71
INFECTION CONTROL COMMITTEE Lung Center of the Philippines
| Date post: | 23-Dec-2015 |
| Category: |
Documents |
| Upload: | ramoli1988 |
| View: | 10 times |
| Download: | 1 times |

INFECTION CONTROL COMMITTEE
Lung Center of the Philippines

TheThe
Hospital GangHospital Gang
ESCHERICHIA COLIgenerally lives a blameless life in the gut
but assumes a life of crime once he is allowed to roam in the hospital
PSEUDOMONAS Normally lives in soil and in water
storage tank. but, once he gets into the hospital, is notoriously difficult to remove
KLEBSIELLA. Lesser known resident of the intestine,
fond of hitchhiking on the hands of doctors and nurses. Known to take over entire wards.
STREPTOCOCCUS Still a common cause of throat infection
but also involved in more seriousoffenses against the rest of the person
PROTEUSA motile young bacterium, anxious to swim into the wrong places. Generally follows up
the dirty work of other bacteria
STAPHYLOCOCCUS AUREUSAlias Goldie the Grape, found
in the nose and on the hands of hospital staff but survives
for days in dusty places

SusceptibleHost
Pathogen Reservoir
Method ofTransmission
Place ofEntry
Place ofExit
Chainof
Infection

Breakingthe
Chainof
Infection
SusceptibleHost
Pathogen Reservoir
Place ofEntry
Place ofExit
Method of Transmission

Routes of Transmission in Healthcare Settings
Droplet
Contact
Airborne

Droplet Transmisson
• droplets generated from the source person primarily during coughing, sneezing & talking• droplets propelled a short distance through the air & deposited on the host’s eyes, nasal mucosa, or mouth• droplets do not remain suspended in the air

Direct - contact Transmission
• direct body surface-to-body surface contact & physical transfer of microorganisms between a susceptible host & an infected or colonized person
• can also occur between 2 patients

Indirect-contact Transmission
• contact of a susceptible host with a contaminated intermediate object, usually inanimate
• contaminated instruments, needles, or dressings, or contaminated hands and gloves

Airborne Transmission
• dissemination of airborne droplet nuclei (5 um or less) • suspended in the air for long periods of time• dispersed widely by air currents• special air handling and ventilation required to prevent transmission

Routes of Transmission Droplet Diphtheria (pharyngeal) Mycoplasma pneumoniaPertussisPneumonic plagueInfluenzaAdenvirusMumpsRubellaParvovirus B19 Invasive N. meningitidis disease (pneumonia, meningitis, sepsis)Invasive H. influenzae type b disease (sepsis, meningitis, pneumonia)
Contact
Enteric infections ( C. difficile, Shigella, hepatitis A)RSV, parainfluenza or enteroviral infectionsDiphtheria ( skin )ImpetigoPediculosisScabiesStaph. furunculosisHerpes simplex virusHerpes zoster (disseminated or in immunocompromised)Viral hemoorharrhagic (Ebola, Lassa, Marburg)
Airborne
TB
Measles
Varicella

Basic Principles of Infection Control
• Separate the infection source from the rest of the hospital
• Cut off any route of transmission

Standard Precautions• Previously called Universal
Precautions• Assumes blood and body fluid of
ANY patient could be infectious• Recommends PPE and other
infection control practices to prevent transmission in any healthcare setting
• Decisions about PPE use determined by type of clinical interaction with patient
Standard Precautions
• Designed to reduce the risk of transmission of microorganisms from both recognized & unrecognized sources of infection in hospitals
• Apply to : blood
all body fluids, secretions, & excretions except sweat, regardless of whether or not they contain visible blood non-intact skin mucous membranes

Transmission-based Precautions
• Droplet Precautions • Contact Precautions
• Airborne Precautions

Droplet Precautions
• Patient placement : - single room - cohorting ( keep at least 1 meter between patients’ beds)
• Use surgical or procedure mask.
• Patient transport : - limit patient movement - use of surgical mask by patient

Contact Precautions• Use gloves & gown for all contact with the patient or the patient’s environment.
• Use either disposable equipment or dedicate equipment to specific patients.
• HCWs should refrain from touching their eyes, nose, or mouth with potentially contaminated gloved or ungloved hands.
• Avoid contaminating environmental surfaces that are not directly related to patient care ( e.g. door handles, light switches ).

