How is equity approached in universalhealth coverage? An analysis of global andcountry policy documents in Benin andSenegalElisabeth Paul1,2* , Céline Deville1, Oriane Bodson1, N’koué Emmanuel Sambiéni3, Ibrahima Thiam4,Marc Bourgeois5, Valéry Ridde6 and Fabienne Fecher1
Abstract
Background: Equity seems inherent to the pursuance of universal health coverage (UHC), but it is not a naturalconsequence of it. We explore how the multidimensional concept of equity has been approached in key globalUHC policy documents, as well as in country-level UHC policies.
Methods: We analysed a purposeful sample of UHC reports and policy documents both at global level and in twoWestern African countries (Benin and Senegal). We manually searched each document for its use and discussion ofequity and related terms. The content was summarised and thematically analysed, in order to comprehend howthese concepts were understood in the documents. We distinguished between the level at which inequity takesplace and the origin or types of inequities.
Results: Most of the documents analysed do not define equity in the first place, and speak about “healthinequities” in the broad sense, without mentioning the dimension or type of inequity considered. Some dimensionsof equity are ambiguous – especially coverage and financing. Many documents assimilate equity to an overallobjective or guiding principle closely associated to UHC. The concept of equity is also often linked to otherconcepts and values (social justice, inclusion, solidarity, human rights – but also to efficiency and sustainability).Regarding the levels of equity most often considered, access (availability, coverage, provision) is the most oftenquoted dimension, followed by financial protection. Regarding the types of equity considered, those most referredto are socio-economic, geographic, and gender-based disparities. In Benin and Senegal, geographic inequities aremostly pinpointed by UHC policy documents, but concrete interventions mostly target the poor. Overall, the UHCpolicy of both countries are quite similar in terms of their approach to equity.
Conclusions: While equity is widely referred to in global and country-specific UHC policy documents, its multipledimensions results in a rather rhetorical utilisation of the concept. Whereas equity covers various levels and types,many global UHC documents fail to define it properly and to comprehend the breadth of the concept.Consequently, perhaps, country-specific policy documents also use equity as a rhetoric principle, without sufficientconsideration for concrete ways for implementation.
Keywords: Universal health coverage, Equity, Global reports, Policy documents, Low- and middle-income countries,Benin, Senegal
* Correspondence: [email protected]é de Liège, Faculty of Social Sciences, Place des Orateurs 3, 4000Liège, Belgium2Université libre de Bruxelles, School of Public Health, Campus Erasme, Routede Lennik 808, 1070 Brussels, CP 591, BelgiumFull list of author information is available at the end of the article
Paul et al. International Journal for Equity in Health (2019) 18:195 https://doi.org/10.1186/s12939-019-1089-9
BackgroundUniversal health coverage (UHC) means that all peoplereceive the health services they need, including healthinitiatives designed to promote better health, prevent ill-ness, and to provide the treatment, rehabilitation andpalliative care of sufficient quality to be effective while atthe same time ensuring that the use of these servicesdoes not expose the user to financial hardship [1]. Equityseems inherent to the pursuance of UHC: for instance,the World Health Report 2008 defines universal cover-age reforms as “reforms that ensure that health systemscontribute to health equity, social justice and the end ofexclusion, primarily by moving towards universal accessand social health protection” [2]; the World Health Or-ganisation (WHO) believes that equity is an intermediateobjective of UHC [3]; and the WHO Consultative Groupon Equity and Universal Health Coverage urges coun-tries to commit to fairness, equity and rights to health inpolicymaking [4]. However, equity is not a natural con-sequence of the implementation of UHC policies. Onthe contrary, the pursuance of UHC implies trade-offswhich are not necessarily favourable to vulnerablepeople, and some policies pursued in the name of UHCmay worsen inequalities [5–8]. Hence the acknowledgedimportance of measuring inequity, and tracking progressin this regard when implementing UHC policies [9, 10].Note first that equity is a commonly used term in pub-
lic health. A narrative review of peer-reviewed literaturepublished in English between 2005 and 2013 retrievedapproximately 9000 papers from PubMed via the searchwords, ‘universal health coverage/care’ and ‘equity/in-equity’ [9]. However, it is a controversial, ambiguousconcept that is intertwined with a number of other con-cepts such as fairness (which is a broader concept andspecifically focuses on the worst-off), equality, socialjustice, social inclusion, solidarity, altruism, and rights tohealth [4, 6, 11–15]. It is opposed to health inequalitiesor disparities, which refer to health differences that areavoidable, unnecessary, and unjust [16]. Health inequi-ties are also closely interconnected with disparities insocial determinants of health [17].Equity in health encompasses various dimensions, some
related to means or processes, some related to ends oroutcomes [13]: equity in healthcare coverage (access, useof services) (often called horizontal equity: equal treatmentfor equal need); equity in health outcomes; equity inhealth financing (often called vertical equity, meaning thateveryone contributes to health financing according toone’s ability to pay); equity in financial protection. Whenassociated to the pursuance of UHC, studies from low-and middle-income countries generally explore theequity impact of UHC based on disaggregated data bygeographical area, socio-economic status and gender;but another key area in which inequity may arise across
both developing and developed contexts is disparities inthe quality of care and access to specialised clinical ser-vices [9]. Other types of disparities in health servicesrelate to race/ethnicity, culture, education, or other so-cial advantages [17–21]. The measurement of health in-equalities remains challenging and is an evolvingconcept [9, 12, 22–25].
MethodsThis paper aims to explore on the one hand how themultidimensional concept of equity has been approachedin key global UHC reports and policy documents, andon the other hand whether and how this understandingimpacts on UHC policies at country level. To do so, weanalysed a sample of key UHC reports and policy docu-ment both at the global level and in two countries: Beninand Senegal. These two countries are the focus of ourresearch project (2015–2019) on UHC policies. They arelocated in Francophone Western Africa, have relativelysimilar health systems and challenges, but have chosenvery different paths to expand financial protection coveragefor healthcare: while Senegal has opted for community-based health insurance (CBHI), Benin is striving to developa national, state-led health insurance [26]. This offers inter-esting comparisons.We used a similar heuristic approach to the one used
by other authors regarding quality in health systems pol-icy [27], and searched the websites of the two major glo-bal institutions shaping UHC policies and in charge ofits global monitoring – the WHO and the World Bank(WB) – for reports and policy documents dedicated toUHC. We selected the most relevant and significantones to build a purposeful sample of 20 key UHCreports and policy documents issued after the release ofthe first World Health Assembly Resolution on UHC(58.33) in 2005 (actually starting in 2008) and until2018. Note that we excluded two documents whose pri-mary focus was to comprehend equity – the report ofthe Commission on social determinants of health [17],and the WB’s database of equity indicators [28] – butwe also identified and included a report of the Inter-national Labour Organisation (ILO) dedicated to socialprotection in health [29]. We manually searched eachdocument for its use and discussion of “equit*”, “inequal*”,“unequal”, and “disparit*”. The content was then sum-marised and analysed, especially in order to understandhow these concepts were comprehended in each docu-ment and to appraise the extent to which the documentswere preoccupied by those concepts. This was donethrough a mixed approach comprising a qualitative con-tent analysis component (thematic analysis of the dis-course utilised to approach equity in the documents) anda quantitative component (counting the number of occur-rences of the terms related to equity in each document, as
Paul et al. International Journal for Equity in Health (2019) 18:195 Page 2 of 21
well as the breadth of its understanding – levels and typesof equity referred to). We distinguished between (i) thelevel at which inequity takes place (social determinants,health outcomes, health systems and policies, access/coverage/use of health services, funding, and financialprotection), and (ii) the origin or types of health inequi-ties (socio-economic, gender-based, etc.). Then, weadopted the same approach to analyse how the conceptof equity was comprehended in three types of UHCpolicy documents in Benin and Senegal: (i) the nationalhealth sector plan (NHSP), (ii) the national health fi-nancing strategies (NHFS) for UHC; and (iii) other pol-icy documents describing the UHC strategy or schemefavoured by the government. The results are presentedin summary tables and the most salient features arethen explained more into details.
ResultsEquity in key global UHC reports and policy documentsTable 1 offers a quantitative overview of the importancegiven to equity, and of the dimensions comprehended,in key global UHC policy documents.Regarding the levels of equity most often considered,
access (availability, coverage, provision, use) is the mostoften quoted dimension (explicitly referred to by 18 docu-ments out of 20), followed by equity in financial protection(14/20 documents), and then equity at the level of healthsystems, policies and/or distribution of resources (13/20documents), with varying focus according to sources. Otherdimensions include equity in financial contribution (fund-ing), in health outcomes, and in social determinants ofhealth (incl. distribution of power, money and resources;health behaviours; water and sanitation). Regarding thetypes of equity considered, those most referred to are socio-economic (wealth/income disparities) (explicitly referred toby 15 documents out of 20), geographic (across regions andurban/rural areas) (mentioned by 13/20 documents), otheror undefined socio-economic disparities (12/20 docu-ments), and gender-based disparities (10/20 documents). Avariety of other criteria (“stratifiers”) are mentionedthroughout the documents: education, age, and cultural fac-tors such as religion, race/ethnicity, and migrant status.A more in-depth and qualitative content analysis of
how equity has been approached in global UHC docu-ments is provided in Table 2.Analysis of that sample of key UHC policy documents
offer a number of interesting comments. First, most doc-uments (15/20) do not define equity in the first place.Second, most documents speak about “health equity” or“inequity in health” in the broad sense, without mention-ing the dimension or type of inequity considered. Third,there is a certain ambiguity in some dimensions of equity:“coverage” is sometimes utilised in the sense of access oravailability of health services, sometimes in the sense of
utilisation of health services; and “financing” sometimesrefers to equity in funding (mobilisation of resources,vertical equity, public spending), sometimes to equityin resource allocation, and even sometimes in financialprotection. Fourth, most documents assimilate equity toan overall objective or guiding principle closely associatedto UHC and the Sustainable Development Goals (SDGs).However, the links alluded to between UHC and equityare not straightforward: overall, it is unclear whether afocus on equity is supposed to enable progress in UHC(equity as a means), whether UHC is supposed to increaseequity (equity as an end), or whether these are two distinctaims. Similarly, it is unclear whether equity is a value orprinciple orienting actions, or whether it is an objective ofsuch actions. Some of the documents try and clarify thelinks between UHC and equity: for instance, the publica-tions from the health financing department of the WHOrecurrently use a model stating that equity in the distribu-tion of resources is a UHC intermediate objective, andequity in service use is a UHC goal [39, 45]; a joint reportviews UHC as “the response to” inequities [36]; and the2017 Global monitoring report makes a clear distinctionbetween equity and UHC [43]. Nevertheless, the globalpicture is unclear in most documents, and the approach ofequity is often more rhetorical than concrete. Fifth, theconcept of equity is also often linked to other conceptsand values such as social justice (or inclusion), solidarity,human rights (including the right to health), and povertyalleviation – but it is even more often associated with effi-ciency, as well as with sustainability.
