A. Videnovic , MD (*) Department of Neurology , Northwestern University, Parkinson’s Disease and Movement Disorders Center , 710 N Lake Shore Drive, Suite 1106 , Chicago , IL 60611 , USA e-mail: [email protected]
K. M. Shannon , MD Department of Neurological Sciences , Rush University Medical Center , 1725 W Harrison Street, Suite 755 , Chicago , IL 60612 , USA
This chapter contains videos segment which can be found at the URL: http://www.springerimages.com/Suchowersky
Video Segment Content
Case 1: Huntington disease.A 65-year-old right-handed woman presented with progressive involuntary movements beginning at age 58. She also complained of unsteadiness and several near-falls. Her family history was not signifi cant for any neurological/psychiatric disease. Her father, however, suddenly disappeared when she was a child. Genetic testing confi rmed that the patient carried the huntingtin mutation. The video demon-strates moderate choreic movements involving her face, hands and feet. Case 2: Huntington disease—eye movement abnormalities.A 49 year-old right-handed man developed concentration diffi culties and irritability in his early 40’s. Mild chorea subsequently emerged, and genetic testing revealed the huntingtin mutation with 48 CAG repeats. His father was found to have a hun-tingtin premutation with 34 CAG repeats. The patient has a child with juvenile Huntington disease. The video shows slowing and delayed initiation of horizontal and vertical saccades, associated with suppressible head jerks. These eye movement abnormalities are considered an early clinical sign of Huntington disease. Case 3: Huntington disease.A 50 year-old women developed involuntary movements of her feet in her early 40’s. Her family history was unremarkable. After ruling out non-genetic causes of chorea she had genetic testing, and was diagnosed with Huntington disease. The video demonstrates choreic movements of her feet.
The patient subsequently obtained an old family video, involving several family members, including her mother. In the fi rst video segment, she can be seen descend-ing the stairs with another woman. She is dressed in blue and appears to the viewer’s right. In the second video segment, she is seated, again wearing blue and to the viewer’s right. Generalized choreiform involuntary movements, dystonia, especially of her right arm, and unsteady gait are demonstrated in the video.
Case 4: Huntington disease—Westphal variant.A 6-year old girl had learning diffi culties and delayed motor milestones since early childhood. Based on these symptoms she was diagnosed with mild cerebral palsy. During her childhood her paternal grandfather was diagnosed with Huntington disease. This prompted extensive genetic testing among family members. She was diagnosed with juvenile Huntington disease, carrying a huntingtin mutation with 75 CAG repeats. The fi rst video segment demonstrates generalized dystonia and par-kinsonism. Her symptoms progressed rapidly. The second video segment shows her four years later. At that time, she was bed bound, severely dysarthric with mild myoclonus and truncal choreic movements. Case 5: Neuro-acanthocytosis.A 45-year old man presented with a two-year history of memory decline and gener-alized involuntary movements. He subsequently developed dysphagia and dysar-thria. Involuntary tongue movements, mainly protrusions, made his feeding diffi cult, and he started to loose weight. The video shows generalized chorea, oro-madibular dystonia, dysarthria with drooling, and dystonia mainly present in lower extremi-ties. Genetic testing for huntingtin mutation was negative. Peripheral smears showed acanthocytes, supporting the diagnosis of neuro-acanthocytosis. The patient required feeding tube placement, and died 10 years after disease onset from aspira-tion pneumonia. Case 6: Sydenham’s chorea.A 7-year old African American boy developed clumsiness, slurred speech and unsteadiness 4 weeks ago. Fidgety involuntary movement initially appeared in his hand, and subsequently spread to his whole body. Family history was negative. Extensive medical work-up at an outside institution was negative, and a diagnosis of possible juvenile Huntington disease was made. Subsequent work-up showed an elevated anti-streptolysin O titer (270; normal <200), and an echocardiogram revealed mild mitral insuffi ciency. The diagnosis of Sydenham’s chorea was made. Choreic movements were successfully treated with valproic acid and haloperidol. He was started on penicillin prophylaxis. The video shows generalized chorea, clumsiness, motor impersistance, and ataxia. Case 7: Hemiballism.A 30 year-old right-handed man presented with involuntary movements of his right arm. The movement initially emerged a few weeks ago, and gradually became more intense. He experienced generalized malaise and lost 10 lbs over a few months prior to the onset of involuntary movements. General physical examination was signifi -cant for neck and axillary lymphadenopathy. Neurological examination showed fl ailing, large amplitude involuntary movements of the right arm, typical of hemibal-lism. Brain MRI showed increased signal on T2 and FLAIR sequences in the left basal ganglia region. He tested positive for HIV. A treatment with anti-retroviral regimen was initiated, and his movements gradually improved. Case 8: Choreiform dyskinesias in Parkinson disease.A 37-year old right-handed man developed right hand rest tremors and stiffness at age 30. He was subsequently diagnosed with Parkinson’s disease, and treated with
252 Huntington Disease and Other Choreas
carbidopa/levodopa. Approximately seven years later he developed generalized involuntary movements. The video shows generalized choreiform movements, typi-cal for dyskinesias occurring in the context of chronic therapy with carbidopa/levodopa. Case 9: Huntington’s disease - gait abnormalitiesA 45-year old woman developed generalized fi dgety movements at age 33. Her twin sister developed similar movements at age 38. Genetic testing confi rmed the huntingtin mutation. Their father died at age 63, and had an unspecifi ed mental illness. The video shows characteristic gait of HD. The gait is wide-based, with lurching, dipping, and hesitations.
Chorea
Introduction and Historical Perspective
In the whole range of medical terminology, there is no such olla podrida as Chorea, which for a century has served as a sort of nosological pot into which authors have case indiscrimi-nately affections characterized by irregular, purposeless movements [ 1 ] .
The term chorea is derived from the Latin word “choreus,” which means dancing. The origins of its use date back in the middle ages. Paracelsus used the term Chorea Sancti Viti to describe epidemic disorders of motion among Europeans. These danc-ing rituals were often linked to prominent saints, one of which was Saint Vitus [ 2 ] . The term “Saint Vitus Dance” was used to describe chorea of all types for many centuries. Thomas Sydenham confused the classifi cation when he used chorea in 1686 to describe a postinfectious movement disorder in children [ 3 ] . Thereafter, postinfectious childhood chorea was called chorea minor, and other choreas, includ-ing the dancing manias, were called chorea major. The link between rheumatic fever and chorea was not recognized until 1831 [ 4 ] . Huntington disease was named after George Huntington, who provided the fi rst detailed description of this familial cho-rea in 1872 [ 5 ] . Neuroacanthocytosis, also known as the Levine–Critchley disease, was initially reported in 1963 [ 6 ] . Since the initial descriptions of chorea, many new clinical entities characterized by chorea have been described, and our understanding of its pathophysiology has widely expanded.
Defi nition and Clinical Manifestations
Chorea is a hyperkinetic movement disorder consisting of involuntary, brief, rapid, purposeless, irregular, nonrhythmic movements that fl ow from one body part to another. Involuntary movements may involve all body parts and occasionally have a hemibody distribution (hemichorea). Frequently, milder movements may resemble
26 A. Videnovic and K.M. Shannon
restlessness or fi dgeting. Choreic movements may be partially suppressed or incor-porated into semipurposeful movement, a phenomenon named parakinesia. Motor impersistence, an inability to maintain a sustained contraction, is another frequent clinical feature of chorea, often referred to as “negative chorea.” Examples of motor impersistence are the darting tongue sign, an inability to keep tongue protruded, and the milkmaid’s grip, defi ned as inability to maintain continuous handgrip.
Ballism (from Greek, “to throw”) is a large amplitude choreiform movement involving the proximal segments of the limb. Chorea may be accompanied by athetosis, slow, writhing, sinuous involuntary movements of the distal limbs, mainly the arms. The term choreoathetosis is often used to describe the coexistence of chorea and athetosis. In some conditions, other involuntary movements, such as dystonia, tics, tremors, or myoclonus, may coexist with chorea as well.
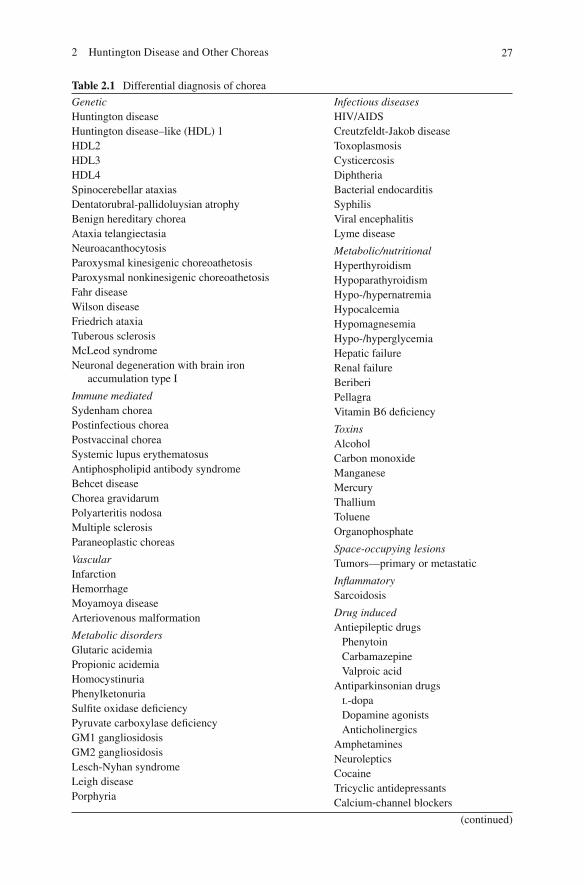
Differential Diagnosis
The differential diagnosis of chorea is broad and encompasses many different causes, including neurodegenerative diseases, genetic mutations, infections, auto-immune disorders, cerebrovascular disease, neoplasms, metabolic derangements, and drug exposures (Table 2.1 ).
Genetic Choreas
Huntington Disease
Epidemiology
Huntington disease (HD) is an autosomal dominant, progressive neurodegenerative illness affecting motor function, cognition, and behavior. The highest prevalence is among the population of Lake Maracaibo in Venezuela. Its estimated prevalence in the USA is 2–10/100,000 [ 7– 9 ] . European prevalence ranges from 5 to 10/100,000. HD is very rare in Africa and almost absent in Asia [ 10 ] . There is no gender predis-position for the development of HD. Age of onset varies from early childhood to late 80s. Peak age of onset is in the 40s and 50s. Juvenile HD cases have onset before age 21 and represent 5.4% of all HD cases [ 11 ] . Juvenile-onset patients inherit the disease mostly from the father [ 12 ] and have high cysteine-adenosine-guanine (CAG) repeat lengths [ 13, 14 ] . Older age of onset is associated with mater-nal transmission of the HD gene. The rate of progression correlates with age of onset and number of CAG repeats but varies greatly, even within families [ 15 ] . Average duration of the illness from onset is 15–17 years. The juvenile cases prog-ress more rapidly with average disease duration of 10 years [ 16 ] .
The clinical triad of HD includes chorea, psychiatric/behavioral disturbances, and cognitive decline. Initial HD symptoms of HD vary widely. Motor signs are present in about 60% of new cases, behavioral problems in 15%, and combination of these two in 25% of cases [ 17 ] .
The motor disorder of HD is severely disabling and combines involuntary move-ments, abnormal control of ocular movements, and derangements of volitional move-ments. Chorea is the most common involuntary movement in patients with HD. Patients are often not aware of the involuntary movements, and these are usually noted by family and friends. Mild chorea is often perceived as clumsiness, and many patients or family members relate a long history of fi dgetiness and jerkiness. Other motor signs include bradykinesia, irregular or clumsy movement, motor impersistence, and dystonia. Subtle motor changes, such as slowing in reaction and movement time [ 18 ] , can be detected in presymptomatic stages of the disease [ 19 ] .
The oculomotor system becomes involved early in the disease process. Delayed initiation and slowing of volitional saccades are one of the earliest clinical signs [ 20, 21 ] . Pursuit eye movements may show saccadic intrusions. Test such as sacca-dometry and a cognitively demanding oculomotor task may be useful as an indica-tor of function in HD [ 22, 23 ] . With progression, eye blinks or head jerks may be required to initiate saccades.
With advancing disease, gait is wide based, with lurching, dipping, bobbing, and frequent falls. Chorea tends to diminish as parkinsonism and dystonia emerge. With further disease progression, swallowing deteriorates and weight loss occurs [ 24 ] . Aspiration pneumonia is common in advanced disease and represents a signifi cant cause of morbidity and mortality. As with other conditions that cause severe motor disability, pneumonia and cardiovascular disease are the most common terminal events [ 25 ] .