Airborne Precautions
Airborne Infection (AI)Isolation Room HCWs to use N95 Mask
Cough EtiquettePatient to wear surgical maskduring transport to other hospitalareas.

Environmental Infection Control
• remove & dilute the air by maximizing natural ventilation through open windows
• use of mechanical ventilation (window fans, exhaust systems)
• air filtration & ultraviolet germicidal irradiation
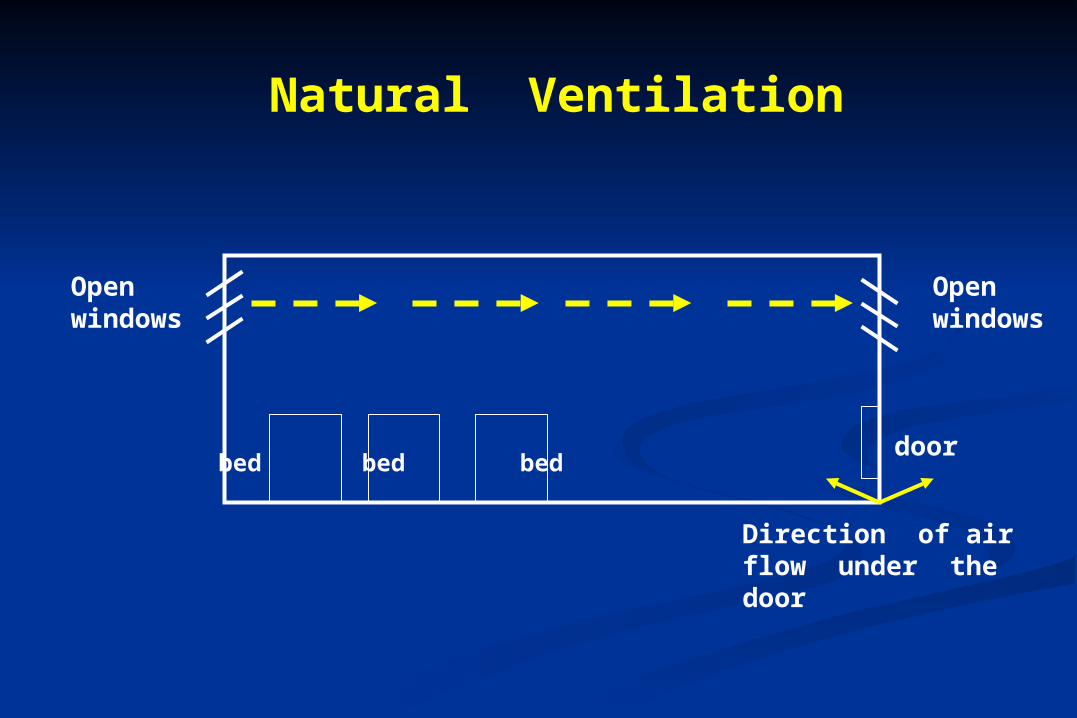
Natural Ventilation
Openwindows
Openwindows
doorbed bed bed
Direction of airflow under thedoor

Recommended Ventilation in Prevention of Airborne
Infections•Negative-pressure ventilation in rooms : air flow into room from adjacent
areas, exhaust air to the outside
•6 or more air changes per hour (ACH) desirable
•6 ACH 99% reduction of concentration of infectious particles

Negative Pressure Ventilation
door bed bed bed
Direction of airflow under thedoor ; negativepressure withrespect to corridor
air conditionerAirflow exhaust
Airflow intake


LCP Airborne Infection Isolation Units








RESPIRATORY
HYGIENE / COUGH
ETIQUETTE
NEW


Respiratory Hygiene / Cough Etiquette
• Cover the nose / mouth when coughing or sneezing.
• Use tissues to contain respiratory secretions and dispose of them in the nearest waste receptacle after use.
• Perform hand hygiene after having contact with respiratory secretions and contaminated objects / materials.
CDC 2003
Standard Precautions• Hand Hygiene Hand washing
Alcohol-based hand rubs
• Personal Protective Equipment (PPE) Gloves Facial protection : mask face shield goggles Gown Foot protection
• Proper handling of needles & sharp devices.

