This article was downloaded by: [Dalhousie University] On: 12 March 2013, At: 12:38 Publisher: Taylor & Francis Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK Journal of Toxicology and Environmental Health, Part A: Current Issues Publication details, including instructions for authors and subscription information: http://www.tandfonline.com/loi/uteh20 Human Health Risk and Exposure Assessment of Chromium (VI) in Tap Water Dennis Paustenbach a , Brent Finley a , Fionna Mowat b & Brent Kerger c a ChemRisk®, Alameda, California, USA b Exponent, Menlo Park, California, USA c Health Science Resource Integration, Inc., Tallahassee, Florida, USA Version of record first published: 07 Jan 2011. To cite this article: Dennis Paustenbach , Brent Finley , Fionna Mowat & Brent Kerger (2003): Human Health Risk and Exposure Assessment of Chromium (VI) in Tap Water, Journal of Toxicology and Environmental Health, Part A: Current Issues, 66:17, 1295-1339 To link to this article: http://dx.doi.org/10.1080/15287390306388 PLEASE SCROLL DOWN FOR ARTICLE Full terms and conditions of use: http://www.tandfonline.com/page/terms-and-conditions This article may be used for research, teaching, and private study purposes. Any substantial or systematic reproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution in any form to anyone is expressly forbidden. The publisher does not give any warranty express or implied or make any representation that the contents will be complete or accurate or up to date. The accuracy of any instructions, formulae, and drug doses should be independently verified with primary sources. The publisher shall not be liable for any loss, actions, claims, proceedings, demand, or costs or damages whatsoever or howsoever caused arising directly or indirectly in connection with or arising out of the use of this material.
Transcript
This article was downloaded by: [Dalhousie University]On: 12 March 2013, At: 12:38Publisher: Taylor & FrancisInforma Ltd Registered in England and Wales Registered Number: 1072954 Registeredoffice: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
Journal of Toxicology and EnvironmentalHealth, Part A: Current IssuesPublication details, including instructions for authors andsubscription information:http://www.tandfonline.com/loi/uteh20
Human Health Risk and ExposureAssessment of Chromium (VI) in TapWaterDennis Paustenbach a , Brent Finley a , Fionna Mowat b & BrentKerger ca ChemRisk®, Alameda, California, USAb Exponent, Menlo Park, California, USAc Health Science Resource Integration, Inc., Tallahassee, Florida,USAVersion of record first published: 07 Jan 2011.
To cite this article: Dennis Paustenbach , Brent Finley , Fionna Mowat & Brent Kerger (2003): HumanHealth Risk and Exposure Assessment of Chromium (VI) in Tap Water, Journal of Toxicology andEnvironmental Health, Part A: Current Issues, 66:17, 1295-1339
To link to this article: http://dx.doi.org/10.1080/15287390306388
PLEASE SCROLL DOWN FOR ARTICLE
Full terms and conditions of use: http://www.tandfonline.com/page/terms-and-conditions
This article may be used for research, teaching, and private study purposes. Anysubstantial or systematic reproduction, redistribution, reselling, loan, sub-licensing,systematic supply, or distribution in any form to anyone is expressly forbidden.
The publisher does not give any warranty express or implied or make any representationthat the contents will be complete or accurate or up to date. The accuracy of anyinstructions, formulae, and drug doses should be independently verified with primarysources. The publisher shall not be liable for any loss, actions, claims, proceedings,demand, or costs or damages whatsoever or howsoever caused arising directly orindirectly in connection with or arising out of the use of this material.
HUMAN HEALTH RISK AND EXPOSURE ASSESSMENT OF CHROMIUM (VI) IN TAP WATER
Dennis J. Paustenbach, Brent L. Finley
ChemRisk®, Alameda, California, USA
Fionna S. Mowat
Exponent, Menlo Park, California, USA
Brent D. Kerger
Health Science Resource Integration, Inc., Tallahassee, Florida, USA
Hexavalent chromium [Cr(VI)] has been detected in groundwater across the United States dueto industrial and military operations, including plating, painting, cooling-tower water, andchromate production. Because inhalation of Cr(VI) can cause lung cancer in some personsexposed to a sufficient airborne concentration, questions have been raised about the possiblehazards associated with exposure to Cr(VI) in tap water via ingestion, inhalation, and dermalcontact. Although ingested Cr(VI) is generally known to be converted to Cr(III) in the stomachfollowing ingestion, prior to the mid-1980s a quantitative analysis of the reduction capacity ofthe human stomach had not been conducted. Thus, risk assessments of the human health hazardposed by contaminated drinking water contained some degree of uncertainty. This articlepresents the results of nine studies, including seven dose reconstruction or simulation studiesinvolving human volunteers, that quantitatively characterize the absorbed dose of Cr(VI) fol-lowing contact with tap water via all routes of exposure. The methodology used here illustratesan approach that permits one to understand, within a very narrow range, the possible intakeof Cr(VI) and the associated health risks for situations where little is known about historicalconcentrations of Cr(VI). Using red blood cell uptake and sequestration of chromium as an invivo metric of Cr(VI) absorption, the primary conclusions of these studies were that: (1) oralexposure to concentrations of Cr(VI) in water up to 10 mg/L (ppm) does not overwhelm thereductive capacity of the stomach and blood, (2) the inhaled dose of Cr(VI) associated withshowering at concentrations up to 10 mg/L is so small as to pose a de minimis cancer hazard,and (3) dermal exposures to Cr(VI) in water at concentrations as high as 22 mg/L do notoverwhelm the reductive capacity of the skin or blood. Because Cr(VI) in water appears yellowat approximately 1–2 mg/L, the studies represent conditions beyond the worst-case scenario
Received 14 June 2002; accepted 11 February 2003. Pacific Gas and Electric (PG&E) primarily funded the research described in this article, at a cost in
excess of $1 million. The costs and time necessary to prepare this article were borne by the authors. Theauthors have served as expert witnesses in litigation involving the health hazards associated with Cr(VI)in tap water.
Current affiliation for Brent L. Finley is Exponent, Oakland, CA, USA. Address correspondence to Dr. Dennis J. Paustenbach, ChemRisk®, 65 Roan Pl, Woodside, CA 94062,
for voluntary human exposure. Based on a physiologically based pharmacokinetic model forchromium derived from published studies, coupled with the dose reconstruction studiespresented in this article, the available information clearly indicates that (1) Cr(VI) ingested intap water at concentrations below 2 mg/L is rapidly reduced to Cr(III), and (2) even traceamounts of Cr(VI) are not systemically circulated. This assessment indicates that exposure toCr(VI) in tap water via all plausible routes of exposure, at concentrations well in excess of thecurrent U.S. Environmental Protection Agency (EPA) maximum contaminant level of 100 µg/L(ppb), and perhaps those as high as several parts per million, should not pose an acute orchronic health hazard to humans. These conclusions are consistent with those recently reachedby a panel of experts convened by the State of California.
Quantitative estimates of human exposure to chemicals in foods, consumerproducts, and the environment are typically based on numerous underlyingassumptions regarding representative chemical concentrations in variousmedia, transport and fate, human behavior patterns, bioavailability, and manyother considerations (Paustenbach, 2000). Some degree of uncertainty existsin many of these exposure parameters and assumptions, and this uncertainty isreflected in the ultimate estimate of exposure and potential health risk. Inmany instances, especially when the exposures occurred in the past and littlesampling information is available, the use of exposure simulation studies,which recreate the actual exposure conditions of interest, can reduce much ofthis uncertainty (Gargas et al., 1994; Finley et al., 1996, 1997; Corbett et al.,1997; Madl & Paustenbach, 2002). As illustrated here, simulation studies, inconjunction with collection of chemical or biological data from human volunteerstudies, can significantly improve the confidence in the ultimate risk assessment.
Depending on the study objectives and desired degree of certainty, dosereconstruction techniques, which can also include simulations, can vary widelywith respect to scope and complexity. For example, a simple hand-wipe testmight be used to assess the amount of lead that leaches from a consumer item(e.g., hose of a vacuum cleaner) onto the skin following normal handling; theseresults then could be used in conjunction with hand-to-mouth transfer andoral bioavailability estimates, and possibly a pharmacokinetic model, to estimatepotential increases in blood lead levels resulting from use of the product. Alter-natively, one may choose to conduct a more direct analysis, in which bloodlead levels are actually measured before and after use of the product; however,in many cases like this one, the dose is often low, and the resulting change ina biological fluid may be too small to measure, so indirect methods are needed.Either approach will yield exposure/dose estimates that contain less uncertaintythan those obtained strictly through literature-based estimates, surrogate data,or “professional judgment.” In recent years, more accurate estimates of histor-ical (past) exposure have been needed in epidemiology studies and in somepersonal injury cases, and, as a consequence, both dose reconstructions andexposure simulations have become more refined and more common (Wier et al.,2001; Widner & Flack, 2002; Madl & Paustenbach, 2002; Williams &Paustenbach, 2002, 2003; Boelter et al., 2002).
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
12:
38 1
2 M
arch
201
3
RISK FROM CR(VI) IN DRINKING WATER 1297
Simulation studies often involve recreating occupational conditions thatare representative of an exposure setting for which few or no data exist. Forexample, Madl and Paustenbach (2002) recently described an occupationalexposure simulation study in which airborne concentrations of benzene andother chemicals were measured in an enclosed “roundhouse” where dieseltrain engines were serviced. Workplace exposures were recreated by operatingthe diesel engines inside a turn-of-the-century roundhouse under a variety ofconditions. The objective of the analysis was to assess whether benzene expo-sures posed an increased risk of certain types of cancers in maintenancepersonnel. At the time, there was little or no information regarding occupationalindoor exposure to benzene due to diesel exhaust.
Exposure simulation and dose reconstruction techniques are being usedmore frequently within regulatory, academic, and legal settings. In the regulatorysetting, for example, the U.S. Environmental Protection Agency (EPA) recentlyconducted a study in which human volunteers ingested capsules containingprescribed amounts of lead-bearing soils (Maddaloni et al., 1998). The oralbioavailability of lead was determined under both fasting and fed conditions,and these data were considered in the development of health-based soilstandards. Others have similarly used human volunteers to assess the oralbioavailability of chromium in soils contaminated with chromite-ore proces-sing residue (Gargas et al., 1994). Another recent study examined the oralbioaccessibility of dioxin from contaminated soils using fresh human gastricfluids (Ruby et al., 2002). Similarly, nearly $5 million in research has beenconducted over the past 15 years in an attempt to quantitatively understandthe amount of soil that is ingested by children each day (Calabrese et al., 1996,1997; Calabrese & Stanek, 1998). This research has used fecal tracer studies toquantitatively measure soil ingestion rates in young children and thereby todiminish the level of uncertainty associated with this parameter (Davis et al.,1990; Calabrese & Stanek, 1991, 1995).
One issue that has drawn the concern of agencies and the courts in recentyears is residential exposure to hexavalent chromium [Cr(VI)] in groundwater.One concern could likely be the magnitude of past exposures. Three yearsago, a more sensitive analytical procedure was adopted for measuring Cr(VI) inwater supplies. Using this method, the California Department of Health Serviceshas evaluated all primary drinking water supplies for 25 million Californians.Surprisingly, they found that as much as 30% of California’s public water sup-ply might contain measurable levels of Cr(VI) (Department of Health Services[DHS], 2002). However, most (70%) of the detections were very low (<5 µg/L)and may be attributable to analytical error or contributions from naturalsources.
To know whether groundwater containing Cr(VI) needs to be remediated,an understanding of the hazard is necessary. If there are concerns about thehazard to the community, then dose reconstruction will often be useful tocharacterize the range of possible exposures. Fortunately, because of the dis-tinct physicochemical properties of Cr(VI), it is possible to characterize the
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
12:
38 1
2 M
arch
201
3
1298 D. J. PAUSTENBACH ET AL.
upper-bound exposures of persons who may have been acutely or chronicallyexposed to Cr(VI) via tap water, as well as the health risks, using both in vitroand in vivo animal studies, and human volunteer studies. This article describessuch studies in an effort to reduce the uncertainty associated with current riskassessments that rely on human in vivo data. The data and the conclusionsfrom the following analysis should be applicable to any setting where exposureto water containing up to 10mg/L Cr(VI) has occurred. The current U.S. EPAmaximum contaminant level (MCL) for total chromium in drinking water is100 µg/L (ppb), or 0.1mg/L (ppm).
TRIVALENT AND HEXAVALENT CHROMIUM: ENVIRONMENTAL OCCURRENCE AND TOXICITY
Environmental OccurrenceTrivalent chromium [Cr(III)], the most environmentally stable valence state
of chromium, occurs naturally in most environmental media as a water-insolubleform (Barnhart, 1997; James et al., 1997). Cr(III) is an essential micronutrientwith a recommended daily requirement in the range of 50–200µg/d for humans(Anderson & Kozlovsky, 1985) and an estimated mean adequate intake levelof 35 µg/d for males and 25 µg/d for females (National Academy of Sciences[NAS], 2001). Cr(III) has extremely low or no toxicity via all routes of humanexposure and does not pose a cancer hazard (Agency for Toxic Substances andDisease Registry [ATSDR], 2001; U.S. EPA, 1998; International Agency forResearch on Cancer [IARC], 1990; World Health Organization [WHO], 1988).
In contrast, Cr(VI) rarely occurs naturally and is produced primarily inindustrial processes and by human activities (e.g., as a combustion product).Many Cr(VI) compounds are highly water soluble and at neutral pH, mono-chromate may be found as a contaminant in groundwater. However, Cr(VI)has a tendency to be reduced to Cr(III) in the presence of low pH and/ororganic material. Although Cr(VI) released to soil is expected to be reduced to thetrivalent state, if the concentration in water is high or the reduction capacity ofthe soil is very low (as in sandy soils), the Cr(VI) may not be reduced before itreaches groundwater.
Occupational exposure to Cr(VI) is associated with dermal irritation andallergic dermatitis following skin contact (Adams, 1990). Respiratory effects,including lung cancer, can result from high exposure to airborne Cr(VI) in theworkplace. The current Occupational Safety and Health Administration(OSHA) permissible exposure limit (PEL) is 52 µg/m3 and OSHA is currently inthe process of setting a new standard anticipated in 2006.
Toxicity of Cr(VI) and Routes of Exposure The potential adverse effects resulting from exposure to chromium are
dependent not only on the form of chromium administered, but also on the
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
12:
38 1
2 M
arch
201
3
RISK FROM CR(VI) IN DRINKING WATER 1299
route of exposure. The possible adverse effects associated with the three primaryroutes of exposure (e.g., ingestion, inhalation, and dermal contact) are depend-ent on the dose and are described separately below.
Adverse Effects of Ingestion of Cr(VI) The ingestion of Cr(VI) granulesor highly concentrated solutions can occur as the result of accident or suicide.In these cases, the damage can be severe and will generally occur shortly afterthe incident. These cases are rare. In contrast, it is plausible that persons in thecommunity could be exposed to Cr(VI) in tap water. Here, exposure occurs viadirect consumption of tap water and its use for beverages, such as coffee, tea,and juices, and in cooking. Figure 1 shows the influence of Eh and pH on chro-mium speciation in a variety of beverages. Some degree of incidental ingestionmay also occur during showering or swimming, although the dose via thesepathways is typically negligible compared with direct ingestion.
Like all chemicals, the likelihood of carcinogenic and noncancer effects oforal exposures to Cr(VI) are dependent on the dose. Ingestion of very highconcentrations of Cr(VI) (>200mg/L) by humans, and acute doses by laboratoryanimals, can result in gastritis, nephrotoxicity, and hepatotoxicity. Death may
FIGURE 1. Eh–pH predominance diagram for soluble chromium species, with location of selectedbeverages : � = lemonade; + = Kool Aid; � = tap water; � = tea; � = drip coffee; � = percolated coffee;x = orange juice.
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
12:
38 1
2 M
arch
201
3
1300 D. J. PAUSTENBACH ET AL.
occur if the doses were sufficient. These noncarcinogenic effects are absent atlower doses (ATSDR, 2001; U.S. EPA, 1984, 1990, 1998; IARC, 1990; WHO,1988; Gross & Heller, 1940).
