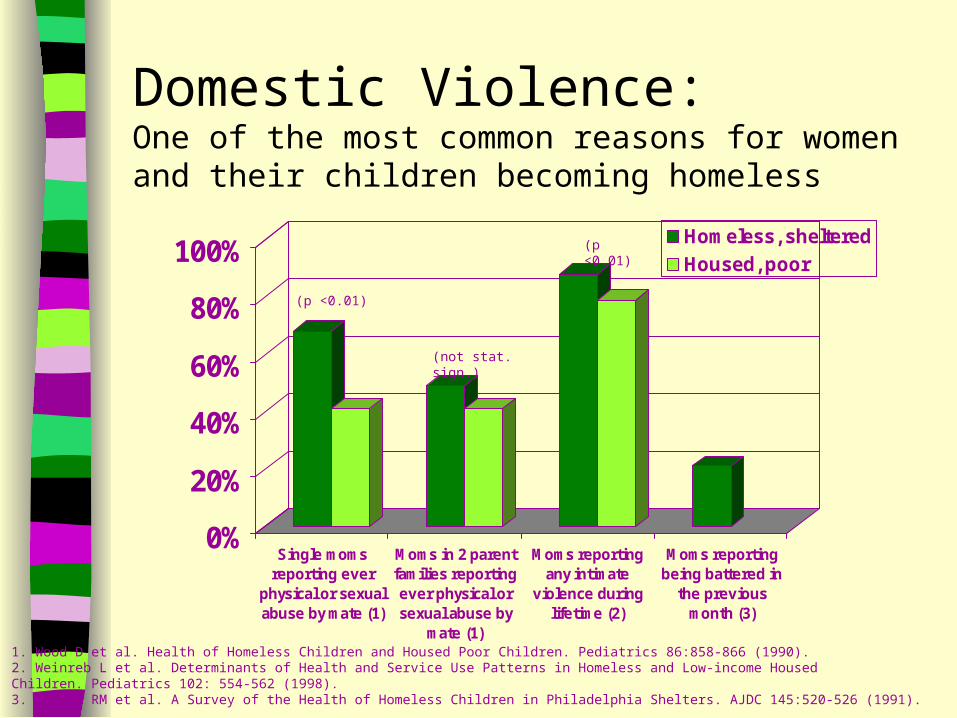
Domestic Violence: One of the most common reasons for women and their children becoming homeless
0%
20%
40%
60%
80%
100%
Single momsreporting ever
physical or sexualabuse by mate (1)
Moms in 2 parentfamilies reportingever physical orsexual abuse by
mate (1)
Moms reportingany intimate
violence duringlifetime (2)
Moms reportingbeing battered in
the previousmonth (3)
Homeless, sheltered
Housed, poor
1. Wood D et al. Health of Homeless Children and Housed Poor Children. Pediatrics 86:858-866 (1990).2. Weinreb L et al. Determinants of Health and Service Use Patterns in Homeless and Low-income HousedChildren. Pediatrics 102: 554-562 (1998).3. Parker RM et al. A Survey of the Health of Homeless Children in Philadelphia Shelters. AJDC 145:520-526 (1991).
(p <0.01)
(p <0.01)
(not stat. sign.)
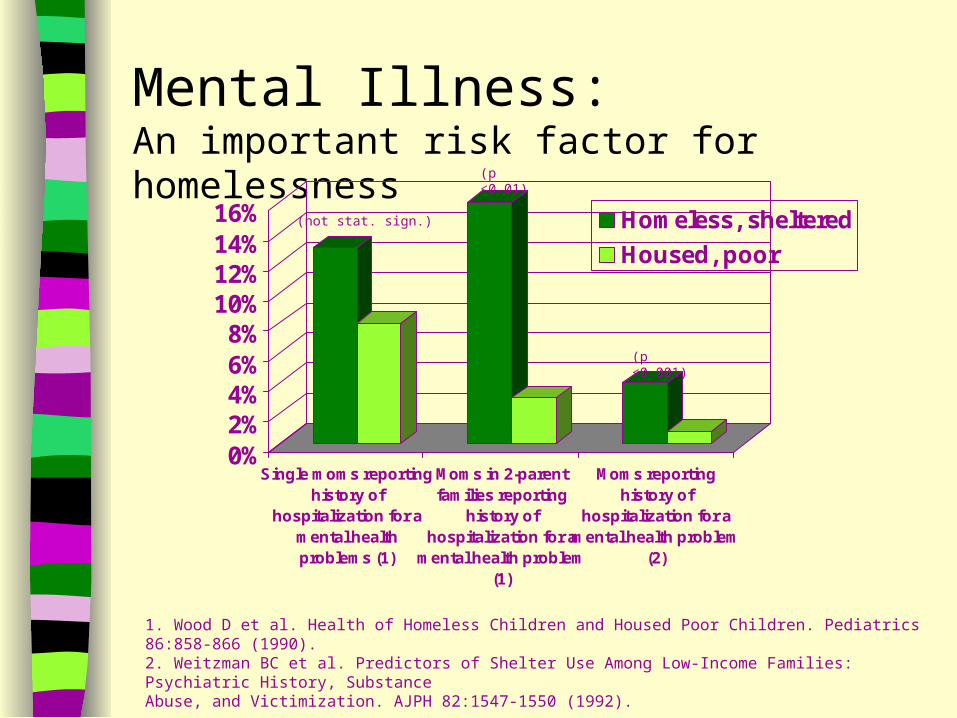
Mental Illness:An important risk factor for homelessness
0%2%4%6%8%
10%12%14%16%
Single moms reportinghistory of
hospitalization for amental healthproblems (1)
Moms in 2-parentfamilies reporting
history ofhospitalization for a
mental health problem(1)
Moms reportinghistory of
hospitalization for amental health problem
(2)
Homeless, sheltered
Housed, poor
(p <0.01)
(p <0.001)
1. Wood D et al. Health of Homeless Children and Housed Poor Children. Pediatrics 86:858-866 (1990).2. Weitzman BC et al. Predictors of Shelter Use Among Low-Income Families: Psychiatric History, SubstanceAbuse, and Victimization. AJPH 82:1547-1550 (1992).