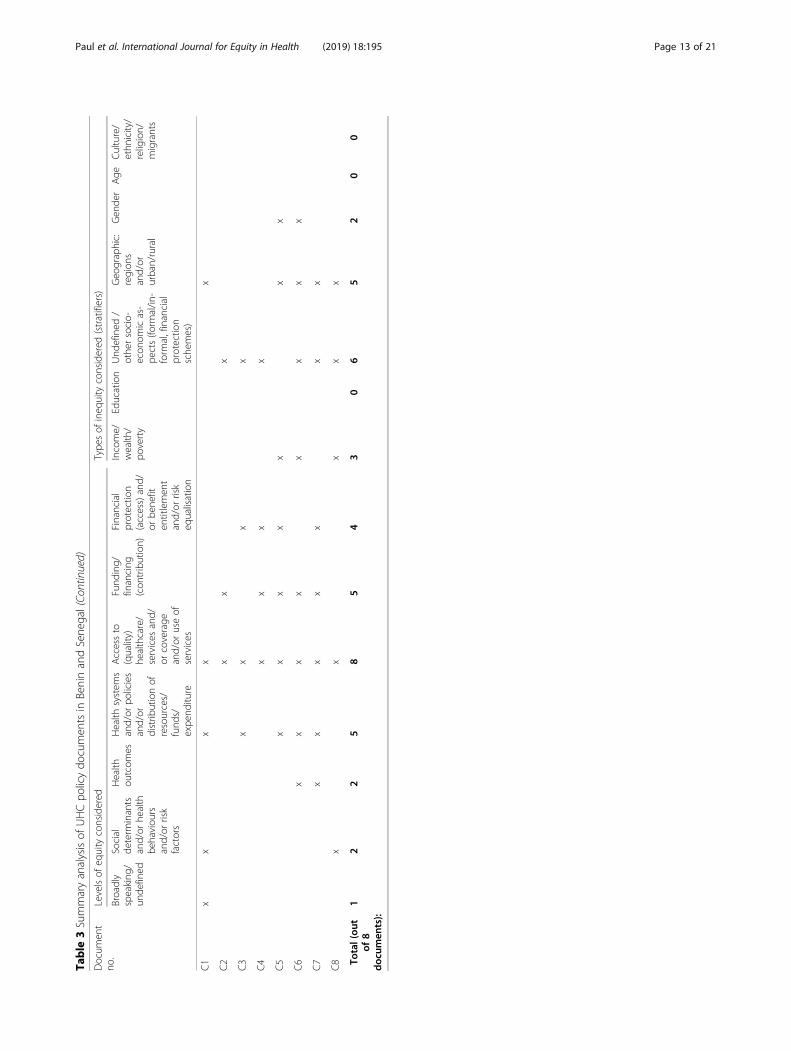
Implications on country UHC policiesTable 3 and Table 4 follow a similar thematic analyticalapproach and summarise the results from the analysison how the concept of equity was comprehended inthree types of country-specific policy documents inBenin and Senegal: (i) the national health sector plan(NHSP), (ii) the national health financing strategy(NHFS); and (iii) other UHC policy documents.The documents from the two countries present simi-
larities, which enables a joint analysis. Note first that anumber of findings are similar to those of the globaldocuments. Most country-specific policy documents (7out of 8) do not define equity in the first place; coverage,access and supply of services are used interchangeably,and the dimensions and types of health equity are oftennot well explicated. Regarding the level of equity consid-ered, all country documents in our sample explicitlyrefer to access / coverage / use of services. Country doc-uments also put a lot of emphasis on improving equityin allocation of resources (especially human resources)across regions (referred to explicitly by 5 documents outof 8), and on funding/financial contribution (5/8 as well).Regarding the types of equity considered, undefined or
Paul et al. International Journal for Equity in Health (2019) 18:195 Page 3 of 21
Table
1Summaryanalysisof
glob
alUHCpo
licydo
cumen
ts
Docum
ent
No.
Source
Title
# page
s# occurren
ces
“equ
it*”
# occurren
ces
“equ
al*”
# occurren
ces
“disparit*”
G1
WHO2008
World
Health
Repo
rt2008:Prim
aryhe
alth
care:N
owmorethan
ever
[2]
148
168
825
G2
WHO2010
World
Health
Repo
rt2010:H
ealth
System
sFinancing:
Thepath
toun
iversalcoverage[30]
128
4132
1
G3
WHO2013
World
Health
Repo
rt2013:ResearchforUniversalHealth
Coverage[31]
168
271
0
G4
WHO2013
Arguing
forUniversalHealth
Coverage[32]
4023
20
G5
WHO2013
UniversalHealth
Coverage:Supp
ortin
gCou
ntry
Needs
[33]
129
70
G6
WHO&WB2013
Backgrou
nddo
cumen
tTowards
UHC:con
cepts,lesson
sandpu
blicpo
licychalleng
es[34]
42
30
G7
WB2013
TheIm
pact
ofUniversalCoverageSche
mes
intheDevelop
ingWorld
[35]
151
219
0
G8
RockefellerFoun
datio
n,Save
the
Children,UNICEF
andWHO2013
UniversalHealth
Coverage:ACom
mitm
entto
Close
theGap
[36]
84373
264
G9
WHO&WB2014
Mon
itorin
gprog
ress
towards
universalh
ealth
coverage
atcoun
tryandglob
allevels–
Fram
ework,measuresandtargets[25]
1420
00
G10
ILO2014
UniversalHealth
Protectio
n:Prog
ress
todate
andtheway
forw
ard[29]
130
5220
0
G11
WB2013
Going
Universal–How
24Develop
ingCou
ntriesAre
Implem
entin
gUniversalHealth
CoverageReform
sfro
mtheBo
ttom
Up[37]
289
5127
0
G12
WHO/region
alofficeforA
frica
2015
TheAfricanHealth
Mon
itorSpecialissue:U
niversalHealth
Coverage[38]
7651
65
G13
WHO&WB2015
Tracking
universalh
ealth
coverage
:firstglob
almon
itorin
grepo
rt[1]
9835
2211
G14
WHO2016
Health
financing
coun
trydiagno
stic:a
foun
datio
nfornatio
nalstrateg
yde
velopm
ent[39]
5862
220
G15
WHO2016
PublicFinancingforHealth
inAfrica:from
Abu
jato
theSD
Gs[40]
9212
10
G16
WHO2017
GlobalR
eport:New
Perspe
ctives
onGlobalH
ealth
Spen
ding
forUniversalHealth
Coverage[41]
404
20
G17
WHO2017
Toge
ther
ontheroad
toun
iversalh
ealth
coverage
–acallto
actio
n[42]
389
100
G18
WHO2017
Develop
inganatio
nalh
ealth
financing
strategy:a
referencegu
ide[43]
4420
20
G19
WHO&WB2017
Tracking
universalh
ealth
coverage
:2017glob
almon
itorin
grepo
rt[43]
8812
430
G20
WHO/Reg
ionalO
ffice
forAfrica
2017
Thestateof
health
intheWHOAfricanRegion
:ananalysisof
thestatus
ofhe
alth,health
services
andhe
alth
system
sin
thecontextof
theSD
Gs[44]
184
38(8)*
2
Total(ou
tof
20doc
umen
ts):
Note:
Thenu
mbe
rof
occurren
cespresen
tedisthenu
mbe
rof
relevant
occurren
ces:exclud
ingin
references
andinde
x/conten
ts,and
exclud
ingad
verbialu
seof
equa
l*[equ
ally,e
qual
to,etc.]
*SD
Gs
Paul et al. International Journal for Equity in Health (2019) 18:195 Page 4 of 21
Table
1Summaryanalysisof
glob
alUHCpo
licydo
cumen
ts(Con
tinued)
Docum
ent
No.
Levelsof
equity
considered
Type
sof
ineq
uity
considered
(stratifiers)
Broadly
speaking
/un
defined
Social
determ
inants
and/or
health
behaviou
rsand/or
risk
factors
Health
outcom
esHealth
system
sand/
orpo
licies
and/or
distrib
ution
ofresources/
fund
s/expe
nditu
re
Accessto
(quality)
healthcare/
services
and/or
coverage
and/or
use
ofservices
Fund
ing/
financing
(con
tribution)
Financial
protectio
n(access)
and/or
bene
fiten
titlemen
tand/or
risk
equalisation
Across
coun
tries
Income/
wealth
/po
verty
Education
Und
efined
/othe
rsocio-
econ
omic
aspe
cts(e.g.
occupatio
n,financial
protectio
nsche
mes)
Geo
graphic:
region
sand/or
urban/rural
Gen
der
Age
Culture/
ethn
icity/
religion/
migrants
G1
xx
xx
xx
xx
xx
xx
xx
G2
xx
xx
xx
xx
xx
x
G3
xx
xx
x
G4
xx
xx
xx
xx
G5
xx
xx
xx
xx
xx
G6
xx
xx
G7
xx
xx
G8
xx
xx
xx
xx
xx
xx
xx
x
G9
xx
xx
x
G10
xx
xx
xx
xx
xx
x
G11
xx
xx
xx
xx
x
G12
xx
xx
xx
G13
xx
xx
xx
xx
xx
xx
G14
xx
xx
xx
x
G15
xx
xx
G16
xx
xx
G17
xx
xx
xx
x
G18
x[UHC
interm
ediate
obj.]
x[final
coverage
goal]
xx[final
coverage
goal]
xx
G19
xx
xx
xx
xx
x
G20
xx
xx
xx
xx
Total(ou
tof
20doc
umen
ts):
127
713
1812
147
155
1213
104
6
Paul et al. International Journal for Equity in Health (2019) 18:195 Page 5 of 21
Table
2Analysisof
theway
equity
isapproached
inglob
alUHCdo
cumen
ts
Docum
ent
no.
Source
Title
Explicitde
finition
ofeq
uity?
