Page 1
Gregory Y. Lauwers, M.D. Vice Chairman
Department of Pathology
Director, Gastrointestinal Pathology Service
Massachusetts General Hospital
Professor of Pathology
Harvard Medical School, Boston, MA
Iatrogenic Pathology of the Intestines:
The More You Look, The More You Find!
Page 2
• Various (but limited) GI side-effect: diarrhea,
constipation, nausea and vomiting.
• Entire gut is variably affected.
• Various mechanisms & patterns of injury: o Erosions/ulcerations/necrosis/fibrosis & stenosis
o Hyperplastic/reactive changes
o Inflammatory infiltrate (lymphocytes/eosinophils)
o Crystals deposition
o Apoptosis / Mitotic arrest / abnormal mitoses
Iatrogenic gut damages are common:
2-8% of pts receiving drugs experience an adverse reaction.
Page 3
Generic injury patterns Specific injury patterns Drugs
Inflammation FAC NSAIDs, NaPO4
Chronic colitis NSAIDs
Microscopic colitis NSAIDs, lansoprazole, ranitidine, PPI, ticlopidine, simvastatin, paroxetine carbamazepine, penicillin, flutamide, cyclo 3 Fort, sertraline
Hypereosinophilia NSAIDs, Estroprogestatifs, Plavix?
Malakoplakia Corticosteroids
Pseudomembranous colitis Antibiotics, PPI
Fibrosis Diaphragms NSAIDs
Strictures KCL, Pancreatic enzymes
Architectural Dilated/damaged crypts
Villous atrophy Sulindac, Mycophenolate, NSAIDs, azathioprine, Olmesartan
Ischemia Ischemic colitis NSAIDs, kayexalate, cocaine, diuretics, sumatriptan,dopamine, methysergide, amphetamines, estrogens, ergotamine, alostron, digitalis, pseudoephedrin, vasopresin, interferon
