52
Hypothalamus and Pituitary
| Date post: | 19-Dec-2015 |
| Category: |
Documents |
| View: | 214 times |
| Download: | 0 times |
Hypothalamus and Pituitary
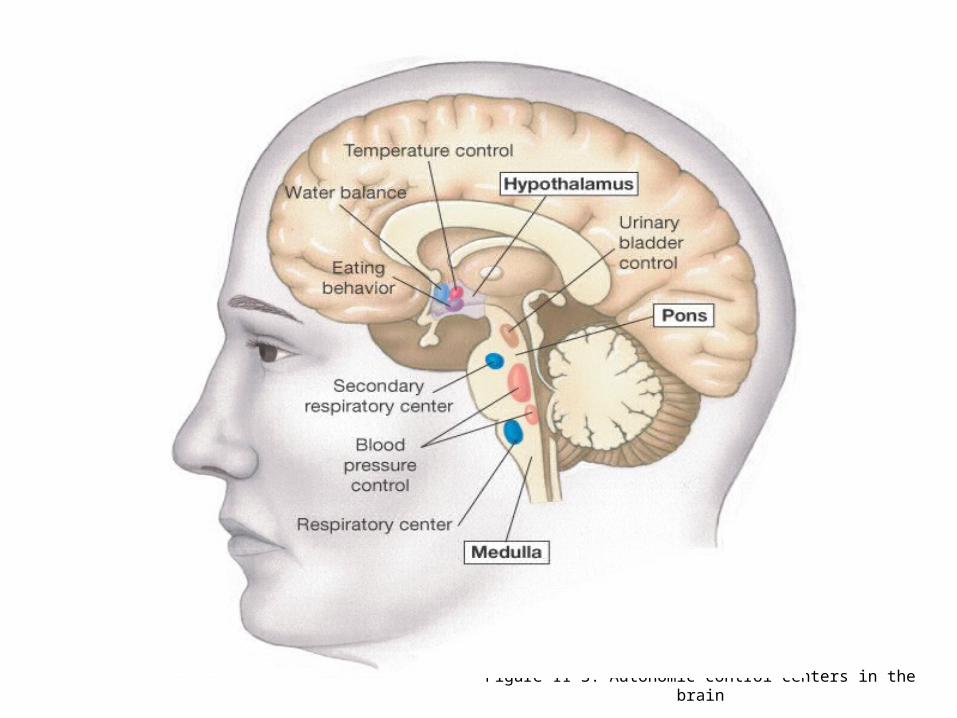
Figure 11-3: Autonomic control centers in the brain

Hypothalamus
• Integrates functions that maintain chemical and temperature homeostasis
• Functions with the limbic system
• Controls the release of hormones from the anterior and posterior pituitary
Hypothalamus
• Synthesizes releasing hormones in cell bodies of neurons
• Hormones are transported down the axon and
stored in the nerve endings
• Hormones are released in pulses
Hypothalamic Releasing Hormones
Seven releasing hormones are made in the hypothalamus– Thyrotropin-releasing hormone (TRH)– Corticotropin-releasing hormone (CRH)– Gonadotropin-releasing hormone (GnRH)– Growth hormone-releasing hormone (GHRH)– Growth hormone-release inhibiting hormone (GHIH)– Prolactin-releasing factor (PRF)– Prolactin-inhibiting hormone (PIH)
Hypothalamus Releasing Hormones: Secretion
• Is influenced by emotions
• Can be influenced by the metabolic state of the individual
• Delivered to the anterior pituitary via the hypothalamic-hypophyseal portal system
• Usually initiates a three-hormone sequence

Anterior Pituitary
Is also called the Adenohypophysis
Secretes tropic hormones in a pulsatile fashion
Synthesizes various hormones in various specific cell populations

