NEW MICROBIOLOGICA, 35, 279-287, 2012 Human cytomegalovirus end-organ disease is associated with high or low systemic viral load in preemptively treated solid-organ transplant recipients Giuseppe Gerna 1 , Daniele Lilleri 1 , Milena Furione 2 , Barbara Castiglioni 3 , Federica Meloni 4 , Teresa Rampino 5 , Manuela Agozzino 1 , Eloisa Arbustini 1 1 Laboratori Sperimentali di Ricerca, Area Trapiantologica, Fondazione IRCCS Policlinico San Matteo, Pavia, Italy; 2 S.S. Virologia Molecolare, S.C. Virologia e Microbiologia, Fondazione IRCCS Policlinico San Matteo, Pavia, Italy; 3 Dipartimento di Malattie Infettive, Università di Pavia, Pavia, Italy 4 Malattie Apparato Respiratorio, Università di Pavia, Pavia, Italy; 5 Dipartimento di Medicina Interna, Sezione di Nefrologia, Università di Pavia, Pavia, Italy INTRODUCTION In the post-transplant period of solid-organ trans- plant recipients (SOTR), human cytomegalovirus (HCMV) infection may be systemic or localized (or both). In either case, the infection may be asymptomatic, or evolve towards HCMV disease. Corresponding author Prof. Giuseppe Gerna Laboratori Sperimentali di Ricerca Area Trapiantologica Fondazione IRCCS Policlinico San Matteo P.le Golgi, 19 - 27100 Pavia, Italy E-mail: [email protected]; [email protected]The prophylactic approach is aimed at preventing both asymptomatic and symptomatic HCMV in- fection/disease (at least until antiviral treatment is administered), while the deferred therapy is recommended only for active HCMV disease. In the case of preemptive therapy, currently in use in most European transplantation centers, viral load cut-offs for initiating preemptive therapy in sys- temic infections have been established according to variable criteria (among different centers). On the other hand, it appears problematic to estab- lish cut-offs for intervention in local infections (end-organ disease) due to the difficulty in es- tablishing the extent of the organ involvement be- cause of improper or insufficient sampling, which Human cytomegalovirus (HCMV) end-organ disease in solid-organ transplant recipients (SOTR) may be associated with either high or low HCMV load in blood. In transplantation Centers where the preemptive therapy approach is adopted, antiviral therapy of systemic HCMV infections is initiated upon reaching pre-determined cut-off levels of vi- ral DNA in blood, whereas no guidelines are provided for local end-organ infection/disease. In the latter case, clini- cians often start antiviral treatment without defining the etiology of local symptoms. Here, we describe 14 cases of SOTR, in which a documented HCMV end-organ disease was observed. Nine patients had a systemic viral load low- er than the cut-off for preemptive therapy and were treated based on viral load of local HCMV disease. The remain- ing five patients had a systemic viral load greater than the preemptive therapy cut-off and were efficiently treated for both the systemic and the local HCMV disease. Thus, HCMV infection in the post-transplant period must be moni- tored virologically both in blood and locally. End-organ disease in preemptively treated patients, seems to be associ- ated with lack of development (primary HCMV infection) or reconstitution (reactivated infection) of HCMV-specific CD4 + and CD8 + T-cell immunity or with its functional impairment. KEY WORDS: HCMV viral load, Solid organ transplant recipients, HCMV systemic infections, HCMV end-organ dis- ease. SUMMARY Received February 02, 2012 Accepted April 24, 2012
Transcript
NEW MICROBIOLOGICA, 35, 279-287, 2012
Human cytomegalovirus end-organ disease is associated with high or low systemic viral load in preemptively treated solid-organ transplant
recipients
Giuseppe Gerna1, Daniele Lilleri1, Milena Furione2, Barbara Castiglioni3, Federica Meloni4, Teresa Rampino5, Manuela Agozzino1, Eloisa Arbustini1
1Laboratori Sperimentali di Ricerca, Area Trapiantologica, Fondazione IRCCS Policlinico San Matteo, Pavia, Italy;2S.S. Virologia Molecolare, S.C. Virologia e Microbiologia, Fondazione IRCCS Policlinico San Matteo, Pavia, Italy;
3Dipartimento di Malattie Infettive, Università di Pavia, Pavia, Italy4Malattie Apparato Respiratorio, Università di Pavia, Pavia, Italy;
5Dipartimento di Medicina Interna, Sezione di Nefrologia, Università di Pavia, Pavia, Italy
INTRODUCTION
In the post-transplant period of solid-organ trans-plant recipients (SOTR), human cytomegalovirus(HCMV) infection may be systemic or localized(or both). In either case, the infection may beasymptomatic, or evolve towards HCMV disease.