Many in vitro, whole-animal, and human volunteer studies indicate thatwhen Cr(VI) comes in contact with biological fluids and tissues, reduction toCr(III) occurs rapidly due to the presence of reducing agents that keep thebody in homeostasis (DeFlora & Wetterhahn, 1989; DeFlora et al., 1997;DeFlora, 2000). As shown in Figure 2, these agents can reduce substantialamounts of Cr(VI). If sufficient Cr(VI) is absorbed such that the route-specificbarriers to oxidative attack are overwhelmed (e.g., tissue capacity is exceeded),then Cr(VI) reduction within the cell may lead to cell damage and/or death
FIGURE 2. Estimates of Cr (VI) sequestration or reduction by organs, cell populations, and fluids in thehuman body. Adapted from De Flora et al. (1997).
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
12:
38 1
2 M
arch
201
3
RISK FROM CR(VI) IN DRINKING WATER 1301
(DeFlora & Wetterhahn, 1989). The pharmacokinetic and pharmacodynamicimplications of this change in valence are complex and highly route dependent.
There is some controversy regarding the carcinogenic hazard posed bychronic ingestion of Cr(VI) in water at relatively low concentrations. For example,a recently published review presented multiple lines of evidence regarding thecarcinogenicity of Cr(VI) following ingestion (Costa, 1997). However, based onhis more than 20years of studying Cr(VI), De Flora concluded that “all experi-mental and epidemiological data, and the underlying mechanisms, point tothe occurrence of thresholds in chromium(VI) carcinogenesis.” Similarly, manyinternational and governmental panels have indicated that the evidence isinsufficient to conclude that Cr(VI) is carcinogenic via the oral route of exposure(Canada, 1997; IARC, 1980, 1990; International Chromium DevelopmentAssociation [ICDA], 1997; WHO, 1988, 1993; Rowbotham et al., 2000). Thisview was reinforced recently by a science advisory board convened by theCalifornia EPA, which specifically addressed the drinking water hazard (Flegalet al., 2001).
There has been some disagreement within the regulatory communityregarding the oral carcinogenicity of Cr(VI). One animal study, which assessedthe cancer hazard posed by ingestion of Cr(VI) in water at more than 100 ppm,reported that there may have been an increased incidence of tumors of theforestomach under the conditions of the test (Borneff et al., 1968). As a conse-quence, hesitance by some regulatory agencies and scientific bodies suggests thatCr(VI) “may” pose a cancer risk following ingestion (Office of EnvironmentalHealth Hazard Assessment [OEHHA], 1999). A few assays also seem to suggestpositive responses for Cr(III) compounds; however, most reviewers believe thatthese positive responses are the result of placing soluble Cr(III) ions in directcontact with extracted deoxyribonucleic acid (DNA), a situation that cannotplausibly occur in whole animals because of the presence of membranes andother factors. Nonetheless, it has been suggested that more should be knownbefore agencies conclude that ingestion is not a possible cancer hazard (Costa,2003).
Adverse Effects Associated with Inhalation of Cr(VI) In contrast withoral exposure, on a mass basis, the respiratory tract has a lesser capacity toreduce Cr(VI) to Cr(III) and thereby protect the cells from toxic effects. Inhalationexposure to Cr(VI) by workers in the chromite-ore processing, metal plating,ferrometals, and pigment manufacturing occupations has been associated withsignificantly elevated rates of lung and nasal cancer (Proctor, Panko et al.,2002; Shi et al., 1999; U.S. EPA, 1998; ICDA, 1997; IARC, 1990).
Respiratory irritation has been observed at concentrations as low as 2µg/m3
in the chrome plating industry (Lindberg & Hedenstierna, 1983). The forms ofCr(VI) used in the industries in which irritation has been observed are usuallycorrosive or otherwise irritating, and it is possible that these properties havecontributed to the observed diseases. Specifically, perhaps repeated irritation andcytotoxicity is the mechanism for tumor formation due to repeated cell turnover,as is the case for formaldehyde (Gibson, 1983). Low levels of Cr(VI) in tap water
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
12:
38 1
2 M
arch
201
3
1302 D. J. PAUSTENBACH ET AL.
would not be corrosive or irritating following the inhalation of mists duringshowering or related activities and would therefore not be expected to pose anacute inhalation hazard.
Questions have been raised about the possible systemic cancer hazardassociated with inhalation or ingestion of Cr(VI). Clear evidence of clinicaldisease due to inhalation exposure at tissues distant from the lung has notbeen observed in any consistent manner in the many occupational studies thathave been conducted (IARC, 1990; Rowbotham et al., 2000; Proctor et al.,2002a). This is not surprising given the mechanism of action that is likelyinvolved in the production of the lung tumors that have been observed, andthe rapid reduction of Cr(VI) to Cr(III) by not only the lung, but also the blood.No regulatory body of which we are aware has stated that there is sufficientpublished information to conclude that Cr(VI) can cause an increased risk ofcancer at tissues distant from the lung.
Adverse Effects Associated with Dermal Contact With Cr(VI) Dermalcontact with Cr(VI) can induce or elicit (in a previously sensitized individual)a Type IV allergic contact dermatitis (ACD) response, and increased incidencesof ACD have been observed in the construction industry (Adams, 1990;Nethercott et al., 1994). Reports of Cr(VI)-induced ACD responses in non-occupational settings are less frequent, but such responses may occur followingextended dermal contact with a Cr(VI)-containing item (e.g., leather shoes)(Marks & Deleo, 1992).
To date, there have been no case reports of elicitation or induction ofACD following contact with dissolved Cr(VI) in tap water or groundwater.Systemic effects due to dermal contact with either Cr(III) or Cr(VI) are virtuallynonexistent, except in rare cases of acute poisoning.
IDENTIFYING EXPOSURE SCENARIOS FOR THE DOSE RECONSTRUCTION OF CHROMIUM-CONTAMINATED TAP WATER
Any dose reconstruction of contaminated tap water should be based onreasonable exposure factors to characterize any specific acute and/or long-termhuman hazards. This includes using representative ranges of chromium con-centrations in tap water, as well as realistic descriptions regarding the likelyroute and frequency of exposure. Possible sources and routes of exposure towater containing concentrations of chromium over background are presentedin Table 1.
The complexities of Cr(VI) interactions with organic matter require carefulconsideration of several lines of evidence regarding its potential genotoxicand/or carcinogenic potential, going beyond simple interpretations of in vitroassays, and taking into consideration the whole-body pharmacokinetics,detoxification mechanisms, and their effects at plausible environmental doses.Evaluation of factors that influence the absorption and change in valence stateof chromium, whether it is ingested, inhaled, or taken up through the skin,must be considered.
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
12:
38 1
2 M
arch
201
3
RISK FROM CR(VI) IN DRINKING WATER 1303
In situations where historical data on Cr(VI) in groundwater or tap waterare either not reliable or not available, it is fortunate that a readily apparent“observational benchmark” can be used to define an upper-bound Cr(VI)concentration. Specifically, for Cr(VI), voluntary human exposure would notbe expected above concentrations of 1 to 2 mg/L, because at this concen-tration, the water nearly always has an apparent yellow color. Due to thediscoloration, swimming in or ingesting water above this concentration ishighly unlikely.
HUMAN VOLUNTEER STUDIES EVALUATING THE INGESTION HAZARD OF CR(VI) IN TAP WATER
It has been generally understood within the toxicology community thatingestion of low doses (<0.1 mg/L) of Cr(VI) should not pose a health hazard.This lack of oral toxicity is believed to be due, in part, to the rapid reduction ofCr(VI) in the stomach to Cr(III) prior to systemic absorption (De Flora et al.,1987; Donaldson & Barreras, 1966). However, only in vitro and some in vivoanimal data (e.g., MacKenzie et al., 1958) and very little in vivo human data(e.g., Donaldson & Barreras, 1966) were available to support this hypothesisfor humans prior to the 1990s. The animal data were suggestive, but not con-clusive, that Cr(VI) would quickly be converted to Cr(III) (Mirsalis et al., 1996).Over time, questions have been raised about the appropriateness of usingrodent studies to predict the human gastrointestinal (GI) tract responses. Thus, itwas concluded that it might be useful (and probably necessary if the issue wereto be resolved in litigation) to conduct studies involving human volunteers.Because it was well understood that there had to be a threshold dose, belowwhich complete and rapid reduction would occur in the stomach, conductingthe tests on volunteers was considered safe and appropriate if the studies were
TABLE 1. Possible Sources of Exposure to Contaminated Water
a Excluded as de minimis exposure based on empirical data for Cr(VI) reduction and/or based on screeningcalculations indicating that relative intake from event would be less than 1% of route-specific doses thatwere assessed in detail.
b All dermal contact exposures were considered de minimis based on Corbett et al. (1997) showing noappreciable Cr(VI) uptake following human volunteer immersion in heated, chlorinated water containing22 mg/L Cr(VI) for 3 h continuously.
Tap water ingestion Shower aerosols Bathing/washingb Beverages mixed with tap watera Swamp cooler aerosolsa Swimmingb Ingestion of foods with residuesa Irrigation sprinkler drift Playing or working in areas with
sprinklersbIngestion of local cow’s milka Splashes while swimminga Ingestion of homegrown Contaminated soil and dustsa Contaminated soil contactb
vegetablesa
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
12:
38 1
2 M
arch
201
3
1304 D. J. PAUSTENBACH ET AL.
designed properly. The studies conducted to quantify historical exposures toCr(VI) in tap water, as well as the human response, are described in the follow-ing sections.
The rationale for conducting these studies is the unique ability of Cr(VI) tointeract with the red blood cell (RBC). The high capacity of the RBC tosequester and bind Cr(VI) has been recognized for decades, and radiolabeledCr(VI) has been used as a biomarker to study the life span of the RBC inhumans (Gray & Sterling, 1950). RBC chromium content has also been used tocharacterize occupational Cr(VI) exposures (Lewalter et al., 1985; Korallus,1986; Miksche et al., 1994). The chromate ion is taken up via the anion trans-port channel (Figure 3), and once inside the RBC, the Cr(VI) is rapidly reducedto unstable intermediates, which become bound to hemoglobin and otherintracellular ligands.
FIGURE 3. Cr(VI) and Cr(III) uptake in red blood cells (RBC). This schematic depicts how Cr(VI) readilyenters the RBC, where it is reduced to short-lived reactive intermediates, Cr(V) and Cr(IV), and bound tohemoglobin (Hb) and soluble ligands (L) such as glutathione and amino acids. Essentially complete bindingof intracellular Cr(VI) to Hb occurs because >30% of RBC mass is Hb. The Hb-bound Cr complexes remainpart of the RBC for its entire life span. Conversely, water-soluble Cr(III) moves across the cell membrane viamuch slower diffusion and perhaps other processes related to the chemical structure of the attached ligands.
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
12:
38 1
2 M
arch
201
3
RISK FROM CR(VI) IN DRINKING WATER 1305
Table 2 summarizes the results of a series of human volunteer studies thatwere conducted to understand the uptake and excretion following ingestion ordermal contact of Cr(VI) under a wide variety of single- and multiple-doseregimens (Finley et al., 1997; Kerger, Paustenbach et al., 1996; Kerger et al.,1997; Paustenbach et al., 1996; Corbett et al., 1997; Kuykendall et al., 1996).These are described separately in the following sections.
Question I: What Are the Effects of Repeated Ingestion of Cr(VI)? Toevaluate the dose-related pharmacokinetics of chromium in humans afterrepeated ingestion, water Cr(VI) concentrations ranging from 0.1 to 10 mg/L(as potassium dichromate [K2Cr2O7]) were consumed daily for durations rangingfrom days to weeks (Paustenbach et al., 1996; Finley et al., 1997). In the firststudy, the uptake and elimination of Cr(VI) were measured to estimate thesteady-state concentrations of chromium in blood and urine following ingestionof 2 L/d of drinking water containing 2mg/L Cr(VI). Ingestion occurred for aperiod of 17 consecutive days (Paustenbach et al., 1996). The objective was todetermine whether all Cr(VI) was reduced before entering the blood and tofurther understand the pharmacokinetics of Cr(VI) following ingestion. In thesecond study, volunteers ingested approximately 333 ml of Cr(VI)-containingdrinking water at 6-h intervals daily for 3d (Finley et al., 1997). This dosingregimen is consistent with residential tap water consumption rates. Oral expo-sure was conducted using a series of concentrations ranging from 0.1 to 10mg/L.
In both studies, urine, plasma, and red blood cell (RBC) chromium con-centrations were measured in each of the human volunteers before, during,and after ingestion of prescribed quantities of water. Urinary chromiumconcentrations are often used as biomarkers of exposure due to the ease ofcollection and analysis, and because systemically absorbed chromium is excretedprimarily in the urine; thus, all postingestion urine voids were collected andassayed. Because urine analysis alone cannot provide information regarding thevalence state of chromium, blood chemistry was also evaluated to distinguishbetween Cr(III) and Cr(VI). A Human Use Committee approved the test proto-cols for each study, and all volunteers were consenting adults (all were eithertoxicologists or physicians) weighing 190 to 220 lb, and 30 to 54yr of age.Each individual recorded diet and exercise during the study, because thesefactors are known to potentially affect the concentration of chromium and/orcreatinine in urine. The only restriction on diet was that they not ingest vitaminsupplements containing vitamin C or chromium.
The volunteers collected each urine void during the study, and thesamples were then analyzed separately for total chromium and creatinine.Often, this required collection of 15 samples per day per volunteer. Over thecourse of these studies, more than 1000 samples of urine were collected andanalyzed. Blood samples were obtained on a specified schedule (sometimesevery day) and were sent to the laboratory for analysis of total chromium inboth the plasma fraction and the RBC fraction. In certain studies, blood andurine samples were analyzed immediately after collection for the presence ofCr(VI). Intermittent samples of urine and blood were also collected for standard
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
12:
38 1
2 M
arch
201
3
1306 D. J. PAUSTENBACH ET AL.
TABLE 2. Summary of Volunteer Uptake Studies on Water-Soluble Chromium Compounds
Study Subjects and regimen Key observations
Kerger et al. (1996) and Kuykendall et al. (1996)
Five healthy adults per dose group, ages 26 to 63. Single bolus dose of 5 mg Cr in 0.5 L of water (10 mg/L) ingested within 2 min. Cr administered in separate studies of inorganic Cr(III); organic Cr(III) from Cr(VI) in orange juice; and dichromate in water. Doses taken 2 to 5 h after last meal.
1. No apparent clinical changes or health effects.
2. Rapid uptake of Cr observed following all three dosing regimens.
4. No sustained elevation of RBC Cr levels, a marker for Cr(VI) uptake.
5. No Cr(VI) measurable in plasma or urine at peak of uptake/excretion.
6. No elevation of DNA-protein cross-links in peripheral lymphocytes.
Finley et al. (1997)
Five healthy adults per dose group, ages 33 to 62. Three daily doses of 0.33 L of Cr(VI) in water for 3 consecutive d. Sequential dosing for 3 d on, 2 d off, at Cr(VI) levels of 0.1, 0.5, or 1 mg/L. Doses taken at least 2 h after last meal.
1. No apparent clinical changes or health effects.
2. Cr uptake and excretion apparent at all dose levels.
3. Similar, low percentage bioavailability for all dose levels.
4. No sustained elevation of RBC Cr levels, a marker for Cr(VI) uptake.
Kerger et al. (1997)
Three healthy adults per dose group, ages 33 to 42. Three daily doses of 0.33 L of Cr(VI) in water for 3 consecutive d, 3 d on, 2 d off, at 5 or 10 mg/L. Doses taken at least 2 h after last meal.
1. No apparent clinical changes or health effects.
2. Bioavailability was markedly higher compared to prior study ≤1 mg/L.
3. No sustained RBC Cr elevation in two of three volunteers; one volunteer had higher bioavailability and moderate elevation of plasma and RBC Cr levels, which suggests Cr(III) tissue loading kinetics.
Paustenbach et al. (1996)
One healthy adult, age 42. Ad libitum ingestion of 2 L/d of 2 mg/L Cr(VI) for 17 consecutive d.
