Page 1
HormonalContraceptives:wheredowebegin?
StephanieSchauner,PharmDClinicalAssociateProfessorUMKCSchoolofPharmacyschauners@umkc.edu
ClinicalPharmacistGoppert-TrinityFamilyCareClinic
KansasCity,MO 1
Page 2
LearningObjectives
Describethemechanismofaction,formulations,doses,andusesofhormonalcontraceptives.Comparethebenefitsvs.risksoforalcontraceptives.Developappropriatecounselingpointstosharewithpatientsregardingoralcontraceptives.Identifyusefulresourcesavailableforhormonaluseofcontraceptives.
2
Page 3
Disclosure:
• StephanieSchauner doesnothaveanypotentialconflictsofinterestinrelationtothispresentation.
3
Page 4
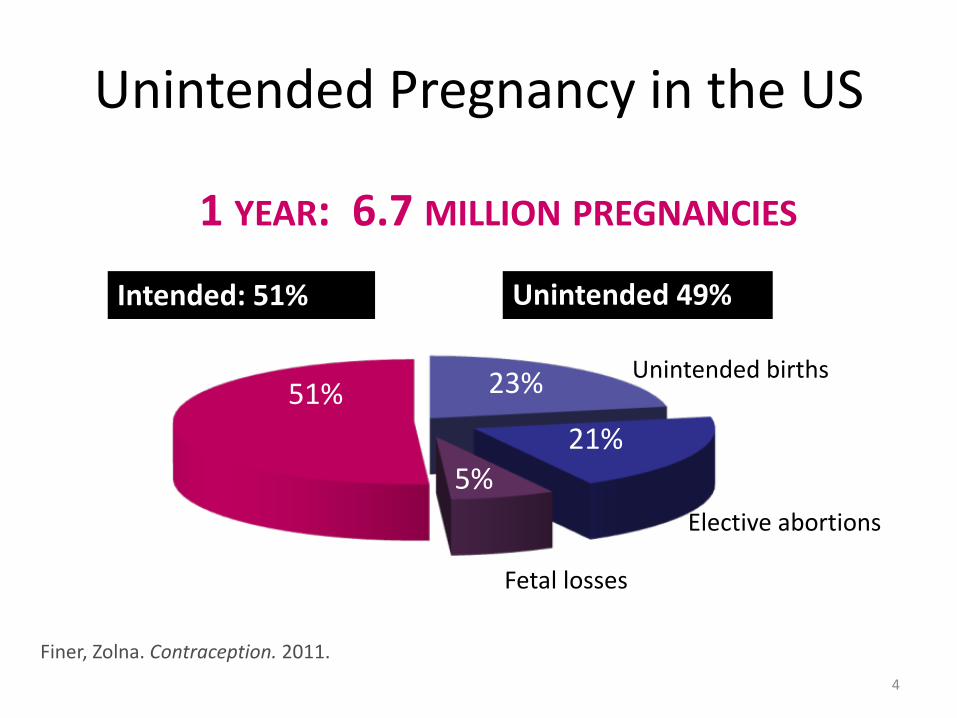
UnintendedPregnancyintheUS
Finer,Zolna.Contraception.2011.
Unintended49%
Unintendedbirths
Electiveabortions
Fetallosses
Intended:51%
51% 23%
21%5%
1YEAR:6.7MILLION PREGNANCIES
4
Page 7
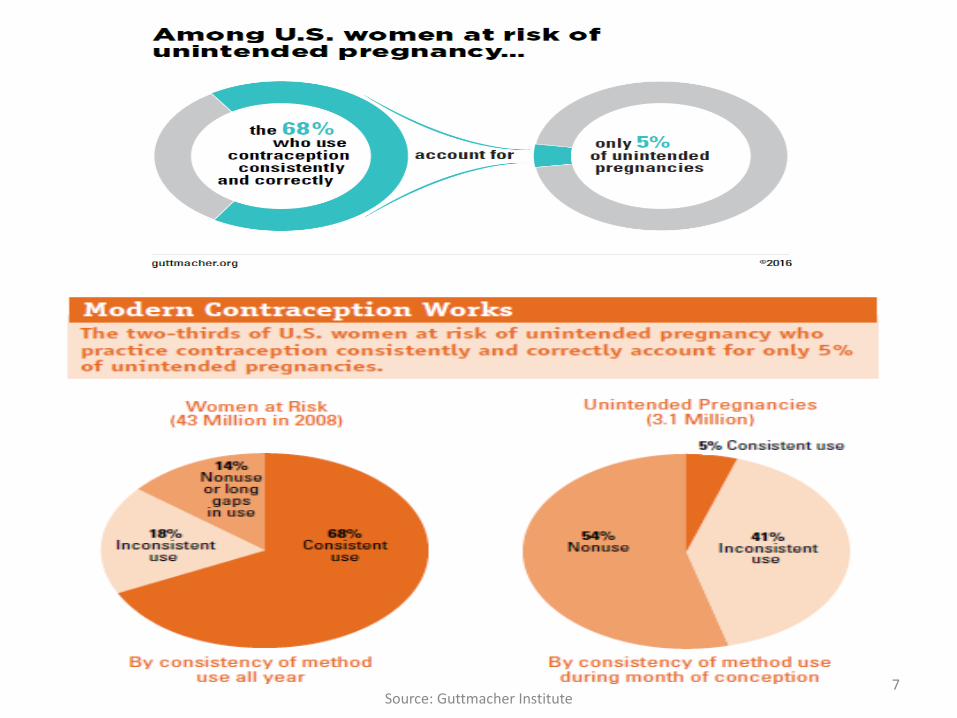
7Source:Guttmacher Institute
Page 8
HealthyPeople2020FamilyPlanningFP-1-16
• IncreasethenumberofintendedpregnanciesFP-1– 51%56%
• Increasethepercentageofwomenaged15to44yearsthatadoptorcontinueuseofthemosteffectiveormoderatelyeffectivemethodsofcontraceptionFP-16
– 63.1%69.3%
healthypeople.gov/2020/topics-objectives/topic/family-planning/objectives 8
Page 9
PharmacistsasPrescribers
• Severalstateswithlegislationpending–Missouri
HowdoIstayuptodatewithmy
knowledgeonthistopic?