(not stat. sign.)
Mental Illness: An under-treated problem
0%
2%
4%
6%
8%
Moms reporting use of prescriptiondrugs for mental health problem
Moms reporting use oftherapist/counselor/mental health
clinic
Homeless, sheltered Housed, poor
(p<0.001)
Weitzman BC et al. Predictors of Shelter Use Among Low-Income Families: Psychiatric History, SubstanceAbuse, and Victimization. AJPH 82:1547-1550 (1992).
Alcohol and drug abuseare associated with homelessness
0%
10%
20%
30%
40%
50%
Substance abuse problems(1)
Substance abuse problems- past 6 mo. (2)
Use of detox center forsubstance abuse (2)
Drug use = "big part" oftheir present problems (3)
Homeless, sheltered mothers Housed, poor mothers
(p<0.05)
(p<0.001)
(p<0.001)
1. Coll CG et al. The Developmental Status and Adaptive Behavior of Homeless and Low-Income Housed Infants and Toddlers. AJPH 88:1371-1374 (1998).2. Weitzman BC et al. Predictors of Shelter Use Among Low-Income Families: Psychiatric History, SubstanceAbuse, and Victimization. AJPH 82:1547-1550 (1992).3. Parker RM et al. A Survey of the Health of Homeless Children in Philadelphia Shelters. AJDC 145:520-526 (1991).
Substance abuseplays an important role in single parent families
0%
10%
20%
30%
40%
50%
60%
Single momsreporting
drug/alcoholabuse of mate
Moms in 2 parentfamilies reporting
drug/alcoholabuse of mate
Single momsreporting drug or
alcohol abuse
Moms in 2 parentfamilies reporting
drug or alcoholabuse
Homeless, sheltered Housed, poor(p<0.05)
(p<0.05)
Wood D et al. Health of Homeless Children and Housed Poor Children. Pediatrics 86:858-866 (1990).
(not stat. sign.)
(not stat. sign.)
Homelessnessis a dynamic state
Children are homeless on average 10 months at a time
25% of homeless children are homeless more than once
U.S. Department of Health & Human Services. Bureau of Primary Health Care. No Place to Call Home. April 2001.
Understanding the specific health problems of homeless children
How do the health issuesof homeless children differ from housed children?
Data are limited* but suggest an overall increased morbidity
The specific areas of concern and increased morbidity reflect “poverty medicine” in the extreme
*most studies are descriptive with small, non-representative samples and often without an appropriate comparison group
Overall Health
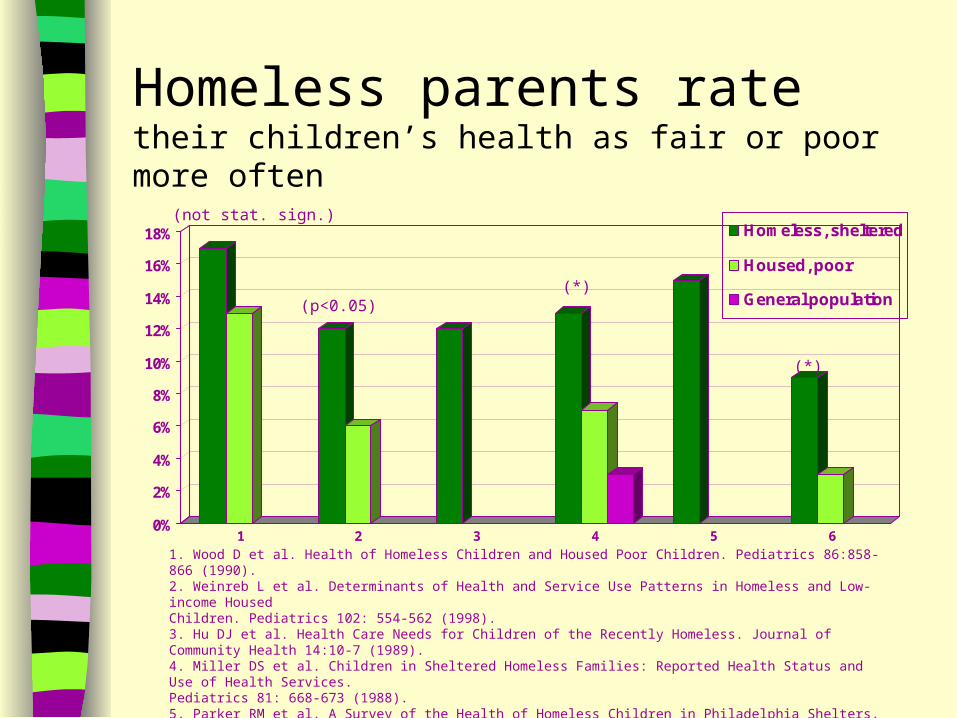
Homeless parents ratetheir children’s health as fair or poor more often
0%
2%
4%
6%
8%
10%
12%
14%
16%
18%
1 2 3 4 5 6
Homeless, sheltered
Housed, poor
General population
1. Wood D et al. Health of Homeless Children and Housed Poor Children. Pediatrics 86:858-866 (1990).2. Weinreb L et al. Determinants of Health and Service Use Patterns in Homeless and Low-income HousedChildren. Pediatrics 102: 554-562 (1998).3. Hu DJ et al. Health Care Needs for Children of the Recently Homeless. Journal of Community Health 14:10-7 (1989).4. Miller DS et al. Children in Sheltered Homeless Families: Reported Health Status and Use of Health Services. Pediatrics 81: 668-673 (1988).5. Parker RM et al. A Survey of the Health of Homeless Children in Philadelphia Shelters. AJDC 145:520-526 (1991)6. Menke EM & Wagner JD. A Comparative Study of Homeless, Previously Homeless, and Never Homeless School-Aged Children’s Health. Issues in Comprehensive Pediatric Nursing 20: 153-173 (1997).* No statistical comparison reported
(not stat. sign.)
