Auris·Nasus·Larynx (Tokyo) 12 (Suppl. I) S 21-S 25, 1985 HOW TO REMOVE, PROCESS, AND STUDY THE TEMPORAL BONE WITH THE ENTIRE EUSTACHIAN TUBE AND ITS ACCESSORY STRUCTURES: A METHOD FOR HISTOPATHOLOGICAL STUDY Isamu SANDO, M.D., D.M.S.,1,2 William DOYLE, Ph.D./,3 Hideji OKUNO, M.D., D.M.S.,1,2 Tetsuo TAKAHARA, M.D., D.M.S.,1.2 Masanori KITAJIRI, M.D., D.M.S.,1,2 and William John COURY lIP 1 Department of Otolaryngology, University of Pittsburgh School of Medicine, 2Department of Otolaryngology, Eye and Ear Hospital of Pittsburgh, and 3Children's Hospital of Pittsburgh, Pittsburgh, Pennsylvania 15213, U.S.A. A very important contribution to the study of otitis media, one of the diseases most often seen in pediatric patients, is the collection and study of temporal bone specimens which include the entire Eustachian tube. During the last few years, we have collected, processed, and studied more than 100 such specimens. Through these experiences, our technique has become so refined that we have some important suggestions to make to otologists who are interested in the histological study of otitis media as well as in the pathology of the Eustachian tube and its relation to middle ear abnormalities. This report describes the method we have found to be most successful for the study of Eustachian tube abnormalities and their relationship to middle ear effusion. Since 1981, we have routinely removed and processed temporal bone specimens which include the entire Eustachian tube (ET) and its accessory structures (the ET cartilage, ET glands, tensor veli palatini muscle (TV PM), levator veli palatini muscle (L VPM), hamulus, etc.) and studied the anatomical and patho- This study was supported by Research Grant RO I 16337-04 from the National Institute of Neurological and Communicative Disorders and Stroke, National Institutes of Health. Request reprints to: Isamu Sando, M.D., D.M.S., Director, Division of Otopathology, Department of Otolaryngology, Eye and Ear Hospital of Pittsburgh, 230 Lothrop Street, Pittsburgh, Pennsylvania 15213, U.S.A. logical evidence for the role of ET abnormali- ties in pathogenesis of middle and inner ear abnormalities, particularly middle ear effusion (MEE). In our removal and study of more than 100 such specimens, we have recognized several factors important to the successful procurement and evaluation of histological specimen of the ET. (We have also identified several factors in ET dysfunction important for the study of otitis media (OM) and other inner and middle ear disorders.) This paper reports the techniques we cur- rently use to remove the temporal bone with the ET attached, to process the specimens so that high-quality histology sections are ob- tained, and to evaluate the histological find- ings observed in these sections. Removing the Temporal Bone Specimens After the brain is removed, the skull base is incised with a Stryker saw approaching from the cranial side and cutting inferiorly, to remove most of the petrous portion of the temporal bone and sphenoid bone in one piece from the preferred side. To be included in this block and seen on its cranial surface are the internal auditory canal, medial two thirds of the ala major (which contains the foramen ovale, foramen spinosum, and fora- men rotundum), almost all of the ala minor, anterior and posterior clenoid processes, fossa hypophysialis and anterior part of the
Transcript
Auris·Nasus·Larynx (Tokyo) 12 (Suppl. I) S 21-S 25, 1985
HOW TO REMOVE, PROCESS, AND STUDY THE TEMPORAL BONE WITH THE ENTIRE EUSTACHIAN
TUBE AND ITS ACCESSORY STRUCTURES: A METHOD FOR HISTOPATHOLOGICAL STUDY
Isamu SANDO, M.D., D.M.S.,1,2 William DOYLE, Ph.D./,3 Hideji OKUNO, M.D., D.M.S.,1,2 Tetsuo TAKAHARA, M.D., D.M.S.,1.2 Masanori KITAJIRI, M.D., D.M.S.,1,2 and William John COURY lIP
1 Department of Otolaryngology, University of Pittsburgh School of Medicine, 2Department of Otolaryngology, Eye and Ear Hospital of Pittsburgh, and
3Children's Hospital of Pittsburgh, Pittsburgh, Pennsylvania 15213, U.S.A.
A very important contribution to the study of otitis media, one of the diseases most often seen in pediatric patients, is the collection and study of temporal bone specimens which include the entire Eustachian tube. During the last few years, we have collected, processed, and studied more than 100 such specimens. Through these experiences, our technique has become so refined that we have some important suggestions to make to otologists who are interested in the histological study of otitis media as well as in the pathology of the Eustachian tube and its relation to middle ear abnormalities. This report describes the method we have found to be most successful for the study of Eustachian tube abnormalities and their relationship to middle ear effusion.
