31
March 2, 2015 Hospital & Physician Relations Executive Summit: Transformation Strategies Delivering Value Through a Strategic Alliance
March 2, 2015
Hospital & Physician Relations Executive Summit: Transformation Strategies
Delivering Value Through a Strategic Alliance

Agenda
I. IntroductionII. Learning ObjectivesIII. Setting the StageIV. Regional Provider Network (RPN)V. Strategic Alliances
10555.003\325111(pptx)-E2

I. IntroductionMeet the Presenters
20555.003\325111(pptx)-E2
Michael Hein, M.D.• Dr. Hein is Chief Executive Officer of the Nebraska-based RPN.• He is a 20-year healthcare veteran with leadership experience in large
integrated healthcare systems, rural primary care practices, inpatient and ambulatory care settings, as well as academic medicine and clinical research.
• As CEO, Dr. Hein provides leadership to the RPN to ensure that the overall vision and objectives of the RPN are achieved.
Darin Libby• Darin is a Principal in ECG’s Healthcare practice.• His practice focuses on strategic planning, hospital/physician ventures, medical
staff development, operational restructuring, and hospital and medical group financial management.
• Darin’s role with RPN began in 2013 with network formation and planning support and continues today with strategic advising, implementation assistance, and project management support.
II. Learning Objectives
30555.003\325111(pptx)-E2
The objective of today’s presentation is to explore how forming a strategic alliance with other provider organizations offers hospitals and physicians
