42
Hypertension and chronic kidney disease in older people Dr Rick Fielding Consultant Renal Medicine Brighton & Sussex University Hospitals
| Date post: | 16-Dec-2015 |
| Category: |
Documents |
| Upload: | derick-owen |
| View: | 236 times |
| Download: | 0 times |

Hypertension and chronic kidney disease in older people
Dr Rick Fielding
Consultant Renal Medicine
Brighton & Sussex University Hospitals

• How big is the CKD problem?• Why is CKD important in the elderly?• What can be done about it?
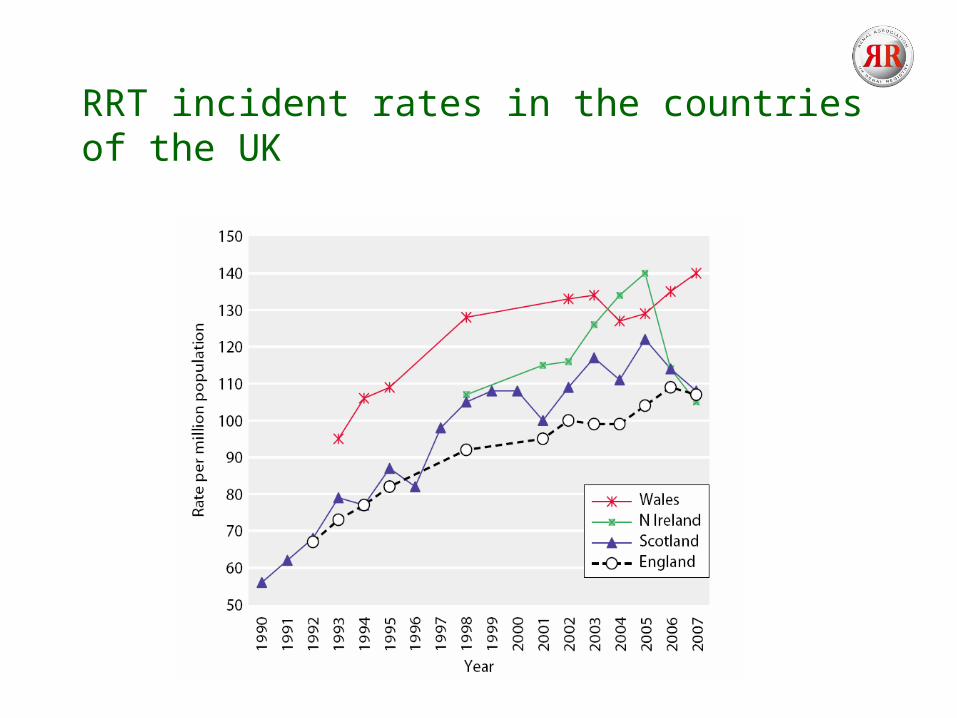
RRT incident rates in the countries of the UK
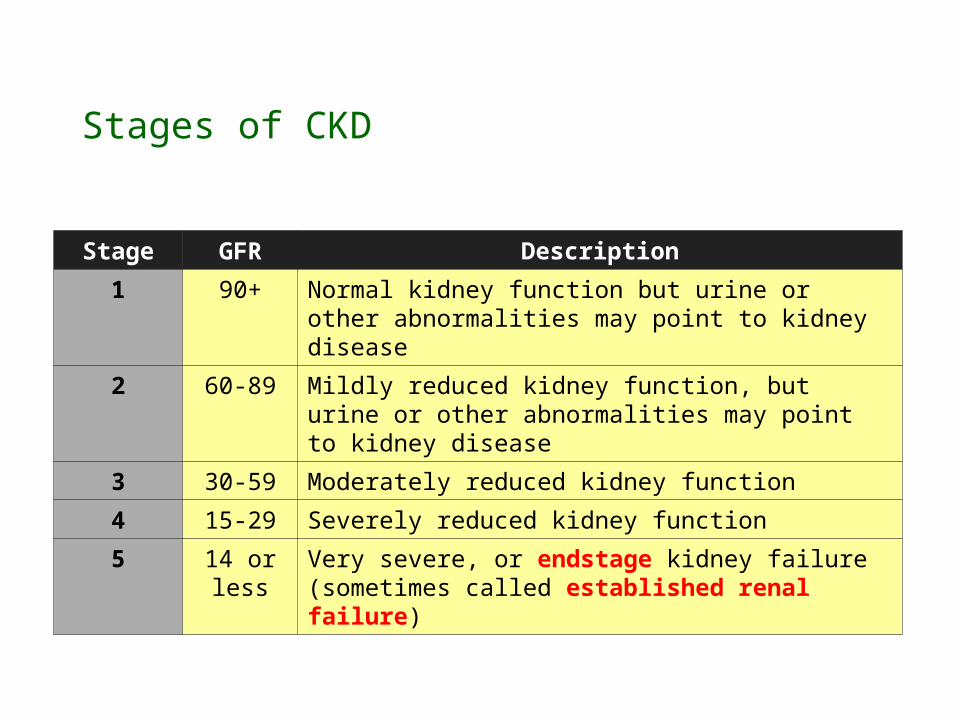
Stages of CKD
Stage GFR Description
1 90+ Normal kidney function but urine or other abnormalities may point to kidney disease
2 60-89 Mildly reduced kidney function, but urine or other abnormalities may point to kidney disease
3 30-59 Moderately reduced kidney function
4 15-29 Severely reduced kidney function
5 14 or less
Very severe, or endstage kidney failure (sometimes called established renal failure)