(p<0.05)(*)
(*)
Hospitalizationis common for homeless children
Homeless Housed, poor
Hospitalization rate children < 18 years presenting to an ED 2
11.6/1000 7.5/1000 Alperstein et al. Am. J. Pub. Hlth. 78:1232-1233 (1988)
Hospitalized in the previous 12 months 1
11% 5% Weinreb et al. Pediatrics 102:554-562 (1998)
Homeless childrenare more likely to be seen in an ED
Homeless, sheltered
Housed, poor
Mean ED visits in previous year
1.6 1.0 p<0.01
Percent with 2 ED visits in the last year
38% 20% p<0.001
Weinreb L et al. Determinants of Health and Service Use Patterns in Homeless and Low-Income Housed Children. Pediatrics 102: 554-562 (1998).
Homeless childrenoften have multiple health problems
Homeless children compared with their housed schoolmates
Odds Ratio (95% confidence interval)
Children with any health problems vs. none
2.5 (1.4-4.5)
Children with multiple health problems vs. one
6.1 (2.3-16.0)
Berti LC et al. Comparison of Health Status of Children Using a School-Based Health Center for Comprehensive Care. Journal of Pediatric Health Care 15:244-250 (2001).
Clinic visits by homeless childrenunderscore increased acute problems Homeless Housed, poor Acute problem found during comprehensive care visit 1
8% 1% p<0.001
Mean number of clinic visits in the past year 2 5.6 3.8 p<0.001
1. Berti LC et al. Comparison of Health Status of Children Using a School-Based Health Center for Comprehensive Care. Journal of Pediatric Health Care 15:244-250 (2001).2. Weinreb L et al. Determinants of Health and Service Use Patterns in Homeless and Low-Income Housed Children. Pediatrics 102: 554-562 (1998).
Infectious Disease
Infectious Disease
Homeless families often live in crowded quarters, which increase the risk of the common infectious diseases of childhood such as upper respiratory infections, ear infections, and diarrhea
Infectious Disease
0%
10%
20%
30%
40%
50%
60%
70%
80%
Clinic visits for communicabledisease (1)
URI symptoms in the last month(2)
Homeless
Housed, poor
General population
(p<0.001)
1. Murata J et al. Disease Patterns in Homeless Children: A Comparison with National Data. Journal ofPediatric Nursing 7:196-204 (1992)2. Wood D et al. Health of Homeless Children and Housed Poor Children. Pediatrics 86:858-866 (1990).* No statistically significant difference between homeless and housed, no statistical comparison with general population reported.
(*)
Infectious Disease:Acute Otitis Media
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
AOM diagnosed during a clinic visit
Homeless childreninvolved in NYCchildren's health project(1999)
Subset of thesehomeless childrenundergoing behavioralevaluations (2000)
General population
The Children’s Health Fund. Still in Crisis: The health status of New York City’s homeless children. 1999.The Children’s Health Fund. The Crisis Continues: The health status of New York City’shomeless children. 2000.* No statistical comparison reported.
(*)
Infectious Disease:Diarrhea
0%
5%
10%
15%
20%
25%
30%
35%
Diarrhea in the last month
Homeless, sheltered
Housed, poor
General population
Wood D et al. Health of Homeless Children and Housed Poor Children. Pediatrics 86:858-866 (1990).*No statistically significant difference between homeless and housed, no statistical comparison with general population reported.
(*)
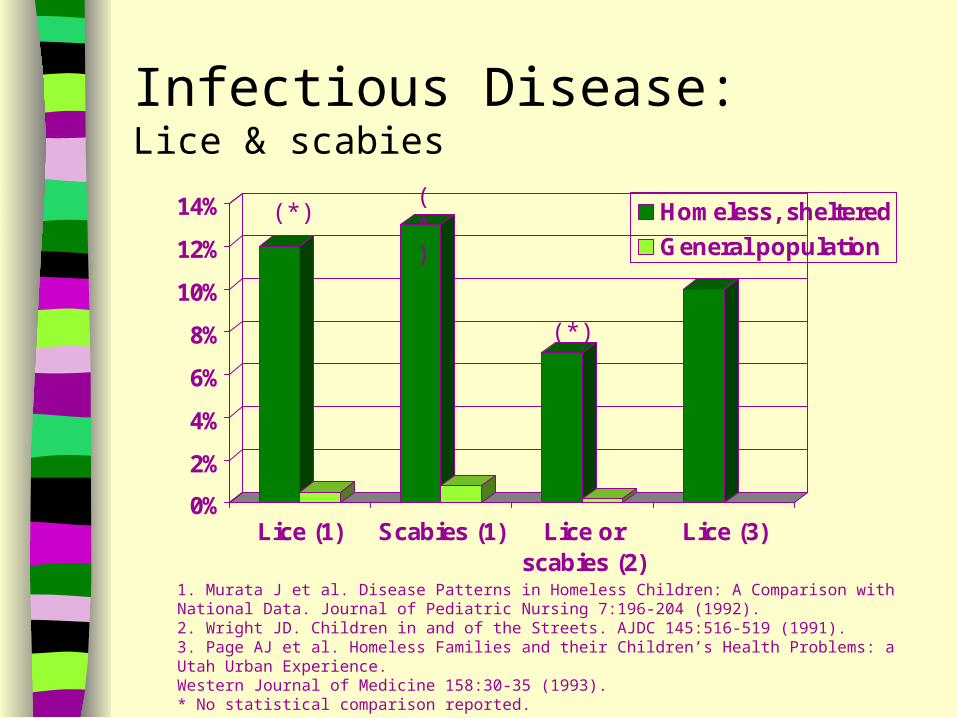
Infectious Disease:Lice & scabies
0%
2%
4%
6%
8%
10%
12%
14%
Lice (1) Scabies (1) Lice orscabies (2)
Lice (3)
Homeless, sheltered
General population
1. Murata J et al. Disease Patterns in Homeless Children: A Comparison with National Data. Journal of Pediatric Nursing 7:196-204 (1992).2. Wright JD. Children in and of the Streets. AJDC 145:516-519 (1991).3. Page AJ et al. Homeless Families and their Children’s Health Problems: a Utah Urban Experience.Western Journal of Medicine 158:30-35 (1993).* No statistical comparison reported.