the opportunity to accelerate population health performance.
Learning Objectives• How independent hospitals can remain independent yet gain the scale and
expertise necessary to deliver care in a value-oriented environment• How a strategic alliance that is focused on improving health across the state and
surrounding region formed in Nebraska• How statewide collaboration across providers allows for pooled risk and clinical
integration
III. Setting the StageThe Triple Aim Framework
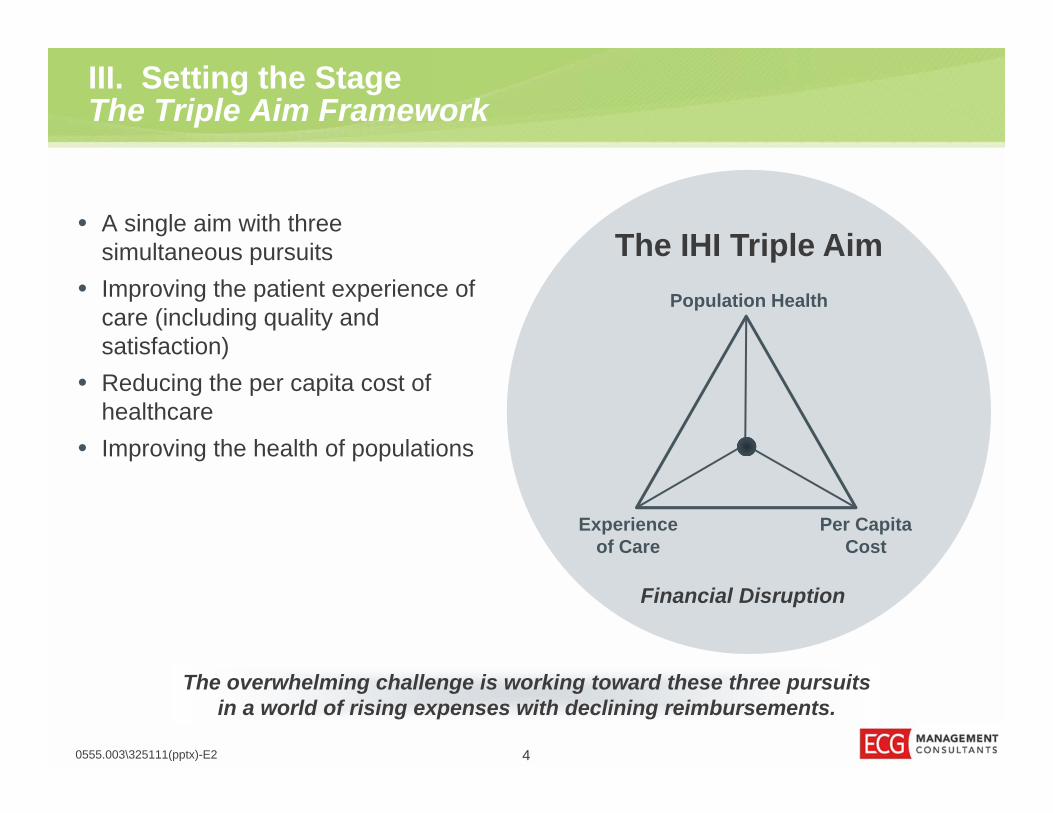
• A single aim with three simultaneous pursuits
• Improving the patient experience of care (including quality and satisfaction)
• Reducing the per capita cost of healthcare
• Improving the health of populations
4
The overwhelming challenge is working toward these three pursuits in a world of rising expenses with declining reimbursements.
0555.003\325111(pptx)-E2
The IHI Triple AimPopulation Health
Experience of Care
Per Capita Cost
Financial Disruption
III. Setting the StageDilemma of a Hospital Board
0555.003\325111(pptx)-E2 5
Is going it
ALONEstill an option
for your hospital?
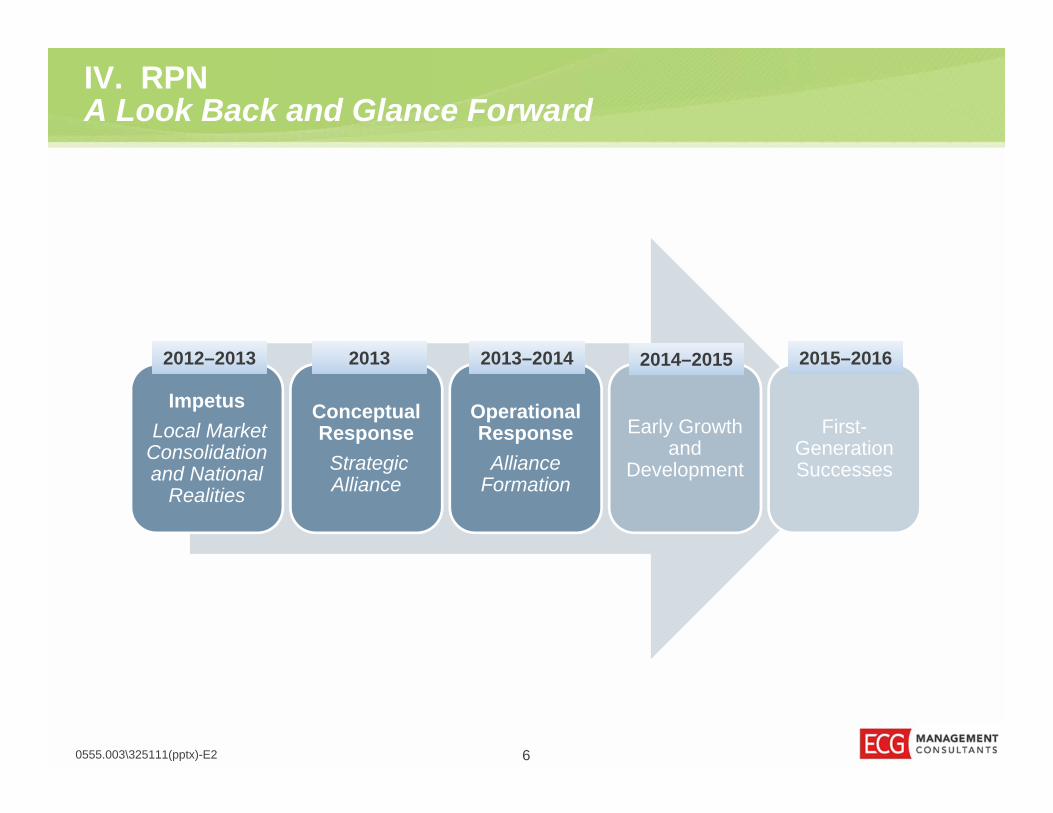
IV. RPNA Look Back and Glance Forward
Impetus Local Market
Consolidation and National
Realities
Conceptual Response
Strategic Alliance
Operational Response
Alliance Formation
Early Growth and
Development
First-Generation Successes
2012–20132012–2013 20132013 2013–20142013–2014 2014–20152014–2015 2015–20162015–2016
0555.003\325111(pptx)-E2 6

