Hyporesponsiveness to social and nonsocial sensory stimuli in children with autism, children with developmental delays, and typically developing children GRACE T. BARANEK, LINDA R. WATSON, BRIAN A. BOYD, MICHELE D. POE, FABIAN J. DAVID, AND LORIN MCGUIRE University of North Carolina at Chapel Hill Abstract This cross-sectional study seeks to (a) describe developmental correlates of sensory hyporesponsiveness to social and nonsocial stimuli, (b) determine whether hyporesponsiveness is generalized across contexts in children with autism relative to controls, and (c) test the associations between hyporesponsiveness and social communication outcomes. Three groups of children ages 11–105 months (N ¼ 178; autism ¼ 63, developmental delay ¼ 47, typical development ¼ 68) are given developmental and sensory measures including a behavioral orienting task (the Sensory Processing Assessment). Lab measures are significantly correlated with parental reports of sensory hyporesponsiveness. Censored regression models show that hyporesponsiveness decreased across groups with increasing mental age (MA). Group differences are significant but depend upon two-way interactions with MA and context (social and nonsocial). At a very young MA (e.g., 6 months), the autism group demonstrates more hyporesponsiveness to social and nonsocial stimuli (with larger effects for social) than developmental delay and typically developing groups, but at an older MA (e.g., 60 months) there are no significant differences. Hyporesponsiveness to social and nonsocial stimuli predicts lower levels of joint attention and language in children with autism. Generalized processes in attention disengagement and behavioral orienting may have relevance for identifying early risk factors of autism and for facilitating learning across contexts to support the development of joint attention and language. There is a paucity of developmental research on the nature of unusual responses to sensory stimuli in children with autism despite numerous phenomenological reports that these prob- lems exist from an early age (Grandin, 1996; Hart, 1991; Jones, Quigney, & Huws, 2003). Prevalence rates of unusual sensory responses are noted in 69% to 90% of preschoolers with autism (Baranek, David, Poe, Stone, & Watson, 2006; Ben-Sasson et al., 2009; Leekam, Nieto, Libby, Wing, & Gould, 2007). Researchers have characterized some of these unusual sensory features into two behavioral response pat- terns: hyperresponsiveness and hyporesponsiveness (Baranek et al., 2006; Ben-Sasson et al., 2009; Hirstein, Iversen, & Ra- machandran, 2001; Miller, Anzalone, Lane, Cermak, & Ol- sten, 2007; O’Neill & Jones, 1997; Schneider et al., 2008). Hyperresponsiveness is an exaggerated behavioral response to sensory stimuli (e.g., aversion to lights, covering ears to sounds, or avoidance of touch). Hyporesponsiveness refers to lack of a behavioral response or insufficient intensity of re- sponse to sensory stimuli (e.g., lack of orienting to novel sounds or diminished response to pain). Psychophysiological studies in autism and related populations have validated these two behavioral constructs (Hirstein et al., 2001; Miller, Reis- man, McIntosh, & Simon, 2001). These two sensory response patterns (hyperresponsive- ness and hyporesponsiveness) are reported to coexist in chil- dren with autism (Baranek et al., 2006; Greenspan & Wieder, 1997; Hirstein et al., 2001; Miller et al., 2007); however, hyporesponsiveness appears more prevalent and specific to autism during early childhood (Baranek et al., 2006; Ben- Sasson et al., 2009; Rogers & Ozonoff, 2005). Some studies have matched autism samples to typical development (TD) controls, but few included developmental delay (DD) com- parison groups to determine the uniqueness of these features. One study utilizing a parent-report questionnaire demon- strated that a pattern of sensory hyporesponsiveness signifi- cantly distinguished children with autism from controls, both TD and DD, with comparable mental ages (MAs; Bara- nek et al., 2006). The developmental nature of sensory hyporesponsiveness in children with autism has not been fully explicated, and its association with broader developmental outcomes is unclear. Results from cross-sectional studies utilizing parent-report formats have been mixed, with some researchers reporting sensory features increasing (e.g., Talay-Ongan & Wood, Address correspondence and reprint requests to: Grace T. Baranek, Divi- sion of Occupational Science (CB 7122), University of North Carolina at Chapel Hill, Chapel Hill, NC 27599-7122; E-mail: [email protected]. This research was supported in part by a grant from the National Institute for Child Health and Human Development (R01-HD42168). We thank the fam- ilies whose participation made this study possible and the staff who collected and processed data for this project. Development and Psychopathology 25 (2013), 307–320 # Cambridge University Press 2013 doi:10.1017/S0954579412001071 307
Transcript
Hyporesponsiveness to social and nonsocial sensory stimuli inchildren with autism, children with developmental delays, andtypically developing children
GRACE T. BARANEK, LINDA R. WATSON, BRIAN A. BOYD, MICHELE D. POE, FABIAN J. DAVID, AND
LORIN MCGUIREUniversity of North Carolina at Chapel Hill
Abstract
This cross-sectional study seeks to (a) describe developmental correlates of sensory hyporesponsiveness to social and nonsocial stimuli, (b) determine whetherhyporesponsiveness is generalized across contexts in children with autism relative to controls, and (c) test the associations between hyporesponsivenessand social communication outcomes. Three groups of children ages 11–105 months (N¼ 178; autism¼ 63, developmental delay¼ 47, typical development¼68) are given developmental and sensory measures including a behavioral orienting task (the Sensory Processing Assessment). Lab measures are significantlycorrelated with parental reports of sensory hyporesponsiveness. Censored regression models show that hyporesponsiveness decreased across groups withincreasing mental age (MA). Group differences are significant but depend upon two-way interactions with MA and context (social and nonsocial). At a veryyoung MA (e.g., 6 months), the autism group demonstrates more hyporesponsiveness to social and nonsocial stimuli (with larger effects for social) thandevelopmental delay and typically developing groups, but at an older MA (e.g., 60 months) there are no significant differences. Hyporesponsiveness to socialand nonsocial stimuli predicts lower levels of joint attention and language in children with autism. Generalized processes in attention disengagement andbehavioral orienting may have relevance for identifying early risk factors of autism and for facilitating learning across contexts to support the development ofjoint attention and language.
There is a paucity of developmental research on the nature ofunusual responses to sensory stimuli in children with autismdespite numerous phenomenological reports that these prob-lems exist from an early age (Grandin, 1996; Hart, 1991;Jones, Quigney, & Huws, 2003). Prevalence rates of unusualsensory responses are noted in 69% to 90% of preschoolerswith autism (Baranek, David, Poe, Stone, & Watson, 2006;Ben-Sasson et al., 2009; Leekam, Nieto, Libby, Wing, &Gould, 2007). Researchers have characterized some of theseunusual sensory features into two behavioral response pat-terns: hyperresponsiveness and hyporesponsiveness (Baraneket al., 2006; Ben-Sasson et al., 2009; Hirstein, Iversen, & Ra-machandran, 2001; Miller, Anzalone, Lane, Cermak, & Ol-sten, 2007; O’Neill & Jones, 1997; Schneider et al., 2008).Hyperresponsiveness is an exaggerated behavioral responseto sensory stimuli (e.g., aversion to lights, covering ears tosounds, or avoidance of touch). Hyporesponsiveness refersto lack of a behavioral response or insufficient intensity of re-
sponse to sensory stimuli (e.g., lack of orienting to novelsounds or diminished response to pain). Psychophysiologicalstudies in autism and related populations have validated thesetwo behavioral constructs (Hirstein et al., 2001; Miller, Reis-man, McIntosh, & Simon, 2001).
These two sensory response patterns (hyperresponsive-ness and hyporesponsiveness) are reported to coexist in chil-dren with autism (Baranek et al., 2006; Greenspan & Wieder,1997; Hirstein et al., 2001; Miller et al., 2007); however,hyporesponsiveness appears more prevalent and specific toautism during early childhood (Baranek et al., 2006; Ben-Sasson et al., 2009; Rogers & Ozonoff, 2005). Some studieshave matched autism samples to typical development (TD)controls, but few included developmental delay (DD) com-parison groups to determine the uniqueness of these features.One study utilizing a parent-report questionnaire demon-strated that a pattern of sensory hyporesponsiveness signifi-cantly distinguished children with autism from controls,both TD and DD, with comparable mental ages (MAs; Bara-nek et al., 2006).
The developmental nature of sensory hyporesponsivenessin children with autism has not been fully explicated, and itsassociation with broader developmental outcomes is unclear.Results from cross-sectional studies utilizing parent-reportformats have been mixed, with some researchers reportingsensory features increasing (e.g., Talay-Ongan & Wood,
Address correspondence and reprint requests to: Grace T. Baranek, Divi-sion of Occupational Science (CB 7122), University of North Carolina atChapel Hill, Chapel Hill, NC 27599-7122; E-mail: [email protected].