Prevalence of CKD
CKD NHANES AusDiab NEOERICA
I 3.3 0.92 3.0 2.03 4.3 10.9 4.24 0.2 0.3 0.175 0.1 0.003 0.04
• 15% of >65yr olds have CKD III-V• 60% of >75yr olds have CKD III-V
• ~8.8% of UK population have CKD 3-5 (3.5 million)

Prevalence of Chronic Kidney Disease (CKD) Stages by Age Group in NHANES 1988-1994 and 1999-2004

The aging kidney
• Heterogeneous• Loss of renal mass• Glomerular and interstitial
fibrosis• Reduced sodium handling• Acid-base balance• Water homeostasis
Macías-Núñez, J. F. and Cameron, J. S. Renal Function and Disease in the Elderly. 1987

What is normal in an elderly population?
• GFR decline of 0.8-1.4 ml/min/1.73m2/yr ?• How do you measure GFR?
– MDRD• Poorly validated in elderly• Poor concordance
– Cystatin-C• ?better detection of changes in GFR• Accuracy uncertain• No reference standard
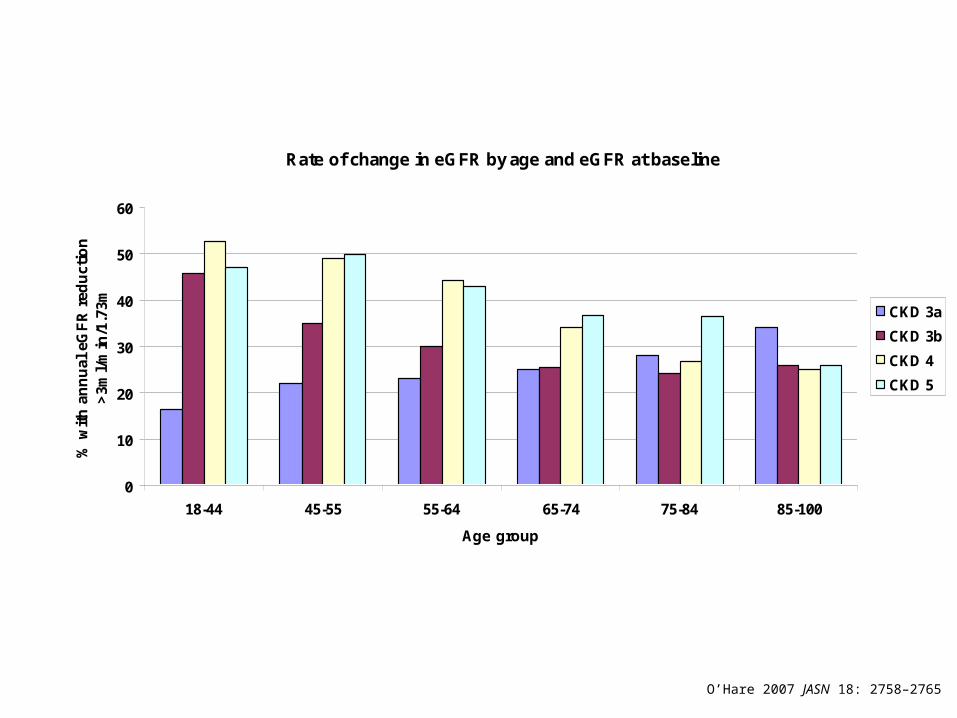
Rate of change in eGFR by age and eGFR at baseline
0
10
20
30
40
50
60
18-44 45-55 55-64 65-74 75-84 85-100
Age group
% w
ith
an
nu
al e
GF
R r
edu
ctio
n
>3m
l/m
in/1
.73m CKD 3a
CKD 3b
CKD 4
CKD 5
O’Hare 2007 JASN 18: 2758–2765

