Hydrocolonic sonography in the evaluation of colonic lesions
R. Dixit,1 V. Chowdhury,1 N. Kumar 2
1Department of Radiodiagnosis, Lok Nayak Hospital, and Associated Maulana Azad Medical College, New Delhi 110002, India2Department of Gastroenterology, G.B. Pant Hospital & Associated, Maulana Azad Medical College, New Delhi 110002, India
Received: 26 January 1998/Revision accepted: 12 August 1998
AbstractBackground:The present study was done to assess thesensitivity, specificity, ease of examination, and limita-tions of hydrocolonic sonography (HCS) to evaluate aheterogeneous spectrum of colonic disorders.Methods:In a prospective study, 100 patients (53 male,47 female) with clinical suspicion of colonic abnormalitywere examined by conventional abdominal sonography,HCS, and colonoscopy on the same day. The patients thenunderwent appropriately planned barium studies. His-topathologic diagnosis was established by colonoscopic/excision biopsies or fine needle aspiration cytology(FNAC) whenever indicated and results correlated.Results:In 94% of patients, it was possible to evaluate theentire colon from the rectosigmoid junction to the cecum.Redundant parts of the colon were not well evaluated bythis technique. The rectum could not be adequately eval-uated, and rectal examination was not included in thestudy. HCS can evaluate in great detail both the coloniclumen and wall and, hence, could suggest the nature ofthe lesion in the majority (87.9%) of cases based oncharacteristic changes in wall stratification, echogenicity,lumenal changes, and site and length of involvement,although distinguishing between benign and malignantlesions was not always possible. In 93% of patients withtuberculous colitis/ileocolitis, the normal wall stratifica-tion was no longer in evidence, with moderate hypo-echoic thickening of the wall (average5 8.34 mm).Malignant lesions (93.7%) showed grossly thickenedbowel wall with loss of stratification and hypoechoic/heterogeneous echo texture. Intralumenal polypoidmasses also were seen in 87.5% of cases, and there wasextension beyond the adventitia and involvement of peri-colonic tissues in 75% of cases. All patients with ulcer-ative colitis had only mild hypoechoic wall thickening;the five-layer structure could be clearly discerned in
87.5% of cases. HCS had an overall sensitivity of 90.9%and a specificity of 94.7% in this study.Conclusions:HCS can be advantageously used for diag-nosis and differential diagnosis of inflammatory and ma-lignant colonic lesions and also for follow-up of patientswith chronic inflammatory large bowel diseases such asulcerative colitis.
Key words: Hydrocolonic sonography—Colonic sonog-raphy—Tubercular colitis—Carcinoma of the colon—Ul-cerative colitis.
Until the 1970s, conventional transabdominal sonographyplayed only a subordinate role in the detection of bowellesions. Although the “target lesion” or “pseudokidney”appearance on routine sonography is a well-recognizedsign that represents thick hypoechoic bowel walls enclos-ing an echogeneic mucin- or air-filled lumen [1–8], de-tailed evaluation of the colonic lumen and wall is notpossible because of subtotal beam reflection by gas withinthe colonic lumen.
Distention of the bowel lumen with water removesmajor obstacles to sonographic evaluation of the colonbecause the beam transmission is significantly improved.Detailed evaluation of the colonic wall, large bowel lu-men, and the surrounding connective tissue is possibleduring transabdominal sonography subsequent to retro-grade water instillation [9–12].
Studies have shown that this new method, termedhydrocolonic sonography (HCS), enables accurate diag-nosis of colon tumors and inflammatory bowel disease[10–13].
The present study was done to assess the sensitivity,specificity, ease of examination, and limitations of HCSto evaluate a heterogeneous spectrum of colonic disor-ders.Correspondence to:R. Dixit
In a prospective study, 100 patients (53 male, 47 female; age range54–70 years) with strong clinical suspicion of colonic lesions wereexamined. Indications for examination included abdominal pain, weightloss, or testing positive for occult blood in stool. In patients withdiarrhea, stool cultures were normal and stool was negative for ova andcysts.
Procedure
A detailed transabdominal sonogram was done on all patients with aSiemens Sonoline SL2 scanner with 3.5- and 7.5-MHz transducers.Patients were then called for HCS after bowel preparation, whichincluded low-residue diet for 3 days and a laxative the night before theexamination.