1. No apparent clinical changes or health effects.
2. Steady state Cr levels reached in blood and urine within 3 to 7 d.
3. No sustained elevation of RBC Cr levels after cessation of exposure.
4. No elevation of DNA-protein cross-links in peripheral lymphocytes.
Corbett et al. (1997)
Four healthy adults, ages 20 to 42. Bathing for 3 h, submerged to shoulders in heated bath (95 °F) with 22 mg /L Cr(VI).
1. No apparent clinical changes or health effects.
2. Limited systemic uptake shown by blood and urine Cr levels.
3. No sustained elevation of RBC Cr levels, a marker for systemic Cr(VI) uptake.
4. Dermal penetration rate for systemic uptake of total Cr (as cumulative urinary Cr) ≤4 × 10−4 cm/h.
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
12:
38 1
2 M
arch
201
3
RISK FROM CR(VI) IN DRINKING WATER 1307
urinalysis, complete blood count (CBC), and Sequential Multiple Analyzer(SMA)-24 blood chemistry screens to ensure the health of the volunteers. Noneof the volunteers involved in any of these studies experienced any apparentadverse health effects as a result of the chromium exposures, nor were any ofthe clinical tests appreciably different when pre- versus postexposure results werecompared.
Results of the exposure simulation studies indicate that, at the lowerconcentrations (0.1, 0.5, 1, and 2mg/L), there was no evidence of measurablesystemic uptake of Cr(VI). This observation is perhaps best illustrated for long-term environmental exposures to waterborne Cr(VI) in the study of a humanvolunteer who ingested 2L/d of water containing 2mg/L Cr(VI) for 17 consecutivedays (Figure 4) (Paustenbach et al., 1996). As shown in Figure 4A, followingonset of dosing, total urinary excretion of chromium was clearly elevated abovepre-study background levels (1.6 ± 1.6 µg/d) for the entire dosing period. Thepeak urine concentration occurred on d 7 (68 µgCr/g creatinine) and steadystate was estimated as 43 µg/d, based on average daily chromium excretion ond 7 to 16. Within 2 to 4d after the final Cr(VI) dose on d 16, approximatebackground elimination of chromium in urine was again observed. The steady-state concentration of chromium in plasma and RBC occurred approximately7d after initial exposure, with peak concentrations occurring on approximatelyd 10 (see Figure 4B). Both plasma and RBC chromium concentrations returnedto background levels within 2–4d after the final dose, and returned to prestudylevels within 1–2 d following cessation of exposure.
In addition to estimation of steady state, the elimination half-life forchromium in plasma was calculated at 3 days after cessation of dosing. Theresults indicate an estimated half-life of 36 h. Although this calculation is basedon ingestion of chromium in a single volunteer, this observation is consistentwith previous investigations in which the oral uptake of Cr(VI) was shown tohave an elimination half-life in humans of approximately 36 h, based onplasma and urine measurements (Kerger, Paustenbach et al., 1996). Bioavailabil-ity was also calculated as the cumulative amount of chromium excreted inurine above background, normalized to the total dose ingested. The relativelylow bioavailability (2%) and lack of sustained elevation of chromium in RBCafter dose cessation indicate that virtually all of the Cr(VI) at a concentration of2mg/L is reduced to Cr(III) in the gut (Paustenbach et al., 1996).
Finley et al. (1997) reported that 3 d of ingesting 1L/d of tap watercontaining 0.1, 0.5, and 1 mg/L Cr(VI) in 5 human volunteers showed meanuniform urinary excretion of chromium averaging between 1.2% and 1.7% ofthe administered total dose (Table 3). No substantial or sustained elevation ofRBC or plasma chromium levels was observed at these Cr(VI) dose levels, indi-cating no measurable uptake of the hexavalent form into the systemic circulation.It is clear that some form of chromium, likely organic complexes of Cr(III), wasabsorbed in the blood for all volunteers at all dose levels. The proportion oftotal chromium excreted in urine represented a uniform percentage of thetotal administered dose for each volunteer at Cr(VI) concentrations from 0.1to 1.0mg/L. The urinary excretion of chromium at 5 mg/L Cr(VI) (1.7%) was
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
12:
38 1
2 M
arch
201
3
1308 D. J. PAUSTENBACH ET AL.
comparable to that observed at lower concentrations, but 10 mg/L Cr(VI)approximately doubled the urinary excretion of chromium (averaging 3.5% ofadministered dose) (Table 3). Even at the highest dose of 10 mg/L Cr(VI), theblood kinetic profiles were consistent with the absorption of Cr(III), not Cr(VI)(Finley et al., 1997). Specifically, increased serum and RBC chromium levels weretransient and did not remain high for an appreciable period of time (Figure 5).
Results indicate an approximate 50% decrease occurring 7 d postdosing,a decline that is hypothesized as evidence of systemic absorption of Cr(III), not
FIGURE 4. Blood concentrations of total chromium following ingestion of 2 mg Cr(VI)/L in water for 17 d:(A) The time course and (B) magnitude of plasma and RBC chromium concentrations. The historicalbackground chromium levels for this volunteer are indicated by the line labeled BKG. Adapted fromPaustenbach et al. (1996).
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
12:
38 1
2 M
arch
201
3
RISK FROM CR(VI) IN DRINKING WATER 1309
Cr(VI) (Paustenbach et al., 1996; Finley et al., 1997), followed by a slower,gradual decline with concurrently elevated plasma and RBC chromium levels.Plasma and RBC concentrations in one subject were clearly elevated (>20µg/L),even 14 d after the last dose. This is likely due to tissue loading with Cr(III)organic complexes, a phenomenon that has also been observed in rats admin-istered chromium tripicolinate (Anderson et al., 1996).
Question II: What Are the Kinetic Differences Between Different Forms of Chromium? To understand whether different forms of chromium had different
pharmacokinetic profiles, the blood and urine levels were studied followingingestion of single doses of both Cr(III) and Cr(VI) in drinking water (Kerger,Paustenbach et al., 1996; Kerger et al., 1997). The forms of chromium studied
TABLE 3. Urinary Excretion of Total Chromium over 4 d Following Oral Ingestion of Cr(VI) in DrinkingWater for Five Human Volunteers
Note. NA, not assessed for that specific subject. The excreted values are the total urinary chromiumexcreted for each of the 3 dosing days and 1 d postdose. Values in parentheses represent percentages ofadministered chromium dose excreted within 4 d after the first dose. Percentage chromium excreted wascalculated by summing the total chromium in urine per day for 3 dosing days and 1 d postdose, aftercorrecting for prestudy background urinary chromium concentrations and dividing by the total amount ofchromium administered. Prestudy mean, historical mean, and historical range from measurements takenprior to dosing. Historical values include background measurements from studies in addition to the currentone in which the volunteer participated. Adapted from Finley et al. (1997).
included highly soluble Cr(III) as chromic trichloride (CrCl3), potassium dichro-mate reduced with orange juice to form organic-ligand forms of Cr(III) [Cr(III)-OJ],and potassium dichromate alone in deionized water (K2Cr2O7). In these studies,human volunteers ingested a single bolus dose of 0.5 L water containing 5 mgchromium (10 mg/L concentration) within 2min on an empty stomach. RBCand plasma chromium profiles were examined 1 to 3 d prior to the study atseveral time points following ingestion, and from minutes after the bolus dosewas administered to 12 d postdosing. Record keeping, study approval by a
FIGURE 5. Concentrations of chromium in plasma and RBCs of volunteers following ingestion of 1 L/dof water containing either 5 or 10 mg Cr(VI). From Finley et al. (1997).
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
12:
38 1
2 M
arch
201
3
RISK FROM CR(VI) IN DRINKING WATER 1311
Human Use Committee, and sample collection and analysis were similar tothose followed by Paustenbach et al. (1996) and Finley et al. (1997).
Kerger, Paustenbach et al. (1996) reported that all three forms of chro-mium were capable of increasing urinary excretion and RBC and plasmacontent of chromium, and that each exhibited quite different pharmacokineticpatterns. Urinary excretion results indicate increasing bioavailability (0.13%,0.60%, and 6.9%) and elimination half-life (10, 15, and 39 h) for the CrCl3,Cr(VI)-OJ, and Cr(VI)-only treatment groups, respectively (Table 4). During thefirst 3–5d, the volunteers excreted 70–82% of the total chromium measuredin urine for CrCl3, 90–96% for Cr(III)-OJ, and 76–82% for the Cr(VI)-only treat-ment group. A dose-related increase in peak concentration and cumulativeurinary excretion has been observed in another study by these investigators(Figure 6). For the Cr(VI)-only group, the elimination half-life was calculated tobe 39.3 h (range, 36–41 h), which supports findings from the study conductedby Paustenbach et al. (1996).
Chromium mixtures tend to form Cr(III) organic complexes, as shown incertain animal studies (e.g., Anderson et al., 1997), and these complexes aredistributed more slowly than ionic complexes. In this study, the Cr(III) organiccomplexes, formed by addition of Cr(VI) to orange juice, were orally absorbed,four times more readily and exhibited a urinary excretion half-life almostdouble that for CrCl3. These data suggest that Cr(VI) intake can result in theformation of Cr(III) organic complexes in the digestive tract, and possibly othertissues, resulting in enhanced uptake into the blood and proportionatelygreater urinary excretion. This was also shown in a study where several com-mon beverages (e.g., coffee, tea, orange juice, and powdered drink mixes)mixed with drinking water were found to readily reduce Cr(VI) concentrationsof at least 8 mg Cr(VI)/ L in approximately 15 min (Chute et al., 1996; Kerger,Richter et al., 1996).
All three chromium mixtures caused temporary elevations in RBC andplasma concentrations, but the magnitude and duration of elevation showeda clear trend: Cr(VI) > Cr(III)-OJ> CrCl3. Peak concentrations for the CrCl3 andCr(VI)-only groups occurred 90min after dosing, while the peak Cr(III)-OJconcentrations occurred between 0 and 240min after dosing (Figure 7). TheCr(III)-only and Cr(VI)-OJ groups both showed temporary increases in RBC andplasma chromium levels and rapidly returned to background levels within1–2 d, an observation also seen in the 2-mg/L Cr(VI) ingestion study byPaustenbach et al. (1996). The Cr(VI)-only group showed much higher RBCand plasma chromium levels that dropped off to near-background levelswithin 1–2wk (Kerger, Paustenbach et al., 1996).
This pattern of uniform elevation and rapid drop in RBC and plasma chro-mium levels following Cr(VI) ingestion is most consistent with the behaviorexpected following systemic uptake of Cr(III)-organic liganded species (Kerger,Paustenbach et al., 1996; Kerger et al., 1997). In most volunteers, the absenceof substantial and sustained elevations in RBC chromium content in the weeksfollowing Cr(VI) ingestion suggests that Cr(VI) is probably reduced rapidly to
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
12:
38 1
2 M
arch
201
3
1312
TABL
E 4.
Urin
ary
Excr
etio
n of
Chr
omiu
m in
Eig
ht H
uman
Vol
unte
ers
Follo
win
g a
Sing
le B
olus
Dos
e (0
.5L
at 1
0m
g C
r/Lite
r) as
Pot
assiu
m D
ichr
omat
e, P
otas
sium
Dic
hrom
ate
Redu
ced
to C
r(III)
in O
rang
e Ju
ice,
or C
hrom
ic C
hlor
ide
in W
ater
Not
e:M
ean
back
grou
nd to
tal u
rinar
y ex
cret
ion
of c
hrom
ium
for t
he 8
vol
unte
ers
rang
ed fr
om 0
.3 to
1.5
µg/d
. For
no-
dete
cts,
one
-hal
f the
det
ectio
n lim
it w
asus
ed. N
o ba
ckgr
ound
adj
ustm
ents
wer
e m
ade
to p
ostd
ose
urin
ary
excr
etio
n va
lues
. Ada
pted
from
Ker
ger,
Paus
tenb
ach
et a
l. (1
996)
.
C
hrom
ic c
hlor
ide
Pota
ssiu
m d
ichr
omat
e re
duce
d in
ora
nge
juic
ePo
tass
ium
dic
hrom
ate
Volu
ntee
r
Peak
(µ
g C
r/g
crea
tinin
e)
Bioa
vaila
bilit
y (%
of d
ose
abso
rbed
; µg
Cr i
n ur
ine)
Elim
inat
ion
half-
life
(h)
Peak
(µ
g C
r/g
crea
tinin
e)
Bioa
vaila
bilit
y (%
of d
ose
abso
rbed
;µg
Cr i
n ur
ine)
Elim
inat
ion
half-
life
(h)
Peak
(µ
g C
r/g
crea
tinin
e)
Bioa
vaila
bilit
y (%
of d
ose
abso
rbed
;µg
Cr i
n ur
ine)
Elim
inat
ion
half-
life
(h)
H1
7.4
0.09
% (4
.5)
4.8
—
—
—
—
—
—
H4
11
0.24
% (1
2)
11
23
0.71
% (3
5.5)
13
29
1.
2% (5
7.5)
41
H
5 —
—
—
36
0.
82%
(41.
0)
10
585
17.5
% (8
75)
43
H6
—
—
—
18
0.57
% (2
8.5)
17
—
—
—
H
7 4.
0 0.
08%
(4.0
) 9.
6 —
—
—
—
—
—
H
8 —
—
—
18
0.
31%
(15.
5)
19
143
6.4%
(320
) 36
H
9 13
0.
09%
(4.5
) 15
—
—
—
—
—
—
H
10
—
—
—
—
—
—
77
2.4%
(120
) 37
A
vera
ge±
stan
dard
err
or8.
9±
2.0
0.13
±0.
04%
(6.3
±1.
9)
10±
2.2
24±
4.3
0.60
±0.
11%
(30.
1±
5.5)
15±
4.0
209
+12
86.
9±
3.7
(343
±18
6)
39±
1.7
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
12:
38 1
2 M
arch
201
3
RISK FROM CR(VI) IN DRINKING WATER 1313
Cr(III) prior to RBC uptake and systemic distribution. The kinetic profiles ofCr(VI) and Cr(III) in the RBC compartment are quite distinct, thereby allowingfor differentiation among chemical forms. Cr(VI) compounds (e.g., chromateanion) that enter the bloodstream are taken up by RBCs via sulfate anion chan-nels (Figure 3) (Ottenwaelder & Wiegand, 1988; Wiegand et al., 1988). Onceinside the RBC, the Cr(VI) is rapidly reduced to short-lived Cr(V) and Cr(IV)species, which bind to hemoglobin and other ligands as Cr(III) (Lewalter et al.,
FIGURE 6. Excretion of chromium in the urine of volunteers following oral ingestion of 1 L/d of watercontaining either 5 or 10 mg Cr(VI). Note difference in scale for volunteer H1 as compared to volunteer H4.Study days in which urine was not sampled are indicated by the notation NS. Adapted from Kerger et al.(1997).
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
12:
38 1
2 M
arch
201
3
1314 D. J. PAUSTENBACH ET AL.
1985; Ottenwaelder & Wiegand, 1988; Wiegand et al., 1988; Coogan et al.,1991; Miksche et al., 1994; Gray & Sterling, 1950; Weber, 1983; Edel &Sabbioni, 1985), resulting in increased total chromium levels that remain ele-vated in the RBC fraction for several weeks. At that point, measurement of
FIGURE 7. (A) Daily plasma and (B) RBC chromium concentrations in 4 volunteers ingesting bolus dose of0.5 L of 10 mg Cr(VI)-OJ/L in 2 min. Mean plasma and RBC background of all volunteers from measure-ments taken prior to dosing are represented by the dotted lines BP and BR, respectively. Adapted fromKerger et al. (1996).
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
12:
38 1
2 M
arch
201
3
RISK FROM CR(VI) IN DRINKING WATER 1315
chromium in the RBC (above background) is a good biomarker, because thebound chromium cannot escape the RBC. Conversely, the soluble inorganicforms of Cr(III) and the Cr(III) ion itself penetrate RBCs to a much lesser degreeand do not generally bind or bind in a more reversible manner to cellular con-stituents in the RBC (Gray & Sterling, 1950; Wiegand et al., 1988). Thus, Cr(III)in vivo can produce a transient increase in RBC levels and is generally rapidlyexcreted in urine.