Corresponding authorProf. Giuseppe GernaLaboratori Sperimentali di RicercaArea TrapiantologicaFondazione IRCCS Policlinico San MatteoP.le Golgi, 19 - 27100 Pavia, ItalyE-mail: [email protected]; [email protected]
The prophylactic approach is aimed at preventingboth asymptomatic and symptomatic HCMV in-fection/disease (at least until antiviral treatmentis administered), while the deferred therapy isrecommended only for active HCMV disease. Inthe case of preemptive therapy, currently in use inmost European transplantation centers, viral loadcut-offs for initiating preemptive therapy in sys-temic infections have been established accordingto variable criteria (among different centers). Onthe other hand, it appears problematic to estab-lish cut-offs for intervention in local infections(end-organ disease) due to the difficulty in es-tablishing the extent of the organ involvement be-cause of improper or insufficient sampling, which
Human cytomegalovirus (HCMV) end-organ disease in solid-organ transplant recipients (SOTR) may be associatedwith either high or low HCMV load in blood. In transplantation Centers where the preemptive therapy approach isadopted, antiviral therapy of systemic HCMV infections is initiated upon reaching pre-determined cut-off levels of vi-ral DNA in blood, whereas no guidelines are provided for local end-organ infection/disease. In the latter case, clini-cians often start antiviral treatment without defining the etiology of local symptoms. Here, we describe 14 cases ofSOTR, in which a documented HCMV end-organ disease was observed. Nine patients had a systemic viral load low-er than the cut-off for preemptive therapy and were treated based on viral load of local HCMV disease. The remain-ing five patients had a systemic viral load greater than the preemptive therapy cut-off and were efficiently treated forboth the systemic and the local HCMV disease. Thus, HCMV infection in the post-transplant period must be moni-tored virologically both in blood and locally. End-organ disease in preemptively treated patients, seems to be associ-ated with lack of development (primary HCMV infection) or reconstitution (reactivated infection) of HCMV-specificCD4+ and CD8+ T-cell immunity or with its functional impairment.
Received February 02, 2012 Accepted April 24, 2012
impedes reliable evaluation of the overall organinvolvement. In addition, routine organ samplingis unfeasible, due to the invasive procedures re-quired. This is why most clinicians are oftenprone to treat transplanted patients with localsymptoms with HCMV-specific antiviral treat-ment in the absence of a documented viral diag-nosis. These problems could apparently be over-come in lung transplant recipients, where lungHCMV infection may be monitored in broncho-alveolar lavage (BAL) samples. This approach isused to guide preemptive therapy of lung infec-tion/disease (Gerna et al., 2009). However, also inthis case lung biopsy is the only approach defin-ing or resolving the diagnostic issue. This paper documents the high variability of therelationship between systemic HCMV load in pe-ripheral blood and organ (local) viral load (in tis-sue biopsies or organ fluids), whenever end-or-gan disease is diagnosed. Treating organ local-ization is not problematic when the patient reach-es the established viral load cut-off for initiatingpreemptive therapy during systemic infection.However, when viral load in blood is below theestablished cut-off, anti-HCMV therapy for organlocalization should be initiated, following the ap-pearance of clinical symptoms, only based ondocumented viral diagnosis.
PATIENTS AND METHODS
PatientsIn a group of more than 500 patients receivingheart, lung, heart-lung, or kidney transplantationat the Transplantation Center of the Istituto diRicovero e Cura a Carattere Scientifico (IRCCS)Policlinico San Matteo, Pavia, Italy, in the period2003-2009, 14 patients had a virologically diag-nosed end-organ disease at different times aftertransplantation. Along with HCMV organ local-ization, all these patients also presented with asystemic HCMV infection associated with differ-ent levels of HCMV viral load in blood.Immunosuppressive regimens were administeredas previously reported (Grossi et al., 1995). At ourcenter prevention of HCMV disease was based onthe preemptive therapy approach, i.e. antiviraltreatment of HCMV infection was initiated uponreaching predetermined cut-off levels of pp65-antigenemia until 2007 (Grossi et al., 1995) or
HCMV DNA copies/ml blood thereafter (Gerna etal., 2007). On this basis, we retrospectively divid-ed patients in this study into two groups: one hadviral load in blood lower than the established cut-off for preemptive therapy, and the other showeda systemic viral load greater than the establishedcut-off. As a result, in the first group, antiviraltreatment for organ localization was initiated in-dependently of the systemic viral load cut-off,whereas in the second group, treatment of localorgan involvement was concomitant with treat-ment for systemic infection.
Diagnosis of HCMV infection and preemptive therapyHCMV asymptomatic and symptomatic systemicinfections/disease were defined as reported(Ljungman et al., 2002). Diagnosis of HCMV in-fection was performed by simultaneous determi-nation of HCMV pp65-antigenemia (Gerna et al.,1992), and DNAemia (Gerna et al., 2006).According to cut-offs established, until 2006 anti-genemia-guided preemptive therapy started treat-ment of primary HCMV infections upon first con-firmed appearance of virus in blood, and reacti-vated HCMV infections when level of virus inblood reached 100 pp65-positive leukocytes/2x105
leukocytes examined (Gerna et al., 2007). Startingfrom 2007, 300,000 HCMV DNA copies/ml bloodwere used as a cut-off for initiating antiviral treat-ment of both primary and reactivated systemicHCMV infections of all types of SOT (Grossi etal., 1995). In lung transplant recipients, HCMV infectionwas also monitored in BAL, and preemptive ther-apy was initiated in the presence of 100,000 DNAcopies/ml BAL (Gerna et al., 2009). Ganciclovir(GCV, 5 mg/kg b.i.d.) was used as a first line treat-ment, and it was replaced by foscarnet (PFA, 90mg/kg b.i.d.) in case of GCV myelotoxicity or druginefficacy or resistance. HCMV load was deter-mined once a week until detection of HCMV in-fection, thereafter testing was performed twice aweek until confirmed virus disappearance fromblood.