Just before the examination, 20 mg of scopolamine N-butyl bromide(Buscopan) were given intravenously and up to 1500 mL of water werethen instilled rectally. The relaxant was injected to achieve optimaldistention of the colon and to suppress the sense of urgency. Continuoustransabdominal scanning was begun at the time of water instillation.Examination began at the rectosigmoid junction and ended at the cecum.Detailed evaluation of the rectum was not included in this study. Therectosigmoid junction was examined with the patient in the anti-Tren-delenberg position at the begining of the examination; the rest of thecolon was examined with the patient in the supine and decubituspositions, after which the patient evacuated the bowel. Careful analysisof the colonic wall echogeneity, stratification, haustral pattern, andcolonic lumen was done in each case to identify an abnormal colon.
Image analysis
The normal colon [9–13] has a wall thickness of 3–4 mm. The colonicwall shows five layers: layers 1, 3, and 5 are echogenic and layers 2 and4 are anechoic or hypoechoic. Layers 1 and 2 adjacent to the lumenrepresent the mucosa; layer 3 represents the submucosa; layer 4 repre-sents the muscularis propria; and layer 5 represents the serosa andsubserosal fatty tissues. The normal colon has an echo-free intestinallumen 4–5 cm wide, into which the haustral septa echo-rich lamellae,project. There is normal peristalsis in addition to normal surroundingconnective tissues.
The diagnosis of colonic tumors or lesions in the present study wasbased on the following features: wall thickness greater than 4 mm, lossof normal wall stratification, intralumenal masses fixed to the wall,lumenal narrowing, loss of haustral pattern, or abnormalities of sur-rounding connective tissues.
The diagnosis of an inflammatory lesion was suggested in cases withmild to moderate wall thickening with following features: preserved orlost wall stratification, no associated intralumenal mass, no evidence ofdirect extension of disease into pericolonic tissues, and involvement ofa long segment of the colon or simultaneous terminal ileal cecal in-volvement.
The diagnosis of a malignant neoplastic lesion was suggested whenthere was any degree of wall thickening with intralumenal masses fixedto the wall and loss of wall stratification at the base of the mass orthickening involving a short segment of colonic length, direct extensionof disease into pericolonic tissues, marked polypoidal wall thickening,or other supportive criteria on routine transabdominal scans such asmetastasis.
A polypoid projection was considered benign when it was smallerthan 1 cm or the wall stratification at the base of the lesion waspreserved.
Total colonscopy with or without fluoroscopic guidance was done inall patients except when the colonoscope could not be negotiated beyondan obstructing lesion after HCS on the same day. This was done by anexperienced gastroenterologist with no prior knowledge of findings onHCS. Tissue biopsies were obtained whenever indicated. Appropriatelyplanned barium studies were then done in all patients, and the findingswere recorded. Pathologic diagnosis was established by colonoscopic/excision biopsies or FNAC, and results were correlated.
Results
In 94% of patients, it was possible to evaluate the entirecolon from the rectosigmoid junction to the cecum byHCS. The rectum could not be adequately evaluated be-cause of the limits of ultrasound beam penetration andoverlying bowel gas; rectal evaluation was not included inthe study. In 6% of cases, a complete examination was notpossible because of excessive obesity and bowel gas.Ascending and descending colons were the best visual-ized parts. Transverse colon and flexures, especially whenredundant, were difficult to evaluate, and the colonic wallstratification could not be regularly visualized in redun-dant parts. The total examination time was 15–20 min, theexamination was tolerated well by the patients, and therewere no side effects or failures of examination.