Corbett et al. (1998) reported that Cr(VI) reduction capacity in plasma islimited in comparison to the capacity of the RBCs. Cr(VI) absorbed into thesystemic circulation at a sufficiently high rate and concentration would leadto rapid and efficient RBC uptake of chromate anion through the sulfate anionchannel, leading to long-sustained and more substantial elevation in RBC chro-mium as compared to plasma (Gray & Sterling, 1950; Weber, 1983; Wiegandet al., 1988). Our bolus-dose studies showed that even ingestion of 5mg Cr(VI)in a 2-min period on an empty stomach did not produce the RBC pattern thatwould indicate appreciable systemic uptake of chromate anion (Figure 7).When the stomach is digesting food or following consumption of liquidsincluding coffee and milk, the reductive capacity increases by orders of magni-tude, and Cr(VI) is converted to Cr(III) even more efficiently (Proctor, Hayset al., 2002).
Question III: What Is the Quantitative Reductive Capacity of Cr(VI) in Actual and Simulated Gastric Fluid? The lack of oral toxicity of Cr(VI) at the doses studied by Paustenbach et al.
(1996), Kerger, Paustenbach et al. (1996), and Finley et al. (1997) is almostcertainly due to the reductive conditions of the GI tract and other tissues. Forexample, the protective mechanisms following ingestion include the protectivemucous and epithelial layers of the upper digestive tract, the influence ofgastric juices and contents, the further reductive capacity of the deeper tissuelayers of the stomach, and an extensive backup capacity for Cr(VI) reductionoffered by blood in the system circulation and by the liver. Other pathways,such as pinocytosis or macrophage ingestion and swallowing, may also bemore important for the less soluble, particulate forms of Cr(VI) (ATSDR, 2001),but these are not the forms that are commonly involved when persons areexposed to chromium-contaminated tap water, the subject of the currentevaluation.
A number of variables that can affect absorption and elimination shouldbe evaluated when studying the effects of ingested chromium. These variablesmay include, among others, the effect of dietary status during Cr(VI) con-sumption (e.g., composition of diet, fasting vs. nonfasting), and the possibleinfluence that medication could have on stomach reduction capacity and/orpH (e.g., antacids).
To investigate a few of these potentially confounding variables, Proctor,Otani et al. (2002) studied the rate of Cr(VI) reduction under a variety of
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
12:
38 1
2 M
arch
201
3
1316 D. J. PAUSTENBACH ET AL.
simulated gastric conditions and in real human gastric juice collected fromfasting volunteers. In the first study, stomach conditions were simulated bypreparing an aqueous mixture of the primary components of gastric fluid(pepsin, mucine, gastric lipase, gastric amylase, etc.), acidifying with hydro-chloric acid, and providing continuous stirring and heating to 37°C. Thisapproach to approximating stomach conditions has been used for many yearsbut has been formalized in a number of different studies that assessed the oralbioavailability of chemicals in soils (Ruby et al., 2002). The rate of Cr(VI)reduction in simulated gastric fluid was measured at various pH values (from1.5 to 4.5). In the second study, actual human stomach juices were removedby gastric lavage. Cr(VI) concentrations (100–400 µg/L) were added to thissimulated stomach fluid following simulated ingestion of Rolaids and in thepresence of food.
In the study involving actual stomach fluid, under fasting conditions, it wasshown that 0.3 to 1 mg Cr(VI)/L was completely reduced in the first 2min ofstudy. The actual human stomach fluid was found to have a 10-fold greatercapacity to reduce Cr(VI) than the simulated stomach fluid. In the study involv-ing simulated fluid, increasing the gastric pH from 1.5 to 4.5 reduced the rateand extent of Cr(VI) reduction by approximately one-third. The presence offood substantially increased Cr(VI) reduction, with 10mg/L reduced within thefirst 4 min. The rate of Cr(VI) reduction was constant, regardless of the initialCr(VI) concentration, suggesting that these results can be extrapolated to therange of plausible concentrations of Cr(VI) in drinking water. In the simulatedconditions, antacids dramatically increased the pH of the stomach (from pH1.5 to 8.2) but had little effect on Cr(VI) reduction rate or capacity as comparedto reduction at pH 4.5. The average half-life of Cr(VI) in simulated stomachconditions is 7 min. These findings support the conclusion that ingested Cr(VI)will be reduced to Cr(III) rapidly. This view is generally consistent with thatreached by an expert panel recently convened by the State of California (Flegalet al., 2001).
Question IV: Does Reduction of Cr(VI) Occur Quickly Enough to Eliminate the Possibility of Reactive Chromium Species Binding with DNA? Research conducted by Kuykendall et al. (1996) examined the in vivo
formation of DNA-protein cross-links (DPX) in peripheral lymphocytes (assayof Zhitkovich & Costa, 1992) of humans following Cr(VI) ingestion. DPX incirculating leukocytes have been proposed as a potential biomarker for Cr(VI)exposure and other reactive chemicals, such as cisplatinum, formaldehyde,copper, and certain arsenic compounds (Costa et al., 1997). Some studiessuggest that DPX are formed by direct involvement of the chemical, such aschromate, which serves as a bridge linking the DNA and proteins (Costa,1990). Such formations may interfere with DNA replication, which may leadto a loss of genetic materials, resulting in mutagenic events (Permana &
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
12:
38 1
2 M
arch
201
3
RISK FROM CR(VI) IN DRINKING WATER 1317
Snapka, 1994). For most agents studied, DPX are only produced at chemicalconcentrations that are cytotoxic to cells in culture, producing complete celldeath (Costa et al., 1996, 1997); thus, DPX may not be a useful biomarkerof human exposure in cases when exposed cells die before DPX would beincreased.
Prior to the volunteer study, Cr(VI)-spiked cell culture experiments wereconducted using Burkitt’s lymphoma cells (BLC) to identify the acute timecourse of DPX formation and a possible threshold dose in cultured leukocytes.Findings from the in vitro study were used to design a protocol for the DPXformation in leukocytes from human volunteers who had ingested a singlebolus dose of 10mg/L Cr(VI) or Cr(III), either as K2Cr2O7 only or Cr(VI) reducedin orange juice to Cr(III), to evaluate the effect of chromium ingestion onformation of DPX in circulating leukocytes. This dosing scheme was designedto represent a worst-case scenario, in that chromium was ingested on anempty stomach, Cr(VI) concentrations were high enough to impart a brightyellow color to the water, and dosing was rapid and considered representativeof ingestion by a very thirsty person.
Blood samples were collected prior to dosing to establish backgroundDPX concentrations in the volunteers’ leukocytes, and at four hourly intervals(0, 60, 120, 180, and 240 min) following dosing for analysis of DPX forma-tion, and results were compared to each volunteer’s own DPX backgroundconcentrations. Blood and urine samples were also collected for up to 2 wkfollowing the dose to further examine the pattern of uptake and excretion ofchromium.
Kuykendall et al. (1996) reported that in vitro concentrations of high dosesof Cr(VI) added directly to a culture medium of BLC indicated an apparentthreshold for DPX induction of approximately 26 to 52 µg/L. A significant,dose-dependent increase of DPX in BLC was observed within 3 to 4h forCr(VI), whereas concentrations of Cr(III) up to 1300 µg/L failed to cause anincrease in DPX. Other studies have shown no in vivo genotoxic responses inrodents at doses up to 20mg/L (Mirsalis et al., 1996).
Results of the KuyKendall et al. volunteer study showed that ingestion of10mg/L Cr(VI) or Cr(III) on a relatively empty stomach failed to induce anymeasurable change in DPX in vivo, even though blood and urine chromiummeasurements indicated systemic uptake of a substantial fraction of theingested chromium (up to 18% based on urine measurements). These resultsare not surprising, because DPX formation has not been found to occur afteroral ingestion of Cr(VI), even at high doses (100–200mg/L), in animals(e.g., Coogan et al., 1991). This suggests that the amount of Cr(VI) absorbedwas not sufficient to produce DPX. These results may also indicate that Cr(VI)was reduced to Cr(III) intragastrically prior to absorption. The pharmacokineticprofile of the absorbed chromium in blood and urine of the volunteersindicates that reduction of Cr(VI) occurred primarily in the stomach, smallintestine, blood, and liver followed by systemic uptake, distribution, andexcretion as Cr(III).
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
12:
38 1
2 M
arch
201
3
1318 D. J. PAUSTENBACH ET AL.
Question V: How Well Do Physiologically Based Models for Ingestion of Cr(III) and Cr(VI) Characterize Kinetics in Humans?To further study the differential absorption and excretion of Cr(VI) and
Cr(III), and reduction of Cr(VI) in body fluids and tissues, blood and urine datafrom the previously described chromium ingestion studies of Kerger, Paustenbachet al. (1996), Paustenbach et al. (1996), and Finley et al. (1997) were comparedto results from a physiologically based pharmacokinetic (PB-PK) model. A PB-PKmodel was designed to model human chromium kinetics (O’Flaherty et al., 2001)based on an existing model of chromium kinetics in rats (O’Flaherty, 1996).Key features of the chromium-specific PB-PK model include differential absorp-tion of Cr(VI) and Cr(III), reduction of Cr(VI) to Cr(III) in body fluids and tissues,modest incorporation of chromium into bone, and concentration-dependenturinary clearance.
Results of the ingestion studies indicated differential absorption and excretionbehaviors for the two forms of chromium, presumably due to the degree ofreduction in the GI tract; thus, the fractional absorption of Cr(VI) was a keyvariable in the PB-PK model. After optimizing the absorption rate constants inthe model, the fraction of orally ingested chromium that was absorbed basedon urinary data varied from 0.7% to 4% (mean of 1.7%) and, based on blooddata, ranged from 3.9% to 12%. The PB-PK model adequately reproduced thetime-dependent kinetic profiles of blood plasma concentrations and rates ofurinary chromium excretion in both the single-dose and repeated oral expos-ure studies (Figure 8). Similar patterns were observed in the human volunteerstudies at Cr(VI) water concentrations up to 2mg/L and daily doses up to 4mg/d.For chronic chromium exposure in drinking water, the PB-PK model indicateda urinary clearance of 1–2L/d, and GI absorption rate constants of 0.25/d forCr(III) and 2.5/d for Cr(VI) were suitable estimates for the general population.Using these parameters, results of the PB-PK model, coupled with the humanvolunteer studies, show that Cr(VI) ingested in tap water at concentrations atleast as high as 2 mg/L are rapidly reduced to Cr(III).
STUDIES TO ASSESS INHALATION RISKS ASSOCIATED WITH CR(VI)-CONTAMINATED TAP WATER
Inhalation exposure to Cr(VI) in tap water can occur during use of anyhousehold appliance that emits aerosols, primarily showers. Vapors are not aconcern because Cr(VI) is nonvolatile under ambient conditions. It has alsobeen suggested that use of a “swamp cooler” (i.e., an evaporative blower usedto cool homes in the desert) may produce increased airborne concentrationsof Cr(VI). Because little was known regarding the dynamics of exposure toCr(VI) in household air from Cr(VI) in tap water, simulation studies wereconducted to evaluate inhalation risks from both swamp coolers and showeringwith Cr(VI)-contaminated water.
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
12:
38 1
2 M
arch
201
3
RISK FROM CR(VI) IN DRINKING WATER 1319
FIGURE 8. Observed and simulated rates of chromium excretion in (A) urine, (B) plasma, and (C) RBC afteringestion of Cr(VI) in water, using data from Kerger, Paustenbach et al. (1996). The simulation was cali-brated to the data by simultaneously optimizing the fits to observed plasma concentrations and urinaryexcretion rates by adjusting the value of the absorption rate constant for Cr(VI) while maintaining theabsorption rate constant for Cr(III) at 0.25/d. Adapted from O’Flaherty et al. (2001).
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
12:
38 1
2 M
arch
201
3
1320 D. J. PAUSTENBACH ET AL.
Question I: What Concentrations of Cr(VI) Can be Inhaled from Swamp Coolers?To assess the range of indoor airborne chromium concentrations that can
plausibly be associated with the use of Cr(VI)-containing tap water, exposuresimulation studies were conducted to measure indoor aerosols resulting fromshowering activities and operation of swamp coolers. A swamp cooler relies onthe evaporation of water to cool the air passing through a wetted batting (Figure 9).An electric pump circulates water through the unit’s distribution system, anda fan acts to “pull” warm outdoor air through the unit, whereupon the influent
FIGURE 9. Schematic diagram of an evaporative cooler. From Finley et al. (1996).
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
12:
38 1
2 M
arch
201
3
RISK FROM CR(VI) IN DRINKING WATER 1321
air is cooled by evaporation and is then distributed through ductwork andvents in the house.
The simulation studies by Finley et al. (1996) were conducted in an actualthree-bedroom home, with air sampling conducted using the triple-impingersampling method adopted by the American Society for Testing and Materials(ASTM) Method D 5281 (Sheehan et al., 1992; Finley et al., 1993; Finley &Mayhall, 1994). A complete description of these tests is offered elsewhere(Sheehan et al., 1992). Six air samples were collected during each of four trials,during which the evaporative cooler operated at full cooling capacity. In alltrials, indoor samplers were placed at breathing-zone height in the living roomand bedrooms. Outdoor (background) samples were taken on the roof, 3mfrom the evaporative cooler intake, and 3m from the front door.
The results showed that there were no differences between outdoor andindoor airborne Cr(VI) concentrations as a result of operating a central swampcooler with cooler influent Cr(VI) water concentrations of 20mg/L measuredover a 24-h period of use. From these data, it was concluded that swamp coolerscould not contribute a significant amount of aerosols to indoor air. Interest-ingly, the concentrations of airborne Cr(VI) in the home (0.3–2.7ng/m3) wereequal to or less than the outdoor concentrations (<0.01–2.0ng/m3). In one trial,background concentrations measured <0.1ng/m3; however, this measurementwas taken immediately after local rainfall, indicating that lower outdoor airconcentrations may have been observed due to the temporary washing out ofairborne particles. Indoor air concentrations averaged 0.18ng/m3 lower thanthe concurrent outdoor levels, and there was no statistical difference betweenthe two, indicating that the evaporative cooler was not a source of airborneCr(VI) in indoor air. This result was observed even when the reservoir water inthe cooler accumulated Cr(VI) up to 200mg/L (due to evaporation), whichturned the water bright yellow.
Question II: What Concentrations of Cr(VI) Can Be Inhaled from Showering? To understand the inhalation hazard, it should be recognized that chro-
mium is not volatile; therefore, the possible hazard is associated with airborneCr(VI) aerosols (as mists, rather than vapors) during showering or use of a dish-washer. Showering would produce greater exposure than using a dishwasher,so showering exposure simulation studies were conducted.
To assess the inhalation exposure of Cr(VI) during showering, a standardshower/bathtub stall was outfitted with a mannequin, simulating an adultstanding in the shower (Finley et al., 1996). Two ASTM sampling trains wereinstalled on either side at breathing-zone height (Figure 10). The shower wasconnected to a pump that allowed for one of three different Cr(VI) waterconcentrations (1, 5, or 10 mg/L) to be sprayed from a high-flow (5.9L/min)shower head and then recirculated for 24 h (per ASTM method). Theseconcentrations were target values; actual measurements of Cr(VI) water con-centrations were 0.89, 5.4, and 11.5mg/L.
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
12:
38 1
2 M
arch
201
3
1322 D. J. PAUSTENBACH ET AL.
The water concentration of Cr(VI) versus the airborne concentration wasmeasured during showering (Figure 11). Results show a linear relationshipbetween Cr(VI) concentrations in the shower water and the shower aerosols(least squares regression of y = 26.6x, with a 95% CI of 19.2 to 33.3 for the
FIGURE 10. Schematic of shower-air sampling experiment. From Finley et al. (1996).
FIGURE 11. A comparison of the airborne concentrations of Cr(VI) in mists during showering at variouscontaminated water concentrations.
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
12:
38 1
2 M
arch
201
3
RISK FROM CR(VI) IN DRINKING WATER 1323
slope). Average airborne concentrations of Cr(VI) aerosols at breathing-zoneheight ranged from 39 to 358ng/m3 when the water concentration of Cr(VI)varied from 0.89 to 11.5 mg/L. The results indicated that elevated concentra-tions of Cr(VI) in shower water create a concentration of mists of watercontaining Cr(VI) that exceed background air levels of Cr(VI) (approximately1–2ng/m3 [Finley et al., 1996]).