Whataretheprocessesand
procedurerequiredforimplementingtheseservices?
DoIknowenoughabout
contraceptivestosafelyprescribe?
9
Page 10
Self-Assessment
• Understandingofthemenstrualcycle
• Knowledgeofavailablecontraceptiveproducts
• Comfortwithabilitytosafelyandeffectivelyprescribeoralcontraceptives
1 2 3 4 5
1 2 3 4 5
1 2 3 4 5
1=Least5=Most10
Page 11
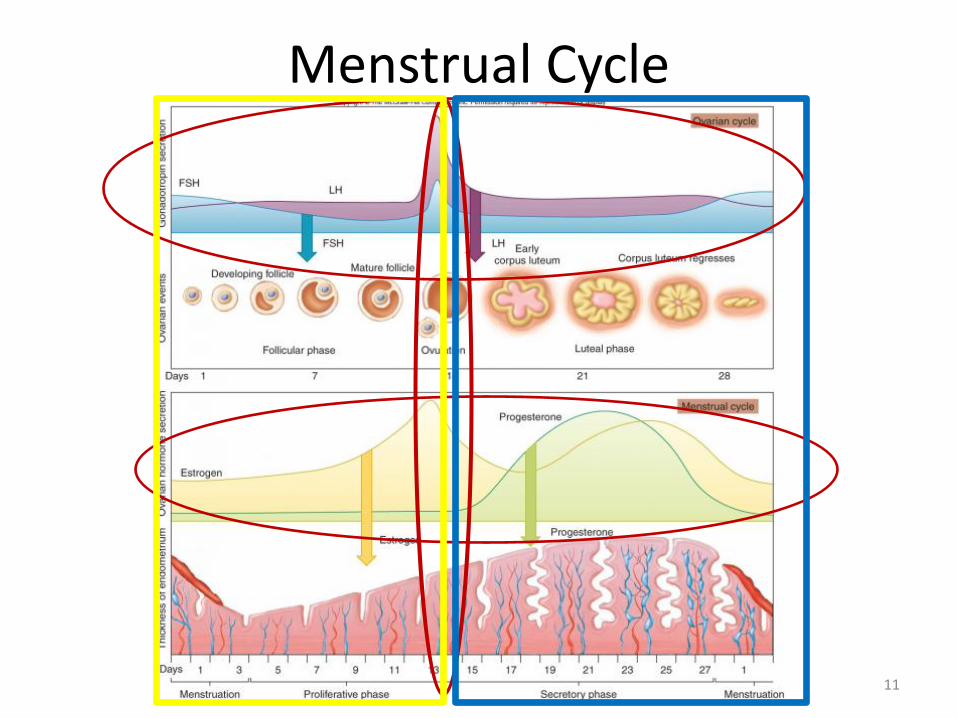
MenstrualCycle
11
Page 12
ClassificationsofContraception• Intercourse-relatedmethods
– Physicalbarriers:condoms,diaphragm,cervicalcap,periodicabstinence• Hormonalmethods
– Combinedcontraceptives(estrogen+progestin)• Oral• Patch• Ring
– Progestinonly• Oral• Injection• Intrauterinedevice
• Non-hormonal• Copperintrauterinedevice
• Permanentmethods– Femaletuballigation– Malevasectomy
12
Page 13
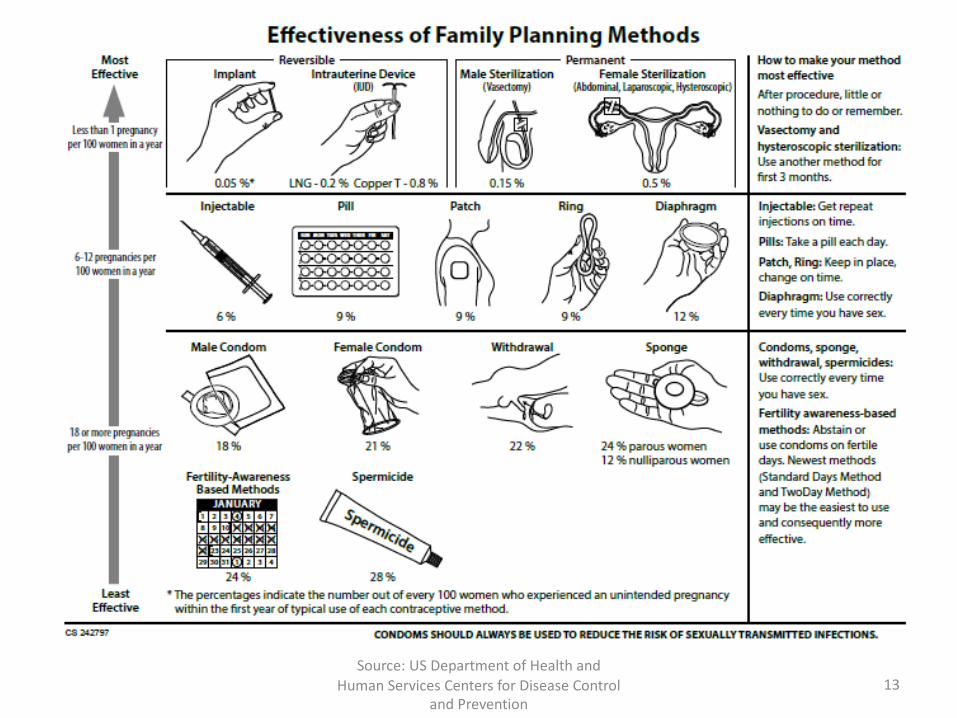
13Source:USDepartmentofHealthand
HumanServicesCentersforDiseaseControlandPrevention
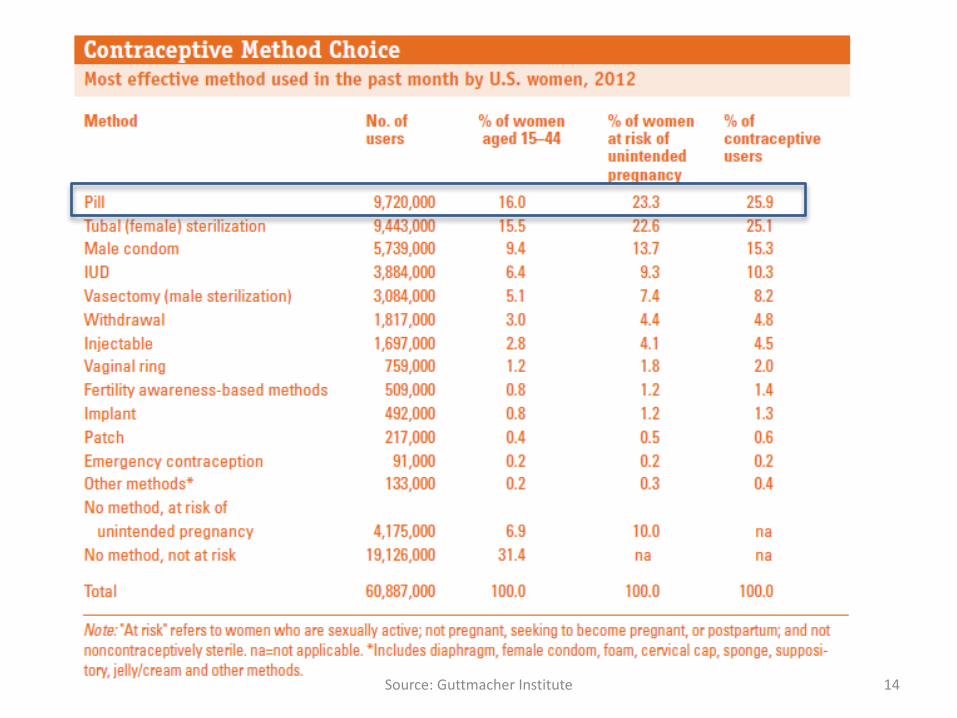
Page 14
14Source:GuttmacherInstitute
Page 15
COMBINEDHORMONALCONTRACEPTIVES(CHC)Oral
Describethemechanismofaction,formulations,doses,andusesof hormonalcontraceptives