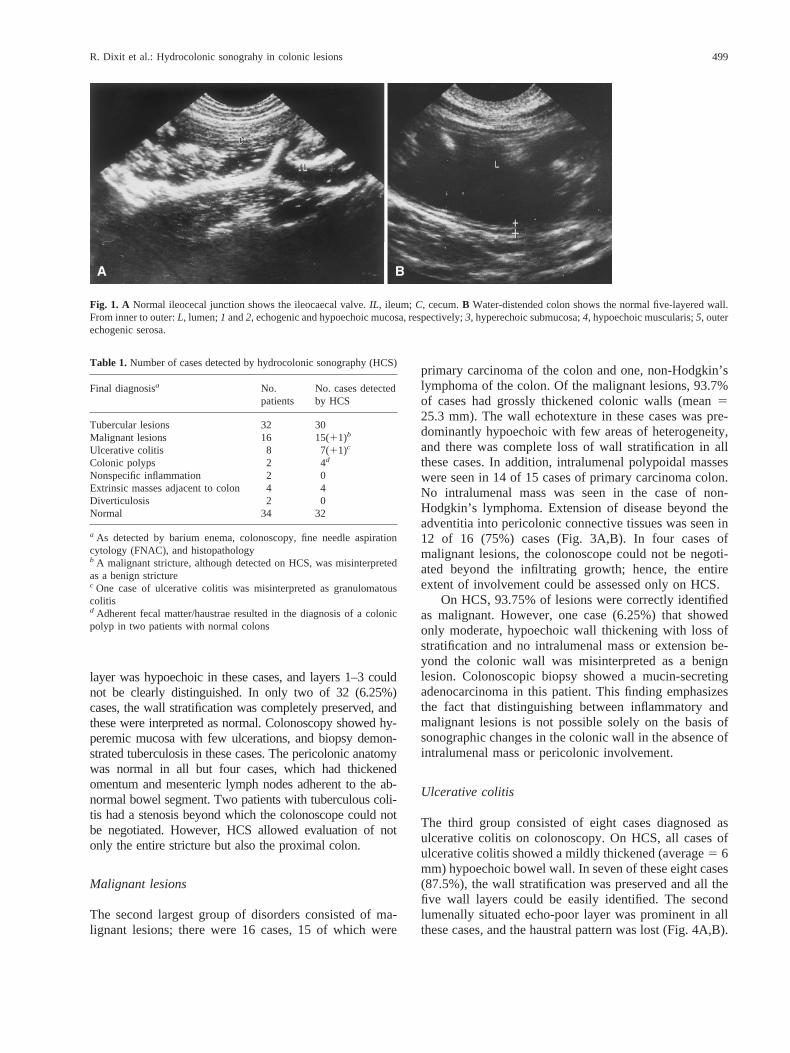
During HCS, the normal colon demonstrated an echo-free intestinal lumen 4–5 cm wide, with ribbon-shapedhaustra projecting into it. The normal colonic wallshowed five layers of different echo patterns; the totalthickness of the wall was 3–4 mm (Fig. 1A,B).
Of the 100 cases examined, 34 were normal and 66were proven to be abnormal on colonoscopic examina-tion/biopsy or barium studies.
Table 1 presents the number of cases that could bedetected by HCS. Table 2 presents the site of involvementin neoplastic and inflammatory colonic lesions accordingto final diagnosis. Table 3 presents the HCS findings ofwall thickness alterations in different malignant and in-flammatory diseases. Table 4 presents the alteration inwall architecture in malignant and inflammatory diseases.
Tuberculous lesions
Thirty of the 32 (93.7%) tuberculous lesions were detectedby HCS, and two cases of ileocecal tuberculosis were missedon HCS. As evident from Tables 2–4, patients with tuber-culous lesions had predominant involvement of the ileocecalregion (28/32, 87.5%). There was segmental involvement ofthe colon in four (12.5%) cases, as indicated by a longsegment stricture with tapered margins. Cases with tubercu-lous colitis showed hypoechoic bowel wall, which wasclearly thickened (average5 8.34 mm), and the haustralpattern was no longer seen. There was complete loss of wallstratification in 24 of 32 (75%) cases (Fig. 2A,B). In six of32 (18.7%) cases, the wall layers were partly lost, the third
498 R. Dixit et al.: Hydrocolonic sonograhy in colonic lesions
layer was hypoechoic in these cases, and layers 1–3 couldnot be clearly distinguished. In only two of 32 (6.25%)cases, the wall stratification was completely preserved, andthese were interpreted as normal. Colonoscopy showed hy-peremic mucosa with few ulcerations, and biopsy demon-strated tuberculosis in these cases. The pericolonic anatomywas normal in all but four cases, which had thickenedomentum and mesenteric lymph nodes adherent to the ab-normal bowel segment. Two patients with tuberculous coli-tis had a stenosis beyond which the colonoscope could notbe negotiated. However, HCS allowed evaluation of notonly the entire stricture but also the proximal colon.