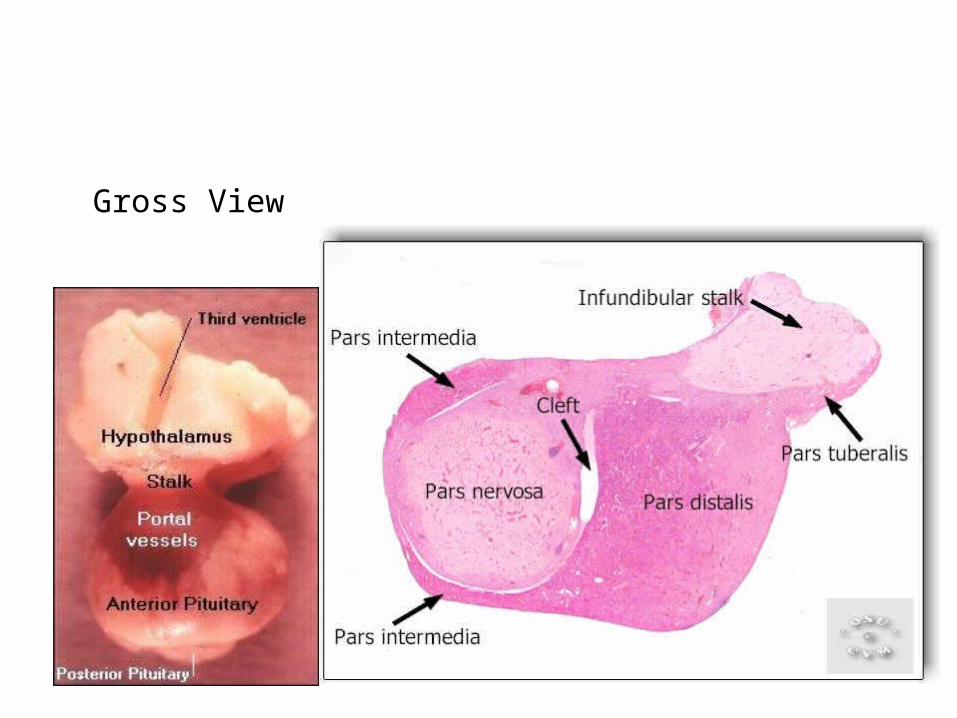
Gross View

Anterior Pituitary Hormones
Each of anterior pituitary hormone is synthesized by a cell population.
Corticotropes - ACTH
Lactotropes - Prolactin
Somatotropes - GH
Thyrotropes - Thyrotropin
Gonadotropes - FSH, LH

Anterior Pituitary Hormones
Growth Hormone (GH, Somatotropin): primary hormone responsible for regulating body growth, and is important in metabolism
Thyroid-stimulating Hormone (TSH): stimulates secretion of thyroid hormone & growth of thyroid gland
Adrenocorticotropic Hormone (ACTH): stimulates cortisol secretion by the adrenal cortex & promotes growth of adrenal cortex

Anterior Pituitary Hormones
Follicle-stimulating Hormone (FSH): Females: stimulates growth & development of ovarian follicles, promotes secretion of estrogen by ovaries. Males: required for sperm production
Luteinizing Hormone (LH): Females: responsible for ovulation, formation of corpus luteum in the ovary, and regulation of ovarian secretion of female sex hormones. Males: stimulates cell in the testes to secrete testosterone
Prolactin: Females: stimulates breast development and milk production. Males: involved in testicular function

HYPOTHALAMIC HORMONE
EFFECTS ON THE ANTERIOR PITUITARY
Thyrotropin-releasing hormone (TRH)
Stimulates release of TSH (thyrotropin) and Prolactin
Corticotropin-releasing hormone (CRH)
Stimulates release of ACTH (corticotropin)
Gonadrotropin-releasing hormone (GnRH)
Stimulates release of FSH and LH (gonadotropins)
Growth hormone-releasing hormone (GHRH)
Stimulates release of growth hormone
Growth hormone-inhibiting hormone (GHIH)
Inhibits release of growth hormone
{Prolactin-inhibiting hormone (PIH)
Stimulates release of prolactin
Prolactin-inhibiting hormone (PIH)
Inhibits release of prolactin

Growth Hormone Activity
Increases plasma free fatty acids (FFA) - source of energy for muscle tissue
Increases hepatic glucose output
Decreases insulin sensitivity in muscle
Is protein anabolic hormone
Growth Hormone Activity
Exerts its growth-promoting through interactions [mainly induction of Insulin-like Growth Factor I (IGF-I)].
IGF-I synthesis is stimulated by GH
Major source of IGF-I is the liver; IGF-I is also locally produced in other tissues

• Hypothalamic stimulation–from CNS • Pituitary stimulation–from hypothalamic trophic Hs• Endocrine gland stimulation–from pituitary trophic Hs
Endocrine Control: Three Levels of Integration