How
equity
isapproached
inthedo
cumen
t
C1
WHO2008
World
Health
Repo
rt2008:Prim
aryhe
alth
care:N
owmorethan
ever
[2]
No
-Chapter
1“The
challeng
esof
achanging
world”de
votesa
sectionto
the“Chang
ingvalues
andrisingexpe
ctations”
which
comprises
asubsectio
non
“Health
equity”
-Equity
isacentralcon
cern
ofChapter
2“Advancing
and
sustaining
universalcoverage”,especially
inthefollowing
sections:
“The
centralp
lace
ofhe
alth
equity
inprim
aryhe
alth
care
(PHC)”
and“M
obilizing
forhe
alth
equity”
-Amon
gthefour
reform
sadvocatedforin
therepo
rt,universal
coverage
reform
sareview
edas
thosethat
“ensurethat
health
system
scontrib
uteto
health
equity,soc
ialjustice
andthe
endof
exclusion,
prim
arily
bymovingtowards
universalaccess
andsocialhe
alth
protectio
n”(pageix,m
essage
oftheDirector
Gen
eral--bo
ldou
rs)
-Therepo
rtpo
intsto
themultiple
dim
ension
sof
health
ineq
uality
-Associatio
nsof
equity
with
UHCandothe
rconcep
ts:
oTherepo
rtexplains
thelin
ksbetwee
nUHCan
deq
uity
–mostly
throug
hsocialhealth
protectio
n,increasin
gfinancial
accessto
healthcare
(bycontrast,out-of-p
ocketpaym
ents
(OOPs)are
deno
uncedas
inequitable)
oEquity
isview
edas
avaluedriving
theprimaryhe
althcare
mov
emen
t,toge
ther
with
solid
arityandsocial
justice
C2
WHO2010
World
Health
Repo
rt2010:H
ealth
System
sFinancing:
Thepath
toun
iversalcoverage[30]
No
-Therepo
rtargu
esin
chapter3that
compu
lsoryprep
aidfund
s,if
possiblepo
oled
into
asing
lepo
ol,enables
toachieveeq
uity
goals
–sometim
escalledeq
uity
fund
s-Itmakes
thecase
forde
cision
sthat
contrib
uteto
equity
incontrib
utions,inpo
oling,
andin
useof
resources
-Associatio
nsof
equity
with
UHCandothe
rconcep
ts:
oEquity
isassociated
repe
ated
lywith
effic
ienc
yo
Itismen
tione
don
cewith
fairne
ssandbasicdecen
cy
C3
WHO2013
World
Health
Repo
rt2013:Research
forUniversalHealth
Coverage[31]
No
-Therepo
rthasasectionde
dicatedto
“Equity
andun
iversal
health
cove
rage”
-Itpo
intsto
the“in
equitableaccess
totheprod
uctsof
research”
(p.45)
-Associatio
nsof
equity
with
UHCandothe
rconcep
ts:
oEquity
isassociated
with
cultural
values,right
tohe
alth
andsocial
justiceas
wellaswith
discrim
ination
oItisalso
associated
with
qua
ntityan
dqua
lityof
services,
andwith
effic
ienc
y
C4
WHO2013
Arguing
forUniversalHealth
Coverage[32]
Yes:“Equ
itable:do
esthe
mechanism
raise
fund
saccordingto
peop
le’s
ability
topay
andarethebe
nefits
distrib
uted
according
tope
ople’she
alth
need
s?”(p.
25)
-Thedo
cumen
tfocuseson
theeq
uity
ofthehe
alth
finan
cing
system
,and
provides
thecase
for“health
fund
ingpo
liciesthat
prom
oteequity,efficiency
andeffectiveness,andensure
thatthe
rightsof
themostvulnerableareno
tforgotten”
-Itsing
lesou
tou
t-of-pocketfinancing
asfailing
badlyin
term
sof
equity
andfinancialriskprotectio
n-Associatio
nsof
equity
with
UHCandothe
rconcep
ts:
oEquity
isassociated
with
effic
ienc
yan
deffectiven
ess,
and(hum
an)rights(tohe
alth)
Paul et al. International Journal for Equity in Health (2019) 18:195 Page 6 of 21
Table
2Analysisof
theway
equity
isapproached
inglob
alUHCdo
cumen
ts(Con
tinued)
Docum
ent
no.
Source
Title
Explicitde
finition
ofeq
uity?
How
equity
isapproached
inthedo
cumen
t
oThedo
cumen
tconsidersthat
equity
ispartof
UHC:
“equ
ityandfinancialriskprotection,which
areintegral
toachievingprog
resstowards
UHC“(p
.25);
“the
equitycriterionfund
amentaltoattaining
UHC”
(p.27);“theequityprinciples
that
shou
ldbe
thefoun
dationof
anyUHC
strategy”(p.32)
C5
WHO2013
UniversalHealth
Coverage:Supp
ortin
gCou
ntry
Needs
[33]
Yes:“Equ
ity:Ifallp
eople
obtain
thehe
alth
services
they
need
with
out
sufferin
gfinancial
hardship,equ
ityin
access
has
been
achieved
”(p.9)
-Associatio
nsof
equity
with
UHCandothe
rconcep
ts:
Thedo
cumen
tconsiderseq
uity
ispartof
UHC:“Thisvision
ofUHC
embo
dies
principles
ofeq
uity
inaccess
toanduseof
services,q
uality
oftheservices
peop
leob
tain,and
financialprotectio
nforpe
ople
need
inghe
alth
services”(p.5);UHCisno
ton
lyabou
the
alth
butalso
“movingcloser
toUHCisalso
abou
teq
uity,d
evelop
men
tpriorities,
socialinclusionandcohe
sion
”(p.10);U
HC“isaco
ncep
tthat
isfund
amen
tally
abou
teq
uity”(p.12)
C6
WHO&WB2013
Backgrou
nddo
cumen
tTowards
UHC:
concep
ts,lessons
andpu
blicpo
licy
challeng
es[34]
No
-Thedo
cumen
tmakes
thecase
forhe
alth
finan
cing
reform
s:“the
objectives
ofun
iversalfinancialprotectio
nandequityintheuseof
needed
services
arebestserved
whenhealth
system
srely
predom
inantly
oncompu
lsoryprepaidfund
s”-Italso
makes
thecase
forstrengthening
theprim
arylevelofcare
C7
WB2013
TheIm
pact
ofUniversalCoverage
Sche
mes
intheDevelop
ingWorld
[35]
No
-Associatio
nsof
equity
with
UHCandothe
rconcep
ts:
oUHCview
edas
amea
nsto
increa
seeq
uity
oEquity
associated
with
effic
ienc
y(and
qua
lity)
C8
Rockefeller
Foun
datio
n,Save
theChildren,
UNICEF
andWHO2013
UniversalHealth
Coverage:ACom
mitm
ent
toClose
theGap
[36]
Yes:“in
equity
–un
fairand
avoidable
ineq
ualities”(p.4
andlater)
-Equity
isacentralcon
cern
ofthisrepo
rt:“Thisrepo
rtfocuseson
how
andwhy
ineq
uity
–un
fairandavoidableineq
ualities–shou
ldbe
prioritised
ascoun
triesprog
ress
onthepath
towards
UHC”
(p.4): o
Therepo
rtrefersto
alltypes
andlevelsof
equity
iden
tified
inTable1
oSection2explains
why
equity
isim
portantforUHC
oSection3provides
aconcep
tualframew
orkforassessing
equity
inpathwaysto
UHC,and
then
lesson
sforeq
uitable
pathwaystowards
UHC
oSection4makes
theecon
omiccase
foreq
uitablepathways
towards
UHC
-Therepo
rtspecifies
that“W
ithinhealth
system
s,equityappliesto
the
goalsof
improved
health
outcom
es,equ
ityinfinance,financialrisk
protectio
nandrespon
siveness,as
wellastheob
jectives
ofgo
odqu
ality
andutilisatio
nbasedon
need
”(p.15)
-Associatio
nsof
equity
with
UHCandothe
rconcep
ts:
oUHCview
edas
amea
nsto
achiev
egreater
equity,or
“the
respon
seto”ineq
uities(p.6);andas
necessitating
considerationforeq
uity
throug
hout
reform
processes
oEquity
relatedto
fairne
ss;callsto
“amoral
andethical
perspe
ctive”
(p.4)
Paul et al. International Journal for Equity in Health (2019) 18:195 Page 7 of 21
Table
2Analysisof
theway
equity
isapproached
inglob
alUHCdo
cumen
ts(Con
tinued)
Docum
ent
no.
Source
Title
Explicitde
finition
ofeq
uity?
How
equity
isapproached
inthedo
cumen
t
C9
WHO&WB2014
Mon
itorin
gprog
ress
towards
universalh
ealth
coverage
atcoun
tryandglob
allevels–
Fram
ework,measuresandtargets[25]
No,bu
tde
finition
ofeq
uity
indicatorsof
coverage
andfinancial
protectio
n
-Theframew
orkformon
itorin
gprog
ress
towards
UHCmon
itorin
gof
UHCpu
tsafocu
son
equity
regardingthetwodiscrete
compo
nentsof
health
system
perfo
rmance
(coverageof
health
services
andfinancialprotectio
n),and
recommends
that“M
easures
shou
ldbe
disagg
regatedby
socioecono
micanddemog
raph
icstrata”
(p.5)
-Theglob
alframew
orkprop
oses
threeprimaryelem
ents
for
disag
gregationthat
canbe
measuredcomparablyin
allsettin
gs:
househ
oldincome,expe
nditu
reor
wealth
(coverageof
thepo
orest
segm
entof
thepo
pulatio
nas
comparedwith
riche
rsegm
ents);
placeof
reside
nce(ru
ralo
rurban);and
gend
er(p.6)
-Each
coun
tryisexpe
cted
toaddfurthe
rmeasuresof
service
coverage
andfurthe
req
uity
stratifiersin
orde
rto
tailorUHC
mon
itorin
gto
itscontext(p.10)
-Recommen
dedindicatorscomprisean
aggreg
atean
dan
equity
mea
sures
-Associatio
nsof
equity
with
UHCandothe
rconcep
ts:
oReckon
sthat
“Atthehe
artof
UHCisaco
mmitmen
tto
equity”(p.6)
C10
ILO2014
UniversalHealth
Protectio
n:Prog
ress
todate
andtheway
forw
ard[29]
No
-Mentio
nsthatOOPs
arethemostinequitablesource
ofhealth
financing
(p.2);theirrem
ovalcanhelpprog
ressinterm
sof
“effectiveandequitableaccessto
health
care,affo
rdabilityand
financialprotectio
ninadditio
nto
availabilityof
quality
services”
(p.6)
-Refersto
“ineq
uitiesin
legalh
ealth
coverage
dueto
political,
legislativeandadministrativefailures”(p.2)
-Has
asectionon
“Mov
ingtowardsEq
uity:N
ationalSocial
Protectio
nFloo
rsas
akeystrategy
forachievingun
iversal
coverage
inhe
alth”
-Associatio
nsof
equity
with
UHCandothe
rconcep
ts:
oUHCan
deq
uity
view
edas
twodistinc
taims(p.iii)
oEquity
associated
with
human
rightsto
socialsecurityand
health
andtherigh
ts-based
approache
sun
derpinning
the
need
foreq
uity
andpo
vertyalleviation(p.iii);w
ithsocial
chan
ge,pov
erty
alleviationtheelim
inationof
dep
rivation
(pp.
