Page 1
How do midwives facilitate women to give birth during physiologicalsecond stage of labour? A systematic review
Healy, M., Nyman, V., Spence, D., Otten, R. H. J., & Verhoeven, C. (2020). How do midwives facilitate women togive birth during physiological second stage of labour? A systematic review. PLoS One, 15(7), [e0226502].https://doi.org/10.1371/journal.pone.0226502
Published in:PLoS One
Document Version:Publisher's PDF, also known as Version of record
Queen's University Belfast - Research Portal:Link to publication record in Queen's University Belfast Research Portal
Publisher rights© 2020 The Authors.This is an open access article published under a Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0/),which permits unrestricted use, distribution and reproduction in any medium, provided the author and source are cited.
General rightsCopyright for the publications made accessible via the Queen's University Belfast Research Portal is retained by the author(s) and / or othercopyright owners and it is a condition of accessing these publications that users recognise and abide by the legal requirements associatedwith these rights.
Take down policyThe Research Portal is Queen's institutional repository that provides access to Queen's research output. Every effort has been made toensure that content in the Research Portal does not infringe any person's rights, or applicable UK laws. If you discover content in theResearch Portal that you believe breaches copyright or violates any law, please contact [email protected] .
Download date:03. Nov. 2021
Page 2
RESEARCH ARTICLE
How do midwives facilitate women to give
birth during physiological second stage of
labour? A systematic review
Maria HealyID1*, Viola Nyman2,3, Dale Spence1, Rene H. J. OttenID
4, Corine
J. Verhoeven5,6,7
1 School of Nursing and Midwifery, Queen’s University Belfast, Belfast, Northern Ireland, United Kingdom,
2 Department of Research and Development, NU-Hospital Group, Trollhattan, Sweden, 3 Institute of Health
and Care Sciences, University of Gothenburg, Gothenburg, Sweden, 4 University Library, Vrije Universiteit
Amsterdam, Amsterdam, Netherlands, 5 Department of Midwifery Science, AVAG, Amsterdam Public Health
Research Institute, Amsterdam UMC, VU Medical Centre, Amsterdam, Netherlands, 6 Department of
Obstetrics and Gynaecology, Maxima Medical Centre, Veldhoven, Netherlands, 7 Division of Midwifery,
School of Health Sciences, University of Nottingham, Nottingham, United Kingdom
* [email protected]
Abstract
Both nationally and internationally, midwives’ practices during the second stage of labour
vary. A midwife’s practice can be influenced by education and cultural practices but ulti-
mately it should be informed by up-to-date scientific evidence. We conducted a systematic
review of the literature to retrieve evidence that supports high quality intrapartum care during
the second stage of labour. A systematic literature search was performed to September
2019 in collaboration with a medical information specialist. Bibliographic databases
searched included: PubMed, EMBASE, Cumulative Index to Nursing and Allied Health Liter-
ature (CINAHL), PsycINFO, Maternity and Infant Care Database and The Cochrane Library,
resulting in 6,382 references to be screened after duplicates were removed. Articles were
then assessed for quality by two independent researchers and data extracted. 17 studies
focusing on midwives’ practices during physiological second stage of labour were included.
Two studies surveyed midwives regarding their practice and one study utilising focus groups
explored how midwives facilitate women’s birthing positions, while another focus group
study explored expert midwives’ views of their practice of preserving an intact perineum dur-
ing physiological birth. The remainder of the included studies were primarily intervention
studies, highlighting aspects of midwifery practice during the second stage of labour. The
empirical findings were synthesised into four main themes namely: birthing positions, non-
pharmacological pain relief, pushing techniques and optimising perineal outcomes; the
results were outlined and discussed. By implementing this evidence midwives may enable
women during the second stage of labour to optimise physiological processes to give birth.
There is, however, a dearth of evidence relating to midwives’ practice, which provides a pos-
itive experience for women during the second stage of labour. Perhaps this is because not
all midwives’ practices during the second stage of labour are researched and documented.
This systematic review provides a valuable insight of the empirical evidence relating to mid-
wifery practice during the physiological second stage of labour, which can also inform
PLOS ONE
PLOS ONE | https://doi.org/10.1371/journal.pone.0226502 July 28, 2020 1 / 19
a1111111111
a1111111111
a1111111111
a1111111111
a1111111111
OPEN ACCESS
Citation: Healy M, Nyman V, Spence D, Otten RHJ,
Verhoeven CJ (2020) How do midwives facilitate
women to give birth during physiological second
stage of labour? A systematic review. PLoS ONE
15(7): e0226502. https://doi.org/10.1371/journal.
pone.0226502
Editor: Christine E East, La Trobe University,
AUSTRALIA
Received: July 4, 2019
Accepted: November 19, 2019
Published: July 28, 2020
Peer Review History: PLOS recognizes the
benefits of transparency in the peer review
process; therefore, we enable the publication of
all of the content of peer review and author
responses alongside final, published articles. The
editorial history of this article is available here:
https://doi.org/10.1371/journal.pone.0226502
Copyright: © 2020 Healy et al. This is an open
access article distributed under the terms of the
Creative Commons Attribution License, which
permits unrestricted use, distribution, and
reproduction in any medium, provided the original
author and source are credited.
Data Availability Statement: All relevant data are
within the paper and its Supporting Information
files.
Page 3
education and future research. The majority of the authors were members of the EU COST
Action IS1405: Building Intrapartum Research Through Health (BIRTH). The study protocol
is registered in the International Prospective Register of Systematic Reviews (PROSPERO;
Registration CRD42018088300) and is published (Verhoeven, Spence, Nyman, Otten,
Healy, 2019).
Introduction
Childbirth is a significant and memorable life event for a woman and her family. Women’s
experiences of birth have both short and long-term effects on their health and wellbeing for
both themselves and their infants [1–6]. As stated by the World Health Organization (WHO)
in 2018, the primary outcome for all pregnant women is to have a ‘positive childbirth experi-ence’. This includes giving birth to a healthy baby in a conducive, safe environment with conti-
nuity of care provided by kind, competent maternity care professionals [7]. In addition, the
WHO has highlighted that most women value a physiological labour and birth. Experiencing
physiological childbirth also has a long-term impact: ‘The health and well-being of a motherand child at birth largely determines the future health and wellness of the entire family’ [8]. Fur-
thermore, childbirth has physical effects on women and their future pregnancies. Although
cesarean delivery is associated with a reduced rate of urinary incontinence and pelvic organ
prolapse, it is also associated with increased risks for fertility, future pregnancy, and long-term
childhood outcomes such as increased odds of asthma and obesity [9].
Normal physiological birth was defined by the WHO as ‘spontaneous in onset, low-risk atthe start of labour and remaining so throughout labour and delivery. The infant is born sponta-neously in the vertex position between 37 and 42 completed weeks of pregnancy. After birthmother and infant are in good condition’ [10]. Labour can be divided into three stages: the first,
second and third stage of labour. The first stage of labour is defined as the time period charac-
terised by regular painful uterine contractions until full dilatation of the cervix and the second
stage of labour as the time period between full dilatation of the cervix and the birth of the baby,
whilst the woman is experiencing an involuntary urge to bear down, due to expulsive uterine
contractions [7]. The third stage is recognised as the period after the birth of the baby ending
with the birth of the placenta and fetal membranes [11].
Normal physiological birth is associated with the non-use of an epidural or other pharma-
cological pain relief, as it may affect the natural course of labour and can lead to rare but
potentially severe adverse maternal effects [10, 12]. The same accounts for induction and aug-
mentation of labour. Especially high doses of synthetic oxytocin may cause more and longer
painful contractions when compared to normal labour [13]. Uvnas-Moberg has highlighted
how the process of physiological labour and birth can be enabled by the interplay of reproduc-
tive hormonal and neuro-hormonal mechanisms when the midwife provides kind and respect-
ful caring practices. These practices promote oxytocin release for effective uterine contractions
during labour and the relaxation of the birth canal [14, 15]. Little is known of the variety of
physical and emotional actions the midwife does when ‘being with’ a woman during birth of
the baby, in particular, how midwives facilitate this physiological process. According to Ken-
nedy et al. it is a research priority to identify and highlight aspects of care that optimise, and
those that disturb, the biological/physiological processes during childbirth [16].
The objective of this systematic review was therefore, to examine the evidence relating to
intrapartum midwifery care, focusing specifically on care during the second stage of labour.
PLOS ONE How midwives facilitate women to give birth during physiological second stage of labour?
PLOS ONE | https://doi.org/10.1371/journal.pone.0226502 July 28, 2020 2 / 19
Funding: This article is based upon work funded by
the COST Action IS1405 BIRTH: "Building
Intrapartum Research Through Health - An
interdisciplinary whole system approach to
understanding and contextualising physiological
labour and birth" (http://www.cost.eu/COST_
Actions/isch/IS1405), supported by EU COST
(European Cooperation in Science and
Technology). Furthermore, the School of Nursing
and Midwifery, Queen’s University Belfast, funded
access to Covidence, the web-based systematic
review software package recommended by
Cochrane. The funders had no role in study design,
data collection and analysis, decision to publish, or
preparation of the manuscript.
Competing interests: The authors have declared
that no competing interests exist.
Abbreviations: CERQual, Confidence in the
Evidence from Reviews of Qualitative research;
GRADE, Grading of Recommendations
Assessment, Development and Evaluation; PEO,
Population, Exposure, Outcomes; PICO, Patient or
Population, Intervention, Comparison, Outcome;
PRISMA, Preferred Reporting Items for Systematic
Reviews and Meta-Analysis; PROSPERO,
International Prospective Register of Systematic
Reviews; WHO, World Health Organization.
Page 4
The structured research questions were formulated using the PICO (Patient or Population,
Intervention, Comparison, Outcome) framework for quantitative research and the PEO (Pop-
ulation, Exposure, Outcomes) question format for qualitative research questions: ‘How do mid-wives facilitate women to give birth during physiological second stage of labour?
The results of this systematic review will support high quality intrapartum care during the
second stage and inform midwifery practice, education and future research and positively
influence this aspect of midwifery care for women.
Methods
We undertook a systematic literature search based on the Preferred Reporting Items for Sys-
tematic Reviews and Meta-Analysis (PRISMA) statement (S1 Checklist) [17]. The Peer Review
of Electronic Search Strategies (PRESS) 2015 Guideline Statement was used to enhance the
quality and comprehensiveness of the electronic literature search [18]. The PICO framework
for quantitative and PEO framework for qualitative studies were also utilised: P: women in sec-
ond stage of labour, I: intrapartum intervention by midwives, C: standard care, O: spontaneous
physiological birth. PEO framework: P: women in second stage of labour, E: midwives’ prac-
tices in the second stage of labour, O: spontaneous physiological birth. Systematic searches of
the bibliographic databases: EMBASE.com, Cinahl, PsycINFO, PubMed, Maternity and Infant
Care Database and The Cochrane Library were conducted.
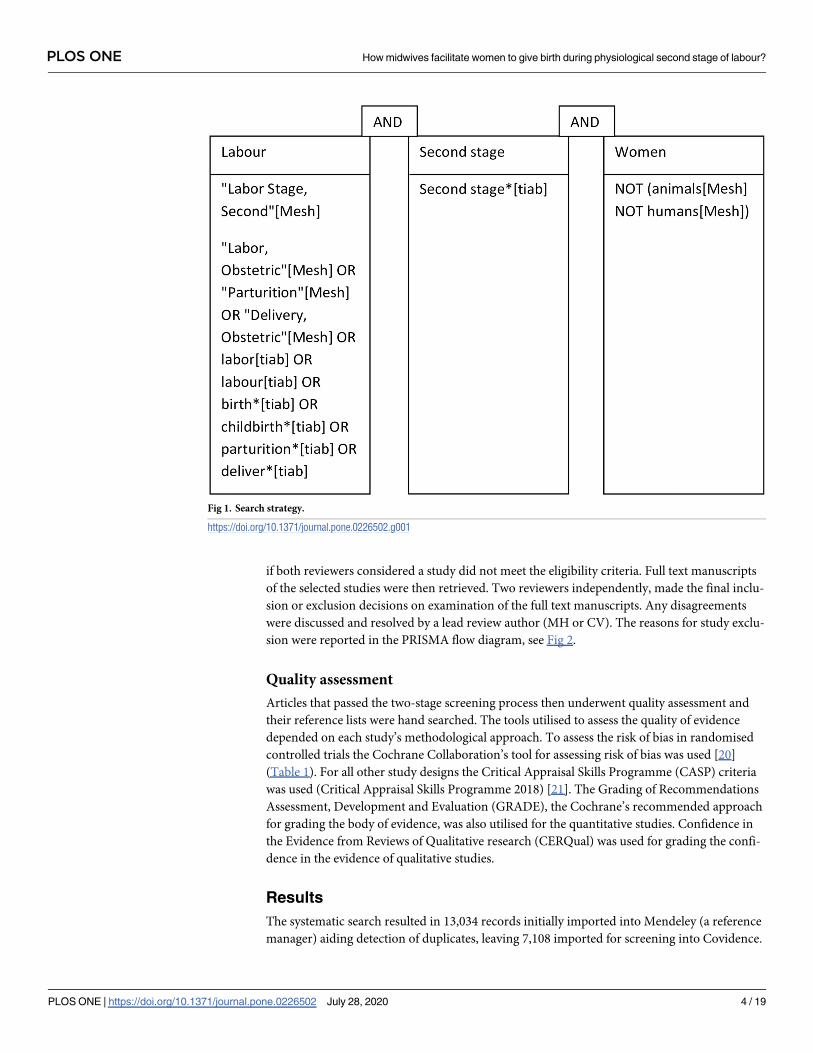
The search strategy included the Boolean terms OR and AND, the search terms included
controlled terms (for example, MeSH terms in PubMed and Emtree in Embase) as well as free
text terms and truncations (�) (S1 Table). We used free text terms only in The Cochrane
Library and synonyms and variations of the keywords in all databases. The search terms
include: “Labor, Obstetric"[Mesh] OR "Parturition"[Mesh] OR "Delivery, Obstetric" [Mesh]
OR labor [tiab] OR labour[tiab] OR birth�[tiab] OR childbirth�[tiab] OR parturition�[tiab]
OR deliver�[tiab] OR “Labor, Stage, Second"[Mesh], see Fig 1.
Inclusion/exclusion criteria
Only full text articles published in peer-reviewed journals were included. All languages were
accepted, as the authors were part of the EU COST Action IS1405: Building IntrapartumResearch Through Health (BIRTH) network and therefore had access for most languages to be
translated, if necessary. All studies describing midwives’ care or practice during second stage
of physiological birth or normal birth were included. Both relevant quantitative and qualitative
studies were eligible for review.
Case studies were excluded. Studies examining midwifery practice of women that focused
only on care during the first or third stage of labour were excluded. Studies including women
who had an epidural, spinal, operative vaginal birth or caesarean section were also excluded.
Furthermore, studies that included women, who had a preterm birth, had their pregnancy
induced or labour augmented with intravenous oxytocin were excluded. Searches of the biblio-
graphic databases were undertaken initially from inception to 8th May 2018. The search was
further refined to include papers published from 1st January 2008 to 8th May 2018, reflecting
the National Institute for Health and Care Excellence (NICE) [19] Intrapartum care guidance
which was updated at the end of 2007. Furthermore, we updated the search to 5th September
2019, in collaboration with a medical librarian. Animal studies were excluded.
Studies were selected for inclusion following a two-stage process using Covidence, which is
a web-based software platform that streamlines the production of systematic reviews, includ-
ing Cochrane reviews. Within the first screening stage each study had the title and abstract
screened by pairs of two independent reviewers (CV, DS, VN, MH) and studies were excluded
PLOS ONE How midwives facilitate women to give birth during physiological second stage of labour?
PLOS ONE | https://doi.org/10.1371/journal.pone.0226502 July 28, 2020 3 / 19
Page 5
if both reviewers considered a study did not meet the eligibility criteria. Full text manuscripts
of the selected studies were then retrieved. Two reviewers independently, made the final inclu-
sion or exclusion decisions on examination of the full text manuscripts. Any disagreements
were discussed and resolved by a lead review author (MH or CV). The reasons for study exclu-
sion were reported in the PRISMA flow diagram, see Fig 2.