What happens to the elderly with CKD?
• No CKD– 0.07% risk of progression to ESKD over 3yr– Mortality 10%
• CKD 3– 1.1% risk of progression to ESKD over 3yr– Mortality 24.3%
• CKD 4– 17.6% risk of progression to ESKD over 3yr– Mortality 45.7%
Keith et al Arch Intern Med 2004;164:659

Effects of CKD on mortality and cardiovascular disease in the elderly - mean 75yr
0
1
2
3
4
5
6
7
8
All causedeath
CV death Non-CVdeath
Heart failure MI Stroke
Ev
en
ts/1
00
yrs
Normal kidney function
CKD 1-2
CKD 3-5
Shilpak at al Ann Int Med 2006;145:237

Baseline eGFR threshold below which risk for ESRDexceeded risk for death for each age group
O’Hare 2007 JASN 18: 2758–2765
What are the challenges in CKD?
• Identify patients at risk of progressive CKD• Reduce cardiovascular death

Progressive CKD
Oxidativestress
Endothelialdysfunction
Inflammation
Vascular compliance
Vitamin Ddeficiency
Dyslipidaemia
Age
Hypertension
Diabetes
African American
Smoking
Increasedhomocysteine
Primarykidney disease
ProteinuriaLow birth
weight
Poverty
Obesity

Progression of non-diabetic CKD
• Progression relates to haemodynamic + metabolic factors– Intra-glomerular hypertension– glomerular hypertrophy– albuminuria >1000 mg/day
• Reduce glomerular pressure and proteinuria


RAS blockade and proteinuria in non-diabetic CKD
• Benefit of ACEi if…– Proteinuria >1000mg/d– Even if normotensive– Combined with
• low Na+ diet• Diuretics
– ? 500-1000mg/d– ? if >70yr

Other drugs and proteinuria in non-diabetic CKD
• ARBs– Antiproteinuric effect equivalent to ACEi at 5-12 months– SMART trial – 269 patients– >1g/d proteinuria on 16mg candesartan– 33% reduction in proteinuria at 128mg candesartan
• Non-dihydropyridine calcium channel antagonists– Effective if >300mg/d irrespective of BP
• Lesser proteinuric effect with– β-blockers– Diuretics– α-blockers
Combination therapy in proteinuria
• ACEi + ARBs– Data in diabetic nephropathy– Limited data in non-diabetic proteinuria– No data to show improved renal outcome
• ACEi +/- ARB + spironolactone– Further reduction in proteinuria– Not on maximum dose of ACEi– Risk of hyperkalaemia

Pragmatic approach to proteinuria in CKD
1. ACEI
2. or ARB
3. + loop diuretic
4. Think about– ACE + ARB – ACE + spironolactone – Non-dihydropyridine calcium channel blockers

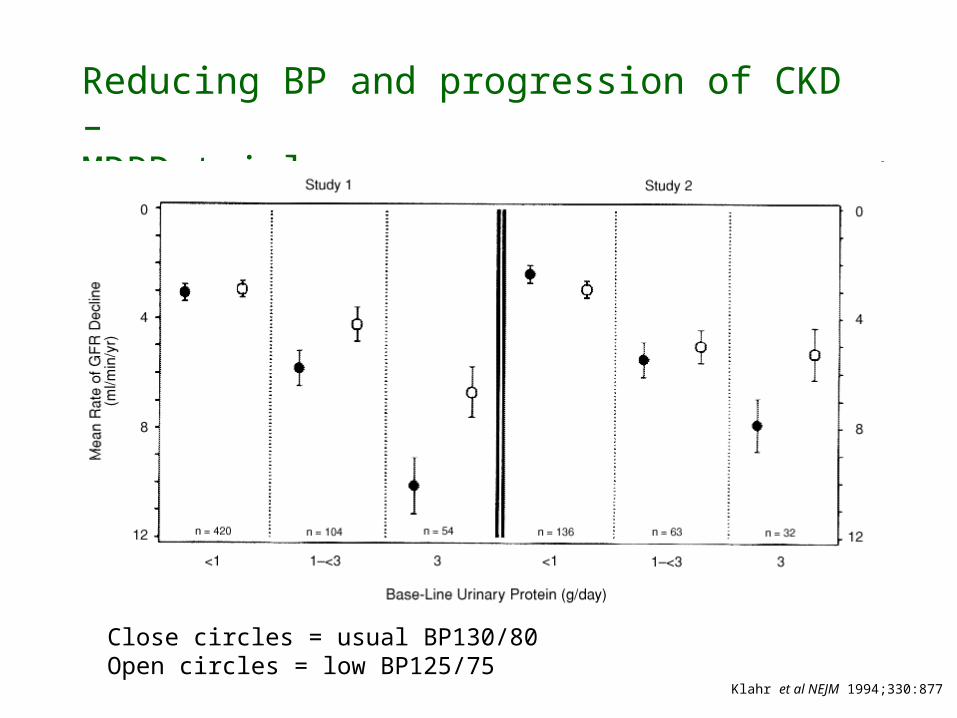
Reducing BP and progression of CKD – MDRD trial
Close circles = usual BP130/80Open circles = low BP125/75
Klahr et al NEJM 1994;330:877