7
IV. RPNIdentifying the Common Mission
0555.003\325111(pptx)-E2
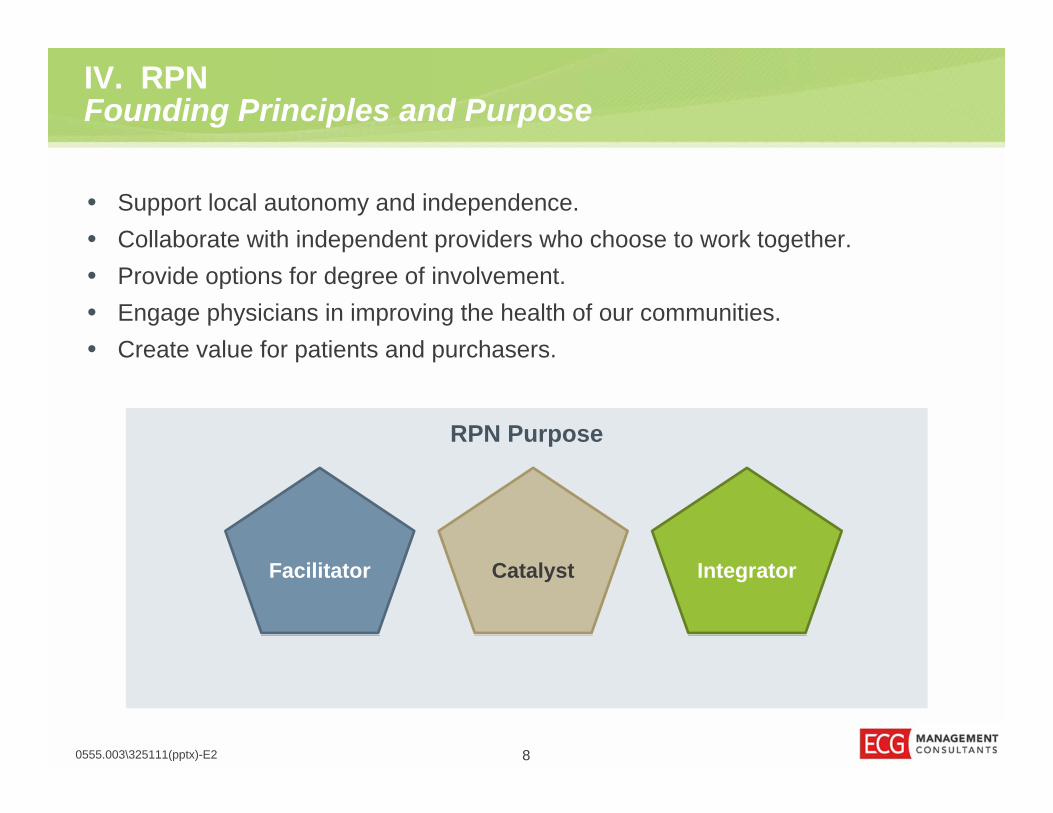
IV. RPNFounding Principles and Purpose
• Support local autonomy and independence.• Collaborate with independent providers who choose to work together.• Provide options for degree of involvement.• Engage physicians in improving the health of our communities.• Create value for patients and purchasers.
CatalystFacilitator Integrator
RPN Purpose
0555.003\325111(pptx)-E2 8

