How to integrate surgery in the treatment of patients with liver-only metastatic disease Dimitri Dorcaratto MD, PhD, FEBS Department of Surgery. Liver-Biliary and Pancreatic Unit Hospital Clínico. University of Valencia
Transcript
How to integrate surgery in thetreatment
of patients with liver-onlymetastatic disease
Dimitri Dorcaratto MD, PhD, FEBSDepartment of Surgery. Liver-Biliary and Pancreatic UnitHospital Clínico. University of Valencia
DISCLOSURE
Nothing to disclose
Should we integrate surgery in the treatmentof patients with liver-only metastatic disease?
www.livermetsurvey-arcad.org
24,925 resected
1361 not resected
December 2016: 302 centers, 69 countries
p = < 0.001
Should we integrate surgery in the treatmentof patients with liver-only metastatic disease?
Should we integrate surgery in the treatmentof patients with liver-only metastatic disease?
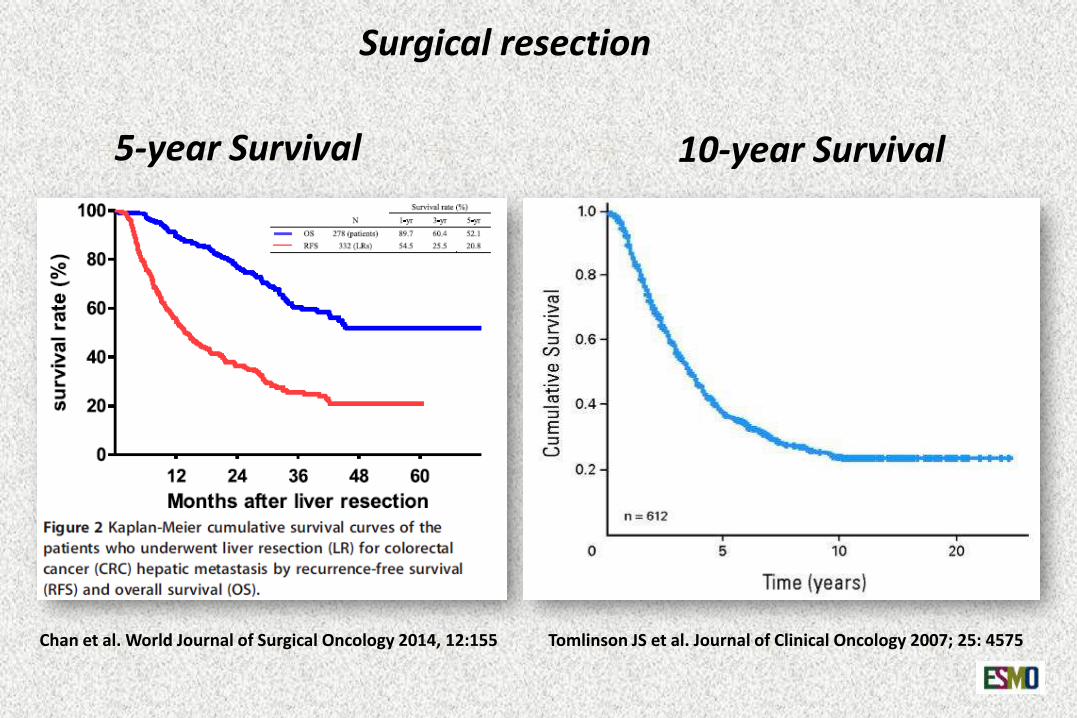
Surgical resection
Chan et al. World Journal of Surgical Oncology 2014, 12:155 Tomlinson JS et al. Journal of Clinical Oncology 2007; 25: 4575
5-year Survival 10-year Survival
Keys • Primary tumour under control
• Complete resection (R0)
• Liver remnant– Normal liver ≥ 25 %
– Neoadjuvant Chemo ≥ 30 %
– Cirrhosis ≥ 40 %
Surgical resection offers a substantial chance of cure
1. Diagnosis and treatment: Multidisciplinary Board
2. Surgical techniques: Anatomy and Technology
3. New strategies and new therapies
Keys
Surgical resection offers a substantial chance of cure
MULTIDISCIPLINARY BOARD
• Diagnostic work-up• Best strategy discussion• Selection for surgical approach• Timing for surgery• Feed-back results
RADIOLOGY
GE
PATHOLOGY
ONCOLOGY
SURGERY
Adam R. et al. Cancer Treatment Reviews 41 (2015) 729–741
ESMO GUIDELINES, 2016
Integrating surgery and oncology
• R0 resection achievable
• Liver remnant adequate
Integrating surgery and oncology
ESMO GUIDELINES, 2016
ESMO GUIDELINES, 2016
Integrating surgery and oncology
• R0 resection achievable
• Liver remnant adequate
• N status of primary
• Disease free interval
• Number of lesions
• Diameter
• CEA
• Extrahepatic disease
• Biology
Goal of preoperative evaluation
Identify potencially resectable patients
Goal of preoperative evaluation