(*)(*)
(*)
Injury
Injury
Homeless children live in less structured and less safe environments that may place them at risk of injury
Injury
0%2%4%6%8%
10%12%14%16%18%20%
Proportion ofoutpatient visits
for injury (1)
Accidentsrequiring medicalcare in the past
year (2)
ED visit forinjury/fall in the
past year (3)
Burn in the lastyear causingscarring (3)
Homeless
Housed, poor
General population
(p<0.05)
(not stat. sign.)
1. Murata J et al. Disease Patterns in Homeless Children: A Comparison with National Data. Journal of Pediatric Nursing 7:196-204 (1992).2. Weinreb L et al. Determinants of Health and Service Use Patterns in Homeless and Low-Income Housed Children. Pediatrics 102: 554-562 (1998).3. Parker RM et al. A Survey of the Health of Homeless Children in Philadelphia Shelters. AJDC 145:520-526 (1991).
Lead
Lead
Elevated blood lead levels are associated with povertyThis is related to increased exposure to dust and dilapidated housingThere may also be increased absorption of lead in settings of poor nutritionIron and calcium deficiencies increase lead absorption
Lead toxicityHomeless Housed, poor Source
Blood lead level > 30mcg/dL
3.8% 1.7% Clinic record review 1
(no statisticalcomparison reported)
Lead poisoning diagnosisin past year
10% Survey results 2
Blood lead level 10-15 mcg/dL 10-15 mcg/dL Children with elevatederythrocyteprotoporphyrin (>35ug/dL) 3
Goal blood lead level 10 mcg/dL 10 mcg/dL National HealthyPeople 2010 4
1. Alperstein G et al. Health Problems of Homeless Children in New York City. AJPH 78:1232-1233 (1988).2. Parker RM et al. A Survey of the Health of Homeless Children in Philadelphia Shelters. AJDC 145:520-526 (1991).3. Fierman AH et al. Status of Immunization and Iron Nutrition in New York City Homeless Children. ClinicalPediatrics 32:151-155 (1993).4. U.S. Department of Health & Human Services. Office of Disease Prevention and Health Promotion. Healthy People 2010: Understanding and Improving Health.
Lead screening is inadequate
Homeless Housed, poor
Screened(9 mo. – 6 yr.)
67% 81%
Weinreb L et al. Determinants of Health and Service Use Patterns in Homeless and Low-Income Housed Children. Pediatrics 102: 554-562 (1998).
Mental Health& Behavior Problems
Mental Health& Behavior Problems
Homeless children are more likely to come from backgrounds of domestic violence, mental illness, and substance abuse
These and other stresses associated with homelessness and poverty impact psychosocial well-being
Mental Health: A chart review of comprehensive care visits at a school-based clinic
0%1%2%3%4%5%6%7%8%9%
Identification of Mental HealthProblems
Homeless students
Housed students
Berti LC et al. Comparison of Health Status of Children Using a School-Based Health Center for Comprehensive Care. Journal Pediatric Health Care 15:244-250 (2001).
(p<0.05)
Depression:A summary of studies reporting performance on the Children’s Depression Inventory - School-Aged Children
0%
20%
40%
60%
1 2 3 4
Homeless
Housed, poor
Estimated prevalence inschool- age generalpopulation
Percent exceeding the cut-off suggesting further psychiatric evaluation
(not stat. sign.) (not stat. sign.)
1. Zima BT et al. Emotional and Behavioral Problems and Severe Academic Delays among Sheltered Homeless Children in Los Angeles County. AJPH 84:260-264 (1994).2. Menke EM & Wagner JD. A Comparative Study of Homeless, Previously Homeless, and Never Homeless School-Aged Children’s Health. Issues of Comprehensive Pediatric Nursing 20: 153-173 (1997).3. Menke EM. The Mental Health of Homeless School-age Children. JCAPN 11:87-98 (1998).4. Bassuk EL et al. Psychosocial characteristics of homeless children and children with homes. Pediatrics 85:257-261 (1990).
Behavior Problems:Children’s performance on the Behavior Problems Index
Mean score
Homeless, sheltered 43
Housed, poor 40
p<0.05
Differences were primarily due to aggressive behaviors such as frequently stubborn, sullen or irritable, hitting other children or adults, frequent temper tantrums
There were similar ratings on withdrawal, delinquency, and immaturity dimensions
Wood D et al. Health of Homeless Children and Housed Poor Children. Pediatrics 86:858-866 (1990).
Behavior Problems: Reported performance on the Child Behavior Checklist - School-Aged Children
0%
5%
10%
15%
20%
25%
30%
35%
40%
1 2 3
HomelessHoused, poor
Percent exceeding the cut-off suggesting further psychiatric evaluation:(criteria T>60 for 1,2, T>65 for 3)
1. Menke EM & Wagner JD. A Comparative Study of Homeless, Previously Homeless, and Never Homeless School-Aged Children’s Health. Issues in Comprehensive Pediatric Nursing 20: 153-173 (1997).2. Bassuk EL et al. Psychosocial characteristics of homeless children and children with homes. Pediatrics 85:257-261 (1990).3. Rescorla L et al. Ability, Achievement and Adjustment in Homeless Children. American Journal of Orthopsychology 61:210-220 (1991).
(not stat. sign.)(not stat. sign.)
(not stat. sign.)