This research was supported in part by a grant from the National Institute forChild Health and Human Development (R01-HD42168). We thank the fam-ilies whose participation made this study possible and the staff who collectedand processed data for this project.
Development and Psychopathology 25 (2013), 307–320# Cambridge University Press 2013doi:10.1017/S0954579412001071
2000) and others reporting the same features decreasing (e.g.,Baranek et al., 2006; Leekam et al., 2007) with age. Discre-pancies across studies may be attributable to methodologicaldifferences in matching procedures (e.g., nature of compari-son groups), sampling procedures (e.g., broad or narrowage range), analytic procedures (e.g., treating age as a categor-ical versus continuous variable), or outcome variables (e.g.,format and sensitivity of measures).
Two studies (Lane, Young, Baker, & Angley, 2010; Liss,Saulnier, Fein, & Kinsbourne, 2006) suggest that there maybe an association between parent-reported levels of sensoryhyporesponsiveness and standardized measures of adaptivebehavior in a subgroup of children with autism. In addition,Liss et al. (2006) found poorer communication and social per-formance was related to high levels of hyporesponsiveness ina subgroup of school-aged children with autism. Uncoveringdevelopmental differences in hyporesponsive sensory pat-terns across various stimuli and contexts with more rigorousmethodologies, and in comparison to children with other de-velopmental delays as well as children with TD, may eluci-date the pathogenesis of these features in autism.
Given the core deficits that define autism spectrum disor-ders (ASDs), researchers have debated whether hyporespon-siveness to sensory stimuli is a generalized phenomenon orwhether hyporesponsiveness is limited to social contexts inthis population (Baranek et al., 2006; Dawson, Meltzoff, Os-terling, Rinaldi, & Brown, 1998; Dawson et al., 2004; Mundy& Newell, 2007; Swettenham et al., 1998). The answer to thisquestion also has implications for understanding causalmechanisms underlying the development of autistic features.In theory, a young child who does not overtly respond tonovel sensory stimuli in the natural environment may missnumerous learning opportunities as well as socially contin-gent responses that are foundational to social communicationand subsequent adaptive development. Lack of response tosocial stimuli may be particularly detrimental to a child’slearning potential, because a substantial amount of knowl-edge early in development, and throughout the lifespan, is ac-quired through interactions with others. However, nonsocialsensory stimuli naturally occurring in the child’s environmentalso present rich opportunities for sharing attention, commu-nicating, and making meaning of those sensory experiences.
Behavioral orienting is one measure of a child’s respon-siveness to novel sensory events, and the development of sen-sory orienting often has been investigated in infants with TDusing gaze shifting paradigms in several prospective studies(Farroni, Simion, Umilta, & Barba, 1999; Hunnius & Geuze,2004; Johnson, 1990; Rothbart, Posner, & Rosicky, 1994).Newborn infants have intact orienting responses to a varietyof social (e.g., faces or voices) and nonsocial (e.g., lights flash-ing or geometric patterns) sensory stimuli, and latency of re-sponse decreases with maturation across the first year of life.By 4–5 months of age, infants with TD are able to disengageeasily from a competing stimulus in a central field to overtlyshift their visual attention to a novel stimulus in their periphery.These inhibitory responses of visual disengagement and gaze
shift are thus integral to orienting to novel sensory stimuli inthe presence of distracters and appear mediated by subcorticalmechanisms (e.g., superior colliculus) connecting with parietaland frontal structures that mature over time.
Some neuropsychological theories have focused primarilyon orienting deficits in the context of social stimuli to accountfor core symptoms in autism (Dawson et al., 1998, 2004;Swettenham et al., 1998), while others have implicated moregeneralized deficits in orienting and/or attention disengage-ment mechanisms that could explain hyporesponsiveness tosensory stimuli across both social and nonsocial contexts, aswell as downstream consequences on social communication(Harris, Courchesne, Townsend, Carper, & Lord, 1999;Townsend et al., 1999; Zwaigenbaum et al., 2005).
Orienting responses to naturally occurring social and non-social sensory stimuli have been studied as a predictor of au-tism diagnostic status. Failure to attend appropriately to stim-uli in a social context (e.g., lack of response to a personcalling the child’s name) was frequently identified to beone of the earliest and specific clinical manifestations of au-tism (Dawson et al., 1998; Landa, Holman, & Garrett-Mayer,2007; Nadig et al. 2007; Wetherby, Watt, Morgan, & Shum-way, 2007; Zwaigenbaum et al., 2005) and, furthermore, wasconsidered an important developmental precursor of joint at-tention (Dawson et al., 2004). Some studies have demon-strated that social orienting was correlated specifically withjoint attention and/or language in young children with autism(Dawson et al., 2004; Leekam & Ramsden, 2006). Nonsocialorienting to sensory stimuli has been less investigated. Daw-son and colleagues (1998) reported no statistically significantcorrelation between nonsocial orienting and joint attention inchildren with autism at an average chronological age (CA) of5 years. However, another noteworthy finding was that non-social orienting significantly discriminated between childrenwith autism and those with DD as well as TD (Dawson et al.,1998, 2004), suggesting the possibility of a more generalizeddeficit in orienting to sensory stimuli.
Some researchers suggest that development of joint atten-tion relies upon two interacting attention-regulating systems,the earlier-developing posterior (parietal) and the later-devel-oping anterior (frontal) neural networks (Posner & Rothbart,2007). The integration of these two generalized attention net-works is hypothesized to be deficient in autism, potentially re-sulting in impaired joint attention abilities (Mundy & Jarrold,2010; Mundy & Newell, 2007). Prospective studies havealso demonstrated that joint attention, especially response tobids from others, is predictive of rate of language growthinto the school years for children with autism (Siller & Sigman,2008). Thus, deficits in early-developing attentional systems,which may be measured in part by general impairments in ori-enting to social as well as nonsocial sensory stimuli, theoreti-cally may have cascading developmental consequences on la-ter-developing social communicative functions, including jointattention and language development, and profound effects onthe long-term prognosis of a child with autism (Dawsonet al., 2004; Mundy & Jarrold, 2010; Mundy & Neal, 2001).
G. T. Baranek et al.308
In summary, the existing literature suggests that youngchildren with autism have high levels of sensory features, par-ticularly hyporesponsiveness, or lack of orienting, to sensorystimuli. Although orienting to stimuli has been shown to bedeficient in autism, the results for nonsocial sensory stimulihave been mixed. Moreover, several neuropsychological the-ories purport a specific role for social orienting deficits as adevelopmental precursor for core social communicative im-pairments (e.g., joint attention and language) in autism; how-ever, orienting to nonsocial sensory stimuli has not been suf-ficiently investigated. Thus, questions still exist regardingwhether or not children with autism show a generalized pat-tern of sensory hyporesponsiveness and to what degree hy-poresponsiveness is affected by various contextual factors(social vs. nonsocial stimuli), stimulus modalities (tactilevs. auditory vs. visual), and/or maturational changes (MAor CA). Likewise, more research is needed to understand as-sociations between generalized sensory hyporesponsivenessand broader developmental outcomes.
The purpose of this study was to describe sensory hypore-sponsiveness to social and nonsocial stimuli as a function ofdevelopmentally related maturation in a large cross-sectionalsample, to determine the degree to which hyporesponsivenessis generalized across contexts in young children with autismrelative to controls and the extent to which it is associatedwith broader social communication outcomes. The specificresearch questions were the following:
1. To what extent do scores on an observed measure of sen-sory hyporesponsiveness in a laboratory task convergewith a parent-report measure of sensory features?
2. To what extent do maturational variables (CA and MA) af-fect children’s levels of hyporesponsiveness to sensorystimuli across groups?
3. Do children with autism, DD, and TD differ in their levelsof hyporesponsiveness to sensory stimuli?
4. Does context (social vs. nonsocial) affect level of hypo-responsiveness to sensory stimuli across sensory modal-ities, and if so, does it have differential effects acrossgroups?
5. Is sensory hyporesponsiveness to either social or nonso-cial stimuli associated with behavioral indices of joint at-tention and receptive and expressive language?
We hypothesized that (a) a behavioral measure of hypo-responsiveness would be significantly correlated withparental reports of hyporesponsiveness in both social andnonsocial contexts, (b) children with autism would show ageneralized pattern of hyporesponsiveness across sensorystimuli in both social and nonsocial contexts, (c) this patternwould significantly differentiate the autism group from bothcomparison groups, and (d) hyporesponsiveness to sensorystimuli in both social and nonsocial contexts would benegatively correlated with joint attention skills and languageabilities.