Population Health
PopulationMedicine
Care Coordination, etc.
Clinical Integration
90555.003\325111(pptx)-E2
The specific activities of the medical care system that, by themselves or in collaboration with partners, promote population health beyond the goals of care of the individuals treated.
The specific activities of the medical care system that, by themselves or in collaboration with partners, promote population health beyond the goals of care of the individuals treated.
The health outcomes of a group of individuals, including the distribution of such outcomes within the group
(80% nonmedical care).
The health outcomes of a group of individuals, including the distribution of such outcomes within the group
(80% nonmedical care).
IV. RPNThe Journey to Population Health
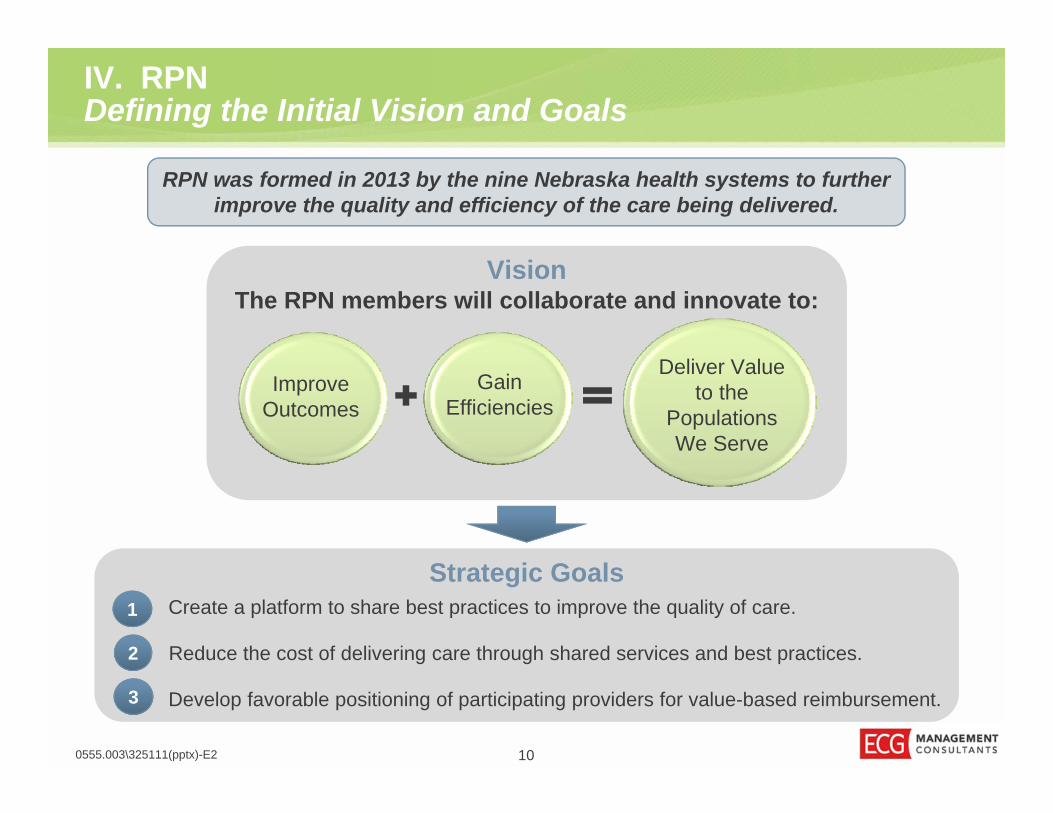
IV. RPNDefining the Initial Vision and Goals
100555.003\325111(pptx)-E2
RPN was formed in 2013 by the nine Nebraska health systems to further improve the quality and efficiency of the care being delivered.
The RPN members will collaborate and innovate to:
Improve Outcomes
Gain Efficiencies
Deliver Value to the
Populations We Serve
Vision
1
2
3
Strategic GoalsCreate a platform to share best practices to improve the quality of care.
Reduce the cost of delivering care through shared services and best practices.
Develop favorable positioning of participating providers for value-based reimbursement.
110555.003\325111(pptx)-E2
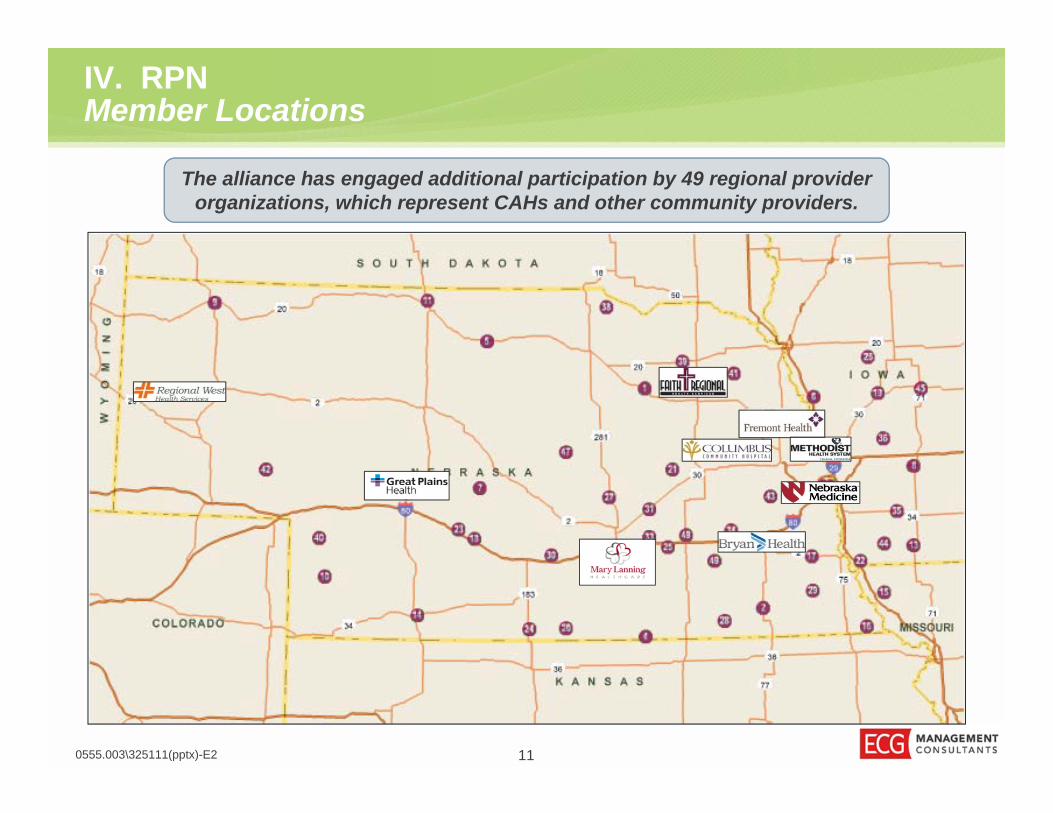
IV. RPNMember Locations
The alliance has engaged additional participation by 49 regional provider organizations, which represent CAHs and other community providers.