Behavior Problems: Reported performance on the Child Behavior Checklist - Homeless School-aged Children
26% met criteria for clinical diagnosis (T>70)More problems in males.Compared to normative data:Homeless males had statistically significantly higher scores for total behavior and subcategories of externalizing, uncommunicative, and obsessive-compulsive behavior.
No statistically significant differences for homeless females.
9% met criteria for clinical diagnosis (T>70)Mean scores were comparable to population means.
Parker RM et al. A Survey of the Health of Homeless Children in Philadelphia Shelters. AJDC 145:520-526 (1991).
Menke EM. The Mental Health of Homeless School-Age Children. JCAPN 11:87-98 (1998).
Behavior Problems: Reported performance on the Child Behavior Checklist – Pre-School Children
Homeless, sheltered children compared with poor, housed childrenStatistically significant worse scores for total problems, externalizing and internalizing subgroup scoresTotal T score > 70 (clinical range)Homeless 21%Housed 5%
Homeless, sheltered children compared with normative dataNo statistically significant differences in scoresTotal T score > 70 (clinical range)Homeless 20%
Rescorla L et al. Ability, Achievement and Adjustment in Homeless Children. American Journal of Orthopsychology 61:210-220 (1991).
Parker RM et al. A Survey of the Health of Homeless Children in Philadelphia Shelters. AJDC 145:520-526 (1991).
Behavior Problems: Reported performance on the Simmons Behavior Checklist - Pre-School Children
Homeless, sheltered children compared with housed, poor children
No statistically significant difference in mean score or specific factor scores
Development
Development
Psychosocial and environmental stresses undermine normal development
Developmental screening has identified more developmental lags in homeless pre-school children
Among school-age children, academic problems are common
Denver Developmental Screening Test Results
Reported prevalence of homeless children failing at least one section—a wide range: 5 percent,1 15 percent,2 54 percent3
Reported prevalence of homeless children failing at least two sections—9 percent 2
Most common area of delay reported is speech/language (prevalence reported = 4 percent,1 13 percent,2 42 percent3)
1.Page AJ et al. Homeless families and their children’s health problems: a Utah urban experience. Western Journal of Medicine 158: 30-35 (1993).2. Wood D et al. Health of Homeless Children and Housed Poor Children. Pediatrics 86:858-866 (1990).3. Bassuk EL et al. Psychosocial characteristics of homeless children and children with homes. Pediatrics 85:257-261 (1990).
Denver Developmental Screening Test Results
0%
10%
20%
30%
40%
50%
60%
Failed 1 ormore sections
Speech Delay Gross MotorDelay
Fine MotorDelay
Personal/SocialDelay
Homeless, sheltered
Housed, poor
Bassuk EL et al. Psychosocial characteristics of homeless children and children with homes. Pediatrics 85:257-261 (1990).
(p<0.05)
(p<0.05)
(p<0.05)
(p<0.05)
(p<0.05)
Psychometric testingof pre-school children and toddlers
Homeless, sheltered pre-school children (age 3 - 5 years) performed more than one standard deviation below general population on tests of:
Homeless, sheltered toddlers (age 2) performed similarly to general population.
Parker RM et al. A Survey of the Health of Homeless Children in Philadelphia Shelters. AJDC 145:520-526 (1991).
Psychometric testingof school-age children
Homeless, sheltered children (age 6 - 12) performed more than one standard deviation below general population on tests of:verbal ability (WISC-revised vocabulary)reading (WRAT-R)
Only 30% of the homeless children were reading at age level
Parker RM et al. A Survey of the Health of Homeless Children in Philadelphia Shelters. AJDC 145:520-526 (1991).
Nutrition & Growth
Nutrition & Growth
Poverty has been associated with both obesity and malnutrition
Obesity reflects a diet containing excessive cheaper, carbohydrate rich foods
1. Miller DS et al. Children in Sheltered Homeless Families: Reported Health Status and Use of Health Services. Pediatrics 81: 668-673 (1988).2. Wood D et al. Health of Homeless Children and Housed Poor Children. Pediatrics 86:858-866 (1990).3. Alperstein G et al. Health Problems of Homeless Children in New York City. AJPH 78:1232-1233 (1988).* No statistical comparison made.
(*)
Accessto nutritious food is problematic
0%
2%
4%
6%
8%
10%
12%
14%
Parents report eating at a fast foodrestaurant or convenience store at least 4
times per week
Homeless, sheltered
Housed, poor
(p<0.01)
Wood D et al. Health of Homeless Children and Housed Poor Children. Pediatrics 86:858-866 (1990).
Accessto adequate amounts of food is problematic
0%
5%
10%
15%
20%
25%
Parents endorse children arehungry and not enough food fairly
often to always
Parents endorse children arehungry and not enough to eat
because of lack of money for 4 ormore days in past month
Homeless, sheltered Housed, poor
(p<0.01) (p<0.01)
Wood D et al. Health of Homeless Children and Housed Poor Children. Pediatrics 86:858-866 (1990).
Evidence of stuntingin homeless children: chronic malnutrition decreases attained height
0
10
20
30
40
50
60
70
<5th 5th-24th
25th-49th
50th-74th
75th-95th
>95th
Homeless
Housed, poor
General Population(NCHS)
Fierman AH et al. Growth Delay in Homeless Children. Pediatrics 88:918-925 (1991).
Percentile Distribution of Height
Evidence of obesityin poor, housed children
0
10
20
30
40
50
60
<5th 5th-24th
25th-49th
50th-74th
75th-95th
>95th
Homeless
Housed, poor
General Population(NCHS)
Fierman AH et al. Growth Delay in Homeless Children. Pediatrics 88:918-925 (1991).
1. Parker RM et al. A Survey of the Health of Homeless Children in Philadelphia Shelters. AJDC 145:520-526 (1991).2. Fierman AH et al. Status of Immunization and Iron Nutrition in New York City Homeless Children. ClinicalPediatrics 32:151-155 (1993).3. Page AJ et al. Homeless families and their children’s health problems: a Utah urban experience. Western Journal of Medicine 158: 30-35 (1993).