The Westphal variant of HD describes an akinetic/dystonic syndrome, usually seen in younger patients. Young-onset HD has distinct phenotype and manifests with parkinsonism, dystonia, myoclonus, dementia, ataxia, and seizures [ 26 ] .
Mood and personality disorders, as well as cognitive decline, may precede motor symptoms of HD [ 27 ] . Neuropsychiatric symptoms are present in 98% of patients [ 27, 28 ] . Irritability and aggressive behavior are frequently present for many years
before the onset of motor symptoms. Other common behavioral problems in HD include personality changes, agitation, impulsiveness, anxiety, mania, apathy, social withdrawal, and sexual disorders. Affective disorder, especially depression, is very common. HD increases suicide risk; suicide is responsible for 7.5% of all deaths in the HD population [ 29 ] . Suicide risk is highest around the time of symptom onset and when the disease fi rst starts to affect aspects of daily living, such as driving and working [ 30 ] . Gene carriers are also at increased risk of suicide [ 26 ] . Subclinical obsessive and compulsive symptoms are present in individuals with prediagnosed HD [ 31 ] . These individuals frequently have obsessive worrying and checking, mainly related to their cognitive errors. Less common but very disabling behavioral changes include paranoia, delusions, hallucinations, and psychosis.
Symptoms of executive dysfunction are early signs of cognitive decline in HD and are related to the abnormalities in the frontostriatal networks [ 32 ] . Common early signs include inattention and planning and organizational diffi culties. Visuospatial processing is affected in patients with HD and deteriorates more rap-idly than memory [ 33 ] . Subtle cognitive changes may interfere with gainful employ-ment or driving even before the diagnosis of HD is considered. Cognitive changes and irritability are also common in “asymptomatic” gene carriers prior to onset of motor symptoms [ 34 ] .
Genetics
HD belongs to a family of neurodegenerative poly-Q disorders. It is caused by an unstable expanded CAG trinucleotide repeat in the IT15 (huntingtin) gene located at the tip of the fourth chromosome (4p16.3) [ 35 ] .
The huntingtin gene codes for the protein huntingtin. Normal huntingtin alleles have fewer than 27 CAG repeats. Individuals who carry alleles with 27–35 CAG repeats have a premutation, and although they will not develop HD during their life-time, their offspring are at increased risk due to the unstable nature of the repeat expansion. These intermediate-size alleles are most prone to instability during pater-nal transmission. Alleles with 36–39 CAG repeats are incompletely penetrant. Completely penetrant disease is associated with 40 or more CAG repeats. While some studies do not suggest a correlation between the length of CAG repeats and the rate of HD progression [ 36 ] , others do, particularly in young-onset disease [ 16, 37– 40 ] .
While there is an inverse correlation between the CAG repeat length and the age at onset, the repeat length contributes only about 50% of the variance in age at onset. Other genetic factors as well as shared and unshared environmental infl u-ences contribute the remainder of variance in age at onset [ 41 ] . The phenomenon of anticipation, earlier onset of disease in subsequent generations, is attributable to the instability inherent in trinucleotide repeat disorders [ 11, 14, 42, 43 ] . Instability depends both on the gender of the affected parent and the parent’s repeat length with increased instability when the transmitting parent is the father and the CAG repeat length is longer [ 43 ] . Juvenile-onset cases, generally associated with repeat lengths greater than 50, most often (>90%) have an affected father [ 13, 14 ] .
30 A. Videnovic and K.M. Shannon
Pathology
The neuropathological hallmark of HD is a marked atrophy of the neostriatum, more prominent in caudate than in putamen [ 44 ] . Medium-sized spiny striatal neu-rons are most susceptible to degeneration in HD. Neuronal loss and gliosis are also present in the cerebral cortex, involving predominantly frontal lobe neurons in lay-ers III, IV, and V. The severity of neuronal loss correlates with the length of CAG repeats [ 42 ] . Vonsattel et al. have developed a semiquantitative histopathologic grading system, with grades ranging from 0 (no neuronal loss) through 4 (95% loss of striatal neurons) [ 44 ] .
Pathogenesis
Huntingtin is widely expressed in the brain and is necessary for developing and sustaining normal brain function. Mutant huntingtin is found in both affected and unaffected regions of the HD brain. Mutant huntingtin has an expanded polyglu-tamine stretch that correlates with CAG repeat length. The mutant protein is resistant to proteolysis and forms aggregates containing ubiquitin, proteasome components, and other intracellular proteins [ 45 ] . Studies in endemic populations show that car-riers of two mutant alleles have a similar phenotype to heterozygotes, suggesting that the mutant protein causes a toxic “gain of function.” Like other neurodegenera-tive diseases characterized by protein aggregation, misfolded protein stress doubt-less contributes to neurodegeneration. However, recent studies suggest that cleavage of mutant huntingtin by caspase 6 is important in the specifi c neurotoxicity of the mutant protein and in the development of nuclear inclusions [ 46 ] . Studies in trans-genic mice in which the mutant gene can be turned off show that blocking expres-sion of the mutant gene leads to the disappearance of neuronal inclusions and improvement in behavioral abnormalities [ 47, 48 ] . Detailed studies of the intracel-lular consequences of mutant huntingtin suggest many different potentially patho-genic processes including interference with the normal function of Huntington, inhibition of ubiquitin-dependent proteasomal proteolysis [ 49 ] , oxidative stress with free-radical toxicity [ 50 ] , glutamate toxicity [ 51, 52 ] , caspase activation [ 53– 57 ] , mitochondrial dysfunction [ 58, 59 ] , interference with DNA transcription, and decreased neurotrophic support [ 60 ] . The role of polyglutamine aggregates in the neurotoxicity remains unclear [ 61 ] . While some investigators think that they are deleterious, others view them as an adaptive response or even neuroprotective.
Diagnostic Work-Up
HD is diagnosed based on the typical clinical manifestations in conjunction with positive family history and confi rmatory genetic testing. Many typical patients do not have a confi rmed family history of HD, though the clinician’s suspicions should be raised when there is a history of early death or disappearance, suicide or accidental death, prominent behavioral changes, or another neurological or psychiatric
312 Huntington Disease and Other Choreas
diagnosis in a parent or sibling. Up to 3% of patients with clinical manifestations suggestive of HD do not have the disease. Several HD-like diseases have been recently described in some HD gene-negative patients.
Neuroimaging
Brain imaging studies in patients with HD may show atrophy of the caudate, puta-men, or whole brain. SPECT and PET scans demonstrate hypometabolism and reduced blood fl ow in the basal ganglia. These changes are present even in the pre-symptomatic stages of HD [ 62– 64 ] . Voxel-based morphometry MRI reveals reduced gray matter volume in the left striatum, bilateral insula, dorsal midbrain, and bilat-eral intraparietal sulcus in presymptomatic gene carriers. This novel imaging tech-nique may be useful in distinguishing HD gene-positive asymptomatic patients from gene-negative individuals and has a potential role following disease progres-sion over time [ 65, 66 ] . A signifi cant reduction of functional anisotropy has been recently demonstrated on cerebral diffusion tensor imaging (DTI) in individuals with HD [ 67 ] .
Electrophysiology
Electrophysiological testing in early stages of HD reveals abnormal cortical soma-tosensory-evoked potentials (SSEPs) in 94% of patients. This technique is however not routinely used for the diagnostic purposes.
Genetic Testing
Genetic testing for HD has been available since 1993 and represents the most cost-effective fi rst step in the diagnostic process. The test is used to confi rm the diagnosis in a clinically affected person or identify presymptomatic gene-positive carriers. Prenatal testing is available as well. The demand for testing of individuals at risk is not as high as initially expected. Presymptomatic testing for HD has signifi cant medical, psychological, ethical, legal, and fi nancial implications for the tested indi-vidual and family. Individuals with limited social networks are particularly vulner-able to detrimental effects of unfavorable genetic testing [ 68 ] . Due to these implications, genetic testing protocols have been developed to include neurologic, genetic, and psychologic counseling before and after testing.
Treatment
The unique feature of HD is that the diagnosis can be made early in the course of the disease and even in the presymptomatic stage. Therefore, signifi cant research efforts are focused on the development of therapies that might modify the course of HD. Although many chemical compounds have shown promise in animal models
32 A. Videnovic and K.M. Shannon
of HD, no agent has been shown to modify the disease. Coenzyme Q10 is the best-studied potential agent in the HD population. An initial pilot study of CoQ10 showed daily doses up to 1,200 mg were well tolerated [ 69 ] . A multicenter, plac-ebo- controlled, randomized clinical trial sponsored by the HSG compared CoQ10 and remacemide (NMDA ion channel blocker) with placebo in a 2 × 2 factorial design in 347 subjects with manifest HD [ 70 ] . At 30 months, there was no differ-ence in the decline in total functional capacity, a global measure. Adverse effects included stomach upset in the CoQ10 group and nausea and vomiting in the rema-cemide group. A study of higher dose of CoQ10 (2CARE study) is currently being developed by the Huntington Study Group. The glutamate antagonist riluzole was found to be well tolerated by HD subjects in a placebo-controlled clinical trial. Riluzole-treated subjects showed improved chorea severity, without improved total functional capacity. Treatment was complicated by elevations of liver transami-nases [ 71, 72 ] . Minocycline, an antibiotic with anti-infl ammatory and anticaspase effects, was safe and well tolerated but showed no effect on any of the clinical outcomes [ 73– 75 ] . A multicenter, double-blind, placebo-controlled trial of ethyl eicosapentaenoate, an unsaturated fatty acid concentrated in fi sh oil, failed to alter the decline in motor scores in subjects with HD, but exploratory analyses showed slowed decline or stability of motor scores in those subjects who took the experi-mental agents per protocol [ 76 ] . A larger multicenter, double-blind, placebo-controlled, randomized study of ethyl eicosapentaenoate (ethyl-EPA) in subjects with mild to moderate HD (TREND-HD) did not demonstrate benefi ts of ethyl-EPA in this study population [ 77 ] . A placebo-controlled trial of creatine supple-mentation at doses 5 g/day did not improve functional status in patients with early HD, but the study was underpowered to detect any but a very robust result [ 78 ] .
Therapeutic interventions in HD focus on symptomatic treatment of motor, behavioral, and psychiatric disturbances. There are no FDA-approved medications for the symptoms of HD, so therapy is primarily based on anecdotal reports and small case series and employs off-label use of medications. Chorea usually improves with antidopaminergic medications such as dopamine antagonists or depleters. There is some support in the literature for treatment of chorea with typical and atypi-cal neuroleptics. Concern about side effects of typical neuroleptics (decline in cog-nition and motor function, impaired swallowing) has increased popularity of atypical agents, though evidence for better effi cacy or tolerability is not yet available. Neuroleptics may be particularly useful in patients who have concomitant psychosis or aggressive behavior. Tetrabenazine binds to the vesicular monoamine transporter (VMAT2), depleting monoamines and serotonin from presynaptic central nervous system neurons. Dopamine is most affected. Tetrabenazine is a popular antichorea agent in Europe, where it has been available for decades. In August 2008, the FDA approved tetrabenazine use for HD-related chorea in the United States [ 79 ] . A recent double-blind, placebo-controlled, multicenter study showed tetrabenazine up to 100 mg/day signifi cantly reduced chorea severity and improved global HD mea-sures [ 80, 81 ] . Tetrabenazine exhibits long-term therapeutic effects as an antichorea agent [ 82, 83 ] . Side effects of tetrabenazine include sedation, depression, akathisia, and parkinsonism. Amantadine, a glutamate antagonist, reduced chorea by 36% at
332 Huntington Disease and Other Choreas
daily doses of 400 mg, in a double-blind, placebo-controlled trial [ 84 ] . Others however did not fi nd similar benefi t [ 85 ] . Successful treatments of dystonia with botulinum toxin injections have been reported in patients with HD [ 86 ] .
Depression in HD responds well to treatment with standard antidepressants. Valproate, carbamazepine, and selective serotonin reuptake inhibitors have been used for the management of mood instability, mania, and irritability. There is con-fl icting evidence on the utility of cholinesterase inhibitors for cognitive impairment in HD, and no study has suggested a substantial benefi t [ 87, 88 ] . Atomoxetine, a norepinephrine reuptake inhibitor, failed to improve self-reported attention and executive function in a recent double-blind, crossover trial in HD [ 89 ] .