15
Page 16
MechanismofAction
• PreventthedevelopmentofthedominantfolliclebysuppressingFSHsecretion
• PreventovulationbysuppressingLHsecretion
• Thickencervicalmucus• Causealterationsintheendometriallining
16
Page 17
EstrogenComponent
• Ethinyl estradiol(EE)–Mostcommonform
• Mestranol– BiologicallyinactiveprodrugofEE– Bioequivalentto35µgofethinylestradiol
• Estradiolvalerate– Convertedtothenaturallyoccurringestrogen,estradiol
17
Page 18
ProgestinComponent
Generation NameFirst(Estrane Family) Norethindrone
Norethindrone acetateEthynodiol diacetate
Second(Gonane Family) LevonorgestrelNorgestrel
Third(Gonane Family) DesogestrelNorgestimate
Fourth (Other) DrospirenoneDienogest
18
Page 19
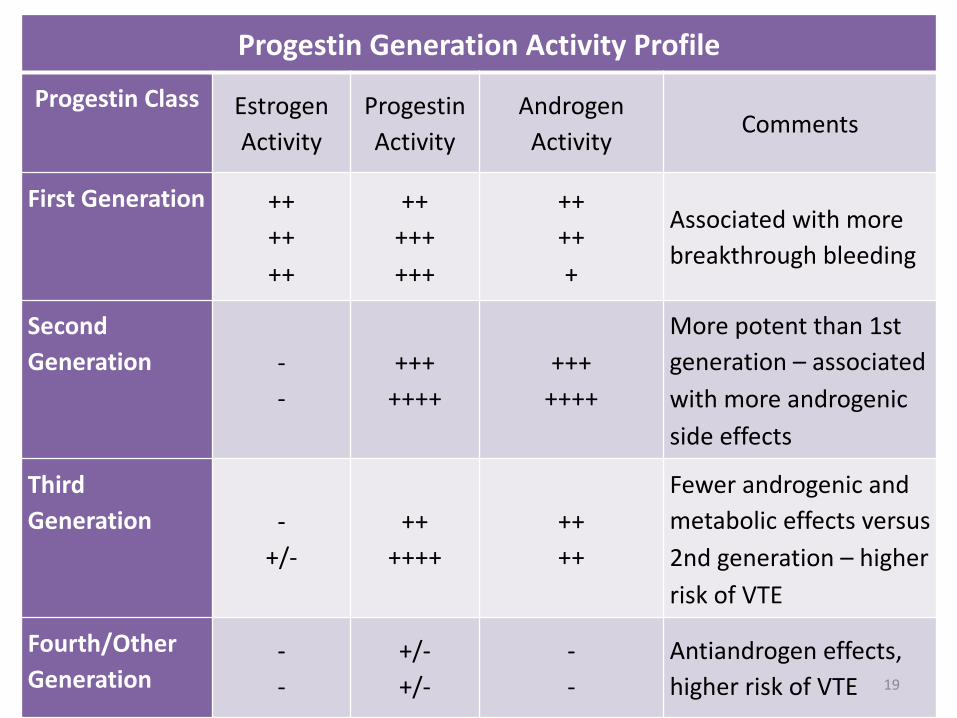
Progestin GenerationActivityProfile
ProgestinClass EstrogenActivity
ProgestinActivity
AndrogenActivity
Comments
FirstGeneration ++++++
++++++++
+++++
Associatedwithmorebreakthroughbleeding
SecondGeneration -
-+++++++
+++++++
Morepotentthan1stgeneration– associatedwithmoreandrogenicsideeffects
ThirdGeneration -
+/-++
++++++++