Endocrine Control: Three Levels of Integration
Figure 7-13: Hormones of the hypothalamic-anterior pituitary pathway
• Stimuli– Stretch– Glucose– Insulin levels
• Reflex– Lower blood glucose– Reduces stimulus– Reduces insulin release
Multiple Stimuli for Hormone Release:
Nervous & Endocrine
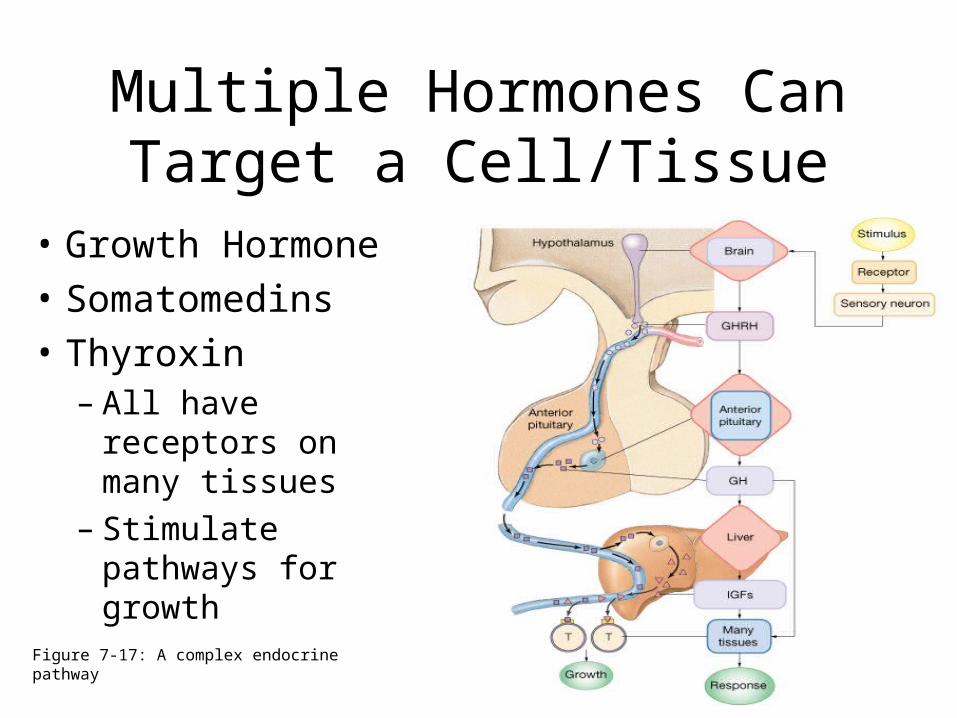
• Growth Hormone
• Somatomedins
• Thyroxin– All have receptors
on many tissues– Stimulate pathways
for growth
Multiple Hormones Can Target a Cell/Tissue
Figure 7-17: A complex endocrine pathway
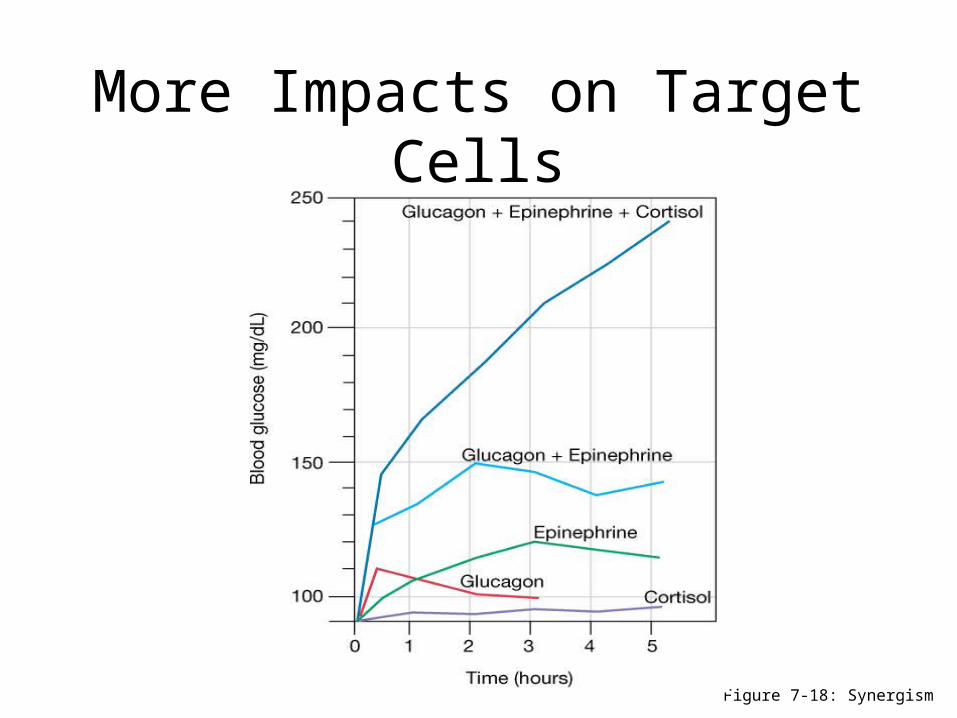
• Synergism: multiple stimuli more than additive– Cortisol +5– Glucagon +10– Epinephrine +20 (added = +35)– Synergistic effect + 140
• Antagonism: glucagons opposes insulin
• Permissiveness: need 2nd hormone to get full expression
More Impacts on Target Cells
More Impacts on Target Cells
Figure 7-18: Synergism
Posterior Pituitary
Comprised of the endings of axons from cell bodies in the hypothalamus (supraoptic and paraventricular)
Axons pass from the hypothalamus to the posterior pituitary via the hypothalamohypophysial tract
Posterior pituitary hormones are synthesized in the cell bodies of neurons in the supraoptic and paraventricular nuclei
Posterior Pituitary
Hormones synthesized in the hypothalamus are transported down the axons to the endings in the posterior pituitary
Hormones are stored in vesicles in the posterior pituitary until release into the circulation
Principal Hormones: Vasopressin & Oxytocin
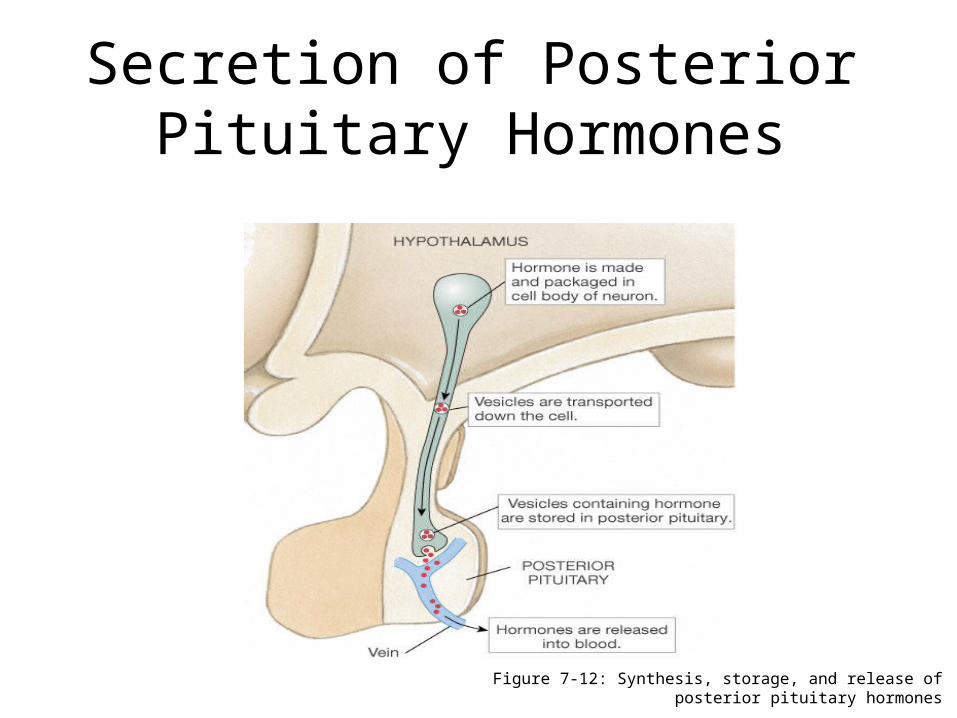
Secretion of Posterior Pituitary Hormones
Figure 7-12: Synthesis, storage, and release of posterior pituitary hormones