Reports on surgical treatments of HD are limited and the number of treated patients is small. Moro et al. reported an improvement of chorea after bilateral pal-lidal deep-brain stimulation [ 90 ] . Pallidotomy has been reported to help severe dys-tonia in a juvenile case [ 91 ] . Porcine striatal implantation did not improve functional status in 12 patients with HD [ 92 ] . Several reports on transplantation of fetal striatal cells failed to document sustained benefi ts [ 93– 96 ] .
Sleep initiation and maintenance diffi culties are common in the HD population. Education about proper sleep hygiene with the use of clonazepam, trazodone, or amitriptyline is a helpful strategy for the management of sleep disturbances. Management of disturbed sleep/wake cycles in HD may result in improved cogni-tive function and apathy in this population [ 97 ] .
Physical, occupational, and speech therapies should be integrated with other treatment modalities.
Dentatorubral-Pallidoluysian Atrophy (DRPLA) (Haw River Syndrome)
Dentatorubral-pallidoluysian atrophy (DRPLA) is an autosomal dominant neurode-generative disorder resulting from an unstable trinucleotide CAG repeat in a gene on chromosome 12. The DRPLA gene encodes atrophin-1, a protein with unknown function. The length of the CAG repeat expansion is inversely correlated with the age of disease onset [ 98 ] and may have a considerable effect on the disease milestones and prognosis in DRPLA patients [ 99 ] . The disease is rare in Caucasians and more prevalent in Japanese population (0.7/100,000 people) [ 100 ] . The usual age at onset is in the third or fourth decade, although early-onset cases (age < 20) have been described.
DRPLA has a broad spectrum of symptoms including chorea, myoclonus, epilepsy, ataxia, dystonia, parkinsonism, and dementia. Similar to HD, genetic anticipation is present in DRPLA families.
Neuropathological fi ndings include degeneration of the dentatorubral system, globus pallidus, subthalamic nucleus, striatum, substantia nigra, inferior olive, and thalamus. Signifi cant white matter atrophy has also been described [ 101, 102 ] .
Treatment is symptomatic.
34 A. Videnovic and K.M. Shannon
Neuroacanthocytosis Syndromes
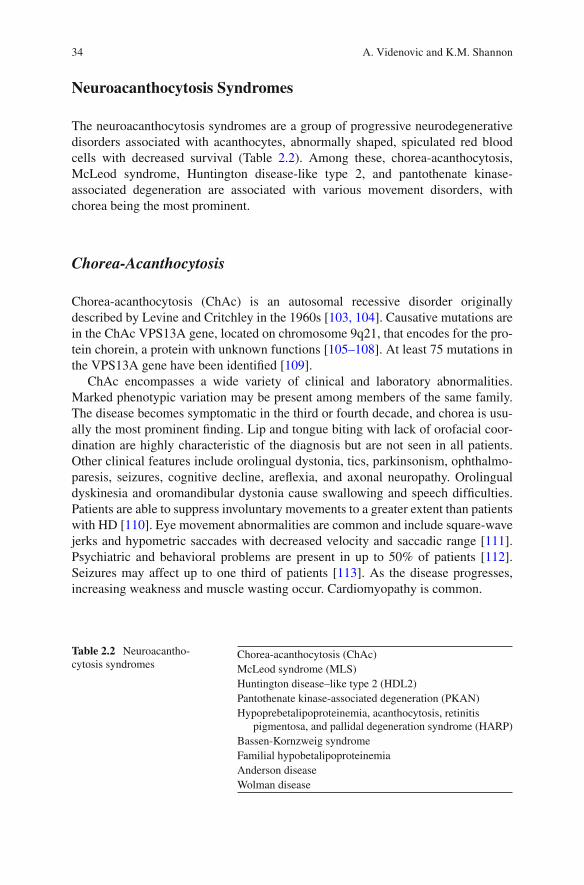
The neuroacanthocytosis syndromes are a group of progressive neurodegenerative disorders associated with acanthocytes, abnormally shaped, spiculated red blood cells with decreased survival (Table 2.2 ). Among these, chorea-acanthocytosis, McLeod syndrome, Huntington disease-like type 2, and pantothenate kinase- associated degeneration are associated with various movement disorders, with chorea being the most prominent.
Chorea-Acanthocytosis
Chorea-acanthocytosis (ChAc) is an autosomal recessive disorder originally described by Levine and Critchley in the 1960s [ 103, 104 ] . Causative mutations are in the ChAc VPS13A gene, located on chromosome 9q21, that encodes for the pro-tein chorein, a protein with unknown functions [ 105– 108 ] . At least 75 mutations in the VPS13A gene have been identifi ed [ 109 ] .
ChAc encompasses a wide variety of clinical and laboratory abnormalities. Marked phenotypic variation may be present among members of the same family. The disease becomes symptomatic in the third or fourth decade, and chorea is usu-ally the most prominent fi nding. Lip and tongue biting with lack of orofacial coor-dination are highly characteristic of the diagnosis but are not seen in all patients. Other clinical features include orolingual dystonia, tics, parkinsonism, ophthalmo-paresis, seizures, cognitive decline, arefl exia, and axonal neuropathy. Orolingual dyskinesia and oromandibular dystonia cause swallowing and speech diffi culties. Patients are able to suppress involuntary movements to a greater extent than patients with HD [ 110 ] . Eye movement abnormalities are common and include square-wave jerks and hypometric saccades with decreased velocity and saccadic range [ 111 ] . Psychiatric and behavioral problems are present in up to 50% of patients [ 112 ] . Seizures may affect up to one third of patients [ 113 ] . As the disease progresses, increasing weakness and muscle wasting occur. Cardiomyopathy is common.
pigmentosa, and pallidal degeneration syndrome (HARP) Bassen-Kornzweig syndrome Familial hypobetalipoproteinemia Anderson disease Wolman disease
352 Huntington Disease and Other Choreas
The diagnosis is based on clinical manifestations, positive family history, and the presence of acanthocytes on the peripheral blood smear (more than 3% of red blood cells). Acanthocytes are usually present in fewer than 50% of specimens in ChAc; therefore, if the suspicion for the disease is high, a dilution test is warranted. Elevated creatine phosphokinase is a common fi nding. Evidence of denervation with fascicu-lations has been noted intermittently on electromyography (EMG).
Brain MRI fi ndings include focal atrophy of the caudate, increased signal in the putamen [ 114 ] , or generalized atrophy with occasional white matter abnormalities [ 115 ] .
Neuropathological fi ndings include neuronal loss and gliosis affecting the stria-tum, pallidum, thalamus, substantia nigra, and anterior horns of the spinal cord [ 116, 117 ] . In contrast to HD, the cerebral cortex is relatively spared. Muscle biopsy reveals neurogenic atrophy, consistent with a possible insult affecting the anterior horn cells or motor axons. Nerve biopsy reveals loss of large myelinated axons. Several abnormalities in the lipid and protein components of red blood cell mem-branes have been identifi ed.
The disease is relentlessly progressive, and no treatment to slow disease progres-sion is available. Self-mutilation behavior may lead to infectious complications; protective devices may be necessary. There are no prospective treatment studies in ChAc. Treatment strategies are mainly extrapolated from experiences in HD. Dopamine antagonists or depleters may improve chorea, and dopaminergic medica-tions are used for the management of parkinsonism. Symptomatic treatment for seizures and systemic complications may be useful. Common causes of death are aspiration pneumonia and complications of cardiomyopathy. Like HD, patients are at increased risk for suicide.
McLeod Syndrome
McLeod syndrome is an X-linked recessive form of neuroacanthocytosis, caused by several different mutations in the XK gene (Xp21) that codes for the XK protein. XK mutations cause reduced expression of Kell erythrocyte antigens.
McLeod syndrome has hematological, hepatological, neuromuscular, and central nervous system manifestations [ 118 ] . The onset of symptoms is in the fourth decade. The spectrum of involuntary movements is broad, including chorea, dystonia, tics, and parkinsonism. Orolingual dyskinesia with self-mutilation is less common than in ChAc. Psychiatric and behavioral symptoms, mainly depression and bipolar dis-order, are common and may be presenting symptoms. Patients are prone to cardio-myopathy and conduction abnormalities. Other manifestations include seizures, motor axonopathy, hemolysis, and liver disease.
Neuroimaging reveals caudate atrophy with white matter abnormalities on T2-weighted MRI [ 115 ] .
Treatment strategies are similar to those applied in ChAc. Special emphasis should be made on the monitoring of heart disease and hemolytic reactions to trans-fusion of mismatched blood.
Pantothenate kinase-associated degeneration (PKAN), formerly known as Hallervorden–Spatz disease, is an autosomal recessive progressive neurodegenera-tive disorder caused by a variety of mutations in the pantothenate kinase 2 (PANK2) gene located on chromosome 20p13. PANK2 is an essential enzyme for coenzyme A biosynthesis, and its dysfunction leads to cysteine accumulation with subsequent iron deposition in the globus pallidus and substantia nigra [ 119, 120 ] . The disorder usually begins in childhood, but adult-onset cases have also been described. Clinical manifestations include chorea, dystonia, dysarthria, rigidity, spasticity, and pigmen-tary retinopathy. Acanthocytosis is mild and not universally present [ 109 ] . The characteristic brain MRI fi nding is the “eye of the tiger sign,” an area of T2 hyper-intensity surrounded by a hypointense rim in the globus pallidus. Treatment is symptomatic.
HARP Syndrome
HARP syndrome, hypoprebetalipoproteinemia, acanthocytosis, retinitis pigmen-tosa, and pallidal degeneration, initially described in 1992, is caused by a mutation of PANK2 [ 121, 122 ] . It belongs to the spectrum of PKAN. Clinical manifestations include oromandibular dystonia, self-mutilation, and chorea.
Huntington Disease-Like (HDL) Disorders
Several disorders that phenotypically resemble HD, but are not associated with HD genotype, have been recently described and named Huntington disease-like disor-ders (HDL).
Huntington disease-like type 1 (HDL1) belongs to a group of prion protein (PrP) diseases. This autosomal dominant disorder is associated with a 192-nucleotide insertion in the prion protein gene on chromosome 20 [ 123 ] . Symptom onset is in the third to fourth decade. Clinical features include chorea, ataxia, rigidity, cogni-tive decline, and seizures. Early psychiatric features are prominent.
Huntington disease-like type 2 (HDL2) is an autosomal dominant disorder caused by a trinucleotide repeat expansion (CTG/CAG) within the gene encoding junctophilin-3 on chromosome 16 [ 124 ] . Due to the limited number of cases, the threshold at which an expansion at the HDL2 locus causes disease remains unknown. Alleles with 43 or more repeats are associated with clinical illness, and alleles with 40–43 repeats are incompletely penetrant. Less is known about alleles with fewer than 39 repeats, but they are believed to have the potential to expand with transmis-sion to incompletely or fully penetrant alleles. The neuropathologic features of HDL2 and HD are very similar but not identical, suggesting that the pathogenetic
372 Huntington Disease and Other Choreas
mechanisms of these diseases may partially overlap [ 125 ] . Nearly all patients have African ancestry. Disease onset is usually in the fourth decade, and survival is usu-ally 10–20 years.
Clinical features include chorea, dystonia, parkinsonism, psychiatric symptoms, and dementia [ 126 ] . Although acanthocytes may be present, they are not as numer-ous as in patients with ChAc and McLeod syndrome [ 127 ] . Brain imaging reveals atrophy of the basal ganglia and cerebral cortex. The diagnosis of HDL2 should be strongly considered in individuals of African descent with an autosomal dominant disorder resembling HD [ 126 ] .
Huntington disease-like type 3 (HDL3) is an autosomal recessive disorder linked to the fourth chromosome [ 128 ] . Disease starts early in life, usually at age 3–4 and is characterized by a wide spectrum of movement disorders including chorea, dys-tonia, myoclonus, ataxia, as well as seizures, cognitive decline, and mutism.
Spinocerebellar ataxia 17 (SCA 17) is an autosomal dominant disorder caused by a CAG/CAA trinucleotide repeat expansion of the TATA-binding protein gene on the sixth chromosome [ 129 ] . The expanded repeat ranges from 47 to 55 triplets in length. SCA 17 may closely resemble HD, and chorea may be the presenting feature [ 130 ] . Other clinical features include pyramidal signs, seizures, and cogni-tive and psychiatric changes [ 131 ] .