IV. RPNGovernance: Board of Managers Composition
The 20 representatives will be selected as follows:• Each founding member will appoint two managers. • The Regional Membership Committee will appoint two managers. • A minimum of 50% of the board will be composed of providers.
120555.003\325111(pptx)-E2
Board of Managers
Bryan Health
Great Plains Health
Columbus Community
Hospital
Faith Regional
Health Services
Fremont Health
Mary Lanning
Healthcare
Nebraska Methodist
Health System
Nebraska Medicine
Regional West
Medical Center
Regional Member
Committee
Members (i.e., Owners)
The RPN Board consists of 20 managers, with a physician and executive manager appointed by each member.

IV. RPNCommittee Structure
0555.003\325111(pptx)-E2
Board of Managers
Payor Contracting
Clinical Leadership and Quality
Data and IT NetworkMembership
Shared Services
• Contract execution
• Financial performance
• Funds flow development
Identification of opportunities for shared services
• Protocol development/enhancement
• UM/QA
• Selection of medical managementopportunities
• Information management and reporting
• Business intelligence
• Infrastructure
• Network development/provider relations
• Credentialing
• Strategic and clinical planning• Communications• Workforce planning• Alignment policy development• Contracting strategy/oversight• Budget development and management
Regional MembersRegional Members
• Identification of regional issues
• Nomination of regional representatives for committees
Several committees have been established to provide recommendations to the Board of Managers regarding priority initiatives of the RPN.
RPN Planning Committee
RPN Planning Committee
13
IV. RPNPursuit #1 — Clinical Integration
140555.003\325111(pptx)-E2
RPN is pursuing clinical integration as the strategy to achieving its vision.
• RPN will need to achieve standards of clinical integration to participate in joint contracting, including:
– Interdependence. – Participation of primary care providers and
specialists, with a requirement for in-network referrals.
– Investments in standards and clinical protocols.
– Integrated IT infrastructure.– Penalties for noncompliance with standards
and protocols. • RPN is building its population health
management capabilities for members’ self-insured employee health plans, which will then be expanded to other populations in the future.

IV. RPNPursuit #1 — Clinical Integration (continued)
Create PHOsJoin With Affiliate
Members
Focus on EHP
Population
Demonstrate Population
Health Capability
Contract to Move
Beyond EHP
Create Health in Our Communities
0555.003\325111(pptx)-E2 15

IV. RPNPursuit #2 — Payor Contracting
160555.003\325111(pptx)-E2
RPN is developing payor relationships and payment structures that align incentives to reduce cost and promote higher-quality care.
• RPN will align with health plans to develop risk-based contracting arrangements.
• Opportunities include:– Commercial shared-risk and pay-for-performance
programs.– Medicare and Medicaid programs.– Direct contracts with self-insured employer health
plans.• RPN will provide the support and infrastructure required
to succeed under these arrangements, including:– Medical management.– Integrated information technology.– Payor contracting negotiation and execution.– Funds flow and incentive designs.– Risk management.
+