End-organ disease diagnosis and treatmentdurationEnd-organ disease was diagnosed as reported(Kotton et al., 2010). ImmunohistochemicalHCMV detection in tissue biopsies was achieved
280 G. Gerna, D. Lilleri, M. Furione, B. Castiglioni, F. Meloni, T. Rampino, M. Agozzino, E. Arbustini
by pre-treating paraffin-embedded tissue sectionswith heat-induced epitope retrieval and thenstaining sections with a mixture of two murinemAbs directed to p52 (Plachter et al., 1992) andthe major immediate-early (IE) UL123 gene prod-uct (Wirgart, 1991). According to the differenttypes of sample, determination of viral load inend-organ disease was performed as follows. Incase of gastrointestinal (GI, esophageal, gastric,enteric) biopsy, viral load was expressed as copynumber/1x105 cells. Cell number was determinedby amplifying a human single-copy housekeep-ing gene (Watzinger et al., 2004). When multiplebiopsy tissue samples were available, extractedDNA from different samples was combined toyield a unique DNA sample. In case of interstitialpneumonia, HCMV load was determined per mlBAL fluid (Gerna et al., 2009). In the presence ofHCMV retinitis, HCMV load was determined perml aqueous humor, as previously reported (Gernaet al., 1994). HCMV end-organ disease was treat-ed with antiviral therapy on the basis of instru-mental findings of organ pathology in associa-tion with immunohistochemical and/or virologicdocumentation of HCMV organ infection (at anyviral load level). Discontinuation of antiviral treat-ment for end-organ disease was based, whenev-er possible, on disappearance of virus from BALor organ biopsies in association with resolution ofclinical symptoms and endoscopic (or ophtal-moscopic) lesions.
HCMV-specific T-cell immune responseevaluationEvaluation of HCMV-specific T-cell response attime of diagnosis of end-organ disease was doneby a previously established assay based on PBMCstimulation by autologous HCMV-infected den-dritic cells (Gerna et al., 2011).
RESULTS
Fourteen cases of HCMV end-organ disease wereexamined. Of these, 9 initiated antiviral treatmentbased on diagnosis of end-organ disease, i.e. pri-or to reaching the cut-off in blood for preemptivetherapy, whereas in 5 patients end-organ diseasewas diagnosed concomitantly with detection ofviral load in blood above the cut-off for pre-emp-tive therapy. Four patients had primary infection
(two per each group), while all the other patientshad reactivated infections.
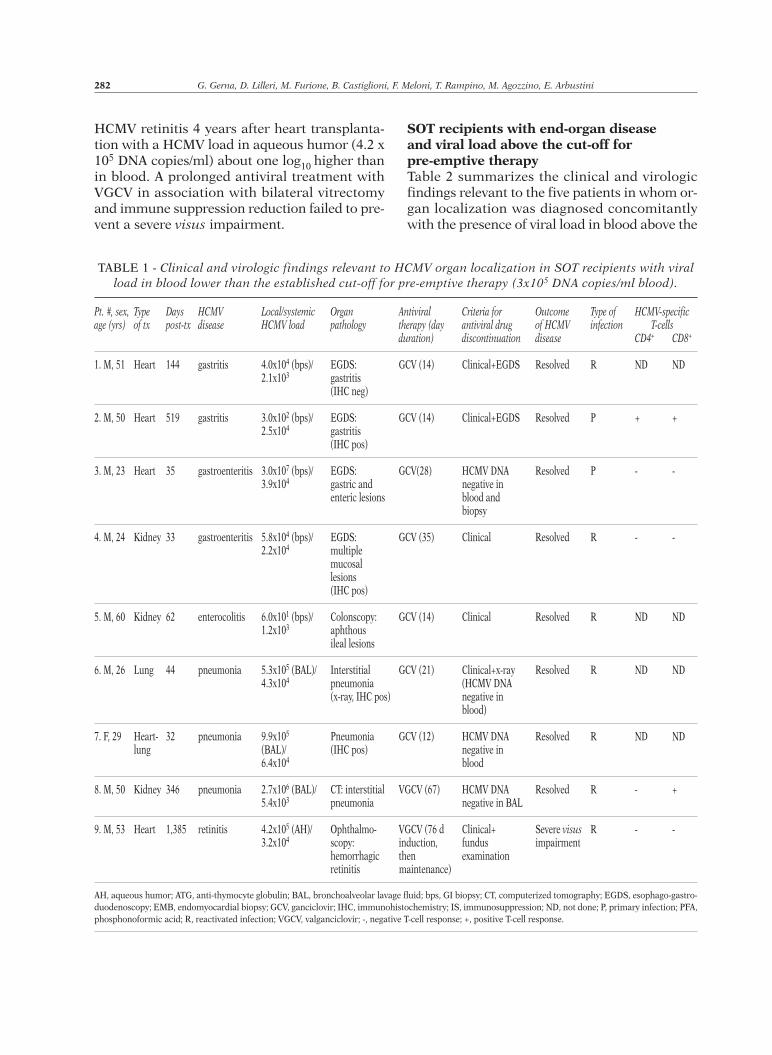
SOT recipients with end-organ disease and viral load below the cut-off for pre-emptive therapyThe clinical and virologic findings relevant to thenine SOT recipients with HCMV end-organ dis-ease diagnosed when viral load in blood was be-low the established cut-off for pre-emptive ther-apy are reported in Table 1. In this group of pa-tients, end-organ disease was diagnosed at a me-dian time of 62 (range 32-1385) days after trans-plantation. Five patients (three heart and two kid-ney transplant recipients) had HCMV gastroin-testinal (GI) disease (GID) (4 with gastritis andone with colitis, as documented by both en-doscopy and immunohistochemistry), three hadHCMV interstitial pneumonia (Figure 1A, pt #7),and one HCMV retinitis. Organ viral load reacheda median value of 4.0x104 (range 6x101- 3.0x107)DNA copies/1x105 cells in the 5 patients with GID.In all these patients, diagnosis was established byendoscopy, and in 2/5 pts. (# 2 and 4) it was con-firmed by immune histochemistry. Ganciclovirtreatment, initiated concomitantly with first vi-ral DNA detection in GI biopsies, had a medianduration of 14 (range 14-35) days, and, by defi-nition, was associated with low viral load in blood(median 2.2x104, range 1.2x103-3.9x104 DNAcopies/ml blood). Treatment was successful in allpatients, as shown by the disappearance of clin-ical symptoms and/or endoscopic resolution ofmucosal lesions, in 4 patients in association withvirologic documentation of viral DNA disappear-ance in the biopsy tissue (pt. #3).In the three patients (one lung, one heart-lung,and one kidney transplant recipient) with radio-logical diagnosis of interstitial pneumonia,HCMV load in BAL samples ranged from 5.3x105
