34
HYPERTENSION Principle of Drug Therapy Mohammad Ilyas, M.D. Assistant Clinical Professor University of Florida / Health Sciences Center Jacksonville, Florida USA 1
| Date post: | 09-Aug-2015 |
| Category: |
Education |
| Upload: | university-of-florida |
| View: | 69 times |
| Download: | 2 times |
HYPERTENSIONPrinciple of Drug Therapy
Mohammad Ilyas, M.D.
Assistant Clinical Professor
University of Florida / Health Sciences Center
Jacksonville, Florida USA
1
Why Treat HTN?
All Symptomatic patients, treatment is Mandatory:
Damage to the vascular epithelium, paving the path for
atherosclerosis (IHD, CVA) or nephropathy due to high
intra-glomerular pressure
Reduction of the blood pressure by 5 mmHg can
decrease the risk of stroke by 34%, of ischaemic heart
disease by 21%.
Hypertension, even asymptomatic needs treatment
2
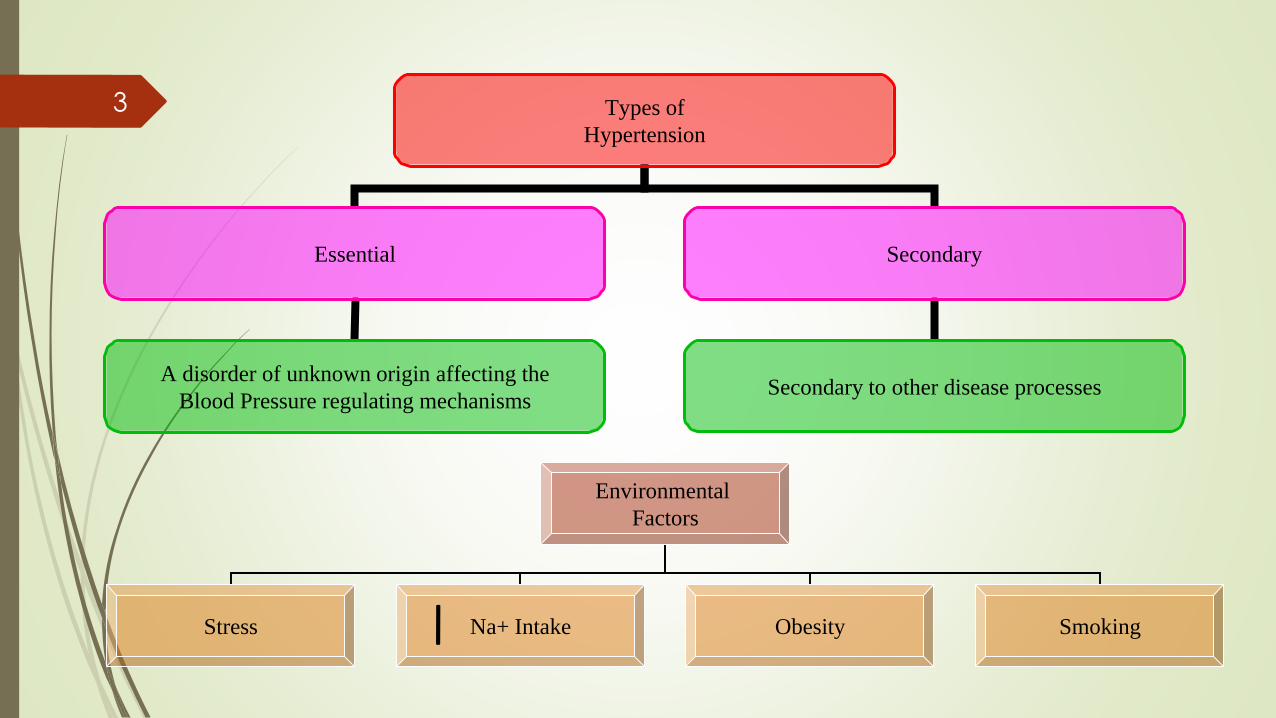
Types of
Hypertension
Essential Secondary
A disorder of unknown origin affecting the
Blood Pressure regulating mechanismsSecondary to other disease processes
Environmental
Factors