Other Genetic Choreas
Wilson Disease
Wilson disease is an autosomal recessive neurodegenerative disorder due to muta-tions in the Wilson disease locus mapped to chromosome 13q14.3. The gene encodes for a copper-binding, membrane-associated, ATPase protein—ATPB7 [ 132 ] . Patients with Wilson disease have a defect of biliary copper excretion, leading to excessive copper accumulation in the liver. Intrahepatic copper damages mitochon-dria, damaging hepatocytes, which spill copper into the systemic circulation. Copper then accumulates in the brain, kidney, erythrocytes, and cornea. Peak disease inci-dence is in the third decade. Initial clinical manifestations may be hepatic, neuro-logic, or psychiatric [ 133 ] . Common neurologic signs and symptoms include dysarthria, dystonia, rigidity, tremor, chorea, and gait dysfunction. Facial dystonia causes the classical lower facial grimace (risus sardonicus). Autonomic disturbances are common. Current guidelines suggest testing patients with liver disease (with or without symptoms) or extrapyramidal features with a past or family history of liver or neurological symptoms [ 134 ] . Routine laboratory work-up includes blood ceru-loplasmin level and 24-h urine copper excretion. A slit-lamp examination should be performed to look for copper deposits in the corneal limbus (Kayser-Fleischer rings). Brain MRI reveals areas of increased T2 signal in the striatum, thalamus, brainstem, and white matter. In a study of 100 individuals with early-onset extrapy-ramidal disorders, the following brain MRI fi ndings were almost pathognomonic of
38 A. Videnovic and K.M. Shannon
WD: “face of giant panda” sign, hyperintensities in tectal plate and central pons (central pontine myelinolysis-like), and simultaneous involvement of basal ganglia, thalamus, and brainstem [ 135 ] . Percutaneous liver biopsy with quantitative copper measurement is the diagnostic gold standard.
Treatment is lifelong. Early pharmacological treatment includes dietary copper restriction and copper chelation. Although penicillamine is the copper chelator tra-ditionally used in Wilson disease, triethylene tetramine dihydrochloride (trientine) has emerged as a better tolerated agent. Tetrathiomolybdate is an investigational copper chelator believed to be safer than penicillamine [ 134 ] . Oral zinc helps to limit copper absorption and is a valuable adjunct to therapy [ 136 ] . Liver transplanta-tion may be life saving in patients with fulminant liver disease and may help with the nervous system illness in patients who have not responded to chelation therapy. The symptoms of Wilson disease should be treated symptomatically.
Fahr Disease
Fahr disease is a progressive neurodegenerative disorder characterized by calcifi ca-tion of the basal ganglia, thalamus, and white matter. Although usually inherited as an autosomal dominant trait, sporadic cases have also been described. The globus pallidus has the most common and prominent calcifi cations. Disease onset is after age 30 in most cases. Parkinsonism or other movement disorders, including chorea, tremor, and dystonia, appear to be the most common presentation. This is usually followed by cognitive impairment and ataxia. Brain imaging confi rms bilateral cal-cifi cations. Since similar calcifi cations may occur in various metabolic, infectious, and genetic disorders, it is important to incorporate them into a diagnostic paradigm. The work-up should rule out parathyroid dysfunction. Treatment is symptomatic.
Other rare causes of genetic choreas include spinocerebellar ataxias 2 and 3, ataxia telangiectasia, ataxia with oculomotor apraxia types 1 and 2, paroxysmal kinesigenic choreoathetosis, neuroferritinopathy, and glutaric aciduria.
Benign Choreas
Benign Hereditary Chorea
Benign hereditary chorea (BHC) is a clinically and genetically heterogeneous syndrome characterized by early-onset chorea. In most cases, it is inherited as an autosomal dominant trait. Mutations in the thyroid transcription factor 1 (TITF-1) gene on chromosome 14 have been linked to BHC [ 137, 138 ] . TTIF-1 is essential for the development of the lung, thyroid, and basal ganglia [ 137– 139 ] . BHC has childhood onset and nonprogressive course [ 140, 141 ] . Chorea tends to decrease in
392 Huntington Disease and Other Choreas
adolescence or early adulthood. Dementia, one of the prominent features in HD, is not seen in patients with BHC. Atypical features such as dystonia, slow saccades, dysarthria, and mild cognitive defi cits may be present. Atypical features seem to cluster in families without genetic linkage to chromosome 14 [ 142 ] . Life expec-tancy in BHC is normal, but symptoms may be socially disabling [ 143 ] . The disor-der is commonly misdiagnosed as HD, ataxia telangiectasia, essential myoclonus, and hereditary dystonias [ 142 ] .
Neuropathological fi ndings in BHC include nonspecifi c astrocytosis in the glo-bus pallidus, thalamus, hippocampus, and periaqueductal gray matter [ 139 ] , as well as a loss of most TITF-1-mediated striatal interneurons [ 144 ] .
18 F-fl uorodeoxyglucose PET is normal in patients with BHC [ 145 ] , in contrast to other neurodegenerative choreas where early reduction in striatal glucose metabo-lism has been observed [ 146, 147 ] .
Treatment should be tailored to the severity of chorea and degree of patient distress.
Senile Chorea
Senile chorea, sometimes referred to as “essential chorea,” is an adult-onset, non-progressive form of chorea. Symptoms usually begin after age 60. There is no fam-ily history of chorea. Cognitive and psychiatric symptoms are absent. While some cases represent HD with a negative family history, in most, there is no huntingtin mutation [ 148 ] . Brain imaging studies are normal. Treatment is symptomatic.
Autoimmune Choreas
Sydenham Chorea
Sydenham chorea (SC), also known as rheumatic or minor chorea, is the prototype of autoimmune chorea. Chorea is one of the major criteria for a diagnosis of acute rheumatic fever, and its presence alone is suffi cient for the diagnosis of the acute attack [ 149 ] . Although the incidence of SC has dramatically declined in the Western world, it still remains the most common cause of acute chorea in children worldwide.
SC affects 20–30% of patients with acute rheumatic fever [ 150 ] . The initial pre-sentation usually occurs around age 8–9, with most cases occurring between 5 and 15 years of age. The female-to-male ratio is 2:1. A family history of rheumatic fever is present in about one third of cases [ 151, 152 ] . The onset of chorea is usually 4–8 weeks after an episode of group A beta-hemolytic streptococcal pharyngitis.
The main clinical features of SC are chorea, hypotonia, and muscular weakness. Chorea tends to be generalized, but 20–30% of patients have hemichorea [ 152 ] .
40 A. Videnovic and K.M. Shannon
Involuntary movements result in a clumsy gait and “jerky,” dysarthric speech with sudden changes in pitch and loudness. “Milkmaid’s grip” and inability to sustain tongue protrusion are commonly seen. SC has recently been linked to a spectrum of obsessive-compulsive disorder [ 153 ] . Obsessive-compulsive behavior and attention defi cits are present in 20–30% of patients [ 154 ] and may precede or occur simulta-neously with or after the onset of chorea [ 155 ] . These symptoms are more common in cases of chronic SC. Other psychiatric manifestations include depression, anxi-ety, and irritability [ 156 ] . Executive dysfunction may be present in a subset of patients with SC, even when chorea is in remission [ 157 ] . The cardiac features of rheumatic fever and arthritis may be absent, and chorea may be the only clinical manifestation in up to 20% of patients [ 150 ] . The Universidade Federal de Minas Gerais (UFMG) Sydenham Chorea Rating Scale has been recently developed [ 158 ] . The scale has 27 items refl ecting activities of daily living, behavioral abnormalities, and motor function of patients with SC. SC is a self-limited illness with spontane-ous remission within 6–9 months [ 159 ] . It may recur in up to 50% of patients [ 160 ] , most commonly within 2–3 years after the initial episode [ 161 ] . The recurrence may not be associated with repeated streptococcal infection [ 162, 163 ] . Patients with history of SC are at increased risk for the development of chorea during pregnancy and with the use of oral contraceptive agents.
Although the association of SC and group A beta-hemolytic streptococcal infec-tion has been clearly established [ 164 ] , the pathophysiology of the disease is not fully understood. The pathogenesis of SC may be related to molecular mimicry between streptococcal and CNS antigens [ 165, 166 ] . Anti-basal ganglia antibodies are present in 50–90% of patients with SC [ 167– 169 ] , but their role remains unknown. These antibodies have been also linked to Tourette syndrome and the pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections (PANDAS). Recent fi ndings of elevated interleukins 4 and 10, as well as chemokines CXCL9 and CKCL10, highlight the potential role of cellular immune mechanisms in the pathogenesis of the SC [ 170, 171 ] .
The diagnosis of SC is based on clinical observation. No confi rmatory test is available. Markers of preceding streptococcal infection such as antistreptolysin-O titers, anti-DNAse B, or positive throat culture for group A streptococcus are often negative due to the long latency between the infection and onset of chorea. Cardiac evaluation is mandatory in all cases, and the use of echocardiography is useful in detection of subclinical carditis [ 172 ] . Systemic lupus erythematosus and antiphos-pholipid antibody syndrome should be ruled out. Brain MRI studies reveal enlarged caudate, putamen, and globus pallidus in patients with SC [ 173 ] . PET and SPECT imaging reveals striatal hypermetabolism and perfusion abnormalities with subse-quent normalization after symptom resolution [ 174– 177 ] .
The most important therapeutic intervention in patients with SC is secondary prophylaxis with penicillin or sulfa drugs in a case of penicillin allergy. Prophylaxis should be maintained at least until age 21. Lifetime prophylaxis is warranted for patients with evidence of rheumatic heart disease. Symptomatic treatment should be restricted to patients with severe chorea that interferes with activities of daily
412 Huntington Disease and Other Choreas
living. Valproic acid is the most widely used and well-tolerated agent for the symp-tomatic treatment of chorea [ 178 ] . Gabapentin and carbamazepine have been also successful in alleviating chorea [ 179, 180 ] . Dopamine-blocking agents, such as pimozide and haloperidol, should be reserved for refractory cases due to potential side effects such as dystonia and parkinsonism [ 181 ] .
An attempt to wean an antichoreic agent should be made after at least 1 month free of chorea. Steroids have shown benefi t in cases of refractory chorea [ 182 ] and shorten the duration of the illness [ 183, 184 ] . Several reports have documented the effi cacy of plasma exchange and intravenous immunoglobulin in the treatment of SC [ 185, 186 ] .
Chorea Gravidarum
Chorea gravidarum (CG), characterized by the presence of chorea during preg-nancy, is a rare condition accounting for 3.6% of all choreas [ 187 ] . Chorea usually emerges in the fi rst trimester, and its intensity diminishes as the pregnancy pro-gresses [ 187 ] . Systemic lupus erythematosus (SLE) and primary antiphospholipid antibody syndrome should be ruled out in all pregnant women with coexistent cho-rea. In most cases, CG has a benign course, but fatal outcomes associated with hyperthermia and rhabdomyolysis have been reported [ 188 ] . If the health of the mother or fetus is affected by the severity of chorea, treatment should be instituted. High-potency neuroleptics are the preferred treatment agents [ 189 ] . Dopamine receptor blockers should be avoided during fi rst trimester, as they are classifi ed as class C risk. Reserpine is contraindicated in pregnancy due to its potential teratogenicity.
Other Autoimmune Choreas
Chorea can be seen in a variety of other autoimmune-mediated diseases, most com-monly in SLE. While neuropsychiatric symptoms may be present in up to 60% of patients with SLE, chorea is present in only 1–2% of patients [ 190, 191 ] . Several studies of juvenile SLE however found a higher prevalence of chorea, in up to 30% of patients [ 192– 194 ] . Although chorea is considered a rare clinical manifestation of primary antiphospholipid antibody syndrome [ 195 ] , a recent report of 124 patients documented presence of chorea in 15% of patients [ 196 ] . Chorea has been also described in paraneoplastic syndromes associated with anti-Hu, anti-Yo, and anti-CRMP5 antibodies in patients with small cell lung carcinoma, renal cell carcinoma, and Hodgkin lymphoma [ 197– 200 ] . Other autoimmune disorders associated with chorea include postinfectious chorea, postvaccinal chorea, Behcet disease, polyar-teritis nodosa, and multiple sclerosis.
42 A. Videnovic and K.M. Shannon
Infectious Choreas
Human immunodefi ciency virus (HIV) is the most common cause of infectious chorea. HIV-associated chorea develops as a result of direct activity of the virus, coexistent opportunistic infection, or side effects from HIV treatment [ 201 ] . Among 46 patients with sporadic chorea, AIDS-related chorea was identifi ed in fi ve patients [ 202 ] . HIV-associated chorea therefore should be considered in a young patient who presents with chorea but without a family history of move-ment disorder. Chorea may spontaneously resolve throughout the course of HIV infection [ 202 ] . Abnormal SPECT imaging of the nigrostriatal dopaminergic sys-tem in a patient with HIV-associated chorea has been recently reported [ 203 ] . Antiretroviral therapy may be useful in the treatment of HIV-associated chorea [ 201, 204 ] .