Since 1981, we have routinely removed and processed temporal bone specimens which include the entire Eustachian tube (ET) and its accessory structures (the ET cartilage, ET glands, tensor veli palatini muscle (TV PM), levator veli palatini muscle (L VPM), hamulus, etc.) and studied the anatomical and patho-
This study was supported by Research Grant RO I 16337-04 from the National Institute of Neurological and Communicative Disorders and Stroke, National Institutes of Health.
Request reprints to: Isamu Sando, M.D., D.M.S., Director, Division of Otopathology, Department of Otolaryngology, Eye and Ear Hospital of Pittsburgh, 230 Lothrop Street, Pittsburgh, Pennsylvania 15213, U.S.A.
logical evidence for the role of ET abnormalities in pathogenesis of middle and inner ear abnormalities, particularly middle ear effusion (MEE). In our removal and study of more than 100 such specimens, we have recognized several factors important to the successful procurement and evaluation of histological specimen of the ET. (We have also identified several factors in ET dysfunction important for the study of otitis media (OM) and other inner and middle ear disorders.)
This paper reports the techniques we currently use to remove the temporal bone with the ET attached, to process the specimens so that high-quality histology sections are obtained, and to evaluate the histological findings observed in these sections.
Removing the Temporal Bone Specimens After the brain is removed, the skull base
is incised with a Stryker saw approaching from the cranial side and cutting inferiorly, to remove most of the petrous portion of the temporal bone and sphenoid bone in one piece from the preferred side. To be included in this block and seen on its cranial surface are the internal auditory canal, medial two thirds of the ala major (which contains the foramen ovale, foramen spinosum, and foramen rotundum), almost all of the ala minor, anterior and posterior clenoid processes, fossa hypophysialis and anterior part of the
S22 I. SANDO et ai.
clivus. The lateral margin of the block should be the most lateral portion of the petrous bone and the medial margin of the block should be along the midline of the skull in the sagittal plane. The cutting angle is perpendicular to the floor of the anterior or middle cranial fossa.
After cutting the skull base, from the cranial side, through the slit-like spaces made in the anterior cranial fossa, the posterior part of the palatine bone, pterygoid process of the sphenoid bone, and the posterior end of the alveolar process of the maxillary bone are severed by the saw and included in the removed specimen. Because the length of this cut (from the anterior cranial fossa to the oral cavity) is so long, we devised a special long-bladed saw to reach the mucous membrane of the palate from above.
After all the bony tissues between the skull base and the posterior part of the oral cavity just mentioned have been severed, a pair of straight, long blunt scissors is inserted through the anterior half of the slit cut under the anterior half of the specimen. The mucous membrane of the hard and soft palates is then cut so that, without damaging the mucosal layer, the intact soft palate as well as the ET and its surrounding structures are included in the temporal bone specimen. Then, the specimen is grasped firmly with a lion-jawed forceps and pulled into the cranial cavity. At this time, the soft tissues under the temporal bone are separated from the specimen. Finally, the internal carotid artery and the internal maxillary artery are ligated.
When properly removed, the specimen includes the entire internal auditory canal, inner ear, middle ear (ME), tympanic membrane, ET, ET cartilage, ET glands, TVPM, L VPM, hamulus, and soft and hard palates. In addition, when the removal has been performed properly, it does not disturb the external configuration of the head, nor does it impair embalming procedures.
Histological Processing The human temporal bone with the ET and
accessory structures attached is processed as
follows: Bone processing (requires 6 to 8 months) 1. Upon removal of the temporal bone
specimen at autopsy, it is placed in 1O/;; formalin for fixation. Change to fresh formalin the next day.
2. Two weeks later, on a Tuesday, rinse the bone in running tap water for 24 hr.
3. For decalcification, the specimen is placed in 5/;; trichloracetic acid (TCA) on Wednesday; the solution is changed every Monday, Wednesday, and Friday for 2 to 3 months (month for infant specimen). A test to detect the end point of decalcification should be done on Wednesday at the beginning of the 4th week in TCA (3rd week for an infant bone).
A) If the test is positive, repeat each following Wednesday until negative.
B) If test is negative, repeat on following Friday and Monday.
C) A total of 4 negative tests is needed before further processing may occur.
4. Wash in running tap water for 24 hr .......................... Monday
5. Trim bone, clean the external auditory canal. ..................... Tuesday
6. 5/;; sodium sulfate at 9: 00 A.M. .......................... Tuesday
7. Distilled water at 4: 30 P.M. .......................... Tuesday
13. Store in cedarwood oil . . . . . .. Friday Mounting 1. Soften the bottom of the block in
ether-alcohol. 2. Score the bottom of the block with a
knife. 3. Attach the block to the holder with
12~--:; celloidin, using pressure. 4. Place the specimen into cedarwood oil. 5. If specimen is to be stored for longer
than 2 years, put into 80% alcohol after one week.