Malignant lesions
The second largest group of disorders consisted of ma-lignant lesions; there were 16 cases, 15 of which were
primary carcinoma of the colon and one, non-Hodgkin’slymphoma of the colon. Of the malignant lesions, 93.7%of cases had grossly thickened colonic walls (mean525.3 mm). The wall echotexture in these cases was pre-dominantly hypoechoic with few areas of heterogeneity,and there was complete loss of wall stratification in allthese cases. In addition, intralumenal polypoidal masseswere seen in 14 of 15 cases of primary carcinoma colon.No intralumenal mass was seen in the case of non-Hodgkin’s lymphoma. Extension of disease beyond theadventitia into pericolonic connective tissues was seen in12 of 16 (75%) cases (Fig. 3A,B). In four cases ofmalignant lesions, the colonoscope could not be negoti-ated beyond the infiltrating growth; hence, the entireextent of involvement could be assessed only on HCS.
On HCS, 93.75% of lesions were correctly identifiedas malignant. However, one case (6.25%) that showedonly moderate, hypoechoic wall thickening with loss ofstratification and no intralumenal mass or extension be-yond the colonic wall was misinterpreted as a benignlesion. Colonoscopic biopsy showed a mucin-secretingadenocarcinoma in this patient. This finding emphasizesthe fact that distinguishing between inflammatory andmalignant lesions is not possible solely on the basis ofsonographic changes in the colonic wall in the absence ofintralumenal mass or pericolonic involvement.
Ulcerative colitis
The third group consisted of eight cases diagnosed asulcerative colitis on colonoscopy. On HCS, all cases ofulcerative colitis showed a mildly thickened (average5 6mm) hypoechoic bowel wall. In seven of these eight cases(87.5%), the wall stratification was preserved and all thefive wall layers could be easily identified. The secondlumenally situated echo-poor layer was prominent in allthese cases, and the haustral pattern was lost (Fig. 4A,B).
Table 1. Number of cases detected by hydrocolonic sonography (HCS)
a As detected by barium enema, colonoscopy, fine needle aspirationcytology (FNAC), and histopathologyb A malignant stricture, although detected on HCS, was misinterpretedas a benign stricturec One case of ulcerative colitis was misinterpreted as granulomatouscolitisd Adherent fecal matter/haustrae resulted in the diagnosis of a colonicpolyp in two patients with normal colons
Fig. 1. A Normal ileocecal junction shows the ileocaecal valve.IL, ileum; C, cecum.B Water-distended colon shows the normal five-layered wall.From inner to outer:L, lumen;1 and2, echogenic and hypoechoic mucosa, respectively;3, hyperechoic submucosa;4, hypoechoic muscularis;5, outerechogenic serosa.
R. Dixit et al.: Hydrocolonic sonograhy in colonic lesions 499
In one (14.2%) case, the normal wall stratification was notidentified. This case was misinterpreted as granulomatous(tuberculous) colitis. However, on colonoscopy this pa-tient was found to have ulcerative colitis with extensivepseudopolyposis. The extent of colonic involvement wascorrectly diagnosed in 87.5% cases of ulcerative colitisand was underestimated in 12.5% cases.
Miscellaneous lesions
Among the miscellaneous lesions studied, there were twocases of colonic polyps, diverticulosis and nonspecificproctocolitis. The two patients with colonic polypsshowed small well-defined lumenal polypoid projectionswith preserved wall stratification and echogenicity at thebase of the polyps. The number of polyps was alsocorrectly interpreted in both cases on HCS (Fig. 5). Thesmallest polyp detected in the present study was 7 mm. Afalse-positive diagnosis of colonic polyps was made intwo cases. In one case, adherent fecal matter was misin-
terpreted as a small polyp; in another, a haustral projec-tion was misinterpreted as a polyp. Colonoscopy wasnormal in both cases, thereby emphasizing the fact thatsmall colonic polyps cannot be diagnosed with confidenceon HCS.