Stress Na+ Intake Obesity Smoking
3
Risk factors for CVD
1. Age above 55 and 65 in Men and Woman respectively
2. Family History
3. Smoking
4. DM and Dyslipidemia
5. Hypertension
6. Obesity
7. Microalbuminuria
4
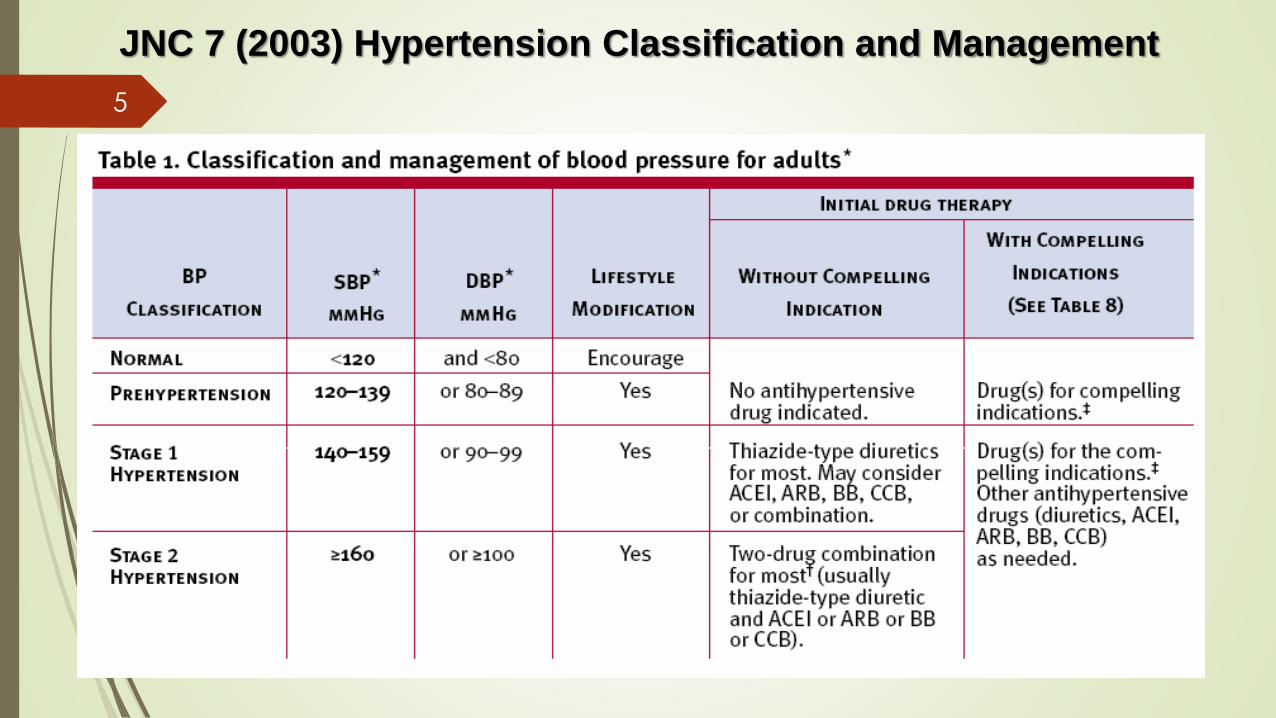
JNC 7 (2003) Hypertension Classification and Management
5
JAMA. 2013;():. doi:10.1001/jama.2013.284427
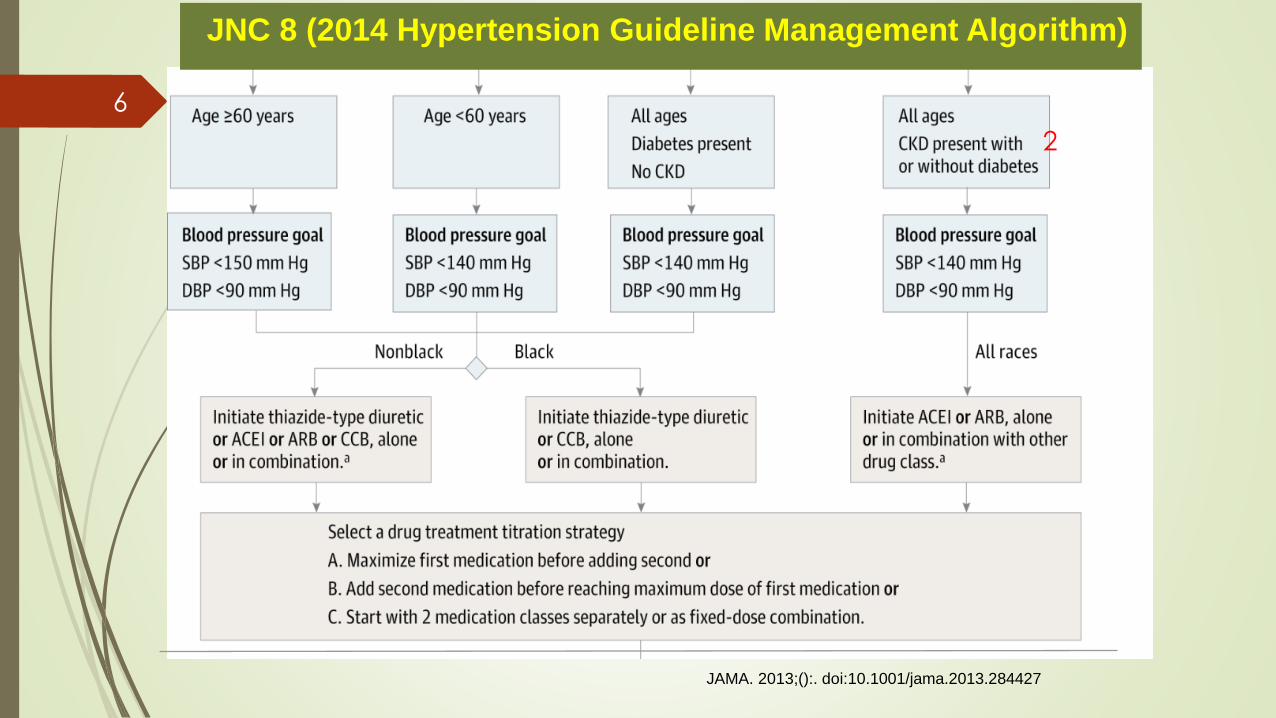
JNC 8 (2014 Hypertension Guideline Management Algorithm)
2
6
JAMA. 2013;():. doi:10.1001/jama.2013.284427
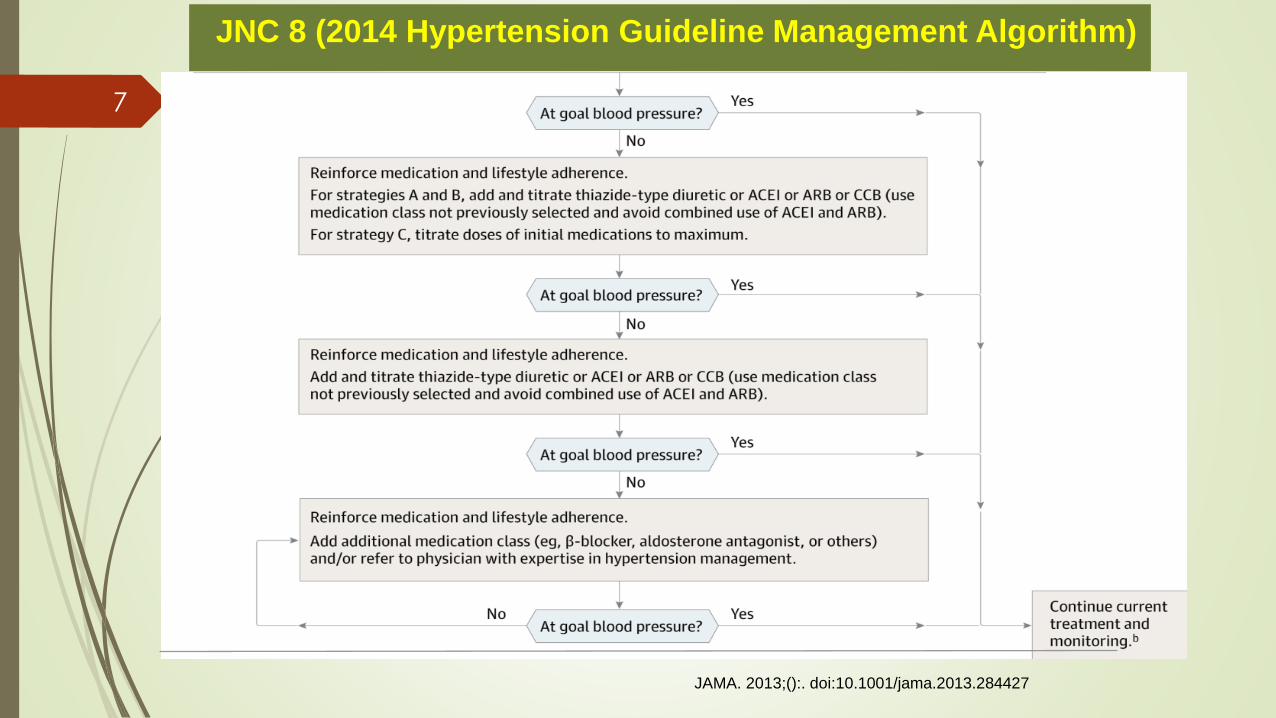
JNC 8 (2014 Hypertension Guideline Management Algorithm)
7
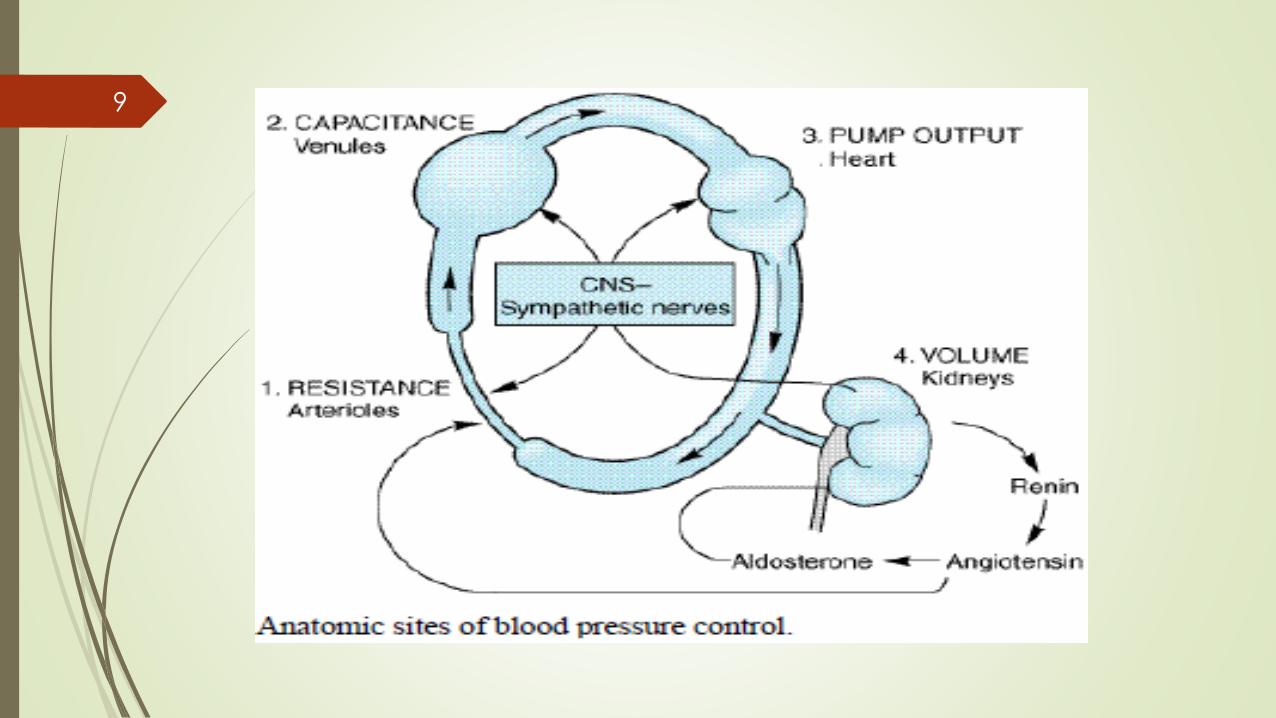
Blood Pressure Regulation
Blood Pressure = Cardiac output (CO) X Resistance to passage of blood through pre-capillary arterioles (PVR)
Physiologically CO and PVR is maintained minute to minute by –arterioles (1) post-capillary venules (2) and Heart (3)
Kidney is the fourth site – volume of intravascular fluid
Baroreflex, humoral mechanism and renin-angiotensin-aldosterone system regulates the above 4 sites