Method
Participants
Three groups of children (N¼ 178) ranging in age from 5 to 105months were included in this study: children with autism (N¼63, age 20–83 months), children with DD (N¼ 47, age 11–105months), and children with TD (N ¼ 68, age 5–79 months).Table 1 and Table 2 provide sample characteristics. Families re-ceived monetary incentives ($25–$75) dependent upon theirparticipation in a larger study, which typically included severalhours of developmental testing, diagnostic confirmation, andvarious sensory processing assessments. The children receiveda small toy or a book for their participation. Using conveniencesampling, participants were recruited through diagnostic evalu-ation clinics, early intervention/day care programs, mentalhealth centers, local agencies, parent support groups, and publicschools in the state of North Carolina. In addition, the Univer-sity of North Carolina Subject Registry was used to directly re-cruit families of children with autism.
Children in the autism group were diagnosed with autistic dis-order by a licensed psychologist or physician, confirmed by theAutism Diagnostic Interview—Revised (Lord, Rutter, & LeCouteur, 1994), and the Autism Diagnostic Observation Sched-ules (ADOS; Lord, Rutter, DiLavore, & Risi, 1999) or the Child-hood Autism Rating Scale (Schopler, Reichler, & Renner 1986).
The DD group comprised children with (a) known devel-opmental disabilities and genetic syndromes associated withintellectual disability (i.e., Down, Williams, Prader–Willi,and Patau syndromes; N¼ 20) and (b) nonspecific idiopathic
developmental delay (i.e., IQ . 2 SD below the mean, or de-lays . 1.5 SD below the mean in at least two developmentaldomains including expressive language, receptive language,cognitive/visual reception, fine or gross motor, and/or adap-tive behavior; N ¼ 30). We excluded children from the DDgroup if they had a clinical diagnosis of an ASD and/or metcriteria for autism on the ADOS (new scoring algorithm byGotham, Risi, Pickles, & Lord, 2007). There were two caseswhere children in the DD group with low MAs (11 and 13months) met ADOS cutoffs for ASD, but these findingswere discrepant from other autism assessments, and the over-all clinical impressions were consistent with their existing di-agnoses of DD (not ASD).
The TD group had neither significant developmental prob-lems nor received any special education/therapy services.They all scored within the normal range on developmental as-sessments. Exclusionary criteria for all groups included thefollowing: comorbid conditions of autism (e.g., fragile X),MA less than 6 months, severe physical impairment (e.g., ce-rebral palsy), uncorrected visual or hearing impairment, and/or currently taking psychoactive medications (including sti-mulants), as reported by parents or medical records.
Instruments
Sensory Processing Assessment (SPA). The SPA (Baranek,1999c) is a 20-min play-based behavioral observation tool ad-ministered in a semistructured format. It is designed to assesssensory response patterns (hyperresponsiveness and hypore-sponsiveness) in young children with autism and relatedDD from approximately 6 months through 6 years of age.The SPA enables naturalistic observation of a child’s behav-ioral responses to tactile, auditory, and visual sensory modal-ities in social and nonsocial contexts through playful interac-tion with novel sensory experiences. There are severalsections to the SPA: approach/avoidance to novel toys, orient-ing to unexpected sensory stimuli, habituation to a repeatedstimulus, and presence/absence of unusual sensory seekingbehaviors. The orienting subscale was used as the primaryoutcome measure of hyporesponsiveness in this study; proce-dures are described in detail below. Test–retest reliability be-tween two raters (n¼ 64) was calculated using intraclass cor-
relations (ICCs) and yielded high reliability (ICC¼ 0.920 forall six orienting items, 0.917 for the three social items, and0.867 for the three nonsocial items).
Sensory Experiences Questionnaire (SEQ). The SEQ (Ver-sion 2.0; Baranek, 1999b; Baranek et al., 2006) asks parentsto respond, on a 5-point Likert scale, to 30 questions about thefrequency of their child’s responses to sensory stimuli in thecontext of daily activities and routines. The SEQ has beenvalidated for children with autism, DD, and TD childrenages 6 months through 6 years, with a demonstrated abilityto discriminate sensory features among known diagnosticgroups (Baranek et al., 2006). Little et al. (2011) have re-ported high levels of internal consistency (a ¼ 0.80) andtest–retest reliability (ICC ¼ 0.92). Summary scores may bederived for hyperresponsiveness and hyporesponsiveness toboth social and nonsocial stimuli.
Mullen Scales of Early Learning (MSEL). Four directly ad-ministered scales of the MSEL (Mullen, 1995) evaluate vi-sual reception, fine motor, receptive language, and expressivelanguage abilities in children from birth to 68 months of age.The MSEL yields standardized T scores as well as ageequivalents for the four scales. The test was standardizedon a sample representative of the US population and has ac-ceptable levels of validity and reliability.
Preschool Language Scale, Fourth Edition (PLS-4). ThePLS-4 (Zimmerman, Steiner, & Pond, 2002) uses parent re-port, responses to directly administered items, and observa-tion of incidental communication throughout the assessmentto assess language understanding and expression of childrenfrom birth to age 6 years 11 months. The PLS-4 is standard-ized on a large sample representative of the 2000 US censusdata and has acceptable levels of validity and reliability.
Joint Attention Assessment. The Joint Attention Assessmentwas developed from tasks used by other investigators (Brady,Steeples, & Fleming, 2005; Leekam, Hunnisett, & Moore,1998; Mundy et al., 2003; Stone, Ousley, Yoder, Hogan, &Hepburn, 1997), with four goals: (a) a specific focus on mea-suring response to and initiation of joint attention (IJA); (b)
Table 2. Developmental characteristics of participants by group
reliable and efficient scoring during administration ratherthan requiring later video coding; (c) interaction contextsthat would appeal to children across a range of ages and func-tioning levels; and (d) measurement of variability in perfor-mance within and between groups of children. No single pre-vious measure of joint attention would allow us to meet all ofthese goals. This measure included eight trials to assess re-sponse to joint attention (RJA), interspersed with eight trialsto provide contexts for IJA. Interrater reliability (n ¼ 53) be-tween two raters was substantial (total joint attention [JA]score: 87.9% exact agreement and k ¼ 0.749; RJA: 91.3%exact agreement and k ¼ 0.831; IJA: 82.8% exact agreementand k¼ 0.666). In addition, Hurwitz (2010) examined conver-gent validity between RJA scores on the Joint Attention As-sessment (potential range of 0 to 8) and scores on the RJAitem of the ADOS (potential range of 0 to 3), using datafrom a sample of 32 children with autism. A strong significantcorrelation was found between the scores (r¼ .85, p , .001).
Procedure
Project staff contacted interested families via telephone,screened participants for eligibility, and scheduled the onsiteassessments to confirm diagnostic groupings. Assessmentstook place at the project laboratory in a community-based lo-cation with a child-friendly space. Two half days were typi-cally sufficient to complete all assessments, but this varieddepending upon the child’s age and developmental level.
Parent-completed assessments included a demographicform, a background information questionnaire, and the Vine-land Adaptive Behavior Scales (Sparrow, Balla, & Cicchetti,1984). The Autism Diagnostic Interview—Revised (Lord etal., 1994) was administered only to parents of children withautism for diagnostic confirmation. Children in all threegroups received a vision and hearing screening, to confirmnormal or corrected normal vision and hearing, and the Child-hood Autism Rating Scale (Schopler et al., 1986). Followingthe screening, children received a standardized cognitive as-sessment appropriate to their age and developmental level:the MSEL (Mullen, 1995), the Leiter International Perfor-mance Scale—Revised (Roid & Miller, 1997), and/or the Bay-ley II—Mental Developmental Index (Bayley, 1993). Nonver-bal MA was used as a measure of intellectual functioning inthis study to maintain independence from the primary out-comes measures that involved language functions. Thus, onthe MSEL, the Visual Reception Scale was used to estimatenonverbal MA, whereas the Receptive and Expressive Lan-guage Scales were used as measures of language age. Partici-pants also completed the PLS-4 (Zimmerman et al., 2002) andthe Joint Attention measure. In addition, the autism and DDgroups received the ADOS (Lord et al., 1999).
The SPA was administered in a small room with child-sizedfurniture, a short bookcase that held opaque boxes for supplies,and a few pieces of child art displayed on the walls. If neces-sary, a parent/familiar adult was present for the assessment tominimize the child’s anxiety. The adult was allowed to sit
with the child, but he or she was not allowed to comment onthe sensory stimuli or interact with items, so that all childrenhad similar instructions and procedures. Some parents optedto view the assessments from an adjoining observation room.