In four cases, small bowel masses adjacent to thecolon were detected. The adjacent colonic lumen showedonly minimal extrinsic compression; hence, colonoscopywas normal in these cases. The cases with nonspecificproctocolitis were interpreted as normal on HCS.Colonoscopy in these cases showed mucosal hyperemiaand a few superficial ulcerations.
Two cases presented very small diverticula in thesigmoid colon on barium enema studies. These could notbe detected on HCS.
Thus, HCS could successfully detect an abnormalityin 60 of the 66 positive cases (sensitivity5 90.9%) and itcorrectly suggested the nature of lesion in 58 of the 66pathological cases (87.9%). There were two false-positivecases in the study, for a specificity of 94.7%.
Discussion
Ultrasonography is the most easily available, noninva-sive, and safe imaging modality for evaluating organsystems. It uses the concept of ultrasound beam reflectionat interphases of different acoustic impedances.
In patients with bowel diseases, diseased bowel seg-ments can be demonstrated by conventional sonographyas a thickened hypoechoic bowel wall [1–8]; however,colonic lumenal gas and mucus in partially collapsedviscus cause subtotal reflection of the beam, thus grosslydegrading the contrast between layers of bowel wall.Thus, conventional sonography is not very sensitive; itdoes not allow detailed evaluation of the colonic lumenand wall architecture; hence, differentiation between dif-ferent types of inflammatory lesions and between malig-nant and inflammatory lesions is not possible.
Filling the colonic lumen with water alters these lim-iting factors in bowel evaluation by clarifying the visual-
Table 2. Number of cases and sites of involvement of neoplastic and inflammatory colonic lesions according to the final diagnosis
a The ileocecal region was the most common site of tuberculous involvementb Malignant lesions were most common at the rectosigmoid junction and sigmoid colon
Table 4. Cases with alterations in wall architecture
Disease Preserved Partiallossa
Completeloss
Echogenicity
Tuberculouslesion
2 6 24 Hypoechoic
Malignant lesion — — 16 Heterogeneous/hypoechoic
Ulcerative colitis 7 — 1 Hypoechoic
a With disruption of the third echogenic layer
500 R. Dixit et al.: Hydrocolonic sonograhy in colonic lesions
Fig. 2. A Barium enema shows a long segment stricture with smooth tapered ends, sug-gestive of a benign stricture involving the descending colon.B HCS demonstrates moder-ate concentric hypoechoic wall thickening with complete loss of layering and loss ofhaustra in the descending colon, extending over a long segment. Pericolonic connectivetissues appear normal (excision biopsy, tuberculosis).
Fig. 3. A Barium enema demonstrates eccentric narrowing at the rectosigmoid junctionwith mucosal irregularity and shouldering, consistent with a malignant stricture.B HCS ofthe same patient shows a heterogeneous intralumenal mass at the rectosigmoid junction(M, mass;R, rectum;SIG, sigmoid) almost obliterating the lumen. Wall layering at thebase is lost, with extension beyond the colonic wall into pericolonic tissues (carcinoma atthe rectosigmoid junction).
Fig. 4. A Double contrast barium enema (DCBE) of a patient shows fine mucosal ulcerations and loss of haustral pattern involving the entirecolon, findings suggestive of ulcerative colitis.B HCS of the same patient shows only mild wall thickening with preserved wall layering;prominent, lumenally situated second hypoechoic layer and loss of haustral pattern; and normal surroundings, suggestive of ulcerative colitis.
R. Dixit et al.: Hydrocolonic sonograhy in colonic lesions 501
ization of both the colonic lumen and its wall stratification[9–12]. With this technique as opposed to barium studiesand colonoscopy, both mural and lumenal diseases can beevaluated properly.
On HCS, the colonic wall shows five layers of differ-ent echogenicity that correspond to anatomic layers, i.e.,layers 1 and 2 represent the mucosa, layer 3 the submu-cosa, layer 4 the muscularis propria, and layer 5 the serosa
Fig. 5. Left Barium enema shows a small rounded filling defect at the rectosigmoid junction(polyp). Right HCS of the same patient shows a small sessile intralumenal projection with intactwall layering at the base, located at the rectosigmoid junction (colonic polyp). HCS also detectedanother small polyp in the sigmoid colon (not shown).