Cutting The specimen in the celloidin block is cut vertically at right angles to the long axis of the petrous bone. Usually the sections are cut at a thickness of 20 ,urn, resulting in about 2,500 to 3,000 vertical sections. Every 20th vertical section for the temporal bone portion and every 40th vertical section for the ET portion is separated for staining; the remainder of the sections are stored in 80% alcohol solution.
Staining The sections separated as just described are stained with hematoxylin and eosin.
Mounting The stained tissue sections are mounted on glass slides in a uniform position and are kept in order by their serial section numbers to facilitate subsequent microscopic examination.
Study of Serial Sections Using the special worksheets we developed,
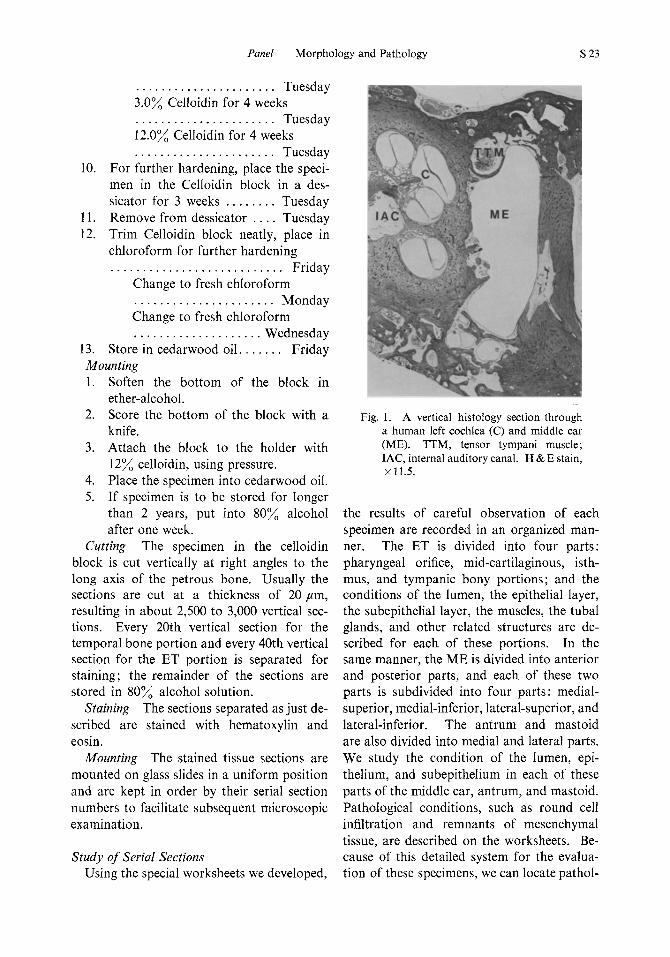
Fig. 1. A vertical histology section through a human left cochlea (C) and middle ear (ME). TIM, tensor tympani muscle; lAC, internal auditory canal. H & E stain, x 11 .5.
the results of careful observation of each specimen are recorded in an organized manner. The ET is divided into four parts : pharyngeal orifice, mid-cartilaginous, isthmus, and tympanic bony portions; and the conditions of the lumen, the epithelial layer, the subepithelial layer, the muscles, the tubal glands, and other related structures are described for each of these portions. In the same manner, the ME is divided into anterior and posterior parts, and each of these two parts is subdivided into four parts: medialsuperior, medial-inferior, lateral-superior, and lateral-inferior. The antrum and mastoid are also divided into medial and lateral parts. We study the condition of the lumen, epithelium, and subepithelium in each of these parts of the middle ear, antrum, and mastoid. Pathological conditions, such as round cell infiltration and remnants of mesenchymal tissue, are described on the worksheets. Because of this detailed system for the evaluation of these specimens, we can locate pathol-
S24 I. SANDO et al.