to 2.7x106 /ml BAL, and in blood from 5.4x103 to6.4x104/ml. Diagnosis was supported by im-munohistochemistry of lung biopsies in two ofthese patients (pts.# 6 and 7), while in the thirdpatient (# 8) only virus in BAL was detected at anhigh level concomitantly with CT signs of inter-stitial pneumonia. However, antiviral treatmentof different duration (12-67 days) was able to re-solve lung infection in all three patients, as shownby clinical, radiological and virological findings.Finally, patient #9 had a severe hemorrhagic
HCMV load and end-organ disease in SOTR 281
HCMV retinitis 4 years after heart transplanta-tion with a HCMV load in aqueous humor (4.2 x105 DNA copies/ml) about one log10 higher thanin blood. A prolonged antiviral treatment withVGCV in association with bilateral vitrectomyand immune suppression reduction failed to pre-vent a severe visus impairment.
SOT recipients with end-organ disease and viral load above the cut-off for pre-emptive therapyTable 2 summarizes the clinical and virologicfindings relevant to the five patients in whom or-gan localization was diagnosed concomitantlywith the presence of viral load in blood above the
282 G. Gerna, D. Lilleri, M. Furione, B. Castiglioni, F. Meloni, T. Rampino, M. Agozzino, E. Arbustini
TABLE 1 - Clinical and virologic findings relevant to HCMV organ localization in SOT recipients with viralload in blood lower than the established cut-off for pre-emptive therapy (3x105 DNA copies/ml blood).
Pt. #, sex, Type Days HCMV Local/systemic Organ Antiviral Criteria for Outcome Type of HCMV-specificage (yrs) of tx post-tx disease HCMV load pathology therapy (day antiviral drug of HCMV infection T-cells
duration) discontinuation disease CD4+ CD8+
1. M, 51 Heart 144 gastritis 4.0x104 (bps)/ EGDS: GCV (14) Clinical+EGDS Resolved R ND ND2.1x103 gastritis
(IHC neg)
2. M, 50 Heart 519 gastritis 3.0x102 (bps)/ EGDS: GCV (14) Clinical+EGDS Resolved P + +2.5x104 gastritis
(IHC pos)
3. M, 23 Heart 35 gastroenteritis 3.0x107 (bps)/ EGDS: GCV(28) HCMV DNA Resolved P - -3.9x104 gastric and negative in
enteric lesions blood and biopsy
4. M, 24 Kidney 33 gastroenteritis 5.8x104 (bps)/ EGDS: GCV (35) Clinical Resolved R - -2.2x104 multiple
mucosal lesions(IHC pos)
5. M, 60 Kidney 62 enterocolitis 6.0x101 (bps)/ Colonscopy: GCV (14) Clinical Resolved R ND ND1.2x103 aphthous
ileal lesions
6. M, 26 Lung 44 pneumonia 5.3x105 (BAL)/ Interstitial GCV (21) Clinical+x-ray Resolved R ND ND4.3x104 pneumonia (HCMV DNA
(x-ray, IHC pos) negative in blood)
7. F, 29 Heart- 32 pneumonia 9.9x105 Pneumonia GCV (12) HCMV DNA Resolved R ND NDlung (BAL)/ (IHC pos) negative in
6.4x104 blood
8. M, 50 Kidney 346 pneumonia 2.7x106 (BAL)/ CT: interstitial VGCV (67) HCMV DNA Resolved R - +5.4x103 pneumonia negative in BAL
9. M, 53 Heart 1,385 retinitis 4.2x105 (AH)/ Ophthalmo- VGCV (76 d Clinical+ Severe visus R - -3.2x104 scopy: induction, fundus impairment
hemorrhagic then examinationretinitis maintenance)
FIGURE 1 - Immunohistochemical detection (arrows) of HCMV-infected (A) alveolar epithelial cells in a trans-bronchial biopsy (pt #7), and (B) endothelial cells in a cardial/esophageal biopsy (pt #10). (C). The lower part of thefigure shows the low-power view of three sections of endomyocardial biopsy of pt #14, while the high-power view ofthe immunostain with anti-HCMV antibodies of the inflammatory infiltrate (squared low-power middle section)with HCMV-positive cells (arrows) is shown in the upper part of the figure. Myocytes, interstitial and endothelialcells of low-power left and right sections do not show either cytopathic effect or signs of inflammation.