Quality assessment
Articles that passed the two-stage screening process then underwent quality assessment and
their reference lists were hand searched. The tools utilised to assess the quality of evidence
depended on each study’s methodological approach. To assess the risk of bias in randomised
controlled trials the Cochrane Collaboration’s tool for assessing risk of bias was used [20]
(Table 1). For all other study designs the Critical Appraisal Skills Programme (CASP) criteria
was used (Critical Appraisal Skills Programme 2018) [21]. The Grading of Recommendations
Assessment, Development and Evaluation (GRADE), the Cochrane’s recommended approach
for grading the body of evidence, was also utilised for the quantitative studies. Confidence in
the Evidence from Reviews of Qualitative research (CERQual) was used for grading the confi-
dence in the evidence of qualitative studies.
Results
The systematic search resulted in 13,034 records initially imported into Mendeley (a reference
manager) aiding detection of duplicates, leaving 7,108 imported for screening into Covidence.
Fig 1. Search strategy.
https://doi.org/10.1371/journal.pone.0226502.g001
PLOS ONE How midwives facilitate women to give birth during physiological second stage of labour?
PLOS ONE | https://doi.org/10.1371/journal.pone.0226502 July 28, 2020 4 / 19
Page 6
Further duplicates were detected by Covidence, with 6,382 remaining for screening. Titles and
abstracts were then reviewed; subsequently 523 articles were retrieved for full text assessment.
Following detailed review 506 articles did not meet the inclusion criteria leaving 17 studies
included in this systematic review. Fig 2 summarises the search strategy and the reasons for
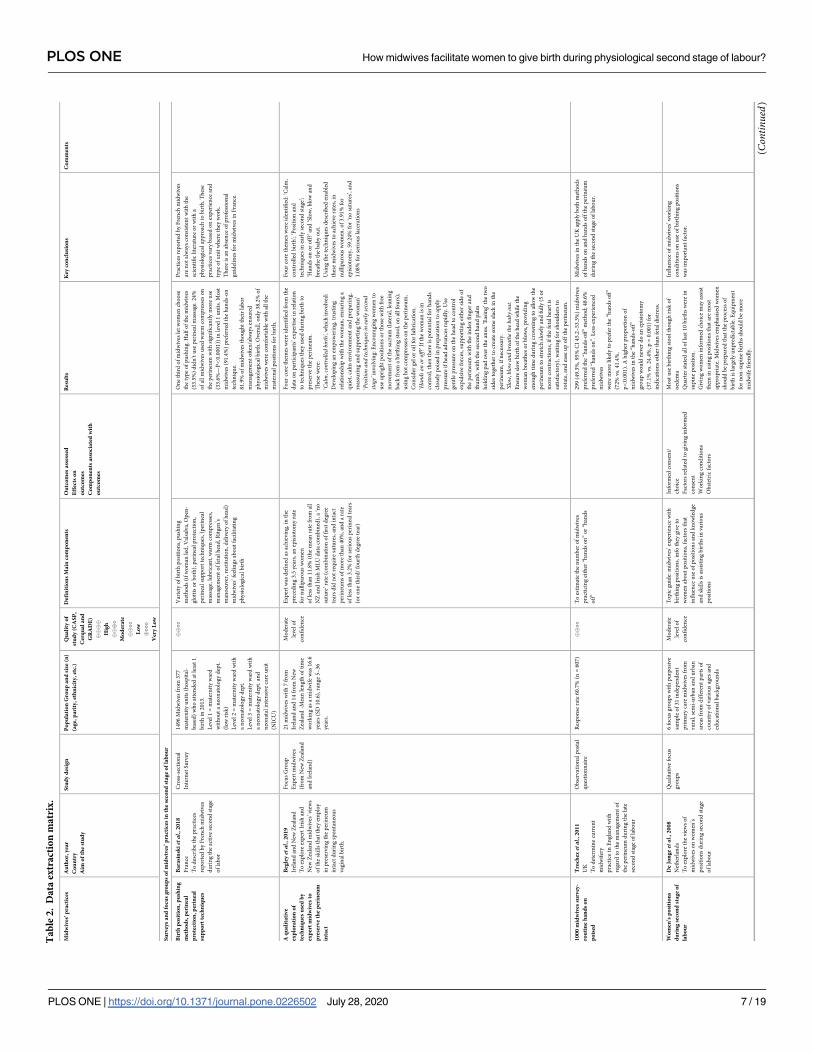
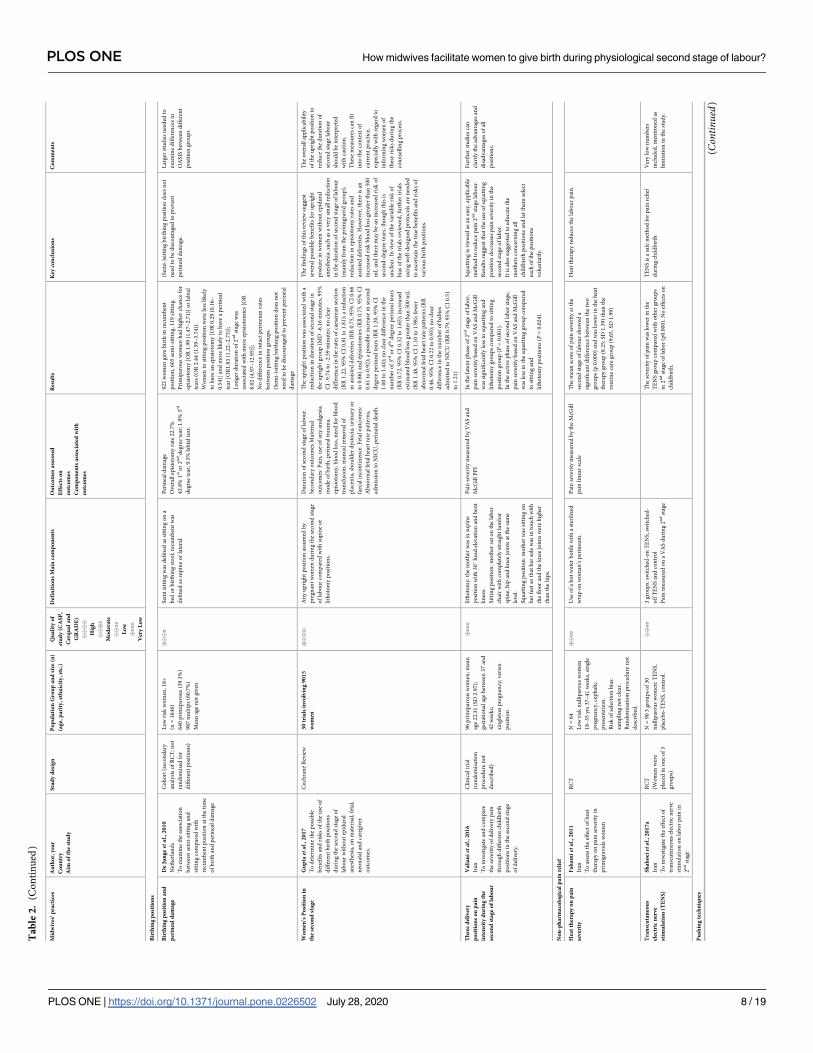
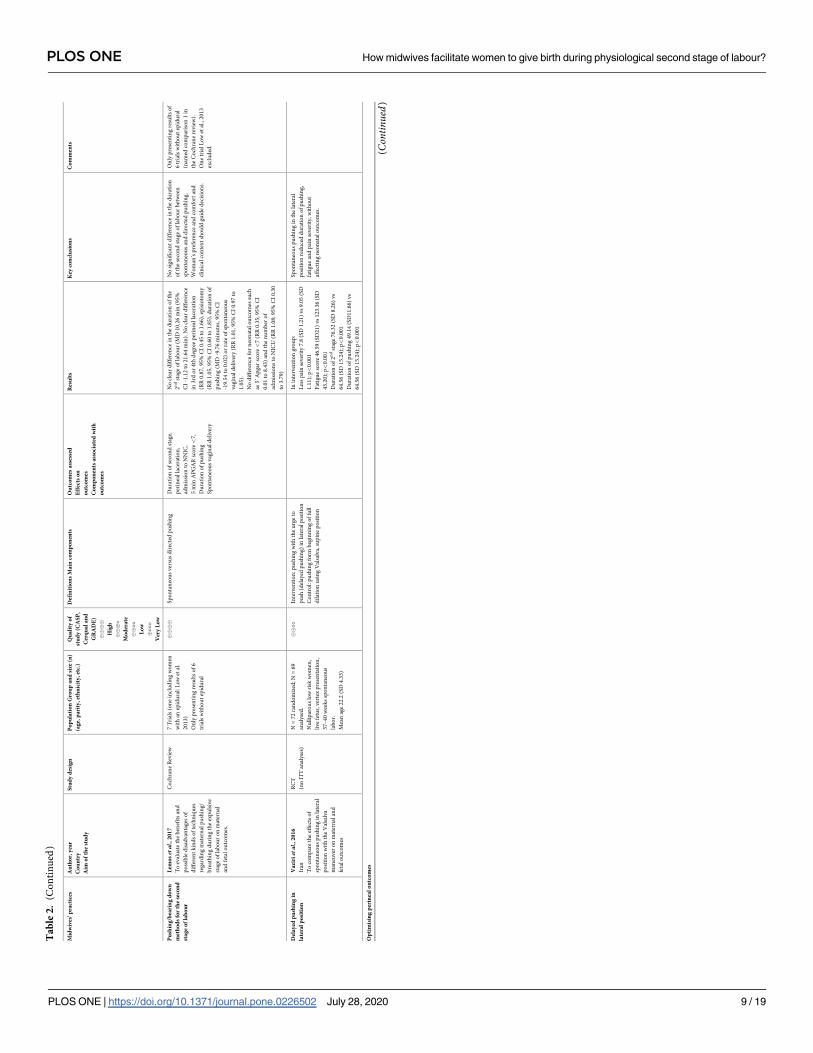
exclusion. Studies were grouped according to the study subject and for each study a data
extraction matrix was completed. The matrix comprised of ten key features of the study
Fig 2. Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) flow chart of articles included.
https://doi.org/10.1371/journal.pone.0226502.g002
PLOS ONE How midwives facilitate women to give birth during physiological second stage of labour?
PLOS ONE | https://doi.org/10.1371/journal.pone.0226502 July 28, 2020 5 / 19
Page 7
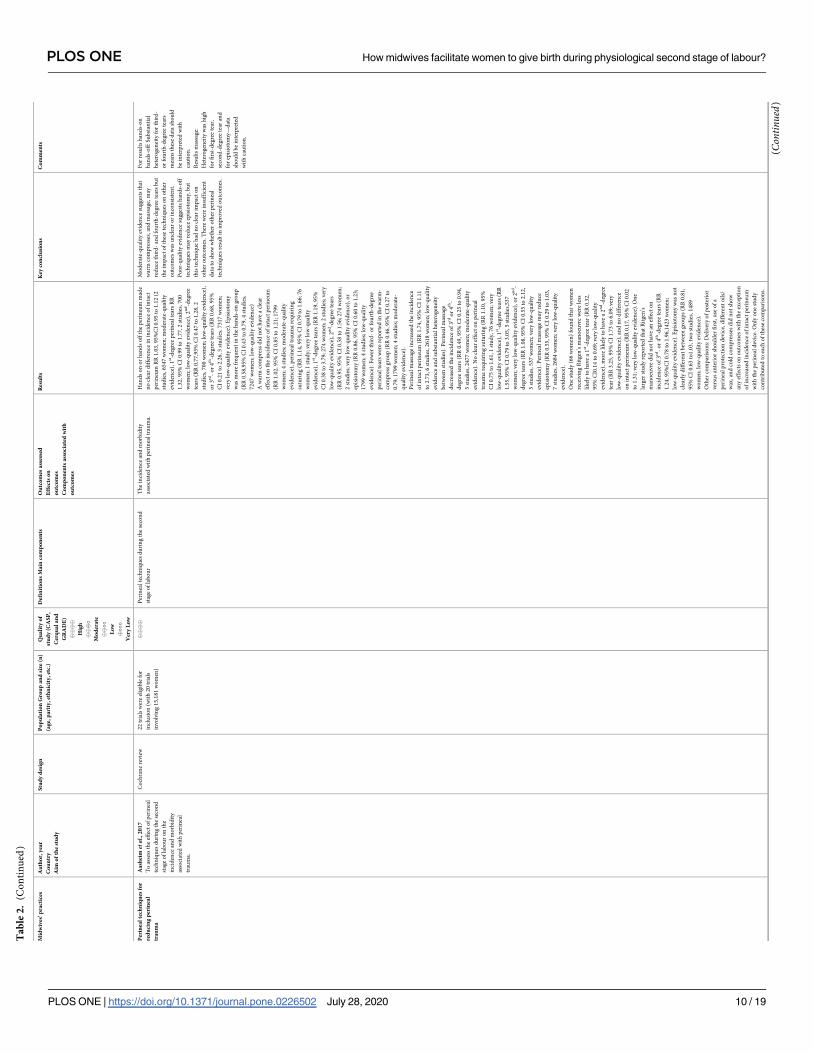
including: theme, author, year, country, study design, quality assessment, relevant participant
data, outcomes assessed, summary of the findings, comments (Table 2).
The seventeen included publications dated from 2008 to 2019. The majority of the studies
were systematic reviews (n = 6, of which 3 were Cochrane reviews) [22–27], randomised con-
trolled trials (n = 6) [28–33], one cohort studies with prospective data collection [34], two sur-
veys [35, 36] and two qualitative focus group studies [37, 38].
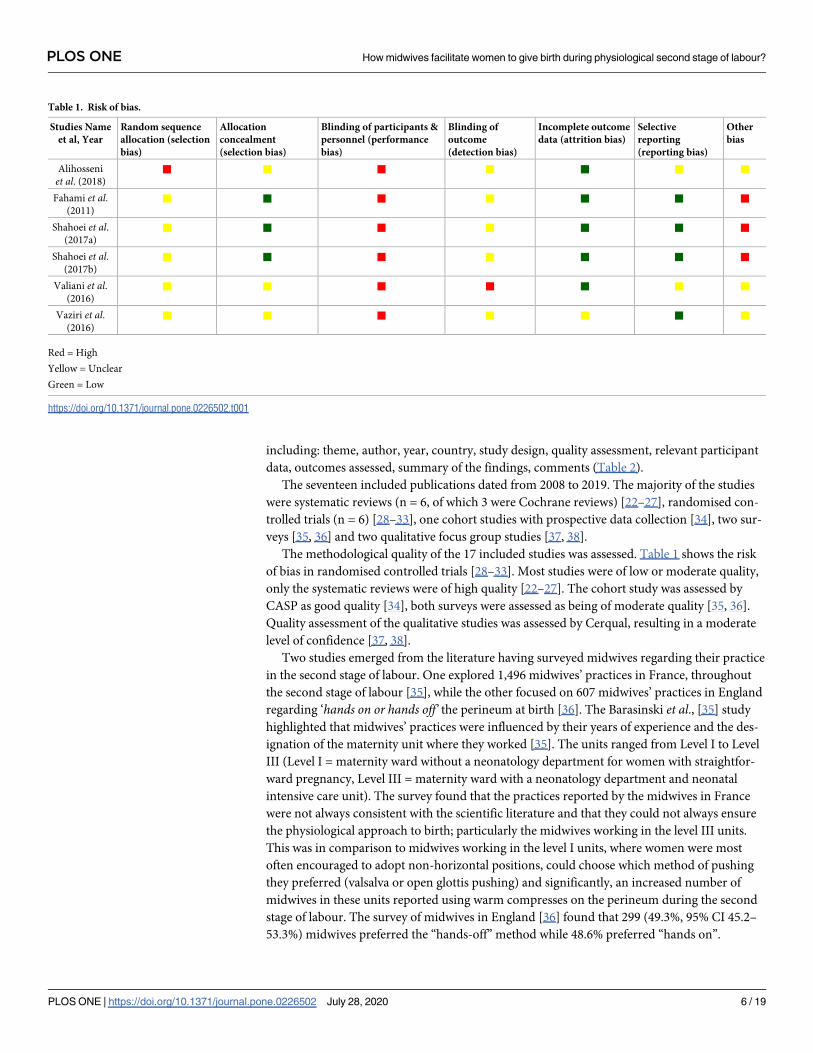
The methodological quality of the 17 included studies was assessed. Table 1 shows the risk
of bias in randomised controlled trials [28–33]. Most studies were of low or moderate quality,
only the systematic reviews were of high quality [22–27]. The cohort study was assessed by
CASP as good quality [34], both surveys were assessed as being of moderate quality [35, 36].