Other trials
• African American Study of Kidney Disease (AASK)– Ramipril more effective than amlodipine or metoprolol in
African Americans– No difference in GFR decline between 128/78 and 141/85 – 22% reduction in composite with ACEi (GFR decline, ESKD
and death)
• Meta-analysis– Risk of progression correlates with:
• Proteinuria >500mg/d• Systolic >120
Wright et al JAMA 2002;288;2421

ACEi in elderly with CKD?
• All CKD trials excluded >70yr olds • More side effects with ACEi
– Hypotension– Hyperkalaemia
• Elderly less likely to have proteinuria– NHANES– >70 yrs + eGFR <60 + ACR >30 = 13%
• Absolute indication?– Proteinuria >1g (uPCR >100)
“Recommendations”
• Target BP…….– Proteinuria low: ACR<70 or PCR<100
• Target BP <140/90 (NICE suggests 130-139/90)
– Proteinuria high: ACR>70 or PCR>100 • Target BP <130/80 (NICE suggests 120-
129/80)• ACEi
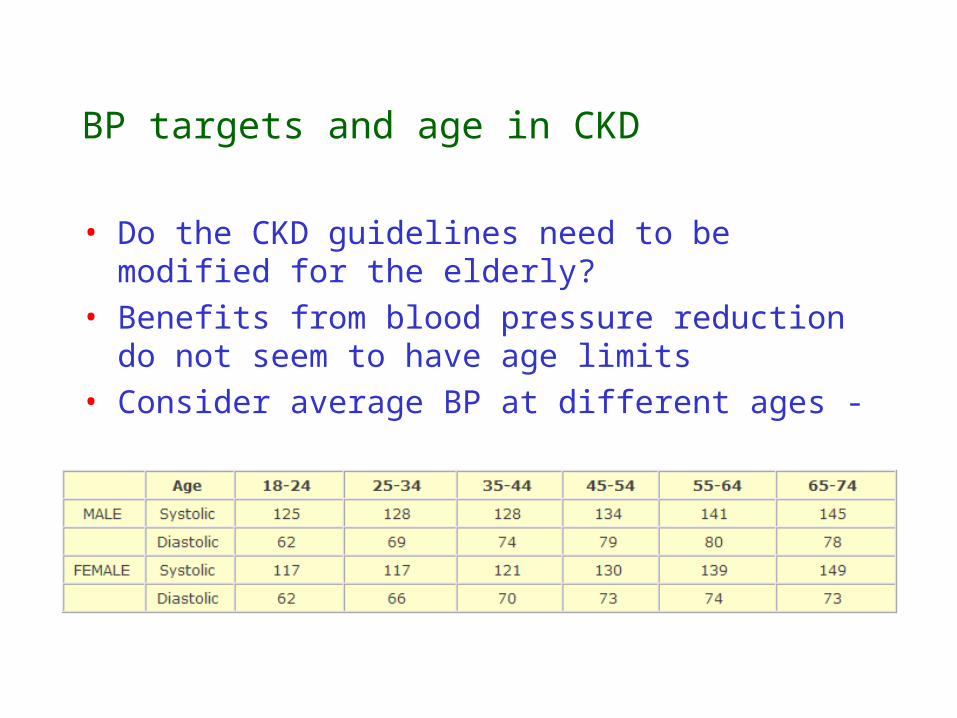
BP targets and age in CKD
• Do the CKD guidelines need to be modified for the elderly?
• Benefits from blood pressure reduction do not seem to have age limits
• Consider average BP at different ages -
Any other strategies to reduce progression or CV risk?
• Lipid lowering therapy?– SHARP– 9500 pts with CKD– Simvastatin vs simva+ezetimibe vs placebo– Composite of major vascular event (MI or stroke)– Reporting Nov 2010
• Correct anaemia with EPO?