a b
c
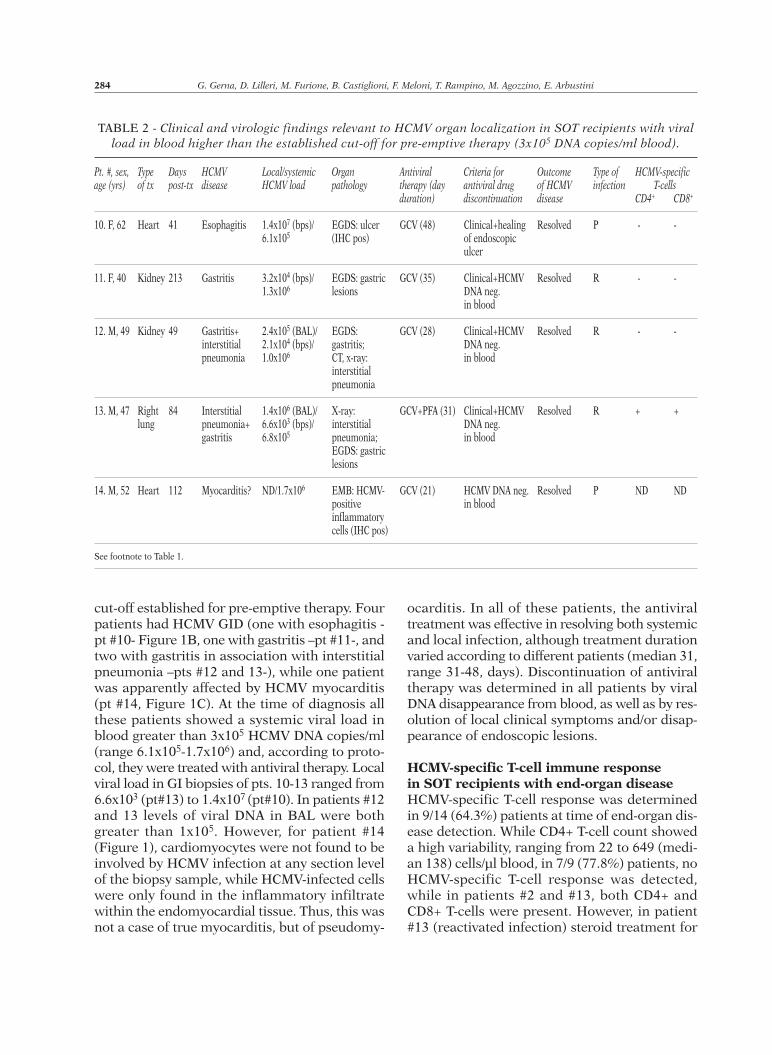
cut-off established for pre-emptive therapy. Fourpatients had HCMV GID (one with esophagitis -pt #10- Figure 1B, one with gastritis –pt #11-, andtwo with gastritis in association with interstitialpneumonia –pts #12 and 13-), while one patientwas apparently affected by HCMV myocarditis(pt #14, Figure 1C). At the time of diagnosis allthese patients showed a systemic viral load inblood greater than 3x105 HCMV DNA copies/ml(range 6.1x105-1.7x106) and, according to proto-col, they were treated with antiviral therapy. Localviral load in GI biopsies of pts. 10-13 ranged from6.6x103 (pt#13) to 1.4x107 (pt#10). In patients #12and 13 levels of viral DNA in BAL were bothgreater than 1x105. However, for patient #14(Figure 1), cardiomyocytes were not found to beinvolved by HCMV infection at any section levelof the biopsy sample, while HCMV-infected cellswere only found in the inflammatory infiltratewithin the endomyocardial tissue. Thus, this wasnot a case of true myocarditis, but of pseudomy-
ocarditis. In all of these patients, the antiviraltreatment was effective in resolving both systemicand local infection, although treatment durationvaried according to different patients (median 31,range 31-48, days). Discontinuation of antiviraltherapy was determined in all patients by viralDNA disappearance from blood, as well as by res-olution of local clinical symptoms and/or disap-pearance of endoscopic lesions.
HCMV-specific T-cell immune response in SOT recipients with end-organ diseaseHCMV-specific T-cell response was determinedin 9/14 (64.3%) patients at time of end-organ dis-ease detection. While CD4+ T-cell count showeda high variability, ranging from 22 to 649 (medi-an 138) cells/µl blood, in 7/9 (77.8%) patients, noHCMV-specific T-cell response was detected,while in patients #2 and #13, both CD4+ andCD8+ T-cells were present. However, in patient#13 (reactivated infection) steroid treatment for
284 G. Gerna, D. Lilleri, M. Furione, B. Castiglioni, F. Meloni, T. Rampino, M. Agozzino, E. Arbustini
TABLE 2 - Clinical and virologic findings relevant to HCMV organ localization in SOT recipients with viralload in blood higher than the established cut-off for pre-emptive therapy (3x105 DNA copies/ml blood).