Identify potencially resectable patients
Keys • Primary tumour under control
• Complete resection (R0)
• Liver remnant– Normal liver ≥ 25 %
– Neoadjuvant Chemo ≥ 30 %
– Cirrhosis ≥ 40 %
Identify potencially resectable patients
ESMO GUIDELINES, 2016
Identify potencially resectable patients
ESMO GUIDELINES, 2016
Identify potencially resectable patients
ESMO GUIDELINES, 2016
Identify potencially resectable patients
ESMO GUIDELINES, 2016
Goal of preoperative evaluation
Identify potencially resectable patients
1. Define the number and segmental distribution of LM
2. Determine surgical resectability
3. Identify extra-hepatic disease
1. Computed tomography
2. Magnetic Resonance Imaging
3. FDG-Positron Emission Tomography
Stepwise imaging approach
1. Define the number and segmental distribution of LM
2. Determine surgical resectability
3. Identify extra-hepatic disease
PREOPERATORY IMAGING
• CT-scan
• MRI
INTRAOPERATORY IMAGING
• INTRA-OPERATIVE ULTRASONOGRAPHY
• FDG-PET
Determine surgical resectability
CT-scan
number and segmental distribution of LM
CT-scanContrast enhancementArterial and portal phases
CRCLM:HypovascularRim enhancement washed outon later phases
Limitations:Exposure to ionizing radiationReactions to iodinated contrastSub-centimetre lesions
7
8
4A 2
7
8
4A 2
8
4A 2/3
7
1
2/34A/B
7
8
34B
8/5
7/6
3
5
6
5
6
5
66
MRI
• No ionizing radiation• Higher contrast resolution• Better for lesions < 1cm• Better steatosis or changes due to chemotherapy
IOUS + surgical exloration may changethe planned surgery up to 20 %
Preoperative evaluation and imaging
Surgical elegibility
1. Complete resection of all lesions
2. Free margin resection (R0)
3. Adequate functional liver remnant
4. Fitness for major abdominal surgery
Liver remnant
Normal liver ≥ 25 %
Neoadjuvant Chemo ≥ 30 %
Cirrhosis ≥ 40 %
Preserved inflow, outflow, biliarydrainage
Preoperative evaluation and imaging
Surgical elegibility
1. Complete resection of all lesions
2. Free margin resection (R0)
3. Adequate functional liver remnant
4. Fitness for major abdominal surgery
Preoperative evaluation and imaging
Surgical elegibility
1. Complete resection of all lesions
2. Free margin resection (R0)