Fewerandrogenicandmetaboliceffectsversus2ndgeneration– higherriskofVTE
Fourth/OtherGeneration
--
+/-+/-
--
Antiandrogeneffects,higher riskofVTE 19
Page 20
Formulations• Monophasic– ratioofestrogen:progestin isfixedthroughoutthecycle
• Multiphasic– Biphasic– Triphasic– Four-phasic
• Extendedcycle– Delaysmenstruation
• Continuouscycle– Eliminatesmenstruation
20
Page 21
DosingofCHCs
• Estrogen– 20mcgisagoodstartingdose– 30mcgiftakingCYP450inducers
• Progestins withlowandrogenicactivity*<1mgnorethindrone (1st generation)≤0.1mgoflevonorgestrel (2nd generation)≤0.25mgofnorgestimate (3rd generation)
21*generalruleofthumb
Page 22
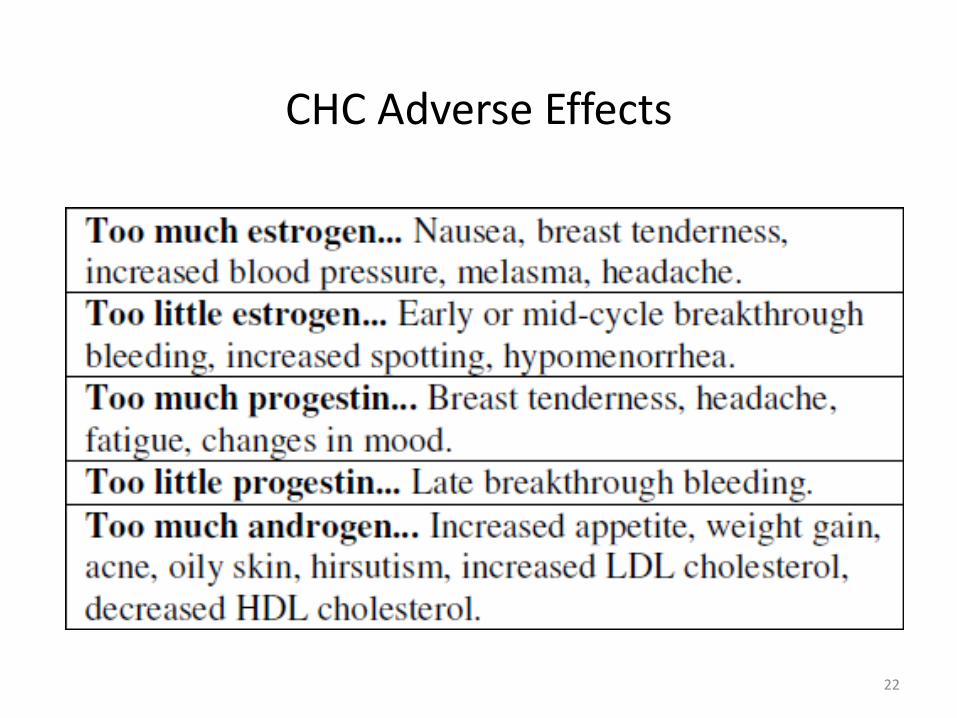
CHCAdverseEffects
22
Page 23
PROGESTIN-ONLYCONTRACEPTIVESOral
23
Page 24
ProgestinONLY
• Advantages– Maybeusedinlactatingwomen– Maybeusedinwomenwithestrogencontraindications
• Disadvantages– Increasedamenorrheaorfrequentspotting– Mustbetakenatsametimeeveryday
• PatientEducation– Misseddose(see“MissedDoses”slides)– Irregularmenses
24
Page 25
Howdothedifferentestrogencomponentsavailableincombinedhormonal
contraceptivescompare?