4,47);with
social
justice(pp.
9,77);with
vulnerab
ility
andsocialexclusion(p.37);w
ithun
iversality
(p.39);w
ithsolid
arity
(p.66);w
ithsocialfairne
ss(p.72);w
ithinclusion(p.111)
oMen
tions
thetrad
e-offbetwee
neq
uity
andqua
lityof
essentialh
ealth
services
(p.45)
C11
WB2015
Going
Universal–How
24Develop
ing
Cou
ntriesAre
Implem
entin
gUniversalHealth
CoverageReform
sfro
mtheBo
ttom
Up[37]
No
-Po
intsrepe
ated
lyto
thetrad
e-offbetwee
neq
uity
inthebe
nefit
packagean
d(fiscal)sustaina
bility
-Associatio
nsof
equity
with
UHCandothe
rconcep
ts:
oEquityrepeatedlyassociated
with
“betterresultsforthe
mon
eyspent”(p.xiv)/
with
efficiencyandeffectiven
ess
oAlsoassociated
with
sustaina
bility,a
ccessibility,q
uality,
integration
;implemen
tability
Paul et al. International Journal for Equity in Health (2019) 18:195 Page 8 of 21
Paul et al. International Journal for Equity in Health (2019) 18:195 Page 9 of 21
Table
2Analysisof
theway
equity
isapproached
inglob
alUHCdo
cumen
ts(Con
tinued)
Docum
ent
no.
Source
Title
Explicitde
finition
ofeq
uity?
How
equity
isapproached
inthedo
cumen
t
equity
infinancing
(pp.
44–45)
-Associatio
nsof
equity
with
UHCandothe
rconcep
ts:
oEquityisapproached
throug
hthelinks
betweenhealth
financing
,UHCgo
alsandinterm
ediate
objectives
–indeed,
equity
inserviceuseisaUHCgo
al,and
thedistrib
utionof
resourcesisaUHCinterm
ediate
objective
oThus
associationof
equitywith
otherU
HCob
jectives/goals:
efficiency,tran
sparen
cyan
daccoun
tability,q
uality,
finan
cialprotection
C15
WHO2016
PublicFinancingforHealth
inAfrica:
from
Abu
jato
theSD
Gs[40]
No
-Associatio
nsof
equity
with
UHCandothe
rconcep
ts:
oEquity
isassociated
with
sustaina
bility
(pp.
8,33),qua
lity
(p.22),efficienc
y(pp.
30,33)
C16
WHO2017
GlobalR
eport:New
Perspe
ctives
onGlobalH
ealth
Spen
ding
forUniversal
Health
Coverage[41]
No
-Associatio
nsof
equity
with
UHCandothe
rconcep
ts:
oEquity
isassociated
with
social
cohe
sion
(p.4),
sustaina
bility
(p.8)
oIntend
sto
prom
ote“equ
itableprog
ress
towards
UHC”
(p.29),thu
sdifferentiatin
gthetw
oconcep
ts
C17
WHO2017
Toge
ther
ontheroad
toun
iversalh
ealth
coverage
–acallto
actio
n[42]
No
-Associatio
nsof
equity
with
UHCandothe
rconcep
ts:
oEquity
isassociated
with
effic
ienc
y(p.14),h
uman
righ
ts(pp.
18,20),g
ender
equa
lity(p.20)
C18
WHO2017
Develop
inganatio
nalh
ealth
financing
strategy:a
referencegu
ide[43]
No
-Associatio
nsof
equity
with
UHCandothe
rconcep
ts:
oCon
side
rsequityin
utilisationor
serviceuserelativeto
need
aspartof
ano
rmativesetof
goa
lsem
bed
ded
inthe
conc
eptof
UHC,tog
ethe
rwith
finan
cial
protectionand
qua
lity;equityin
thedistributionof
health
system
resourcesas
partof
asetof
interm
ediate
objectives,tog
ethe
rwith
effic
ienc
y,tran
sparen
cyan
dacco
untability
(p.1)
oEquity
also
associated
with
effectiven
essandthe
managem
entof
expe
nditu
regrow
th(p.12)
C19
WHO&WB2017
Tracking
universalh
ealth
coverage
:2017
glob
almon
itorin
grepo
rt[43]
No
-Has
alotin
common
with
thefirstglob
almon
itorin
grepo
rton
UHCas
forits
approach
ofeq
uity
(lack
ofdata
preven
ting
comparin
gtheUHCservicecoverage
inde
xacross
keydimen
sion
sof
ineq
uality,linkwith
SDGsandUHC,etc.)
-Associatio
nsof
equity
with
UHCandothe
rconcep
ts:
oTherepo
rtreckon
sthat“Unlesshealth
interventio
nsare
desig
nedto
prom
oteequity,effo
rtsto
attainUHCmay
lead
toimprovem
entsinthenatio
nalaverage
ofservicecoverage
whileinequalitiesworsenatthesametim
e”(p.viii)–
therefore
makingacleardistinctionbetweenUHCan
deq
uity
C20
WHO/Reg
ional
Office
forAfrica
2017
Thestateof
health
intheWHOAfrican
Region
:ananalysisof
thestatus
ofhe
alth,
health
services
andhe
alth
system
sin
the
contextof
theSD
Gs[44]
No
-Therepo
rthigh
lightstheinequitiesbetweenthecountries
oftheWHO
African
region
,and
also
withincountries
-Itoriginallymen
tions
theineq
uitiesin
thecoun
trieshe
alth
security
status
(p.33)
Paul et al. International Journal for Equity in Health (2019) 18:195 Page 10 of 21
Table
2Analysisof
theway
equity
isapproached
inglob
alUHCdo
cumen
ts(Con
tinued)
Docum
ent
no.
Source
Title
Explicitde
finition
ofeq
uity?
How
equity
isapproached
inthedo
cumen
t
-Itno
tices
theintercon
nectionbe
tweenthedifferent
levelsof
ineq
uity:“Theseineq
uitiesin
health
arearesultof
ineq
uitiesin
investmen
tsin
andou
tcom
esfro
mtheseinvestmen
t”(p.83)
-Associatio
nsof
equity
with
UHCandothe
rconcep
ts:
oEquity
isassociated
repe
ated
lywith
sustaina
bility,
effic
ienc
yan
deffectiven
ess;andon
cewith
resource
adeq
uacy
(p.71)
andhu
man
rights(p.84)
oTherepo
rtno
tices
thatthe2030
Agend
aforS
ustainab
leDevelop
men
thas“astrong
focuson
equity”(p.1)
oItalso
states
that
“progresstowards
UHCandtheSD
Gs,
particularlyfro
mtheeq
uity
perspe
ctive”
(p.83),sug
gesting
that
equity
isadimen
sion
ofUHC&SD
Gs
Paul et al. International Journal for Equity in Health (2019) 18:195 Page 11 of 21
Table
3Summaryanalysisof
UHCpo
licydo
cumen
tsin
BeninandSene
gal
Docum
ent
no.
Source
Title
# page
s# occurren
ces
“equ
it*”
# occurren
ces
“equ
al*”
# occurren
ces
“disparit*”
C1
Sene
gal/M
oH2009
PNDS(NHSP)2
009–2018
[46]
8613
55
C2
Sene
gal/M
oH2013
Strategicplan
forthede
velopm
entof
universalh
ealth
insurancein
Sene
gal2013–2017
[47]
127
132
0
C3
Sene
gal/M
oH2017
Sector
Investmen
tPlan
2017–2021[48]
252
40
C4
Sene
gal/M
oHStrategicde
velopm
entplan
oftheAge
ncyforun
iversalh
ealth
insurance[49]
665
216
C5
Sene
gal/M
oH2017
Nationalh
ealth
financing
strategy
(NHFS)[50]
3316
76
C6
Benin/MoH
2010
PNDS(NHSP)2
009–2018
[51]
966
57
C7
Benin/MoH
2015
Nationalh
ealth
financing
strategy
(NHFS)2
016–2020
[52]
4321
11
C8
Benin/Governm
ent2019
Projectdo
cumen
t:Insuranceforthestreng
then
ingof
human
capital(ARC
H)[53]
459
42
Total(ou
tof
8doc
umen
ts):
Note:
Thenu
mbe
rof
occurren
cespresen
tedisthenu
mbe
rof
relevant
occurren
ces:exclud
ingin
references
andinde
x/conten
ts,and
exclud
ingad
verbialu
seof
equa
l*[equ
ally,e
qual
to,etc.]
Paul et al. International Journal for Equity in Health (2019) 18:195 Page 12 of 21
Table
3Summaryanalysisof
UHCpo
licydo
cumen
tsin
BeninandSene
gal(Co
ntinued)
Docum
ent
no.
Levelsof
equity
considered
Type
sof
ineq
uity
considered
(stratifiers)
Broadly
speaking
/un
defined
Social
determ
inants
and/or
health
behaviou
rsand/or
risk
factors
Health
outcom
esHealth
system
sand/or
policies
and/or
distrib
utionof
resources/
fund
s/expe
nditu
re
Accessto
(quality)
healthcare/
services
and/
orcoverage
and/or
useof
services
Fund
ing/
financing
(con
tribution)
Financial
protectio
n(access)and/
orbe
nefit
entitlemen
tand/or
risk
equalisation
Income/
wealth
/po
verty
Education
Und
efined
/othe
rsocio-
econ
omicas-
pects(fo
rmal/in
-form
al,financial
protectio
nsche
mes)
Geo
graphic:
region
sand/or
urban/rural
Gen
der
Age
Culture/
ethn
icity/
religion/
migrants
C1
xx
xx
x
C2
xx
x
C3
xx
xx
C4
xx
xx
C5
xx
xx
xx
x
C6
xx
xx
xx
xx
C7
xx
xx
xx
x
C8
xx
xx
x
Total(ou
tof
8doc
umen
ts):
12
25
85
43
06
52
00
Paul et al. International Journal for Equity in Health (2019) 18:195 Page 13 of 21
Table
4Analysisof
theway
equity
isapproached
inUHCpo
licydo
cumen
tsin
BeninandSene
gal
Docum
ent
no.
Source
Title
Definition
ofeq
uity?