Fig. 6. Left Barium meal follow through (FT) shows a stricture terminal ileum with a deformedileocecal junction and contracted cecum, suggestive of ileocecal tuberculosis.Right HCS of thesame patient shows involvement of the ileocecal junction with hypoechoic, moderate wall thick-ening in the region of the cecum and terminal ileum, in addition to loss of wall layering but intactserosa (biopsy demonstrated tuberculosis).
Fig. 7. A Barium enema demonstrates narrowing of the upper descending colon with mucosal ulcerations.B HCS shows moderate hypoechoic wallthickening with a nearly complete loss of wall stratification and associated lumenal narrowing and loss of haustration. Pericolonic connective tissuesappear normal (chronic granulomatous colitis).
502 R. Dixit et al.: Hydrocolonic sonograhy in colonic lesions
and subserosal fatty tissue [13]. Thus, HCS enables adegree of accuracy in the evaluation of bowel structurethat has been achieved thus far only by endolumenalsonography [14, 15].
The present study group consisted of a heterogeneousspectrum of disorders, and the characteristic changes inwall thickness, echogenicity, stratification, and lumenalchanges on HCS in association with the site and length ofinvolvement were highly suggestive of the etiology inmost cases.
Granulomatous colitis of tuberculous etiology was themost common lesion detected, with the ileocecal regionas the most frequent site of involvement (87.5%; Fig. 6),and female the sex usually involved. On HCS, it waspossible to diagnose and localize 30 of 32 (93.75%) casesof granulomatous tuberculous colitis correctly. In thesecases, the colon presented a clearly thickened (average58.34 mm) echo-poor bowel wall with mostly total (75%)and sometimes partial (18.7%) loss of wall stratification(Fig. 7). These findings are not unique to tuberculosis andare similar to those described for Crohn disease [9, 12,16]. No literature is available on the evaluation of tuber-culosis with this technique.
The partial loss of stratification with disruption of thethird echogenic layer (the submucosa) may be explainedby the origin of the tuberculous granuloma in the submu-cosal layer. Pathologically, after penetration of theMy-cobacteriumthrough the mucosa, the initial response is alocalized acute inflammation in the lymphoid tissues ofthe submucosa. After 2–3 weeks, a tubercle with epithe-loid cells forms, which undergoes caseous necrosis 2–4weeks later, and fibrous scarring may develop.
The second largest group of disorders consisted ofmalignant lesions, with 15 cases of primary carcinoma ofthe colon and one case of non-Hodgkin’s lymphoma. Ofthese malignant lesions, all were correctly localized, butone (6.25%) was misinterpreted as a benign stricture.
Malignant lesions showed heterogeneous intralume-nal masses, with loss of wall architecture at the base ofthe lesion in 87.5% cases (Fig. 8). The wall thickening inmalignant lesions was gross (average5 25.3 mm), withtotal loss of wall stratification and heterogeneous/hypo-echoic echo texture. Twelve cases (75%) showed exten-sion of disease into pericolonic connective tissues (Fig. 9)on HCS. Of the 15 cases of primary carcinoma of thecolon, eight had surgery. Two of these did not haveextension of disease beyond the adventitia either on HCSor on histopathology. Of the six surgical cases that ap-peared to have extension beyond the adventitia on HCS,all six showed extension into pericolonic tissues at sur-gery. The rest of the cases did not have surgery.
It has been previously reported that the diagnosis ofcolonic carcinoma can be suggested based on the sono-graphic evidence of an intralumenal mass fixed to thewall, a lesion within the wall, and invasion of surroundingconnective tissues. Du¨x et al. [17] reported a sensitivity of
73% in the diagnosis of colorectal carcinoma when HCSwas done without bowel preparation and rectal evaluationwas included in the study, whereas Limberg [11] reporteda sensitivity of 97% in the detection of colorectal malig-nancy when HCS was done after bowel preparation andrectal evaluation was not included in the study. Detailedevaluation of the colonic wall also helps in the accuratestaging of malignancy [10, 11, 17, 18]. Staging was notattempted in the present study because not all patients hadsurgery: either the case was inoperable or the patientrefused surgery. A diagnosis of lymphoma was suggestedin a patient who had gross, lobulated, eccentric, longsegment hypoechoic wall thickening but no intralumenalmass. Ultrasound-guided FNAC from this bowel massshowed non-Hodgkin’s lymphoma (Fig. 10).