A. Estradiolvalerate isthemostcommonformoccurringincommerciallyavailableoralcontraceptives
B. Estradiolvalerate isthemosteffectiveformC. Ethinyl estrodial isconvertedtoanaturally
occurringestrogenD. Mestranolisthebiologicallyinactive
prodrugofethinyl estradiol
25
Page 26
Whichofthefollowingistruewhencomparingmonophasichormonalcontraceptivestomultiphasichormonalcontraceptives?
A. MonophasicarehardertouseB. Monophasicareafixedratioofestrogento
progestinthroughoutthecycleC. Multiphasichavemorestudiestosupport
theiruseD. Multiphasicareassociatedwithlessside
effects
26
Page 27
COMBINEDHORMONALCONTRACEPTIVES(CHC)Oral
Objective2Comparethebenefitsvs.risksoforalcontraceptives.
27
Page 28
Choosingthe“Right”Contraceptive
• Mustconsiderthepatient’s:– Medicalhistory
• Doesthepatienthaveacontraindicationtoestrogen?– Medicationuse
• Whatothermedicationsdoesthepatienttake?• Arethereanysignificantdruginteractionsmayimpactthecontraceptiveofchoice?
– Preferences• Doesthepatient“know”whattheyprefertouse?Why?• Isthepatientpreference:safe,realistic,affordable,etc
– Adherence• Canthepatientmaintaintheregimen?
28
Page 29
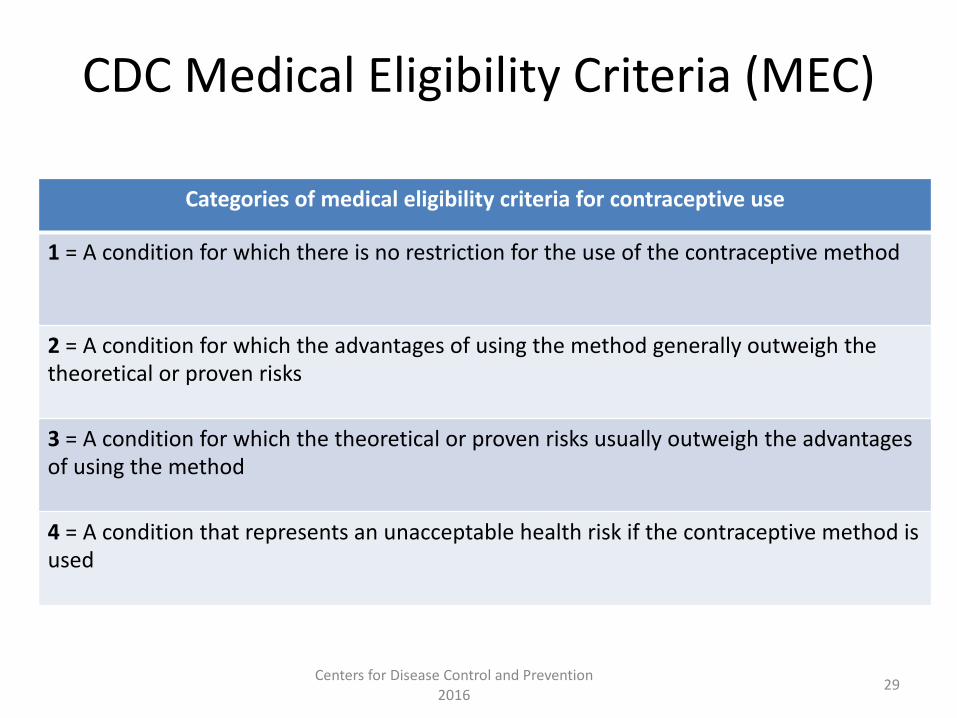
CDCMedicalEligibilityCriteria(MEC)
Categoriesof medicaleligibilitycriteriaforcontraceptiveuse
1 =Aconditionforwhichthereisnorestrictionfortheuseofthecontraceptivemethod
2=Acondition forwhichtheadvantagesofusingthemethodgenerallyoutweighthetheoreticalorprovenrisks
3 =Aconditionforwhichthetheoreticalorprovenrisksusuallyoutweightheadvantagesofusingthemethod
4 =Aconditionthatrepresentsanunacceptablehealthriskifthecontraceptivemethodisused