Local agents like Nitric oxide
In hypertensives – Baroreflex and renal blood-volume control system – set at higher level
All antihypertensives act via interfering with normal mechanisms
8
9

Baroreceptor reflex arc
Postural baroreflex:
10
The Renal response
Long-term blood pressure control – by controlling blood volume
Reduction in renal pressure - intrarenal redistribution of pressure and increased absorption of salt and water
Decreased pressure in renal arterioles and sympathetic activity –renin production – angiotensin II production
Angiotensin II:
Causes direct constriction of renal arterioles
Stimulation of aldosterone synthesis – sodium absorption and increase in intravascular blood volume
11

12

Start one drug, titrate to maximum dose, and then add a second drug
Start one drug and then add a second drug before achieving maximum dose of the initial drug
Begin with 2 drugs at the same time, either as 2 separate pills or as a single pill combination
Strategies to Dose of Antihypertensive Drugs13
Principle of Pharmacologic Therapy
Initial mono-therapy in uncomplicated hypertension
Thiazide diuretics, long-acting calcium channel blockers and ACE
inhibitors or angiotensin II receptor blockers.
Beta blockers are not commonly used for initial mono therapy in
the absence of a specific indication
Combination therapy - with drugs from different classes
has a substantially greater blood pressure lowering effect
than doubling the dose of a single agent.
14
Pre-hypertension
Individuals who are pre-hypertensive are not candidates for drug therapy but
Should be firmly and unambiguously advised to practice lifestyle modification
Those with pre-HTN, who also have diabetes or kidney disease, drug therapy is indicated if a trial of lifestyle modification fails to reduce their BP to 130/80 mmHg or less.
15
Isolated Systolic Hypertension
Not distinguished as a separate entity as far as management is concerned.
SBP should be primarily considered during treatment and not just diastolic BP.
Systolic BP is more important cardiovascular risk factor after age 50.
Diastolic BP is more important before age 50.