The single malignant stricture that was misinter-preted as benign had only moderate hypoechoic wallthickening with no intralumenal mass and normal peri-serosal connective tissues. This patient had a mucin-secreting adenocarcinoma diffusely infiltrating thecolonic wall in the rectosigmoid region but no intralu-menal projections. We diagnosed it as an inflammatorystricture, thereby emphasizing that the technique can-not always distinguish between a benign and malignantlesion confined to the colonic wall. The high sensitivityin the detection of colonic malignancy in the presentstudy is due in part to advanced cases and exclusion ofrectal lesions.
Eight cases of ulcerative colitis comprised the thirdlargest group. In patients with inflammatory bowel dis-ease such as ulcerative colitis, conventional sonography,although of value in the detection of complications, al-lows only a rough estimate of the extent of disease. Incontrast, HCS allows detailed evaluation of inflammatorybowel disease. In the present study, patients with ulcer-ative colitis showed mild wall thickening with preservedwall stratification in 87.5% of cases. In one case withextensive pseudopolyposis, the wall stratification was lostover a very long segment of colon, which was misinter-preted as granulomatous colitis. Because of mild wallthickening over a long segment of colon, the possibility ofmalignancy was not considered. These findings are inagreement with those of previous studies [9, 12, 18]. Thepreserved wall stratification, which distinguishes ulcer-ative colitis from granulomatous colitis in most cases,was seen in these studies and in the majority of cases(seven of eight) in the present study. The structuralchanges demonstrated by HCS correspond well with find-ings obtained by computed tomography. In patients withCrohn disease, a homogeneous wall thickening was foundon computed tomography; in patients with ulcerative co-litis, only moderate wall thickening with recognizablestratification could be seen [19, 20].
Although the changes due to ulcerative colitis are welldocumented by HCS, the extent of colonic involvement wasunderestimated as compared with colonoscopy, which can
R. Dixit et al.: Hydrocolonic sonograhy in colonic lesions 503
Fig. 8. A Barium enema demonstrates an eccentric short segment narrowing at the rectosig-moid junction with evidence of shouldering.B HCS shows a broad-based polypoid projec-tion at the rectosigmoid junction. Wall stratification at the base of the lesion is not clearlyvisible here but is clearly visible in the sigmoid. Findings suggest carcinoma of the rectosig-moid junction.
Fig. 9. A Barium enema demonstrates abrupt, complete obstruction to the passage of bariumin the sigmoid colon, with a polypoid filling defect at the apex of the obstruction.B HCSshows gross hypoechoic wall thickening with a polypoid intralumenal projection causingcomplete obliteration of the lumen. Wall layers in the normal colonic wall can be distin-guished but are completely lost in the abnormal bowel segment. The bright line of adventitiaalso is not visible in the region of the mass.
Fig. 10. A Barium enema of an adolescent male demonstrates a long stricture of the de-scending colon, with no mucosal irregularity.B Transverse section of the fluid-distendeddescending colon shows gross lobulated wall thickening with loss of the normal layeringand associated lumenal narrowing and hypoechoic echotexture. Pericolonic tissues are nor-mal (non-Hodgkin’s lymphoma).
504 R. Dixit et al.: Hydrocolonic sonograhy in colonic lesions
detect very early mucosal lesions. This finding is also inagreement with that of previous studies [9, 12, 18].
The miscellaneous group included colonic polyps,nonspecific inflammatory strictures, diverticulosis (twocases), and an extrinsic mass (four cases). Of these,diverticulosis and nonspecific inflammatory stricturecould not be detected by HCS, and a false-positivediagnosis of colonic polyp was made in two cases,indicating that small polyps (,7 mm) cannot be reli-ably diagnosed by HCS.
Hence, HCS was found to have an excellent sensitiv-ity of 90.9% and a specificity of 94.7%, which are com-parable to those of studies by Limberg [9–12].