Dental Health
Dental cariesand lack of dental care is common among the poor
36% of children have dental problems according to homeless families surveyed 1
28% of children have visible caries according to providers of health care for homeless children 2
10 times rate of poor dentition in homeless children compared with general population according to national homeless health care providers 3
1. Miller DS et al. Children in Sheltered Homeless Families: Reported Health Status and Use of Health Services. Pediatrics 81: 668-673 (1988).2. Page AJ et al. Homeless families and their children’s health problems: a Utah urban experience. Western Journal of Medicine 158: 30-35 (1993).3. Wright JD. Children in and of the Streets. AJDC 145:516-519 (1991).
Access to Dental Care
0%5%
10%15%20%25%30%35%40%45%50%
Percent of school aged children who have notseen a dentist in the previous year
Homeless
Previouslyhomeless, poorNever homeless
Menke EM & Wagner JD. A Comparative Study of Homeless, Previously Homeless, and Never Homeless School-Aged Children’s Health. Issues in Comprehensive Pediatric Nursing 20: 153-173 (1997).*No statistical comparison reported.
(*)
Immunization Delay
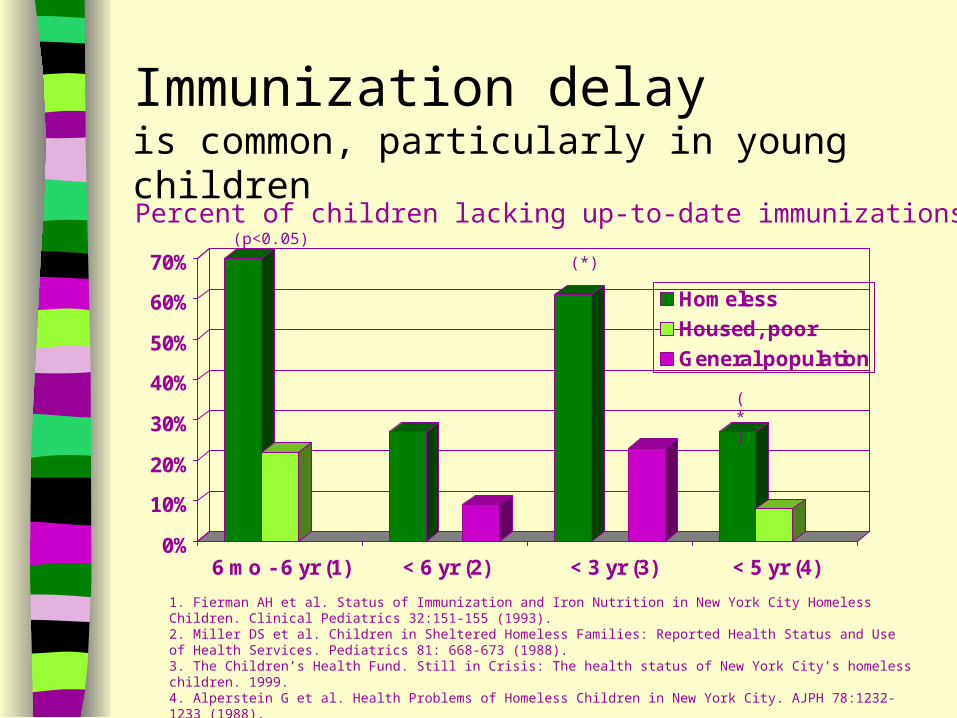
Immunization delayis common, particularly in young children
0%
10%
20%
30%
40%
50%
60%
70%
6 mo - 6 yr (1) < 6 yr (2) < 3 yr (3) < 5 yr (4)
Homeless
Housed, poor
General population
Percent of children lacking up-to-date immunizations(p<0.05)
(*)
1. Fierman AH et al. Status of Immunization and Iron Nutrition in New York City Homeless Children. Clinical Pediatrics 32:151-155 (1993).2. Miller DS et al. Children in Sheltered Homeless Families: Reported Health Status and Use of Health Services. Pediatrics 81: 668-673 (1988).3. The Children’s Health Fund. Still in Crisis: The health status of New York City’s homeless children. 1999. 4. Alperstein G et al. Health Problems of Homeless Children in New York City. AJPH 78:1232-1233 (1988).*No statistical comparison reported.
(*)
Immunization delayin school-aged children
0%
2%
4%
6%
8%
10%
12%
14%
16%
6-12 yr (1) 8-12 yr (2)
Homeless
Housed, poor
Percent of children lacking up-to-date immunizations
1. Berti LC et al. Comparison of Health Status of Children Using a School-Based Health Center for Comprehensive Care. Journal of Pediatric Health Care 15:244-250 (2001).2. Menke EM & Wagner JD. A Comparative Study of Homeless, Previously Homeless, and Never Homeless School-Aged Children’s Health. Issues in Comprehensive Pediatric Nursing 20: 153-173 (1997).* no statistical comparison reported
(not stat. sign.)
(*)
Asthma
Asthma ratesincrease with poverty
Dust mites, cockroaches, rodents, and indoor molds are common asthma triggers found in most shelter housingUpper respiratory infection is common in homeless children and is a well-identified asthma triggerThere is increasing evidence that psychosocial stress may also be an important asthma trigger
Asthma
0%
5%
10%
15%
20%
25%
30%
35%
40%
Asthmadiagnosis (1)
Asthmadiagnosis (2)
Asthmasymptoms in the
past month (3)
Asthmasymptoms in the
past month (4)
Hospitalized forasthma in thepast year (5)
Homeless
Housed, poor
General population
1. Berti LC et al. Comparison of Health Status of Children Using a School-Based Health Center for Comprehensive Care. Journal of Pediatric Health Care 15:244-250 (2001).2. The Children’s Health Fund. Still in Crisis: The health status of New York City’s homeless children. 1999.3. Wood D et al. Health of Homeless Children and Housed Poor Children. Pediatrics 86:858-866 (1990).4. Weinreb L et al. Determinants of Health and Service Use Patterns in Homeless and Low-Income Housed Children. Pediatrics 102: 554-562 (1998).5. Parker RM et al. A Survey of the Health of Homeless Children in Philadelphia Shelters. AJDC 145:520-526 (1991).* No statistical comparison reported.