16
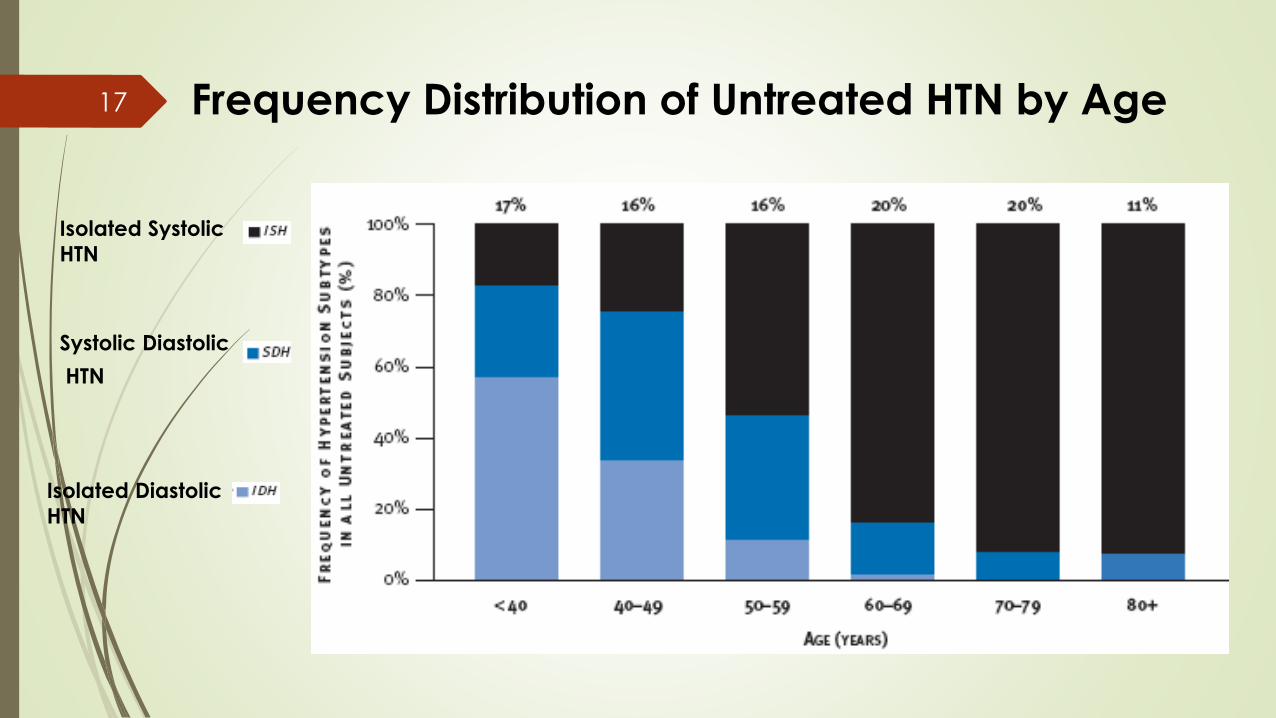
Frequency Distribution of Untreated HTN by Age17
Isolated Systolic
HTN
Isolated Diastolic
HTN
Systolic Diastolic
HTN

Treatment of Hypertension
7 compelling Indications:
Heart failure
Coronary artery disease
H/o MI
H/o stroke
Diabetes
Chronic Renal failure
18
You must know
Classification of Antihypertensive
Antihypertensive mechanisms:
Diuretics, ACE inhibitors, ARBs, Beta-blockers, alpha-blockers,
CCBs, Vasodilators and central sympatholytics
Pateint status of Drugs
Preparation and dosage of commonly used drugs.
Common Adverse effects of Drugs
19
General principles
Stage I:
Start with a single most appropriate drug with a low dose.
Preferably start with Thiazides. Others like beta-blockers, CCBs, ARBs and ACE inhibitors may also be considered. CCB – in case of elderly and stroke prevention. If required increase the dose moderately
Partial response or no response – add from another group of drug, but remember it should be a low dose combination
If not controlled – change to another low dose combination
In case of side effects lower the dose or substitute with other group
Stage 2: Start with 2 drug combination – one should be diuretic
20
Combination therapy
In clinical practice a large number of patients require combination therapy – the combination should be rational and from different patterns of haemodynamic effects
Sympathetic inhibitors (not beta-blockers) and vasodilators + diuretics
Diuretics, CCBs, ACE inhibitors and vasodilators + beta blockers (blocks renin release)
Hydralazine and CCBs + beta-blockers (tachycardia countered)
ACE inhibitors + diuretics
3 (three) Drug combinations: CCB+ACE/ARB+diuretic; CCB+Beta blocker+ diuretic; ACEI/ARB+ beta blocker+diuretic
21
Principle of Combination
Never combine:
Alpha or beta blocker and clonidine - antagonism
Nifedepine and diuretic synergism
Hydralazine with prazosin
Diltiazem and verapamil with beta blocker – bradycardia
Methyldopa and clonidine
Hypertension and pregnancy:
No drug is safe in pregnancy
Avoid diuretics, propranolol, ACE inhibitors, Sodium nitroprusside etc
Safer drugs: Hydralazine, Methyldopa, cardioselective beta blockers and prazosin
22
Nocturnal therapy
The average nocturnal blood pressure is approximately 15
percent lower than daytime values.
Failure of the blood pressure to fall by at least 10 percent
during sleep is called "non-dipping," and is a stronger
predictor of adverse cardiovascular outcomes than daytime
blood pressure.
Shifting at least one antihypertensive medication from the
morning to the evening both may restore the normal
nocturnal blood pressure dip, and reduces 24-hour mean
blood pressure.
Nocturnal antihypertensive therapy may reduce the
incidence of cardiovascular disease
23
Resistant hypertension
Resistance is usually defined as a diastolic blood pressure
above 90 mmHg despite intake of three or more
antihypertensive medications including a diuretic.