Using these results, the mass of water aerosols dispersed into the showerair was measured. For a Cr(VI) concentration in the water during showering1mg/L the associated airborne concentration would be 26.6 ng/m3 for a totaluptake of approximately 5–10ng of Cr(VI) per shower event is expected(assuming that 0.1–0.2m3 is inhaled during a long [>10min] shower). Theselow-nanogram quantities of inhaled Cr(VI) are not expected to exceed thereductive capacity of the mucous lining, macrophage cells, and tissue of thelungs (De Flora et al., 1997; De Flora, 2000).
Finley et al. (1996) calculated the lifetime average daily doses (LADDs) ofCr(VI) due to showering and compared them to background concentrations ofCr(VI) measured in outdoor air (assuming that a home is supplied with watercontaining either 2 or 10mg/L Cr(VI) for 30yr, and a resident takes one 10-minshower or bath per day) (see Table 5). The plausible upper-bound lifetimecancer risk associated with continuous exposure to background Cr(VI) in out-door air was estimated at 1.6 × 10−7 for a person exposed from birth to age 30,and 9.5×10−8 for ages 30–60. At a plausible maximum tap water concentrationof 2 mg/L Cr(VI), the risks attributable to shower aerosol exposures were one-fourth to one-seventh of those corresponding to background air concentrationsof Cr(VI) (about 1ng/m3), ranging from 2.1 × 10−8 to 1.1 × 10−7 for the child/adult scenario, and from 2.6 × 10−8 to 1.3 × 10−7 for the adult-only scenario Inshort, showering activities resulted in some inhalation of aerosols or mistscontaining Cr(VI); however, even when shower water contained up to 10 mg/LCr(VI), the theoretical incremental lifetime dose due to typical shower and
TABLE 5. Lifetime Average Daily Dose and Estimated Upper-Bound Lifetime Cancer Risks from ScenariosInvolving Inhalation of Cr(VI)
Note: Adapted from Finley et al. (1996). a See Results section in text for calculations.
Scenario Lifetime average daily dose (mg/kg-d)a
Lifetime cancer risk (per million)a
30 yr exposure to outdoor air (average of all outdoor measurements)
bath use over a 30-yr period would be similar to that associated with 30yr ofcontinuous exposure to background airborne Cr(VI) concentrations. Finley et al.(1996) concluded that exposure to indoor aerosols from water containingCr(VI) does not create a meaningful health hazard at concentrations up to10mg/L, an unlikely scenario for chronic, unrecognized contamination of water.
STUDIES TO ASSESS UPTAKE OF Cr(VI) THROUGH SKIN
Dermal contact with tap water in the home can occur during a variety ofactivities, including, among others, showering, bathing, and swimming. Thepatch-testing technique is most often used to identify concentrations of Cr(VI)and Cr(III) that produce allergic responses in sensitized individuals. Histori-cally, in these kinds of tests, the diagnostic patches contain relatively highCr(VI) concentrations, well above those expected to occur in the environment(Paustenbach et al., 1992). For example, in a study by Nethercott et al. (1994),responses were seen at concentrations of 4.4 µg Cr(VI)/cm2, a concentrationunlikely to be found in the environment. Using lower concentrations (rangingfrom 0.018 to 0.88 µg/cm2), a minimum elicitation threshold of 0.089 µg/cm2
was established for Cr(VI). The result of this study is consistent with the factthat, like most charged metals, Cr(VI) is not expected to penetrate intact skin toa significant degree and would therefore be unlikely to contribute substantially toan absorbed chromium dose in a residential exposure scenario. However, todetermine whether extended dermal contact with highly contaminated waterwould (1) elicit ACD in Cr(VI)-sensitized individuals or (2) result in measurablechromium absorption, a human exposure simulation study was conducted.
Question I: Is Dermal Absorption of Cr(VI) from Bathing Activities Significant? A study was conducted by Corbett et al. (1997) in which volunteers spent
3h immersed in a 450-gal heated (91 ± 2°F) bath containing 22mg/L Cr(VI) (asK2Cr2O7) to quantitatively evaluate the systemic uptake of chromium followingprolonged dermal contact. Chromium uptake and elimination were evaluatedin four adult males (ages 20 to 44yr) following patch testing to determinewhether the volunteers had been previously sensitized to chromium; none ofthe volunteers exhibited a reaction to the patch test. Blood samples were col-lected on the day prior to exposure, within 1 h after the single 3-h bathingevent (d 1), and on d 2 and 4. Every urine void was collected starting on theday prior and through d 5. Both blood and urine samples were analyzed usingmethods similar to those described for the ingestion studies. The dermaluptake rate (µg Cr/cm2 skin-h) was defined as the total amount of chromiumexcreted above daily historical background levels for each volunteer (taken asthe sum of the µg Cr/d excreted in urine for each volunteer, less his historicalbackground excretion) divided by the estimated exposed surface area for eachvolunteer (cm2) and the duration of exposure (3h):
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
12:
38 1
2 M
arch
201
3
RISK FROM CR(VI) IN DRINKING WATER 1325
A comparison value for dermal Cr(VI) uptake was also calculated using theU.S. EPA guidance for dermal exposure assessment (U.S. EPA, 1992).
The average and range of background urinary concentrations and systemicuptake of total chromium reported by Corbett et al. (1997) for each volunteerare presented in Table 6. The calculated uptake rates for total chromiumbased on 5-d urinary excretion were all very low, averaging approximately1.5 × 10−4 µg/cm2-h, demonstrating an average dermal uptake rate about4 orders of magnitude below the 1.0 µg/cm2-h rate calculated by the U.S. EPA(1992) based on the Baranowska-Dutkiewicz (1981) study. When expressed astotal daily excretion of chromium in the urine (µg/d for each volunteer), itappears that all volunteers may have excreted a small incremental amount ofchromium within 1–2d after the bathing event. In general, volunteers excretedchromium at daily levels within their own historical background excretion range.One volunteer (H1) exhibited a dermal uptake rate sevenfold higher than theaverage for the other volunteers; however, this is consistent with this individ-ual’s specific trends of higher background urinary and blood measurements ofchromium and his higher uptake and excretion of total chromium in the oralCr(VI) exposure studies (Kerger et al., 1997; Finley et al., 1997).
For the RBC and plasma data reported by Corbett et al. (1997), transientincreases in total chromium concentrations were observed during and imme-diately following the exposure for all volunteers. The observed changes in RBCor plasma chromium were not sustained in any of the volunteers, indicatingthat the limited uptake of chromium was likely in the form of Cr(III)-organicliganded species, not as Cr(VI). Because absorption of Cr(VI) would result inthe irreversible binding of Cr(VI) to hemoglobin within the RBC, the pattern ofblood uptake and urinary excretion observed was consistent with Cr(III) uptakeand distribution.
The Corbett et al. (1997) study suggests that the apparent rate of systemicuptake of chromium due to dermal contact with highly soluble Cr(VI) rangesfrom 3.5 × 10−5 to 4.1 × 10−4 µg Cr/cm2-h. A 3-h dermal exposure to Cr(VI)showed no measurable systemic uptake of the hexavalent species, based onthe premise that RBC chromium concentrations would remain elevated abovehistorical background levels (postexposure) if appreciable systemic uptake ofCr(VI) had occurred (Lewalter et al., 1985).
For comparison purposes, Corbett et al. (1997) calculated the total doseabsorbed using the U.S. EPA guidance for dermal exposure, which is based onthe gross dermal penetration rate (1.0 µg Cr/cm2-h) reported by Baranowska-Dutkiewicz (1981). The discrepancy between the two values is likely attribut-able to several factors discussed by Corbett et al. (1997). For example, theBaranowska-Dutkiewicz (1981) study involved a crude determination of Cr(VI)absorption on the forearm skin of volunteers using a 500 mg/L solution
Dermal uptake ratetotal urinary chromium output
surface area exposed exposure period×----------------------------------------------------------------------------------------------------=
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
12:
38 1
2 M
arch
201
3
1326
TABL
E 6.
Estim
ated
Sys
tem
ic U
ptak
e Ra
te o
f Chr
omiu
m F
ollo
win
g 3
h of
Der
mal
Exp
osur
e to
22
mg
Cr(V
I)/ L
in H
uman
s
Not
e:A
dapt
ed fr
om C
orbe
tt et
al.
(199
7).
aEx
pose
d su
rface
are
a 64
% o
f to
tal b
ody
surfa
ce a
rea
(legs
=36
%,
3/4
trunk
=28
%)
base
d on
nom
ogra
m u
sing
wei
ght
and
heig
ht t
o de
term
ine
surfa
ce a
rea
(ICRP
, 198
4).
bD
etec
tion
limit
0.5
µg/L
. cD
erm
al u
ptak
e ra
te is
equ
al to
the
5-d
tota
l Cr e
xcre
ted
in u
rine
divi
ded
by th
e su
rface
are
a ex
pose
d an
d th
e le
ngth
of e
xpos
ure
for e
ach
volu
ntee
r. dTo
tal C
r exc
rete
d fo
r d 1
–5, l
ess
the
aver
age
hist
oric
al b
ackg
roun
d le
vel f
or e
ach
volu
ntee
r. eD
A eve
nt =
Cw
× k
p ×
t even
t; D
Ato
tal =
DA
even
t × su
rface
are
a (U
.S. E
PA, 1
992)
.
Subj
ect n
umbe
r
Expo
sed
surfa
ce a
reaa
(cm
2 )
Hist
oric
al
back
grou
ndb
(µg/
d)
Estim
ated
syst
emic
up
take
rate
at
22m
g/La,
c
Tota
l Cr e
xcre
tion
abov
e hi
stor
ical
ba
ckgr
ound
d (µg)
Tota
l dos
e ab
sorb
ed
usin
g U
.S. E
PA m
etho
de (µ
g)
H1
14,3
36
1.5
(0.2
5–2.
6)4.
1E−
04
17.5
19
87
H4
13,9
52
0.5
(0.3
–1.4
)3.
3E−
05
1.4
1934
H
5 13
,312
0.
6 (0
.2–0
.93)
7.5E
−05
3.
0 18
45
H7
11,3
92
1.0
(0.2
5–1.
7)7.
0E−
05
2.4
1579
A
vera
ge fo
r all
subj
ects
13,3
83
0.9
(0.2
5–2.
6)1.
5E−
04
6.1
1855
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
12:
38 1
2 M
arch
201
3
RISK FROM CR(VI) IN DRINKING WATER 1327
occluded under a watchglass and quantified by attempting to recover residualCr(VI). This study design gives little insight on the actual penetration rate ofchromium and provides no information on systemic dose or the valency ofchromium species that might reach the vascular zone of the dermis. Usingconservative assumptions regarding the skin surface area exposed, Corbettet al. (1997) calculated using the U.S. EPA model (assumed uptake rate =1.0µgCr/cm2-h) that the model overstated the absorbed dose of total chromium byabout 110- to 1400-fold for the study volunteers.
Question II: What Is the Potential for Elicitation of ACD Resulting from Contact with Cr(VI) in Standing Water? It is difficult to use the work of Nethercott et al. (1994) or other patch test
data to identify concentrations of Cr(VI) in surface water that could pose an ACDhazard. Thus, to evaluate the potential for elicitation of ACD from contact withstanding water in the environment, 26 persons known to be allergic to Cr(VI)were exposed to 25–29mg/L Cr(VI) by immersion of one arm for 30min per dayon 3 consecutive days in a potassium dichromate bath (Fowler et al., 1999).The 26 volunteers were selected from the group of 54 persons who had partic-ipated in the Nethercott et al. (1994) patch test study. Each volunteer waschallenged with Cr(VI) by immersion of their entire forearm, wrist, lower partof hand, elbows, and part of their upper arm in a K2Cr2O7 bath. Graded mor-phological descriptors that are typical of contact eczema (e.g., papules, vesicu-lation, scaling, erythema) were used to evaluate responses, since developmentof these descriptors related to an inflammatory response could represent anallergic or irritant process. Subjective data (itching or tingling) and histopatho-logical analysis of biopsied vesicles were also used to evaluate responses.
Results of the study indicated that, in round 1, 14 of the 26 study participantshad no response of any kind to the Cr(VI) challenge during the observationperiod up to 96 h postdosing. Four of these volunteers displayed or reportedsome subjective or observable morphological response; however, these responseswere determined by the physicians to be insignificant or inconsistent with ACD.In all cases, the responses had either resolved or were substantially resolvingby 6d after the initial exposure. The participants who were further evaluatedin round 2 exhibited a response that appeared to be inflammation of the sweatducts, as supported by results from histopathological examination.
The morphological and histopathological findings do not describe eczematousdermatitis (either ACD or irritant contact dermatitis) and were instead categorizedas acute eccrine contact inflammation (Fowler et al. 1999). Irritant responsessimilar to those observed here have been reported from exposure to dish deter-gent, heat-composed polyethylene film, and even water (Grammer-West et al.,1996; Thestrup-Pedersen et al., 1989; Kligman, 1996). Under the exposureconditions evaluated in this study, a concentration up to 29mg/L Cr(VI) in water isnot expected to elicit ACD in Cr(VI)-sensitized individuals. It was thereforeconcluded that exposure to similar concentrations of Cr(VI) in the environmentdoes not pose an ACD hazard, even to chromium-sensitized persons.
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
12:
38 1
2 M
arch
201
3
1328 D. J. PAUSTENBACH ET AL.
DISCUSSION
Recent improvements in analytical chemistry now make it possible tomeasure concentrations of Cr(VI) in groundwater at least as low as 0.1 µg/L.This capability produced some level of public concern in southern Californiain 2000 and 2001 when Cr(VI) was detected in many drinking water supplies(Creasy & Flegal, 1999; Blankstein, 2001; Frzek et al., 2001). These data werereleased about a year or two after the movie Erin Brockovich—which describeda California community allegedly exposed to Cr(VI) in groundwater—was quitepopular. At the same time, the California EPA published its public health goal(PHG) for chromium in drinking water, which suggested that a cancer riskmight be associated with the ingestion of Cr(VI) in tap water and recom-mended that concentrations not exceed 2 µg/L of total chromium (DHS,2002). In contrast, the U.S. EPA was embracing its water standard, the MCL of100 µg/L of total chromium. Not surprisingly, the public was concerned aboutthe risks posed by any concentration of Cr(VI) found in some water supplies.
This issue attracted the attention of the California legislature (Creasy &Flegal, 1999; Blankstein, 2001; Frzek et al., 2001), which considered severaldifferent actions. One of the proposals would have required that all drinkingwater suppliers in California install remedial technologies on wells to ensurethat Cr(VI) would not be present at measurable levels in tap water. The associatedcost of installing this kind of remedial technology in California was estimatedto be tens of millions of dollars per year. The legislature and governor wantedother approaches to also be considered to resolve this issue.
Risk assessment methodologies are generally considered the best scientificapproach to inform decision-makers about how to address these kinds ofcomplex public health issues. However, quite often, complete exposure ortoxicology data, which are directly applicable to characterizing the risks associ-ated with specific exposure scenarios, are not available. In these situations, it isnecessary to assemble all that is known about the toxicology of the agent viaeach route of entry, collect relevant exposure information, and identify datagaps and sources of uncertainty. If the uncertainty can be reduced and datagaps can be filled through additional toxicology studies, epidemiology studies,or exposure studies (including modeling or dose reconstruction), then thesestudies should be conducted if the magnitude of the concern or possible riskswarrants the effort. Although much has been written over the years aboutCr(VI), the body of data available in the mid 1990s was probably not sufficientto address all of the questions likely to have been raised by courts or publichealth officials faced with questions about chromium-contaminated ground-water. Thus, the series of studies described in this article were conducted in anattempt to reduce uncertainties about the strength of the available scientificinformation regarding the acute or chronic (e.g., carcinogenic) hazard posedby drinking water containing Cr(VI) concentrations of up to 10mg/L.
