24
HTA Regulation and Economic Evaluation in Europe: where are we? Professor Alistair McGuire, LSE, London Istanbul, May 2009
| Date post: | 29-Dec-2015 |
| Category: |
Documents |
| Upload: | cynthia-bryant |
| View: | 217 times |
| Download: | 0 times |

HTA Regulation and Economic Evaluation in Europe: where are
we?
Professor Alistair McGuire,
LSE, London
Istanbul, May 2009

Outline
• Introduction
• Background
• Some specific regulatory regimes and specific countries

LevelsHealth Expenditure as % of GDP
0.0
2.0
4.0
6.0
8.0
10.0
12.0
14.0
16.0
18.0
Year
Hea
lth
exp
end
. as
% o
f G
DP USA
UK
Germany
Turkey
Spain
Italy
Greece
France

Health expenditure growth versus GDP Growth
Health care growth is outpacing GDP growth in all OECD countries (bar Finland) and has done for the past 35 years
France 13.5 12.4 9.3 7.2 6.6 3.8 6.3Germany 16.2 11.2 7.7 4.7 5.2 3.4 4.5UK 12.9 9.8 8.1 6.8 6.9 6.1 7.9USA 11 12.6 10.6 9.2 5.9 4.6 7Canada 9.8 10.2 10.1 6.6 3.4 4.1 6.6Turkey 11.2 2.1 20.5 4.1 22.1 7.9GDP per capita (US$ PPP) Compound annual rate of growth 1970-1975 1975-1980 1980-1985 1985-1990 1990-1995 1995-2000 2000-2005France 9.7 10.2 6.5 6.3 3.2 4.3 3.2Germany 8.8 11 6.9 5.9 1.1 3 3.8UK 8.6 9.1 7.2 6.3 3.9 5.2 5.2USA 8.5 10.1 7.6 5.6 3.6 4.6 3.9Canada 9.5 10.0 7.0 4.7 3.0 4.5 4.3Turkey 9.3 10.5 8.9 5.7 13.1 4.9
Health Care Expenditure per capita Compound annual growth rate