Suboptimal therapy
Extracellular volume expansion
Poor compliance with medical or dietary therapy
Identifiable or secondary hypertension
Office or "white coat" hypertension
Ingestion of substances that can elevate the blood
pressure
24
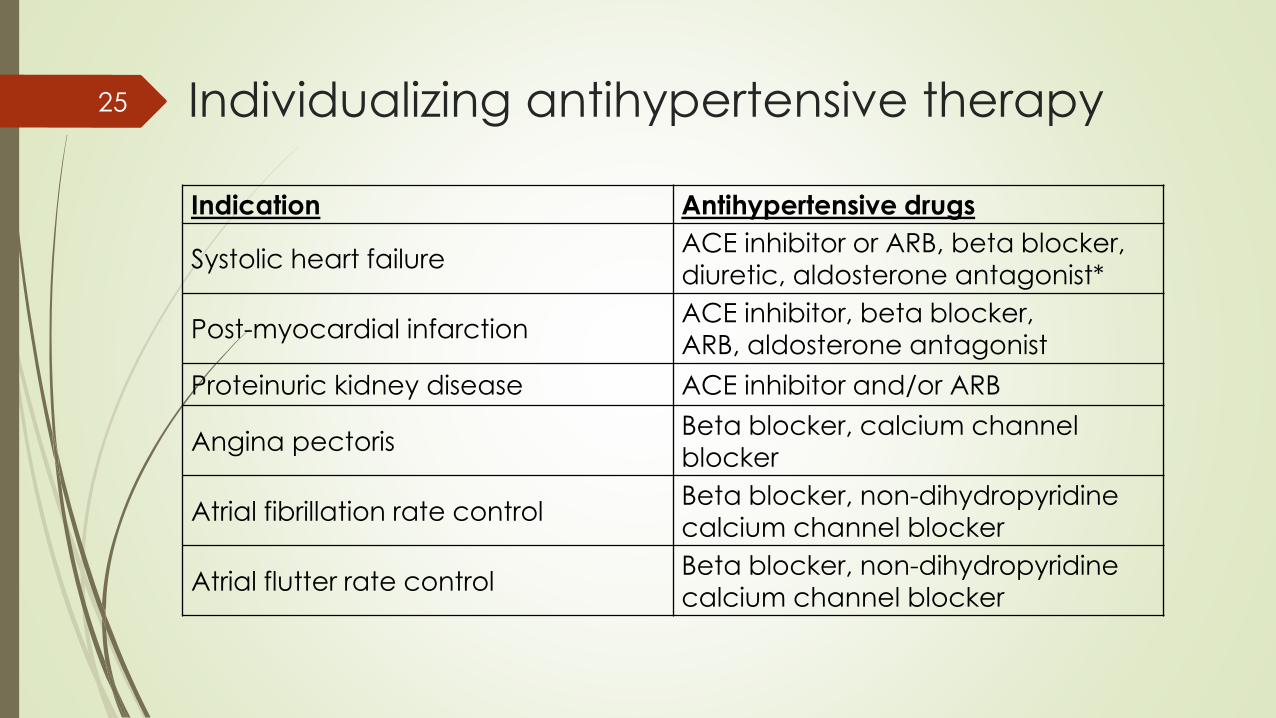
Individualizing antihypertensive therapy
Indication Antihypertensive drugs
Systolic heart failureACE inhibitor or ARB, beta blocker, diuretic, aldosterone antagonist*
Post-myocardial infarctionACE inhibitor, beta blocker,
ARB, aldosterone antagonist
Proteinuric kidney disease ACE inhibitor and/or ARB
Angina pectorisBeta blocker, calcium channel
blocker
Atrial fibrillation rate control Beta blocker, non-dihydropyridinecalcium channel blocker
Atrial flutter rate control Beta blocker, non-dihydropyridine
calcium channel blocker
25

Individualizing antihypertensive therapy
Benign prostatic hyperplasia Alpha blocker
Essential tremorBeta blocker
(noncardioselective)
Hyperthyroidism Beta blocker
MigraineBeta blocker, calcium
channel blocker
Osteoporosis Thiazide diuretic