Vascular insults, such as ischemic or hemorrhagic stroke, are common causes of chorea in the elderly. In a large prospective study of 1,500 patients with stroke, 3.9% developed involuntary movements. Chorea was the commonest movement disorder affecting 35.7% of patients [ 212 ] . Hemichorea was the most common form, and recovery occurred in 75% of patients. Thalamus, lentiform nucleus, or adjacent white matter are the most common locations of ischemic or hemorrhagic lesions associated with a chorea [ 212– 214 ] . Vascular chorea tends to diminish spontaneously over the time [ 215 ] . Chorea may be the presenting manifestation of Moyamoya disease [ 216, 217 ] . Another rare cause of chorea is the so-called post-pump chorea, associated with an open heart surgery in the pediatric population. Among 668 children who underwent cardiac surgery, 1.2% developed chorea [ 218 ] . Symptoms begin 3–12 days postoperatively. Involuntary movements mainly affect the mouth, tongue, and face [ 218, 219 ] . Although most likely a complica-tion of extracorporeal circulation [ 220 ] , the pathophysiology of postpump chorea is not fully understood. Residual motor, cognitive, and behavioral impairment is common [ 221 ] .
Symptomatic treatment may be attempted in cases with severe vascular chorea. Dopamine receptor blockade and depletion of presynaptic catecholamines remain the mainstay of pharmacological treatments [ 215, 222 ] . Marked improvement with levetiracetam and topiramate has been recently reported [ 223, 224 ] . Several reports have documented benefi cial effects of stereotactic neurosurgery in the treatment of vascular chorea [ 225, 226 ] .
432 Huntington Disease and Other Choreas
Metabolic/Toxic Choreas
A variety of systemic, metabolic, nutritional, and toxin-induced disorders are asso-ciated with chorea (Table 2.1 ).
Hormonal disorders, such as hyperthyroidism and hypoparathyroidism, can cause both generalized and focal chorea [ 227, 228 ] . Chorea tends to improve with the correction of these hormonal abnormalities.
Acute-onset chorea can occur in the presence of nonketotic hyperglycemia in type 2 diabetes mellitus [ 229– 231 ] . Although the pathophysiology of this syndrome remains unknown, mitochondrial dysfunction with postanoxic striatal injury during periods of prolonged hyperglycemia may be the culprits [ 229, 232 ] . Brain MRI imaging reveals a hyperintense T1 pallidal signal, and SPECT shows hyperperfu-sion of the basal ganglia [ 233 ] . Chorea usually resolves with adequate glycemic control [ 230, 234 ] .
Exposure to various toxins such as alcohol, thallium, mercury, carbon monoxide, cyanide, or manganese can also cause choreiform movements.
Drug-Induced Chorea
Drug-induced chorea is one of the most common forms of chorea encountered in clinical practice. The most common drugs associated with chorea are anticonvul-sants [ 235– 237 ] , anticholinergics [ 238 ] , stimulants [ 239 ] , and dopaminergic agents [ 240 ] . Chorea induced by oral contraceptive agents is particularly common in patients with a history of Sydenham chorea or chorea gravidarum suggesting an immunological basis for the pathophysiology in these patients [ 241 ] . Chorea may emerge early in the course of treatment or be the consequence of long-term therapy.
Withdrawal emergent syndrome is the emergence of choreiform movements in the setting of dopamine-receptor blocking agent withdrawal in the absence of tar-dive dyskinesia.
Tardive dyskinesia is a syndrome of involuntary, choreiform movements associ-ated with the long-term treatment with dopamine-receptor blocking agents. This syndrome occurs in up to 30% of chronically treated patients. Most commonly, movements affect the orobuccal region, causing stereotyped chewing movements with tongue protrusions and facial grimacing. The choreic movements of tardive dyskinesia tend to be more stereotyped than chorea of other etiologies. Risk factors include gender, age, duration of exposure, and preexisting neurological condition. Elderly women are the most susceptible. Supersensitivity of dopamine receptors linked with genetic predisposition and oxidative stress may be the main culprits [ 242, 243 ] . Treatment with second-generation, atypical neuroleptics has been asso-ciated with signifi cantly lower risk for the development of tardive dyskinesias [ 244 ] . Tetrabenazine, although not available in the United States, may be considered in refractory cases.
44 A. Videnovic and K.M. Shannon
Conclusion
Chorea is a hyperkinetic movement disorder associated with many inherited and sporadic diseases affecting basal ganglia structures or their interconnections. Because of its broad differential diagnosis, a careful history, detailed neurological examination, and appropriate diagnostic work-up are needed to establish an accu-rate etiological classifi cation in a timely and cost-effective manner. Treatment remains symptomatic.
References
1. Osler W. On chorea and choreiform affections. Philadelphia: P. Blakiston, Son & Co.; 1894. 2. Krack P. Relicts of dancing mania: the dancing procession of Echternach. Neurology.
1999;53:2169–72. 3. Sydenham T. Schedula monitoria de novae febris ingressu. London: G. Kettilby; 1686. 4. Eftychiadis AC, Chen TS. Saint vitus and his dance. J Neurol Neurosurg Psychiatry.
2001;70:14. 5. Huntington G. On chorea. Med Surg Rep. 1872;26:317–21. 6. Rovito DA, Pirone FJ. Acanthrocytosis associated with schizophrenia. Am J Psychiatry.
1963;120:182–5. 7. Conneally PM. Huntington disease: genetics and epidemiology. Am J Hum Genet.
1984;36:506–26. 8. Folstein SE, Chase GA, Wahl WE, McDonnell AM, Folstein MF. Huntington disease in
Maryland: clinical aspects of racial variation. Am J Hum Genet. 1987;41:168–79. 9. Kokmen E, Ozekmekci FS, Beard CM, O’Brien PC, Kurland LT. Incidence and prevalence of
Huntington’s disease in Olmsted County, Minnesota (1950 through 1989). Arch Neurol. 1994;51:696–8.
10. Harper PS. The epidemiology of Huntington’s disease. Hum Genet. 1992;89:365–76. 11. Nance MA. Genetic testing of children at risk for Huntington’s disease. US Huntington
Disease Genetic Testing Group. Neurology. 1997;49:1048–53. 12. Martin JB, Gusella JF. Huntington’s disease. Pathogenesis and management. N Engl J Med.
1986;315:1267–76. 13. Andrew SE, Goldberg YP, Kremer B, et al. The relationship between trinucleotide (CAG)
repeat length and clinical features of Huntington’s disease. Nat Genet. 1993;4:398–403. 14. Duyao M, Ambrose C, Myers R, et al. Trinucleotide repeat length instability and age of onset
in Huntington’s disease. Nat Genet. 1993;4:387–92. 15. Mahant N, McCusker EA, Byth K, Graham S. Huntington’s disease: clinical correlates of
disability and progression. Neurology. 2003;61:1085–92. 16. Foroud T, Gray J, Ivashina J, Conneally PM. Differences in duration of Huntington’s disease
based on age at onset. J Neurol Neurosurg Psychiatry. 1999;66:52–6. 17. Di Maio L, Squitieri F, Napolitano G, Campanella G, Trofatter JA, Conneally PM. Onset
symptoms in 510 patients with Huntington’s disease. J Med Genet. 1993;30:289–92. 18. Smith MA, Brandt J, Shadmehr R. Motor disorder in Huntington’s disease begins as a dys-
function in error feedback control. Nature. 2000;403:544–9. 19. Kirkwood SC, Siemers E, Bond C, Conneally PM, Christian JC, Foroud T. Confi rmation of
subtle motor changes among presymptomatic carriers of the Huntington disease gene. Arch Neurol. 2000;57:1040–4.
20. Robert MP, Nachev PC, Hicks SL, Golding CV, Tabrizi SJ, Kennard C. Saccadometry of conditional rules in presymptomatic Huntington’s disease. Ann N Y Acad Sci. 2009;1164:444–50.
452 Huntington Disease and Other Choreas
21. Golding CV, Danchaivijitr C, Hodgson TL, Tabrizi SJ, Kennard C. Identifi cation of an oculomotor biomarker of preclinical Huntington disease. Neurology. 2006;67:485–7.
22. Blekher T, Johnson SA, Marshall J, et al. Saccades in presymptomatic and early stages of Huntington disease. Neurology. 2006;67:394–9.
23. Hicks SL, Robert MP, Golding CV, Tabrizi SJ, Kennard C. Oculomotor defi cits indicate the progression of Huntington’s disease. Prog Brain Res. 2008;171:555–8.
24. Djousse L, Knowlton B, Cupples LA, Marder K, Shoulson I, Myers RH. Weight loss in early stage of Huntington’s disease. Neurology. 2002;59:1325–30.
25. Sorensen SA, Fenger K. Causes of death in patients with Huntington’s disease and in unaf-fected fi rst degree relatives. J Med Genet. 1992;29:911–4.
26. Nance MA, Myers RH. Juvenile onset Huntington’s disease—clinical and research perspec-tives. Ment Retard Dev Disabil Res Rev. 2001;7:153–7.
27. Paulsen JS, Ready RE, Hamilton JM, Mega MS, Cummings JL. Neuropsychiatric aspects of Huntington’s disease. J Neurol Neurosurg Psychiatry. 2001;71:310–4.
28. Litvan I, Paulsen JS, Mega MS, Cummings JL. Neuropsychiatric assessment of patients with hyperkinetic and hypokinetic movement disorders. Arch Neurol. 1998;55:1313–9.
29. Di Maio L, Squitieri F, Napolitano G, Campanella G, Trofatter JA, Conneally PM. Suicide risk in Huntington’s disease. J Med Genet. 1993;30:293–5.
30. Paulsen JS, Hoth KF, Nehl C, Stierman L. Critical periods of suicide risk in Huntington’s disease. Am J Psychiatry. 2005;162:725–31.
31. Beglinger LJ, Paulsen JS, Watson DB, et al. Obsessive and compulsive symptoms in prediag-nosed Huntington’s disease. J Clin Psychiatry. 2008;69:1758–65.
32. Ho AK, Sahakian BJ, Brown RG, et al. Profi le of cognitive progression in early Huntington’s disease. Neurology. 2003;61:1702–6.
33. Bamford KA, Caine ED, Kido DK, Cox C, Shoulson I. A prospective evaluation of cognitive decline in early Huntington’s disease: functional and radiographic correlates. Neurology. 1995;45:1867–73.
34. Berrios GE, Wagle AC, Markova IS, Wagle SA, Rosser A, Hodges JR. Psychiatric symptoms in neurologically asymptomatic Huntington’s disease gene carriers: a comparison with gene negative at risk subjects. Acta Psychiatr Scand. 2002;105:224–30.
35. The Huntington’s Disease Collaborative Research Group. A novel gene containing a trinucle-otide repeat that is expanded and unstable on Huntington’s disease chromosomes. Cell. 1993;72:971–83.
36. Kieburtz K, MacDonald M, Shih C, et al. Trinucleotide repeat length and progression of ill-ness in Huntington’s disease. J Med Genet. 1994;31:872–4.
37. Antonini A, Leenders KL, Eidelberg D. [11C]raclopride-PET studies of the Huntington’s disease rate of progression: relevance of the trinucleotide repeat length. Ann Neurol. 1998;43:253–5.
38. Brandt J, Bylsma FW, Gross R, Stine OC, Ranen N, Ross CA. Trinucleotide repeat length and clinical progression in Huntington’s disease. Neurology. 1996;46:527–31.
39. Aylward EH, Li Q, Stine C, et al. Longitudinal change in basal ganglia volume in patients with Huntington’s disease. Neurology. 1997;48:394–9.
40. Rosenblatt A, Liang KY, Zhou H, et al. The association of CAG repeat length with clinical progression in Huntington disease. Neurology. 2006;66:1016–20.
41. Wexler NS, Lorimer J, Porter J, et al. Venezuelan kindreds reveal that genetic and environ-mental factors modulate Huntington’s disease age of onset. Proc Natl Acad Sci U S A. 2004;101:3498–503.
42. Furtado S, Suchowersky O, Rewcastle B, Graham L, Klimek ML, Garber A. Relationship between trinucleotide repeats and neuropathological changes in Huntington’s disease. Ann Neurol. 1996;39:132–6.
43. Maat-Kievit A, Losekoot M, Zwinderman K, et al. Predictability of age at onset in Huntington disease in the Dutch population. Medicine (Baltimore). 2002;81:251–9.
45. Li H, Li SH, Johnston H, Shelbourne PF, Li XJ. Amino-terminal fragments of mutant hun-tingtin show selective accumulation in striatal neurons and synaptic toxicity. Nat Genet. 2000;25:385–9.