Pharmaceutical market value (ex manufacturers prices € 2004)
Source: UK OFT, 2007
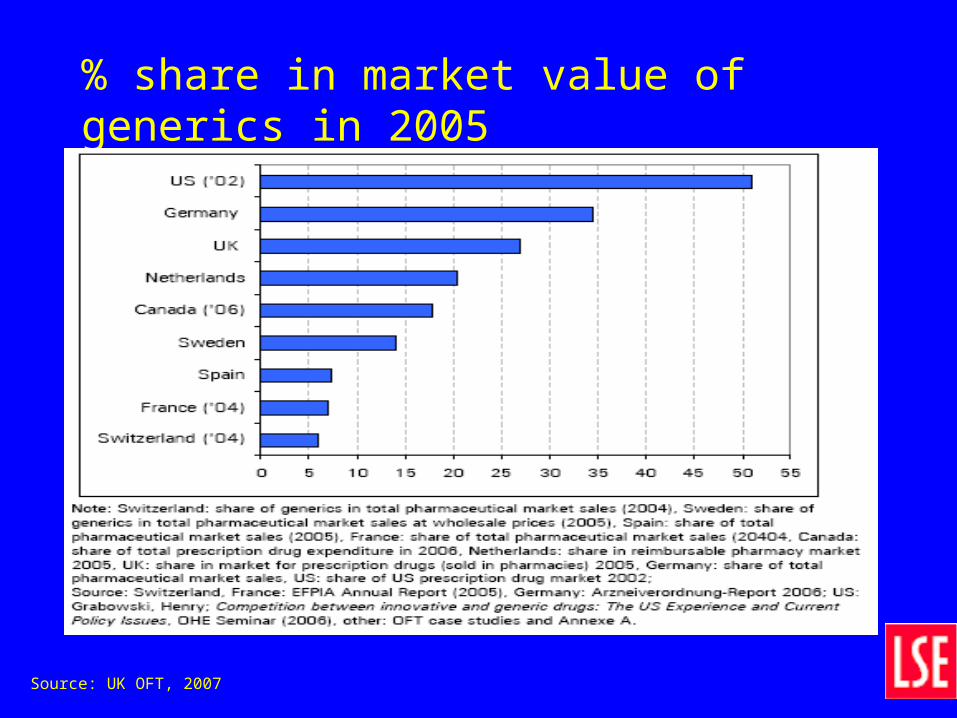
% share in market value of generics in 2005
Source: UK OFT, 2007
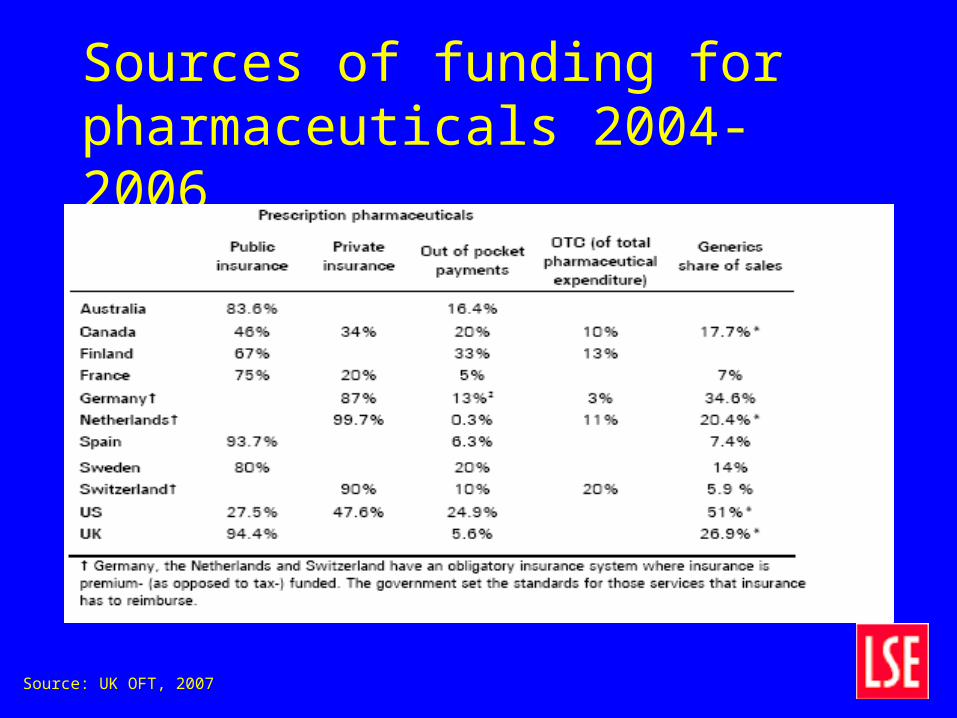
Sources of funding for pharmaceuticals 2004-2006
Source: UK OFT, 2007
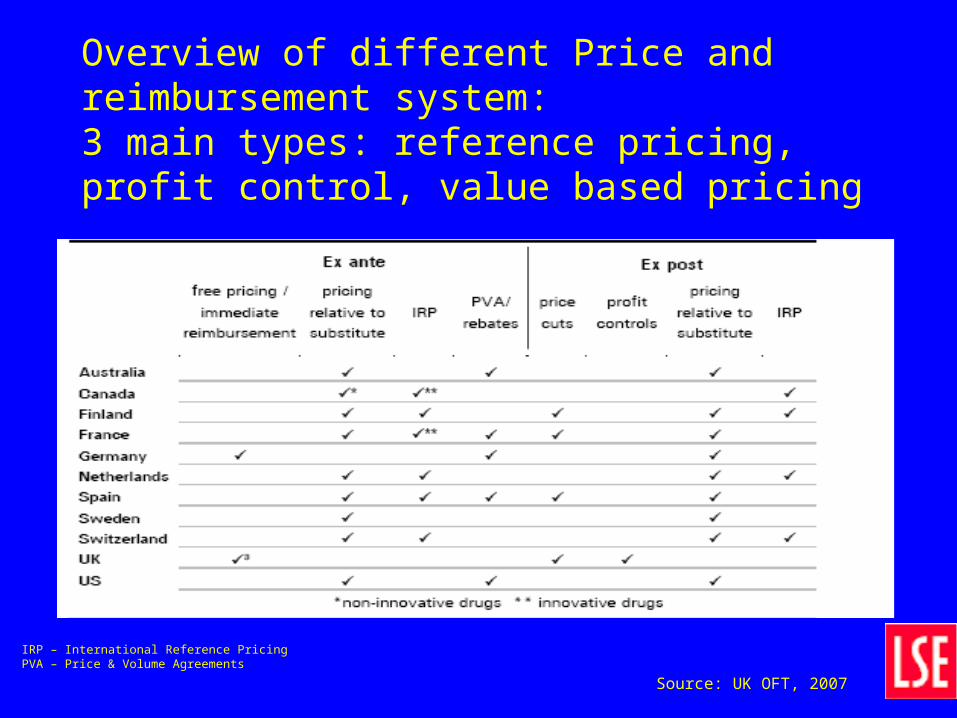
Overview of different Price and reimbursement system:3 main types: reference pricing, profit control, value based pricing
IRP – International Reference PricingPVA – Price & Volume Agreements
Source: UK OFT, 2007