The SPA was administered to the child by a trained re-search assistant (RA) and videotaped for reliability scoring.The SPA orienting subscale consisted of six items, counter-balanced for three modalities (tactile, auditory, and visual)and two contexts (social and nonsocial). The six stimuli wereadministered unexpectedly in the periphery during a competingcondition (attention disengagement condition) while thechild was engaged visually with a toy at midline while seatedon the floor. The presence or absence of orienting responsesand latency to orient, as measured by the number of trials todemonstrate an orienting response, were scored. Each stimu-lus was unimodal: two were auditory (sound stick and namecall), two were visual (penlight and hand wave), and two weretactile (air puff and shoulder tap). Three of these stimuli weresocial in context—intended to obtain the child’s response tostimuli with an apparent social purpose (name call, shouldertap, or hand wave). The other three stimuli were nonsocial incontext, intended to have no apparent social purpose (soundstick, air puff, or penlight). Attempts were made to matchthe social and nonsocial stimuli in terms of duration/fre-quency, distance, and intensity (i.e., tactile ¼ two puffs/taps per second presented behind the child; auditory ¼ sim-ilar decibel levels of voice/sound stick activated 3–5 ft.away from child; visual ¼ two flashes/waves administeredper second, 18–24 in. away from child); however, some var-iation across coders and contexts occurred given the nature oftesting young children in semistructured play situations. Pre-vious studies have used similar quasiexperimental proceduresthat were judged to be ecologically valid (Dawson et al.,1998, 2004). Each target stimulus was presented to the childas he or she was engaged with a distracter (quiet toy held at mid-line). Stimuli were interspersed among the toys in the SPA tomaximize novelty and minimize habituation, and right/left pre-sentations of stimuli were counterbalanced across subjects. Ori-enting was measured behaviorally by the child’s eyes and/orhead visibly disengaging from the central stimulus and turningin the direction of the unexpected, novel stimulus. All compet-ing environmental distractions were minimized. Each stimuluswas repeated until a clear behavioral orienting response was ob-served, to a maximum of three trials. Thus, possible orientingscores for each item were 1, 2, 3 (corresponding to the trial dur-ing which the child responded), and 4 (no response). A cutoff ofthree trials was established because very few children during pi-lot testing responded after the third trial.
Sum scores were calculated to achieve an overall orientingmean (average of all six items), social mean (three items),nonsocial mean (three items), auditory mean (two items), vi-sual mean (two items), and tactile mean (two items). Highermean scores indicate less responsiveness to sensory stimuli.The Cronbach alpha was computed on a subsample of 64cases used in the reliability analyses. Internal consistency ofthe scales was computed, with the caveat that only three items
Sensory hyporesponsiveness in autism 311
comprised each subscale (three social items, a¼ 0.561; threenonsocial items, a ¼ 0.556; six items total, a ¼ 0.649). Allitems contributed relatively equally to the total scale alpha.
Three RAs were trained by the first author to administerand score the SPA to criterion (�90% agreement by section).On completion of the preliminary training protocol, the firstauthor viewed videotapes of all training administrations to en-sure procedural fidelity. The RAs then independently admin-istered and scored the SPA. No rater was aware of any specificresearch aims. All assessments were videotaped and archived.Periodic reliability checks were completed to confirm proce-dural fidelity and interrater reliability. Due to transitions in per-sonnel over the course of a multiyear project, one new coderindependently scored all SPA videos that had been previouslycoded by one of three original coders for added consistency.Consensus scores were determined for any items with disagree-ments between the new coder and previous coders, and theseconsensus scores were used in the statistical analyses.
The Joint Attention Assessment followed the SPA admin-istration and was conducted in the same room. The child wasseated at a child-sized table directly across from the examiner.Pictures were placed on the walls 90 degrees to the child’sright and left sides, four pictures per side. Four of the RJAtrials directed the child’s attention to the left and four directedthe child’s attention to the right; a graduated sequence of cueswas used, from head turn alone to head turn with a point, tohead turn with a point and verbal directive “Look,” to headturn with point and verbal labeling of the target. Turningthe head at least 45 degrees in the indicated direction follow-ing the cue was scored as a correct response. For the inter-spersed IJA trials, materials were presented on the table; ac-tivities included pulling toys from an opaque bag, lookingat a book that included three defaced pages, and providinga bin of dress-up clothes, among others. The child was cred-ited with a correct response if at any time during each trial heor she initiated an alternating gaze between an object and theexaminer, used a gesture such as pointing or showing accom-panied by eye contact and/or a vocalization, or verbally com-mented on the activity accompanied by eye contact and/or agesture directed at the examiner. RAs were trained to admin-ister the items consistent with guidelines in an assessmentmanual, with observation and feedback provided by the sec-ond author. In addition, the RAs were required to achieve atleast 80% reliability in scoring both the RJA and IJA portionsfor three consecutively scored videotaped assessments as partof the training process. Periodic reliability checks were com-pleted to confirm procedural fidelity and interrater reliabilityof at least 80% for the RJA and IJA scoring. Scoring was de-rived by crediting one point for each trial on which the childexhibited RJA or IJA skills, respectively. To allow for the in-clusion of JA scores in cases when not all trials were adminis-tered or a trial was later invalidated owing to procedural errors,we took the total number of points awarded for RJA or IJAtrials and then divided by the number of valid trials adminis-tered; thus, the JA scores included in our analyses rangedfrom 0 to 1. Higher scores indicate better joint attention skills.
Due to the large number of children with autism or DD whoscored at the floor of the standardized scores on the MSELReceptive and Expressive Language Scales and the PLS-4,we computed a ratio score of the age equivalent score/CAfor each child on each language measure. This eliminated flooreffects in the language measures for children in all groups. Amean of the two ratio scores was used to represent compositescores for receptive and expressive language, respectively.
Analyses
To answer our first question, we used Pearson correlations toexamine the convergent validity between our laboratory mea-sure of sensory hyporesponsiveness (i.e., SPA orienting sub-scale) with a parent-report measure (i.e., SEQ). For the re-maining questions, inferential analyses were performed byfitting a series of censored regression models. All analysescontrolled for mother’s education and child’s gender becausethere were significant group differences for these variables. Areview of the descriptive data revealed that a number of thesubjects scored at the minimum and maximum scores, result-ing in truncated normal distributions. For this reason, re-peated-measures Tobit-censored regression models (StataPress, 2007) were fit. These models allow us to simultane-ously account for the floor and ceiling effects in the sensorymeasure as well as repeated measures within subjects. Theyalso allowed us to directly test whether there were significantdifferences between the contexts (social vs. nonsocial) in sen-sory responsiveness. The initial set of analyses examined theassociation among CA, MA, and the hyporesponsivenessscore, as well as group differences and context interactions.Then the association between hyporesponsiveness and jointattention or language was examined by adding these variablesto the previously described censored regression models. Thisinvolved fitting four separate models, which included eitherlanguage (receptive and expressive) or joint attention (RJAand IJA) as a predictor along with group, context, MA, gen-der, and mother’s education as covariates.
Results
The initial analysis determined that total scores on the labora-tory measure of hyporesponsiveness (i.e., the SPA orientingsubscale) were significantly positively correlated with totalscores on the parent-report measure (i.e., the SEQ), r ¼ .39,p , .001. Examining stimulus contexts separately, the SPAwas correlated positively with the SEQ for both social (r ¼.34, p , .001) and nonsocial sensory items (r¼ .25, p¼ .005).