Way
equity
isapproached
inthedo
cumen
t
C1
Sene
gal/M
oH2009
PNDS(NHSP)2009–2018[46]
No
-ThePlan
states
that
morethan
before,equity
inhe
alth
servicedistributionan
dfin
ancial
access
(financingthede
mand-side
)wereprioritised
-Strategies
anno
uncedto
improveeq
uity
inhe
alth
servicedistrib
ution:
oMakingaminim
umhe
althcare
supply
capacityavailable
intheregions
(includ
ingcreatin
gdistrictho
spitals)
oRe
vising
thehe
alth
map
(normsin
term
sof
infrastructure,eq
uipm
entandpe
rson
nelp
erlevel
ofcare)to
makeitmoream
bitio
usin
term
sof
supp
lycapacitiesof
services
/en
surin
gabe
tter
distrib
utionof
health
facilitiesthroug
hout
thecoun
try
oIm
provingtheresource
allocatio
nsystem
(not
furthe
rexplaine
d)-Anu
mbe
rof
measuresareanno
uncedto
reinforcetheregu
latory
functio
nof
theState,includ
ing
regardingissues
ofeq
uity,g
ender,d
iscrim
ination,
andsocial
protection
-Associatio
nsof
equity
with
UHCandothe
rconcep
ts:
oEquity
isview
edas
aprinc
iple
guiding
theim
plemen
tation
oftheNHSP
,tog
ethe
rwith
participation,multisectoriality,transparen
cy,solidarity,and
gend
ero
Ineq
uitiesarealso
associated
with
exclusion
C2
Sene
gal/M
oH2013
Strategicplan
forthede
velopm
entof
universal
health
insurancein
Sene
gal2013–2017
[47]
No
-Thestrategicplan
startsfro
mtheob
servationthat
theevolutionof
thecoun
try’she
alth
system
hasno
tprom
oted
equity
inaccess
tohe
alth
care,hou
seho
ldfinancialprotectio
n,andeq
uity
inhe
alth
financing
;ho
wever,freeandsubsidised
healthcare
initiatives
have
enabledto
increase
equity
-Theplan
refersto
the2012
UNGAresolutio
non
UHCwhich
calls
oneach
UNMem
berStateto
avoid
out-of-pocketpaym
entsandto
finance
itshe
alth
system
throug
hmoreeq
uitableandsupp
ortive
mechanism
s-Theplan
intend
sto
reform
thehe
alth
finan
cing
system
byexpan
dinghe
alth
insuranc
eto
rural
andinform
alsectors,throug
hpromotionof
commun
ity-based
health
insuranc
e(CBHI)and
subsidisationof
prem
iumsforthepo
orest,andthecreatio
nof
theNationalH
ealth
Solidarity
Fund
-Prog
ressiven
essin
health
financing
isto
been
suredthroug
hthede
velopm
entof
inform
ationsystem
sto
scaleco
ntributions
based
onho
useh
olds’ab
ility
topay
forhe
alth
care
(not
furthe
rde
velope
d)-Thelogicalframew
orkof
theplan
hasan
impact
indicatorof
equity
ofaccess,m
easuredthroug
hhe
alth
serviceutilisatio
nrates
-Associatio
nsof
equity
with
UHCandothe
rconcep
ts:
oThevalues
andprinciples
oftheplan
are:solid
arity,
equity
andsocial
justice,
qua
lity,
effic
ienc
y,goo
dgov
erna
nce,
andpartnership
oEquity
isview
edas
abasicprinc
iple
toen
sure
socialinclusion,theinclusionof
thepo
orand
vulnerablegrou
ps,and
equitableaccess
tocare
C3
Sene
gal/M
oH2017
Sector
Investmen
tPlan
2017–2021[48]
No
-In
orde
rto
respon
dto
uneq
uald
istributionof
infrastructures
throug
hout
thecoun
try,theplan
anno
uncesthat
itsprioritieswerede
fined
taking
into
accoun
tthegaps
iden
tifiedby
the“hea
lthan
dsocial
map
”andeq
uity
criteria
with
afocuson
high
-impact
interven
tions
(with
outfurthe
rde
tail)
-Itwillgive
priorityto
twoessentialcom
pone
nts:dem
andfin
ancing
andco
nstruc
tion
ofne
winfrastruc
ture
C4
Sene
gal/M
oH2017
Strategicde
velopm
entplan
oftheAge
ncyfor
universalh
ealth
insurance[49]
No
-Theplan
states
that
respectforeq
uity
isafund
amen
talelemen
tin
improvingaccess
tocare
and
redu
cing
poverty;anditalso
refersto
the2012
UNGAResolutio
non
UHC
-Theplan
recalls
that
theun
iversalh
ealth
insurance(“C
MU”)po
licyisstrong
lyaffirmed
asthestrategy
toen
sure
equitableaccess
toqu
ality
health
care
with
outanyform
ofexclusionfortheen
tirepo
pulatio
nof
Sene
gal,andthat
itisbasedon
thede
velopm
entof
mutualh
ealth
insuranceandthestreng
then
ingof
freehe
althcare
initiatives
-One
ofthemainstrategies
envision
edissupp
ortto
theaffiliation
ofthepoo
rest
(ben
eficiariesof
social
assistance
prog
rammes,including
equalo
pportunity
card
holders)to
CBHIs
-Associatio
nsof
equity
with
UHCandothe
rconcep
ts:
oEquity
ispartof
theAge
ncy’svision
inorde
rto
fight
exclusion,andof
itsvalues
unde
rtheform
Paul et al. International Journal for Equity in Health (2019) 18:195 Page 14 of 21
Table
4Analysisof
theway
equity
isapproached
inUHCpo
licydo
cumen
tsin
BeninandSene
gal(Co
ntinued)
Docum
ent
no.
Source
Title
Definition
ofeq
uity?
Way
equity
isapproached
inthedo
cumen
t
offairan
deq
ualtreatmen
tforeverySene
galese
C5
Sene
gal/M
oH2017
Nationalh
ealth
financing
strategy
(NHFS)[50]
No
-Thestrategy
isbasedon
asituationanalysisthat
emph
asises
theineq
uitable
distributionof
resources,
includ
inghu
man
resources,espe
ciallybe
tweenregion
sandlivingen
vironm
entsbu
talso
betw
eenlevels
ofcare
-In
particular,the
iden
tifiedob
staclesto
equitable
access
tohe
alth
services
are:remoten
ess,isolation,
inadeq
uate
accommod
ationforpe
rson
swith
disabilities,high
costof
health
services,and
lack
ofavailabilityof
health
facilities
-Thecompu
lsorycontrib
utorysche
meto
health
insuranceforem
ployeesin
theprivatesector
isalso
judg
edineq
uitable
-Thestrategy
reckon
sthat
theprincipleof
equity
willbe
clearly
positio
nedin
thecriteria
that
supp
ort
decision
son
theallocation
ofresourcesin
orde
rto
democratizeaccess
tohe
alth
services
-Thestrategy
comprises
four
strategicorientations:
oThefirston
eintend
sto
improvetheavailabilityof
quality
health
services,w
ithafocu
son
ensuring
equitable
access
toqu
ality
health
services
–no
tablythroug
hthe“den
sificationand
democratisationof
thesupp
lyof
health
services”(re
vising
thehe
alth
andsocialmap)
oThesecond
oneintend
sto
expand
protectio
nagainsthe
alth-related
financialrisk,also
with
afocu
son
equity
throug
hprom
otionof
CBH
Isto
theruraland
inform
alsectors,subsidisationof
thecontrib
utionof
thepo
orest,andun
ificatio
nof
governance
mechanism
sof
thevario
usUHC
sche
mes
oThethird
oneintend
sto
target
behaviou
raland
environm
entald
eterminantsof
health
oThefourth
oneintend
sto
raisemoreresources,andim
provetheirefficiency,no
tablythroug
hthe
applicationof
budg
etallocatio
ncriteria
(not
furthe
rexplaine
d)-Associatio
nsof
equity
with
UHCandothe
rconcep
ts:
oSu
staina
ble
dev
elop
men
tne
cessitatestherespectof
theprinciples
ofeq
uity
andgen
der
equa
lity
oThestrategy
isbasedon
avision
ofaSene
galw
here
allp
opulations
have
access
toqu
ality
health
services
basedon
sustainablefinancing
that
respectstheprinciples
ofeq
uity
andsolidarity;
thesearch
foreq
uity
willbe
combine
dwith
theprincipleof
solidarity
toen
sure
thesocial
inclusionof
thepo
orandvulnerablegrou
psin
health
riskcoverage
mechanism
s
C6
Benin/MoH
2010
PNDS(NHSP)2009–2018[51]
No
-Theplan
isbasedon
asituationanalysisthat
pointsto
ineq
uitabledistrib
utionof
staff,as
wellasfinancial
barriersthat
dono
tfavour
equitableaccess
tohe
althcare
-Theplan
intend
sto
give
priorityto
equitable
finan
cing
andsoun
dmanagem
entof
health
expe
nditu
re-Associatio
nsof
equity
with
UHCandothe
rconcep
ts:
oThe20
25vision
oftheplan
intend
sto
ensure
thepe
rmanen
tavailabilityof
quality,equitable
andaccessiblehe
althcare
services
topo
pulatio
nsof
allcateg
ories,basedon
thevalues
ofsolidarity
andrisksharing
C7
Benin/MoH
2015
Nationalh
ealth
financing
strategy
(NHFS)2
016–
2020
[52]
No
-Thesituationanalysispo
intsto
great
geo
graphicald
isparities–no
tablyin
thedistrib
utionof
human
resources–andto
thefragm
entatio
nof
financing
sche
mes
that
lead
toineq
uitableaccess
tohe
althcare
-Thestrategy
isbasedon
seve
ralp
rinc
ipleslin
kedto
equity,including
:equ
itableandeasy
access
toqu
ality
health
care
ataffordablecostsaccordingto
need
s,theavailabilityof
health
care
provisionto
the
entirepo
pulatio
n,solidarity
andrisksharingbasedon
obligationandno
n-exclusion,andprotectio
nagainstfinancialrisk;eq
uitablesourcesof
financing
arelooked
for
-Thestrategy
comprises
threestrategicorientations:
oIm
proveandstream
linetheutilisation
ofresourcesin
thehe
alth
sector
oIm
plem
entthehe
alth
insurancesche
meandintegrateothe
rfinancialprotectio
nsche
mes
oGuarantee
that
thehe
alth
finan
cing
system
iseq
uitable,sustainableandpred
ictable
-Con
cretely,theprop
osed
measuresto
improveeq
uity
are:
oTherevision
oftheMinistryof
Health
’sbud
getallocation
procedu
resto
ensure
equity
and
Paul et al. International Journal for Equity in Health (2019) 18:195 Page 15 of 21
Table
4Analysisof
theway
equity
isapproached
inUHCpo
licydo
cumen
tsin
BeninandSene
gal(Co
ntinued)
Docum
ent
no.
Source
Title
Definition
ofeq
uity?