When conducting a risk assessment, three major components serve as theunderpinnings of the risk characterization: hazard identification, dose-response
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
12:
38 1
2 M
arch
201
3
RISK FROM CR(VI) IN DRINKING WATER 1329
assessment, and exposure assessment. When assessing chromium in tap water,each component deserves special attention due to the unique behavior of thechemical. Fortunately, quite a number of relevant studies have been con-ducted over the years that provide a sound basis for assessing this hazard. Theadditional studies described in this article provide supplemental support tothe historical analyses, and in the aggregate they indicate that plausible con-centrations of chromium (less than 2 to 4mg/L) in drinking water should notpose a human health risk.
Hazard Identification When assessing the cancer hazard posed by a chemical, it is useful to
support the conclusions of epidemiology studies with biological or mechanisticdata from animal or human studies (Hathaway, 1989; U.S. EPA, 2003). Withinthe scientific community, it has generally been accepted that Cr(VI) in drinkingwater was unlikely to pose a cancer hazard in humans following chronic expos-ure at any reasonable dose. The belief that the risk associated with ingestingwaterborne Cr(VI) in drinking water is negligible was supported by indirectevidence from in vivo animal studies, where the ingestion of various concen-trations of Cr(VI) failed to induce adverse effects. For example, Mirsalis et al.(1996) evaluated the hazard following ad libitum and bolus administration ofdrinking water containing Cr(VI) (as K2Cr2O7) concentrations of 1, 5, and20mg/L. They found that the ingestion of drinking water failed to inducepositive genotoxicity findings in the in vivo–in vitro rat hepatocyte unscheduledDNA synthesis test or the mouse bone marrow micronucleus test, two standardgenotoxicity assays.
Numerous studies have shown that Cr(VI) is reduced to Cr(III) in the presenceof organic material, acidic pH and other reducing conditions, and acidic gastricfluids present in the GI tract, and that these conditions create a substantialbarrier to distribution of Cr(VI) to other organs. Dosimetry is a key issue,because at some dose, the route-specific barriers and reducing capacity of thebody could be overwhelmed, despite the often multiple and overlapping orredundant protective mechanisms involved (e.g., Figure 2). The reductivecapacity of the GI tract was cited in the U.S. EPA decision to raise the chromiumdrinking water standard (MCL) from 50 to 100 µg/L (U.S. EPA, 1991). Theresults of the ingestion studies described herein indicate that the human GItract can rapidly reduce ingested Cr(VI) to Cr(III) at water concentrations up to10mg/L. This is consistent with observations of others (De Flora et al., 1997;De Flora & Wetterhahn, 1989; De Flora, 2000). Proctor, Otani et al. (2002)recently validated the reduction of Cr(VI) by evaluating human gastric juice. Inaddition, a comprehensive review of the toxicology and epidemiology ofCr(VI) in drinking water was published recently (Proctor, Hays et al., 2002) andthese authors concluded that the published literature clearly showed that noincreased risk of cancer would be expected from ingestion of Cr(VI) at currentdrinking water standards. This same view was reached by a panel of expertsconvened by the State of California (Flegal et al., 2001).
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
12:
38 1
2 M
arch
201
3
1330 D. J. PAUSTENBACH ET AL.
Other organs or tissues that have high reductive capacities include theblood and liver. Specifically, blood proteins, amino acids, antioxidants likeglutathione and ascorbate, and other agents present in blood have the capa-city to reduce relatively large quantities of Cr(VI) (Capellmann & Bolt, 1992;Ottenwaelder & Wiegand, 1988; Wiegand et al., 1988). The high capacity ofRBCs to rapidly sequester and bind Cr(VI) has been recognized for several dec-ades, and radiolabeled Cr(VI) has actually been used as a biomarker to studythe lifespan of RBCs in humans (Gray & Sterling, 1950). RBC chromium contenthas also been used to characterize occupational Cr(VI) exposures (Lewalteret al., 1985; Korallus, 1986; Miksche et al., 1994).
Dose-Response Assessment Studies in animals or humans are typically the basis for the dose-response
assessment. For a cancer dose-response analysis to be conducted, there needsto be an increase in the cancer incidence rate in the treatment groups orexposed human cohort versus controls. To date, there has only been one animalstudy wherein lifetime exposure to Cr(VI)-contaminated drinking water wasevaluated (Borneff et al., 1968). This study had so many flaws that it has generallybeen considered an inappropriate basis upon which to predict the human cancerrisk (Flegal et al., 2001). For the sake of completeness, however, it should benoted that the California OEHHA derived a cancer potency factor of 0.19 mg/kg-d based on that study. Due to the flaws in that analysis, OEHHA withdrewthat recommendation in 2001 (Bureau of National Affairs [BNA], 2001).
Most risk assessments of Cr(VI) rely on the U.S. EPA reference dose (RfD).The current RfD is 3 × 10−3 mg/kg-d and is based on a 1-y drinking water studyin rats conducted by MacKenzie et al. (1958) (IRIS, 2002). The confidence inthe RfD is relatively low, however, because of the small number of animalstested, the small number of parameters measured, and the lack of toxic effectat the highest dose tested (IRIS, 2002). In addition, an uncertainty factor (UF)of 300 representing two 10-fold decreases in dose to account for both theexpected interhuman and interspecies variability in the toxicity of the chemicalin lieu of specific data and an additional factor of 3 to compensate for theless-than-lifetime exposure duration of the principal study are incorporatedinto the oral RfD. Finally, a modifying factor of 3 was incorporated to accountfor inadequecies of the toxicological database for a total safety factor of 1000.These adjustment factors are unusually high given the available information. Itis acknowledged that UFs are commonly used in risk assessments to ensureadequate protection to the population of interest.
One could also use a PB-PK approach to reduce some of the uncertaintyassociated with assessing the risks associated with ingesting Cr(VI). A PB-PKapproach has the capacity to quantitatively account for the reduction of Cr(VI)by various tissues at various doses. For example, the published information onthe chemistry of Cr(VI) and data on the reduction kinetics observed in animalsor humans was recently assembled and accounted for in a robust and com-prehensive model (O’Flaherty et al., 2001). Their model showed that, at
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
12:
38 1
2 M
arch
201
3
RISK FROM CR(VI) IN DRINKING WATER 1331
concentrations perhaps as great as 10mg/L, one would not expect Cr(VI) to bepresent in the blood delivered to target organs—for example, the kidneys—due to the reduction that occurs in the stomach, intestines, and blood.
When predicting the possible risk associated with exposure via inhalationof Cr(VI), most assessments rely on the reference concentration (RfC) andcancer potency factor. The current RfC for chromic acid mists and dissolvedCr(VI) aerosols is 8 × 10−6 mg/m3 and it is based on a human subchronic occu-pational study conducted by Lindberg and Hedenstierna (1983) (IRIS, 2002).As with the RfD, the confidence in the inhalation RfC (due to shortcomings inthis study) is low because of uncertainties regarding the exposure characterizationand the role of direct contact. It is noteworthy that the cancer potency factor(as air unit risk) is 1.2 × 10−2 µg/m3 based on a human lung cancer study byMancuso (1975). However, the cancer mortality in the Mancuso study (1975)was assumed to be due to Cr(VI) rather than other airborne toxicants or smoking,which was further assumed to be no less than one-seventh of total chromium(IRIS, 2002). Over the next few years, it is expected that the inhalation cancerpotency factor will be reevaluated based on the studies of workers conductedby Gibb et al. (2000) and Crump et al. (2003).
Exposure Assessment For Cr(VI) in tap water, it is not difficult to quantitatively characterize
the universe of plausible water concentrations and the quantity of Cr(VI) thatenters humans via ingestion, inhalation, and dermal contact. Many factorsneed to be considered to characterize the magnitude of exposure (Table 1) butthe task is manageable. In general, annual average and peak doses can beestimated as a function of measured or modeled historical groundwater con-centrations. Exposure scenarios should be evaluated in accordance with eachindividual’s stated frequency of exposure (e.g., number of showers per day orweek, or minutes per day in the shower). LADDs and corresponding cancerrisks can be calculated for each person who might have been exposed, andaverage and maximum daily doses can be estimated to characterize the non-cancer hazard.
When conducting a dose reconstruction for an individual or a community,the timing of residence and/or working in the affected area should be con-sidered for each person, using estimated age-specific intakes and body weights.Plausible exposure assumptions should be used to realistically predict humanexposure. For example, water concentrations that exceed 1 to 2mg/L Cr(VI),the concentration that results in observable yellow water, thus would not beplausible for most environmental situations involving routine exposure to tapwater in the United States. The quantity of tap water ingested should be basedon data collected from interviews or from national surveys reporting age-,region-, and gender-specific data on tap water ingestion (Pennington, 1983;Ershow & Cantor, 1989). In some hot and dry climates, a desert modifyingfactor can be included to increase the daily water dose for field workers basedon consumption data (Adolph, 1969).
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
12:
38 1
2 M
arch
201
3
1332 D. J. PAUSTENBACH ET AL.
Risk Characterization Several analyses have been conducted to assess the potential oral carcino-
genicity of Cr(VI) using human data from exposed populations (e.g., U.S. EPA1998; OEHHA, 1999; Proctor, Otani et al., 2002). Animal data are also avail-able to help understand the carcinogenicity of Cr(VI) (e.g., Borneff et al., 1968;MacKenzie et al., 1958). The preponderance of epidemiological studies ofresidential populations exposed to Cr(VI) in drinking water suggest that Cr(VI)does not pose a carcinogenic risk via the oral pathway, because none of thesestudies found a correlation between Cr(VI) exposure and cancer at any site. Allof these epidemiological studies, however, suffer from methodological weak-nesses to varying degrees, and it cannot be concluded that they offer strongevidence that Cr(VI) does not pose a cancer risk from oral exposure at somedose, although at reasonable doses, this is highly unlikely. The animal data arenot definitive because most studies looked at effects following less than lifetimeexposures and evaluated an incomplete set of possible endpoints (Proctor,Hays et al., 2002). A comprehensive review of the historical epidemiologicalstudies regarding the carcinogenicity of Cr(VI) via ingestion indicates that Cr(VI)is not carcinogenic in humans via the oral route of exposure at permissabledrinking water standards (Proctor, Otani et al., 2002).
Some additional uncertainty involves the importance of varying stomachpH (particularly as influenced by increasing alkaline pH and the reductioncapacity of the gastric environment) and presence or absence of food duringingestion. The available information is that, even for those who eat antacids orwho ingest chromium on an empty stomach and probably have a less efficientreduction capacity than a normal stomach, the available studies indicate thatthis will have minimal impact on the health risk. Since most risk assessmentsrespond to uncertainty by adopting “worst-case” scenarios, this uncertainty isin part reflected in the ultimate estimate of exposure and potential health risk.
Particular concerns have been raised about two potential susceptiblepopulations with regard to Cr(VI) in drinking water: infants and adults whodo not secrete normal amounts of stomach acid, or who use antacids exten-sively. With regard to the risk to infants, the concern is based on their having astomach pH too alkaline to cause reduction of ingested Cr(VI) to Cr(III). Thescientific literature, however, suggests that the secretion of acid in the stomachof infants starts very early in life, achieving a stomach pH of 3 within approxi-mately 24h of birth (Avery et al., 1966), indicating that normal infants prob-ably should not be viewed as a particularly susceptible population. Whileeating a meal transiently raises the pH of the stomach, the resulting elevationin pH generally persists for only a few hours in children (Nagita et al., 1996) oradults (De Flora et al., 1987). However, the presence of food in the stomachslows transit to the small intestine and greatly increases the reductive capacity ofthe stomach and increases the stomach capacity to reduce Cr(VI) to Cr(III). As faras adults taking antacids to neutralize “excess” stomach acid, the effects ofantacids are transient. Proctor, Hays et al. (2002) found no difference in the
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
12:
38 1
2 M
arch
201
3
RISK FROM CR(VI) IN DRINKING WATER 1333
reduction rate at pH 8 and pH 4.5. Thus, we may conclude that ingestedCr(VI) will likely pose little (if any) risk to the most susceptible population iden-tified. This is consistent with the conclusions reached by an expert panelrecently convened by the State of California (Flegal et al., 2001).
Based on results of the human volunteer exposure simulation studiespresented herein, the questions of the possible uncertainty noted earlier hasbeen greatly reduced and potentially eliminated. Since simulation studiesre-create actual exposure conditions, results of human ingestion studies aremore representative of actual risks to persons ingesting Cr(VI) in tap water thantypical animal studies. By altering the pH of both simulated (via chemical addition)and actual (via addition of antacids) gastric fluid, little change was observed inthe rate of Cr(VI) reduction (Proctor, Hays et al., 2002). The presence of foodindicated a much more rapid reduction of Cr(VI) when compared to the fastingstate; however, even in the absence of food, reduction of Cr(VI) concentrationswell in excess of the current MCL was achieved. Thus, as a result of these studies,the potential variation in stomach pH and fasting status should not be a sourceof uncertainty when assessing risks of Cr(VI) when ingested in tap water.
Although it is intuitively apparent that inhalation and dermal exposure toplausible concentrations of Cr(VI) in tap water would not provide a dose ofsignificance, the studies described herein were conducted nonetheless, to satisfyquestions that had been (or will be) raised by the courts. Based on the resultsof these human exposure studies, even if one assumes 100% retention andabsorption of inhaled Cr(VI) aerosols, the inhalation hazard is not significantlydifferent from that due to background exposure to airborne Cr(VI) (Finley et al.,1996). In fact, the inhaled dose of Cr(VI) associated with showering at concen-trations up to 10 mg/L is so small as to pose a de minimis cancer hazard.
Although dermal contact with tap water occurs when showering, bathing,and swimming, if the water is contaminated with either Cr(III) or Cr(VI), onewould not expect appreciable absorption of either species. Even if very smallamounts of Cr(VI) penetrate the epidermis, one would expect that the substan-tial quantities of organic reducing agents in the skin would readily convertCr(VI) to Cr(III). Further, because most Cr(III) compounds are less soluble andpermeable than Cr(VI), the concentration-dependent reduction of Cr(VI) cangreatly attenuate penetration of the metal to the deeper skin layers where vascu-lar uptake occurs (Gammalgaard et al., 1992). As a result of these studies, thepotential dermal hazard from contact with Cr(VI) is no longer a source ofuncertainty, since Cr(VI) concentrations as high as 22 mg/L do not overwhelmthe reductive capacity of the skin or blood (Corbett et al., 1997). The dermalhazard can thus be considered insignificant.
Based on results of the studies mentioned herein, if tap water is contami-nated with Cr(VI), ingestion is clearly the route of exposure that presents theprimary health hazard. As noted, although there is every indication that virtu-ally all of the Cr(VI) will be reduced prior to systemic circulation, the support-ing data are derived from short-term studies. For example, the longest animaland human studies where contaminated water was ingested and blood
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
12:
38 1
2 M
arch
201
3
1334 D. J. PAUSTENBACH ET AL.
was collected was about 1y. For this reason, at the request of the CaliforniaLegislature, the National Toxicology Program agreed to conduct a two-speciesclassic rodent bioassay of ingested Cr(VI); these results should be available in2006. Their Web site offers more information about doses and other details(http://ntp-server.niehs.nih.gov).
The overwhelming weight of evidence presented in both the historicalstudies conducted by various researchers and those conducted over the past5years by our group, clearly indicates that ingestion of Cr(VI) in drinking waterat concentrations at least as high as 100 µg/L, and possibly much higher,should not pose an increased acute or chronic health risk. The absence of clinicalfindings in the various human studies described in this report supportthe current health advisories and regulatory guidelines concerning Cr(VI)(e.g., IRIS, 2002), which indicate that one would not expect a cancer hazardto be associated with ingestion of chromium-contaminated drinking water.Based on the results of chromium ingestion studies presented here and elsewhere,the current U.S. EPA MCL of 100µg/L for Cr(VI) clearly contains a significantmargin of safety for preventing both acute and chronic health hazards.
REFERENCES Adams, R. M. 1990. Histologic diagnosis of inflammatory skin diseases, pp. 223–226. Philadelphia: Lea and
Febiger. Adolph, E. F. 1969. Physiology of man in the desert. New York: Hafner. Agency for Toxic Substances and Disease Registry. 2001. Toxicological profile for chromium (update).