Pt. #, sex, Type Days HCMV Local/systemic Organ Antiviral Criteria for Outcome Type of HCMV-specificage (yrs) of tx post-tx disease HCMV load pathology therapy (day antiviral drug of HCMV infection T-cells
11. F, 40 Kidney 213 Gastritis 3.2x104 (bps)/ EGDS: gastric GCV (35) Clinical+HCMV Resolved R - -1.3x106 lesions DNA neg.
in blood
12. M, 49 Kidney 49 Gastritis+ 2.4x105 (BAL)/ EGDS: GCV (28) Clinical+HCMV Resolved R - -interstitial 2.1x104 (bps)/ gastritis; DNA neg. pneumonia 1.0x106 CT, x-ray: in blood
interstitial pneumonia
13. M, 47 Right 84 Interstitial 1.4x106 (BAL)/ X-ray: GCV+PFA (31) Clinical+HCMV Resolved R + +lung pneumonia+ 6.6x103 (bps)/ interstitial DNA neg.
gastritis 6.8x105 pneumonia; in bloodEGDS: gastric lesions
14. M, 52 Heart 112 Myocarditis? ND/1.7x106 EMB: HCMV- GCV (21) HCMV DNA neg. Resolved P ND NDpositive in bloodinflammatorycells (IHC pos)
See footnote to Table 1.
heart rejection was administered, while in patient#2 (primary infection) HCMV disease occurred>18 months after transplantation, concomitantlywith development of primary T-cell response.
DISCUSSION
Two entirely different clinical scenarios may oc-cur in SOT recipients with HCMV end-organ dis-ease. HCMV disease may take place in the pres-ence of low HCMV viral load in blood, or in as-sociation with a high systemic viral load. In trans-plantation centers where the pre-emptive thera-py approach is routinely adopted, therapeutic de-cisions may vary widely according to these twoclinical situations. In the presence of clinical symptoms suggestingan HCMV organ localization, even in the pres-ence of low (or absent) viral load in blood, theetiologic diagnosis of HCMV organ involvementmust be established as rapidly as possible. On theother hand, in the case of high viral load in blood,the initiation of antiviral therapy, based on sys-temic viral DNA cut-off, is effective also for end-organ disease. In both cases, however, therapydiscontinuation should not be decided solely onthe basis of virus disappearance from blood, butadditional requirements need to be met, i.e. ame-lioration/resolution of local clinical symptoms,resolution/healing of endoscopic lesions possiblyin association with disappearance of viral DNAin biopsy samples, or in local secretions. In thisstudy, a special warning comes from the analysisof pt #14 in whom myocardial involvement byHCMV infection was only apparent, i.e. due tothe inflammatory infiltrate in the absence of car-diomyocyte infection.Among HCMV tissue-invasive diseases, GID is themost frequently occurring in SOT recipients, in-cluding esophagitis, gastritis, duodenitis andsmall bowel enteritis, and colitis (Lemonovichand Watkins, 2012). Other less frequently in-volved organ are lungs (pneumonitis), liver (he-patitis), pancreas (pancreatitis), and eye (retini-tis). In general, risk factors associated signifi-cantly with the development of HCMV diseaseare primary infections following universal pro-phylaxis (often associated with late-onset HCMVdisease, allograft failure and mortality), and thelevel of the immunosuppression or reconstitution
of HCMV-specific immunity (Arthurs et al., 2008;Eid et al., 2010). In our series, using pre-emptivetherapy, we had 4/14 (28.6%) patients with pri-mary infection, thus confirming that primary in-fection is a risk factor for end-organ disease alsoin association with pre-emptive therapy. It hasbeen reported that gastrointestinal lesions werepresent in 3/4 solid organ transplant recipientsdeveloping HCMV drug-resistance in the era ofvalganciclovir prophylaxis (Eid et al., 2008a). Inaddition, Halme et al. detected HCMV in biopsiesof liver transplant recipients, as well as in patientssuffering from chronic liver disease or even inotherwise healthy patients with dyspeptic symp-toms (Halme et al., 2008). Therefore, the solepresence of cells with nuclear inclusion bodiesdoes not seem to be enough for initiating the an-tiviral therapy, since same findings have also beenobserved in GI tract of immunocompetent indi-viduals. Similarly, control endoscopy at the end of treat-ment to verify resolution of lesions and/or viralDNA disappearance does not necessarily meanprotection from HCMV relapse (Eid et al., 2010).In our opinion, tissue section examination mustbe performed whenever possible. However, re-sults must be interpreted with caution, both forantiviral therapy initiation and discontinuation.HCMV presence in lungs and BAL merits specialanalysis (Gerna et al., 2009). While diagnosis ofHCMV pneumonitis requires the presence ofHCMV-infected epithelial cells surrounded by in-flammatory infiltrates in biopsy lung sections, thesole presence of nuclear inclusion body bearingcells is not sufficient to make a diagnosis ofHCMV pneumonitis. In addition, the HCMV pres-ence in BAL is not per se indicative of HCMV lungpathology. A recent study correlating viral loadin BAL with HCMV detection in lung biopsiesfound that levels >1x105 DNA copies /ml BALwere detected in 100% of LTR with HCMV pneu-monia (lung infection + inflammatory infiltrates),in 25-30% of patients with HCMV infection inlungs and no inflammatory infiltrates, and in on-ly 3% of LTR with no sign of lung infection.HCMV-specific T-cell immunity seems to controlHCMV infection during the post-transplantationperiod (Gerna et al., 2009). However, preliminaryfindings seem to indicate that different T-cell pop-ulations are responsible for local lung and sys-temic immunity (Shlobin et al., 2006).