46. Graham RK, Deng Y, Slow EJ, et al. Cleavage at the caspase-6 site is required for neuronal dysfunction and degeneration due to mutant huntingtin. Cell. 2006;125:1179–91.
47. Martin-Aparicio E, Yamamoto A, Hernandez F, Hen R, Avila J, Lucas JJ. Proteasomal-dependent aggregate reversal and absence of cell death in a conditional mouse model of Huntington’s disease. J Neurosci. 2001;21:8772–81.
48. Yamamoto A, Lucas JJ, Hen R. Reversal of neuropathology and motor dysfunction in a con-ditional model of Huntington’s disease. Cell. 2000;101:57–66.
49. Seo H, Sonntag KC, Isacson O. Generalized brain and skin proteasome inhibition in Huntington’s disease. Ann Neurol. 2004;56:319–28.
50. Browne SE, Bowling AC, MacGarvey U, et al. Oxidative damage and metabolic dysfunction in Huntington’s disease: selective vulnerability of the basal ganglia. Ann Neurol. 1997;41:646–53.
51. Young AB, Greenamyre JT, Hollingsworth Z, et al. NMDA receptor losses in putamen from patients with Huntington’s disease. Science. 1988;241:981–3.
52. Tabrizi SJ, Cleeter MW, Xuereb J, Taanman JW, Cooper JM, Schapira AH. Biochemical abnormalities and excitotoxicity in Huntington’s disease brain. Ann Neurol. 1999;45:25–32.
53. Gervais FG, Singaraja R, Xanthoudakis S, et al. Recruitment and activation of caspase-8 by the Huntingtin-interacting protein Hip-1 and a novel partner Hippi. Nat Cell Biol. 2002;4:95–105.
54. Ona VO, Li M, Vonsattel JP, et al. Inhibition of caspase-1 slows disease progression in a mouse model of Huntington’s disease. Nature. 1999;399:263–7.
55. Kiechle T, Dedeoglu A, Kubilus J, et al. Cytochrome C and caspase-9 expression in Huntington’s disease. Neuromolecular Med. 2002;1:183–95.
56. Wellington CL, Ellerby LM, Hackam AS, et al. Caspase cleavage of gene products associated with triplet expansion disorders generates truncated fragments containing the polyglutamine tract. J Biol Chem. 1998;273:9158–67.
57. Wellington CL, Ellerby LM, Gutekunst CA, et al. Caspase cleavage of mutant huntingtin precedes neurodegeneration in Huntington’s disease. J Neurosci. 2002;22:7862–72.
58. Trushina E, Dyer RB, Badger II JD, et al. Mutant huntingtin impairs axonal traffi cking in mammalian neurons in vivo and in vitro. Mol Cell Biol. 2004;24:8195–209.
59. Ferrante RJ, Andreassen OA, Jenkins BG, et al. Neuroprotective effects of creatine in a trans-genic mouse model of Huntington’s disease. J Neurosci. 2000;20:4389–97.
60. Zuccato C, Ciammola A, Rigamonti D, et al. Loss of huntingtin-mediated BDNF gene tran-scription in Huntington’s disease. Science. 2001;293:493–8.
61. Michalik A, Van Broeckhoven C. Pathogenesis of polyglutamine disorders: aggregation revisited. Hum Mol Genet. 2003;12:R173–86.
62. Feigin A, Leenders KL, Moeller JR, et al. Metabolic network abnormalities in early Huntington’s disease: an [(18)F]FDG PET study. J Nucl Med. 2001;42:1591–5.
63. Harris GJ, Codori AM, Lewis RF, Schmidt E, Bedi A, Brandt J. Reduced basal ganglia blood fl ow and volume in pre-symptomatic, gene-tested persons at-risk for Huntington’s disease. Brain. 1999;122:1667–78.
64. Aylward EH, Sparks BF, Field KM, et al. Onset and rate of striatal atrophy in preclinical Huntington disease. Neurology. 2004;63:66–72.
65. Kassubek J, Juengling FD, Kioschies T, et al. Topography of cerebral atrophy in early Huntington’s disease: a voxel based morphometric MRI study. J Neurol Neurosurg Psychiatry. 2004;75:213–20.
66. Thieben MJ, Duggins AJ, Good CD, et al. The distribution of structural neuropathology in pre-clinical Huntington’s disease. Brain. 2002;125:1815–28.
67. Weaver KE, Richards TL, Liang O, Laurino MY, Samii A, Aylward EH. Longitudinal diffu-sion tensor imaging in Huntington’s disease. Exp Neurol. 2009;216:525–9.
472 Huntington Disease and Other Choreas
68. Licklederer C, Wolff G, Barth J. Mental health and quality of life after genetic testing for Huntington disease: a long-term effect study in Germany. Am J Med Genet A. 2008;146A:2078–85.
69. Feigin A, Kieburtz K, Como P, et al. Assessment of coenzyme Q10 tolerability in Huntington’s disease. Mov Disord. 1996;11:321–3.
70. Huntington Study Group. A randomized, placebo-controlled trial of coenzyme Q10 and rem-acemide in Huntington’s disease. Neurology. 2001;57:397–404.
71. Huntington Study Group. Dosage effects of riluzole in Huntington’s disease: a multicenter placebo-controlled study. Neurology. 2003;61:1551–6.
72. Rosas HD, Koroshetz WJ, Jenkins BG, et al. Riluzole therapy in Huntington’s disease (HD). Mov Disord. 1999;14:326–30.
73. Huntington Study Group. Minocycline safety and tolerability in Huntington disease. Neurology. 2004;63:547–9.
74. Bonelli RM, Heuberger C, Reisecker F. Minocycline for Huntington’s disease: an open label study. Neurology. 2003;60:883–4.
75. Thomas M, Ashizawa T, Jankovic J. Minocycline in Huntington’s disease: a pilot study. Mov Disord. 2004;19:692–5.
76. Puri BK, Leavitt BR, Hayden MR, et al. Ethyl-EPA in Huntington disease: a double-blind, randomized, placebo-controlled trial. Neurology. 2005;65:286–92.
77. Huntington Study Group TREND-HD Investigators. Randomized controlled trial of ethyl-eicosapentaenoic acid in Huntington disease: the TREND-HD study. Arch Neurol. 2008;65:1582–9.
78. Verbessem P, Lemiere J, Eijnde BO, et al. Creatine supplementation in Huntington’s disease: a placebo-controlled pilot trial. Neurology. 2003;61:925–30.
79. Yero T, Rey JA. Tetrabenazine (xenazine), an FDA-approved treatment option for Huntington’s disease-related chorea. P T. 2008;33:690–4.
80. Ondo WG, Tintner R, Thomas M, Jankovic J. Tetrabenazine treatment for Huntington’s dis-ease-associated chorea. Clin Neuropharmacol. 2002;25:300–2.
81. Huntington Study Group. Tetrabenazine as antichorea therapy in Huntington disease: a ran-domized controlled trial. Neurology. 2006;66:366–72.
82. Frank S. Tetrabenazine as anti-chorea therapy in Huntington disease: an open-label continu-ation study. Huntington Study Group/TETRA-HD Investigators. BMC Neurol. 2009;9:62.
83. Fasano A, Cadeddu F, Guidubaldi A, et al. The long-term effect of tetrabenazine in the man-agement of Huntington disease. Clin Neuropharmacol. 2008;31:313–8.
84. Verhagen Metman L, Morris MJ, Farmer C, et al. Huntington’s disease: a randomized, con-trolled trial using the NMDA-antagonist amantadine. Neurology. 2002;59:694–9.
85. O’Suilleabhain P, Dewey Jr RB. A randomized trial of amantadine in Huntington disease. Arch Neurol. 2003;60:996–8.
86. Tan EK, Jankovic J, Ondo W. Bruxism in Huntington’s disease. Mov Disord. 2000;15:171–3.
87. Fernandez HH, Friedman JH, Grace J, Beason-Hazen S. Donepezil for Huntington’s disease. Mov Disord. 2000;15:173–6.
88. de Tommaso M, Specchio N, Sciruicchio V, Difruscolo O, Specchio LM. Effects of rivastig-mine on motor and cognitive impairment in Huntington’s disease. Mov Disord. 2004;19:1516–8.
89. Beglinger LJ, Adams WH, Paulson H, et al. Randomized controlled trial of atomoxetine for cognitive dysfunction in early Huntington disease. J Clin Psychopharmacol. 2009;29:484–7.
90. Moro E, Lang AE, Strafella AP, et al. Bilateral globus pallidus stimulation for Huntington’s disease. Ann Neurol. 2004;56:290–4.
91. Cubo E, Shannon KM, Penn RD, Kroin JS. Internal globus pallidotomy in dystonia second-ary to Huntington’s disease. Mov Disord. 2000;15:1248–51.
92. Fink JS, Schumacher JM, Ellias SL, et al. Porcine xenografts in Parkinson’s disease and Huntington’s disease patients: preliminary results. Cell Transplant. 2000;9:273–8.
48 A. Videnovic and K.M. Shannon
93. Bachoud-Levi AC, Gaura V, Brugieres P, et al. Effect of fetal neural transplants in patients with Huntington’s disease 6 years after surgery: a long-term follow-up study. Lancet Neurol. 2006;5:303–9.
94. Bachoud-Levi AC, Remy P, Nguyen JP, et al. Motor and cognitive improvements in patients with Huntington’s disease after neural transplantation. Lancet. 2000;356:1975–9.
95. Hauser RA, Furtado S, Cimino CR, et al. Bilateral human fetal striatal transplantation in Huntington’s disease. Neurology. 2002;58:687–95.
97. Pallier PN, Morton AJ. Management of sleep/wake cycles improves cognitive function in a transgenic mouse model of Huntington’s disease. Brain Res. 2009;1279:90–8.
98. Ikeuchi T, Koide R, Onodera O, et al. Dentatorubral-pallidoluysian atrophy (DRPLA). Molecular basis for wide clinical features of DRPLA. Clin Neurosci. 1995;3:23–7.
99. Hasegawa A, Ikeuchi T, Koike R, et al. Long-term disability and prognosis in dentatorubral-pallidoluysian atrophy: a correlation with CAG repeat length. Mov Disord. 2010;25(11):1694–700.
100. Takano H, Cancel G, Ikeuchi T, et al. Close associations between prevalences of dominantly inherited spinocerebellar ataxias with CAG-repeat expansions and frequencies of large normal CAG alleles in Japanese and Caucasian populations. Am J Hum Genet. 1998;63:1060–6.
101. Warner TT, Lennox GG, Janota I, Harding AE. Autosomal-dominant dentatorubropallidoluy-sian atrophy in the United Kingdom. Mov Disord. 1994;9:289–96.
102. Munoz E, Campdelacreu J, Ferrer I, et al. Severe cerebral white matter involvement in a case of dentatorubropallidoluysian atrophy studied at autopsy. Arch Neurol. 2004;61:946–9.
103. Levine IM, Estes JW, Looney JM. Hereditary neurological disease with acanthocytosis. A new syndrome. Arch Neurol. 1968;19:403–9.
104. Critchley EM, Clark DB, Wikler A. Acanthocytosis and neurological disorder without beta-lipoproteinemia. Arch Neurol. 1968;18:134–40.
105. Rampoldi L, Danek A, Monaco AP. Clinical features and molecular bases of neuroacantho-cytosis. J Mol Med. 2002;80:475–91.
106. Rampoldi L, Dobson-Stone C, Rubio JP, et al. A conserved sorting-associated protein is mutant in chorea-acanthocytosis. Nat Genet. 2001;28:119–20.
107. Rubio JP, Danek A, Stone C, et al. Chorea-acanthocytosis: genetic linkage to chromosome 9q21. Am J Hum Genet. 1997;61:899–908.
108. Ueno S, Maruki Y, Nakamura M, et al. The gene encoding a newly discovered protein, chor-ein, is mutated in chorea-acanthocytosis. Nat Genet. 2001;28:121–2.
109. Danek A, Walker RH. Neuroacanthocytosis. Curr Opin Neurol. 2005;18:386–92. 110. Shibasaki H, Sakai T, Nishimura H, Sato Y, Goto I, Kuroiwa Y. Involuntary movements in
chorea-acanthocytosis: a comparison with Huntington’s chorea. Ann Neurol. 1982;12:311–4. 111. Gradstein L, Danek A, Grafman J, Fitzgibbon EJ. Eye movements in chorea-acanthocytosis.