Health Care Regulation
• Fee-for-service lists (primary care)
• DRG pricing of hospitals
• Price caps for pharmaceuticals
• Licensing of pharmaceuticals considers– Safety issues
– Efficacy issues
– Quality issues
• Cost-effectiveness analysis as a 4th hurdle
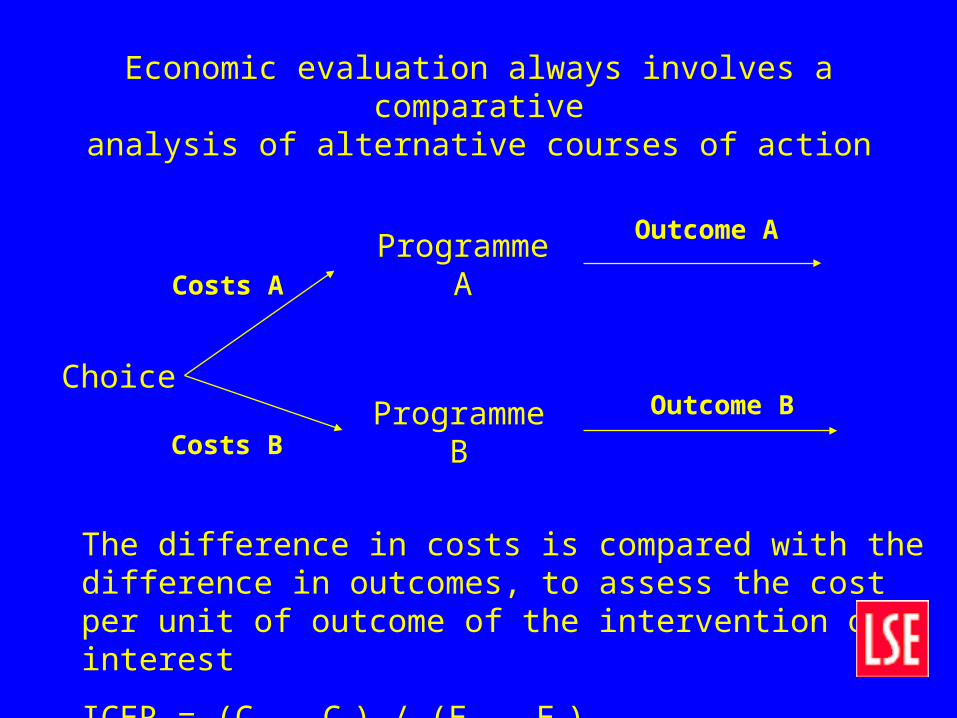
Economic evaluation always involves a comparativeanalysis of alternative courses of action
Choice
Programme A
Programme B
Costs A
Costs B
Outcome A
Outcome B
The difference in costs is compared with the difference in outcomes, to assess the cost per unit of outcome of the intervention of interest
ICER = (CA – CB) / (EA – EB)
BACKGROUND TO THE EUROPEAN SITUATION
• Variety of approaches to assessment, drug pricing and reimbursement
• Great diversity in health care systems• Increasingly formal requirements for economic
evaluation• On occasion industry has set the standard by
presenting economic data
Specific Country examples
• Economic evaluation and role in– Germany– UK
Germany
• Historical – “Free” Pricing of Drugs
• Background– Pharmaceuticals “responsible” for some
Regions going over budget– Pharmaceutical expenditure rising faster than
other health care expenditure 2001 by 11% compared to 2.5%)