Way
equity
isapproached
inthedo
cumen
t
efficiency;bu
dget
shou
ldbe
allocatedon
thebasisof
existin
gresourcesandpe
rform
ance,inline
with
andlinkedto
resourcesfro
mcommun
ityfund
ing
oPo
pulatio
ns’con
tributionto
theState-ledhe
alth
insuranc
esche
mein
functio
nof
their
income(and
exem
ptionforthepo
orest)
-Associatio
nsof
equity
with
UHCandothe
rconcep
ts:
oThestrategy
isbasedon
thesamevision
astheNHSP
2009–2018;as
wellason
thefollowing
values:(i)accoun
tabilityandleadership,(ii)eq
uity,socialjustice,ethics
andgo
odgo
vernance,and
(iii)effectiven
essandefficiency
oEquity
repe
ated
lyassociated
with
sustaina
bility
andeffic
ienc
y
C8
Benin/
Governm
ent
2019
Projectdo
cumen
t:Insuranceforthe
streng
then
ingof
human
capital(ARC
H)[53]
Yes:see
next
column
-Theoverallo
bjectiveof
theARC
Hprojectisto
increase
capacity
andaccess
tobasicsocialservices
and
econ
omicop
portun
ities
inasustainableandeq
uitable
way
forBenine
sepe
ople,especially
thepo
orest
-Theprojectcomprises
4packages
ofsocial
protectionservices
(health
insurance,training
,creditand
retirem
ent)to
improvetheim
pact
ofprog
rammes
andeq
uity
inaccess
tobasicservices
-In
thecontextof
theim
plem
entatio
nof
theARC
Hhe
alth
insuranceservice,eq
uity
isapproached
intw
orespects:(i)eq
uity
ofaccess,i.e.facilitatin
gaccess
forallB
eninesecitizen
sto
thepackageof
basic
bene
fits,accordingto
theirindividu
alhe
alth
need
s,and(ii)c
ontributory(vertical)eq
uity,w
hich
aims
toinvolveeach
socialstratum
inthefunctio
ning
oftheARC
Hsystem
accordingto
theirability
topay
-Associatio
nsof
equity
with
UHCandothe
rconcep
ts:
oEquity
associated
with
effic
ienc
y,econ
omiesof
scaleandsustaina
bility
Paul et al. International Journal for Equity in Health (2019) 18:195 Page 16 of 21
broad socio-economic disparities (e.g. formal vs. informalsector, vulnerable populations) are referred to by 6 docu-ments out of 8, while geographic (including rural/urban)inequalities are the most widely used explicit stratifier.However, in the documents reviewed, no mention wasmade to inequity in service quality or due to differences ineducation, age, or cultural aspects. Moreover, the exam-ined country policy documents tend to refer to theprinciple of equity in a quite rhetoric way, in associationwith other broad concepts (e.g. solidarity, social justice)but also predominantly with efficiency and sustainability.The supposedly predominant policy document in each
country, that is the NHSP, covers the period 2009–2018in both countries. The NHSP of Benin reckons the exist-ence of inequitable distribution of staff, as well as finan-cial barriers that do not favour equitable access tohealthcare, and intends “give priority to equitable finan-cing”. It is based on a vision that intends to “ensure thepermanent availability of quality, equitable and access-ible healthcare services to populations of all categories,based on the values of solidarity and risk sharing” (ourtranslation). However, no concrete measure to improveequity is proposed in the NHSP [51]. That of Senegalannounces that “priority is given to the equitable distri-bution of the supply of services and the financing ofhealth demand” and that “the provision of a minimumsupply of care per region and the judicious spatial distribu-tion of diagnostic and treatment facilities will ensure moreequitable care”; this is presumed to be achieved through a“resource allocation system made more equitable” and a“greater attention given to the operationalisation of thehealth map” (our translation). If more concrete strategiesto improve equity are indicated than in the one of Benin,the NHSP of Senegal also refers to equity in a vague, rhet-oric way, as a guiding principle among others such as “par-ticipation, multisectoriality, transparency, solidarity, andgender” [46]. More concrete actions are to be found in thesubsequent Sector Investment Plan that intends to “givepriority to two essential components: demand financingand construction of new infrastructure” [48].Both countries have also issued a national health
financing strategy towards UHC (NHFS). That of Beninputs the emphasis on equity in financing and considersthe need to “find places to collect (taxes, indirect taxes)that meet equity concerns” and to ensure “more equit-able distribution of budget allocations” (our translation)[52]. That of Senegal diagnoses “an inequitable distribu-tion of (human, material and financial) resources” (espe-cially between regions and living environments, but alsobetween levels of care) and states that “the principle ofequity will be clearly positioned in the criteria that sup-port decisions on the allocation of resources in order todemocratise access to health services” (our translation).The strategy comprises four strategic orientations, the
first two having a focus on equity in access to qualityhealthcare and financial protection [50]. However, be-yond those principled statements, none of these plansproposes any concrete action (such as resource alloca-tion criterion) to advance equity.Finally, the two countries have chosen different strat-
egies to increase financial protection coverage: whileSenegal has opted for CBHIs [47, 49], Benin has optedfor a State-led project, called ARCH, which comprisesfor packages of social protection services (health insur-ance, training, credit and retirement) [53].Overall, despite differences in contexts and in political
choices and discourses, the UHC policies of the two coun-tries are quite similar in terms of their approach to equity.Both countries acknowledge important health disparities –especially geographic ones – and assign them to inequitiesin resource allocations and on insufficient financial protec-tion. On the supply side, both countries intend to revisebudget allocation procedures to ensure equity and effi-ciency – yet, the documents examined for Benin do notexplain how to do so, while the UHC policy documents inSenegal mention the “health map” (i.e., the norms in termsof infrastructure, equipment and personnel per level ofcare) as a concrete way to do it [46, 48, 50]. On thedemand side, both countries intend to increase financialhealth coverage by promoting a health insurance schemefor the rural and informal sectors, and subsidising the con-tributions of the poor to those schemes. They also recog-nise the problems arising from the fragmentation offinancing schemes and consider setting up a common pool,but have not yet succeeded in this respect [47, 52]. Finally,both countries are aware of the importance of social deter-minants of health; Senegal intends to act in this respectthrough multisectorial action, while Benin has rather optedfor developing a whole package of social protection pro-grammes through the ARCH project [50, 53].
DiscussionOur study has a number of methodological limitations.It is based mostly on a documentary review, and on apurposeful sample of reports and documents. We havedeliberately excluded documents targeted on equity soas to appraise whether non-specific UHC documentsapprehended this concept. We have based our analysismostly on the documentary review, without complemen-tary methods other than our personal knowledge andexpertise, accumulated during our four-year researchproject and prior experience in the two focus countries.We have not analysed how these documents were pro-duced, but their origin and formulation process couldexplain whether or not equity is taken into account.Our results show that the concept of equity is often
used in an imprecise and even rhetoric manner, both inglobal and in country-specific UHC policy documents.
Paul et al. International Journal for Equity in Health (2019) 18:195 Page 17 of 21
This is true both with respect to the levels of equity con-sidered (access, coverage and use are often used inter-changeably) and to the types of equity considered (withoften undefined “socio-economic” disparities). Financialequity is particularly misunderstood in many documentsunder review: most examined documents confuse equityin resource mobilisation and equity in resource alloca-tion – while actually “[e]quity in financing has to dowith how revenues are raised, not with how the moneyis spent” [39].Our study was based on an analysis of policy docu-
ments – but beyond stated policies, there might be im-portant policy-implementation gaps. Our experience inBenin and Senegal shows that the two countries struggleto improve resource allocation and to increase financialprotection coverage. In Benin, after the notable failure ofthe attempt of the previous government to develop anational health insurance scheme, the current govern-ment’s ARCH project has endured long delays before itstarted to be piloted in July 2019 [54]. In Senegal, at theend of December 2018, only 19% of the total populationbenefitted from health risk coverage through CBHI,against an objective of 26% [55]. According to the recentGlobal monitoring report, the UHC Service CoverageIndex (SDG 3.8.1) was at 39.6 for Benin in 2017 (downfrom 40.2 in 2015) and at 45.4 for Senegal in 2017 (upfrom 43.8 in 2015) [56]. How can that be explained?Whereas equity is a central concept in public health(thus as the policy-making level in the health sector), itis not apprehensible as such by all disciplines, whichmay lead to some difficulties as for translating policesinto practice. Indeed, before they can be implemented,policies have to be translated into legal and institutionalframeworks. However, the notion of equity merely doesnot exist as such in law. In Common Law systems, theterm “equity” refers to a particular set of doctrines andprocedures involved with civil law, which complementthe statutory laws, but with no real connection to themeaning used in public health. In civil law legal systems,equity does not exist as a concept, but is comprehendedthrough other concepts such as equality and non-discrimination, protection of minorities, minimum base,proportionality or ability to pay, or fiscal federalism. Itcan also be addressed through economic and fundamen-tal social rights, including the right to health, whichimply positive obligations on behalf of government. Yet,the choice of the legal concept that will be used to trans-late the equity goal will not be without consequence.Since equity encompasses many dimensions, a number
of questions arise when aiming to increase equity in thecontext of UHC policies. First, which aspects of equityshould be prioritised? For instance, should UHC policiesguarantee basic rights to the whole population, or targetthe poorest (or other disadvantaged groups) first? A
recent narrative review found that the majority of papersreviewed in public health found that UHC programmesshould focus first on increasing coverage and decreasingeconomic barriers to access amongst the most disadvan-taged groups (“progressive universalism”) [9]. However,there is no consensus on how to realise that objective[57]. In particular, the implementation of targeted strat-egies (compared to universal ones) involve importantpitfalls, such as the political unsustainability of thereforms, as well as the fact that “benefits meant exclu-sively for the poor often end up being poor benefits”[58]. Moreover, the levels and types of equity to beprioritised depend on the values of the society in which ittakes place, and should logically vary from one country toanother. Yet, we observe that while global documents con-sider many stratifiers, country-specific documents’ diagno-sis focuses on geographic and urban/rural inequities,which are probably the easiest type of disparities to beapprehended with existing data. Paradoxically, in thetwo countries under study, few concrete interventionsare implemented to improve balance in the allocationof resources, while policies targeting the poorest orthe most vulnerable exist for instance (e.g. freehealthcare for children under five or caesarean sec-tions, subsidisation of the ARCH social health insur-ance in Benin and adhesion to CBHI in Senegal).There is therefore a mismatch between the diagnosisof problems, and the solutions proposed. The urbanbias in political decision in low- and middle-incomecountries has been known for decades [59]. Domesticpolitical interests may probably explain why thehealth insurance policy are high in the politicalagenda of the Presidents of both Benin and Senegal.In Benin, the integrated social protection programmeis designed to strengthen the human capital of thecountry in view of supporting its development, in linewith the neoliberal vision of its government [53]. InSenegal, the choice of the CBHI model – against thetide of the international experience pointing to itslimited potential to progress towards UHC [60] – wasinfluenced by domestic mutualist lobbies supportedby the American cooperation agency [61].Second, once the equity objective has been defined,
the question arises how to translate it into the countrylegal and institutional frameworks? Many alternativesmay be possible in this respect, but the similarities interms of equity objectives between the two studiedcountries – which have however chosen very differentpaths to reach UHC – raises questions about the cap-acity of countries to actually translate global guidelinesinto practice in a context-specific way. The question ofhow to translate a moral imperative into practice hasbeen questioned for decades, as testified by the tensionsaround whether and how to provide “equal opportunity”
Paul et al. International Journal for Equity in Health (2019) 18:195 Page 18 of 21
in society [62]. The development of a UHC policy maybe a strictly political agenda, but it may also be pushedback by constitutional or statutory constraints, inter-national agreements or conventions; the UHC policymay have various degrees of binding forces – the rightto health may be inscribed up to the level of the consti-tution (in which case it creates positive obligations forthe state to secure the effective enjoyment of it). Moregenerally, social rights and the right to health may havedifferent legal values; if there is a legally binding com-mitment towards UHC, citizens could claim it directlyor indirectly before the authorities, especially the courts.The stand-still rule (meaning that when a certain levelof social protection or a right is reached, there is noturning back) may be used to guarantee financial com-mitments. Beyond access, equity in finance should alsobe searched for, implying that the distribution of theburden of financing health services is “fair”, thus refer-ring to the extent to which financing is progressive orregressive i.e. whether the burden falls disproportion-ately on the better-off, or worse-off, in society, relativeto their capacity to contribute [63]. As outlined above,the two countries studied intend to render health finan-cing more progressive and to pool resources at a highlevel, but no major progress has been achieved so far. InBenin, there is still no clear and sustainable mechanismsin place to finance the ARCH project [64]. In Senegal,the legal and institutional frameworks are not totally inline with the UHC policy [65].Third, once formalised, how should the implementa-
tion of equity policies be facilitated? Once again, policiescould be seductive but difficult to translate into appro-priate decrees then implemented, be it for political ortechnical reasons [57], so wide policy-implementationgaps may take place [66]. Thus the content of policydocuments does not necessarily reflect what is done inthe field. The two country-specific cases suggest this islikely to happen as they put emphasis on re-equilibratingresource allocation within the health system, without de-fining allocation criteria or proposing any firm commit-ment to it – except for the reference to the health mapin Senegal. Furthermore, during implementation, UHCpolicies should be closely monitored since they may haveunexpected effects on equity. For instance, a recentstudy on maternal healthcare in Senegal shows thatwhile a demand-side intervention (abolition of user fees)benefitted the poorer households more, thereby reducinginequity, a supply-side intervention (expansion of theavailability of maternal health services) benefitted thericher households more, thereby increasing inequity [67].Finally, it is worth remarking that improving equity
in health necessitates intervention beyond the healthsector, and beyond national frontiers. Indeed, UHC isnot enough to ensure the right to health, and requires
important changes to render the environment health-ier [68]. Besides, national policies which target onlydomestic factors have limited ability to address healthinequities, without engaging with the global politicaleconomy and acting on global health inequity deter-minants [69].