(p<0.05)(*)
(p<0.01)(not stat. sign.)
Vision
Problems with visionare common among homeless children
0%
5%
10%
15%
20%
25%
30%
1 2 3
Homeless
Housed
Percent with visual acuity deficits identified during screening
(p<0.01)
1. Berti LC et al. Comparison of Health Status of Children Using a School-Based Health Center for Comprehensive Care. Journal of Pediatric Health Care 15:244-250 (2001).2. Parker RM et al. A Survey of the Health of Homeless Children in Philadelphia Shelters. AJDC 145:520-526 (1991).3. Page AJ et al. Homeless families and their children’s health problems: a Utah urban experience. Western Journalof Medicine 158: 30-35 (1993).
Child Abuse
Child Abuse
It is well known that perpetrators of child abuse are often victims of abuse themselves
As such, it is not surprising that many homeless children are at risk of abuse
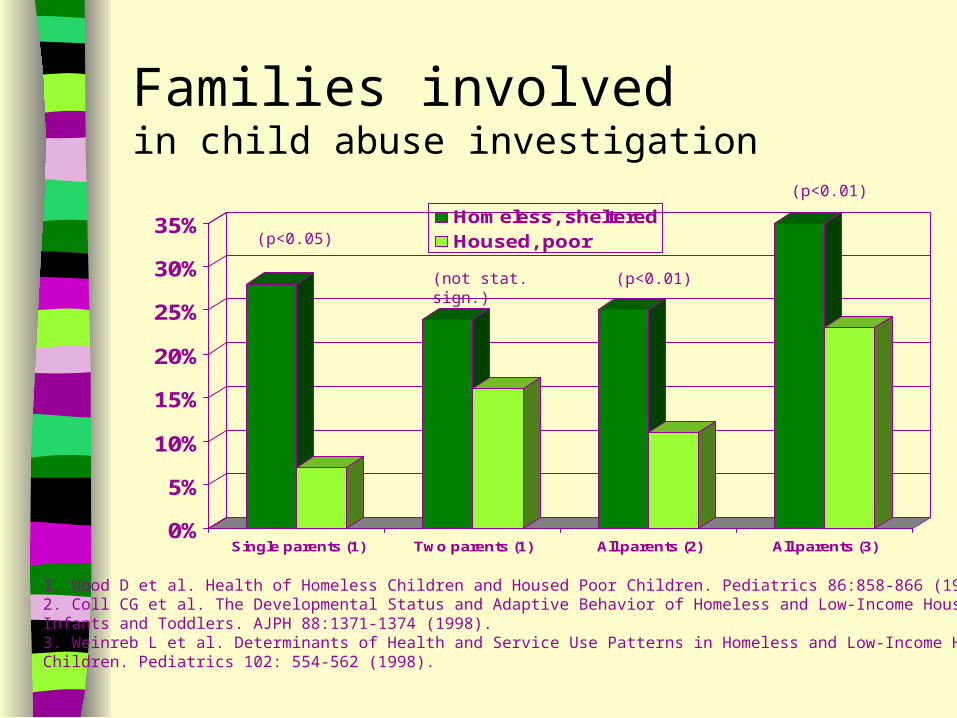
Families involvedin child abuse investigation
0%
5%
10%
15%
20%
25%
30%
35%
Single parents (1) Two parents (1) All parents (2) All parents (3)
Homeless, shelteredHoused, poor(p<0.05)
(not stat. sign.) (p<0.01)
(p<0.01)
1. Wood D et al. Health of Homeless Children and Housed Poor Children. Pediatrics 86:858-866 (1990).2. Coll CG et al. The Developmental Status and Adaptive Behavior of Homeless and Low-Income Housed Infants and Toddlers. AJPH 88:1371-1374 (1998).3. Weinreb L et al. Determinants of Health and Service Use Patterns in Homeless and Low-Income Housed Children. Pediatrics 102: 554-562 (1998).
Families reportingabuse of their children
0%
2%
4%
6%
8%
10%
12%
Physically abused in thepast year (1)
Ever physically orsexually abused (2)
Homeless
Housed, poor
1. Parker RM et al. A Survey of the Health of Homeless Children in Philadelphia Shelters. AJDC 145:520-526 (1991). 2. Weinreb L et al. Determinants of Health and Service Use Patterns in Homeless and Low-Income Housed Children. Pediatrics 102: 554-562 (1998).
(not stat. sign.)
Homeless Child Syndrome
In summary, the typical homeless child problem list will include:
poverty-related health problemsimmunization delaysuntreated or under-treated acute and chronic problemsmental health, behavior and academic problemschild abuse/neglect
Modifying health care plans and prevention strategies
Homelessnesscarries a stigma
Determining housing status requires asking questions in a sensitive and non-threatening manner
Suggested assessment questions
Do you have safe and permanent housing?
Where are you staying? How long have you been there?
Have there been any changes in your housing situation since your last visit?
Suggested assessment questions (continued)
Do you have any concerns about your housing?