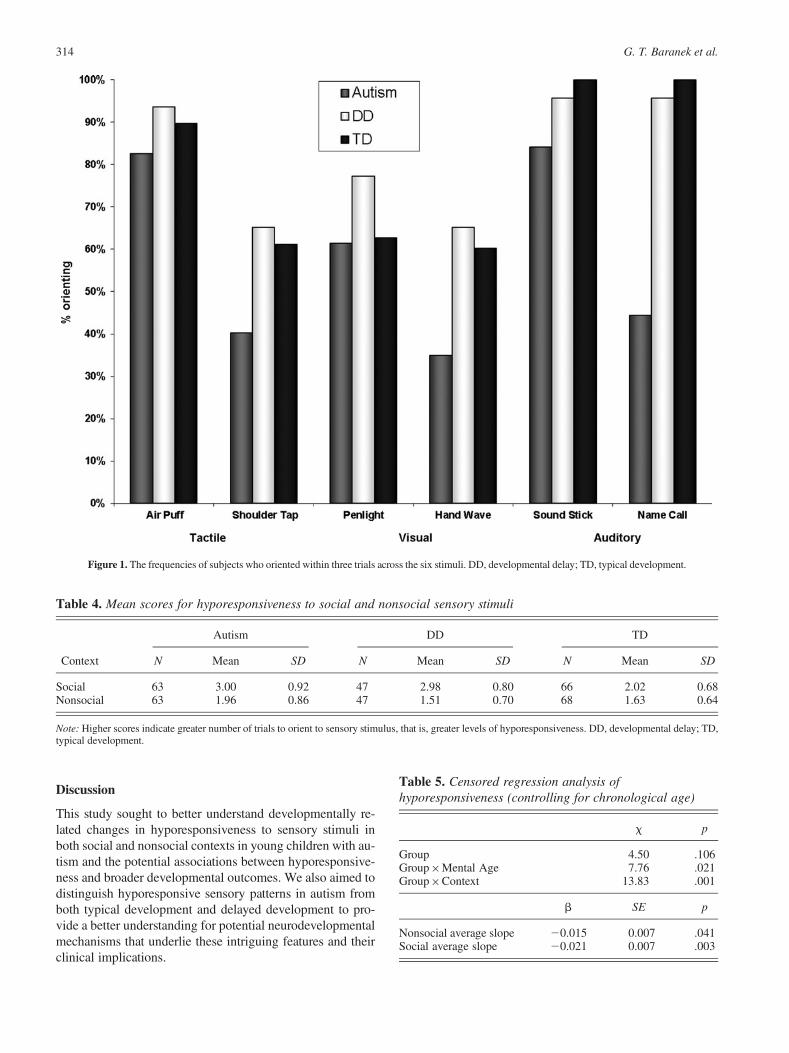
Descriptive statistics in Table 3 show the frequencies ofchildren in each group who responded across individual trialsfor each of the sensory stimuli on the SPA. Figure 1 graphi-cally depicts the percentage of children who oriented to anyof the three trials across the six sensory stimuli and denotesa trend for greater orienting for the typical group and lesserorienting for the autism group across stimuli in different mod-alities. Mean scores for hyporesponsiveness in social or non-
G. T. Baranek et al.312
social contexts, as measured by the initial trial to which achild oriented, are summarized in Table 4.
To answer the question of whether maturational variablesaccounted for degree of hyporesponsiveness across groups,the regression analyses demonstrated that hyporesponsive-ness decreased in all groups as a function of CA (b ¼–0.020, p , .001) or MA (b ¼ –0.023, p , .001). We foundthat MA (controlling for CA) accounted for a significantamount of the variance in hyporesponsiveness across thegroups (b ¼ –0.020, p ¼ .005), and we used this develop-mental variable as the basis for the remaining analyses.
To what degree (a) do the groups differ in level of hypo-responsiveness and (b) does context (social vs. nonsocial)affect the level of hyporesponsiveness across the groups? Toanswer these two questions, the regression analysis was exam-ined and indicated that group differences were present but de-pended upon the two-way interactions with MA and context.However, the three-way Group�MA�Context was not signif-icant (x2 ¼ 1.11, p ¼ .57) and was dropped from the model.When looking at MA (controlling for CA) we found an overallsignificant difference between the groups in developmentallyrelated change (x2 ¼ 7.76, p¼ .021) across the social and non-social contexts combined. At 6 months MA, the autism groupshowed significantly higher scores (i.e., more hyporesponsive-ness) than did the DD and TD groups. Table 5 shows modelgroup differences. By 60 months MA there were no significantdifferences among groups. (see Figure 2 and Figure 3). The dif-ference in the size of the group effect varied significantly be-tween social versus nonsocial contexts (x2 ¼13.83, p ¼.001), with a larger effect size for the social context (see Table 5
and Table 6). There were no statistically significant differencesbetween the DD and TD groups (all ps . .10).
Our last question inquired as to whether sensory hypore-sponsiveness was associated with behavioral indices of jointattention and language across the three groups. We found thatRJA showed a significant negative correlation with hypore-sponsiveness (b ¼ –0.83, SE ¼ 0.37, p ¼ .025) and did notvary significantly by group or context (social or nonsocial).However, there was a significant interaction with MA (b ¼0.047, SE ¼ 0.02, p ¼ .026), resulting in a significant corre-lation at younger MA (e.g., at 6 months: b ¼ –1.71, SE ¼0.46, p , .001) but not at older MA (e.g., at 60 months: b¼ 0.80, SE¼ 0.90, p¼ .38). The results for IJA were similarwith a significant negative correlation between hyporespon-siveness and IJA (b ¼ –1.63, SE ¼ 0.59, p ¼ .006) that didnot vary significantly by group or context (social or nonso-cial). The IJA�MA interaction showed a nonsignificant trend( p ¼ .063) in the same direction as the findings for RJA.
The autism group also showed a significant negative cor-relation between sensory hyporesponsiveness and language,such that children with more problems responding to sensorystimuli had lower language ratio scores (language age/CA).This was true for both receptive (b ¼ –2.0, SE ¼ 0.68, p ¼.004) and expressive language ratio scores (b ¼ –2.1, SE ¼0.73, p¼ .005) and did not vary as a function of social versusnonsocial context (all ps . .10). The Language Ratio�MAinteractions were statistically nonsignificant (both receptiveand expressive p . .10). The correlations between hypore-sponsiveness and language scores in the TD and DD groupdid not reach statistical significance (all p . .05).
Table 3. Frequency of scores (percentages) across individual stimuli for Trials 1, 2, 3, or no response
This study sought to better understand developmentally re-lated changes in hyporesponsiveness to sensory stimuli inboth social and nonsocial contexts in young children with au-tism and the potential associations between hyporesponsive-ness and broader developmental outcomes. We also aimed todistinguish hyporesponsive sensory patterns in autism fromboth typical development and delayed development to pro-vide a better understanding for potential neurodevelopmentalmechanisms that underlie these intriguing features and theirclinical implications.
Figure 1. The frequencies of subjects who oriented within three trials across the six stimuli. DD, developmental delay; TD, typical development.
Table 4. Mean scores for hyporesponsiveness to social and nonsocial sensory stimuli
Note: Higher scores indicate greater number of trials to orient to sensory stimulus, that is, greater levels of hyporesponsiveness. DD, developmental delay; TD,typical development.
Table 5. Censored regression analysis ofhyporesponsiveness (controlling for chronological age)
x p
Group 4.50 .106Group×Mental Age 7.76 .021Group×Context 13.83 .001
b SE p
Nonsocial average slope 20.015 0.007 .041Social average slope 20.021 0.007 .003
G. T. Baranek et al.314
Figure 2. Hyporesponsiveness to nonsocial sensory stimuli as a function of mental age controlling for chronological age. DD, developmentaldelay; TD, typical development.
Figure 3. Hyporesponsiveness to social sensory stimuli as a function of mental age controlling for chronological age. DD, developmental delay;TD, typical development.
Sensory hyporesponsiveness in autism 315
Convergence of observed and parent-report measuresof sensory hyporesponsiveness
The SPA and the SEQ had significant positive correlations, in-dicating convergent validity and supporting the assumption thatthe results from our observational measure have some general-izability to the child’s sensory features as perceived by theirparents in everyday life. However, the magnitude of the overallcorrelation was moderate, indicating that these two measuresare also tapping somewhat different aspects of sensory hypo-responsiveness (e.g., broad vs. specific) and/or reflect differ-ences related to format (e.g., observed vs. parent report) orcontext (e.g., familiar vs. unfamiliar environments) of the mea-sures. Statistical models utilizing multimodal measures of sen-sory features, controlling for measurement format, may be morereliable and provide a more comprehensive understanding ofthe constructs of interest and their relationship to various devel-opmental outcomes in future research (Boyd et al., 2010).
Developmentally related changes in sensoryhyporesponsiveness
The results confirmed that hyporesponsiveness, as measuredby a sensory orienting task in the laboratory, was affected bymaturational variables. These results are consistent with pre-vious work demonstrating similar effects with questionnairedata (Baranek et al., 2006), but they extend the findings specif-ically across three sensory modalities and two contexts (socialand nonsocial) using an observational lab measure, the SPA.MA accounted for a significantly greater proportion of the var-iance than CA in explaining decreasing hyporesponsiveness asa function of maturation across all three groups of children.Thus, as mental abilities increased, children in all three groupsbecame more responsive to sensory stimuli across social andnonsocial contexts. This may indicate maturation in neuralmechanisms underlying general sensory processing and atten-tion abilities, improvements in general learning, and/or devel-opment of compensatory strategies. However, our findings fur-ther demonstrated a novel interaction between group and slope(i.e., a developmentally related decrease in hyporesponsive-ness) that more fully explicated the nature of these behaviors.At the youngest MA (6 months), group differences were signif-icant and large, but by 60 months, these differences were no
longer statistically significant. Thus, indicators of sensory hy-poresponsiveness were most sensitive to group differences atthe lowest MAs, with the autism group faring the worst.