Pseudomembranous colitis
Apoptosis / IELs ‘Apoptotic ileitis / colitis’ Mycophenolate, Ipilimubab NSAIDs, NaPO4, 5-FU
Melanosis coli NSAIDs; Laxatives
Increased / abnormal mitosis Increased number Colchicine/ Taxane
Mitotic arrest
Erosion / perforation NSAIDs, KCL, Iron, Kayexalate, Cochicine, Yttrium 90,corticosteroids
Epithelial atypia IV cyclosporin
Dx methodology: temporal relationship / improvement with
withdrawal & test w/ rechallenge is ‘unpractical’.
….in most cases: index of suspicion / clinicopathologic exercise
Page 5
Mimics of Enteropathies (e.g., celiac disease)
• Various drugs can elicit intraepithelial
lymphocytosis with or without epithelial
damage,
– Olmesartan, angiotensin II receptor antagonist
(Benicar®)
– CTLA-4 monoclonal antibody (ipilimumab®)
adjuvant to tumor vaccination therapy
(melanoma, RCC, ovarian Ca).
Page 6
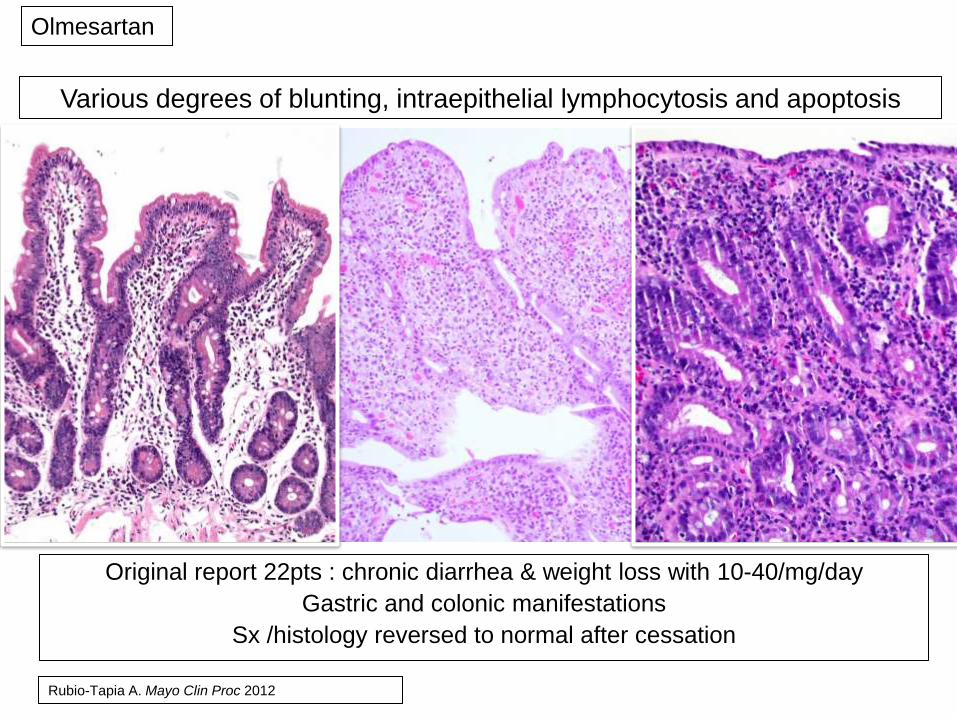
Original report 22pts : chronic diarrhea & weight loss with 10-40/mg/day
Gastric and colonic manifestations
Sx /histology reversed to normal after cessation
Various degrees of blunting, intraepithelial lymphocytosis and apoptosis
Olmesartan
Rubio-Tapia A. Mayo Clin Proc 2012
Page 7
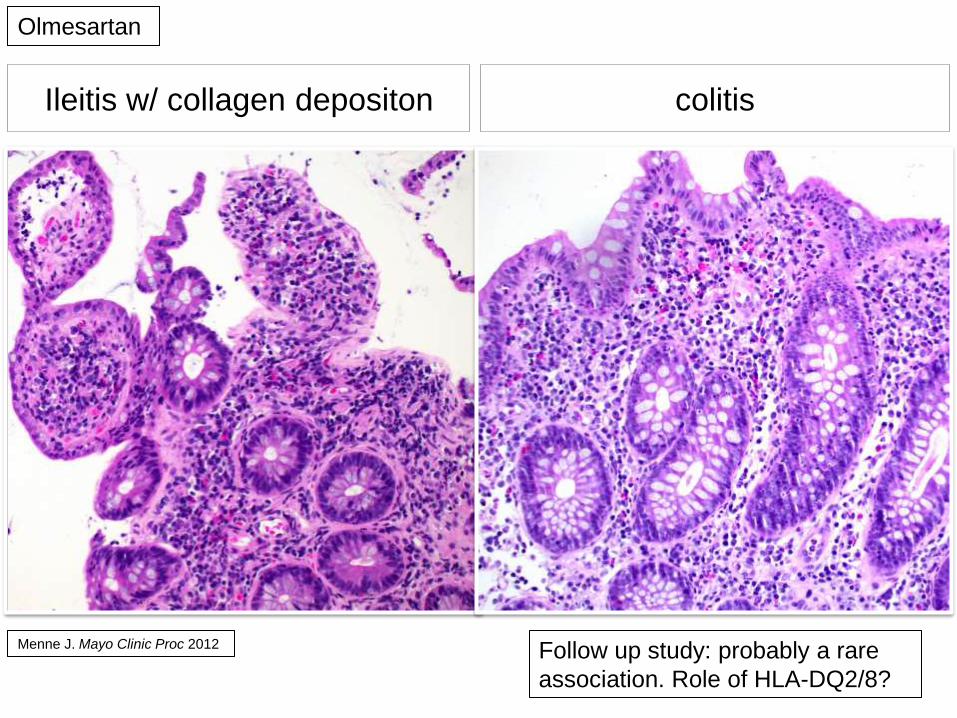
Ileitis w/ collagen depositon colitis
Olmesartan
Menne J. Mayo Clinic Proc 2012 Follow up study: probably a rare
association. Role of HLA-DQ2/8?
Page 8
APOPTOTIC & EROSIVE PATTERNS OF
INJURY
• Immunosuppressive or antineoplastic agents
(predominantly).