Raynaud's syndromeDihydropyridine calcium
channel blocker
26
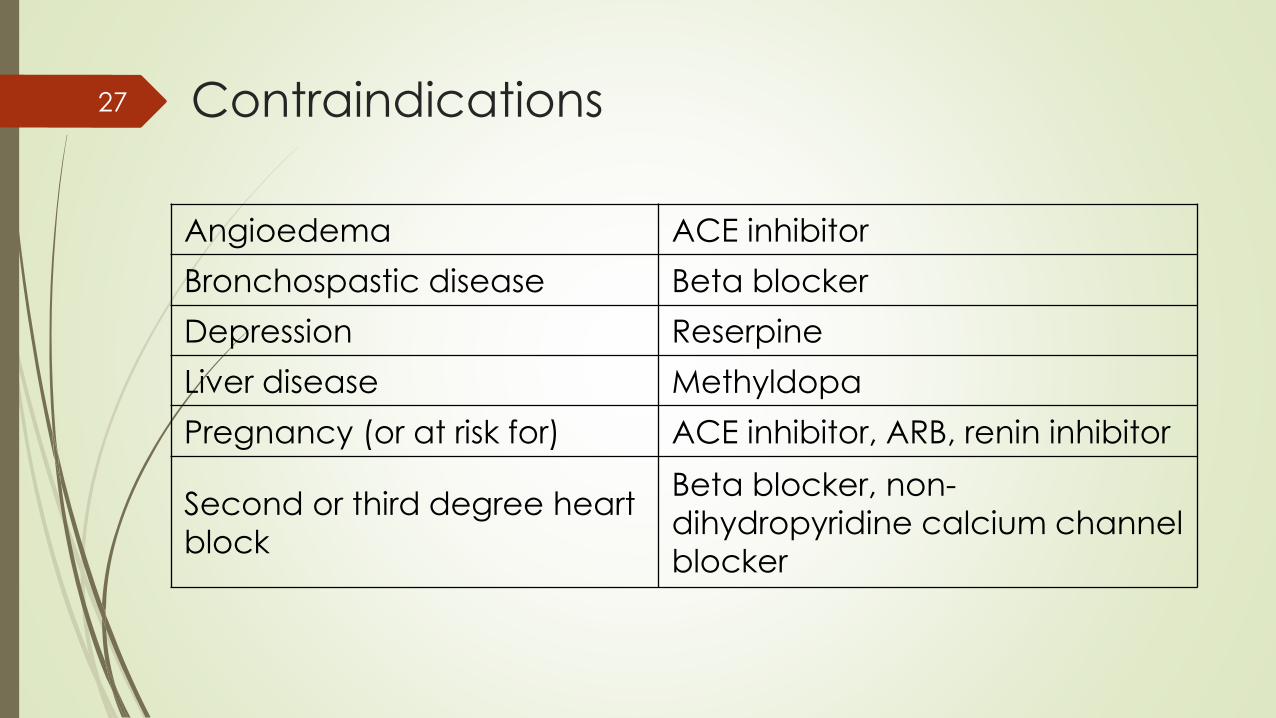
Contraindications
Angioedema ACE inhibitor
Bronchospastic disease Beta blocker
Depression Reserpine
Liver disease Methyldopa
Pregnancy (or at risk for) ACE inhibitor, ARB, renin inhibitor
Second or third degree heart
block
Beta blocker, non-
dihydropyridine calcium channel
blocker
27
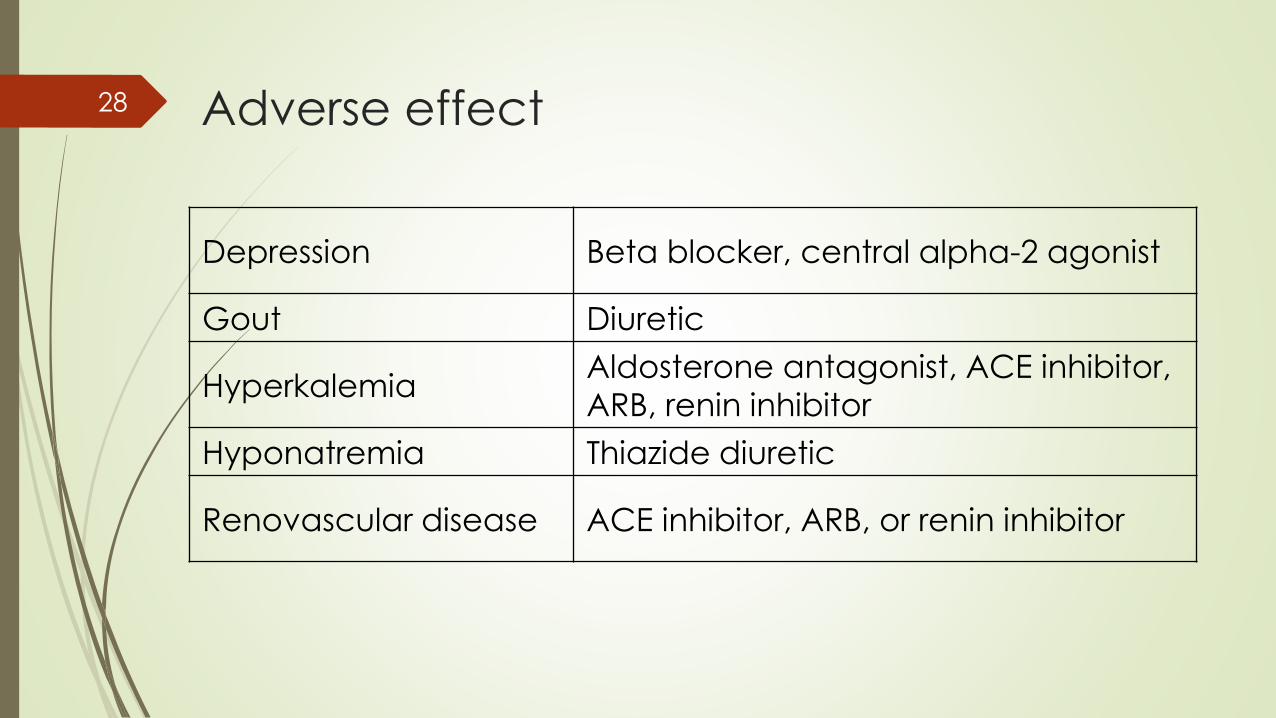
Adverse effect
Depression Beta blocker, central alpha-2 agonist
Gout Diuretic
HyperkalemiaAldosterone antagonist, ACE inhibitor,
ARB, renin inhibitor
Hyponatremia Thiazide diuretic
Renovascular disease ACE inhibitor, ARB, or renin inhibitor
28
Discontinuing therapy
If the BP is well control on monotherapy
55 % of patients remain normotensive for at least one to two years
More gradual tapering of drug dose is indicated in well-controlled
patients taking multiple drugs
Abrupt cessation of therapy with a short-acting beta-blocker (such
as propranolol) or the short-acting alpha-2-agonist clonidine can
lead to a potentially fatal withdrawal syndrome.