Functional ability in the elderly with CKD
• 3x more likely to be frail than if normal renal function (10% vs 4%)– Associated with increased hospitalisation– Institutionalisation– Death
• Increased falls– 30%/yr of >75yr olds with ESKD
• Cognitive decline– 70% of >55yr olds with ESKD
• Nutrition• Poor cardiovascular fitness

What happens to elderly patients with progressive CKD?
“The aim of dialysis is not only to prolong life but also to restore quality by permitting a sufficiently independent existence with minimal support”

UK Renal Registry 11th Annual Report
Figure 7.3b: Kaplan-Meier 10-year survival of incident patients 1997-2006 cohort (from day 0), w ith censoring at transplantation
0
10
20
30
40
50
60
70
80
90
100
0.0 0.5 1.0 1.5 2.0 2.5 3.0 3.5 4.0 4.5 5.0 5.5 6.0 6.5 7.0 7.5 8.0 8.5 9.0 9.5 10.0
Period (years)
Perc
enta
ge s
urv
ival
18-34
35-4445-54
55-6465-74
75+
40
45
50
55
60
65
70
75
80
85
90
95
100
18-34
35-44
45-54
55-64
65-74
75-84
85+ 18-34
35-44
45-54
55-64
65-74
75-84
85+ 18-34
35-44
45-54
55-64
65-74
75-84
85+
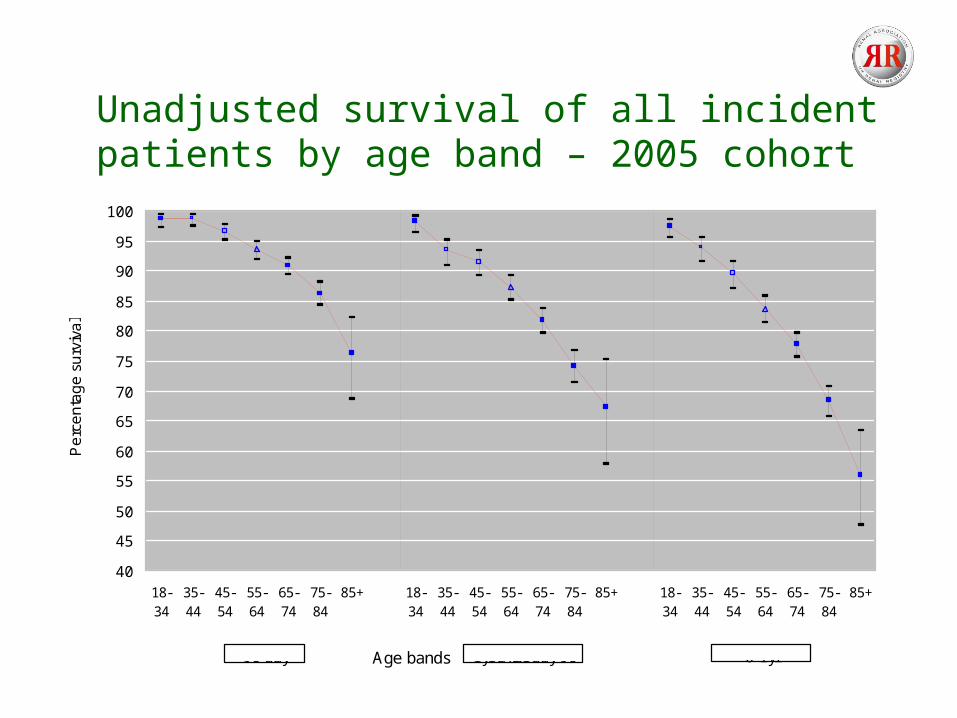
Age bands
Pe
rce
nta
ge
su
rviv
al
90 day 1yr after day 90 0-1yr
Unadjusted survival of all incident patients by age band – 2005 cohort

Figure 3.5: Incident rates by age and gender in 2007
0
100
200
300
400
500
600
700
20-2
4
25-2
9
30-3
4
35-3
9
40-4
4
45-4
9
50-5
4
55-5
9
60-6
4
65-6
9
70-7
4
75-7
9
80-8
4
85+
Age band
Rat
e pe
r m
illio
n po
pula
tion
MalesAll UKFemales