Oxytocin
Is synthesized as the precursor hormone: prepro-oxyphysin
Acts primarily on the mammary gland and uterus
Increases contraction of smooth muscle of the vas deferens
Oxytocin
Secretion is increased during labor
May also act to facilitate sperm transport in uterus (non-pregnancy state)

Posterior Pituitary: Regulation of Osmolality
Plasma osmolality is monitored by osmoreceptors in the hypothalamus
Increases in plasma osmolality stimulates secretion of vasopressin
Small changes above the normal plasma osmotic pressure (285 mosm/kg) stimulate release of vasopressin
Vasopressin (ADH)
Is also known as antiduretic hormone (ADH)
Participates in body water regulation (Water is lost from lungs, sweat, feces and urine on a daily basis)

Osmolality
• Refers to the amount of solutes in a solution
• Loss or gain of water without solutes (free water
gain or loss) changes the osmolality of ECF
• Must be regulated to maintain normal cell activity

Vasopressin (ADH) Secretion
Secretion is Stimulated by:
1. Large decreases in blood volume
2. Decreases in blood pressure
3. Pain, fear, trauma, and stress
Vasopressin Activity
Decreases water excretion by kidneys (V2 receptors)
Constricts blood vessels (V1 receptors)- arteriolar smooth muscle
Increases adrenocorticortropin hormone (V1B receptors) secretion from the anterior pituitary
AVP and Water Balance
• The maintenance of water balance in the body is extremely important for proper functioning of cells.
• There are two main compartments of the body: intracellular and extracellular (includes interstitial space and plasma).
• Water moves freely between compartments depending upon osmotic gradients.
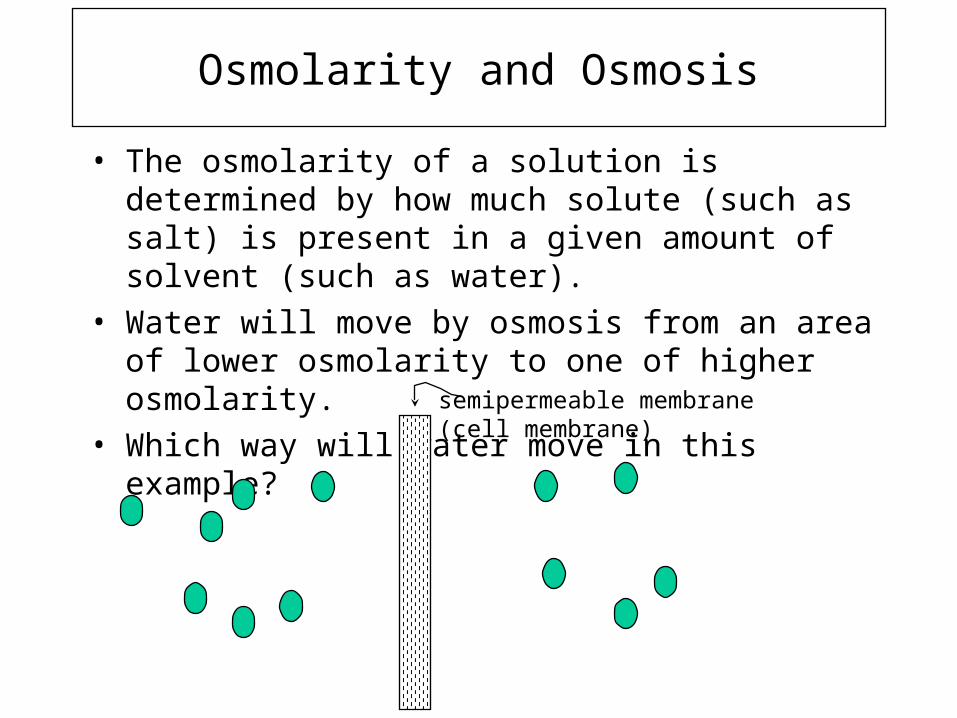
Osmolarity and Osmosis
• The osmolarity of a solution is determined by how much solute (such as salt) is present in a given amount of solvent (such as water).
• Water will move by osmosis from an area of lower osmolarity to one of higher osmolarity.
• Which way will water move in this example?semipermeable membrane(cell membrane)