Quality assessment of the qualitative studies was assessed by Cerqual, resulting in a moderate
level of confidence [37, 38].
Two studies emerged from the literature having surveyed midwives regarding their practice
in the second stage of labour. One explored 1,496 midwives’ practices in France, throughout
the second stage of labour [35], while the other focused on 607 midwives’ practices in England
regarding ‘hands on or hands off’ the perineum at birth [36]. The Barasinski et al., [35] study
highlighted that midwives’ practices were influenced by their years of experience and the des-
ignation of the maternity unit where they worked [35]. The units ranged from Level I to Level
III (Level I = maternity ward without a neonatology department for women with straightfor-
ward pregnancy, Level III = maternity ward with a neonatology department and neonatal
intensive care unit). The survey found that the practices reported by the midwives in France
were not always consistent with the scientific literature and that they could not always ensure
the physiological approach to birth; particularly the midwives working in the level III units.
This was in comparison to midwives working in the level I units, where women were most
often encouraged to adopt non-horizontal positions, could choose which method of pushing
they preferred (valsalva or open glottis pushing) and significantly, an increased number of
midwives in these units reported using warm compresses on the perineum during the second
stage of labour. The survey of midwives in England [36] found that 299 (49.3%, 95% CI 45.2–
53.3%) midwives preferred the “hands-off” method while 48.6% preferred “hands on”.
Table 1. Risk of bias.
Studies Name
et al, Year
Random sequence
allocation (selection
bias)
Allocation
concealment
(selection bias)
Blinding of participants &
personnel (performance
bias)
Blinding of
outcome
(detection bias)
Incomplete outcome
data (attrition bias)
Selective
reporting
(reporting bias)
Other
bias
Alihosseni
et al. (2018)
■ ■ ■ ■ ■ ■ ■
Fahami et al.(2011)
■ ■ ■ ■ ■ ■ ■
Shahoei et al.(2017a)
■ ■ ■ ■ ■ ■ ■
Shahoei et al.(2017b)
■ ■ ■ ■ ■ ■ ■
Valiani et al.(2016)
■ ■ ■ ■ ■ ■ ■
Vaziri et al.(2016)
■ ■ ■ ■ ■ ■ ■
Red = High
Yellow = Unclear
Green = Low
https://doi.org/10.1371/journal.pone.0226502.t001
PLOS ONE How midwives facilitate women to give birth during physiological second stage of labour?
PLOS ONE | https://doi.org/10.1371/journal.pone.0226502 July 28, 2020 6 / 19
Page 8
Ta
ble
2.
Da
taex
tra
ctio
nm
atr
ix.
Mid
wiv
es’
pra
ctic
esA
uth
or,
yea
r
Co
un
try
Aim
of
the
stu
dy
Stu
dy
des
ign
Po
pu
lati
on
Gro
up
an
dsi
ze(n
)
(ag
e,p
ari
ty,
eth
nic
ity
,et
c.)
Qu
ali
tyo
f
stu
dy
(CA
SP
,
Cer
qu
al
an
d
GR
AD
E)
����
Hig
h
����
Mo
der
ate
����
Lo
w
����
Ver
yL
ow
Def
init
ion
sM
ain
com
po
nen
tsO
utc
om
esa
sses
sed
Eff
ects
on
ou
tco
mes
Co
mp
on
ents
ass
oci
ate
dw
ith
ou
tco
mes
Res
ult
sK
eyco
ncl
usi
on
sC
om
men
ts
Su
rvey
sa
nd
focu
sg
rou
ps
of
mid
wiv
es’
pra
ctic
esin
the
seco
nd
sta
ge
of
lab
ou
r
Bir
thp
osi
tio
n,
pu
shin
g
met
ho
ds,
per
inea
l
pro
tect
ion
,p
erin
eal
sup
po
rtte
chn
iqu
es
Ba
rasi
nsk
ietal
.,2
01
8
Fra
nce
To
des
crib
eth
ep
ract
ices
rep
ort
edb
yF
ren
chm
idw
ives
du
rin
gth
eac
tiv
ese
con
dst
age
of
lab
or
Cro
ss-s
ecti
on
al
Inte
rnet
Su
rvey
14
96
Mid
wiv
esfr
om
37
7
mat
ern
ity
un
its
(ho
spit
al-
bas
ed)
wh
oat
ten
ded
atle
ast
1
bir
thin
20
13
.
Lev
el1
=m
ater
nit
yw
ard
wit
ho
ut
an
eon
ato
log
yd
ept.
(lo
wri
sk)
Lev
el2
=m
ater
nit
yw
ard
wit
h
an
eon
ato
log
yd
ept.
Lev
el3
=m
ater
nit
yw
ard
wit
h
an
eon
ato
log
yd
ept.
and
neo
nat
alin
ten
siv
eca
reu
nit
(NIC
U)
����
Var
iety
of
bir
thp
osi
tio
ns,
pu
shin
g
met
ho
ds
(if
wo
man
led
,V
alsa
lva,
Op
en-
glo
ttis
or
bo
th),
per
inea
lp
rote
ctio
n,
per
inea
lsu
pp
ort
tech
niq
ues
,(p
erin
eal
mas
sag
e,lu
bri
can
t,w
arm
com
pre
sses
,
man
agem
ent
of
feta
lh
ead
,R
itg
en’s
man
oeu
ver
,re
stit
uti
on
,d
eliv
ery
of
hea
d)
mid
wiv
es’
feel
ing
sab
ou
tfa
cili
tati
ng
ph
ysi
olo
gic
alb
irth
On
eth
ird
of
mid
wiv
esle
tw
om
ench
oo
se
the
typ
eo
fp
ush
ing
.H
alf
of
the
mid
wiv
es
(53
.5%
)d
idn
’tu
sep
erin
eal
mas
sag
e.2
4%
of
all
mid
wiv
esu
sed
war
mco
mp
ress
eso
n
the
per
ineu
mw
ith
sig
nif
ican
tly
mo
reu
se
(33
.6%
—P<
0.0
00
1))
inle
vel
1u
nit
s.M
ost
mid
wiv
es(9
1.4
%)
pre
ferr
edth
eh
and
s-o
n
tech
niq
ue.
81
.9%
of
mid
wiv
esth
ou
gh
tth
eir
lab
or
man
agem
ent
oft
en/a
lway
sen
sure
d
ph
ysi
olo
gic
alb
irth
.O
ver
all,
on
ly3
8.2
%o
f
mid
wiv
esw
ere
com
fort
able
wit
hal
lth
e
mat
ern
alp
osi
tio
ns
for
bir
th.
Pra
ctic
esre
po
rted
by
Fre
nch
mid
wiv
es
are
no
tal
way
sco
nsi
sten
tw
ith
the
scie
nti
fic
lite
ratu
reo
rw
ith
a
ph
ysi
olo
gic
alap
pro
ach
tob
irth
.T
hes
e
pra
ctic
esvar
yb
ased
on
exp
erie
nce
and
typ
eo
fu
nit
wh
ere
they
wo
rk.
Th
ere
isan
abse
nce
of
pro
fess
ion
al
gu
idel
ines
for
mid
wiv
esin
Fra
nce
.
Aq
ua
lita
tiv
e
exp
lora
tio
no
f
tech
niq
ues
use
db
y
exp
ert
mid
wiv
esto
pre
serv
eth
ep
erin
eum
inta
ct
Beg
leyetal
.,2
01
9
Irel
and
and
New
Zea
lan
d
To
exp
lore
exp
ert
Iris
han
d
New
Zea
lan
dm
idw
ives
’vie
ws
of
the
skil
lsth
atth
eyem
plo
y
inp
rese
rvin
gth
ep
erin
eum
inta
ctd
uri
ng
spo
nta
neo
us
vag
inal
bir
th.
Fo
cus
Gro
up
Ex
per
tm
idw
ives
(fro
mN
ewZ
eala
nd
and
Irel
and
)
21
mid
wiv
esw
ith
7fr
om
Irel
and
and
14
fro
mN
ew
Zea
lan
d-M
ean
len
gth
of
tim
e
wo
rkin
gas
am
idw
ife
was
16
.6
yea
rs(S
D1
0.6
),ra
ng
e5
–3
6
yea
rs.
Mo
der
ate
level
of
con
fid
ence
Ex
per
tw
asd
efin
edas
ach
iev
ing
,in
the
pre
ced
ing
3.5
yea
rs,
anep
isio
tom
yra
te
for
nu
llip
aro
us
wo
men
of
less
than
11
.8%
(th
em
ean
rate
fro
mal
l
NZ
and
Iris
hM
LU
dat
aco
mb
ined
),a
‘no
sutu
re’ra
te(c
om
bin
atio
no
ffi
rst
deg
ree
tear
sd
idn
ot
req
uir
esu
ture
s,an
din
tact
per
ineu
ms
of
mo
reth
an4
0%
,an
da
rate
of
less
than
3.2
%fo
rse
rio
us
per
inea
lte
ars
(or
on
eth
ird
/fo
urt
hd
egre
ete
ar)
Fo
ur
core
them
esw
ere
iden
tifi
edfr
om
the
dat
ao
np
arti
cip
ants
’ex
per
tise
inre
lati
on
tote
chn
iqu
esth
eyu
sed
du
rin
gb
irth
to
pre
serv
eth
ep
erin
eum
.
Th
ese
wer
e:
‘Cal
m,
cont
rolle
dbi
rth’
,w
hic
hin
vo
lved
:
Dev
elo
pin
gan
emp
ow
erin
g,
tru
stin
g
rela
tio
nsh
ipw
ith
the
wo
man
,en
suri
ng
a
qu
iet,
calm
envir
on
men
tan
dp
rep
arin
g,
reas
suri
ng
and
sup
po
rtin
gth
ew
om
an’
‘Pos
ition
and
tech
niqu
esin
early
seco
ndst
age’
invo
lvin
g:
En
cou
rag
ing
wo
men
to
use
up
rig
ht
po
siti
on
so
rth
ose
wit
hfr
ee
mo
vem
ent
of
the
sacr
um
(lat
eral
,le
anin
g
bac
kfr
om
ab
irth
ing
sto
ol,
on
all
fou
rs),
usi
ng
ho
tco
mp
ress
eso
nth
ep
erin
eum
,
Co
nsi
der
gel
or
oil
for
lub
rica
tio
n.
‘Han
dson
orof
f?’If
the
wo
man
isin
con
tro
l,th
enth
ere
isp
ote
nti
alfo
rh
and
s
clo
sely
po
ised
inp
rep
arat
ion
toap
ply
pre
ssu
reif
hea
dad
van
ces
rap
idly
.U
se
gen
tle
pre
ssu
reo
nth
eh
ead
toco
ntr
ol
exp
uls
ive
forc
es,
sup
po
rtin
gei
ther
sid
eo
f
the
per
ineu
mw
ith
the
ind
exfi
ng
eran
d
thu
mb
,w
ith
the
seco
nd
han
dp
alm
ho
ldin
gp
ado
ver
the
anu
s.‘E
asin
g’
the
two
sid
esto
get
her
tocr
eate
som
esl
ack
inth
e
per
ineu
m,
ifn
eces
sary
.
‘Slo
w,
blow
and
brea
the
theb
aby
out.
En
sure
slo
wb
irth
of
the
hea
dw
hil
eth
e
wo
man
bre
ath
eso
rb
low
s,p
rovid
ing
eno
ug
hti
me
du
rin
gcr
ow
nin
gto
allo
wth
e
per
ineu
mto
stre
tch
slo
wly
and
full
y(5
or
mo
reco
ntr
acti
on
s,if
the
feta
lh
eart
is
sati
sfac
tory
),w
aiti
ng
for
sho
uld
ers
to
rota
te,
and
ease
up
off
the
per
ineu
m.
Fo
ur
core
them
esw
ere
iden
tifi
ed:
‘Cal
m,
con
tro
lled
bir
th’;
‘Po
siti
on
and
tech
niq
ues
inea
rly
seco
nd
stag
e’;
‘Han
ds
on
or
off
?’an
d‘S
low
,b
low
and
bre
ath
eth
eb
aby
ou
t.
Usi
ng
the
tech
niq
ues
des
crib
eden
able
d
thes
em
idw
ives
toac
hie
ve
rate
s,in
nu
llip
aro
us
wo
men
,o
f3
.91
%fo
r
epis
ioto
my,
59
.24
%fo
r‘n
osu
ture
s’,
and
1.0
8%
for
seri
ou
sla
cera
tio
ns
10
00
mid
wiv
essu
rvey
-
rou
tin
eh
an
ds
on
po
ised
Tro
chez
etal
.,2
01
1
UK
To
det
erm
ine
curr
ent
mid
wif
ery
pra
ctic
ein
En
gla
nd
wit
h
reg
ard
toth
em
anag
emen
to
f
the
per
ineu
md
uri
ng
the
late
seco
nd
stag
eo
fla
bo
ur
Ob
serv
atio
nal
po
stal
qu
esti
on
nai
re
Res
po
nse
rate
60
.7%
(n=
60
7)
����
To
esti
mat
eth
en
um
ber
of
mid
wiv
es
pra
ctic
ing
eith
er“h
and
so
n”
or
“han
ds
off
”
29
9(4
9.3
%,
95
%C
I4
5.2
–5
3.3
%)
mid
wiv
es
pre
ferr
edth
e“h
and
s-o
ff”
met
ho
d;
48
.6%
pre
ferr
ed“h
and
so
n”.
Les
s-ex
per
ien
ced
mid
wiv
es
wer
em
ore
lik
ely
top
refe
rth
e“h
and
so
ff”
(72
%v
s.4
1.4
%,
p<
0.0
01
).A
hig
her
pro
po
rtio
no
f
mid
wiv
esin
the
“han
ds-
off
”
gro
up
wo
uld
nev
erd
oan
epis
ioto
my
(37
.1%
vs.
24
.4%
,p
=0
.00
1)
for
ind
icat
ion
so
ther
than
feta
ld
istr
ess.
Mid
wiv
esin
the
UK
app
lyb
oth
met
ho
ds
of
han
ds
on
and
han
ds
off
the
per
ineu
m
du
rin
gth
ese
con
dst
age
of
lab
ou
r.
Wo
men
’sp
osi
tio
ns
du
rin
gse
con
dst
ag
eo
f
lab
ou
r
De
Jon
geetal
.,2
00
8
Net
her
lan
ds
To
exp
lore
the
vie
ws
of
mid
wiv
eso
nw
om
en’s
po
siti
on
sd
uri
ng
seco
nd
stag
e
of
lab
ou
r
Qu
alit
ativ
efo
cus
gro
up
s
6fo
cus
gro
up
sw
ith
pu
rpo
siv
e
sam
ple
of
31
ind
epen
den
t
pri
mar
yca
rem
idw
ives
fro
m
rura
l,se
mi-
urb
anan
du
rban
area
sfr
om
dif
fere
nt
par
tso
f
cou
ntr
yo
fv
ario
us
ages
and
edu
cati
on
alb
ack
gro
un
ds
Mo
der
ate
lev
elo
f
con
fid
ence
To
pic
gu
ide:
mid
wiv
es’ex
per
ien
cew
ith
bir
thin
gp
osi
tio
ns,
info
they
giv
eto
wo
men
abo
ut
po
siti
on
s,fa
cto
rsth
at
infl
uen
ceu
seo
fp
osi
tio
ns
and
kn
ow
led
ge
and
skil
lsis
assi
stin
gb
irth
sin
var
iou
s
po
siti
on
s
Info
rmed
con
sen
t/
cho
ice
Fac
tors
rela
ted
tog
ivin
gin
form
ed
con
sen
t
Wo
rkin
gco
nd
itio
ns
Ob
stet
ric
fact
ors
Mo
stu
seb
irth
ing
sto
ol
tho
ug
hri
sko
f
oed
ema
Qu
arte
rst
ated
all
of
last
10
bir
ths
wer
ein
sup
ine
po
siti
on
.