– Mycophenolic Acid
– CTLA-4 monoclonal antibody
– Anti-metabolites (methotrexate; capecitabine)
– TNF-α antagonists (infliximab)
Page 9
Effects of Bowel Prep (Oral NaP)
Driman DK Human Pathol 1998
o Focal active colitis: 3.5%
o Increased crypt apoptosis (>5 apoptotic bodies/100 crypts)
o Normal architecture
Page 10
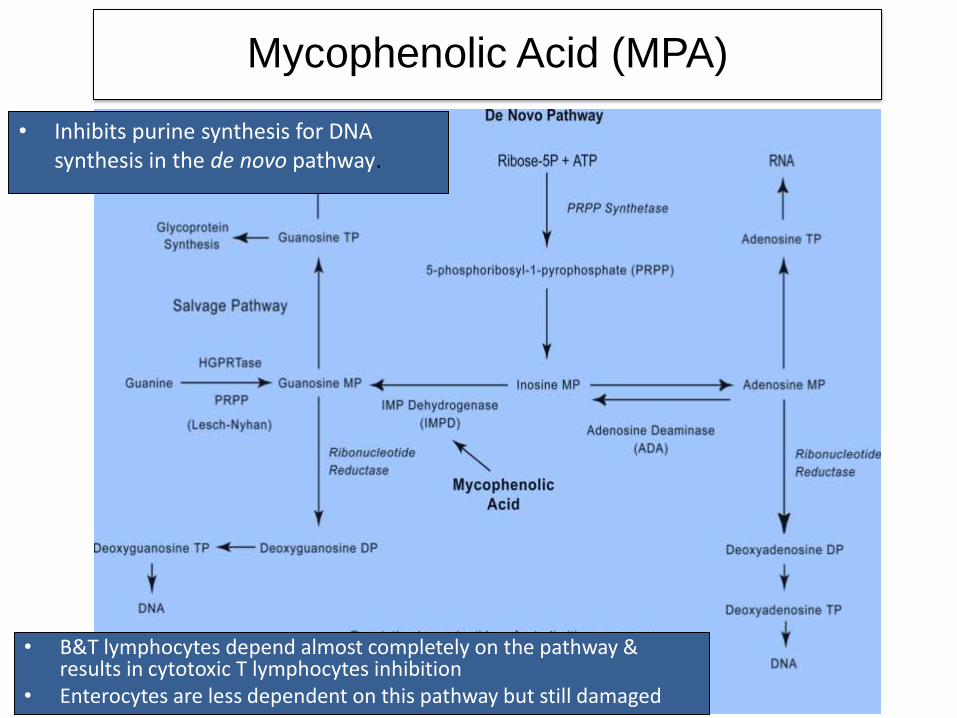
Mycophenolic Acid (MPA)
• B&T lymphocytes depend almost completely on the pathway & results in cytotoxic T lymphocytes inhibition
• Enterocytes are less dependent on this pathway but still damaged
• Inhibits purine synthesis for DNA synthesis in the de novo pathway.
Page 11
• mycophenolate mofetil (CellCept®),
• mycophenolate sodium (Myofortic®)
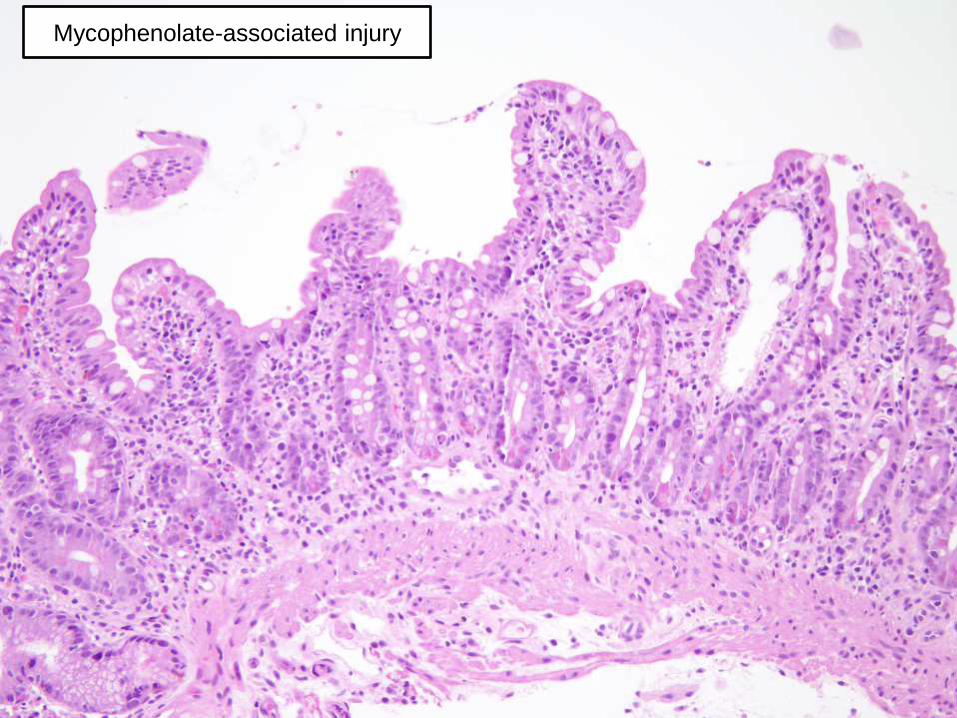
• Gastrointestinal injuries in ~45% of pts:
o GVHD like alterations throughout the GIT
o Active esophagitis with ulceration or erosion,
o Chemical gastropathy; focally enhanced gastritis,
o Crohn-like damages in the duodenum.