29CentersforDiseaseControlandPrevention2016
Page 30
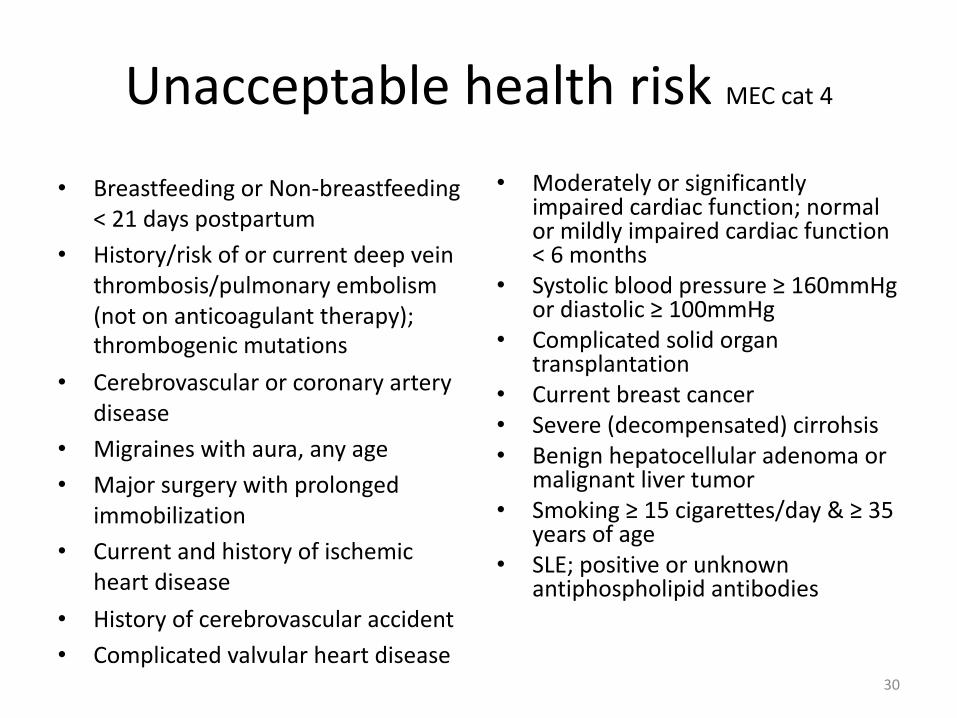
UnacceptablehealthriskMECcat4
• BreastfeedingorNon-breastfeeding<21dayspostpartum
• History/riskoforcurrentdeepveinthrombosis/pulmonaryembolism(notonanticoagulanttherapy);thrombogenic mutations
• Cerebrovascular orcoronaryarterydisease
• Migraineswithaura,anyage• Majorsurgerywithprolonged
immobilization• Currentandhistoryofischemic
heartdisease• Historyofcerebrovascularaccident• Complicatedvalvular heartdisease
• Moderatelyorsignificantlyimpairedcardiacfunction;normalormildlyimpairedcardiacfunction<6months
• Systolicbloodpressure≥160mmHgordiastolic≥100mmHg
• Complicatedsolidorgantransplantation
• Currentbreastcancer• Severe(decompensated)cirrohsis• Benignhepatocellularadenomaor
malignantlivertumor• Smoking≥15cigarettes/day&≥ 35
yearsofage• SLE;positiveorunknown
antiphospholipidantibodies
30
Page 31
ExamplefromCDCMEC
31
Page 32
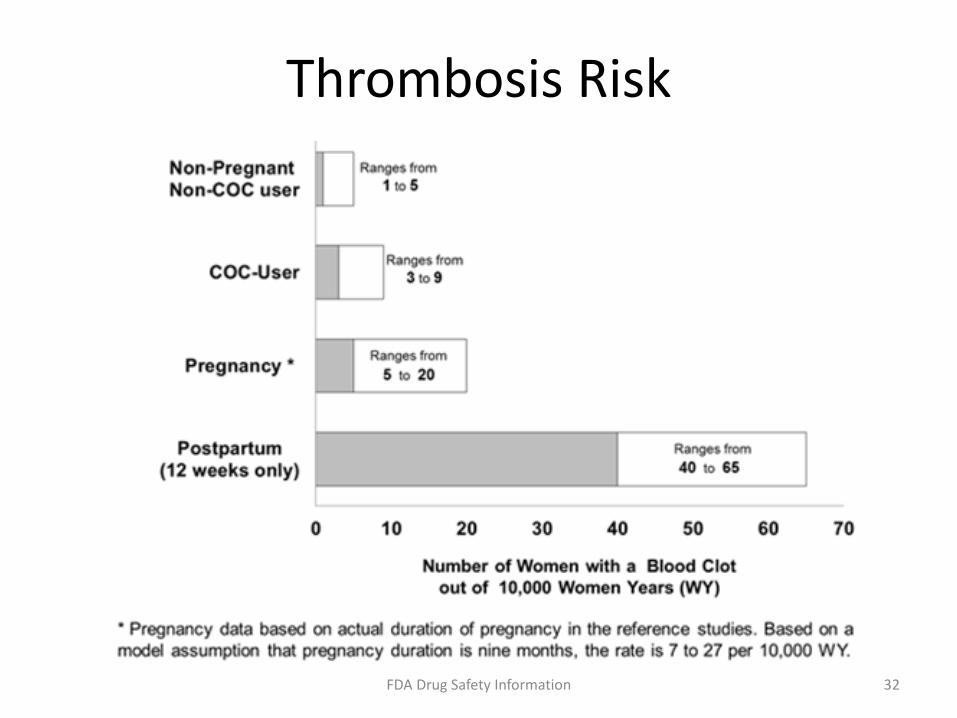
ThrombosisRisk
32FDADrugSafetyInformation
Page 33
VTERiskandContraceptive
Patch3rd &4th generationCHCsVaginalring
Progestin-only(IUD,oral,implant)
FirstgenerationCHCsSecondgenerationCHCs
33
GreaterRisk
LowerRisk
Page 34
DrugInteractions
• Interferenceofabsorption• Liverenzymeinduction– anti-epilepticdrugs(AEDs)
• Usealternativecontraception• Reportedantibioticcases:– Tetracycline– Minocycline– Erthromycin– Penicillins– Cephalosporins
34
Page 35
DrugInteractionsDrugsinterferingwithOCEfficacy OCinterferingwithEfficacy ofOtherDrugs
↑ ↓ ↑ ↓