ConclusionOverall, it appears from our study that while equity iswidely referred to in global and country-specific UHC pol-icy documents and seems self-evident, its context-specificinterpretations and applications may vary, and the conceptis often utilised in a rather rhetoric and/or political way.Whereas the concept of equity covers many levels andtypes, and except for very specific ones, many global UHCdocuments fail to define it properly and to comprehendthe breadth of the concept. Consequently, perhaps,country-specific policy documents also take it for grantedand use equity as a broad principle, without defining itproperly and without proposing concrete ways to imple-ment it. In the two countries under study, while UHC pol-icy documents recognise the need to tackle geographicdisparities, they actually fail to define binding rules to allo-cate resources (financial, human, material) in a moreequitable way. As for policies aimed at protecting thepoorest or the most vulnerable, they are either untargeted(e.g. all children under five or all pregnant women, what-ever their socioeconomic status) or face difficulties inidentifying the target population (the poorest) [71, 72]. Anexplanation may be found in the lack of tools that com-prehend other types of inequities. Incidentally, “The use offacility data or other administrative sources presents chal-lenges as they […] typically do not collect variables rele-vant for equity analyses other than geographical location”[43]. Henceforth, collecting routine data disaggregated onthe basis of other stratifiers could be a first step in takingbetter account of equity in UHC policies, and to bettertarget populations most in need of special care. Thiswould contribute to rendering the UHC policies moreeffective and more sustainable. In any case, only strongcollaboration between policymakers, social scientists,financiers and lawyers can tailor UHC policies to specificcountry needs, and help translate them into institutionalframeworks to facilitate their implementation.
AbbreviationsARCH: Assurance pour le renforcement du capital humain (Benin);CBHI: Community-based health insurance; ILO: International LabourOrganisation; MoH: Ministry of Health; NHFS: National health financingstrategies; NHSP: National health sector plan; PNDS: Plan national dedéveloppement sanitaire (NHSP); SDGs: Sustainable Development Goals;UHC: Universal health coverage; WB: World Bank; WHO: World HealthOrganisation
AcknowledgementsWe thank the Wallonia-Brussels Federation for the ARC funding.
Paul et al. International Journal for Equity in Health (2019) 18:195 Page 19 of 21
Authors’ contributionsEP analysed the documents and wrote the first draft of the paper. All authorscontributed to the design of the study, approved the selection of thedocuments reviewed, contributed to the analysis and gave their consent onthe final draft.
FundingThe research was funded through the ARC grant for Concerted ResearchActions, financed by the Wallonia-Brussels Federation.
Availability of data and materialsThe documents reviewed are public.
Ethics approval and consent to participateNot relevant.
Consent for publicationNot relevant.
Competing interestsWe declare we have no competing interests.
Author details1Université de Liège, Faculty of Social Sciences, Place des Orateurs 3, 4000Liège, Belgium. 2Université libre de Bruxelles, School of Public Health,Campus Erasme, Route de Lennik 808, 1070 Brussels, CP 591, Belgium.3Université de Parakou, Faculté des lettres, arts et sciences humaines (FLASH)et Laboratoire de recherches sur les dynamiques sociales et ledéveloppement local (Lasdel), Parakou, Benin. 4University of Thiès, ResearchCenter in Economics and Applied Finance (CREFAT), Thiès, Senegal.5Université de Liège, Faculty of Law, Political Science and Criminology, andTax Institute, Place des Orateurs 3, 4000 Liège, Belgium. 6IRD (French Institutefor Research on Sustainable Development), CEPED (IRD-Université de Paris),Universités de Paris, ERL INSERM SAGESUD, 45 rue des Saints Pères, 75006Paris, France.
Received: 18 July 2019 Accepted: 12 November 2019
References1. World Health Organization. Tracking universal health coverage: first global
monitoring report. Geneva, Switzerland: World Health Organization; 2015.2. World Health Organization. World Health Organization (WHO). Primary
Health Care: Now More than Ever, The World Health Report 2008. [Internet].World Health Organization; 2008 [cited 2017 Nov 13]. Available from: http://www.who.int/whr/2008/en/
3. Kutzin J. Health financing for universal coverage and health systemperformance: concepts and implications for policy. Bull World Health Organ.2013;91(8):602–11.
4. World Health Organization. Making fair choices on the path to universalhealth coverage. Final report of the WHO Consultative Group on Equity andUniversal Health Coverage [Internet]. World Health Organization; 2014 [cited2017 Nov 13]. Available from: http://www.who.int/choice/documents/making_fair_choices/en/
5. O’Connell T, Rasanathan K, Chopra M. What does universal health coveragemean? Lancet Lond Engl. 2014;383(9913):277–9.
6. Norheim OF. Ethical perspective: five unacceptable trade-offs on the path touniversal health coverage. Int J Health Policy Manag. 2015;4(11):711–4.
7. Umeh CA, Feeley FG. Inequitable access to health care by the poor incommunity-based health insurance programs: a review of studies from low-and middle-income countries. Glob Health Sci Pract. 2017;5(2):299–314.
8. Fenny AP, Yates R, Thompson R. Social health insurance schemes in Africaleave out the poor. Int Health. 2018;10(1):1–3.
9. Rodney AM, Hill PS. Achieving equity within universal health coverage: anarrative review of progress and resources for measuring success. Int JEquity Health. 2014;13:72.
10. Roberts MJ, Hsiao WC, Reich MR. Disaggregating the universal coveragecube: putting equity in the picture. Health Syst Reform. 2015;1(1):22–7.
11. Braveman P. What are health disparities and health equity? We needto be clear. Public Health Rep Wash DC 1974. 2014;129 Suppl 2(Suppl 2):5–8.
12. Wagstaff A, van Doorslaer E, Paci P. Equity in the finance and delivery ofhealthcare: some tentative cross-country comparisons. Oxf Rev Econ Policy.1989;5(1):89–112.
13. Cohen AB, Grogan CM, Horwitt JN. The many roads toward achievinghealth equity. J Health Polit Policy Law. 2017;42(5):739–48.
14. Potvin L, Mantoura P, Ridde V. Evaluating equity in health promotion. GlobalPerspectives on Health Promotion Effectiveness. Springer. McQueen D.V.,Jones C.M: In; 2007.
15. McIntyre D, Mooney G. Where now with equity? In: McIntyre D, Mooney G,editors. The economics of health equity [internet]. Cambridge: CambridgeUniversity Press; 2007. p. 249–68. Available from: https://www.cambridge.org/core/books/economics-of-health-equity/where-now-with-equity/F08F2F5CB4DEE82E1576DF486B1BFF58.
16. Whitehead M. The concepts and principles of equity and health. Int JHealth Serv Plan Adm Eval. 1992;22(3):429–45.
17. Commission on Social Determinants of Health. Closing the gap in ageneration: Health equity through action on the social determinants ofhealth. Geneva: World Health Organization; 2008.
18. Braveman PA. Health disparities and health equity: concepts andmeasurement. Annu Rev Public Health. 2006;27:167–94.
19. Braveman PA, Kumanyika S, Fielding J, LaVeist T, Borrell LN, Manderscheid R,et al. Health disparities and health equity: the issue is justice. Am J PublicHealth. 2011;101(S1):S149–55.
20. O’Connell TS, Bedford KJA, Thiede M, McIntyre D. Synthesizing qualitativeand quantitative evidence on non-financial access barriers: implications forassessment at the district level. Int J Equity Health. 2015;14:54.
21. Hall M, Graffunder C, Metzler M. Policy approaches to advancing healthequity. J Public Health Manag Pract. 2016;22:S50–9.