3. Adequate functional liver remnant
4. Fitness for major abdominal surgery
Clinical Scenarios
Resectable M1and fit for surgery
Non-resectable M1 but fit for surgery Conversion surgery after combined therapies
Unresectable M1 or unfit for surgery
Resectable M1 in patients
fit for surgery
Surgical technique
ANATOMY
and
TECHNOLOGY
Management of colorectal cancer presenting with synchronous liver metastasesSiriwardena AK et al. Nature Reviews Clinical Oncology 2014; 11: 446–459
The Brisbane 2000 terminology of hepatic anatomy and resections.The terminology committee of the IHPBA.Journal: HPB 2000;2:333-339 http://www.ahpba.org/liverterms.php
Liver anatomy
Retractor Kent / Makuuchii
Argon Beam Coagulator
Intra-operativeultrasonography
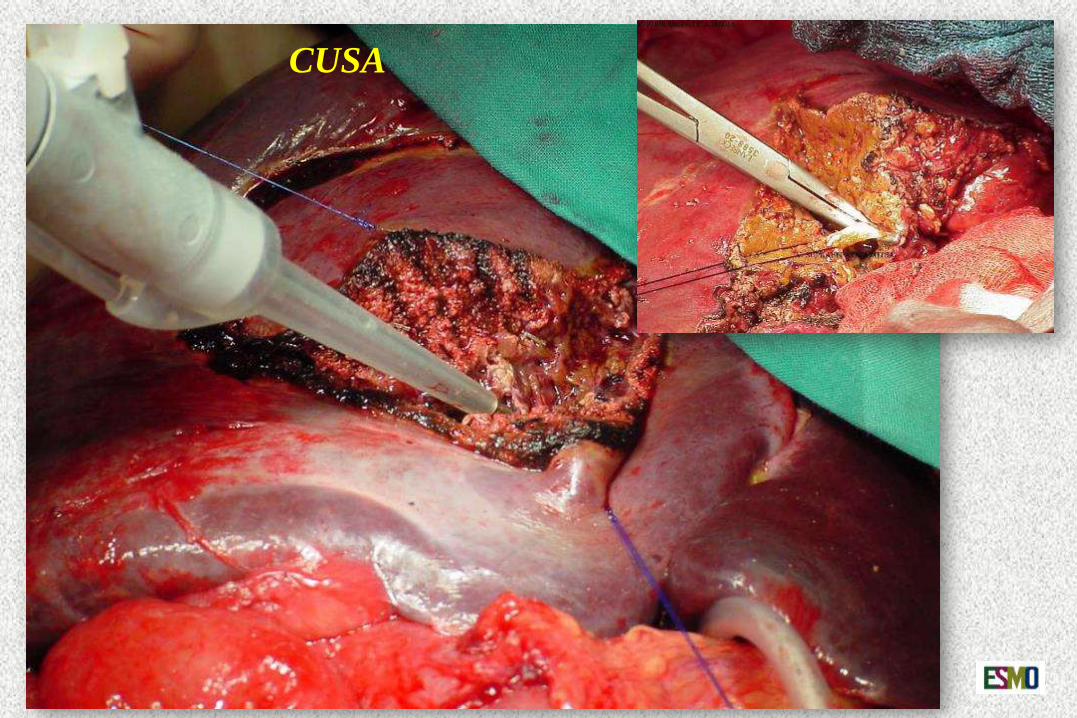
CUSA
Tissuelink®
CUSA
Open approach
Laparoscopic approach
Laparoscopic approach
Surgical standards
MORBIDITY < 30 %
MORTALITY < 5 %
Goal anatomical knowledge and technology
Non-resectable M1 in patients fit
for surgery
Strategies
✓Neoadjuvant Chemotherapy
✓Radiofrequency ablation
✓Portal embolization
✓Two-stage hepatectomy
✓Combinations
M1 UNRESECTABLE M1 RESECTABLE
Chemo
NEOADJUVANT CHEMOTHERAPY
Conversion is the goal
M1 UNRESECTABLE M1 RESECTABLE
Chemo
NEOADJUVANT CHEMOTHERAPY
Conversion is the goal
M Karoui, et al. Ann Surg vol 243, Number 1; January 2006 and Folprecht G. Eur J Cancer. 2011 Sep;47 Suppl 3:S52-60.
RADIOFREQUENCY ABLATION
RADIOFREQUENCY ABLATION
RADIOFREQUENCY ABLATION
RADIOFREQUENCY ABLATION
PORTAL EMBOLIZATION
A B
TWO STAGE HEPATECTOMY
± portal embolization
5-Year S32-64 %
Median survival
24-44 m
Drop-out35 %
Torzilli G et al. Liver Cancer 2017
Fernando A. Alvarez, Jose Iniesta, Jose Lastiri, Marina Ulla, Fernando Bonadeo Lassalle y Eduardo de Santibañes. Cir Esp 2011; 89 (10):645-649
Associated liver partition and portal vein ligation for staged hepatectomy (ALPPS)
• Two-stage hepatectomy with very short interval • Minimizes the drop-out risk• Extraordinarily rapid hypertrophy of the FRL (10 days) • Rescue in patients with portal embolization failure
Clearance of the FRL+ portal vein ligation+ liver parenchyma division
Hepatectomy when the FRLis considered to be large enough