AscorbicacidAPAP-scheduledAtorvastatinRosuvastatin
NNRTIsPIs
AnticonvulsantsAntibioticsRifampin
TheophyllineSt. John’sWort
NNRTI-nevirapinePIs
SulfonamidesGriseofulvinBosentanTacrolimusModafinil
AlprazolamChlordiazepoxide
DiazepamTheophyllineCaffeine
CyclosporineCorticosteroids
AlcoholB-Blockers
TCAsRopiniroleZolmitriptan
TemazepamWarfarin
Thyroid agentsHypoglycemicsMethyldopaMetforminAmprenavir
35
Page 36
AdditionalBenefitsofCHCs
• Regulatemenstrualcycle• Decreaseriskofanemia• Decreaseincidenceofovariancysts• Decreaseriskofovariananduterinecancers• Decreaseacne• Decreasepelvicinflammatoryrisk
36
Page 37
PatientEducationforOralCHCUse
• Compliance• Misseddoses(see“MissedDosesslides)• NoprotectionagainstSTIs/HIV– Condomuse
• Signs/symptomsofVTE– ACHES• Abdominalpain,chestpain,headache,eyeproblems,severelegpain
• Druginteractions37
Page 38
COMBINEDHORMONALCONTRACEPTIVES(CHC)Oral
Objective3 Developappropriatecounselingpoints toshare
withpatientsregardingoral contraceptives.38
Page 39
InitiatingOralContraceptives
• QuickStart– Contraceptivemethodstartedimmediately– Backupmethodx7days
• Day1Start– Contraceptivemethodstartedonthefirstdayofmenses
• SundayStart– FirstSundayafternextmensesbegins– Backupmethodx7days
39
Page 40
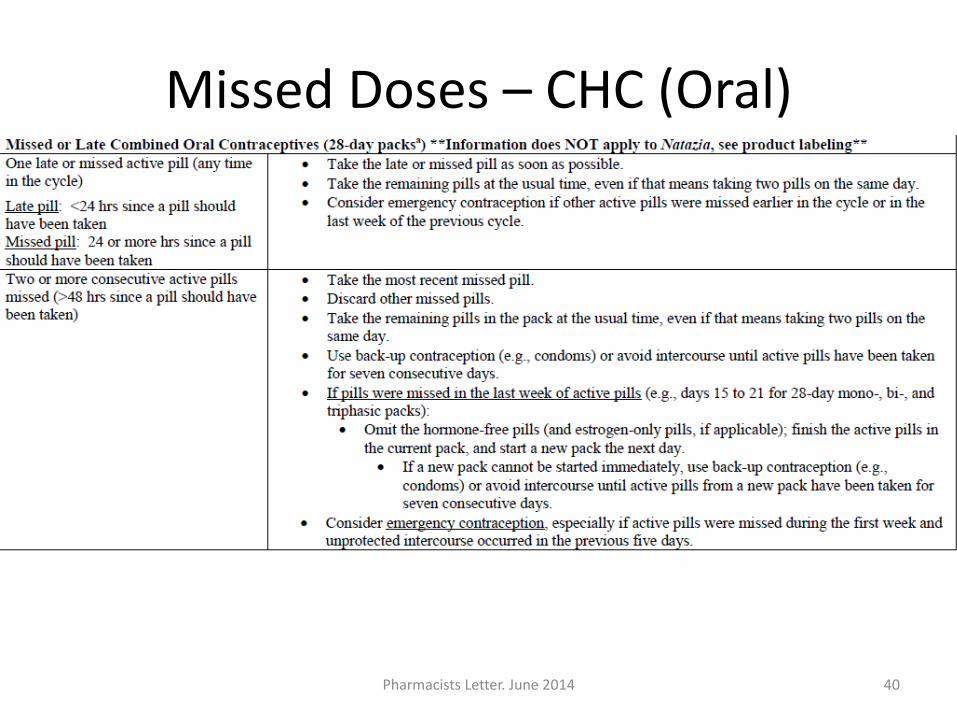
MissedDoses– CHC(Oral)
40PharmacistsLetter.June2014
Page 41
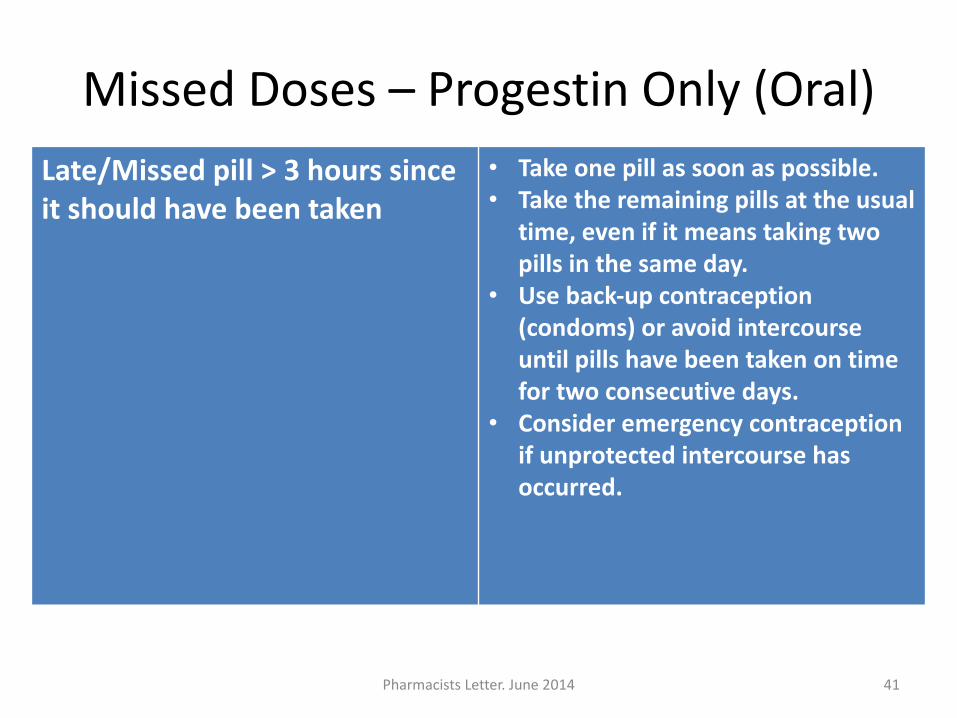
MissedDoses– ProgestinOnly(Oral)Late/Missedpill>3hourssinceitshouldhave beentaken
• Takeonepillassoonaspossible.• Takethe remainingpillsattheusual
time,evenifitmeanstakingtwopillsinthesameday.