The methodology used in this study has advantages overprevious studies in this area and helps to shed light on whydiscrepancies exist among findings in previous studies. Themajority of studies in this area have utilized between-groupdesigns taking a narrower cross section of CA and matchinggroups on one or more key variables (e.g., MA). Althoughseveral studies investigated the differential contextual effects(social vs. nonsocial) of hyporesponsiveness in autism (e.g.,Dawson et al., 1998, 2004), most have not considered possi-ble interactions between generalized hyporesponsiveness anddevelopmental level or the association of generalized hypo-responsiveness to broader outcomes.
Our study demonstrates a more complex picture of the devel-opmental psychopathology of sensory hyporesponsiveness. Thematurational level at which behaviors are sampled impacts di-rectly upon the degree to which these deficits are apparent inchildren with autism. Furthermore, the developmental mecha-nisms underlying changes in behavioral responsiveness appearmore critical than stimulus context (i.e., social or nonsocial) indetecting group differences as well as predicting to broader so-cial communication outcomes. The implications of this workmay be relevant for identifying early risk factors; that is, at lowermaturational levels, items tapping generalized hyporesponsive-ness (i.e., orienting to novel social and nonsocial sensory stim-uli) may be useful to identify children at risk for autism aswell as those with other developmental delays, but the sensitivityand utility of such items potentially decreases as children’s cog-nitive capacities mature. Although the literature is mixed with re-spect to the presence of early sensory symptoms in autism, fewstudies included sensory measures and/or relied heavily on retro-spective parent reports that may be less sensitive to these featuresin infancy. Several studies have reported early manifestations ofsensory features either preceding or occurring simultaneouslywith other symptoms of autism by 12 months of age (Baranek,1999a; Dalhgren & Gillberg, 1989; Zwaigenbaum et al., 2005).
Our findings also have implications for understanding thedevelopment of generalized sensory orienting processes inearly childhood and the association of deficits in orientingto broader social communicative outcomes. Previous researchin autism indicated that social orienting was correlated with
Table 6. Test of group differences to social and nonsocial sensory stimuli across mental age
joint attention (Dawson et al., 2004), but effects for nonsocialorienting were not equitably examined in relation to joint atten-tion and language variables. Our findings further clarify thenature of these associations, indicating that lack of orientingto both social and nonsocial sensory stimuli is associatedwith lower joint attention in children with autism, as well asthose with DD or typical development, and this associationis strongest at lower MAs. Thus, we theorize that orienting tosensory stimuli is a domain-general process (occurring inboth social and nonsocial contexts) that is foundational tothe development of joint attention for all groups of children.Although different neurological mechanisms may subserveIJA (anterior attentional system) versus RJA (posterior atten-tional system; Mundy & Jarrold, 2010; Mundy & Newell,2007), both processes appear associated with early-developingskills in orienting to sensory stimuli based on our findings. Hy-poresponsiveness to sensory stimuli during early critical peri-ods for infants at risk for autism would likely interact withother core deficits of autism and, thus, hypothetically may pro-duce cascading effects on more complex developmental skills,particularly in the social communication domain. As Mundyand Jarrold (2010) stated, the efficiency of social learningand social cognition results from the basic processes of the in-tegration of self-initiated visual attention as well as the abilityto process and follow the visual attention of others. With prac-tice and experience, these coactive systems allow the infant toattend to and learn from multiple sources of social informationand receive socially contingent responses from other people.Bjorne, Johansson, and Balkenius (2006) discuss the possibleimplications of prolonged difficulties in attention disengage-ment (that are one potential explanation of orienting difficul-ties) among children with autism for complex contextual learn-ing. They posit that this would be especially problematic forsocial learning. Although our data suggest that children withautism demonstrate individual differences in the rate of acqui-sition of sensory orienting skills (i.e., normalize responsesthrough maturation, experience, and/or intervention at differentages), the lost opportunities for learning during early develop-mental periods where sensory orienting is most critical maydetrimentally impact the acquisition and/or quality of later-developing joint attention skills that are dependent on the inter-action of both anterior and posterior neural mechanisms.
Our data on the associations between orienting to sensorystimuli and joint attention and language, even though cross-sectional, suggest a developmental model. For all groups,sensory hyporesponsiveness had a significant negative rela-tion to joint attention at low MAs, but by 60 months, the re-lation was no longer significant. Thus, by the maturationalpoint at which the group differences in hyporesponsivenesshave dissipated, individual variability in joint attention skillsno longer is explained by ability to orient to sensory stimuli.As children mature and improve in their generalized orientingabilities, they may reach a threshold level such that respon-siveness to sensory stimuli per se no longer imposes a con-straint on their ability to engage in joint attention. From otherresearch, however, we know that children with autism con-
tinue to experience problems, particularly in initiating jointattention, at older MAs than do children with other DD or typ-ical development (Sigman & Ruskin, 1999), suggesting otherfactors (e.g., motivation/social reward, effortful control, ex-ecutive functions, etc.) may also constrain their developmentof joint attention skills (Mundy, 2011). Future studies need touse longitudinal methods, including an evaluation of nonlin-ear trajectories and mediating variables, to unravel the com-plex interactions between early and later-developing symp-toms across different developmental domains.
In partial contrast to the lack of group differences in theanalyses involving the correlation of sensory responsivenessand joint attention, the language skills of children with autismshowed a statistically significant association with sensory re-sponsiveness that did not reach significance in the other twogroups. The association we found between sensory hypore-sponsiveness on a laboratory task and lower communicationis consistent with at least one other study that used a parent-re-port measure with children with autism (Liss et al., 2006).
One striking finding was that 100% of children with TD andmore than 90% of children with DD oriented to auditory stim-uli within three trials. Thus, in this very important modality forlanguage learning, children without autism are orienting quitewell to auditory stimuli even at very young MAs. In contrast,children with autism were slower to orient to both nonsocialand social auditory stimuli, and less than half of the grouporiented to name call within three trials. Research using phys-iological methods has similarly demonstrated latencies in audi-tory processing and hypothesized a relation to cortical matura-tion deficits in autism (Gage, Siegel, & Roberts, 2003). Theinverse relation between hyporesponsiveness and language de-velopment in the autism group in our study hypothetically mayreflect the aforementioned cascading impact of the orientingdifficulties among children with autism.
These findings raise some complex questions regardinggroup differences in pathways subserving language learningand potential mediators of language outcomes. Future longi-tudinal studies with larger samples and multimodal measuresare needed to test developmental transactions among sensoryhyporesponsiveness, joint attention, and language develop-ment across diagnostic groups.
Specificity of hyporesponsiveness to autism: Effectsof context
Specificity of deficits in autism may be best understood in a de-velopmental context. Orienting skills are a key to early socialengagement, environmental exploration, and learning. Asmentioned above, the autism group oriented less to all sensorystimuli compared with controls, and this was particularly evi-dent at younger MAs. These findings provide support for the-ories of generalized deficits in sensory processing and/or atten-tion, rather than solely a social cognitive deficit, that mayunderlie hyporesponsiveness to both social and nonsocial sen-sory stimuli in young children with autism (e.g., Harris et al.,1999; Townsend et al., 1999; Zwaigenbaum et al., 2005).
Sensory hyporesponsiveness in autism 317
Adding to the findings of Dawson et al. (1998, 2004), whoconcluded that social orienting was specifically associatedwith joint attention, the present study demonstrates that non-social sensory orienting is also associated with joint attention,and this finding is evident across all three groups of children.Our study further clarifies these associations, indicating thatmaturational variables may account for some of the individualdifferences. The associations between sensory responsive-ness and joint attention are greatest at very young MAswhen perhaps learning opportunities are more dependentupon the integrity of reflexive attentional processes, butthey decline in importance at higher MAs as volitionalmechanisms play a larger role in social learning. However,given that children with autism showed larger impairmentsin responsiveness to social than to nonsocial stimuli, theremay be an interaction of two mechanisms underlying this pro-file. Our findings are consistent with theories purported byMundy and colleagues (2007, 2010, 2011) that deficits in au-tism may result from difficulties in the integration of two at-tentional neural networks, a posterior system supportingearly-developing and more reflexive aspects of generalizedsensory orienting and RJA, and an anterior system supportinglater-developing and more volitional social–cognitive behav-iors including IJA. Deficits in the later-developing anteriorsystem may be linked to difficulty processing social rewardsin autism and further explain why social orienting behaviorsare often reported to be more problematic than nonsocial ori-enting behaviors at later developmental stages.