How many times have you moved in the last year? Homeless mothers living in shelters move an average of three to four times per year
Altering your plan of care
Determine the safety of the living environment
If it is not safe, provide access to resources
Altering your plan of care
Recognize that homelessness is dynamic
Reassess potential for homelessness at every encounter
Altering your plan of care
Use acute problem visits as a “window of opportunity”
Provide a thorough medical, developmental and psychological history as well as physical exam
Altering your plan of care
Be alert to medical conditions that result from lack of access to medical care, preceded homelessness, or occur with homelessness
Prescribing practices should reflect the fact that the child may be living and eating in a shelter or on the street
Altering your plan of care
Pay particular attention to health care maintenance
Provide immunizations and screening for lead toxicity, anemia, visual acuity, and hearing loss
Monitor growth and nutrition
Altering your plan of care
Provide a “medical home”
Include primary pediatric care plus access to subspecialty care, developmental and psychological evaluation/treatment, medication and medical devices, case management, and 24 hr/7day access through an answering service
Altering your plan of care
Address continuity of care limitations
Ensure patient transportation and availability of providers
Ensure means of communication taking into consideration that patients often have limited phone access
Altering your plan of care
Screen parents for depression, substance abuse, and child abuse or neglect
Make appropriate referrals
As a final reality check, ask the parent if there is anything in the plan that will be difficult or impossible to follow
Know how to find resources for your homeless patients and their families
Finding resources
Web-based information
Health Care for the Homeless Information Resource Center
www.hchirc.comWeb site supported by Health Resources & Service Administration, U.S. Department of Health & Human ServicesIncludes state-based directory of health care for the homeless projectsLinks to federal agencies, national and student organizationsLinks to hotlines including domestic violence and crisis lines
Finding resources
Web-based information
National Health Care for the Homeless Council and HCH Clinicians’ Network
www.nhchc.org Web site for membership organization serving health care providers working with homeless people across the U.S.Features numerous publications including Healing Kids: the pediatric interest group updateIncludes sections on training, research, public policy and advocacyLinks to other organizations and agencies serving homeless populations
Finding resources
Print-based informationNo place to call home: Overview of outreach and primary health care services for the Homeless Children’s Program. 2001. (Health Care for the Homeless Information Resource Center; phone 1 888-439-3300)
America’s Homeless Children: New Outcasts. A Public Policy Report from The Better Homes Fund. 1999. (617/964-3834)
Homelessness and Children
“It is hard to imagine a social environment less conducive to health or normal maturation and development.”
—J.D. Wright
References used in this presentation
U.S. Conference of Mayors. A Status Report on Hunger and Homelessness in America’s Cities: a 27-city survey. December 2001
The Institute for Children and Poverty. Homeless in America: A Children’s Story. Part One. New York. 1999.The Better Homes Fund. Homeless Children: America’s New Outcasts. 1999. Bassuk EL. Homeless Families. Scientific American 265:66-74 (1991).Urban Institute. America’s Homeless II: Population & Services. February 2000.
(www.urban.org/presentations/AmericasHomelessII/index/htm) Bassuk EL et al. Homelessness in female-headed families: childhood and adult risk and protective factors.
AJPH 87:242-248 (1997). National Coalition for the Homeless. NCH Fact sheet #1. Why Are People Homeless?June 1999. Wood D et al. Health of Homeless Children and Housed Poor Children. Pediatrics 86:858-866 (1990).Weinreb L et al. Determinants of Health and Service Use Patterns in Homeless and Low-Income Housed
Children. Pediatrics 102: 554-562 (1998).Parker RM et al. A Survey of the Health of Homeless Children in Philadelphia Shelters. AJDC 145:520-526
(1991).Weitzman BC et al. Predictors of Shelter Use Among Low-Income Families: Psychiatric History, Substance
Abuse, and Victimization. AJPH 82:1547-1550 (1992). Coll CG et al. The Developmental Status and Adaptive Behavior of Homeless and Low-Income Housed Infants
and Toddlers. AJPH 88:1371-1374 (1998).Parker RM et al. A Survey of the Health of Homeless Children in Philadelphia Shelters. AJDC 145:520-526
(1991).U.S. Department of Health & Human Services. Bureau of Primary Health Care. No Place to Call Home. April
2001. Wood D et al. Health of Homeless Children and Housed Poor Children. Pediatrics 86:858-866 (1990).Hu DJ et al. Health Care Needs for Children of the Recently Homeless. Journal of Community Health 14:10-7
(1989).
References used in this presentation
Miller DS et al. Children in Sheltered Homeless Families: Reported Health Status and Use of Health Services. Pediatrics 81: 668-673 (1988).
Menke EM & Wagner JD. A Comparative Study of Homeless, Previously Homeless, and Never Homeless School-Aged Children’s Health. Issues in Comprehensive Pediatric Nursing 20: 153-173 (1997).
Berti LC et al. Comparison of Health Status of Children Using a School-Based Health Center for Comprehensive Care. Journal of Pediatric Health Care 15:244-250 (2001).
Murata J et al. Disease Patterns in Homeless Children: A Comparison with National Data. Journal of Pediatric Nursing 7:196-204 (1992).
The Children’s Health Fund. Still in Crisis: The health status of New York City’s homeless children. 1999. The Children’s Health Fund. The Crisis Continues: The health status of New York City’s homeless children.
2000.Wright JD. Children in and of the Streets. AJDC 145:516-519 (1991).Page AJ et al. Homeless Families and their Children’s Health Problems: a Utah Urban Experience. Western
Journal of Medicine 158:30-35 (1993). Alperstein G et al. Health Problems of Homeless Children in New York City. AJPH 78:1232-1233 (1988).Fierman AH et al. Status of Immunization and Iron Nutrition in New York City Homeless Children. Clinical
Pediatrics 32:151-155 (1993).U.S. Department of Health & Human Services. Office of Disease Prevention & Health Promotion. Healthy
People 2010: Understanding and Improving Health. Zima BT et al. Emotional and Behavioral Problems and Severe Academic Delays among Sheltered Homeless
Children in Los Angeles County. AJPH 84:260-264 (1994).Menke EM. The Mental Health of Homeless School-Age Children. JCAPN 11:87-98 (1998).Bassuk EL et al. Psychosocial characteristics of homeless children and children with homes. Pediatrics
85:257-261 (1990). Rescorla L et al. Ability, Achievement and Adjustment in Homeless Children. American Journal of
Orthopsychology 61:210-220 (1991). Fierman AH et al. Growth Delay in Homeless Children. Pediatrics 88:918-925 (1991). Wright JD. Children in and of the Streets. AJDC 145:516-519 (1991).