IV. RPNPursuit #3 — Shared Services
170555.003\325111(pptx)-E2
RPN is seeking to reduce the cost of delivering care through shared services.
Rationale for Shared Services• Enhance communication channels to share and
implement best practices irrespective of joint contracting.
• Negotiate using the combined size for greater purchasing power with vendors outside of GPOs.
• Effectively deploy capital dollars with a combined approach to strategic planning.
Areas of Opportunity• Vendor contracts and pricing• Provider credentialing• Best practices and education• Medical delivery support• Centralized corporate functions

IV. RPNPursuit #3 — Shared Services (continued)
Create Legal and
Operational Framework
Assess Existing
Opportunities
Find and “Pluck” the
“Low-Hanging
Fruit”
Mature Analysis
Capabilities and Trust
Tackle Higher-
Return, More Complex
Opportunities
Reduce the Overall Cost
of Care
0555.003\325111(pptx)-E2 18
IV. RPNPursuit #4 — Health Information Technology
190555.003\325111(pptx)-E2
RPN aims to develop the optimal IT infrastructure for managing population health.
• Health Information Exchange Capabilities—Data linkages necessary to exchange clinical data at the point of care.
• Analytics and Reporting —– Tracking provider performance,
identifying clinical variation, and reporting.– Implementing a population management
and risk assessment tool across the network to identify opportunities for care improvement and cost savings.
• Effective IT Utilization — Support efforts to improve the use and functionality of members’ existing technologies. Examples include assisting with achieving EHR meaningful use requirements and sharing best practices.

IV. RPNAspirational Goals
• Create health in the communities we serve.• Build unity of purpose, function, and results over time.• Be one of a kind in structure, culture, processes, and results.
0555.003\325111(pptx)-E2 20
Create Health Be One of a KindBuild Unity

IV. RPNMembership Groups
• Founding Members• Affiliate Members (Phase 2)• Associate Members (Phase 1)• Contractors
0555.003\325111(pptx)-E2 21

IV. RPNEarly Wins
• First shared services contract realizing member cost reductions:– Blood products — approximately $0.5 million over 3 years– Others soon to follow
• Crimson Tool from The Advisory Board Group– Founding members Employee Health Plan (EHP) – Clinicians able to analyze population management opportunities– Provides “First-Look” opportunity for clinical improvement in EHP population
0555.003\325111(pptx)-E2 22