Patients with multiple co-morbidities may not benefit from dialysis
• Can we predict those who are likely to do poorly?
• Renal association and The Gold Standards Framework– “ if patient should have at least 1 core and 1 disease specific
indicator then that a patient may benefit from a palliative care approach”
– Core indicators are likely to be• Recent, significant functional decline (loss of ADLs)• Dependency in 3 or more ADLs• Multiple co-morbidities• Weight loss• Serum albumin less than 25• Karnofsky score less than or equal to 50%
Conservative management of CKD 5
• Outlined in the NSF
“Patients with progressive renal failure in whom dialysis is deemed inappropriate or who choose not to start RRT should continue to receive the benefit of the resources available to the renal service to provide a robust support package.”
• Supportive care should be offered as alternative to dialysis– Does NOT mean no treatment– Continued support from multidisciplinary team– Symptom treatment– Treatment of anaemia with erythropoietin

What’s the evidence?
• Study done at The Lister– Cohort of low clearance pts 19% (63)
recommended for palliative therapy, pts more functionally impaired but co-morbidity score not an independent factor
– 10 opted for dialysis – median survival on dialysis 8.3 m,vs 6.3 m (NS)– death in hospital: dialysis 65% vs palliative 27%

Dialysis vs conservative care
Murtagh et al NDT 2007;22:1955–1962
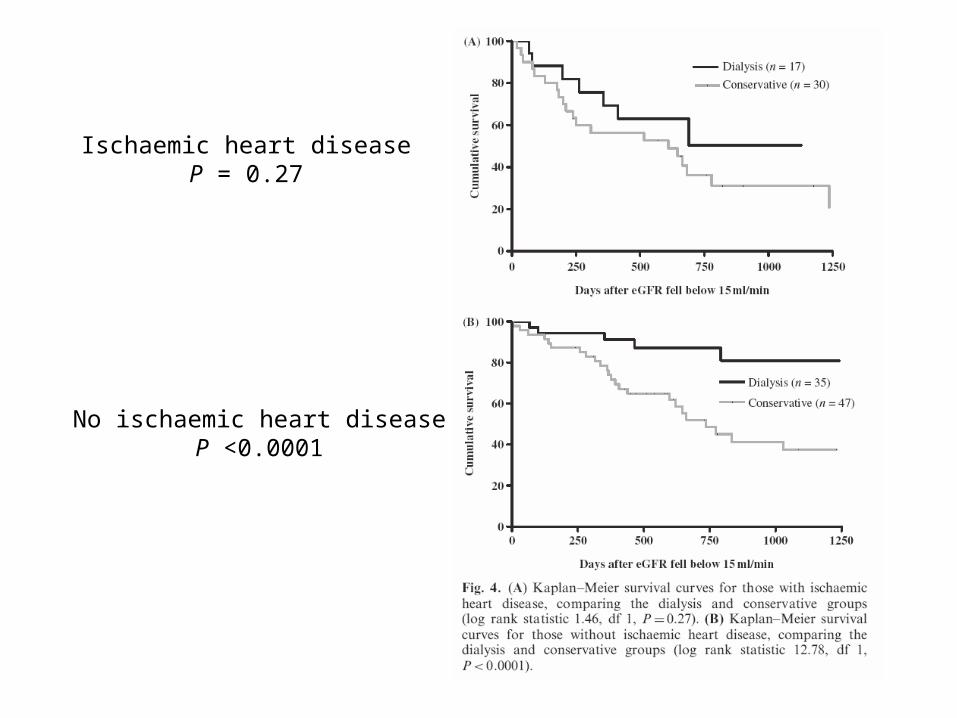
Ischaemic heart diseaseP = 0.27
No ischaemic heart diseaseP <0.0001
Dialysis in nursing home residents
• “treatment may improve functioning and/or alleviate symptoms, even if it does not extend life”
• 3,702 nursing home residents with ESRD (mean age 73.4y
• MDS-ADL score
Tamura et al NEJM 2009: 361, 1539–1547

Tamura et al NEJM 2009: 361, 1539–1547
Functional status before dialysis was maintained
in only 13% of survivors

To summarise….
• Majority of CKD in elderly– Non-proteinuric– Non-progressive
• CKD guidelines are not one-size-fits-all
• The main challenge is reducing cardiovascular death
• Which patients will benefit from dialysis?