HEALTH CARE WORKER’S HANDS
Probably the MOST common means by which spread of
infection by direct contact can occur


The Hand Takes Germs from :- the skin, dirty wounds, pus excretions of the sick- the body, the hands, the clothes of the physicians and hospital personnel
The Hand Takes Germs from :- the skin, dirty wounds, pus excretions of the sick- the body, the hands, the clothes of the physicians and hospital personnel

The Hand Takes Germs from :- the skin, dirty wounds, pus excretions of the sick- the body, the hands, the clothes of the physicians and hospital personnel
The Hand Takes Germs from :- the skin, dirty wounds, pus excretions of the sick- the body, the hands, the clothes of the physicians and hospital personnel
The Hand Infects- newly operated
- the child, the chronically ill- the old patient
- ALL sick people- ALL hospital personnel
The Hand Takes Germs from :- the skin, dirty wounds, pus excretions of the sick- the body, the hands, the clothes of the physicians and hospital personnel
The Hand Takes Germs from :- the skin, dirty wounds, pus excretions of the sick- the body, the hands, the clothes of the physicians and hospital personnel
The Hand Infects- newly operated
- the child, the chronically ill- the old patient
- ALL sick people- ALL hospital personnel
The Hand contaminates- the physicians’ instruments
- clean laundry- toiletries
- sanitary equipments- dishes and silver etc.
The Hand contaminates- the physicians’ instruments
- clean laundry- toiletries
- sanitary equipments- dishes and silver etc.

The Hand Takes Germs from :- the skin, dirty wounds, pus excretions of the sick- the body, the hands, the clothes of the physicians and hospital personnel
The Hand Takes Germs from :- the skin, dirty wounds, pus excretions of the sick- the body, the hands, the clothes of the physicians and hospital personnel
The Hand Infects- newly operated
- the child, the chronically ill- the old patient
- ALL sick people- ALL hospital personnel
The Hand contaminates- the physicians’ instruments
- clean laundry- toiletries
- sanitary equipments- dishes and silver etc.
The Hand contaminates- the physicians’ instruments
- clean laundry- toiletries
- sanitary equipments- dishes and silver etc.
The Hand transfer Germs from:
bed sheets, dirty underwear, moist towels, sinks and
bathtubs, toiletries
The Hand transfer Germs from:
bed sheets, dirty underwear, moist towels, sinks and
bathtubs, toiletries

Hand Hygiene
• Required for Standard and Expanded Precautions
• Perform…• Immediately after removing PPE
• Between patient contacts
• Wash hands thoroughly with soap and water or use alcohol-based hand rub

Types of Hand Hygiene
Level 1 : Handwashing – plain soap + water
Level 2 : Hand Antisepsis - antimicrobial soap or alcohol-based products
Level 3 : Surgical Hand Scrub
HANDWASHING
• Considered to be one of the MOST important procedures in the prevention of hospital-acquired infection
• defined as vigorous, brief rubbing together of all surfaces of lathered hands, followed by rinsing under stream of water for at least 10 seconds

After removing gloves Before and after
patient contact After contact with
blood or body fluids from any patient
After taking blood pressure or vital signs from any patient
Handwashing – When?

After using bathroom
After blowing or wiping nose
Before preparing food
Before eating
Handwashing – When?