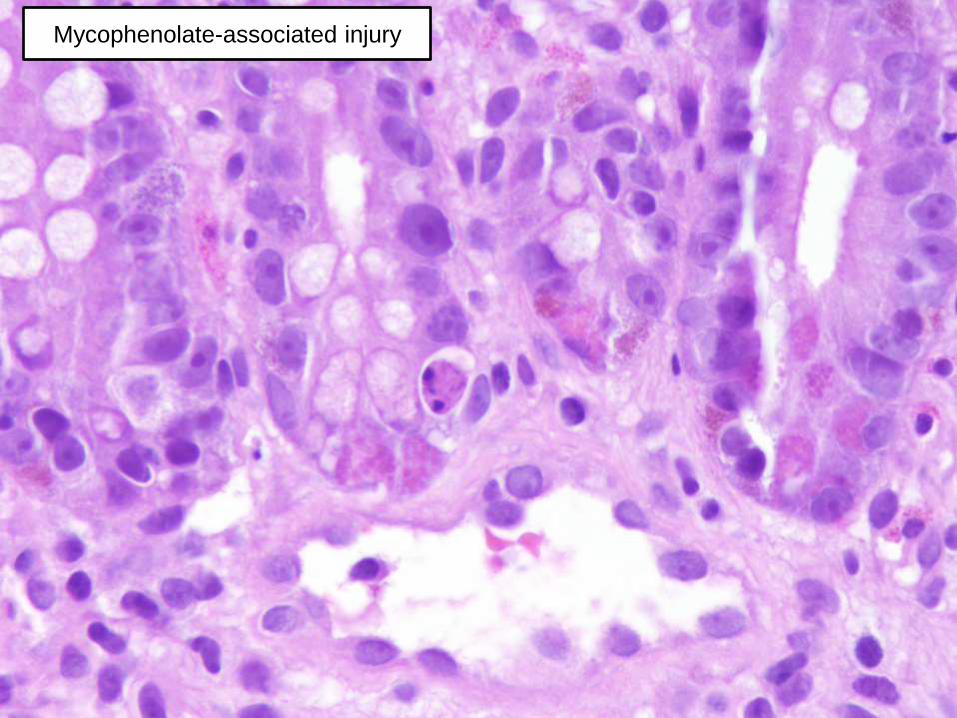
o Cryptitis, crypt withering and distortion, reparative
changes and increased neuroendocrine cells in colon.
Mycophenolic Acid (MPA)
Page 12
Mycophenolate-associated injury
Page 13
Mycophenolate-associated injury
Page 14
Mycophenolate-associated injury
Colon
Page 15
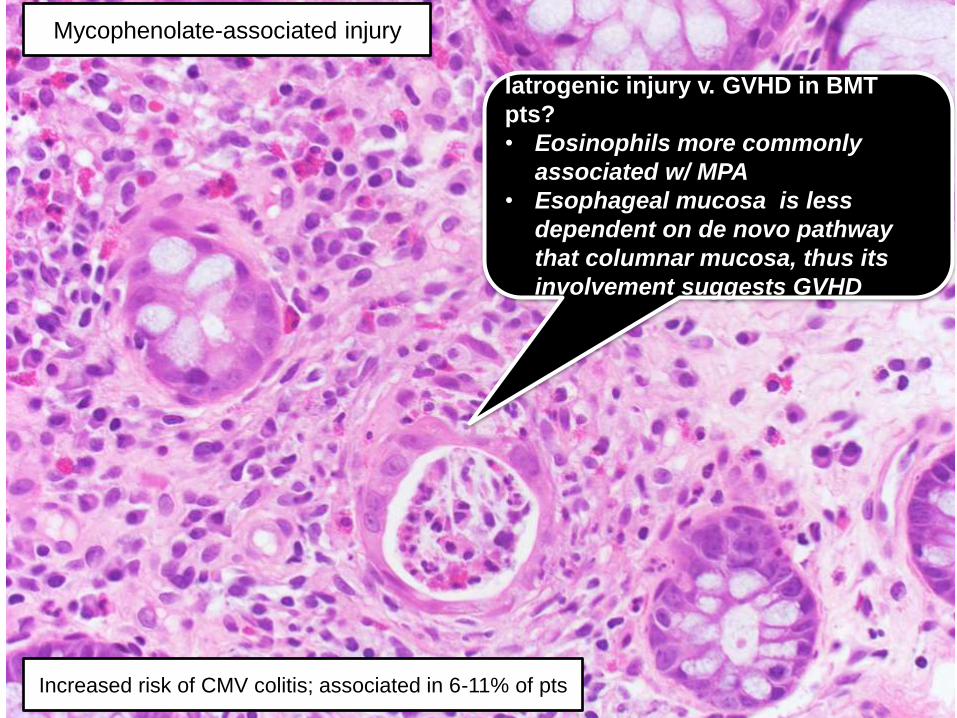
Iatrogenic injury v. GVHD in BMT
pts?