IV. RPNNext 12 Months
• Maturing the vision, mission, and purpose, and creating a corporate identity• Sharpening the strategic focus• Expanding management capabilities• Completing early-win shared services opportunities• Increasing consistency in EHP offerings and structures• Defining our network• Improving the analytical and performance improvement capacity• Developing the early framework for a learning community• Beginning clinical improvement efforts within each PHO• Building purposeful relationships with payors and employers
0555.003\325111(pptx)-E2 23
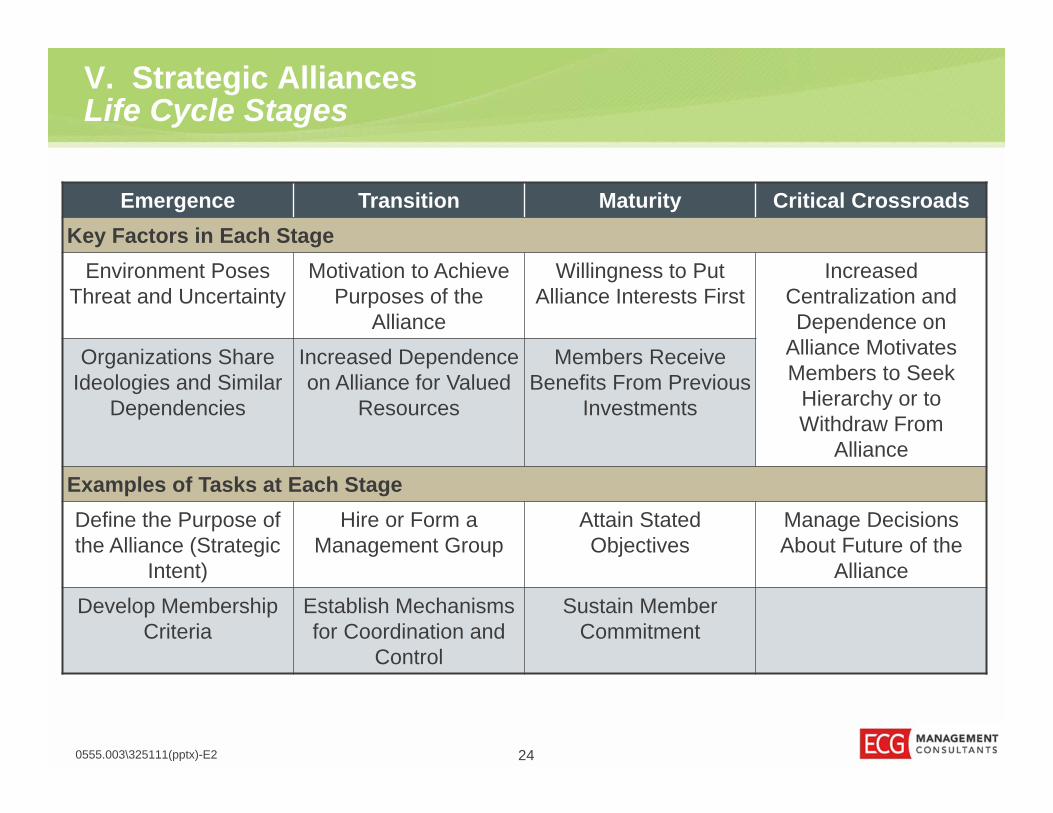
Emergence Transition Maturity Critical CrossroadsKey Factors in Each Stage
Environment Poses Threat and Uncertainty
Motivation to AchievePurposes of the
Alliance
Willingness to Put Alliance Interests First
Increased Centralization and Dependence on
Alliance Motivates Members to Seek
Hierarchy or to Withdraw From
Alliance
Organizations Share Ideologies and Similar
Dependencies
Increased Dependence on Alliance for Valued
Resources
Members ReceiveBenefits From Previous
Investments
Examples of Tasks at Each StageDefine the Purpose of the Alliance (Strategic
Intent)
Hire or Form a Management Group
Attain Stated Objectives
Manage Decisions About Future of the
AllianceDevelop Membership
CriteriaEstablish Mechanisms for Coordination and
Control
Sustain Member Commitment
V. Strategic AlliancesLife Cycle Stages
0555.003\325111(pptx)-E2 24
“The granddaddy of all mistakes is competing to be the best,
going down the same path as everybody else and thinking that somehow you can achieve better
results.”– Michael Porter
25
V. Strategic AlliancesCreate New Opportunities
0555.003\325111(pptx)-E2
V. Strategic Alliances Rule #1 — Be Nimble
260555.003\325111(pptx)-E2

V. Strategic Alliances Rule #2 — Anticipate the Future
0555.003\325111(pptx)-E2 27

V. Strategic AlliancesRule #3 — Have World-Class BCI
0555.003\325111(pptx)-E2 28

Questions
0555.003\325111(pptx)-E2 29
QuestionsAnswersQ. A.

Reference Articles
• Sarah Klein and Douglas McCarthy, “All Health Care is Local: The Power of Community to Drive Improvement,” The Commonwealth Fund, September 11, 2014. Available here.
• Michael E. Porter and Thomas H. Lee, “The Strategy that Will Fix Healthcare,” Harvard Business Review, October 2013. Reprint R131OB. Available here.
• Edward J. Zodiac et al., “Managing Strategic Alliances,” in Lawton Burns et al. (eds.), Shortell & Kaluzny's Health Care Management: Organization Design & Behavior (sixth edition), Delmar Cengage Learning, New York, 2011, pp. 321–346. Available here.
• Jonathan Hughes and Jeff Weiss, “Simple Rules for Making Alliances Work,” Harvard Business Review, November 2007. Available here.
• Brook Manville, “For big goals, a ‘thick we’ community trumps a network,” Financial Review,September 23, 2014. Available here. Harvard Business Review blog version here.
• Malcolm Gladwell, “How David Beats Goliath: When Underdogs Break the Rules,” The New Yorker, May 11, 2009. Available here.
• Kate Lovrien, “The Virtual Primary Healthcare Revolution: What Health Systems Need to Know,” Becker’s Hospital Review, February 3, 2014. Available here.
• The Advisory Board Company, Expert Perspectives, “The Extreme Pessimist’s Argument for Population Health,” Spring 2014, Vol. 2, pp. 6–9.
0555.003\325111(pptx)-E2 30

