Handwashing Handwashing –– How? How?
Handwashing procedure
• Running water• Soap• Friction• Alcohol-based hand rub

The Hands are moistened and 3The Hands are moistened and 3--5 ml formulation is applied to cupped hands. The 5 ml formulation is applied to cupped hands. The hands are then rubbed together 5 times as follows : hands are then rubbed together 5 times as follows :
Defined Technique for Hand WashingDefined Technique for Hand Washing
1. PALM to PALM1. PALM to PALM 2. Right Palm over 3. PALM t2. Right Palm over 3. PALM to PALMo PALMdorsum and vice versadorsum and vice versa fingers interlaced fingers interlaced
4. Back of4. Back of fingerrsfingerrs 5. Rotational rubbing of5. Rotational rubbing of 6. Rotational rubbing, 6. Rotational rubbing, to opposing palms, right thumb clasped into opposing palms, right thumb clasped in backwards and forwards backwards and forwards fingers interlocked left palm and vice versafingers interlocked left palm and vice versa with clasped fingers ofwith clasped fingers of
right hright hand in leftand in leftpalm anpalm and vice versad vice versa

Handwashing Steps
Wet hands and wrists.
Apply soap or alcohol-based hand rub.
Step 1

Handwashing Steps
Right palm over left , left over right.
Step 2

Handwashing Steps
Palm to palm , fingers interlaced.
Step 3

Handwashing Steps
Back fingers to opposing fingers interlocked.
Step 4

Handwashing Steps
Rotational rubbing of right thumb clasped in left palm and vice versa.
Step 5

Handwashing Steps
Rotational rubbing backwards andforwards with tops of fingers and thumb of right hand in left and vice versa.
Step 6

Handwashing Steps
Step 7
Rinse hands wellunder runningwater.

HYGIENIC HAND RUB• An alternative method
of hand disinfection if
hands are not visibly
soiled.
• A rapid and effective alternative to hand washing (e.g. ward rounds with no water and no wash basin)

HYGIENIC HAND RUB• Alcohol-based products are
more effective for standard handwashing or hand sepsis by HCWs than soap or antimicrobial soaps.
• Alcohol solutions containing 60% - 95% are most effective. Higher concentrations are
less potent.
(HICPAC / SHEA / APIC / IDSA Hand Hygiene Task Force)

HYGIENIC HAND RUBALCHOLIC HAND
RUBS DO NOT CLEANSE,
therefore hands should be cleaned
with soap and water in the presence of visible
contamination

HYGIENIC HAND RUB
PROCEDURE: • Apply 3-5 ml of fast acting antiseptic (e.g.
alcohol hand rub containing glycerol as an emollient to
prevent excessive drying of hands).
• Rub hands together after application of alcohol-based products until all the alcohol has evaporated.


What infections can be caused by needlestick injuries?
Pathogens that pose the most serious health risks : • Hepatitis B Virus (HBV)• Hepatitis C Virus (HCV)• Human immunodeficiency virus (HIV) – causes AIDS

Preventing needlestick injuries is the best way to protect yourself from
these blood-borne infections.
Who is at risk of needlestick injury ?
Any worker who may come in contact with needles is at risk :
• doctors• nursing staff
• laboratory workers• housekeepers

What kinds of needles usually causeneedlestick injuries?
• Hypodermic needles• Blood collection needles• Suture needles• Needles used in IV delivery systems

What work practices increase the risk ofneedlestick injuries?
• Recapping used needles.• Transferring a body fluid between containers.• Failing to dispose of used needles properly in puncture-resistant sharps containers.

How can you protect yourself fromneedlestick injuries? (1)
• Avoid the use of needles where safe and effective alternatives are available.
• Use devices with safety features.
• Avoid recapping needles.
• Plan for safe handling and disposal of needles before using them.
• Promptly dispose of used needles in appropriate sharps disposal containers.

Syringes with Safety Features

Handling Needles & Other Sharps
• Handle all needles & sharp instruments with care.
• Use devices with safety features.
• Never recap used needles with hands.
• Recap needles using the “scooping” method.

• Plan safe handling and disposal before beginning any procedure using needles.
• Dispose of used needle device promptly in appropriate sharps disposal containers.
Proper Sharps Disposal
Puncture – resistant Container

How can you protect yourself fromneedlestick injuries? (2)
• Report all needlestick and sharps-related injuries promptly to the employees’ physician to ensure that you receive appropriate medical care.
• Tell your supervisor about any needlestick hazards you observe.
• Get a hepatitis B vaccination.
• Participate in training related to infection prevention.

PREVENTION IS
PRIMARY!
PREVENTION IS
PRIMARY!Protect patients…protect healthcare personnel…
promote quality healthcare!

