Giv
ing
wo
men
info
rmed
cho
ice
may
assi
st
them
inu
sin
gp
osi
tio
ns
that
are
mo
st
app
rop
riat
e.M
idw
ives
emp
has
ised
wo
men
sho
uld
be
pre
par
edth
atth
ep
roce
sso
f
bir
this
larg
ely
un
pre
dic
tab
le.
Eq
uip
men
t
for
no
n-s
up
ine
bir
ths
sho
uld
be
mo
re
mid
wif
efr
ien
dly
.
Infl
uen
ceo
fm
idw
ives
’w
ork
ing
con
dit
ion
so
nu
seo
fb
irth
ing
po
siti
on
s
was
imp
ort
ant
fact
or.
(Con
tinue
d)
PLOS ONE How midwives facilitate women to give birth during physiological second stage of labour?
PLOS ONE | https://doi.org/10.1371/journal.pone.0226502 July 28, 2020 7 / 19
Page 9
Ta
ble
2.
(Co
nti
nu
ed)
Mid
wiv
es’
pra
ctic
esA
uth
or,
yea
r
Co
un
try
Aim
of
the
stu
dy
Stu
dy
des
ign
Po
pu
lati
on
Gro
up
an
dsi
ze(n
)
(ag
e,p
ari
ty,
eth
nic
ity
,et
c.)
Qu
ali
tyo
f
stu
dy
(CA
SP
,
Cer
qu
al
an
d
GR
AD
E)
����
Hig
h
����
Mo
der
ate
����
Lo
w
����
Ver
yL
ow
Def
init
ion
sM
ain
com
po
nen
tsO
utc
om
esa
sses
sed
Eff
ects
on
ou
tco
mes
Co
mp
on
ents
ass
oci
ate
dw
ith
ou
tco
mes
Res
ult
sK
eyco
ncl
usi
on
sC
om
men
ts
Bir
thin
gp
osi
tio
ns
Bir
thin
gp
osi
tio
na
nd
per
inea
ld
am
ag
e
De
Jon
geetal
.,2
01
0
Net
her
lan
ds
To
exam
ine
the
asso
ciat
ion
bet
wee
nse
mi-
sitt
ing
and
sitt
ing
com
par
edw
ith
recu
mb
ent
po
siti
on
atth
eti
me
of
bir
than
dp
erin
eal
dam
age
Co
ho
rt(s
eco
nd
ary
anal
ysi
so
fR
CT
;n
ot
ran
do
mis
edfo
r
dif
fere
nt
po
siti
on
s)
Lo
wri
skw
om
en,
18
+
(n=
16
46
)
64
0p
rim
ipar
ou
s(3
9.3
%)
98
7m
ult
ips
(60
.7%
)
Mea
nag
en
ot
giv
en
����
Sem
isi
ttin
gw
asd
efin
edas
sitt
ing
on
a
bed
or
bir
thin
gst
oo
l;re
cum
ben
tw
as
def
ined
assu
pin
eo
rla
tera
l.
Per
inea
ld
amag
e
Over
all
epis
ioto
my
rate
22
.7%
.
43
.8%
1st
or
2n
dd
egre
ete
ar;
1.9
%3
rd
deg
ree
tear
,9
.3%
lab
ial
tear
.
92
2w
om
eng
ave
bir
thin
recu
mb
ent
po
siti
on
,6
05
sem
i-si
ttin
g,
11
9si
ttin
g.
Pri
mip
aro
us
wo
men
had
hig
her
chan
cefo
r
epis
ioto
my
[OR
1.9
9(1
.47
–2
.71
)]o
rla
bia
l
tear
s(O
R2
.44
(1.5
9–
3.7
4))
.
Wo
men
insi
ttin
gp
osi
tio
nw
ere
less
lik
ely
toh
ave
anep
isio
tom
y[O
R0
.29
(0.1
6–
0.5
4)]
and
mo
reli
kel
yto
hav
ea
per
inea
l
tear
[OR
1.8
3(1
.22
–2
.73
)];
Lo
ng
erd
ura
tio
no
f2
nd
stag
ew
as
asso
ciat
edw
ith
mo
reep
isio
tom
ies
[OR
8.0
2(4
.97
–1
2.9
5)]
;
No
dif
fere
nce
inin
tact
per
ineu
mra
tes
bet
wee
np
osi
tio
ng
rou
ps.
(Sem
i-)s
itti
ng
bir
thin
gp
osi
tio
nd
oes
no
t
nee
dto
be
dis
cou
rag
edto
pre
ven
tp
erin
eal
dam
age
(Sem
i-)s
itti
ng
bir
thin
gp
osi
tio
nd
oes
no
t
nee
dto
be
dis
cou
rag
edto
pre
ven
t
per
inea
ld
amag
e.
Lar
ger
stu
die
sn
eed
edto
exam
ine
dif
fere
nce
sin
OA
SIS
bet
wee
nd
iffe
ren
t
po
siti
on
gro
up
s
Wo
men
’sP
osi
tio
nin
the
seco
nd
sta
ge
Gu
pta
etal
.,2
01
7
To
det
erm
ine
the
po
ssib
le
ben
efit
san
dri
sks
of
the
use
of
dif
fere
nt
bir
thp
osi
tio
ns
du
rin
gth
ese
con
dst
age
of
lab
ou
rw
ith
ou
tep
idu
ral
anes
thes
ia,
on
mat
ern
al,
feta
l,
neo
nat
alan
dca
reg
iver
ou
tco
mes
.
Co
chra
ne
Rev
iew
30
tria
lsin
vo
lvin
g9
01
5
wo
men
����
An
yu
pri
gh
tp
osi
tio
nas
sum
edb
y
pre
gn
ant
wo
men
du
rin
gth
ese
con
dst
age
of
lab
ou
rco
mp
ared
wit
hsu
pin
eo
r
lith
oto
my
po
siti
on
s.
Du
rati
on
of
seco
nd
stag
eo
fla
bo
ur.
Sec
on
dar
yo
utc
om
esM
ater
nal
ou
tco
mes
:P
ain
,u
seo
fan
yan
alg
esia
,
mo
de
of
bir
th,
per
inea
ltr
aum
a,
epis
ioto
my
,b
loo
dlo
ss,
nee
dfo
rb
loo
d
tran
sfu
sio
n,
man
ual
rem
ov
alo
f
pla
cen
ta,
sho
uld
erd
yst
oci
a,u
rin
ary
or
faec
alin
con
tin
ence
.F
etal
ou
tco
mes
:
Ab
no
rmal
feta
lh
eart
rate
pat
tern
s,
adm
issi
on
toN
ICU
,p
erin
atal
dea
th.
Th
eu
pri
gh
tp
osi
tio
nw
asas
soci
ated
wit
ha
red
uct
ion
ind
ura
tio
no
fse
con
dst
age
in
the
up
rig
ht
gro
up
(MD
-6.1
6m
inu
tes,
95
%
CI
-9.7
4to
-2.5
9m
inu
tes;
no
clea
r
dif
fere
nce
inth
era
tes
of
caes
area
nse
ctio
n
(RR
1.2
2,
95
%C
I0
.81
to1
.81
);a
red
uct
ion
inas
sist
edd
eliv
erie
s(R
R0
.75
,9
5%
CI
0.6
6
to0
.86
)an
dep
isio
tom
ies
(RR
0.7
5,
95
%C
I
0.6
1to
0.9
2);
ap
oss
ible
incr
ease
inse
con
d
deg
ree
per
inea
lte
ars
(RR
1.2
0,
95
%C
I
1.0
0to
1.4
4);
no
clea
rd
iffe
ren
cein
the
nu
mb
ero
f3
rdo
r4
thd
egre
ep
erin
eal
tear
s
(RR
0.7
2,
95
%C
I0
.32
to1
.65
);in
crea
sed
esti
mat
edb
loo
dlo
ssg
reat
erth
an5
00
mL
(RR
1.4
8,
95
%C
I1
.10
to1
.98
);fe
wer
abn
orm
alfe
tal
hea
rtra
tep
atte
rns
(RR
0.4
6,
95
%C
I0
.22
to0
.93
);n
ocl
ear
dif
fere
nce
inth
en
um
ber
of
bab
ies
adm
itte
dto
NIC
U(R
R0
.79
,9
5%
CI
0.5
1
to1
.21
)
Th
efi
nd
ing
so
fth
isre
vie
wsu
gg
est
sever
alp
oss
ible
ben
efit
sfo
ru
pri
gh
t
po
stu
rein
wo
men
wit
ho
ut
epid
ura
l
anes
thes
ia,
such
asa
ver
ysm
all
red
uct
ion
inth
ed
ura
tio
no
fse
con
dst
age
of
lab
ou
r
(mai
nly
fro
mth
ep
rim
igra
vid
gro
up
),
red
uct
ion
inep
isio
tom
yra
tes
and
assi
sted
del
iver
ies.
Ho
wev
er,
ther
eis
an
incr
ease
dri
skb
loo
dlo
ssg
reat
erth
an5
00
mL
and
ther
em
ayb
ean
incr
ease
dri
sko
f
seco
nd
-deg
ree
tear
s,th
ou
gh
this
is
un
clea
r.In
vie
wo
fth
ev
aria
ble
risk
of
bia
so
fth
etr
ials
revie
wed
,fu
rth
ertr
ials
usi
ng
wel
l-d
esig
ned
pro
toco
lsar
en
eed
ed
toas
cert
ain
the
tru
eb
enef
its
and
risk
so
f
var
iou
sb
irth
po
siti
on
s.
Th
eo
ver
all
app
lica
bil
ity
of
the
up
rig
ht
po
siti
on
to
red
uce
the
du
rati
on
of
seco
nd
stag
ela
bo
ur
sho
uld
be
inte
rpre
ted
wit
hca
uti
on
.
Th
ese
mea
sure
sca
nfi
t
into
the
con
tex
to
f
curr
ent
pra
ctic
e,
esp
ecia
lly
wit
hre
gar
dto
info
rmin
gw
om
eno
f
thes
eri
sks
du
rin
gth
e
cou
nse
llin
gp
roce
ss.
Th
ree
del
iver
y
po
siti
on
so
np
ain
inte
nsi
tyd
uri
ng
the
seco
nd
sta
ge
of
lab
ou
r
Va
lia
nietal
.,2
01
6
Iran
To
inv
esti
gat
ean
dco
mp
are
the
sev
erit
yo
fd
eliv
ery
pai
n
thro
ug
hd
iffe
ren
tch
ild
bir
th
po
siti
on
sin
the
seco
nd
stag
e
of
del
iver
y.
Cli
nic
altr
ial
(ran
do
mis
atio
n
pro
ced
ure
no
t
des
crib
ed)
96
pri
mip
aro
us
wo
men
;m
ean
age
22
.31
(SD
2.9
7);
ges
tati
on
alag
eb
etw
een
37
and
42
wee
ks;
sin
gle
ton
pre
gn
ancy
;v
erte
x
po
siti
on
����
lith
oto
my
:th
em
oth
erw
asin
sup
ine
po
siti
on
wit
h3
0˚
hea
del
evat
ion
and
ben
t
kn
ees.
Sit
tin
gp
osi
tio
n:
mo
ther
sat
on
the
lab
or
chai
rw
ith
com
ple
tely
stra
igh
tlu
mb
ar
spin
e,h
ipan
dk
nee
join
tsat
the
sam
e
lev
el.
Sq
uat
tin
gp
osi
tio
n:
mo
ther
was
sitt
ing
on
her
feet
soth
ath
erso
lew
asin
tou
chw
ith
the
flo
or
and
the
kn
eejo
ints
wer
eh
igh
er
than
the
hip
s.
Pai
nse
ver
ity
mea
sure
db
yV
AS
and
McG
ill
PP
I
Inth
ela
ten
tp
has
eo
f2
nd
stag
eo
fla
bo
r,
pai
nse
ver
ity
bas
edo
nV
AS
and
McG
ill
was
sig
nif
ican
tly
less
insq
uat
tin
gan
d
lith
oto
my
gro
up
sco
mp
ared
tosi
ttin
g
po
siti
on
gro
up
(P=
0.0
01
).
Inth
eac
tiv
ep
has
eo
fse
con
dla
bo
rst
age,
pai
nse
ver
ity
bas
edo
nV
AS
and
McG
ill
was
less
inth
esq
uat
tin
gg
rou
pco
mp
ared
tosi
ttin
gan
d
lith
oto
my
po
siti
on
s(P
=0
.02
4).
Sq
uat
tin
gis
vie
wed
asan
easy
,ap
pli
cab
le
met
ho
dto
red
uce
pai
n2
nd
stag
ela
bo
ur.
Res
ult
ssu
gg
est
that
the
use
of
squ
atti
ng
po
siti
on
dec
reas
esp
ain
sev
erit
yin
the
seco
nd
stag
eo
fla
bo
r.
Itis
also
sug
ges
ted
toed
uca
teth
e
mo
ther
sco
nce
rnin
gal
l
chil
db
irth
po
siti
on
san
dle
tth
emse
lect
each
of
the
po
siti
on
s
vo
lun
tari
ly.
Fu
rth
erst
ud
ies
can
clar
ify
the
adv
anta
ges
and
dis
adv
anta
ges
of
all
po
siti
on
s.
No
n-p
ha
rma
colo
gic
al
pa
inre
lief
Hea
tth
era
py
on
pa
in
sev
erit
y
Fa
ha
mietal
.,2
01
1
Iran
To
asse
ssth
eef
fect
of
hea
t
ther
apy
on
pai
nse
ver
ity
in
pri
mig
rav
ida
wo
men
RC
TN
=6
4
Lo
wri
skn
ull
ipar
ou
sw
om
en
18
–3
5y
rs3
7–
41
wee
ks,
sin
gle
pre
gn
ancy
,ce
ph
alic
pre
sen
tati
on
.
Ris
ko
fse
lect
ion
bia
s:
sam
pli
ng
no
tcl
ear.
Ran
do
mis
atio
np
roce
du
ren
ot
des
crib
ed.
����
Use
of
ah
ot
wat
erb
ott
lew
ith
ast
eril
ized
wra
po
nw
om
an’s
per
ineu
m.
Pai
nse
ver
ity
mea
sure
db
yth
eM
cGil
l
pai
nli
nea
rsc
ale
Th
em
ean
sco
reo
fp
ain
sev
erit
yat
the
seco
nd
stag
eo
fla
bo
ur
sho
wed
a
sig
nif
ican
td
iffe
ren
ceb
etw
een
the
two
gro
up
s(p
0.0
00
)an
dw
aslo
wer
inth
eh
eat
ther
apy
gro
up
(8.2
5;
SD
1.3
9)
than
the
rou
tin
eca
reg
rou
p(9
.65
,S
D1
.99
)
Hea
tth
erap
yre
du
ces
the
lab
ou
rp
ain
.
Tra
nsc
uta
neo
us
elec
tric
ner
ve
stim
ula
tio
n(T
EN
S)
Sh
ah
oeietal
.,2
01
7a
Iran
To
inv
esti
gat
eth
eef
fect
of
tran
scu
tan
eou
sel
ectr
icn
erv
e
stim
ula
tio
no
nla
bo
rp
ain
in
2n
dst
age
RC
T
(Wo
men
wer
e
pla
ced
ino
ne
of
3
gro
up
s)
N=
90
3g
rou
ps
of
30
nu
llip
aro
us
wo
men
:T
EN
S,
pla
ceb
o-T
EN
S,
con
tro
l.