• Eosinophils more commonly
associated w/ MPA
• Esophageal mucosa is less
dependent on de novo pathway
that columnar mucosa, thus its
involvement suggests GVHD
Mycophenolate-associated injury
Increased risk of CMV colitis; associated in 6-11% of pts
Page 16
CTLA-4 monoclonal antibody (ipilimumab®)
• How does if works? – CTLA-4 is expressed on Tregs and following antigenic
stimulation, it inhibits T cell signaling and proliferation.
– mAb against CTLA-4 result in increased expansion of tumor-specific T cells & enhancing tumor destruction.
• Complications: – Dermatitis and vitiligo.
– Enterocolitis.
Villous blunting of small bowel / cryptitis in colon
Lymphoplasmacytic expansion of lamina propria, intraepithelial lymphocytosis and apoptosis.
Page 17
CTLA-4 monoclonal antibody (ipilimumab®)
Page 18
CTLA-4 monoclonal antibody (ipilimumab®)
Page 19
CTLA-4 monoclonal antibody (ipilimumab®)
Page 20
CTLA-4 monoclonal antibody (ipilimumab®)
Page 21
Abnormal Mitosis & Mimics of Dysplasia
• Eosinophilic transformation w / w-o withering glandular structures
• Nuclear pseudostratification
• Vacuolated cytoplasm
• Monster nuclei w/w-o nucleoli intermixed w/ normal nuclei
• Apoptosis / Mitotic arrest atypical mitotic figures
• Eosinophilic inflammation; Lymphocytic exocytosis
• Stromal edema or fibrosis
• Ectatic capillary vessels
Page 22
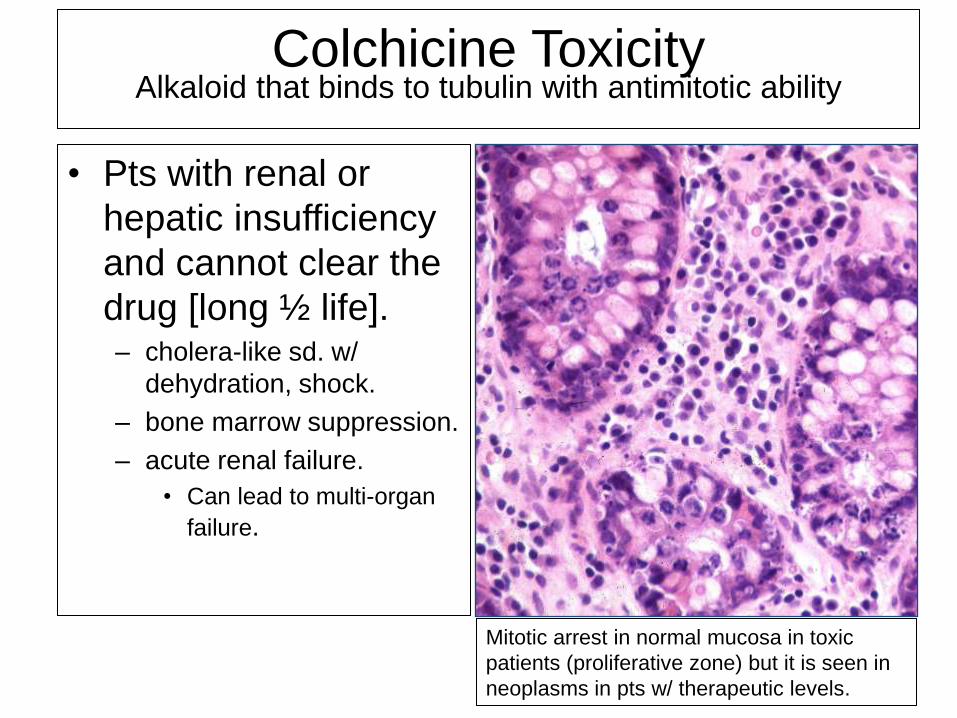
Colchicine Toxicity
Alkaloid that binds to tubulin with antimitotic ability
• Pts with renal or
hepatic insufficiency
and cannot clear the
drug [long ½ life]. – cholera-like sd. w/
dehydration, shock.