It is interesting that neurobiological and neurophysiologicalfindings in autism have implicated aberrant functional connec-tivity (e.g., Belmonte et al., 2004; Minshew & Hobson, 2008;Uhlhaas & Singer, 2006) that may arise early in developmentand involve a variety of networks and structures (e.g., amyg-dala, dorsolateral prefrontal cortex, parietal lobe, cerebellum,and superior temporal sulcus) associated with orienting to nov-elty, multisensory integration, and/or disengagement of visualattention (Dawson et al., 1998; Macaluso, Frith, & Driver,2001; Tommerdahl, Tannan, Holden, & Baranek, 2008; Town-send et al., 1999). Further research using cutting-edge tech-nologies is needed to unravel the developmental neurobiologyunderlying sensory hyporesponsiveness in autism.
Methodological considerations
This study has several methodological advantages over pre-vious work. Past studies on the sensory response patterns ofchildren with autism relied heavily on caregiver-report instru-ments (Baranek et al., 2006; Kientz & Dunn, 1997; Laneet al., 2010; Talay-Ongan & Wood, 2000; Watling, Deitz, &
White, 2001) that are prone to recall biases, situational differ-ences, and developmental expectations affecting perceptionsof behavior. We utilized a laboratory task to measure observedlevels of sensory hyporesponsiveness. Direct observation-basedsensory assessments may provide a more controlled and sensi-tive measure of hyporesponsiveness than parent-report mea-sures in early development (Baranek et al., 2008).
Although previous studies have provided preliminary evi-dence to address the question of context (Dawson et al., 1998;Swettenham et al., 1998), the present study extends the litera-ture by examining sensory patterns across three modalities(tactile, auditory, and visual) as well as two contexts (socialand nonsocial) with a sample of young children with autismand matched controls. The use of a mixed-model regressionanalysis with a large sample and a broader age range alloweda more direct test for group differences while accounting fordevelopmentally related changes not previously studied sys-tematically. Furthermore, this study confirms an associationof sensory orienting to broader developmental outcomesin joint attention and language development in childrenwith autism.
Limitations include the small number of stimuli in eachcondition that precluded directly analyzing group differencesby modality and also floor effects of the SPA (i.e., many chil-dren receiving zero scores) at the highest developmental ages.Comparisons across modalities were not made since the phys-ical properties of stimuli are difficult to equate across sensorymodalities. Although the naturalistic paradigm provided eco-logical validity, future studies may wish to implement com-puterized tasks to experimentally equate the psychophysicalproperties of stimuli across modalities in social and nonsocialcontexts, present greater numbers of trials for each stimulus,and control for possible confounding effects of live “social”administration for both social and nonsocial items.
Cross-sectional designs controlling for maturational vari-ables allow invaluable inferences about developmental mecha-nisms underlying psychopathology; however, longitudinalstudies are needed to more definitively answer questions re-garding developmental change and long-range prediction tobroader outcomes. Future studies may also wish to further dif-ferentiate high-level from low-level JA behaviors with moredetailed coding procedures to determine to what extent thesevary as a function of maturational variables and diagnosticgroup. Although the use of a mixed DD group allows forsome generalization, future studies could investigate differen-tial associations/disassociations that potentially exist acrosshomogeneous subsamples of children with various types ofDD to further our understanding of the developmental psycho-pathology and specificity of these phenomena.
References
Baranek, G. T. (1999a). Autism during infancy: A retrospective video anal-ysis of sensory-motor and social behaviors at 9–12 months of age. Jour-nal of Autism and Developmental Disorders, 29, 213–224.
Baranek, G. T. (1999b). Sensory Experiences Questionnaire (SEQ). Unpub-lished manuscript, University of North Carolina at Chapel Hill.
Baranek, G. T. (1999c). Sensory Processing Assessment for Young Children(SPA). Unpublished manuscript, University of North Carolina at ChapelHill.
Baranek, G. T., David, F. J., Poe, M. D., Stone, W. L., & Watson, L. R.(2006). Sensory Experiences Questionnaire: Discriminating sensory fea-
G. T. Baranek et al.318
tures in young children with autism, developmental delays, and typicaldevelopment. Journal of Child Psychology and Psychiatry, 47, 591–601.
Baranek, G. T., Roberts, J. E., David, F. J., Sideris, J., Mirrett, P. L., Hatton,D. D., et al. (2008). Developmental trajectories and correlates of sensoryprocessing functions in young boys with fragile X syndrome. Physicaland Occupational Therapy in Pediatrics, 28, 79–98.
Bayley, N. (1993). Bayley Scales of Infant Development—Second edition(BSID-II). San Antonio, TX: Psychological Corporation.
Belmonte, M. K., Allen, G., Beckel-Mitchener, A., Boulanger, L. M., Carper,R. A., & Webb, S. J. (2004). Autism and abnormal development of brainconnectivity. Journal of Neuroscience, 24, 9228–9231.
Ben-Sasson, A., Hen, L., Fluss, R., Cermak, S. A., Engel-Yeger, B., & Gal,E. (2009). A meta-analysis of sensory modulation symptoms in indi-viduals with autism spectrum disorders. Journal of Autism and Develop-mental Disorders, 39, 1–11.
Bjorne, P., Johansson, B., & Balkenius, C. (2006). Effects of early sensori-motor disorder on contextual learning in autism. Revue Europeenne dePsychologie Applique, 56, 247–252.
Boyd, B. A., Baranek, G. T., Sideris, J., Poe, M. D., Watson, L. R., Patten, E.,et al. (2010). Sensory features and repetitive behaviors in children withautism and developmental delays. Autism Research, 3, 78–87.
Brady, N. C., Steeples, T., & Fleming, K. (2005). Effects of prelinguisticcommunication levels on initiation and repair of communication in chil-dren with disabilities. Journal of Speech, Language, and Hearing Re-search, 48, 1098–1113.
Dahlgren, S. O., & Gillberg, C. (1989). Symptoms in the first two years oflife: A preliminary population study of infantile autism. European Ar-chives of Psychology and Neurological Sciences, 238, 169–174.
Dawson, G., Meltzoff, A. N., Osterling, J., Rinaldi, J., & Brown, E. (1998).Children with autism fail to orient to naturally occurring social stimuli.Journal of Autism and Developmental Disorders, 28, 479–485.
Dawson, G., Toth, K., Abbott, R., Osterling, J., Munson, J., Estes, A., et al.(2004). Early social attention impairments in autism: Social orienting,joint attention, and attention to distress. Developmental Psychology, 40,271–283.
Farroni, T., Simion, F., Umilta, C., & Barba, B. D. (1999). The gap effect innewborns. Developmental Science, 2, 174–186.
Gage, N., Siegel, B., & Roberts, T. (2003). Cortical auditory system matura-tional abnormalities in children with autism disorder: An MEG investiga-tion. Developmental Brain Research, 144, 201–210.
Gotham, K., Risi, S., Pickles, A., & Lord, C. (2007). The Autism DiagnosticObservation Schedule (ADOS): Revised algorithms for improved diag-nostic validity. Journal of Autism and Developmental Disorders, 37,613–627.
Grandin, T. (1996). Emergence: Labeled autistic. New York: Warner Books.Greenspan, S., & Wieder, S. (1997). Developmental patterns and outcomes in
infants and children with disorders in relating and communicating: Achart review of 200 cases of children with autistic spectrum diagnoses.Journal of Developmental and Learning Disorders, 1, 87–141.
Harris, N. S., Courchesne, E., Townsend, J., Carper, R. A., & Lord, C.(1999). Neuroanatomic contributions to slowed orienting of attention inchildren with autism. Cognitive Brain Research, 8, 61–71.
Hart, C. (1991). Without reason: A family copes with two generations of au-tism. New York: NAL.
Hirstein, W., Iversen, P., & Ramachandran, V. S. (2001). Autonomic re-sponses of autistic children to people and objects. Proceedings of theRoyal Society of London: Biological Sciences, 268, 1883–1888.
Hunnius, S., & Geuze, R. H. (2004). Gaze shifting in infancy: A longitudinalstudy using dynamic faces and abstract stimuli. Infant Behavior and De-velopment, 27, 397–416.
Hurwitz, S. (2010). Joint attention revisited: Examining heterogeneity amongchildren with autism. Dissertation Abstracts International, 71 (08) (Pub-lication No. AAT 3409920).
Johnson, M. H. (1990). Cortical maturation and the development of visual at-tention in early infancy. Journal of Cognitive Neuroscience, 2, 81–95.
Jones, R. S. P., Quigney, C., & Huws, J. C. (2003). Firsthand accounts of sen-sory perceptual experiences in autism: A qualitative analysis. Journal ofIntellectual and Developmental Disability, 28, 112–121.
Kientz, M. A., & Dunn, W. (1997). A comparison of the performance of chil-dren with and without autism on the Sensory Profile. American Journalof Occupational Therapy, 51, 530–537.