����
3g
rou
ps:
swit
ched
-on
TE
NS
,sw
itch
ed-
off
TE
NS
and
con
tro
l
Pai
nm
easu
red
on
aV
AS
du
rin
g2
nd
stag
e
Th
ese
ver
ity
of
pai
nw
aslo
wer
inth
e
TE
NS
gro
up
com
par
edw
ith
oth
erg
rou
ps
in2
nd
stag
eo
fla
bo
r(p
0.0
00
).N
oef
fect
so
n
chil
db
irth
.
TE
NS
isa
safe
met
ho
dfo
rp
ain
reli
ef
du
rin
gch
ild
bir
th
Ver
ylo
wn
um
ber
s
incl
ud
ed,
men
tio
ned
as
lim
itat
ion
inth
est
ud
y.
Pu
shin
gte
chn
iqu
es
(Con
tinue
d)
PLOS ONE How midwives facilitate women to give birth during physiological second stage of labour?
PLOS ONE | https://doi.org/10.1371/journal.pone.0226502 July 28, 2020 8 / 19
Page 10
Ta
ble
2.
(Co
nti
nu
ed)
Mid
wiv
es’
pra
ctic
esA
uth
or,
yea
r
Co
un
try
Aim
of
the
stu
dy
Stu
dy
des
ign
Po
pu
lati
on
Gro
up
an
dsi
ze(n
)
(ag
e,p
ari
ty,
eth
nic
ity
,et
c.)
Qu
ali
tyo
f
stu
dy
(CA
SP
,
Cer
qu
al
an
d
GR
AD
E)
����
Hig
h
����
Mo
der
ate
����
Lo
w
����
Ver
yL
ow
Def
init
ion
sM
ain
com
po
nen
tsO
utc
om
esa
sses
sed
Eff
ects
on
ou
tco
mes
Co
mp
on
ents
ass
oci
ate
dw
ith
ou
tco
mes
Res
ult
sK
eyco
ncl
usi
on
sC
om
men
ts
Pu
shin
g/b
eari
ng
do
wn
met
ho
ds
for
the
seco
nd
sta
ge
of
lab
ou
r
Lem
osetal
.,2
01
7
To
eval
uat
eth
eb
enef
its
and
po
ssib
led
isad
van
tag
eso
f
dif
fere
nt
kin
ds
of
tech
niq
ues
reg
ard
ing
mat
ern
alp
ush
ing
/
bre
ath
ing
du
rin
gth
eex
pu
lsiv
e
stag
eo
fla
bo
ur
on
mat
ern
al
and
feta
lo
utc
om
es.
Co
chra
ne
Rev
iew
7T
rial
s(o
ne
incl
ud
ing
wo
men
wit
han
epid
ura
l:L
ow
etal
.
20
13
)
On
lyp
rese
nti
ng
resu
lts
of
6
tria
lsw
ith
ou
tep
idu
ral
����
Sp
on
tan
eou
sver
sus
dir
ecte
dp
ush
ing
Du
rati
on
of
seco
nd
stag
e,
per
inea
lla
cera
tio
n,
adm
issi
on
toN
NIC
,
5m
inA
PG
AR
sco
re<
7,
Du
rati
on
of
pu
shin
g
Sp
on
tan
eou
sv
agin
ald
eliv
ery
No
clea
rd
iffe
ren
cein
the
du
rati
on
of
the
2n
dst
age
of
lab
ou
r(M
D1
0.2
6m
in(9
5%
CI
-1.1
2to
21
.64
min
).N
ocl
ear
dif
fere
nce
in3
rdo
r4
thd
egre
ep
erin
eal
lace
rati
on
(RR
0.8
7,
95
%C
I0
.45
to1
.66
),ep
isio
tom
y
(RR
1.0
5,
95
%C
I0
.60
to1
.85
),d
ura
tio
no
f
pu
shin
g(M
D-9
.76
min
ute
s,9
5%
CI
-19
.54
to0
.02
)o
rra
teo
fsp
on
tan
eou
s
vag
inal
del
iver
y(R
R1
.01
,9
5%
CI
0.9
7to
1.0
5).
No
dif
fere
nce
for
neo
nat
alo
utc
om
essu
ch
as5
’Ap
gar
sco
re<
7(R
R0
.35
;9
5%
CI
0.0
1to
8.4
3)
and
the
nu
mb
ero
f
adm
issi
on
sto
NIC
U(R
R1
.08
;9
5%
CI
0.3
0
to3
.79
)
No
sig
nif
ican
td
iffe
ren
cein
the
du
rati
on
of
the
seco
nd
stag
eo
fla
bo
ur
bet
wee
n
spo
nta
neo
us
and
dir
ecte
dp
ush
ing
.
Wo
man
’sp
refe
ren
cean
dco
mfo
rtan
d
clin
ical
con
tex
tsh
ou
ldg
uid
ed
ecis
ion
s.
On
lyp
rese
nti
ng
resu
lts
of
6tr
ials
wit
ho
ut
epid
ura
l
(nam
edco
mp
aris
on
1in
the
Co
chra
ne
revie
w).
On
etr
ial
Lo
wet
al.,
20
13
excl
ud
ed.
Del
ay
edp
ush
ing
in
late
ral
po
siti
on
Va
zirietal
.,2
01
6
Iran
To
com
par
eth
eef
fect
so
f
spo
nta
neo
us
pu
shin
gin
late
ral
po
siti
on
wit
hth
eV
alsa
lva
man
euv
ero
nm
ater
nal
and
feta
lo
utc
om
es
RC
T
(no
ITT
anal
yse
s)
N=
72
ran
do
miz
ed;
N=
69
anal
yse
d.
Nu
llip
aro
us
low
risk
wo
men
,
live
fetu
s,v
erte
xp
rese
nta
tio
n,
37
–4
0w
eek
ssp
on
tan
eou
s
lab
or.
Mea
nag
e2
2.2
(SD
4.3
3)
����
Inte
rven
tio
n:
pu
shin
gw
ith
the
urg
eto
pu
sh(d
elay
edp
ush
ing
)in
late
ral
po
siti
on
Co
ntr
ol:
pu
shin
gfo
rmb
egin
nin
go
ffu
ll
dil
atio
nu
sin
gV
alsa
lva,
sup
ine
po
siti
on
Inin
terv
enti
on
gro
up
:
Les
sp
ain
sever
ity
7.8
(SD
1.2
1)
vs
9.0
5(S
D
1.1
1);
p<
0.0
01
Fat
igu
esc
ore
46
.59
(SD
21
)vs
12
3.3
6(S
D
43
.20
);p<
0.0
01
Du
rati
on
of
2n
dst
age
76
.32
(SD
8.2
6)
vs
64
.56
(SD
15
.24
);p<
0.0
01
Du
rati
on
of
pu
shin
g4
9.1
4(S
D1
1.6
6)
vs
64
.56
(SD
15
.24
);p<
0.0
01
Sp
on
tan
eou
sp
ush
ing
inth
ela
tera
l
po
siti
on
red
uce
dd
ura
tio
no
fp
ush
ing
,
fati
gu
ean
dp
ain
sev
erit
y,
wit
ho
ut
affe
ctin
gn
eon
atal
ou
tco
mes
.
Op
tim
isin
gp
erin
eal
ou
tco
mes
(Con
tinue
d)
PLOS ONE How midwives facilitate women to give birth during physiological second stage of labour?
PLOS ONE | https://doi.org/10.1371/journal.pone.0226502 July 28, 2020 9 / 19
Page 11
Ta
ble
2.
(Co
nti
nu
ed)
Mid
wiv
es’
pra
ctic
esA
uth
or,
yea
r
Co
un
try
Aim
of
the
stu
dy
Stu
dy
des
ign
Po
pu
lati
on
Gro
up
an
dsi
ze(n
)
(ag
e,p
ari
ty,
eth
nic
ity
,et
c.)
Qu
ali
tyo
f
stu
dy
(CA
SP
,
Cer
qu
al
an
d
GR
AD
E)
����
Hig
h
����
Mo
der
ate
����
Lo
w
����
Ver
yL
ow
Def
init
ion
sM
ain
com
po
nen
tsO
utc
om
esa
sses
sed
Eff
ects
on
ou
tco
mes
Co
mp
on
ents
ass
oci
ate
dw
ith
ou
tco
mes
Res
ult
sK
eyco
ncl
usi
on
sC
om
men
ts
Per
inea
lte
chn
iqu
esfo
r
red
uci
ng
per
inea
l
tra
um
a
Aa
shei
metal
.,2
01
7
To
asse
ssth
eef
fect
of
per
inea
l
tech
niq
ues
du
rin
gth
ese
con
d
stag
eo
fla
bo
ur
on
the
inci
den
cean
dm
orb
idit
y
asso
ciat
edw
ith
per
inea
l
trau
ma.
Co
chra
ne
rev
iew
22
tria
lsw
ere
elig
ible
for
incl
usi
on
(wit
h2
0tr
ials
inv
olv
ing
15
,18
1w
om
en)
����
Per
inea
lte
chn
iqu
esd
uri
ng
the
seco
nd
stag
eo
fla
bo
ur
Th
ein
cid
ence
and
mo
rbid
ity
asso
ciat
edw
ith
per
inea
ltr
aum
a.
Han
ds
on
or
han
ds
off
the
per
ineu
mm
ade
no
clea
rd
iffe
ren
cein
inci
den
ceo
fin
tact
per
ineu
mR
R1
.03
,9
5%
CI
0.9
5to
1.1
2(2
stu
die
s,6
54
7w
om
en;
mo
der
ate-
qu
alit
y
evid
ence
),1
st-d
egre
ep
erin
eal
tear
sR
R
1.3
2,
95
%C
I0
.99
to1
.77
,2
stu
die
s,7
00
wo
men
;lo
w-q
ual
ity
evid
ence
),2
nd-d
egre
e
tear
s(R
R0
.77
,95
%C
I0
.47
to1
.28
,2
stu
die
s,7
00
wo
men
;lo
w-q
ual
ity
evid
ence
),
or
3rd
-o
r4
th-d
egre
ete
ars
(RR
0.6
8,
95
%
CI
0.2
1to
2.2
6,
5st
ud
ies,
73
17
wo
men
;
ver
ylo
w-q
ual
ity
evid
ence
).E
pis
ioto
my
was
mo
refr
equ
ent
inth
eh
and
s-o
ng
rou
p
(RR
0.5
8,9
5%
CI
0.4
3to
0.7
9,
4st
ud
ies,
72
47
wo
men
;lo
w-q
ual
ity
evid
ence
)
Aw
arm
com
pre
ssd
idn
ot
hav
ea
clea
r
effe
cto
nth
ein
cid
ence
of
inta
ctp
erin
eum
(RR
1.0
2,
95
%C
I0
.85
to1
.21
;1
79
9
wo
men
;4
stu
die
s;m
od
erat
e-q
ual
ity
evid
ence
),p
erin
eal
trau
ma
req
uir
ing
sutu
rin
g(R
R1
.14
,9
5%
CI
0.7
9to
1.6
6;
76
wo
men
;1
stu
dy;
ver
ylo
w-q
ual
ity
evid
ence
),1
st-d
egre
ete
ars
(RR
1.1
9,
95
%
CI
0.3
8to
3.7
9;
27
4w
om
en;
2st
ud
ies;
ver
y
low
-qu
alit
yev
iden
ce),
2n
d-d
egre
ete
ars
(RR
0.9
5,
95
%C
I0
.58
to1
.56
;2
74
wo
men
;
2st
ud
ies;
ver
ylo
w-q
ual
ity
evid
ence
),o
r
epis
ioto
my
(RR
0.8
6,
95
%C
I0
.60
to1
.23
;
17
99
wo
men
;4
stu
die
s;lo
w-q
ual
ity
evid
ence
).F
ewer
thir
d-
or
fou
rth
-deg
ree
per
inea
lte
ars
wer
ere
po
rted
inth
ew
arm
-
com
pre
ssg
rou
p(R
R0
.46
,9
5%
CI
0.2
7to
0.7
9;
17
99
wo
men
;4
stu
die
s;m
od
erat
e-
qu
alit
yev
iden
ce).
Per
inea
lm
assa
ge
incr
ease
dth
ein
cid
ence
of
inta
ctp
erin
eum
(RR
1.7
4,
95
%C
I1
.11
to2
.73
,6
stu
die
s,2
61
8w
om
en;
low
-qu
alit
y
evid
ence
and
sub
stan
tial
het
ero
gen
eity
bet
wee
nst
ud
ies)
.P
erin
eal
mas
sag
e
dec
reas
edth
ein
cid
ence
of
3rd
or
4th
-
deg
ree
tear
s(R
R0
.49
,9
5%
CI
0.2
5to
0.9
4,
5st
ud
ies,
24
77
wo
men
;m
od
erat
e-q
ual
ity
evid
ence
).N
ocl
ear
effe
cto
np
erin
eal
trau
ma
req
uir
ing
sutu
rin
g(R
R1
.10
,9
5%
CI
0.7
5to
1.6
1,
1st
ud
y,
76
wo
men
;ver
y
low
-qu
alit
yev
iden
ce),
1st
-deg
ree
tear
s(R
R
1.5
5,
95
%C
I0
.79
to3
.05
,5
stu
die
s,5
37
wo
men
;ver
ylo
w-q
ual
ity
evid
ence
),o
r2
nd-
deg
ree
tear
s(R
R1
.08
,9
5%
CI
0.5
5to
2.1
2,
5st
ud
ies,
53
7w
om
en;
ver
ylo
w-q
ual
ity
evid
ence
).P
erin
eal
mas
sag
em
ayre
du
ce
epis
ioto
my
(RR
0.5
5,
95
%C
I0
.29
to1
.03
,
7st
ud
ies,
26
84
wo
men
;ver
ylo
w-q
ual
ity
evid
ence
).
On
est
ud
y(6
6w
om
en)
fou
nd
that
wo
men
rece
ivin
gR
itg
en’s
man
oeu
vre
wer
ele
ss
lik
ely
toh
ave
a1
st-d
egre
ete
ar(R
R0
.32
,
95
%C
I0.1
4to
0.6
9;
ver
ylo
w-q
ual
ity
evid
ence
),m
ore
lik
ely
toh
ave
a2
nd-d
egre
e
tear
(RR
3.2
5,
95
%C
I1
.73
to6
.09
;ver
y
low
-qu
alit
yev
iden
ce),
and
no
dif
fere
nce
on
inta
ctp
erin
eum
(RR
0.1
7,
95
%C
I0
.02
to1
.31
;ver
ylo
w-q
ual
ity
evid
ence
).O
ne
larg
erst
ud
yre
po
rted
that
Rit
gen
’s
man
oeu
vre
did
no
th
ave
anef
fect
on
inci
den
ceo
f3
rd-
or
4th
-deg
ree
tear
s(R
R
1.2
4,
95
%C
I0
.78
to1
.96
,14
23
wo
men
;
low
-qu
alit
yev
iden
ce).
Ep
isio
tom
yw
asn
ot
clea
rly
dif
fere
nt
bet
wee
ng
rou
ps
(RR
0.8
1,
95
%C
I0
.63
to1
.03
,tw
ost
ud
ies,
14
89
wo
men
;lo
w-q
ual
ity
evid
ence
).
Oth
erco
mp
aris
on
s:D
eliv
ery
of
po
ster
ior
ver
sus
ante
rio
rsh
ou
lder
firs
t,u
seo
fa
per
inea
lp
rote
ctio
nd
evic
e,d
iffe
ren
to
ils/
wax
,an
dco
ldco
mp
ress
esd
idn
ot
sho
w
any
effe
cts
on
ou
tco
mes
wit
hth
eex
cep
tio
n
of
incr
ease
din
cid
ence
of
inta
ctp
erin
eum
wit
hth
ep
erin
eal
dev
ice.
On
lyo
ne
stu
dy
con
trib
ute
dto
each
of
thes
eco
mp
aris
on
s.