Invest Ophthalmol Vis Sci. 2005;46:1979–87. 112. Hardie RJ, Pullon HW, Harding AE, et al. Neuroacanthocytosis. A clinical, haematological
and pathological study of 19 cases. Brain. 1991;114:13–49. 113. Kazis A, Kimiskidis V, Georgiadis G, Voloudaki E. Neuroacanthocytosis presenting with
epilepsy. J Neurol. 1995;242:415–7. 114. Okamoto K, Ito J, Furusawa T, et al. CT and MR fi ndings of neuroacanthocytosis. J Comput
Assist Tomogr. 1997;21:221–2. 115. Nicholl DJ, Sutton I, Dotti MT, Supple SG, Danek A, Lawden M. White matter abnormalities
on MRI in neuroacanthocytosis. J Neurol Neurosurg Psychiatry. 2004;75:1200–1. 116. Vital A, Bouillot S, Burbaud P, Ferrer X, Vital C. Chorea-acanthocytosis: neuropathology of
brain and peripheral nerve. Clin Neuropathol. 2002;21:77–81. 117. Rinne JO, Daniel SE, Scaravilli F, Pires M, Harding AE, Marsden CD. The neuropathological
features of neuroacanthocytosis. Mov Disord. 1994;9:297–304. 118. Witt TN, Danek A, Reiter M, Heim MU, Dirschinger J, Olsen EG. McLeod syndrome:
a distinct form of neuroacanthocytosis. Report of two cases and literature review with empha-sis on neuromuscular manifestations. J Neurol. 1992;239:302–6.
492 Huntington Disease and Other Choreas
119. Johnson MA, Kuo YM, Westaway SK, et al. Mitochondrial localization of human PANK2 and hypotheses of secondary iron accumulation in pantothenate kinase-associated neurode-generation. Ann N Y Acad Sci. 2004;1012:282–98.
120. Gordon N. Pantothenate kinase-associated neurodegeneration (Hallervorden-Spatz syn-drome). Eur J Paediatr Neurol. 2002;6:243–7.
121. Orrell RW, Amrolia PJ, Heald A, et al. Acanthocytosis, retinitis pigmentosa, and pallidal degeneration: a report of three patients, including the second reported case with hypoprebeta-lipoproteinemia (HARP syndrome). Neurology. 1995;45:487–92.
122. Houlden H, Lincoln S, Farrer M, Cleland PG, Hardy J, Orrell RW. Compound heterozygous PANK2 mutations confi rm HARP and Hallervorden-Spatz syndromes are allelic. Neurology. 2003;61:1423–6.
123. Moore RC, Xiang F, Monaghan J, et al. Huntington disease phenocopy is a familial prion disease. Am J Hum Genet. 2001;69:1385–8.
124. Holmes SE, O’Hearn E, Rosenblatt A, et al. A repeat expansion in the gene encoding juncto-philin-3 is associated with Huntington disease-like 2. Nat Genet. 2001;29:377–8.
125. Rudnicki DD, Pletnikova O, Vonsattel JP, Ross CA, Margolis RL. A comparison of Huntington disease and Huntington disease-like 2 neuropathology. J Neuropathol Exp Neurol. 2008;67:366–74.
127. Walker RH, Rasmussen A, Rudnicki D, et al. Huntington’s disease—like 2 can present as chorea-acanthocytosis. Neurology. 2003;61:1002–4.
128. Margolis RL, O’Hearn E, Rosenblatt A, et al. A disorder similar to Huntington’s disease is associated with a novel CAG repeat expansion. Ann Neurol. 2001;50:373–80.
129. Koide R, Kobayashi S, Shimohata T, et al. A neurological disease caused by an expanded CAG trinucleotide repeat in the TATA-binding protein gene: a new polyglutamine disease? Hum Mol Genet. 1999;8:2047–53.
130. Bauer P, Laccone F, Rolfs A, et al. Trinucleotide repeat expansion in SCA17/TBP in white patients with Huntington’s disease-like phenotype. J Med Genet. 2004;41:230–2.
131. De Michele G, Maltecca F, Carella M, et al. Dementia, ataxia, extrapyramidal features, and epilepsy: phenotype spectrum in two Italian families with spinocerebellar ataxia type 17. Neurol Sci. 2003;24:166–7.
132. Tanzi RE, Petrukhin K, Chernov I, et al. The Wilson disease gene is a copper transporting ATPase with homology to the Menkes disease gene. Nat Genet. 1993;5:344–50.
133. Kitzberger R, Madl C, Ferenci P. Wilson disease. Metab Brain Dis. 2005;20:295–302. 134. Das SK, Ray K. Wilson’s disease: an update. Nat Clin Pract Neurol. 2006;2:482–93. 135. Prashanth LK, Sinha S, Taly AB, Vasudev MK. Do MRI features distinguish Wilson’s disease
from other early onset extrapyramidal disorders? An analysis of 100 cases. Mov Disord. 2010;25:672–8.
137. do Carmo Costa M, Costa C, Silva AP, et al. Nonsense mutation in TITF1 in a Portuguese family with benign hereditary chorea. Neurogenetics. 2005;6:209–15.
138. Breedveld GJ, van Dongen JW, Danesino C, et al. Mutations in TITF-1 are associated with benign hereditary chorea. Hum Mol Genet. 2002;11:971–9.
139. Kleiner-Fisman G, Rogaeva E, Halliday W, et al. Benign hereditary chorea: clinical, genetic, and pathological fi ndings. Ann Neurol. 2003;54:244–7.
140. Harper PS. Benign hereditary chorea. Clinical and genetic aspects. Clin Genet. 1978;13:85–95.
141. Haerer AF, Currier RD, Jackson JF. Hereditary nonprogressive chorea of early onset. N Engl J Med. 1967;276:1220–4.
142. Breedveld GJ, Percy AK, MacDonald ME, et al. Clinical and genetic heterogeneity in benign hereditary chorea. Neurology. 2002;59:579–84.
143. Fernandez M, Raskind W, Matsushita M, Wolff J, Lipe H, Bird T. Hereditary benign chorea: clinical and genetic features of a distinct disease. Neurology. 2001;57:106–10.
50 A. Videnovic and K.M. Shannon
144. Kleiner-Fisman G, Calingasan NY, Putt M, Chen J, Beal MF, Lang AE. Alterations of striatal neurons in benign hereditary chorea. Mov Disord. 2005;20:1353–7.
145. Kuwert T, Lange HW, Langen KJ, et al. Normal striatal glucose consumption in two patients with benign hereditary chorea as measured by positron emission tomography. J Neurol. 1990;237:80–4.
146. Tanaka M, Hirai S, Kondo S, et al. Cerebral hypoperfusion and hypometabolism with altered striatal signal intensity in chorea-acanthocytosis: a combined PET and MRI study. Mov Disord. 1998;13:100–7.
147. Ginovart N, Lundin A, Farde L, et al. PET study of the pre- and post-synaptic dopaminergic markers for the neurodegenerative process in Huntington’s disease. Brain. 1997;120:503–14.
148. Shinotoh H, Calne DB, Snow B, et al. Normal CAG repeat length in the Huntington’s disease gene in senile chorea. Neurology. 1994;44:2183–4.
149. American Heart Association. Guidelines for the diagnosis of rheumatic fever. Jones Criteria, 1992 update. Special Writing Group of the Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease of the Council on Cardiovascular Disease in the Young of the American Heart Association. JAMA. 1992;268:2069–73.
150. Cardoso F, Eduardo C, Silva AP, Mota CC. Chorea in fi fty consecutive patients with rheu-matic fever. Mov Disord. 1997;12:701–3.
151. Aron AM, Freeman JM, Carter S. The natural history of Sydenham’s chorea. Review of the literature and long-term evaluation with emphasis on cardiac sequelae. Am J Med. 1965;38:83–95.
152. Zomorrodi A, Wald ER. Sydenham’s chorea in western Pennsylvania. Pediatrics. 2006;117:e675–9.
153. Swedo SE, Rapoport JL, Cheslow DL, et al. High prevalence of obsessive-compulsive symp-toms in patients with Sydenham’s chorea. Am J Psychiatry. 1989;146:246–9.
154. Maia DP, Teixeira Jr AL, Quintao Cunningham MC, Cardoso F. Obsessive compulsive behav-ior, hyperactivity, and attention defi cit disorder in Sydenham chorea. Neurology. 2005;64:1799–801.
155. Asbahr FR, Negrao AB, Gentil V, et al. Obsessive-compulsive and related symptoms in chil-dren and adolescents with rheumatic fever with and without chorea: a prospective 6-month study. Am J Psychiatry. 1998;155:1122–4.
156. Ridel KR, Lipps TD, Gilbert DL. The prevalence of neuropsychiatric disorders in Sydenham’s chorea. Pediatr Neurol. 2010;42:243–8.
157. Beato R, Maia DP, Teixeira Jr AL, Cardoso F. Executive functioning in adult patients with Sydenham’s chorea. Mov Disord. 2010;25:853–7.
158. Teixeira Jr AL, Maia DP, Cardoso F. UFMG Sydenham’s chorea rating scale (USCRS): reli-ability and consistency. Mov Disord. 2005;20:585–91.
160. Cardoso F, Vargas AP, Oliveira LD, Guerra AA, Amaral SV. Persistent Sydenham’s chorea. Mov Disord. 1999;14:805–7.
161. Dajani A, Taubert K, Ferrieri P, Peter G, Shulman S. Treatment of acute streptococcal phar-yngitis and prevention of rheumatic fever: a statement for health professionals. Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease of the Council on Cardiovascular Disease in the Young, the American Heart Association. Pediatrics. 1995;96:758–64.
162. Korn-Lubetzki I, Brand A, Steiner I. Recurrence of Sydenham chorea: implications for patho-genesis. Arch Neurol. 2004;61:1261–4.
163. Berrios X, Quesney F, Morales A, Blazquez J, Bisno AL. Are all recurrences of “pure” Sydenham chorea true recurrences of acute rheumatic fever? J Pediatr. 1985;107:867–72.
164. Taranta A, Stollerman GH. The relationship of Sydenham’s chorea to infection with group A streptococci. Am J Med. 1956;20:170–5.
165. Kirvan CA, Swedo SE, Kurahara D, Cunningham MW. Streptococcal mimicry and antibody-mediated cell signaling in the pathogenesis of Sydenham’s chorea. Autoimmunity. 2006;39:21–9.
512 Huntington Disease and Other Choreas
166. Kirvan CA, Swedo SE, Heuser JS, Cunningham MW. Mimicry and autoantibody-mediated neuronal cell signaling in Sydenham chorea. Nat Med. 2003;9:914–20.
167. Singer HS, Loiselle CR, Lee O, Garvey MA, Grus FH. Anti-basal ganglia antibody abnor-malities in Sydenham chorea. J Neuroimmunol. 2003;136:154–61.
168. Husby G, van de Rijn I, Zabriskie JB, Abdin ZH, Williams Jr RC. Antibodies reacting with cytoplasm of subthalamic and caudate nuclei neurons in chorea and acute rheumatic fever. J Exp Med. 1976;144:1094–110.
169. Church AJ, Cardoso F, Dale RC, Lees AJ, Thompson EJ, Giovannoni G. Anti-basal ganglia antibodies in acute and persistent Sydenham’s chorea. Neurology. 2002;59:227–31.
170. Church AJ, Dale RC, Cardoso F, et al. CSF and serum immune parameters in Sydenham’s chorea: evidence of an autoimmune syndrome? J Neuroimmunol. 2003;136:149–53.
171. Teixeira Jr AL, Cardoso F, Souza AL, Teixeira MM. Increased serum concentrations of monokine induced by interferon-gamma/CXCL9 and interferon-gamma-inducible protein 10/CXCL-10 in Sydenham’s chorea patients. J Neuroimmunol. 2004;150:157–62.
172. Panamonta M, Chaikitpinyo A, Kaplan EL, Pantongwiriyakul A, Tassniyom S, Sutra S. The relationship of carditis to the initial attack of Sydenham’s chorea. Int J Cardiol. 2004;94:241–8.
173. Giedd JN, Rapoport JL, Kruesi MJ, et al. Sydenham’s chorea: magnetic resonance imaging of the basal ganglia. Neurology. 1995;45:2199–202.
175. Dilenge ME, Shevell MI, Dinh L. Restricted unilateral Sydenham’s chorea: reversible con-tralateral striatal hypermetabolism demonstrated on single photon emission computed tomo-graphic scanning. J Child Neurol. 1999;14:509–13.
176. Kabakus N, Balci TA, Kurt A, Kurt AN. Cerebral blood fl ow abnormalities in children with Sydenham’s chorea: a SPECT study. Indian Pediatr. 2006;43:241–6.