HCMV load and end-organ disease in SOTR 285
A more uncommon feature of HCMV end-organdisease is HCMV retinitis (Eid et al., 2008b),which is currently diagnosed based on fundus-copic examination, but may be virologically di-agnosed by disclosing viral DNA in aqueous hu-mor, as we demonstrated in a series of AIDS pa-tients (Gerna et al., 1994). In the only patient ofour series, the amount of viral DNA detected inaqueous humor was rather high (>105 DNAcopies/ml).In the present study, lack of specific T-cell im-mune response appears to be consistently asso-ciated with HCMV end-organ disease. In fact, ofthe 9 patients tested, 6 were lacking both HCMV-specific CD4+ and CD8+ T-cell response, one hadonly specific CD8+ T-cells, while of the two pa-tients showing a T-cell response, one (#13, reac-tivated infection) was under steroid treatment,and the other (#2, primary infection) had end-or-gan disease while developing HCMV-specific T-cell primary response. We already observed in the past that HCMV-spe-cific CD8+ T-cells are often unable to controlHCMV infection, while steroid therapy may im-pair T-cell response (Gerna et al., 2011). In addi-tion, for patient #2 it can be hypothesized thatprimary T-cell response developing concomitant-ly with HCMV end-organ localization was not ful-ly protective against HCMV disease. It has been a matter of debate which viral assayis more sensitive in detecting HCMV end-organdisease in SOT recipients. HCMV pp65-antigen-emia and qualitative/quantitative PCR have beencompared for sensitivity and specificity in a num-ber of published reports (Fica et al., 2007; Janget al., 2009; Grim et al., 2010). Both assays haveshown levels of sensitivity between 50% and 80%,with a slightly higher level of specificity for bothassays. In addition, sensitivity increased if testswere performed within 6 months after trans-plantation (Fica et al., 2007). In our series, weconsistently found the presence of viral DNA inblood of transplanted patients at the time of or-gan involvement diagnosis by using real-timePCR (Gerna et al., 2006). It cannot be excludedthat in some cases end-organ disease may not beassociated with detection of virus in peripheralblood. However, in some studies symptomaticsystemic HCMV infection/disease was not differ-entiated from end-organ disease (Marchetti et al.,2011). On the other hand, virus in blood may not
provide specific indications on which organ maybe involved in the HCMV end-organ disease. The pre-emptive therapy approach appears gen-erally effective in preventing HCMV end-organdisease, considering that it was diagnosed in lessthan 3% of patients in our series. However,HCMV disease prevention is not 100% success-ful, especially when HCMV organ localization oc-curs in the presence of low viral load in blood orearly after transplantation. In these cases, localinfection must be timely diagnosed endoscopi-cally and virologically, and documentation ofHCMV infection is needed before deciding on thetherapeutic approach to be adopted.
ACKNOWLEDGEMENTSWe are indebted to all the technical staff of theVirology section of the Struttura Complessa ofVirology and Microbiology for performing the viralassays. We acknowledge the careful and devoted se-cretarial support of Daniela Sartori and the Englishrevision by Laurene Kelly. This work was partiallysupported by grants from the Fondazione CarloDenegri, Torino, and by the Ministero della Salute,Ricerca Corrente Fondazione IRCCS PoliclinicoSan Matteo, grant 80207.
REFERENCES
ARTHURS S.K., EID A.J., PEDERSEN R.A., KREMERS W.K.,COSIO F.G., PATEL R., RAZONABLE R.R. (2008).Delayed-onset primary cytomegalovirus disease andthe risk of allograft failure and mortality after kid-ney transplantation. Clin. Infect. Dis. 46, 840-846.
EID A.J., ARTHURS S.K., DEZIEL P.J., WILHELM M.P.,RAZONABLE R.R. (2008a). Emergence of drug-re-sistant cytomegalovirus in the era of valganciclovirprophylaxis: therapeutic implications and out-comes. Clin. Transplant. 22, 162-170.
EID A.J., BAKRI S.J., KIJPITTAYARIT S., RAZONABLE R.R.(2008b). Clinical features and outcomes of cy-tomegalovirus retinitis after transplantation.Transpl. Infect. Dis. 10, 13-18.
EID A.J., ARTHURS S.K., DEZIEL P.J., WILHELM M.P.,RAZONABLE R.R. (2010). Clinical predictors of re-lapse after treatment of primary gastrointestinalcytomegalovirus disease in solid organ transplantrecipients. Am. J. Transpl. 10, 157-161.
FICA A., CERVERA C., PÉREZ N., MARCOS M.A., RAMÍREZ
J., LINARES L., SOTO G., NAVASA M., COFAN F., RICART
M.J., PÉREZ-VILLA F., PUMAROLA T., MORENO A.(2007). Immunohistochemically proven cy-tomegalovirus end-organ disease in solid organ
286 G. Gerna, D. Lilleri, M. Furione, B. Castiglioni, F. Meloni, T. Rampino, M. Agozzino, E. Arbustini
transplant patients: clinical features and usefulnessof conventional diagnostic tests. Transpl. Infect. Dis.9, 203-210.
GERNA G., REVELLO M.G., PERCIVALLE E., MORINI F.(1992). Comparison of different immunostainingtechniques and monoclonal antibodies to the low-er matrix phosphoprotein (pp65) for optimal quan-titation of human cytomegalovirus antigenemia. J.Clin. Microbiol. 30, 1232-1237.