Mo
der
ate-
qu
alit
yev
iden
cesu
gg
ests
that
war
mco
mp
ress
es,
and
mas
sag
e,m
ay
red
uce
thir
d-
and
fou
rth
-deg
ree
tear
sb
ut
the
imp
act
of
thes
ete
chn
iqu
eso
no
ther
ou
tco
mes
was
un
clea
ro
rin
con
sist
ent.
Po
or-
qu
alit
yev
iden
cesu
gg
ests
han
ds-
off
tech
niq
ues
may
red
uce
epis
ioto
my
,b
ut
this
tech
niq
ue
had
no
clea
rim
pac
to
n
oth
ero
utc
om
es.
Th
ere
wer
ein
suff
icie
nt
dat
ato
sho
ww
het
her
oth
erp
erin
eal
tech
niq
ues
resu
ltin
imp
rov
edo
utc
om
es.
Fo
rre
sult
sh
and
s-o
n
han
ds-
off
:S
ub
stan
tial
het
ero
gen
eity
for
thir
d-
or
fou
rth
-deg
ree
tear
s
mea
ns
thes
ed
ata
sho
uld
be
inte
rpre
ted
wit
h
cau
tio
n.
Res
ult
sm
assa
ge:
Het
ero
gen
eity
was
hig
h
for
firs
t-d
egre
ete
ar,
seco
nd
-deg
ree
tear
and
for
epis
ioto
my—
dat
a
sho
uld
be
inte
rpre
ted
wit
hca
uti
on
.
(Con
tinue
d)
PLOS ONE How midwives facilitate women to give birth during physiological second stage of labour?
PLOS ONE | https://doi.org/10.1371/journal.pone.0226502 July 28, 2020 10 / 19
Page 12
Ta
ble
2.
(Co
nti
nu
ed)
Mid
wiv
es’
pra
ctic
esA
uth
or,
yea
r
Co
un
try
Aim
of
the
stu
dy
Stu
dy
des
ign
Po
pu
lati
on
Gro
up
an
dsi
ze(n
)
(ag
e,p
ari
ty,
eth
nic
ity
,et
c.)
Qu
ali
tyo
f
stu
dy
(CA
SP
,
Cer
qu
al
an
d
GR
AD
E)
����
Hig
h
����
Mo
der
ate
����
Lo
w
����
Ver
yL
ow
Def
init
ion
sM
ain
com
po
nen
tsO
utc
om
esa
sses
sed
Eff
ects
on
ou
tco
mes
Co
mp
on
ents
ass
oci
ate
dw
ith
ou
tco
mes
Res
ult
sK
eyco
ncl
usi
on
sC
om
men
ts
Per
inea
lh
eati
ng
pa
ds
Ali
ho
ssen
ietal
.,2
01
8
Iran
To
det
erm
ine
the
effe
cto
f
per
inea
lh
eati
ng
pad
on
the
freq
uen
cyo
fep
isio
tom
ies
and
per
inea
lte
ars
inp
rim
ipar
ou
s
fem
ales
.
Sin
gle
bli
nd
clin
ical
tria
l
11
4p
rim
ipar
ou
sw
om
en
recr
uit
ed,
con
clu
din
gw
ith
54
inte
rven
tio
nan
d5
3co
ntr
ol
in
gro
up
Ag
e1
8–
35
yea
rs
Sin
gle
ton
,te
rmp
reg
nan
cies
����
Ah
eate
dp
adw
asp
lace
do
nth
eex
tern
al
reg
ion
of
the
per
ineu
m.
Itw
asp
lace
do
nth
ep
erin
eum
atth
est
art
of
the
seco
nd
stag
eo
fla
bo
r,b
yth
e
trai
ned
mid
wif
ean
dre
mo
ved
fro
mth
e
per
ineu
md
uri
ng
the
mo
ther
’str
ansf
erto
the
lab
ou
rro
om
.
Th
eef
fect
of
the
per
inea
lh
eati
ng
pad
on
the
freq
uen
cyo
fep
isio
tom
ies
and
per
inea
lte
ars.
Th
ere
sult
ssh
ow
eda
sig
nif
ican
td
iffe
ren
ce
bet
wee
nth
etw
og
rou
ps
inte
rms
of
the
epis
ioto
my
rate
(41
%v’s
21
%,
p=
0.0
25
).
Th
ere
was
no
sig
nif
ican
td
iffe
ren
ce
bet
wee
nth
etw
og
rou
ps
inte
rms
of
freq
uen
cyo
ffi
rst
and
seco
nd
-deg
ree
tear
s,
wit
hth
efi
rst
deg
ree
tear
sb
ein
go
bse
rved
amo
ng
13
(24
.1%
)an
d1
4w
om
en(2
6.4
%)
of
the
con
tro
lan
din
terv
enti
on
gro
up
s,
resp
ecti
vel
y.
Th
efr
equ
ency
of
seco
nd
-
deg
ree
tear
sin
the
con
tro
lan
d
inte
rven
tio
ng
rou
ps
was
nin
e(1
6.7
%)
and
sev
en(1
3.2
%),
resp
ecti
vel
y.
Th
ere
was
no
fou
rth
-deg
ree
tear
inea
chg
rou
p.
Th
ere
sult
so
fth
ecu
rren
tst
ud
yre
vea
led
that
the
use
of
per
inea
lh
eati
ng
pad
du
rin
gth
ese
con
dst
age
of
lab
or
can
be
effe
ctiv
ein
dec
reas
ing
the
epis
ioto
my
rate
(sta
tist
ical
lysi
gn
ific
ant)
and
inta
ct
per
ineu
m(t
ho
ug
hn
ot
stat
isti
call
y
sig
nif
ican
t)in
pri
mip
aro
us
wo
men
.
Th
ere
sult
so
fth
isst
ud
y
hav
eto
be
inte
rpre
ted
care
full
yb
ecau
seo
fth
e
ver
ylo
wq
ual
ity
of
the
stu
dy.
Per
inea
lm
ass
ag
e
du
rin
gla
bo
ur:
a
syst
ema
tic
rev
iew
an
d
met
a-a
na
lysi
so
f
ran
do
miz
edco
ntr
oll
ed
tria
ls
Aq
uin
oetal
.,2
01
8
To
eval
uat
ew
het
her
per
inea
l
mas
sag
ete
chn
iqu
esd
uri
ng
vag
inal
del
iver
yd
ecre
ases
the
risk
of
per
inea
ltr
aum
a.
Asy
stem
atic
rev
iew
and
met
a-an
aly
sis
of
ran
do
mis
ed
con
tro
lled
tria
ls
Nin
eR
CT
sre
po
rtin
go
n3
,37
4
wo
men
����
Per
inea
lm
assa
ge
du
rin
gth
ese
con
dst
age
of
lab
ou
r(w
ith
or
wit
ho
ut
the
use
of
wat
er-s
olu
ble
lub
rica
nt)
Pri
mar
yo
utc
om
e:S
ever
ep
erin
eal
trau
ma.
Sec
on
dar
yo
utc
om
esw
ere
inci
den
ces:
of
epis
ioto
my
,fi
rst,
and
seco
nd
-deg
ree
tear
and
inta
ctp
erin
eum
.
Wo
men
ran
do
mis
edto
rece
ive
per
inea
l
mas
sag
ed
uri
ng
seco
nd
stag
eo
fla
bo
ur
had
asi
gn
ific
antl
ylo
wer
inci
den
ceo
fse
ver
e
per
inea
ltr
aum
a,co
mp
ared
toth
ose
wh
o
did
no
t(R
R0
.49
,9
5%
CI
0.2
5–
0.9
4).
All
the
seco
nd
ary
ou
tco
mes
wer
en
ot
sig
nif
ican
t,ex
cep
tfo
rth
ein
cid
ence
of
inta
ctp
erin
eum
,w
hic
hw
assi
gn
ific
antl
y
hig
her
inth
ep
erin
eal
mas
sag
eg
rou
p(R
R
1.4
0,
95
%C
I1
.01
–1
.93
),an
dfo
rth
e
inci
den
ceo
fep
isio
tom
yw
hic
hw
as
sig
nif
ican
tly
low
erin
the
per
inea
lm
assa
ge
gro
up
(RR
0.5
6,
95
%C
I0
.38
–0
.82
).
Per
inea
lm
assa
ge
du
rin
gla
bo
ur
is
asso
ciat
edw
ith
sig
nif
ican
tlo
wer
risk
of
sev
ere
per
inea
ltr
aum
a,su
chas
thir
d-
and
fou
rth
-deg
ree
tear
san
dep
isio
tom
y.
Per
inea
lm
assa
ge
was
usu
ally
do
ne
by
a
mid
wif
ein
the
seco
nd
stag
eo
fla
bo
ur
du
rin
go
rb
etw
een
con
trac
tio
ns
and
du
rin
gp
ush
ing
tim
e,w
ith
the
ind
exo
r
mid
dle
fin
ger
,u
sin
ga
wat
er-s
olu
ble
lub
rica
nt.
Wa
rmp
erin
eal
com
pre
sses
du
rin
gth
e
seco
nd
sta
ge
of
lab
ou
r
for
red
uci
ng
per
inea
l
tra
um
a
Ma
go
gaetal
.,2
01
9
To
eval
uat
eth
eef
fect
iven
ess
of
war
mco
mp
ress
esd
uri
ng
the
seco
nd
stag
eo
fla
bo
ur
in
red
uci
ng
per
inea
ltr
aum
a
Asy
stem
atic
rev
iew
and
met
a-an
aly
sis
of
ran
do
miz
ed
con
tro
lled
tria
ls
Sev
entr
ials
,in
clu
din
g2
10
3
wo
men
����
Wo
men
assi
gn
edto
the
inte
rven
tio
n
gro
up
rece
ived
war
mco
mp
ress
es,
imm
erse
din
war
mta
pw
ater
.T
hes
ew
ere
hel
dag
ain
stth
ew
om
an’s
per
ineu
m
du
rin
gan
din
bet
wee
np
ush
esin
seco
nd
stag
e.W
arm
com
pre
sses
usu
ally
star
ted
wh
enth
eb
aby
’sh
ead
beg
anto
dis
ten
d
the
per
ineu
mo
rw
hen
ther
ew
asac
tiv
e
feta
ld
esce
nt
inth
ese
con
dst
age
of
lab
ou
r.
Th
ein
cid
ence
of
per
inea
ltr
aum
aA
hig
her
rate
of
inta
ctp
erin
eum
inth
e
inte
rven
tio
ng
rou
pco
mp
ared
toth
e
con
tro
lg
rou
p(2
2.4
%vs
15
.4%
;R
R1
.46
,
95
%C
I1
.22
to1
.74
);a
low
erra
teo
fth
ird
deg
ree
tear
s(1
.9%
vs
5.0
%;
RR
0.3
8,
95
%
CI
0.2
2to
0.6
4),
fou
rth
deg
ree
tear
s(0
.0%
vs
0.9
%;
RR
0.1
1,
95
%C
I0
.01
to0
.86
)
thir
dan
dfo
urt
hd
egre
ete
ars
com
bin
ed
(1.9
%v
s5
.8%
;R
R0
.34
,9
5%
CI
0.2
0to
0.5
6)
and
epis
ioto
my
(10
.4%
vs
17
.1%
;R
R
0.6
1,
95
%C
I0
.51
to0
.74
).
War
mco
mp
ress
esap
pli
edd
uri
ng
the
seco
nd
stag
eo
fla
bo
ur
incr
ease
the
inci
den
ceo
fin
tact
per
ineu
man
dlo
wer
the
risk
of
epis
ioto
my
and
sever
ep
erin
eal
trau
ma.
Ha
nd
s-o
nv
ersu
s
ha
nd
s-o
ffte
chn
iqu
es
for
the
pre
ven
tio
no
f
per
inea
ltr
au
ma
du
rin
g
va
gin
al
del
iver
y
Pie
rce-
Wil
lia
msetal
.,2
01
9
To
eval
uat
ew
het
her
ah
and
s-
on
tech
niq
ue
du
rin
gv
agin
al
del
iver
yre
sult
sin
less
inci
den
ceo
fp
erin
eal
trau
ma
than
ah
and
s-o
ffte
chn
iqu
e
Asy
stem
atic
rev
iew
and
met
a-an
aly
sis
of
ran
do
miz
ed
con
tro
lled
tria
ls
Fiv
eR
CT
sre
po
rtin
go
n7
,28
7
wo
men
����
Han
ds-
on
tech
niq
ue
ver
us
han
ds-
off
du
rin
gv
agin
ald
eliv
ery
Pri
mar
yo
utc
om
e:S
ever
ep
erin
eal
trau
ma
def
ined
asth
ird
-o
rfo
urt
h-
deg
ree
lace
rati
on
s.
Wo
men
ran
do
miz
edto
the
han
ds-
on
tech
niq
ue
had
sim
ilar
inci
den
ceo
fse
ver
e
per
inea
ltr
aum
a(1
.5ver
sus
1.3
%;
RR
2.0
0,
95
%C
I0
.56
–7
.15
).T
her
ew
asn
o
sig
nif
ican
tb
etw
een
-gro
up
dif
fere
nce
in
the
inci
den
ceo
fin
tact
per
ineu
m,
firs
t-,
seco
nd
-an
dfo
urt
h-d
egre
ela
cera
tio
n.
Han
ds-
on
tech
niq
ue
was
asso
ciat
edw
ith
incr
ease
dri
sko
fth
ird
-deg
ree
lace
rati
on
s
(2.6
ver
sus
0.7
%;
RR
3.4
1,
95
%C
I1
.39
–
8.3
7)
and
of
epis
ioto
my
(13
.6v
ersu
s9
.8%
,
RR
1.5
9,
95
%C
I1
.14
–2
.22
)co
mp
ared
to
the
han
ds-
off
tech
niq
ue.
Han
ds-
on
tech
niq
ue
du
rin
gsp
on
tan
eou
s
vag
inal
del
iver
yo
fsi
ng
leto
ng
esta
tio
ns
resu
lts
insi
mil
arin
cid
ence
of
sever
al
per
inea
ltr
aum
asco
mp
ared
toa
han
ds-
off
tech
niq
ue.
Th
ein
cid
ence
of
thir
d-
deg
ree
lace
rati
on
san
do
fep
isio
tom
y
incr
ease
sw
ith
the
han
ds-
on
tech
niq
ue.
Over
all
the
resu
lts
are
sim
ilar
toA
ash
eim
etal
.,
(20
17
)
exce
pt
for
the
risk
of
thir
d-d
egre
ela
cera
tio
ns.
Th
eef
fect
of
per
inea
l
ma
ssa
ge
du
rin
g2
nd
sta
ge
of
lab
ou
ro
n
nu
llip
aro
us
wo
men
per
ineu
m
Sh
ah
oeietal
.,2
01
7b
Iran
To
det
erm
ine
the
effe
cto
f
per
inea
lm
assa
ge
inth
e2
nd
stag
eo
fla
bo
ro
np
erin
eal
lace
rati
on
s,ep
isio
tom
y,
and
per
inea
lp
ain
inn
ull
ipar
ou
s
wo
men
.
RC
TN
=1
90
nu
llip
aro
us
wo
men
;
38
–4
2w
eek
s,si
ng
leto
n,
ver
tex
po
siti
on
,
����
Per
inea
lm
assa
ge
of
30
min
du
rin
g2
nd
stag
e
Rat
eo
fep
isio
tom
yan
dp
erin
eal
lace
rati
on
seco
nd
ary
ou
tco
mes
wer
eco
mp
aris
on
of
per
inea
lp
ain
afte
r3
day
s,1
0d
ays,
and
3m
on
ths
afte
rch
ild
bir
th.
Ep
isio
tom
yra
tew
as6
9.4
7%
inth
e
inte
rven
tio
ng
rou
pan
d9
2.3
1%
inth
e
con
tro
lg
rou
p(p<
0.0
5).
Th
ere
sult
s
revea
led
23
.2%
of
1st
and
2.1
%o
f2
nd-
deg
ree
per
inea
lla
cera
tio
nin
the
inte
rven
tio
ng
rou
p,
and
no
ves
tib
ula
r
lace
rati
on
or
3rd
-an
d4
th-d
egre
e
lace
rati
on
sin
the
inte
rven
tio
ng
rou
p.