Germany• Regulatory structure changing
– Reference pricing for multi-source products– Prescription budgets (recently abolished)– Negative reimbursement list to be replaced with a
positive list– Co-payment system– HTA reports by IQWiG to cover economic evaluation
of pharmaceuticals• Based on within treatment group comparator• Clinical evidence at cornerstone• Identification of an efficiency frontier
Germany – IQWiG proposals
• Efficiency frontier approach• Comparison of new pharmaceutical products
across relevant dimensions of effectiveness• Various measures of effectiveness allowed• Effectiveness data drawn from clinical trials• Modelling of long term outcomes based on trial
outcomes• Value of effectiveness to be determined• # of on-going techinical issues to be resolved
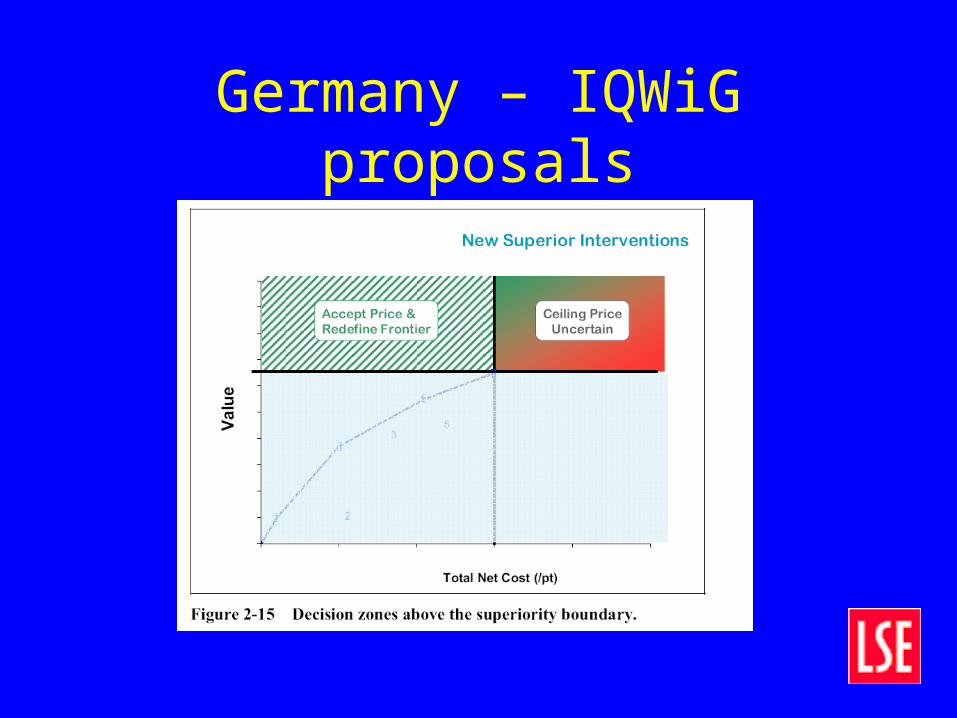
Germany – IQWiG proposals
UK
• Concern over rising expenditure on new products• Regulation dominated by Pharmaceutical Pricing
Reimbursement Scheme (PPRS)– Voluntary profit-capping scheme– “Free” pricing system– Negative list
• PPRS– Profit cap scheme
• NICE currently asks for evidence on cost-effectiveness– Value based pricing proposed (OFT)

NICE: UK• Cost-effectiveness thresholds
– Under £20,000 per QALY accept– £20,000 to £30,000 per QALY
• Issues of uncertainty• Innovative nature of programme• Particular features of intervention• Wider societal aspects
– Above £30,000 per QALY unlikely unless other good reason
• Is it a rationing device? Does it inhibit use?– Obviously yes; but in most cases guidance has been
positive and use has increased– Most guidance is about APPROPRIATE use

NICE Outcomes• UK National Cancer Director reviewed use of cancer drugs
– Industry was concerned about NICE recommendations and continuing variation in use
• Considered 16 drugs evaluated by NICE
• Findings– Overall use general increases after NICE approval
– Geographical variation in use lessens over time after approval
Source:UK NHS Cancer Director: IMS data
NICE Outcomes
• Expectation– NICE would limit up-take and generally have negative
impact on diffusion
• Outturn– Varies across individual intervention– But generally positive…if restricted– Has occurred during a time of unprecedented pre-war
growth in UK health expenditure (7% per annum real growth over 1999/2000 to 2007/08: c6% of GDP to c10% GDP)
• What would happen if health care expenditure was not growing?

Recent recommendations by OFT (2007)
• 1. All new products subject to a NICE ex-ante review, with an agreed cost per Qaly threshold
• 2. Prices are set by DoH on basis of above review• 3. Periodic review and price adjustment when market
conditions change• 4. Prices can rise or decline as a consequence of the review• 5. Patent expiry of a molecule implies a price cut for the
molecule and price cuts for similar molecules; • 6. Use risk-sharing and non-linear pricing agreements to help
set the “right” prices• 7. in short-term continue PPRS in combination with VBP as
above• 8. A fixed drug budget

Pricing issues - Ex ante VBP• Ex ante assessment of pricing plus periodic ex post
adjustment• Trade-off innovation incentive and market incentive• IF ex ante assessment based on product value and
coupled with ex post adjustment based on product value– Innovative incentives reduced– Ex ante pricing based on efficacy does not necessarily
reward innovation– Could apply risk-sharing more widely
Pricing issues - Ex post VBP• If ex post pricing is adopted based on value of
product the protection of innovation is weakened and the risk of innovation is returned to the firm– Firms may choose less “risky” innovations (potentially
high value products)
– Firms may not choose high risk innovation strategies (as payoff to discovery tends to zero relative to the ex post reimbursement inducement to minimise risk)
– Variation in innovation decreased
– Variance of risk minimised

Conclusions• Regulation increasingly mapped to “Value based medicine”• “Free” pricing systems changing regulations• CEA is increasingly used as a supplement to negative or
positive listing• CEA – may be a follow-through regulation
– price given in first instance for a set period– CEA evidence collected prospectively over a number of years within
post-marketing context
• Regulation is here to stay– Question of optimal form of regulation– Optimal timing of imposition

