177. Lee PH, Nam HS, Lee KY, Lee BI, Lee JD. Serial brain SPECT images in a case of Sydenham chorea. Arch Neurol. 1999;56:237–40.
178. Genel F, Arslanoglu S, Uran N, Saylan B. Sydenham’s chorea: clinical fi ndings and compari-son of the effi cacies of sodium valproate and carbamazepine regimens. Brain Dev. 2002;24:73–6.
179. Harel L, Zecharia A, Straussberg R, Volovitz B, Amir J. Successful treatment of rheumatic chorea with carbamazepine. Pediatr Neurol. 2000;23:147–51.
180. Kothare SV, Pollack P, Kulberg AG, Ravin PD. Gabapentin treatment in a child with delayed-onset hemichorea/hemiballismus. Pediatr Neurol. 2000;22:68–71.
181. Teixeira AL, Cardoso F, Maia DP, Cunningham MC. Sydenham’s chorea may be a risk factor for drug induced parkinsonism. J Neurol Neurosurg Psychiatry. 2003;74:1350–1.
182. Cardoso F, Maia D, Cunningham MC, Valenca G. Treatment of Sydenham chorea with corticosteroids. Mov Disord. 2003;18:1374–7.
183. Paz JA, Silva CA, Marques-Dias MJ. Randomized double-blind study with prednisone in Sydenham’s chorea. Pediatr Neurol. 2006;34:264–9.
184. Barash J, Margalith D, Matitiau A. Corticosteroid treatment in patients with Sydenham’s chorea. Pediatr Neurol. 2005;32:205–7.
185. Garvey MA, Snider LA, Leitman SF, Werden R, Swedo SE. Treatment of Sydenham’s chorea with intravenous immunoglobulin, plasma exchange, or prednisone. J Child Neurol. 2005;20:424–9.
186. Jordan LC, Singer HS. Sydenham chorea in children. Curr Treat Options Neurol. 2003;5:283–90.
187. Cardoso F. Chorea gravidarum. Arch Neurol. 2002;59:868–70. 188. Donaldson JO. Neurologic emergencies in pregnancy. Obstet Gynecol Clin North Am.
1991;18:199–212. 189. Smith MS, Evatt ML. Movement disorders in pregnancy. Neurol Clin. 2004;22:783–98. 190. Brey RL, Holliday SL, Saklad AR, et al. Neuropsychiatric syndromes in lupus: prevalence
using standardized defi nitions. Neurology. 2002;58:1214–20.
52 A. Videnovic and K.M. Shannon
191. Sanna G, Bertolaccini ML, Cuadrado MJ, et al. Neuropsychiatric manifestations in systemic lupus erythematosus: prevalence and association with antiphospholipid antibodies. J Rheumatol. 2003;30:985–92.
192. Olfat MO, Al-Mayouf SM, Muzaffer MA. Pattern of neuropsychiatric manifestations and outcome in juvenile systemic lupus erythematosus. Clin Rheumatol. 2004;23:395–9.
193. Steinlin MI, Blaser SI, Gilday DL, et al. Neurologic manifestations of pediatric systemic lupus erythematosus. Pediatr Neurol. 1995;13:191–7.
194. Quintero-Del-Rio AI, Van M. Neurologic symptoms in children with systemic lupus erythe-matosus. J Child Neurol. 2000;15:803–7.
195. Asherson RA, Cervera R. Unusual manifestations of the antiphospholipid syndrome. Clin Rev Allergy Immunol. 2003;25:61–78.
196. Kalashnikova LA, Dobrynina LA, Aleksandrova EN, Novikov AA. Neurological appear-ances of primary antiphospholipid syndrome. Zh Nevrol Psikhiatr Im S S Korsakova. 2005;13(Suppl):19–24.
197. Nuti A, Ceravolo R, Salvetti S, Gambaccini G, Bonuccelli U, Capochiani E. Paraneoplastic choreic syndrome during non-Hodgkin’s lymphoma. Mov Disord. 2000;15:350–2.
198. Muehlschlegel S, Okun MS, Foote KD, Coco D, Yachnis AT, Fernandez HH. Paraneoplastic chorea with leukoencephalopathy presenting with obsessive-compulsive and behavioral dis-order. Mov Disord. 2005;20:1523–7.
199. Kinirons P, Fulton A, Keoghan M, Brennan P, Farrell MA, Moroney JT. Paraneoplastic limbic encephalitis (PLE) and chorea associated with CRMP-5 neuronal antibody. Neurology. 2003;61:1623–4.
200. Dorban S, Gille M, Kessler R, Pieret F, Declercq I, Sindic CJ. Chorea-athetosis in the anti-Hu syndrome. Rev Neurol (Paris). 2004;160:126–9.
201. Cardoso F. HIV-related movement disorders: epidemiology, pathogenesis and management. CNS Drugs. 2002;16:663–8.
202. Piccolo I, Defanti CA, Soliveri P, Volonte MA, Cislaghi G, Girotti F. Cause and course in a series of patients with sporadic chorea. J Neurol. 2003;250:429–35.
203. Sporer B, Linke R, Seelos K, Paul R, Klopstock T, Pfi ster HW. HIV-induced chorea: evidence for basal ganglia dysregulation by SPECT. J Neurol. 2005;252:356–8.
204. Trocello JM, Blanchet A, Bourdain F, Meyohas MC, Vidailhet M. Resolution of choreic movements associated with HIV encephalitis with anti-retroviral therapy. Rev Neurol (Paris). 2006;162:89–91.
205. Alarcon F, Duenas G, Cevallos N, Lees AJ. Movement disorders in 30 patients with tubercu-lous meningitis. Mov Disord. 2000;15:561–9.
206. Kalita J, Ranjan P, Misra UK, Das BK. Hemichorea: a rare presentation of tuberculoma. J Neurol Sci. 2003;208:109–11.
207. Willoughby Jr RE, Tieves KS, Hoffman GM, et al. Survival after treatment of rabies with induction of coma. N Engl J Med. 2005;352:2508–14.
208. Jones AL, Bouchier IA. A patient with neurosyphilis presenting as chorea. Scott Med J. 1993;38:82–4.
210. McKee D, Talbot P. Chorea as a presenting feature of variant Creutzfeldt-Jakob disease. Mov Disord. 2003;18:837–8.
211. Bowen J, Mitchell T, Pearce R, Quinn N. Chorea in new variant Creutzfeldt-Jacob disease. Mov Disord. 2000;15:1284–5.
212. Alarcon F, Zijlmans JC, Duenas G, Cevallos N. Post-stroke movement disorders: report of 56 patients. J Neurol Neurosurg Psychiatry. 2004;75:1568–74.
213. Lee MS, Marsden CD. Movement disorders following lesions of the thalamus or subthalamic region. Mov Disord. 1994;9:493–507.
214. Dewey Jr RB. Jankovic J. Hemiballism-hemichorea. Clinical and pharmacologic fi ndings in 21 patients. Arch Neurol. 1989;46:862–7.
532 Huntington Disease and Other Choreas
215. Ghika-Schmid F, Ghika J, Regli F, Bogousslavsky J. Hyperkinetic movement disorders during and after acute stroke: the Lausanne Stroke Registry. J Neurol Sci. 1997;146:109–16.
216. Zheng W, Wanibuchi M, Onda T, et al. A case of moyamoya disease presenting with chorea. Childs Nerv Syst. 2006;22:274–8.
218. Medlock MD, Cruse RS, Winek SJ, et al. A 10-year experience with postpump chorea. Ann Neurol. 1993;34:820–6.
219. Huntley DT, al-Mateen M, Menkes JH. Unusual dyskinesia complicating cardiopulmonary bypass surgery. Dev Med Child Neurol. 1993;35:631–6.
220. Thobois S, Bozio A, Ninet J, Akhavi A, Broussolle E. Chorea after cardiopulmonary bypass. Eur Neurol. 2004;51:46–7.
221. du Plessis AJ, Bellinger DC, Gauvreau K, et al. Neurologic outcome of choreoathetoid encephalopathy after cardiac surgery. Pediatr Neurol. 2002;27:9–17.
222. Ristic A, Marinkovic J, Dragasevic N, Stanisavljevic D, Kostic V. Long-term prognosis of vascular hemiballismus. Stroke. 2002;33:2109–11.
223. Driver-Dunckley E, Evidente VG. Hemichorea-hemiballismus may respond to topiramate. Clin Neuropharmacol. 2005;28:142–4.
224. D’Amelio M, Callari G, Gammino M, et al. Levetiracetam in the treatment of vascular cho-rea: a case report. Eur J Clin Pharmacol. 2005;60:835–6.
225. Krauss JK, Loher TJ, Weigel R, Capelle HH, Weber S, Burgunder JM. Chronic stimulation of the globus pallidus internus for treatment of non-dYT1 generalized dystonia and chore-oathetosis: 2-year follow up. J Neurosurg. 2003;98:785–92.
226. Choi SJ, Lee SW, Kim MC, et al. Posteroventral pallidotomy in medically intractable posta-poplectic monochorea: case report. Surg Neurol. 2003;59:486–90; discussion 90.
227. Isaacs JD, Rakshi J, Baker R, Brooks DJ, Warrens AN. Chorea associated with thyroxine replacement therapy. Mov Disord. 2005;20:1656–7.
228. Ristic AJ, Svetel M, Dragasevic N, Zarkovic M, Koprivsek K, Kostic VS. Bilateral chorea-ballism associated with hyperthyroidism. Mov Disord. 2004;19:982–3.
229. Oh SH, Lee KY, Im JH, Lee MS. Chorea associated with non-ketotic hyperglycemia and hyperintensity basal ganglia lesion on T1-weighted brain MRI study: a meta-analysis of 53 cases including four present cases. J Neurol Sci. 2002;200:57–62.
230. Lin JJ, Chang MK. Hemiballism-hemichorea and non-ketotic hyperglycaemia. J Neurol Neurosurg Psychiatry. 1994;57:748–50.
231. Lee BC, Hwang SH, Chang GY. Hemiballismus-hemichorea in older diabetic women: a clini-cal syndrome with MRI correlation. Neurology. 1999;52:646–8.
232. Brouillet E, Hantraye P, Ferrante RJ, et al. Chronic mitochondrial energy impairment pro-duces selective striatal degeneration and abnormal choreiform movements in primates. Proc Natl Acad Sci U S A. 1995;92:7105–9.
233. Lai SL, Tseng YL, Hsu MC, Chen SS. Magnetic resonance imaging and single-photon emis-sion computed tomography changes in hypoglycemia-induced chorea. Mov Disord. 2004;19:475–8.
234. Chu K, Kang DW, Kim DE, Park SH, Roh JK. Diffusion-weighted and gradient echo mag-netic resonance fi ndings of hemichorea-hemiballismus associated with diabetic hyperglyce-mia: a hyperviscosity syndrome? Arch Neurol. 2002;59:448–52.
236. Harrison MB, Lyons GR, Landow ER. Phenytoin and dyskinesias: a report of two cases and review of the literature. Mov Disord. 1993;8:19–27.
237. Zaatreh M, Tennison M, D’Cruz O, Beach RL. Anticonvulsants-induced chorea: a role for pharmacodynamic drug interaction? Seizure. 2001;10:596–9.
238. Matsumoto K, Nogaki H, Morimatsu M. A case of choreoathetoid movements induced by anticholinergic drugs, trihexyphenidyl HCl and dosulepin HCl. Nippon Ronen Igakkai Zasshi. 1992;29:686–9.
54 A. Videnovic and K.M. Shannon
239. Morgan JC, Winter WC, Wooten GF. Amphetamine-induced chorea in attention defi cit-hyperactivity disorder. Mov Disord. 2004;19:840–2.
240. Fahn S. The spectrum of levodopa-induced dyskinesias. Ann Neurol. 2000;47:S2–9; discus-sion S11.
241. Miranda M, Cardoso F, Giovannoni G, Church A. Oral contraceptive induced chorea: another condition associated with anti-basal ganglia antibodies. J Neurol Neurosurg Psychiatry. 2004;75:327–8.
242. Ossowska K. Neuronal basis of neuroleptic-induced extrapyramidal side effects. Pol J Pharmacol. 2002;54:299–312.
243. Margolese HC, Chouinard G, Kolivakis TT, Beauclair L, Miller R. Tardive dyskinesia in the era of typical and atypical antipsychotics. Part 1: pathophysiology and mechanisms of induc-tion. Can J Psychiatry. 2005;50:541–7.
244. Correll CU, Leucht S, Kane JM. Lower risk for tardive dyskinesia associated with second-generation antipsychotics: a systematic review of 1-year studies. Am J Psychiatry. 2004;161:414–25.