Th
ere
wer
e5
.1%
of
ves
tib
ula
rla
cera
tio
n,
7.7
%o
f1
st-d
egre
ela
cera
tio
n,
2.6
%o
f2
nd-
deg
ree
lace
rati
on
,an
d1
.1%
of
3rd
deg
ree
lace
rati
on
inth
eco
ntr
ol
gro
up
.
Co
mp
aris
on
of
po
stp
artu
mp
ain
sho
wed
that
the
sever
ity
of
pai
n3
day
san
d3
mo
nth
saf
ter
chil
db
irth
was
sig
nif
ican
t
low
erin
the
inte
rven
tio
ng
rou
p(p
=0
.01
,
p=
0.0
08
,re
spec
tivel
y),
the
sever
ity
of
pai
n
on
the
10
thd
ayd
idn
ot
dif
fer
sig
nif
ican
tly
(p=
0.7
8)
Per
inea
lm
assa
ge
du
rin
gth
ese
con
dst
age
of
lab
ou
rca
nre
du
ceth
en
eed
for
epis
ioto
my,
and
avo
idp
erin
eal
inju
ries
,
and
per
inea
lp
ain
.
NIC
U:n
eon
atal
inte
nsi
ve
care
un
it;M
D:m
ean
dif
fere
nce
;OR
:O
dd
sra
tio
;R
R:re
lati
ve
risk
;C
I:co
nfi
den
cein
terv
al;V
AS
:vis
ual
anal
og
ue
scal
e;O
AS
IS:o
bst
etri
can
alsp
hin
cter
inju
ries
;T
EN
S:
tran
scu
tan
eou
sel
ectr
ical
ner
ve
stim
ula
tio
n;
SD
:st
and
ard
dev
iati
on
htt
ps:
//doi.o
rg/1
0.1
371/jo
urn
al.p
one.
0226502.t002
PLOS ONE How midwives facilitate women to give birth during physiological second stage of labour?
PLOS ONE | https://doi.org/10.1371/journal.pone.0226502 July 28, 2020 11 / 19
Page 13
Less-experienced midwives were more likely to prefer the “hands off” (72% vs. 41.4%,
p<0.001). A higher proportion of midwives in the “hands-off” group would never do an episi-
otomy (37.1% vs. 24.4%, p = 0.001) for indications other than fetal distress.
A further study explored the views of 31 midwives in the Netherlands, in relation to facili-
tating women’s birthing positions during the second stage of labour [38]. This qualitative
study utilised six focus groups to collate the data, which were interpreted using Thachuk’s
approach [39]. Thachuk’s work defines how women are involved in decision making in differ-
ent maternity care models; for example, the medical model of informed consent in comparison
to the midwifery model of informed choice. The influence of midwives’ working conditions
on the use of birthing positions was an important factor in this study, in particular midwives
who conformed to the medical philosophy of care. When asked, 8 (26%) midwives reported
that all of the last 10 births they had facilitated was with the woman in the supine position, an
additional 6 (19%) midwives stated 8 out of the last 10 were also supine. Midwives suggested
that equipment for non-supine births should be more user-friendly. The birth positions mid-
wives preferred were also influenced by their exposure during their initial education and expe-
rience during their career. This study acknowledged that giving women informed choice may
assist them in using positions that are most appropriate [38].
Begley et al., conducted a focus group study in Ireland and New Zealand among 21 expert
midwives to explore techniques used by expert midwives to preserve the perineum intact [37].
In this study a midwife was defined as an “expert” as her practice reflected an episiotomy rate
of less than 11.8% (the mean rate from all New Zealand and Irish Midwife-led Unit data com-
bined), rate of women in their care who have an intact perineum of more than 40%, their ‘no
suture’ rate (combination of the number of women with first degree tears that did not require
sutures), and a rate of less than 3.2% for serious perineal tears (or one third/fourth degree tear)
in the previous 3.5 years of practice. Four core themes were identified: ‘Calm, controlled birth’,
‘Position and techniques in early second stage’, ‘Hands on or off?’ and ‘Slow, blow and breathe
the baby out.’ Using the techniques described enabled these midwives to achieve rates, in nul-
liparous women, of 3.91% for episiotomy, 59.24% for ‘no sutures’, and 1.08% for serious
lacerations.
Themes
The remainder of the included studies were primarily intervention studies highlighting evi-
dence-based aspects of midwifery practice during the second stage of labour, with the potential
of informing future practice. These empirical findings were synthesised into four main themes
namely: birthing positions, non-pharmacological pain relief, pushing techniques and optimis-
ing perineal outcomes.
Birthing positions. The use of a squatting position is reported to decrease pain severity in
the second stage of labour, thus positively affecting labour pain reduction for women. In addi-
tion, squatting is viewed as an easy, applicable method to reduce pain during the second stage
of labour [32]. Primiparous women who adopt a sitting position are less likely to have an episi-
otomy and more likely to have a perineal tear [24, 34] with no clear difference however,
reported in the number of 3rd or 4th degree perineal tears [24]. It is acknowledged that women
should not be discouraged from adopting (semi-)sitting birthing positions to prevent perineal
damage. Notably, longer duration of second stage was associated with more women experienc-
ing episiotomies [34]. The upright position is, nonetheless, associated with a reduction in
duration of second stage. If progress in labour is slower, then variation in position should be
considered, particularly if the woman is in the supine position. Magnetic resonance (MR)
PLOS ONE How midwives facilitate women to give birth during physiological second stage of labour?
PLOS ONE | https://doi.org/10.1371/journal.pone.0226502 July 28, 2020 12 / 19
Page 14
pelvimetry also showed that an upright birthing position significantly expands the female pel-
vic bony dimensions, suggesting facilitation of labour and birth [34].
Non-pharmacological pain relief. Two studies described methods of non-pharmacologi-
cal pain relief adopted by midwives [29, 30]. A randomised sterilized control trial, using a heat
pack (hot water bottle) during the second stage, with a sterilized wrap placed on the woman’s
perineum for a minimum of five minutes. Pain was assessed using the McGill Pain linear scale
during immediately following birth to assess the pain level during the second stage of labour.
The mean score of pain severity relating to the second stage of labour showed a statistically sig-
nificant difference between the two groups (p 0.000) and was lower in the heat therapy group
than the routine care group [29]. The effect of transcutaneous electrical nerve stimulation
(TENS) on the severity of pain during labour in primiparous women was examined [30]. The
findings indicated the severity of pain during the second stage of labour was lower in the
TENS group compared with the placebo and control groups (p = 0.000).
Pushing techniques. During normal physiological birth, when the cervix is fully dilated
and/or the fetal head is on the pelvic floor, the mother will feel the urge to push and aided with
expulsive contractions maternal pushing will lead to the birth of the baby. In the literature two
different techniques of pushing are described: directed, coached, or Valsalva pushing with
physiological or spontaneous pushing: Valsalva and physiological or spontaneous pushing.
Directed pushing according to the Valsalva technique is repeated, prolonged breath holding
and bearing down which causes the glottis to close and increases intrathoracic pressure. Pre-
dominantly resulting in closed glottis pushing for 3 to 4 times during each contraction. Physio-
logical or spontaneous pushing is defined as full dilatation of the cervix and commencement of
pushing only when women feel the urge to push. No specific instructions are given about tim-
ing and duration; mostly resulting in non-directed, multiple short pushes, with no sustained
breath holding [25].
Studies comparing these two techniques have been primarily concerned with the effect of
pushing style on neonatal acid-base status and/or the length of second stage. Some studies
have directly addressed the relationship between the pushing method and perineal or pelvic
floor injury or have included it in their analyses. The Cochrane review by Lemos et al., [25]
found a mean reduction in the duration of second stage of labour by ten minutes and less third
or fourth degree perineal tears, however, these results were not statistically significant and no
conclusive (Table 1). A study by Vaziri et al., [33] compared spontaneous pushing with the
urge to push (delayed pushing) in lateral position with immediate pushing (from the begin-
ning of full dilation) using Valsalva in supine position. This study concluded that spontaneous
pushing in the lateral position reduced duration of pushing, fatigue and pain severity, without
affecting neonatal outcomes [33]. While the Cochrane review authors [25] highlighted their
inability to report which technique of pushing is best for the mother or baby, the spontaneous
pushing technique was found by Vaziri et al., [33] to be a safe method without causing any
harm to the baby.
Optimising perineal outcomes. There are two main maternity care options to guide the
birth of the fetal head, the hands-on or the hands-off (ordinarily with hands-poised) method.
The hands-on method aims to prevent severe perineal tears by supporting the perineum dur-
ing fetal crowning. The other hand is placed on the fetal head and the mother is asked to with-
hold from pushing, aiming to control the speed of the birth of the head. Lateral flexion of the
fetal head is applied to facilitate delivery of the shoulders. With the hands-off (or hands-
poised) method the hands do not touch the perineum or fetal head, allowing spontaneous
delivery of the head and the shoulders; and the woman is guided in controlled pushing.
A Cochrane review by Aasheim et al. [22] found that hands-on or hands-off the perineum
showed no clear supporting evidence in the incidence of intact perineum, first degree perineal
PLOS ONE How midwives facilitate women to give birth during physiological second stage of labour?
PLOS ONE | https://doi.org/10.1371/journal.pone.0226502 July 28, 2020 13 / 19
Page 15
tears, second degree tears or third- or fourth-degree tears. However, episiotomy was per-
formed more frequently in the hands-on group. A recent systematic review by Pierce-Williams
et al., showed almost similar results. Hands-on technique during spontaneous vaginal delivery
of singleton gestations resulted in similar incidence of several perineal traumas compared to a
hands-off technique. However, the incidence of third-degree lacerations and of episiotomy
increases with the hands-on technique [27].
According to the Cochrane review by Aasheim et al. supporting the perineum with a warm
cloth or compress did not have a clear effect on the incidence of intact perineum, perineal
trauma requiring suturing, first degree tears, second degree tears or episiotomy. However,
fewer third or fourth-degree tears were reported in the warm-compress group [22]. A recent
systematic review of Magoga et al., however, showed that warm compresses applied during the
second stage of labour increases the incidence of intact perineum and lower the risk of episiot-
omy and severe perineal trauma. This systematic review included seven trials reporting on
2,103 women. This study showed that the use of a perineal heating pad during the second stage
of labour can be effective in decreasing the episiotomy rate in primiparous women [26]. These
results are consistent with the study of Alihosseni et al. [28].
Perineal massage during labour is usually done in the second stage, during or between con-
tractions and during pushing time, with the index and middle fingers, using a water-soluble
lubricant. The purpose of this technique is to gently stretch the perineum from side to side.
Perineal massage increased the incidence of intact perineum and decreased the incidence of
third- or fourth-degree tears. Perineal massage had no clear effect on first or second degree
suturing, however, it may reduce episiotomy [22] A further study examined the effectiveness
of perineal massage [31] showing that in primiparous women a perineal massage of 30 minutes
during the second stage of labour reduced the episiotomy rate (69% in the massage group, and
92% in the control group). According to a recent systematic review and meta-analysis of nine
randomised controlled trials reporting on 3374 women, perineal massage during second stage
of labour is associated with significant lower risk of severe perineal trauma, such as third- and
fourth-degree lacerations and episiotomies [23].
Additional findings relating to other midwifery practices during the second stage of labour
were also reported within the Cochrane review [33], including: whether the posterior or the
anterior shoulder should be born first, the use of different oils/wax or cold compress on the
perineum and the use of a perineal protection device. For the majority it is not clear if these
techniques had a beneficial effect on preventing perineal trauma, with the exception of an
increased incidence of intact perineum with the use of a perineal protection device.
Discussion
This systematic review focused specifically on midwives’ practices during the second stage of
labour for women experiencing a physiological labour and birth. The results provide insight in
how midwives practices are influenced by their years of experience, the designation of the
maternity unit where they work, (for example, a midwife-led unit or an obstetric unit) and
that midwives practices are not always consistent with the scientific literature or with a physio-
logical approach to birth.
In relation to birthing positions, women can adopt various positions to give birth, largely,
upright (such as, standing, squatting, kneeling) and supine (such as lateral, lithotomy, dorsal,
semi-recumbent). The limited number of studies relating to birth position included in this
review reported on perineal damage and pain severity and included midwives’ perspectives/
practices. Ultimately, women should be facilitated to adopt the position they deem most
PLOS ONE How midwives facilitate women to give birth during physiological second stage of labour?
PLOS ONE | https://doi.org/10.1371/journal.pone.0226502 July 28, 2020 14 / 19
Page 16
comfortable to give birth and should be educated with regards to all childbirth positions,
encouraging them to select each of the positions voluntarily.
For non-pharmacological pain relief, transcutaneous electrical nerve stimulation seems to
be effective in reducing pain during birth and it has no consequences for women and their
infants [30]. The empirical evidence also supports the use of heat therapy in the form of a heat
pack for women in the physiological second stage of labour, as it can effectively reduce labour
pain [29]. No included studies discussed the effects of water on reducing pain during birth.
Regarding pushing techniques, we found no significant difference in the duration of the
second stage of labour between spontaneous and directed pushing. While a Cochrane review
highlighted an inability to report which technique of pushing is best for the mother or baby.
Woman’ preference, comfort and clinical context should therefore guide decisions [25].
As highlighted above a Cochrane review [22] and a systematic review by Pierce-Williams
et al. [27] found that hands-on or hands-off the perineum showed no clear supporting evi-
dence in the incidence of intact perineum, first degree perineal tears, second degree tears or
fourth degree tears, with episiotomy being performed more frequently in the hands-on group.
These reviews were inconsistent regarding third degree tears. The lack of heterogeneity of
studies within the Cochrane review for third-or fourth-degree tears means these data should
be interpreted with caution. In conclusion, there is insufficient evidence to promote one of
these midwifery practices over the other in regard to preventing perineal tears [22].
High-quality evidence suggests that compresses emerged in warm tap water increase the
incidence of intact perineum and lower the risk of episiotomy and third and fourth-degree
tears [26]. This low-cost highly effective intervention could easily be implemented in all birth
settings. To optimise perineal outcomes during the second stage of labour, perineal massage
can reduce the need for episiotomy, avoid perineal injuries and perineal pain [22].
Strengths and limitations
This is a full systematic review with searches across multiple databases reporting on published
research on how midwives can facilitate women to give birth during the physiological second
stage of labour. The methods of our review are transparent with full protocol published in
PROSPERO in advance of the review [40].
In view of the variable risk of bias of the included trials, further trials using well-designed
protocols are needed to ascertain the true benefits and risks of various midwifery practices
during the second stage of labour.
When studying research about how to facilitate women to give birth during physiological
second stage of labour, we came upon scarce evidence regarding the care and support provided
by midwives. These non-clinical aspects of labour and birth matter to woman, and are essential
components of quality intrapartum care for women and their family [WHO Intrapartum care
2018]. Only one article was included in our systematic review regarding this [37]. Begley et al.
underlined in her qualitative study the importance of developing an empowering, trusting
relationship with the woman, ensuring a quiet, calm environment, reassuring and supporting
the woman to optimise her birth outcome. There is a dearth of evidence relating to non-clini-
cal aspects of midwives’ practice during the second stage of labour, such as continuous sup-
port, emotional support, companionship, effective communication and respectful care. These
aspects of care are often not regarded as priorities [7]. Perhaps this is because not all midwives’
practices are documented and therefore researched. More research is needed on how midwives
practices may affect a woman’s experience of labour and birth outcomes.
For this review the second stage of labour was defined as the time period between full dilata-
tion of the cervix and the birth of the baby, whilst the woman is experiencing an involuntary
PLOS ONE How midwives facilitate women to give birth during physiological second stage of labour?