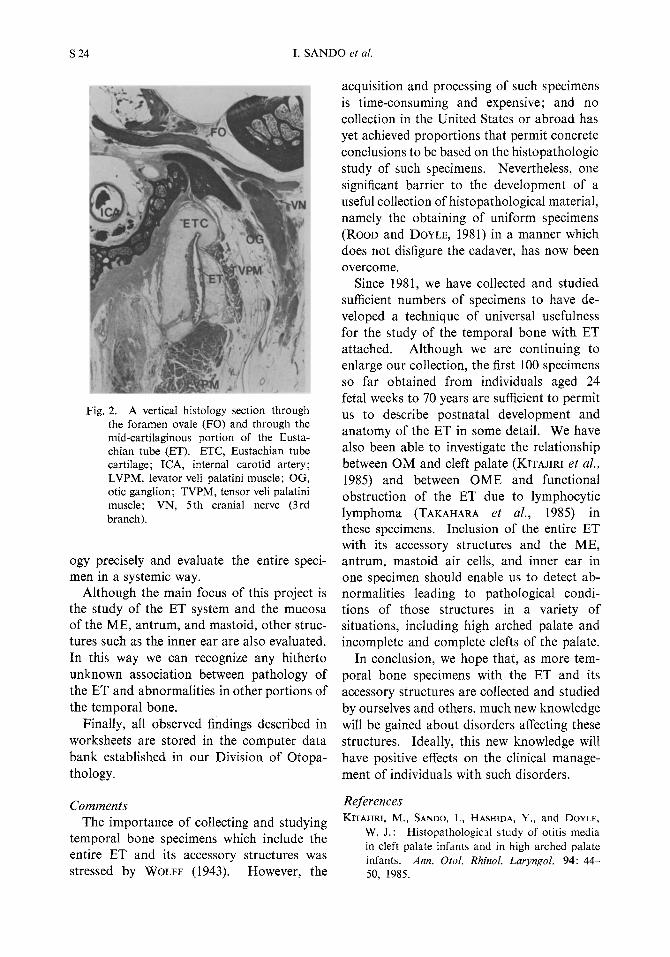
Fig. 2. A vertical histology section through the foramen ovale (FO) and through the mid-cartilaginous portion of the Eustachian tube (ET). ETC, Eustachian tube cartilage; ICA, internal carotid artery; LVPM, levator veli palatini muscle; OG, otic ganglion; TVPM, tensor veli palatini muscle; VN, 5th cranial nerve (3rd branch).
ogy precisely and evaluate the entire specimen in a systemic way.
Although the main focus of this project is the study of the ET system and the mucosa of the ME, antrum, and mastoid, other structures such as the inner ear are also evaluated. In this way we can recognize any hitherto unknown association between pathology of the ET and abnormalities in other portions of the temporal bone.
Finally, all observed findings described in worksheets are stored in the computer data bank established in our Division of Otopathology.
Comments The importance of collecting and studying
temporal bone specimens which include the entire ET and its accessory structures was stressed by WOLFF (1943). However, the
acquisition and processing of such specimens is time-consuming and expensive; and no collection in the United States or abroad has yet achieved proportions that permit concrete conclusions to be based on the histopathologic study of such specimens. Nevertheless, one significant barrier to the development of a useful collection of histopathological material, namely the obtaining of uniform specimens (ROOD and DOYLE, 1981) in a manner which does not disfigure the cadaver, has now been overcome.
Since 1981, we have collected and studied sufficient numbers of specimens to have developed a technique of universal usefulness for the study of the temporal bone with ET attached. Although we are continuing to enlarge our collection, the first 100 specimens so far obtained from individuals aged 24 fetal weeks to 70 years are sufficient to permit us to describe postnatal development and anatomy of the ET in some detail. We have also been able to investigate the relationship between OM and cleft palate (KITAJIRI et at., 1985) and between OME and functional obstruction of the ET due to lymphocytic lymphoma (TAKAHARA et at., 1985) in these specimens. Inclusion of the entire ET with its accessory structures and the ME, antrum, mastoid air cells, and inner ear in one specimen should enable us to detect abnormalities leading to pathological conditions of those structures in a variety of situations, including high arched palate and incomplete and complete clefts of the palate.
In conclusion, we hope that, as more temporal bone specimens with the ET and its accessory structures are collected and studied by ourselves and others, much new knowledge will be gained about disorders affecting these structures. Ideally, this new knowledge will have positive effects on the clinical management of individuals with such disorders.
References KITAJIRI, M., SANDO, I., HASHIDA, Y., and DOYLE,
W. J.: HistopathologiCll study of otitis media in cleft palate infants and in high arched palate infants. Ann. Otol. Rhinol. Laryngol. 94: 44-50, 1985.
Panel Morphology and Pathology S 25
ROOD, S. R., and DOYLE, W. J.: An extreme morphological variation of the auditory tube cartilage: A case report. Clejt Palate J. 18: 293-298, 1981.
TAKAHARA, T., SANDO, I., BLUESTONE, C. D., and MYERS, E. N.: Poorly differentiated lymphocyt-
ic lymphoma invading the anterior Eustachian tube: A case report. Rhinal. Laryngol. 1985 (in press).
part of the Ann. alai.
WOLFF, D.: The auditory or eustachian tube. Laryngoscope 53: 400--408, 1943.