The Main Point....
• If there is insufficient fluid in the extracellular space, osmolarity increases, and water will begin to leave cells.
• This is a bad thing to have happen, cells will not be happy!
• One must regulate the amount of water in the body.
The Role of the Kidney in Water Balance
• The kidney removes about 170 liters/day of water from the blood.
• 99% of this water is reabsorbed from the urine back into the bloodstream.
• The kidney is an important site at which the water content of the body is regulated.
AVP and Water Balance
Old name: antidiuretic hormone (ADH) From where? Synthesized in the brain (what part?), released from
posterior pituitary. Stim by hypo-osmotic neurons in response to incr
osmolarity of blood or decr blood vol., and by pain, some drugs, low bp.
Action: increases permeability of the distal convoluted tubule and collecting ducts to water
Result: - increased water reabsorption from urine- decreased urine volume- decreased osmolality of interstitial fluids- increased blood pressure
Regulation of AVP Secretion
Response to osmolality of interstitial fluid:- Osmoreceptors in the brain detect changes in osmolality of the interstitial fluid or blood.- Increased osmolality results in increased [solutes] AVP release- increased water reabsorption- decreased osmolality of fluids- Decreased osmolality results in decreased ADH release = NEGATIVE FEEDBACK!- decreased water reabsorption- increased osmolality of fluids