Atlanta, GA: ATSDR, U.S. Public Health Service.Anderson, R. A., Bryden, N. A., and Polansky, M. M. 1997. Lack of toxicity of chromium chloride and chromium
tripicolinate in rats. J. Am. Coll. Nutr. 16:273–279.Anderson, R. A., and Kozlovsky, A. S. 1985. Chromium intake, absorption and excretion of subjects
consuming self-collected diet. Am. J. Clin. Nutr. 41:1177–1183. Avery, G. B., Randolph, J. G., and Weaver, T. 1966. Gastric acidity in the first day of life. Pediatrics
37:1005–1007. Baranowska-Dutkiewicz, B. 1981. Absorption of hexavalent chromium by skin in man. Arch. Toxicol.
47:47–50. Barnhart, J. 1997. Occurrences, uses, and properties of chromium. Regul. Toxicol. Pharmacol. 26:S3–S7. Blankstein, A. 2001. Bill on chromium VI standard to be proposed. Los Angeles Times, February 23. Boelter, F. W., Crawford, G. N., and Podraza, D. M. 2002. Airborne fiber assessment of dry asbestos-
containing gaskets and packings found in intact industrial and maritime fittings. Am. Ind. Hyg. Assoc. J.63:732–740.
Borneff, J., Engelhardt, K., Griem, W., Kunte, H., and Reichert, J. 1968. Carcinogenic substances in water andsoil. XXII. Mouse drinking study with 3,4-benzpyrene and potassium chromate. Arch. Hyg. 152:43–53.
Bureau of National Affairs (BNA) Reporter. November 20, 2001. Daily Environment Report No. 222. Page A-11.Calabrese, E. J., and Stanek, E. J. III. 1991. A guide to interpreting soil ingestion studies. II. Qualitative and
quantitative evidence of soil ingestion. Regul. Toxicol. Pharmacol. 13:278–292. Calabrese, E. J., and Stanek, E. J. III. 1995. Resolving intertracer inconsistencies in soil ingestion estimation.
Environ. Health Perspect. 103:454–457. Calabrese, E. J. and Stanek, E. J. III. 1998. Soil ingestion in children and adults: A dominant influence in site-
specific risk assessment. Environ. Law Rep. 28:10,660–10,671. Calabrese, E. J., Stanek, E. J., and Barnes, R. 1996. Methodology to estimate the amount and particle size of
soil ingested by children: Implications for exposure assessment at waste sites. Regulo. Toxicol. Pharmacol.24:264–268.
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
12:
38 1
2 M
arch
201
3
RISK FROM CR(VI) IN DRINKING WATER 1335
Calabrese, E. J., Stanek, E. J. III, Pekow, P., and Barnes, R. M. 1997. Soil ingestion estimates for childrenresiding on a Superfund site. Ecotoxicol. Environ. Safety 36:258–268.
Capellmann, M., and Bolt, H. M. 1992. Chromium(VI) reducing capacity of ascorbic acid of human plasmain vitro. Arch. Toxicol. 66:45–50.
Chute, S. M., Overman, S. K., Kerger, B. D., Finley, B. L., and Paustenbach, D. J. 1996. The chromium(VI)reductive capacity of household beverages: Implications for risk assessment. Toxicologist 30:4.
Coogan, T. P., Squibb, K. S., Motz, J., Kinney, P. L., and Costa, M. 1991. Distribution of chromium withincells of the blood. Toxicol. Appl. Pharmacol. 108:157–166.
Costa, M. 1990. Analysis of DNA-protein complexes induced by chemical carcinogens. J. Cell. Biochem.44:127–135.
Corbett, G. E., Dodge, D. G., O’Flaherty, E., Liang, J., Throop, L., Finley, B. L., and Kerger, B. D. 1998.In vitro reduction kinetics of hexavalent chromium in human blood. Environ. Res. 7:7–11.
Corbett, G. E., Finley, B. L., Paustenbach, D. J., and Kerger, B. D. 1997. Systemic uptake of chromium inhuman volunteers following dermal contact with hexavalent chromium (22 mg/L): Implications for riskassessment. J. Expos. Anal. Environ. Epidemiol. 7:179–189.
Costa, M. 1997. Toxicity and carcinogenicity of Cr(VI) in animal models and humans. Crit. Rev. Toxicol.27:431–442.
Costa, M. 2003. Potential hazards of hexavalent chromate in our drinking water. Toxicol. Appl. Pharmacol.188:1–5.
Costa, M., Harris, M., Paustenbach, D., and Gargas, M. 1997. DNA-protein cross-links produced by variouschemicals in cultured human lymphoma cells. J. Toxicol. Environ. Health 50:433–449.
Costa, M., Zhikovich, A., Gargas, M., Paustenbach, D., Finley, B., Kuykendall, J., Billings, R., Carlson, T. J.,Wetterhahn, K., Xu, J., Patierno, S., and Bogdanffy, M. 1996. Interlaboratory validation of a new assayfor DNA-protein crosslinks. Mutat. Res. 369:13–21.
Creasy, C. L. and Flegal, A. R. 1999. Elemental analyses of groundwater: Demonstrated advantageof low-flow sampling and trace-metal clean techniques over standard techniques. Hydrogeo. J.7:161–167.
Crump, C., Crump, K. S., Hack, E., Luippold, R. S., Mundt, K. A., Panko, J. P., Liebig, E. W., Paustenbach, D. J.,and Proctor, D. 2003. Dose-response analysis of hexavalent chromium and lung cancer mortality. RiskAnal. (in review).
Davis, S., Waller, P., Buschom, R., Ballou, J., and White, P. 1990. Quantitative estimates of soil ingestion innormal children between the ages of 2 and 7 years: Population-based estimates using aluminum,silicon, and titanium as soil trace elements. Arch. Environ. Health 45:112–122.
De Flora, S. 2000. Threshold mechanisms and sites specificity in chromium(VI) carcinogenesis. Carcinogenesis21:533–541.
De Flora, S., Badolati, G. S., Serra, D., Picciotto, A., Magnolia, M. R., and Savarino, V. 1987. Circadianreduction of chromium in the gastric environment. Mutat. Res. 192:169–174.
De Flora, S., Camoirano, A., Bagnasco, M., Bennicelli, C., Corbett, G. E., and Kerger, B. D. 1997. Estimatesof the chromium(VI) reducing capacity in human body compartments as a mechanism for attenuatingits potential toxicity and carcinogenicity. Carcinogenesis 18:531–537.
De Flora, S., and Wetterhahn, K. 1989. Mechanisms of chromium metabolism and genotoxicity. Life Chem.Rep. 7:169–244.
Department of Health Services (DHS). 2002. Chromium-6 (hexavalent chromium) in drinking water:An overview of sampling results. www.dhs.ca.gov/ps/ddwem/chemicals/chromium6/Cr + 6index.htm.Last updated 2 April 2001. Sacramento: California DHS.
Donaldson, R. M., Jr., and Barreras, R. F. 1966. Intestinal absorption of trace quantities of chromium. J. Lab.Clin. Med. 68:484–493.
Edel, J., and Sabbioni, E. 1985. Pathways of Cr(III) and Cr(VI) in the rat after intratracheal administration.Hum. Toxicol. 4:409–416.
Ershow, A. G., and Cantor, K. P. 1989. Total water and tapwater intake in the United States: Population-based estimates of quantities and sources. Bethesda, MD: National Cancer Institute and Life SciencesResearch Office, Federation of American Societies for Experimental Biology.
Finley, B. L., Fehling, K., Falerios, M., and Paustenbach, D. J. 1993. Field validation of sampling and analysisof airborne hexavalent chromium. Appl. Occup. Environ. Hyg. 8:191–200.
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
12:
38 1
2 M
arch
201
3
1336 D. J. PAUSTENBACH ET AL.
Finley, B. L., Kerger, B. D., Corbett, G. E., Katona, M., Gargas, M., Reitz, R., and Paustenbach, D. J. 1997.Human ingestion of chromium(VI) in drinking water: Pharmacokinetics following repeated exposure.Toxicol. Appl. Pharmacol. 142:151–159.
Finley, B. L., Kerger, B. D., Dodge, D. G., Meyers, S. M., Richter, R. O., and Paustenbach, D. J. 1996.Assessment of airborne hexavalent chromium in the home following use of contaminated tap water.J. Expos. Anal. Environ. Epidemiol. 6:229–245.
Finley, F. L., and Mayhall, D. A. 1994. Airborne concentrations of chromium due to contaminated interiorbuilding surfaces. Appl. Occup. Hyg. 9:433–441.
Flegal, R., Last, J., McConnell, E. E., Schenker, M., and Witschi, H. 2001. Scientific review of toxicological andhuman health issues related to the development of a public health goal for chromium(VI). Sacramento,CA: Governor’s Task Force. http://www.oehha.ca.gov/public_info/facts/pdf/CrPanelRptFinal901.pdf
Fowler, J.F., Kauffman, C. L., Marks, J. G., Proctor, D. M., Fredrick, M. M., Otani, J. M., Finley, B. L.,Paustenbach, D. J., and Nethercott, J. R. 1999. An environmental hazard assessment of low-leveldermal exposure to hexavalent chromium in solution among chromium-sensitized volunteers.J. Occup. Enivron. Med. 41:150–160.
Frzek, J. P., Mumma, M. T., McLaughlin, J. K., Henderson, J. K., and Blot, W. J. 2001. Cancer mortality inrelation to environmental chromium exposure. J. Occup. Environ. Med. 43:635–640.
Gammalgaard, B., Fullerton, A., Avnstorp, C., and Meene, T. 1992. Permeation of chromium salts throughhuman skin in vitro. Contact Dermatitis 27:302–310.
Gargas, M. L., Norton, R. B., Harris, M. A., Paustenbach, D. J., and Finley, B. L. 1994. Urinary excretion ofchromium following ingestion of chromite-ore processing residues in humans: implications forbiomonitoring. Risk Anal. 14:1019–1024.
Gibb, H. J., Lees, P. S., Pinsky, P. F., and Rooney, B. C. 2000. Lung cancer among workers in chromiumchemical production. Am. J. Ind. Med. 38:115–126.
Gibson, J. E., ed. 1983. Formaldehyde toxicity. Washington DC: Hemisphere. Grammer-West, N., Fitzpatrick, J., Jackson, R., Horton, H., and Damiano, M. 1996. Comparison of the
irritancy of hand washing dish liquids with modified patch-testing methods. J. Am. Acad. Dermatol.35:258–259.
Gray, S. J., and Sterling, K. 1950. The tagging of red cells and plasma proteins with radioactive chromium.J. Clin. Invest. 29:1604–1613.
Gross, E., and Heller, O. 1940. Chemie und Krebs. Berlin: Verlag Chemie. Hathaway, J. A. 1989. Role of epidemiologic studies in evaluating the carcinogenicity of chromium
compounds. Sci. Total Environ. 86:169–179. Integrated Risk Information System (IRIS). 2002. U.S. Washington, DC: Environmental Protection Agency.
http://www.epa.gov/iris/. International Agency for Research on Cancer. 1980. Some metals and metallic compounds. IARC Monogr.
Eval. Carcinogen. Risk of Chem. Hum. 230. International Agency for Research on Cancer. 1990. Chromium, nickel and welding. IARC Monogr. Eval.
Carcinogen. Risks Hum. 49:49–256. International Chromium Development Association. 1997. Criteria document for hexavalent chromium.
Paris: ICDA. International Commission on Radiological Protection (ICRP). 1984. Report of the task on reference manual,
pp. 8–20. New York: Pergomon Press.James, B. R., Petura, J. C., Vitale, R. J., and Mussoline, G. R. 1997. Oxidation-reduction chemistry of chro-
mium: Relevance to the regulation and remediation of chromate-contaminated soils. J. Soil. Contam.6:569–580.
Kararli, T. T. 1995. Comparison of the gastrointestinal anatomy, physiology, and biochemistry of humansand commonly used laboratory animals. Biopharm. Drug Dispos. 16:351–380.
Kerger, B. D., Finley, B. L., Corbett, G. E., Dodge, D. G., and Paustenbach, D. J. 1997. Ingestion of chro-mium(VI) in drinking water by human volunteers: Absorption, distribution, and excretion of single andrepeated doses. J. Toxicol. Environ. Health 50:67–95.
Kerger, B. D., Paustenbach, D. J., Corbett, G. E., and Finley, B. L. 1996. Absorption and elimination oftrivalent and hexavalent chromium in humans following ingestion of a bolus dose in drinking water.Toxicol. Appl. Pharmacol. 141:145–158.
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
12:
38 1
2 M
arch
201
3
RISK FROM CR(VI) IN DRINKING WATER 1337
Kerger, B. D., Richter, R. O., Chute, S. M., Dodge, D. G., Overman, S. K., Liang, J., Finley, B. L., andPaustenbach, D. J. 1996. Refined exposure assessment for ingestion of tapwater contaminated withhexavalent chromium: Consideration of exogenous and endogenous reducing agents. J. Expos. Assess.Environ. Epidemiol. 6:163–179.
Kligman, A. 1996. Hydration injury to human skin. In The irritant contact dermatitis syndrome, pp. 187–194.New York: CRC Press.
Korallus, U. 1986. Chromium compounds: Occupational health, toxicological and biological monitoringaspects. Toxicol Environ Chem. 12:47–59.
Kuykendall, J. R., Kerger, B. D., Jarvi, E. J., Corbett, G. E., and Paustenbach, D. J. 1996. Measurement ofDNA-protein cross-links in human leukocytes following acute ingestion of chromium in drinking water.Carcinogenesis 17:1971–1977.
Lewalter, J., Korallus, U., Harzdorf, C., and Weidemann, H. 1985. Chromium bond detection in isolatederythrocytes: A new principle of biological monitoring of exposure to hexavalent chromium. Int. Arch.Occup. Environ. Health 55:305–318.
Lindberg, E., and Hedensteirna, G. 1983. Chrome plating: Symptoms, finding in the upper airways andeffects on lung function. Arch. Environ. Health 38:367–374.
MacKenzie, R. D., Byerrum, R. U., Decker, C. F., Hoppert, C. A., and Langham, R. F. 1958. Chronic toxicitystudies II. Hexavalent and trivalent chromium administered in drinking water to rats. Arch. Ind. Health.18:232–234.
Maddaloni, M., Lolacono, N., Manton, W., Blum, C., Drexler, J., and Graziano, J. 1998. Bioavailability of soil-borne lead in adults, by stable isotope dilution. Environ. Health. Perspect. 106(suppl. 6): 1589–1594.
Madl, A., and Paustenbach, D. J. 2002. Airborne concentration of benzene due to diesel locomotiveexhaust in a roundhouse. J. Toxicol. Environ. Health A 65:1945–1964.
Mancuso, T. F. 1975. Consideration of chromium as an industrial carcinogen. International Conference onHeavy Metals in the Environment, Toronto, Canada. October 27–31. pp. 343–356.
Marks, J., and Deleo, V. A. 1992. Contact and occupational dermatology. St. Louis, MO: Mosby Year Book.Miksche, L., Lewalter, J., and Korallus, U. 1994. Determination of chromium in erythrocytes: A new
principle for biological monitoring in chromium(VI) exposed workers. Proceedings of a Department ofEnergy Symposium on Biomarkers, San Diego, CA, February.
Miller, J. S. 1950. Effect of chromates on nose, throat, and ear. AMA Arch. of Otolaryngology. pp. 172–178.Mirsalis, J. C., Hamilton, C. M., O’Loughlin, K. G., Paustenbach, D. J., Kerger, B. D., and Patierno, S. 1996.
Chromium(VI) at plausible drinking water concentrations is not genotoxic in the in vivo bone marrowmicronucleus or liver UDS assays. Environ. Mol. Mutat. 28:60–63.
Nagita, A., Amemoto, K., Yoden, A., Aoki, S., Sakaguchi, M., Ashida, K., and Mino, M. 1996. Diurnal variationin intragastric pH in children with and without peptic ulcers. Pediatr. Res. 40:528–532.
National Academy of Sciences. 2001. Chromium. In Dietary reference intakes for vitamin A, vitamin K,arsenic, boron, chromium, copper, iodine, iron, manganese, molybdenum, nickel, silicon, vanadium,and zinc, p. 6. Washington, DC: National Academy Press.
