14
Human Immunodeficiency Virus An Overview
Human Immunodeficiency Virus
An Overview
Human Immunodeficiency Virus
Acquired Immunodeficiency syndrome (AIDS)
first described in 1981
Belong to the lentivirus subfamily of the
retroviridae
Enveloped RNA virus, 120nm in diameter
Mode of transmission
Sexual transmission
Blood/blood products
Vertical transmission - the transmission from mother to
the newborn

HIV IS FOUND IN BODY FLUIDS
Semen
Breast milk
Blood
Vaginal fluid
3
Tears
Saliva
Sweat
Urine
You CANNOT get HIV from…

HIV-1 and HIV-2
HIV-1 and HIV-2 are
• Transmitted through the same routes
• Associated with similar opportunistic infections
HIV-2 is less easily transmitted
HIV-1 is more common worldwide
HIV-2 is found in West Africa, Mozambique.
HIV-2 is less pathogenic
Duration of HIV-2 infection is shorter
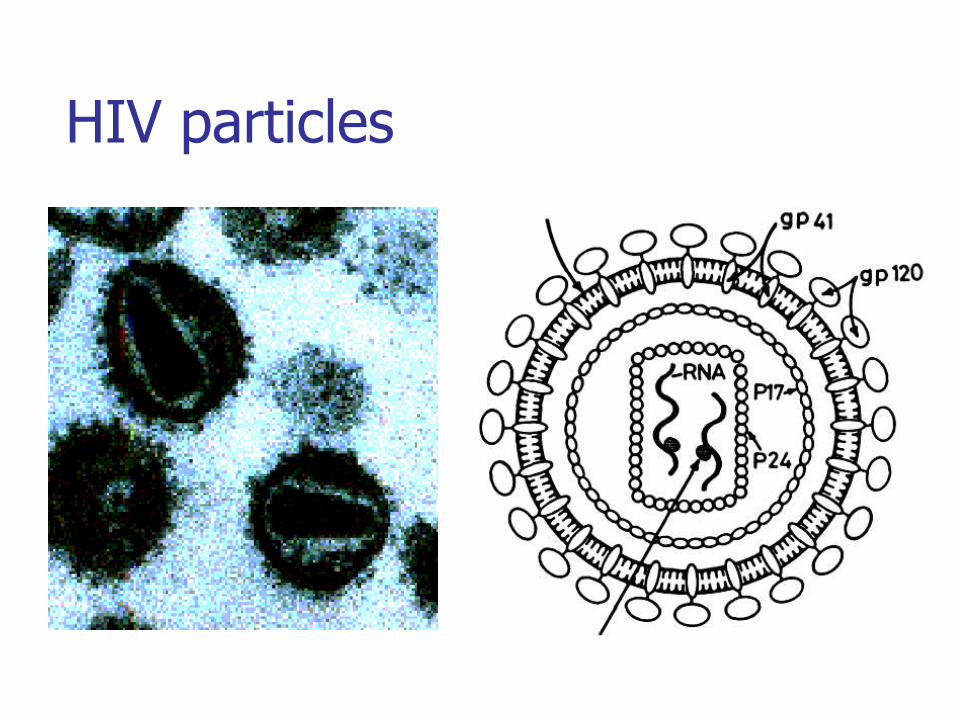
HIV particles
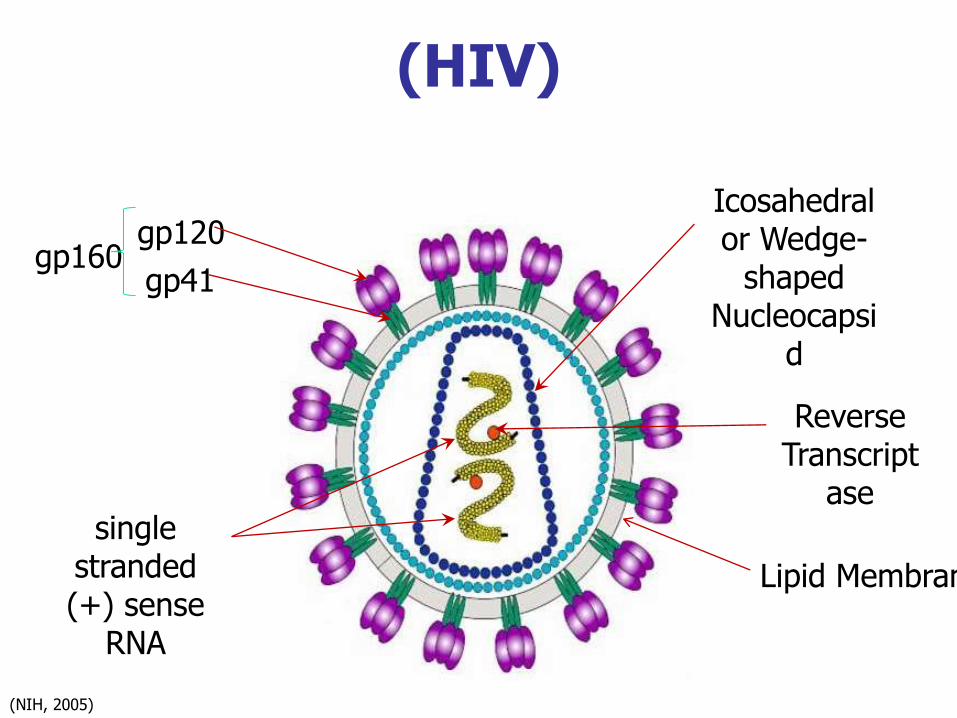
(HIV)
Icosahedral or Wedge-
shaped Nucleocapsi
d
Reverse Transcript
ase
Lipid Membrane
single stranded (+) sense
RNA
gp120
gp41gp160
(NIH, 2005)