Regulation of AVP Secretion
Response to changes in blood pressure:- Blood pressure receptors in heart, aortic arch, and carotid artery- Increased blood pressure results in decreased AVP release
- decreased water reabsorption- decreased blood volume, blood pressure
- Decreased blood pressure results in increased AVP release
- increased water reabsorption- increased blood volume, pressure
Regulation of AVP Secretion AVP release is also inhibited by alcohol, caffeine
(diuretics) – dehydrating effect “dry mouth” or intense thirst morning after INCREASED urine output.
- decreased water reabsorption- increased urinary volume- potential for dehydration
Some drugs can also antagonize ADH release: diuretics used to treat high bp, edema, or CHF.
Insufficient AVP results in disease: diabetes insipidus (DI)- impaired water reabsorption from DCT, collecting ducts- increase urine volume 10 times and intense thirst.
DI can be caused by a blow to the head or other hypothalamic damage.
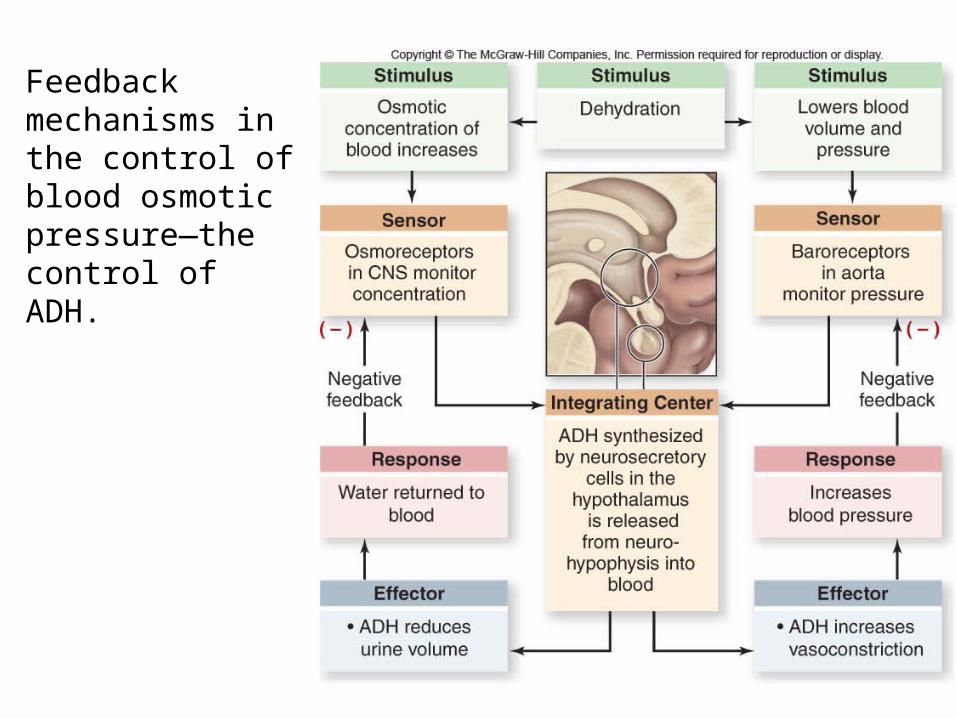
Feedback mechanisms in the control of blood osmotic pressure—the control of ADH.
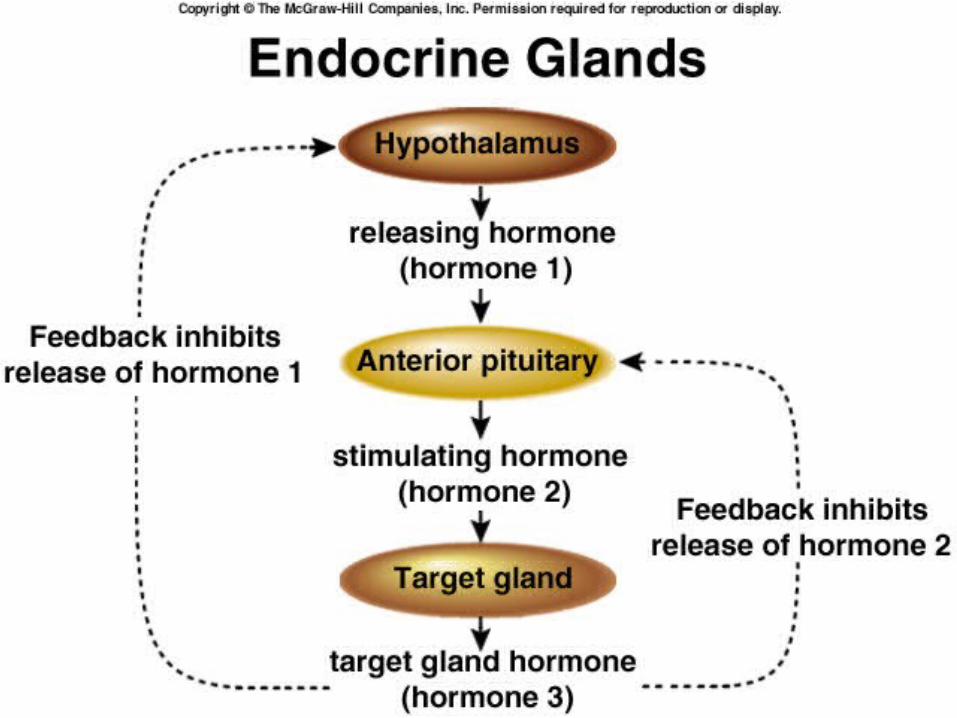
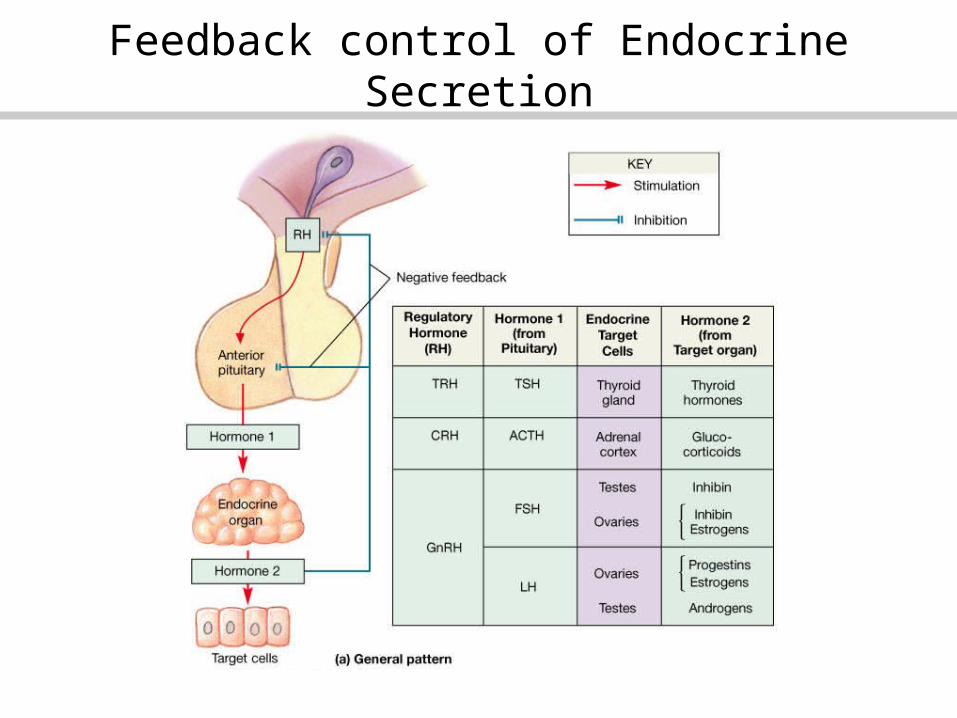
Feedback control of Endocrine Secretion