Gradual discontinuation of these agents over a period of weeks
should prevent this problem.
29
Pearls
The only thiazide that will work with an elevated creatinine is metolazone (zaroxolyn)
If creatinine is elevated than use a loop diuretic
If potassium is elevated, evaluate current meds and use a diuretic
If potassium is low – ask why
If edema present – and ask why
Elderly patients benefit from blood pressure management
Black patients benefit from ACE/ARB – may need to use larger doses to obtain BP lowering effect
30
Pearls Cont.
Metabolic acidosis and hyperkalemai?
Take blood pressure periodically lying and
standing so as not to miss supine (orthostatic)
hypertension associated with autonomic
insufficiency – this is treated differently
31

Treatment failure – Why ?
“Drugs don’t work in patients who
don’t take them”
C. Everett Koop, MD, Former US Surgeon General
32
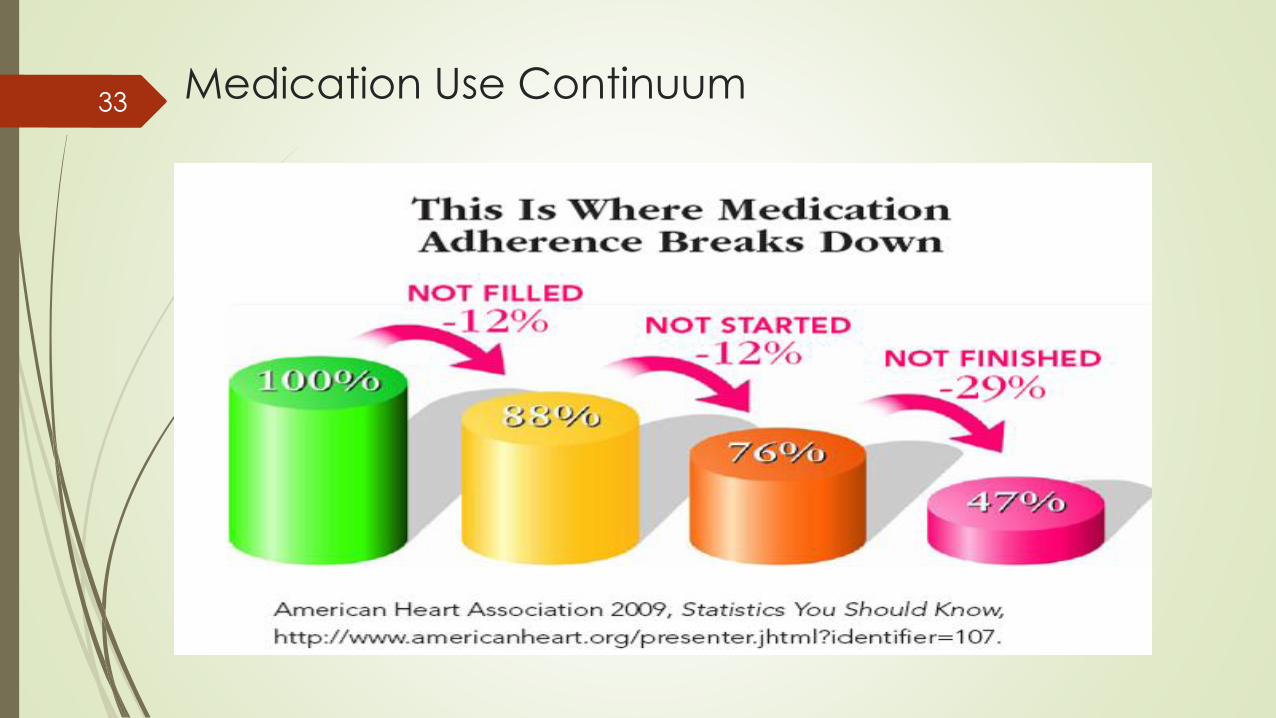
Medication Use Continuum33

Osterberg, L. et al. N Engl J Med 2005;353:487-497
Adherence to Medication According to Frequency of Doses
34

