GERNA G., BALDANTI F., SARASINI A., FURIONE M.,PERCIVALLE E., REVELLO M.G., ZIPETO D., ZELLA D.(1994). Effect of foscarnet induction treatment onquantitation of human cytomegalovirus (HCMV)DNA in peripheral blood polymorphonuclear leuko-cytes and aqueous humor of AIDS patients withHCMV retinitis. Antimicrob. Agents Chemother. 38,38-44.
GERNA G., VITULO P., ROVIDA F., LILLERI D., PELLEGRINI
M.G. (2006). Impact of human metapneumovirusand human cytomegalovirus versus other respira-tory viruses on the lower respiratory tract infec-tions of lung transplant recipients. J. Med. Virol.78, 408-416. Erratum in: J. Med. Virol. 80, 1869(2008).
GERNA G., BALDANTI F., TORSELLINI M., MINOLI L.,VIGANÒ M., OGGIONNI T., RAMPINO T., CASTIGLIONI B.,GOGLIO A., COLLEDAN M., MAMMANA C., NOZZA F.,LILLERI D.; BERGAMO TRANSPLANT GROUP. (2007).Evaluation of cytomegalovirus DNAaemia versuspp65-antigenaemia cutoff for guiding preemptivetherapy in transplant recipients. A randomizedstudy. Antivir. Ther. 12, 63-72.
GERNA G., LILLERI D., ROGNONI V., AGOZZINO M., MELONI
F., OGGIONNI T., PELLEGRINI C., ARBUSTINI E.,D’ARMINI A.M. (2009). Preemptive therapy for sys-temic and pulmonary human cytomegalovirus in-fection in lung transplant recipients. Am. J.Transplant. 9, 1142-1150.
GERNA G., LILLERI D., CHIESA A., ZELINI P., FURIONE M.,COMOLLI G., PELLEGRINI C., SARCHI E., MIGOTTO C.,BONORA M.R., MELONI F., ARBUSTINI E. (2011).Virologic and immunologic monitoring of cy-tomegalovirus to guide preemptive therapy in sol-id organ transplantation. Am. J. Transplant. 11,2463-2471.
GRIM S.A., PEREIRA E., GUZMAN G., CLARK N.M. (2010).CMV PCR as a diagnostic tool for CMV gastroin-testinal disease after solid organ transplantation.Transplantation. 90, 799-801.
GROSSI P., MINOLI L., PERCIVALLE E., IRISH W., VIGANÒ
M., GERNA G. (1995). Clinical and virological mon-itoring of human cytomegalovirus infection in 294
HALME L., LEMPINEN M., AROLA J., SARKIO S.,HOCKERSTEDT K., LAUTENSCHLAGER I. (2008). Highfrequency of gastroduodenal cytomegalovirus infec-tion in liver transplant patients. APMIS 116, 99-106.
JANG E.-Y., PARK S.Y., LEE E.J., SONG E.H., CHONG Y.P.,LEE S.O., CHOI S.H., WOO J.H., KIM Y.S., KIM S.H.(2009). Diagnostic performance of the cy-tomegalovirus (CMV) antigenemia assay in patientswith CMV gastrointestinal disease. Clin. Infect. Dis.48, e121-124.
KOTTON C.N., KUMAR D., CALIENDO A.M., ASBERG A.,CHOU S., SNYDMAN D.R., ALLEN U., HUMAR A., ON BE-HALF OF THE TRANSPLANTATION SOCIETY INTERNATIONAL
CMV CONSENSUS GROUP. (2010). International con-sensus guidelines on the management of cy-tomegalovirus in solid organ transplantation.Transplantation. 89, 779-795.
LEMONOVICH T.L., WATKINS R.R. (2012). Update on cy-tomegalovirus infections of the gastrointestinal sys-tem in solid organ transplant recipients. Curr. Infect.Dis. Rep. 14, 33-40.
LJUNGMAN P., GRIFFITHS P., PAYA C. (2002). Definitions ofcytomegalovirus infection and disease in transplantrecipients. Clin. Infect. Dis. 34, 1094-1097.
MARCHETTI S., SANTANGELO R., MANZARA S., D’ONGHIA
S., FADDA G., CATTANI P. (2011). Comparison of real-time PCR and pp65 antigen assays for monitoringthe development of cytomegalovirus disease in re-cipients of solid organ and bone marrow trans-plants. New Microbiol. 34, 157-164.
PLACHTER B., NORDIN M., WIRGART B.Z., MACH M., STEIN
H., GRILLNER L., JAHN G. (1992). The DNA-bindingprotein P52 of human cytomegalovirus reacts withmonoclonal antibody CCH2 and associates with thenuclear membrane at late times after infection.Virus Res. 24, 265-276.
SHLOBIN O.A., WEST E.E., LECHTZIN N., MILLER S.M.,BORJA M., ORENS J.B., DROPULIC L.K., MCDYER J.F.(2006). Persistence cytomegalovirus-specific mem-ory responses in the lung allograft and blood fol-lowing primary infection in lung transplant recip-ients. J. Immunol. 176, 2625-2634.
WATZINGER F., SUDA M., PREUNER S., BAUMGARTINGER R.,EBNER K., BASKOVA L., NIESTERS H.G., LAWITSCHKA
A., LION T. (2004). Real-time quantitative PCR assayfor detection and monitoring of pathogenic humanviruses in immunosuppressed pediatric patients. J.Clin. Microbiol. 42, 5189-5198.
WIRGART B.Z. (1991). Development of rapid methodsfor early diagnosis of cytomegalovirus infections(dissertation). Stockholm: Karolinska Hospital.