Feedback control of Endocrine Secretion

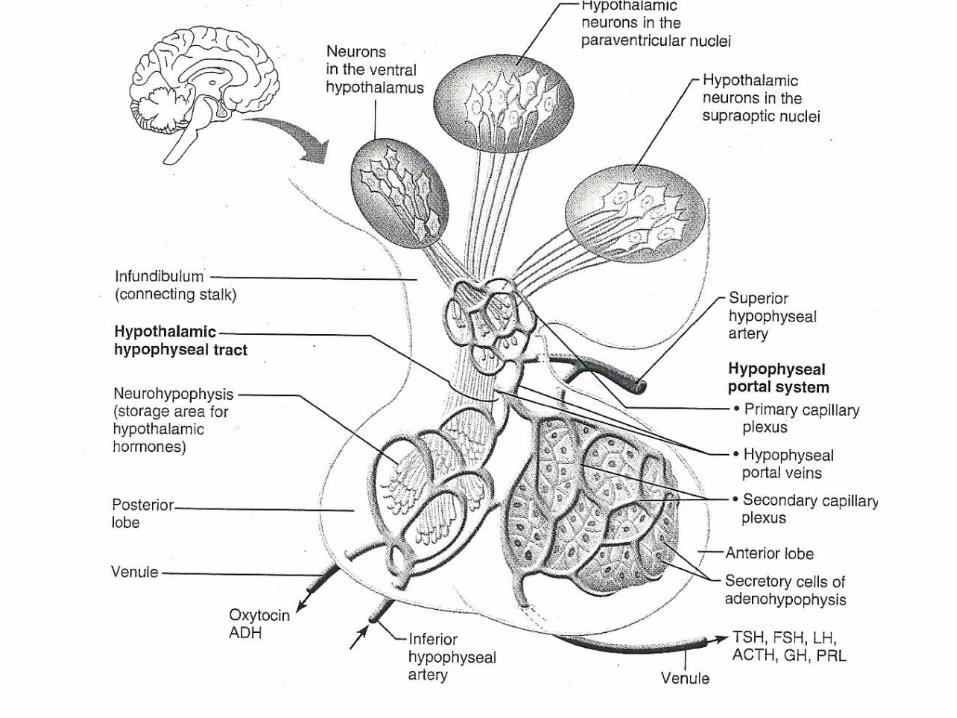
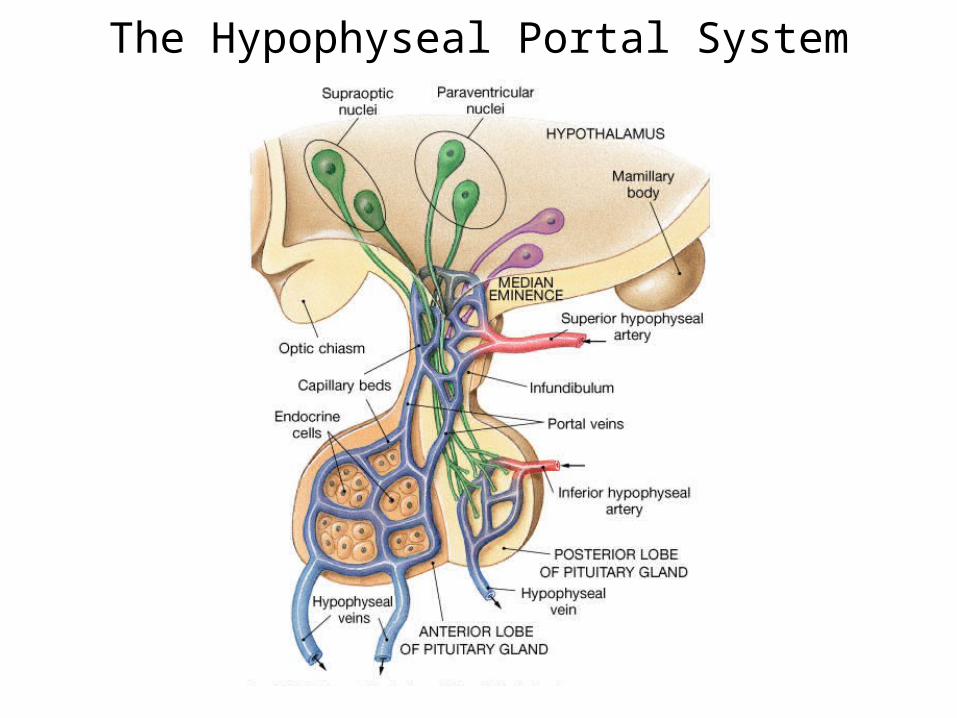
The Hypophyseal Portal System