PLOS ONE | https://doi.org/10.1371/journal.pone.0226502 July 28, 2020 15 / 19
Page 17
urge to bear down, due to expulsive uterine contractions [7]. However, another definition of
the second stage of labour has been noted. Bjelke et al. outlines a definition of the second stage
of labour, which included two phases, the passive and the active phase [41]. The passive phase
is defined as full dilatation of the cervix before or in the absence of involuntary expulsive con-
tractions. During this phase the presenting part descends passively down in the maternal pel-
vis, eventually generating a reflex that causes a strong urge to push. The active phase is the
stage of expulsive efforts. This division of the second stage of labour, into two phases is rarely
reported. Further research could focus on how to manage the passive phase of the second stage
of labour.
Culture, birth settings and work practices effect the possibility of the physiological approach
to birth being enabled or not [35]. It is essential therefore that women with a straightforward
pregnancy� [42] can take an informed choice [43] and gain access to midwife-led services to
plan their birth at home or within a midwife-led unit, where the physiological approach to
birth is enabled. Gaining access to a midwife-led unit can be enabled by utilising an evi-
denced-based guideline for admission to either an alongside or freestanding midwife-led unit
and midwives can facilitate care by following a normal labour and birth care pathway [42, 44].
Conclusion
This review systematically collated pertinent literature by retrieving 6,382 studies after the
removal of duplicates. Following synthesis empirical evidence of different aspects of midwifery
practices relating to care during the second stage of labour were retrieved including: Birthing
positions, non-pharmacological pain relief, pushing techniques and optimising perineal out-
comes. By implementing this evidence midwives may enable women during the second stage
of labour to optimise physiological processes to give birth. There is however, a dearth of evi-
dence relating to midwives’ practice during the second stage of labour and further robust stud-
ies are required. There is also limited knowledge of how midwives’ practices may affect a
woman’s experience of the second stage of labour. Nevertheless, this systematic review pro-
vides a summary of the current empirical evidence of midwives’ practices of physiological sec-
ond stage of labour and can inform midwifery practice, education and future research in the
support of high-quality intrapartum care.�Straightforward singleton pregnancy, is one in which the woman does not have any pre-
existing condition impacting on her pregnancy, a recurrent complication of pregnancy or a
complication in this pregnancy which would require on-going consultant input, has reached
37 weeks’ gestation and� Term +14 days [42].
Supporting information
S1 Checklist. PRISMA 2009 checklist.
(DOC)
S1 Table. Search strategy tables.
(DOCX)
Acknowledgments
The authors gratefully thank Mary Dharmachandran (subject librarian at the Royal College of
Midwives, UK) for her valuable contribution to this systematic review.
PLOS ONE How midwives facilitate women to give birth during physiological second stage of labour?
PLOS ONE | https://doi.org/10.1371/journal.pone.0226502 July 28, 2020 16 / 19
Page 18
Author Contributions
Conceptualization: Maria Healy, Corine J. Verhoeven.
Data curation: Maria Healy, Viola Nyman, Dale Spence, Rene H. J. Otten, Corine J.
Verhoeven.
Formal analysis: Maria Healy, Dale Spence, Corine J. Verhoeven.
Funding acquisition: Maria Healy.
Investigation: Viola Nyman, Corine J. Verhoeven.
Methodology: Maria Healy, Rene H. J. Otten, Corine J. Verhoeven.
Project administration: Maria Healy.
Software: Maria Healy.
Supervision: Maria Healy.
Writing – original draft: Maria Healy, Viola Nyman, Dale Spence, Rene H. J. Otten, Corine J.
Verhoeven.
Writing – review & editing: Maria Healy, Viola Nyman, Dale Spence, Rene H. J. Otten, Cor-
ine J. Verhoeven.
References1. Dahlen HG, Dowling H, Tracy M, Schmied V, Tracy S. Maternal and perinatal outcomes amongst low
risk women giving birth in water compared to six birth positions on land. A descriptive cross sectional
study in a birth centre over 12 years. Midwifery. 2013; 29 (7): 759–764. https://doi.org/10.1016/j.midw.
2012.07.002 PMID: 22884894
2. Lemola S, Stadlmayr W, Grob A. Maternal adjustment five months after birth: The impact of the subjec-
tive experience of childbirth and emotional support from the partner. Journal of Reproductive and Infant
Psychology. 2007; 25(3): 190–202. https://doi.org/10.1080/02646830701467231.
3. Creedy DK, Shochet IM, Horsfall J. Childbirth and the development of acute trauma symptoms: inci-
dence and contributing factors. Birth. 2000; 27(2): 104–11. https://doi.org/10.1046/j.1523-536x.2000.
00104.x PMID: 11251488
4. Czarnocka J, Slade P. Prevalence and predictors of post-traumatic stress symptoms following child-
birth. Br J Clin Psychol. 2000; 39(1):35–51. https://doi.org/10.1348/014466500163095 PMID:
10789027
5. Waldenstrom U, Schytt E. A longitudinal study of women’s memory of labour pain—from 2 months to 5
years after the birth. BJOG. 2009 Mar; 116(4):577–83. https://doi.org/10.1111/j.1471-0528.2008.
02020.x PMID: 19076128
6. Lundgren I, Karlsdottir SI, Bondas T. Long-term memories and experiences of childbirth in a Nordic con-
text—a secondary analysis. International Journal of Qualitative Studies on Health and Well-being.
2009; 4(2): 115–128. https://doi.org/10.1080/17482620802423414
7. World Health Organization. WHO recommendations: intrapartum care for a positive childbirth experi-
ence. 2018; Geneva, Switzerland. https://www.who.int/reproductivehealth/publications/intrapartum-
care-guidelines/en/
8. World Health Organization. World health report 2005: Make every mother and child count. 2005;
Geneva, Switzerland. https://www.who.int/whr/2005/whr2005_en.pdf.
9. Keag OE, Norman JE, Stock SJ. Long-term risks and benefits associated with cesarean delivery for
mother, baby, and subsequent pregnancies: Systematic review and meta-analysis. PLoS Med. 2018
Jan 23; 15(1):e1002494. https://doi.org/10.1371/journal.pmed.1002494 PMID: 29360829
10. World Health Organisation. Care in normal birth: a practical guide. Technical Working Group, Birth.
1997; 24(2): 121–3.
11. Begley CM, Gyte GM, Devane D, McGuire W, Weeks A, Biesty LM. Active versus expectant manage-
ment for women in the third stage of labour. Cochrane Database Syst Rev. 2019; 13(2):CD007412.
https://doi.org/10.1002/14651858.CD007412.pub5 PMID: 30754073
PLOS ONE How midwives facilitate women to give birth during physiological second stage of labour?
PLOS ONE | https://doi.org/10.1371/journal.pone.0226502 July 28, 2020 17 / 19
Page 19
12. Anim-Somuah M, Smyth RMD, Cyna AM, Cuthbert A. Epidural versus non-epidural or no analgesia for
pain management in labour. Cochrane Database Syst Rev 2018 May 21; 5:CD000331. https://doi.org/
10.1002/14651858.CD000331.pub4 PMID: 29781504
13. Uvnas Moberg K, Ekstrom-Bergstrom A, Berg M, Buckley S, Pajalic Z, Hadjigeorgiou E, et al. Maternal
plasma levels of oxytocin during physiological childbirth—a systematic review with implications for uter-
ine contractions and central actions of oxytocin. BMC Pregnancy Childbirth. 2019 Aug 9; 19(1):285.
https://doi.org/10.1186/s12884-019-2365-9 PMID: 31399062
14. Uvnas -Moberg K. The Hormone of Closeness. London: Pinter & Martin Ltd; 2012.
15. Uvnas -Moberg K. How kindness, warmth, empathy and support promote the progress of labour: a
physiological perspective. In: The Roar Behind the Silence. London: Pinter and Martin Ltd; 2015.
16. Kennedy HP, Yoshida S, Costello A, Declercq E, Dias MA, Duff E, et al. Asking different questions:
research priorities to improve the quality of care for every woman, every child. Lancet Glob Health.
2016; 4(11): e777–e779. https://doi.org/10.1016/S2214-109X(16)30183-8 PMID: 27663682
17. Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M, et al. Preferred Reporting Items for
Systematic Review and Meta-Analysis Protocols (PRISMA-P) 2015 statement. Syst Rev. 2015; 4(1):1.
https://doi.org/10.1186/2046-4053-4-1 PMID: 25554246
18. McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of
Electronic Search Strategies: 2015 Guideline Statement. J Clin Epidemiol. 2016; 75:40–6. https://doi.
org/10.1016/j.jclinepi.2016.01.021 PMID: 27005575
19. National Institute for Health and Care Excellence (NICE). Intrapartum care: Care of healthy women and
their babies during childbirth. Clinical guideline [CG55]. 2007; NICE.
20. Higgins JP, Green S. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0. The
Cochrane Collaboration, 2011. www.handbook.cochrane.org.
21. Critical Appraisal Skills Programme 2018. CASP Checklists. https://casp-uk.net/casp-tools-checklists/.
22. Aasheim V, Nilsen AB, Reinar LM, Lukasse M. Perineal techniques during the second stage of labour
for reducing perineal trauma. Cochrane Database Syst Rev. 2017; 13; 6:CD006672. https://doi.org/10.
1002/14651858.CD006672.pub3 PMID: 28608597
23. Aquino CI, Guida M, Saccone G, Cruz Y, Vitagliano A, Zullo F, et al. Perineal massage during labor: a
systematic review and meta-analysis of randomized controlled trials. J Matern Fetal Neonatal Med.
2018 Sep 19:1–13. https://doi.org/10.1080/14767058.2018.1512574 PMID: 30107756
24. Gupta JK, Sood A, Hofmeyr GJ, Vogel JP. Position in the second stage of labour for women without epi-
dural anaesthesia. Cochrane Database Syst Rev. 2017; 25; 5:CD002006. https://doi.org/10.1002/
14651858.CD002006.pub4 PMID: 28539008
25. Lemos A, Amorim MM, Dornelas de Andrade A, de Souza AI, Cabral Filho JE, Correia JB. Pushing/
bearing down methods for the second stage of labour. Cochrane Database of Syst Rev. 2017; 26; 3:
CD009124. https://doi.org/10.1002/14651858.CD009124.pub3 PMID: 28349526
26. Magoga G, Saccone G, Al-Kouatly HB, Dahlen GH, Thornton C, Akbarzadeh M, et al. Warm perineal
compresses during the second stage of labor for reducing perineal trauma: A meta-analysis. Eur J
Obstet Gynecol Reprod Biol. 2019 Sep; 240:93–98. https://doi.org/10.1016/j.ejogrb.2019.06.011
PMID: 31238205
27. Pierce-Williams RA, Saccone G, Berghella V. Hands-on versus hands-off techniques for the prevention
of perineal trauma during vaginal delivery: a systematic review and meta-analysis of randomized con-
trolled trials. J Matern Fetal Neonatal Med. 2019 Jun 3:1–9. https://doi.org/10.1080/14767058.2019.
1619686 PMID: 31092083
28. Alihosseni F, Abedi P, Afshary P, Haghighi MR, Hazeghi N. Investigating the Effect of Perineal Heating
Pad on the Frequency of Episiotomies and Perineal Tears in Primiparous Females. Med Surg Nurs J.
2018; 7(1): e82588. https://doi.org/10.5812/msnj.82588
29. Fahami F, Behmanesh F, Valiani M, Ashouri E. Effect of heat therapy on pain severity in primigravida
women. Iran J Nurs Midwifery Res. 2011; 16(1):113–6. PMID: 22039388
30. Shahoei R, Shahghebi S, Rezaei M, Naqshbandi S. The effect of transcutaneous electrical nerve stimu-
lation on the severity of labor pain among nulliparous women: A clinical trial. Complement Ther Clin
Pract. 2017; 28:176–180. https://doi.org/10.1016/j.ctcp.2017.05.004 PMID: 28779926
31. Shahoei R, Zaheri F, Nasab LH, Ranaei F. The effect of perineal massage during the second stage of
birth on nulliparous women perineal: A randomisation clinical trial. Electron Physician. 2017 25; 9
(10):5588–5595. https://doi.org/10.19082/5588 PMID: 29238501
32. Valiani M, Rezaie M, Shahshahan Z. Comparative study on the influence of three delivery positions on
pain intensity during the second stage of labour. Iran J Nurs Midwifery Res. 2016; 21(4):372–378.
https://doi.org/10.4103/1735-9066.185578 PMID: 27563320
PLOS ONE How midwives facilitate women to give birth during physiological second stage of labour?
PLOS ONE | https://doi.org/10.1371/journal.pone.0226502 July 28, 2020 18 / 19
Page 20
33. Vaziri F, Arzhe A, Asadi N, Pourahmad S, Moshfeghy Z. Spontaneous Pushing in Lateral Position ver-
sus Valsalva Maneuver During Second Stage of Labor on Maternal and Fetal Outcomes: A Random-
ized Clinical Trial. Iran Red Crescent Med J. 2016 Aug 10; 18(10):e29279. https://doi.org/10.5812/ircmj.
29279 PMID: 28180019
34. De Jonge A, Van Diem MT, Scheepers PL, Buitendijk SE, Lagro-Janssen AL. Risk of perineal damage
is not a reason to discourage a sitting birthing position: A secondary analysis. Int J Clin Pract. 2010; 64
(5):611–8. https://doi.org/10.1111/j.1742-1241.2009.02316.x PMID: 20456214
35. Barasinski C, Debost-Legrand A, Lemery D, Vendittelli F. Practices during the active second stage of
labor: A survey of French midwives. Midwifery. 2018; 60: 48–55. https://doi.org/10.1016/j.midw.2018.
02.001 PMID: 29494852
36. Trochez R, Waterfield M, Freeman RM. Hands on or hands off the perineum: a survey of care of the per-
ineum in labour (HOOPS). Int Urogynecol J. 2011; 22(10):1279–85. https://doi.org/10.1007/s00192-
011-1454-8 PMID: 21611790
37. Begley C, Guilliland K, Dixon L, Reilly M, Keegan C, McCann C, et al. A qualitative exploration of tech-
niques used by expert midwives to preserve the perineum intact. Women Birth. 2019; 32(1):87–97.
https://doi.org/10.1016/j.wombi.2018.04.015 PMID: 29730096
38. De Jonge A, Teunissen DA, Van Diem MT, Scheepers PL, Lagro-Janssen AL. Women’s positions dur-
ing the second stage of labour: views of primary care midwives. J Adv Nurs. 2008; 63(4):347–56.
https://doi.org/10.1111/j.1365-2648.2008.04703.x PMID: 18727762
39. Thachuk A. Midwifery, informed choice, and reproductive autonomy: a relational approach. Feminism
Psychology. 2007; 17(1): 39–56 https://doi.org/10.1177/0959353507072911
40. Verhoeven CJ, Spence D, Nyman V, Otten RHJ, Healy M. How do midwives facilitate women to give
birth during physiological second stage of labour? A protocol for a systematic review. Syst Rev. 2019
Jan 3; 8(1):1. https://doi.org/10.1186/s13643-018-0916-1 PMID: 30606256
41. Bjelke M, Lendahls L, Oscarsson M. Management of the passive phase of the second stage of labour in
nulliparous women—Focus group discussions with Swedish midwives. Midwifery. 2019; 75:89–96.
https://doi.org/10.1016/j.midw.2019.04.011 PMID: 31071586
42. GAIN/RQIA (2016a). Guideline for admission to midwife-led units in Northern Ireland and Northern Ire-
land normal labour and birth care pathway, Belfast: RQIA. https://www.rqia.org.uk/RQIA/files/3a/
3a7a37bb-d601-4daf-a902-6b60e5fa58c2.pdf
43. GAIN/RQIA (2016b). Planning to give birth in a midwife-led unit in Northern Ireland, Belfast: RQIA.
https://www.rqia.org.uk/RQIA/files/71/71cffe60-dd2d-405d-bd86-5728f5623fab.pdf.
44. Healy M, Gillen P. Planning birth in and admission to a midwife-led unit: development of a GAIN evi-
dence-based guideline. Evidence Based Midwifery,2016; 14(3): 82–86.
PLOS ONE How midwives facilitate women to give birth during physiological second stage of labour?
PLOS ONE | https://doi.org/10.1371/journal.pone.0226502 July 28, 2020 19 / 19