Conclusions
HCS by overcoming the technical limitation of con-ventional sonography greatly improves the sensitivityand specificity of sonography in the detection of co-lonic lesions. As compared with barium studies andcolonoscopy, this technique allows detailed evaluationof the colonic lumen, wall, and surrounding connectivetissues, which allows better evaluation of both intrinsicand extrinsic lesions and of lesions infiltrating beyondthe adventitia. In cases of narrow stenosis, it allowsdetailed evaluation of the entire stricture and of theproximal colon, unlike colonoscopy, which cannot benegotiated beyond an obstruction.
The technique does have limitations. The visualiza-tion of redundant parts of the colon is poor by thistechnique, and in very obese patients and in patientswith excessive bowel gas colonic visualization may notbe adequate. The rectum cannot be evaluated with thistechnique, and this is a serious limitation because alarge number of colorectal cancers occur in the rectum.Definite distinction between benign and malignant le-sions is not always possible. The extent of inflamma-tory lesions is also underestimated as compared withcolonoscopy.
Although the procedure of HCS is cumbersome andcauses some discomfort to the patient, it can be usedadvantageously for the diagnosis and differential diagno-sis of colonic lesions in selected cases.
References
1. Lutz HT, Petzold R. Ultrasonographic patterns of space occupyinglesions of the stomach and intestine.Ultrasound Med Biol1976;2:129–132
2. Holt S, Samuel E. Grey scale ultrasound in Crohn’s disease.Gut1979;20:590–595
3. Worlicek H, Lutz H, Heyder N, et al. Ultrasound findings inCrohn’s disease and ulcerative colitis: a prospective study.J ClinUltrasound1987;15:153–163
4. Bluth El, Merritt CRB, Sullivan MA. Ultrasonic evaluation of thestomach, small bowel and colon.Radiology1979;133:677–680
5. Bluth El. Ultrasound evaluation of small bowel abnormalities.Am JGastroenterol1983;78:788–793
6. Fakhry JR, Berk RN. “The target pattern” characteristic sono-graphic feature of stomach and bowel abnormalities.AJR1981;137:969–972
7. Fleischer AC, Muhletaler CA, James AE Jr. Sonographic patternsarising from normal and abnormal bowel.RCNA1989;18:145–159
8. Fleischer AC, Muhletaler CA, James AE Jr. Sonographic assess-ment of the bowel wall.AJR1981;136:887–891
9. Limberg B. Diagnosis of acute ulcerative collitis and colonicCrohns disease by colonic sonography.J Clin Ultrasound1989;17:25–31
10. Limberg B. Diagnosis of large bowel tumours by colonic sonogra-phy. Lancet1990;335:144–146
11. Limberg B. Diagnosis and staging of colonic tumours by conven-tional abdominal sonography as compared with Hydrocolonicsonography.N Engl J Med1992;327:65–69
12. Limberg B, Osswald B. Diagnosis and differential diagnosis ofulcerative colitis and Crohn’s disease by hydrocolonic sonography.Am J Gastroenterol1994;89:1051–1057
13. Kimmey MB, Martin RW, Haggitt RC, et al. Histologic correlatesof gastrointestinal ultrasound images.Gastroenterology1989;96:433–441
14. Hildebrandt U, Feifel G. Preoperative staging of rectal cancer byintrarectal ultrasound.Dis Colon Rectum1985;28:42–46
15. Tio L, Cohen P, Coene PP, et al. Endosonography and computedtomography of esophageal carcinoma.Gastroenterology1989;96:1478–1486
16. Limberg B. Sonographic features of colonic Crohn’s disease: com-parison of in vivo and in vitro studies.J Clin Ultrasound1990;18:161–166
17. Dux M, Roeren T, Kuntz C, et al. TNM staging of gastrointestinaltumours by hydrosonography: results of a histopathologically con-trolled study in 60 patients.Abdom Imaging1997;22:24–34
18. Hernandez-Socorro CR, Guerra C, Hernandez-Romero J, et al.Colorectal carcinomas: diagnosis and preoperation staging by hy-drocolonic sonography.Surgery1995;117:609–615
19. Gore RM, Marn CS, Kirby DF, et al. CT findings in ulcerativegranulomatous and indeterminate colitis.AJR1984;143:279–284
20. Lubat E, Balthazar EJ. The current role of computerized tomogra-phy in inflammatory disease of the bowel.Am J Gastroenterol1988;83:107–113
R. Dixit et al.: Hydrocolonic sonograhy in colonic lesions 505