Negative Feedback Controls: Long and Short Loop Reflexes
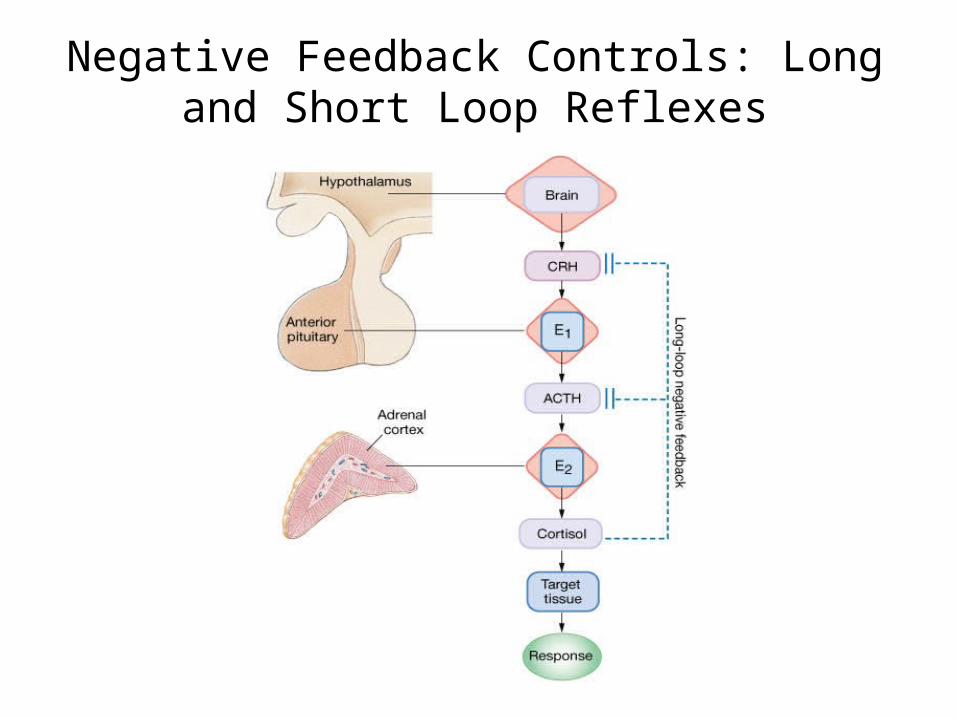
Negative Feedback Controls: Long and Short Loop Reflexes

• "no bad hormones – just too much or too little"• Exogenous medication
– Replaces & exceeds normal– Cause atrophy of gland
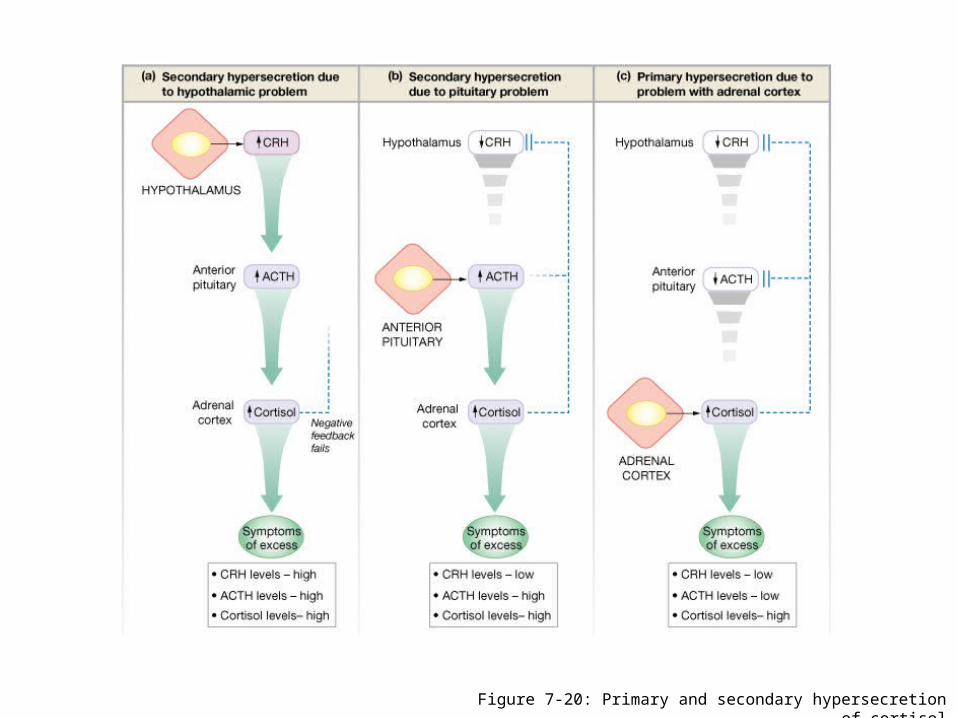
• Hypersecretion: too much– Tumors or cancer– Grave's disease- thyroxin
• Hyposecretion: too little– Goiter – thyroxin– Diabetes – insulin
Pathologies: Over or Under Production

Pathologies: Over or Under Production

• Downregulation – hyperinsulinemia
• Transduction abnormalities– Testicular feminization syndrome– Pseudohypothyroidism
• Abnormalities of control mechanisms
Pathologies: Due to Receptors
Pathologies: Due to Receptors
Figure 7-20: Primary and secondary hypersecretion of cortisol

