Landa, R. J., Holman, K. C., & Garrett-Mayer, E. (2007). Social and commu-nication development in toddlers with early and later diagnosis of autismspectrum disorders. Archives of General Psychiatry, 64, 853–864.
Lane, A. E., Young, R. L., Baker, A. E. Z., & Angley, M. T. (2010). Sensoryprocessing subtypes in autism: Association with adaptive behavior. Jour-nal of Autism and Developmental Disorders, 40, 112–122.
Leekam, S. R., Hunnisett, E., & Moore, C. (1998). Targets and cues: Gaze-following in children with autism. Journal of Child Psychology and Psy-chiatry, 39, 951–962.
Leekam, S. R., Nieto, C., Libby, S. J., Wing, L., & Gould, J. (2007). Describ-ing the sensory abnormalities of children and adults with autism. Journalof Autism and Developmental Disorders, 37, 894–910.
Leekam, S. R., & Ramsden, C. A. (2006). Dyadic orienting and joint atten-tion in preschool children with autism. Journal of Autism and Develop-mental Disorders, 36, 185–197.
Liss, M., Saulnier, C., Fein, D., & Kinsbourne, M. (2006). Sensory andattention abnormalities in autistic spectrum disorders. Autism, 10, 155–172.
Little, L., Freuler, A., Houser, M. B., Guckian, L., Carbine, K., David, F. J.,et al. (2011). Brief report: Psychometric validation of the Sensory Experi-ences Questionnaire. American Journal of Occupational Therapy, 65,207–210.
Lord, C., Rutter, M., DiLavore, P., & Risi, S. (1999). The Autism DiagnosticObservation Schedule (ADOS). Los Angeles: Western PsychologicalServices.
Lord, C., Rutter, M., & Le Couteur, A. (1994). Autism Diagnostic Interview–Revised: A revised version of a diagnostic interview for caregivers ofindividuals with possible pervasive developmental disorders. Journalof Autism and Developmental Disorders, 24, 659–685.
Macaluso, E., Frith, C. D., & Driver, J. (2001). Multimodal mechanisms ofattention related to rates of spatial shifting in vision and touch. Experi-mental Brain Research, 137, 445–454.
Miller, L. J., Anzalone, M. E., Lane, S. J., Cermak, S. A., & Osten, E. T.(2007). Concept evolution in sensory integration: A proposed nosologyfor diagnosis. American Journal of Occupational Therapy, 61, 135–140.
Miller, L. J., Reisman, J. E., McIntosh, D. N., & Simon, J. (2001). An eco-logical model of sensory modulation: Performance of children with fra-gile X syndrome, autistic disorder, attention-deficit/hyperactivity disor-der, and sensory modulation dysfunction. In S. Smith-Roley, E. I.Blanche, & R. C. Schaaf (Eds.), Understanding the nature of sensory in-tegration with diverse populations (pp. 57–88). San Antonio, TX: Ther-apy Skill Builders.
Minshew, N. J., & Hobson, J. A. (2008). Sensory sensitivities and performanceon sensory perceptual tasks in high-functioning individuals with autism.Journal of Autism and Developmental Disorders, 38, 1485–1498.
Mullen, E. M. (1995). Mullen Scales of Early Learning (AGS Edition). LosAngeles: Western Psychological Services.
Mundy, P. (2011). The social behavior of autism: A parallel and distributedinformation processing perspective. In D. G. Amaral, G. Dawson, & D.H. Geschwind (Eds.), Autism spectrum disorders (pp. 149–171).New York: Oxford University Press.
Mundy, P., Delgado, C., Block, J., Venezia, M., Hogan, A., & Seibert, J.(2003). A manual for the abridged Early Social Communication Scales(ESCS). Coral Gables, FL: University of Miami, Department of Psychol-ogy.
Mundy, P., & Neal, R. (2001). Neural plasticity, joint attention, and a trans-actional social-orienting model of autism. In L. M. Glidden (Ed.), Inter-national review of research in mental retardation: Vol. 23. Autism (pp.139–168). San Diego, CA: Academic Press.
Mundy, P., & Newell, L. (2007). Attention, joint attention and social cogni-tion. Current Directions in Psychological Science, 16, 269–274.
Nadig, A. S., Ozonoff, S., Young, G. S., Rozga, A., Sigman, M., & Rogers, S.J. (2007). A prospective study of response to name in infants at risk forautism. Journal of Pediatrics, 161, 378–383.
O’Neill, M., & Jones, R. S. (1997). Sensory-perceptual abnormalities in au-tism: A case for more research? Journal of Autism and DevelopmentalDisorders, 27, 283–293.
Posner, M. I., & Rothbart, M. K. (2007). Research on attention networks as amodel for the integration of psychological science. Annual Review of Psy-chology, 58, 1–23.
Rogers, S. J., & Ozonoff, S. (2005). Annotation: What do we know about sen-sory dysfunction in autism? A critical review of the empirical evidence.Journal of Child Psychology and Psychiatry, 46, 1255–1268.
Roid, G. H., & Miller, L. J. (1997). Leiter International Performance ScaleRevised. Wood Dale, IL: Stoelting.
Sensory hyporesponsiveness in autism 319
Rothbart, M. K., Posner, M. I., & Rosicky, J. (1994). Orienting in normaland pathological development. Development and Psychopathology, 6,635–652.
Schneider, M. L., Moore, C. F., Gajewski, L. L., Larson, J. A., Roberts, A. D.,& Converse, A. K. (2008). Sensory processing disorder in a primatemodel: Evidence from a longitudinal study of prenatal alcohol and prena-tal stress effects. Child Development, 79, 100–113.
Schopler, E., Reichler, R. J., & Renner, B. R. (1986). The Childhood AutismRating Scale. Los Angeles: Western Psychological Services.
Sigman, M., & Ruskin, E. (1999). Continuity and change in the social com-petence of children with autism, Down syndrome, and developmental de-lays. Monographs of the Society for Research in Child Development, 64,1–114.
Siller, M., & Sigman, M. (2008). Modeling longitudinal change in the lan-guage abilities of children with autism: Parent behaviors and child char-acteristics as predictors of change. Developmental Psychology, 44, 1691–1704.
Sparrow, S., Balla, D., & Cicchetti, D. (1984). Vineland Adaptive BehaviorScales. Circle Pines, MN: American Guidance Service.
Stata Press. (2007). Longitudinal/Panel—Data Reference Manual: Release10. College Station, TX: Author.
Stone, W. L., Ousley, O. Y., Yoder, P. J., Hogan, K. L., & Hepburn, S. L.(1997). Nonverbal communication in two- and three-year-old childrenwith autism. Journal of Autism and Developmental Disorders, 27,677–696.
Swettenham, J., Baron-Cohen, S., Charman, T., Cox, A., Baird, G., Drew, A.,et al. (1998). The frequency and distribution of spontaneous attentionshifts between social and nonsocial stimuli in autistic, typically develop-
ing, and nonautistic developmentally delayed infants. Journal of ChildPsychology and Psychiatry, 39, 747–753.
Talay-Ongan, A., & Wood, K. (2000). Unusual sensory sensitivities in au-tism: A possible crossroads. International Journal of Disability, Develop-ment and Education, 47, 201–212.
Tommerdahl, M., Tannan, V., Holden, J. K., & Baranek, G. T. (2008). Ab-sence of stimulus-driven synchronization effects on sensory perceptionin autism: Evidence for local underconnectivity? Behavioral and BrainFunctions, 4, 19.
Townsend, J., Courchesne, E., Covington, J., Westerfield, M., Harris, N. S.,Lyden, P., et al. (1999). Spatial attention deficits in patients with acquiredor developmental cerebellar abnormality. Journal of Neuroscience, 19,5632–5643.
Uhlhaas, P. J., & Singer, W. (2006). Neural synchrony in brain disorders:Relevance for cognitive dysfunctions and pathophysiology. Neuron,52, 155–168.
Watling, R. L., Deitz, J., & White, O. (2001). Comparison of Sensory Profilescores of young children with and without autism spectrum disorders.American Journal of Occupational Therapy, 55, 416–423.
Wetherby, A. M., Watt, N., Morgan, L., & Shumway, S. (2007). Social com-munication profiles of children with autism spectrum disorders late in thesecond year of life. Journal of Autism and Developmental Disorders, 37,960–975.
Zimmerman, I. L., Steiner, V. G., & Pond, R. E. (2002). Preschool LanguageScale, Fourth Edition (PLS-4). San Antonio, TX: Psychological Corporation.
Zwaigenbaum, L., Bryson, S., Rogers, T., Roberts, W., Brian, J., & Szatmari,P. (2005). Behavioral manifestations of autism in the first year of life. In-ternational Journal of Developmental Neuroscience, 23, 143–152.