Replication The first step of infection is the binding of gp120
to the CD4 receptor of the T helper cell
Macrophages, monocytes and dendritic cells express
CD4 receptors and also infected by the virus
which is followed by penetration and uncoating.
The gp41 mediates fusion of the viral envelope
with the cell membrane,
The RNA genome is then reverse transcribed
into a DNA provirus which is integrated into the
cell genome.
This is followed by the synthesis and maturation
of virus progeny.
Clinical Features1-The acute stage:
Begins 2-4 weeks after infection with a mononucleosis-
like picture
it resolves spontaneously in 2 weeks.
2-A latent stage:
For up to 10 years follows.
The patient is asymptomatic.
AIDS-related complex or persistent generalized
lymphadenopathy.
3-Full-blown AIDS.
AIDS
Opportunistic infection
Protozoal pneumocystis carinii , Toxoplasmosis
Fungal Candidiasis, crytococcosis, histoplasmosis
Bacterial Mycobacterium avium, MTB, AMB
Viral CMV, HSV, VZV, JCV
tumors
The most frequent opportunistic tumour, Kaposi's sarcoma
Malignant lymphomas
The most frequent neurological disorder is AIDS
encephalopathy
Other manifestations include characteristic skin
eruptions and persistent diarrhoea.

Kaposi’s Sarcoma
HIV Pathogenesis Immunosuppression in AIDS is due to depletion of T
helper cells.
Antibodies to HIV appear 3-4 weeks after infection.
An immune response, by cytotoxic T cells and humoral
immunity, controls the infection in the acute stage
In the acute stage, HIV is present at a high level in blood
It then derease to a certain low level during the Latent
stage.
AIDS develop when severe decrease in CD4 cells occur.

Laboratory Diagnosis
Decreased CD4 count and inversion of the
CD4/CD8 ratio
Serology detects antibodies against p24 or gp41,
gp120 or gp160 and others by ELISA and RIBA.
Detection of viral nucleic acid in clinical samples
by PCR
Detection of viral antigens i.e. p24 by ELISA,
Virus isolation from lymphocytes, bone marrow or
plasma
Treatments Reverse Transcriptase (RT) Inhibitors – interrupt
early stage of viral replication
1) Nucleoside/nucleotide RT inhibitors• Insert faulty DNA building blocks into HIV genome
• Prevents completion of DNA chain → no replication
2) Non-nucleoside RT inhibitors• Bind to reverse transcriptase and prevents reverse transcription
Protease Inhibitors – interrupt late stage of viral replication in the HIV life cycle
Fusion Inhibitors – new class of drugs• Fuzeon interferes with HIV ability to enter the cell
Nevirapine
Zidovudine
Indinavir Ritonavir Saquinavir
HAART
HAART (highly active anti-retroviral therapy): 2
nucleoside reverse transcriptase inhibitors and a
protease inhibitor. e.g. AZT, lamivudine and
indinavir.
Since the use of HAART, mortality from HIV has
declined dramatically in the developed world.
It may be possible to reduce toxicity, improve
efficacy and prevent resistance.
Reduces the amount of virus circulating in blood
to nearly undetectable levels.

