Nethercott, J., Paustenbach, D. J., Adams, R., Horowitz, S., Finley, B. E., Fowler, J., Marks, J., Morton, C.,and Taylor, J. 1994. A study of chromium induced allergic contact dermatitis with 54 volunteers:Implications for environmental risk assessment. Occup. Environ. Med. (Lon) 51:371–380.
Office of Environmental Health Hazard Assessment. 1999. Public health goal for chromium in drinkingwater. Berkeley: Office of Environmental Health Hazard Assessment, California Environmental ProtectionAgency.
O’Flaherty, E. J. 1993. Physiologically based models for bone-seeking elements. IV. Kinetics of lead dispositionin humans. Toxicol. Appl. Pharmacol. 118:16–29.
O’Flaherty, E. J. 1996. A physiologically based model of chromium kinetics in the rat. Toxicol. Appl. Pharmacol.138:54–64.
O’Flaherty, E. J., Kerger, B. D., Hays, S. M., and Paustenbach, D. J. 2001. A physiologically based modelfor the ingestion of chromium(III) and chromium(VI) by humans. Toxicol. Sci. 60:196–213.
Ottenwaelder, H., and Wiegand, H. J. 1988. Uptake of 51Cr(VI) by human erythrocytes: Evidence for acarrier-mediated transport mechanism. Sci. Total Environ. 71:561–566.
Paustenbach, D. 2000. The practice of exposure assessment: A state-of-the-art review. J. Toxicol. Environ.Health. 3:179–291.
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
12:
38 1
2 M
arch
201
3
1338 D. J. PAUSTENBACH ET AL.
Paustenbach, D. J., Hays, S., Brien, B., Dodge, D. G., and Kerger, B. D. 1996. Observation of steady statein blood and urine following human ingestion of hexavalent chromium in drinking water. J. Toxicol.Environ. Health 49:453–461.
Paustenbach, D. J., Sheehan, P. J., Paull, J. M., Wisser, L. M., and Finley, B. L. 1992. Review of the allergiccontact dermatitis hazard posed by chromium-contaminated soil: Identifying a “safe” concentration.J. Toxicol. Environ. Health. 37:177–207.
Pennington, J. A. 1983. Revision of the total diet study food list and diets. J. Am. Diet. Assoc. Res.82:166–173.
Permana, P. A., and Snapka, R. M. 1994. Aldehyde-induced DNA-protein crosslinks disrupt specific stagesof SV 40 DNA replication. Carcinogenesis 15:1031–1036.
Proctor, D. M., Hays, S. M., Ruby, M. V., Liu, S., Sjong, A., Goodman, M., and Paustenbach, D. J. 2002.Rate of hexavalent chromium reduction by human gastric fluid. Abstr. 1700. Final Program andAbstracts. 41st Annual Meeting of Society of Toxicology, 17–21 March, Nashville, TN.
Proctor, D. M., Otani, J. M., Finley, B. L., Paustenbach, D. J., Bland, J. A., Speizer, N., and Sargent, E. V.,2002. Is hexavalent chromium carcinogenic via ingestion? A weight-of-evidence review. J ToxicolEnviron. Health Part A 65:701–46.
Proctor, D. M., Panko, J. P., Liebig, E. W., Scott, P. K., Buczynski, M. A., Barnhart, R. J., Harris, M. A., andMorgan, R. J. 2002. Exposure reconstruction for hexavalent chromium in a chromate production plant:1940–1973. Appl. Occup. Environ. Hyg.
Rowbotham, A. L., Levy, L. S., and Shuker, L. K. 2000. Chromium in the environment: An evaluation ofexposure of the UK general population and possible adverse health effects. J. Toxicol. Environ. Health.B 3:145–178.
Ruby, M. V., Fehling, K. A., and Paustenbach, D. J. 2002. Estimation of the oral bioaccessibility of dioxins/furans in weathered soil. US–Vietnam Scientific Conference on Human Health and EnvironmentalEffects of Agent Orange/Dioxin, 3–6 March, Ha Noi, Vietnam.
Sheehan, P. J., Ricks, R., Ripple, S., and Paustenbach, D. 1992. Field evaluation of a sampling and analyticalmethod for environmental levels of airborne hexavalent chromium. Am. Ind. Hyg. Assoc. J. 53:57–68.
Shi, X., Chiu, A., Chen, C. T., Halliwell, B., Castranova, V., and Vallyathan, V. 1999. Reduction ofchromium (VI) and its relationship to carcinogenesis. J. Toxicol. Environ. Health. B 2:87–104.
Thestrup-Pedersen, K., Madsen, J., and Rasmussen, K. 1989. Cumulative skin irritancy from heat-decomposed polyethylene plastic. In, Current topics in contact dermatitis, eds. P. Frosch, A.Dooms-Goosens, J. Lachapelle, R. Rycroft, and R. Scheper, pp. 412–416. New York: Springer-Verlag.
U.S. Environmental Protection Agency. 1984. Health effects assessment for chromium. Final report.Research Triangle Park, NC: Environmental Criteria and Assessment Office. EPA-600/8–83–014F.PB85–115905.
U.S. Environmental Protection Agency. 1990. Noncarcinogenic effects of chromium: Update to healthassessment document. Research Triangle Park, NC: U.S. EPA.
U.S. Environmental Protection Agency. 1991. National primary drinking water regulations—Syntheticorganic chemicals and inorganic chemicals; Monitoring for unregulated contaminants, national prim-ary drinking water regulation implementation, national secondary drinking water regulations. Fed. Reg.56:3526–3597.
U.S. Environmental Protection Agency. 1992. Dermal exposure guidelines. Washington, DC: U.S. EPA. U.S. Environmental Protection Agency. 1998. Toxicological profile update on hexavalent chromium.
Integrated Risk Information System (IRIS). Cincinnati, OH: U.S. EPA http:/ /www.epa.gov/iris. U.S. Environmental Protection Agency. 2003. Proposed EPA cancer guidelines. Washington, DC: U.S. EPA. Weber, H. 1983. Long-term study of the distribution of soluble chromate-51 in the rat after a single intra-
tracheal administration. J. Toxicol. Environ. Health 11:749–764. Widner, T., and Flack, S. M. 2002. Dose reconstructions for radionuclides and chemical: Case study involving
Federal facilities at Oak Ridge, Tennessee. In Human and ecological risk assessment, theory and practice,ed. D. J. Paustenbach, pp. 735–869. New York: John Wiley and Sons.
Wier, F., Tolar, G., and Meraz, L. 2001. Characterization of vehicular brake service personnel exposure toairborne asbestos and particulate. Appl. Occup. Environ. Hyg. 16:1139–1146.
Wiegand, H. J., Ottenwaelder, H., and Bolt, H. M. 1988. Recent advances in biological monitoring ofhexavalent chromium compounds. Sci. Total Environ. 71:309–315.
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
12:
38 1
2 M
arch
201
3
RISK FROM CR(VI) IN DRINKING WATER 1339
Williams, P. R. D., and Paustenbach, D. J. 2002. Risk characterization: Principles and practice. J. Toxicol.Environ. Health B 5:337–496.
Williams, P. R. D., and Paustenbach, D. J. 2003. Reconstruction of benzene exposures for the pliofilmcohort (1936–1976) using Monte Carlo techniques. J. Toxicol. Environ. Health, Part A. 66:677–781.
World Health Organization. 1988. Environmental health criteria 61: Chromium. Geneva: WHO. World Health Organisation. 1993. Recommendations. In Guidelines for drinking-water quality, 2nd ed.,
vol. 1, pp. 45–46. Geneva: WHO. Zhitkovich, A., and Costa, M. 1992. A simple, sensitive assay to detect DNA-protein crosslinks in intact cells



















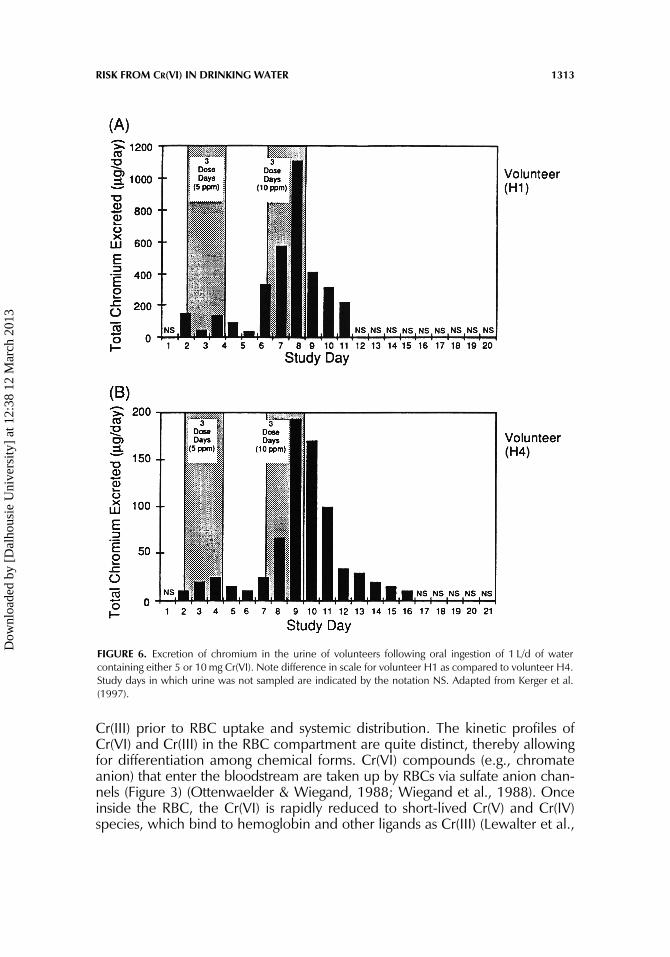





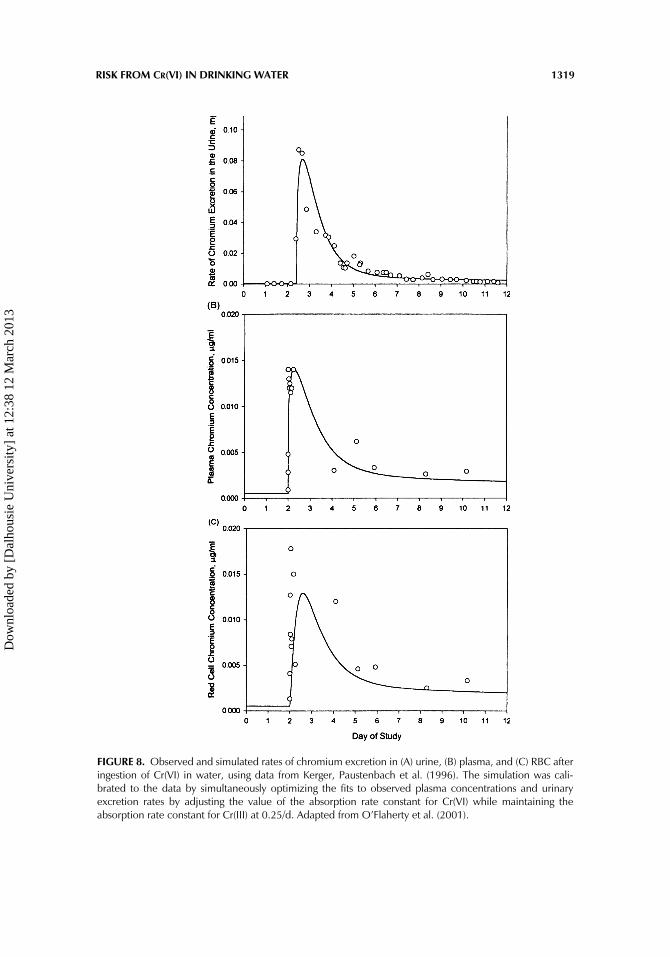


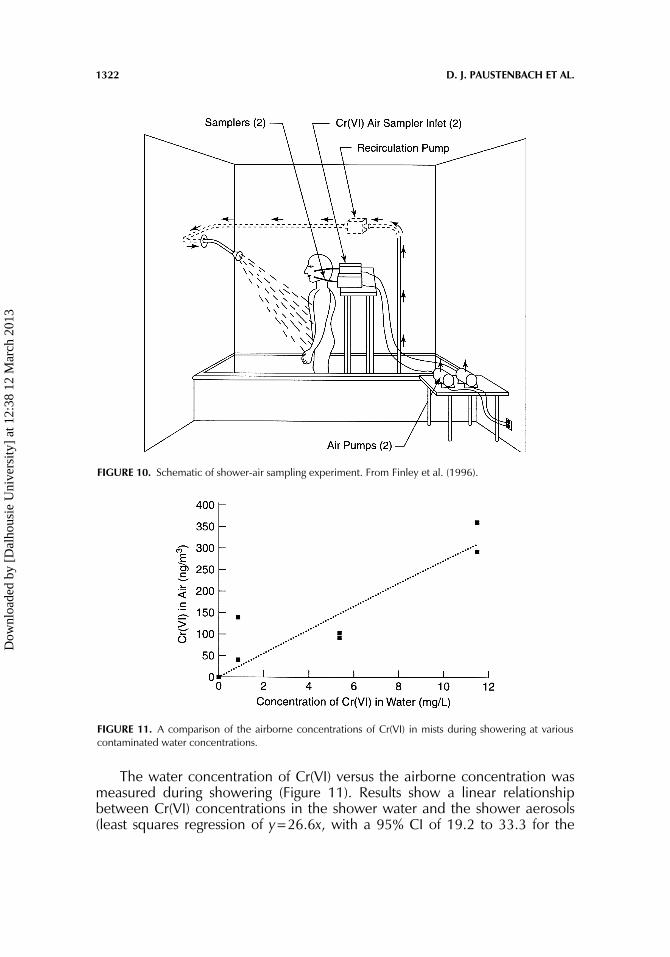



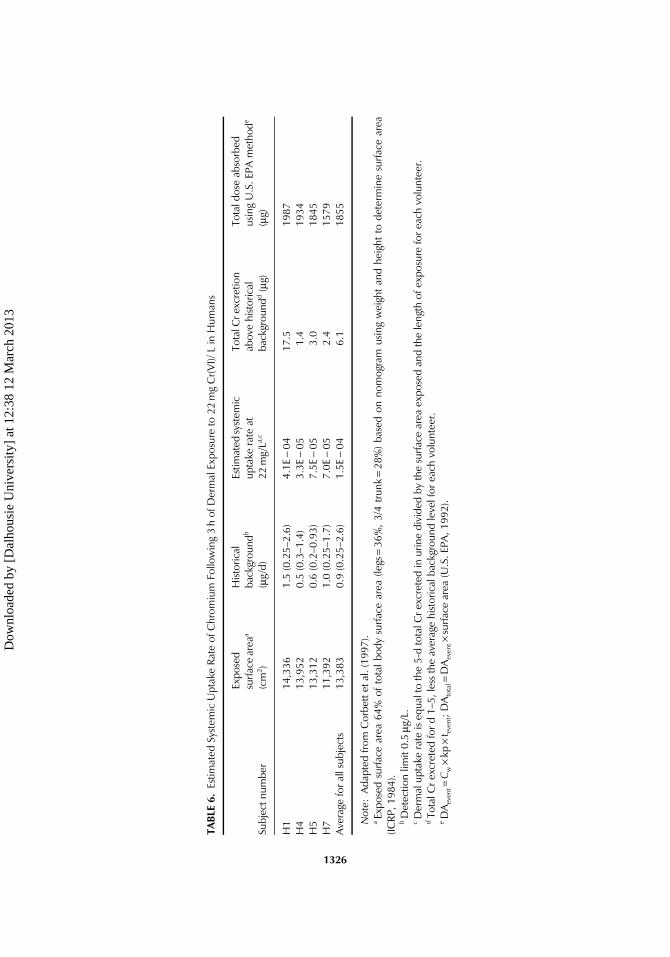





























![Occupational Exposure to Hexavalent Chromium [Cr(VI)] Doug Fletcher, CIH, CSP OSHA - OAO.](https://static.documents.pub/doc/80x56/56649e4a5503460f94b3dff6/occupational-exposure-to-hexavalent-chromium-crvi-doug-fletcher-cih-csp.jpg)