• Useback-upcontraception(condoms)oravoidintercourseuntilpillshavebeentakenontimefortwoconsecutivedays.
• Consideremergencycontraceptionifunprotectedintercoursehasoccurred.
41PharmacistsLetter.June2014
Page 42
Monitoring
• 3-6monthsafterinitiation• Followupwithaprimarycareprovider• Wellwomanexam• Papanicolaou andpelvicexam• Breastexams– selfandclinical• Appropriatelabwork
42
Page 43
AccordingtotheCDCMECdocument,aconditionthatrepresentsanunacceptable
healthriskifthecontraceptivemethodisused,wouldbenotedwithanumber4.
A. TrueB. False
43
Page 44
LYisa22y.o.femalewhorecentlystartedanoralCHCcontaining30mcgofEEand0.15mglevonorgestrel.Sheisonherthirdpackof
pillsandstatesshefeelsreallytired,iscrankyallthetime,andshehasgained3lbs.Shewantstokeeptakingapill,butisgoingtostopthisoneduetotheproblemssheishaving.Whatcourseofactionwould
yourecommend?
A. Stayonthesamepill.Theseadverseeffectswillgoaway.
B. SwitchtoaCHCwith3mgofdrospirenone.C. SwitchtoaCHCwith20mcgofEE.D. SwitchtoaCHCwith0.35mgofnorgestimate.
Page 45
COMBINEDHORMONALCONTRACEPTIVES(CHC)Oral
Objective4 Identifyusefulresourcesavailablefor
hormonalcontraceptives. 45
Page 46
UsefulResources• CDCMedicalEligibilityCriteriaforContraceptiveUse
• http://www.cdc.gov/mmwr/volumes/65/rr/pdfs/rr6503.pdf• WorldHealthOrganization– http://www.who.int/topics/family_planning/en/– MedicalEligibilityCriteriaforContraceptiveUse
• http://www.who.int/reproductivehealth/publications/family_planning/9789241563888/en
• PharmacistsLetter• PlannedParenthood– http://www.plannedparenthood.com
• AssociationofReproductiveHealthProfessionals(ARHP)– http://www.arhp.org
• http://www.womenshealth.gov46
Page 47
References1. DiPiro,JT.Pharmacotherapy,APathophysiologic Approach.McGrawHill.2014.2. Guitierrez,K.(2008)inPrimaryPharmacotherapeutics:Clinical ReasoningCare(2nd ed)Saunders.St.Louis,MO.
Chapter58:HormonalContraceptivesandRelatedDrugs.3. AssociationofReproductiveHealthProfessionals.Web.4Feb2013.http://www.arhp.org4. Women’sHealth.Web.4Feb2013.http://www.womenshealth.gov5. Lexi-CompOnline.http://www.lexi.com6. ManagingContraceptivePillPatientsbyRichardP.Dickey13th edition7. WorldHealthOrganization.Web.4Feb2013.http://www.who.int/topics/contraception/en/8. CentersforDiseaseControlandPrevention.MedicalEligibilityCriteriaforContraceptiveUse.
http://www.cdc.gov/mmwr/volumes/65/rr/pdfs/rr6503.pdf9. Koda-Kimble,M,etal.AppliedTherapeutics:TheClinicalUseofDrugs.EighthEdition.LippincottWilliams&Wilkins.
2005.Chapter45:Contraception.10. PlannedParenthood.Web.4Feb2013.http://www.plannedparenthood.org/health-topics/morning-after-
pill/emergency-contraception-pill-chart-19304.htm11. UnintendedPregnancyintheUnitedStates.Guttmacher Institute.March201612. ContraceptiveUseintheUnitedStates.Guttmacher Institute.October2015.13. TheNationalCampaigntoPreventTeenandUnplannedPregnancy.Briefly:UnplannedPregnancyAmong20-
Somethings:TheFullStory.May2008.Availableathttp://www.thenationalcampaign.org/resources/pdf/briefly-unplanned-pregnancy-among-20somethings-the-full-story.pdf.AccessedMarch10,2011.
14. Lesnewski,Retal.“PreventingGapsWhenSwitchingContraceptives.”AmericanFamilyPhysician83(2011):567-570.http:www.reproductiveaccess.org
15. MissedDosesofHormonalContraception.PharmacistLetter.June2014.16. HormonalContraception.PharmacistLetter.March2013.17. FamilyPlanning.HealthyPeople2020.OfficeofDiseasePreventionandHealthPromotion.Web.14July2016.
https://www.healthypeople.gov/2020/topics-objectives/topic/family-planning/objectives
47