22. Wagstaff A, Paci P, van Doorslaer E. On the measurement of inequalities inhealth. Soc Sci Med. 1991;33(5):545–57.
23. O’Donnell O, van Doorslaer E, Wagstaff A, Lindelow M. Analyzing HealthEquity Using Household Survey Data : A Guide to Techniques and TheirImplementation [Internet]. Washington DC: The World Bank; 2008. Availablefrom: https://openknowledge.worldbank.org/handle/10986/6896 License: CCBY 3.0 IGO.
24. Hosseinpoor AR, Bergen N, Koller T, Prasad A, Schlotheuber A, Valentine N,et al. Equity-oriented monitoring in the context of universal healthcoverage. PLoS Med. 2014;11(9):e1001727.
25. World Health Organization, World Bank. Monitoring progress towardsuniversal health coverage at country and global levels – Framework,measures and targets. 2014 May.
26. Deville C. Same objective, different paths : An analysis of Universal HealthCoverage policies in Benin and Senegal. International Conference on GlobalDynamics of Social Policy Social policy dynamics in (West and Central)Africa; 2018 Oct 25; University of Bremen.
27. Jordan K, Marten R, Gureje O, Daelmans B, Kruk ME. Where is quality inhealth systems policy? An analysis of global policy documents. Lancet GlobHealth. 2018;6(11):e1158–61.
28. Wagstaff A, Eozenou P, Neelsen S, Smitz M. The 2018 health equity andfinancial protection indicators database - overview and insights. World BankGroup; 2018.
29. Scheil-Adlung X. Universal Health Protection: Progress to date and the wayforward. Social Protection Policy Papers, Paper 10. International LabourOrganization (ILO); 2014.
30. World Health Organization. Health Systems Financing – The Path to UniversalCoverage, The World Health Report 2010 [Internet]. World Health Organization;2010 [cited 2017 Nov 13]. Available from: http://www.who.int/whr/2010/en/
31. World Health Organization. World Health Report 2013: Research forUniversal Health Coverage. Geneva, Switzerland; 2013.
32. World Health Organization. Arguing for universal health coverage. Geneva,Switzerland: World Health Organization; 2013.
33. World Health Organization. Universal Health Coverage: Supporting CountryNeeds. 2013.
34. World Health Organization and World Bank. WHO/World Bank Ministerial-levelMeeting on Universal Health Coverage 18-19 February 2013, WHOheadquarters, Geneva, Switzerland. Report on the ministerial level roundtableon Universal Health Coverage [Internet]. Geneva: WHO/World Bank; 2013.
35. Giedion U, Alfonso EA, Diaz Y. The impact of universal coverage schemes inthe developing world : a review of the existing evidence. Universal HealthCoverage (UNICO) studies series ; no. 25 [Internet]. Washington D.C. : TheWorld Bank; 2013 [cited 2017 Nov 13]. Available from: http://documents.
Paul et al. International Journal for Equity in Health (2019) 18:195 Page 20 of 21
36. Brearley L, Marten R, O’Connell T. Universal health coverage: a commitmentto close the gap. New York: The Rockefeller Foundation, Save the Children,UNICEF and the World Health Organization; 2013.
37. Cotlear D, Nagpal S, Smith O, Tandon A, Cortez R. Going universal – how 24developing countries are implementing universal health coverage reformsfrom the bottom up [internet]. Washington, DC: The World Bank; 2015[cited 2017 Nov 13]. Available from: http://documents.worldbank.org/curated/en/936881467992465464/pdf/99455-PUB-Box393200B-OUO-9-PUBDATE-9-28-15-DOI-10-1596-978-1-4648-0610-0-EPI-210610.pdf
38. WHO/ regional office for Africa. The African Health Monitor Special issue:Universal Health Coverage. 2015.
39. McIntyre D, Kutzin J. Health financing country diagnostic: a foundationfor national strategy development [Internet]. World Health Organization;2016 [cited 2017 Dec 18]. Available from: http://www.who.int/iris/handle/10665/204283
40. World Health Organization. Public Financing for Health in Africa: from Abujato the SDGs. Geneva, Switzerland; 2016. Report No.: WHO/HIS/HGF/Tech.Report/16.2.
41. World Health Organization. Global Report: New Perspectives on Global HealthSpending for Universal Health Coverage. World Health Organization; 2017.
42. World Health Organization. Together on the road to universal healthcoverage: a call to action. Geneva, Switzerland: World Health Organization;2017. Report No.: WHO/HIS/HGF/17.1.
43. Kutzin J, Witter S, Jowett M, Bayarsaikhan D. Developing a national healthfinancing strategy: a reference guide. Health financing guidance series no 3.World health Organization. 2017.
44. World Health Organization, World Bank. 2017;2017.45. WHO Regional Office for Africa. The state of health in the WHO African
region: an analysis of the status of health, health services and healthsystems in the context of the sustainable development goals. Brazzaville:world health Organization; 2018.
46. République du Sénégal, Ministère de la santé et de la prévention. Plannational de développement sanitaire PNDS 2009-2018. 2009.
47. Ministère de la Santé et de l’Action sociale. Plan stratégique de développementde la Couverture Maladie Universelle au Sénégal 2013-2017. 2013.
48. République du Sénégal Ministère de la Santé et de l’Action sociale.Programme d’investissements sectoriels 2017-2021. 2017.
49. Ministère de la Santé et de l’Action sociale, Agence de la CouvertureMaladie Universelle. Plan stratégique de développement de l’Agence de laCouverture Maladie Universelle 2017-2021. 2017.
50. République du Sénégal, Ministère de la Santé et de l’Action sociale (MSAS).Stratégie nationale de financement de la santé (SNFS) pour tendre vers lacouverture sanitaire universelle 2017.
51. République du Bénin, Ministère de la Santé. Plan national dedéveloppement sanitaire 2009-2018. 2010.
52. Ministère de la Santé. Stratégie Nationale de Financement de la Santé pourla Couverture sanitaire Universelle du Bénin 2016–2022 (SNFS). 2015.
53. Présidence de la République du Bénin. Assurance pour le Renforcement duCapital Humain (ARCH). Fiche de projet 2017.
54. Deville C, Fecher F, Poncelet M. L’Assurance pour le renforcement du capitalhumain (ARCH) au Bénin : processus d’élaboration et défis de mise enœuvre. Rev Fr Aff Soc. 2018;1:107–23.
55. Agence de la Couverture Maladie Universelle, Direction de l’Assurancemaladie. Rapport de performance de l’année 2018. Ministère de la Santé etde l’Action sociale; 2019 Jan.
56. World Health Organization. Primary Health Care on the Road to UniversalHealth Coverage (conference edition). World Health Organization; 2019.
57. Paul E, Fecher F, Meloni R, van Lerberghe W. Universal health coverage infrancophone sub-Saharan Africa: assessment of Global Health experts’confidence in policy options. Glob Health Sci Pract. 2018;6(2):260.
58. Sen A. The Political Economy of Targeting. In: Public Spending and thePoor: Theory and Evidence [Internet]. Johns Hopkins University Press for theWorld Bank. Baltimore, MD: van de Walle, Dominique, and Kimberly Nead;1995. p. 11–24. Available from: documents.worldbank.org/curated/en/404991468778782212/pdf/multi0page.pdf.
59. Lipton M. Why poor people stay poor: urban Bias in world development.Cambridge, MA: Harvard University Press; 1977.
60. Mathauer I, Mathivet B, Kutzin J. Community based health insurance: Howcan it contribute to progress towards UHC? Health Financing Policy Brief No
3 [Internet]. World Health Organization; 2017 [cited 2017 Nov 13]. Availablefrom: http://apps.who.int/iris/bitstream/10665/255629/1/WHO-HIS-HGF-PolicyBrief-17.3-eng.pdf?ua=1
61. Caffin J-H. L’aide au développement et le financement basé sur laperformance : quelle performativité ? Analyse du processus deconceptualisation et de diffusion du financement basé sur la performancedans la gestion des systèmes de santé africains par la Banque Mondiale etl’USAID. Etude du cas du Programme national de financement basé sur lesrésultats du Ministère de la Santé du Sénégal. [Paris]: Ecole Doctorale deManagement Panthéon-Sorbonne; 2018.
62. Rawls J. Justice as fairness: a restatement. Kelly: Belknap Press. Erin L; 2001.63. Jowett M, Kutzin J. Raising revenues for health in support of UHC: strategic
issues for policy makers. Health Financing Policy Brief n°1, WHO/HIS/HGF/PolicyBrief/15.1 [Internet]. World Health Organization; 2015 [cited 2017 Nov13]. Available from: http://apps.who.int/iris/bitstream/10665/192280/1/WHO_HIS_HGF_PolicyBrief_15.1_eng.pdf?ua=1
64. Paul E, Sambieni NE, Wangbe J-P, Fecher F, Bourgeois M. Fiscal challengeson the path towards universal health coverage: the case of Benin. Mimeo,University of Liege; 2019.
65. Badiane M-C, Bourgeois M, Dioh A. Financing Universal Health Coverage inSenegal: Why and how lawyers must be involved to reach the financingobjectives. Mimeo, University of Saint-Louis (Senegal); 2018.
66. Ridde V. ‘The problem of the worst-off is dealt with after all other issues’:the equity and health policy implementation gap in Burkina Faso. Soc SciMed 1982. 2008 Mar;66(6):1368–78.
67. Parmar D, Banerjee A. How do supply- and demand-side interventionsinfluence equity in healthcare utilisation? Evidence from maternalhealthcare in Senegal Soc Sci Med. 2019;241:112582.
68. Ooms G, Brolan C, Eggermont N, Eide A, Flores W, Forman L, et al. Universalhealth coverage anchored in the right to health. Bull World Health Organ.2013;91(1):2–2A.
69. McNamara CL. Relieving the tension between national health equity strategiesand global health equity. Scand J Public Health. 2019;47(6):608–10.
70. Coady D, Grosh M, Hoddinott J. Targeting of transfers in developingcountries : review of lessons and experience [Internet]. The World Bank;2004 [cited 2019 Jul 11]. Available from: http://documents.worldbank.org/curated/en/464231468779449856/Targeting-of-transfers-in-developing-countries-review-of-lessons-and-experience
71. Deville C, Escot F, Ridde V, Touré L. Les processus d’identification des pluspauvres à l’épreuve du terrain : Une comparaison Bénin-Mali-Sénégal: InRoskilde University; 2018.
72. Kutzin J, Witter S, Jowett M, Bayarsaikhan D. Developing a national healthfinancing strategy: a reference guide. Health Financing Guidance no.3[Internet]. World Health Organization; 2017 [cited 2017 Dec 18]. Availablefrom: http://apps.who.int/iris/handle/10665/254757
Publisher’s NoteSpringer Nature remains neutral with regard to jurisdictional claims inpublished maps and institutional affiliations.
Paul et al. International Journal for Equity in Health (2019) 18:195 Page 21 of 21