– bone marrow suppression.
– acute renal failure.
• Can lead to multi-organ
failure.
Mitotic arrest in normal mucosa in toxic
patients (proliferative zone) but it is seen in
neoplasms in pts w/ therapeutic levels.
Page 23
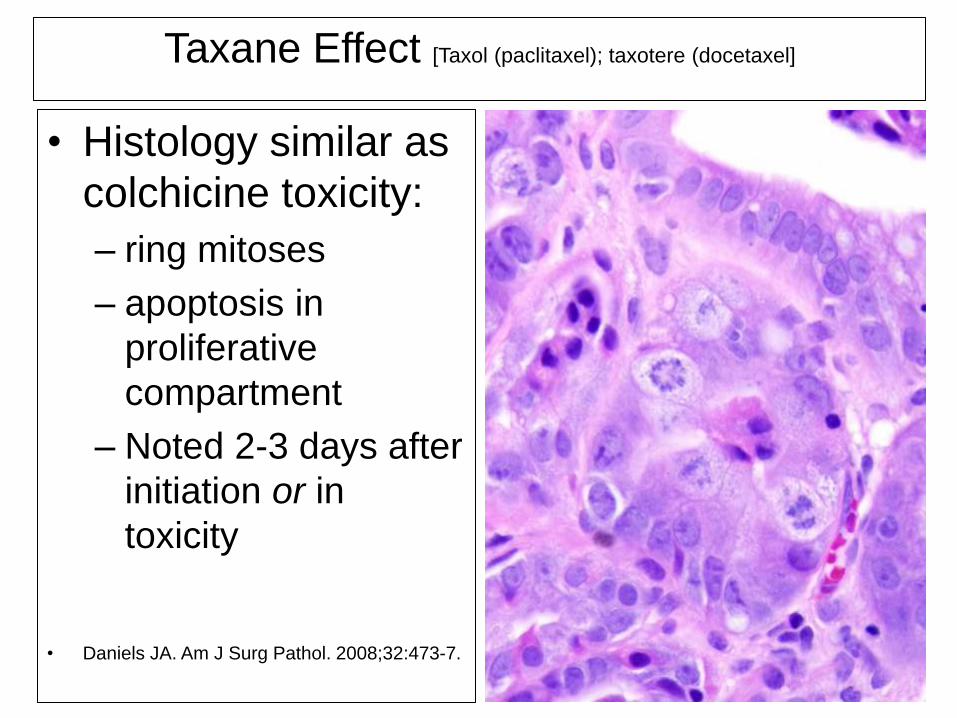
Taxane Effect [Taxol (paclitaxel); taxotere (docetaxel]
• Histology similar as
colchicine toxicity:
– ring mitoses
– apoptosis in
proliferative
compartment
– Noted 2-3 days after
initiation or in
toxicity
• Daniels JA. Am J Surg Pathol. 2008;32:473-7.
Page 25
Rectal Cancer protocol: Folfiri
Page 26
Ulcerative & Chronic Ileitis / Colitis
Pattern of Injury
• NSAIDs and other compounds can present w/ an
ulcerative & chronic patterns of mucosal injury.
• NSAIDs block cyclo-oxygenases 1 and 2.
– Incidence of adverse effects reported in up to
70% with long-term Rx
– Major pathology: ulceration and hemorrhage,
more likely with high doses.
Page 27
Prevalence of NSAID-induced enteropathy is
underestimated. – > 50% of pts have
mucosal damage in the
Small Bowel (Video
capsule endoscopy).
– Mucosal erythema,
– Erosions, ulcers,
perforation
– Diaphragm disease and
strictures.
Page 28
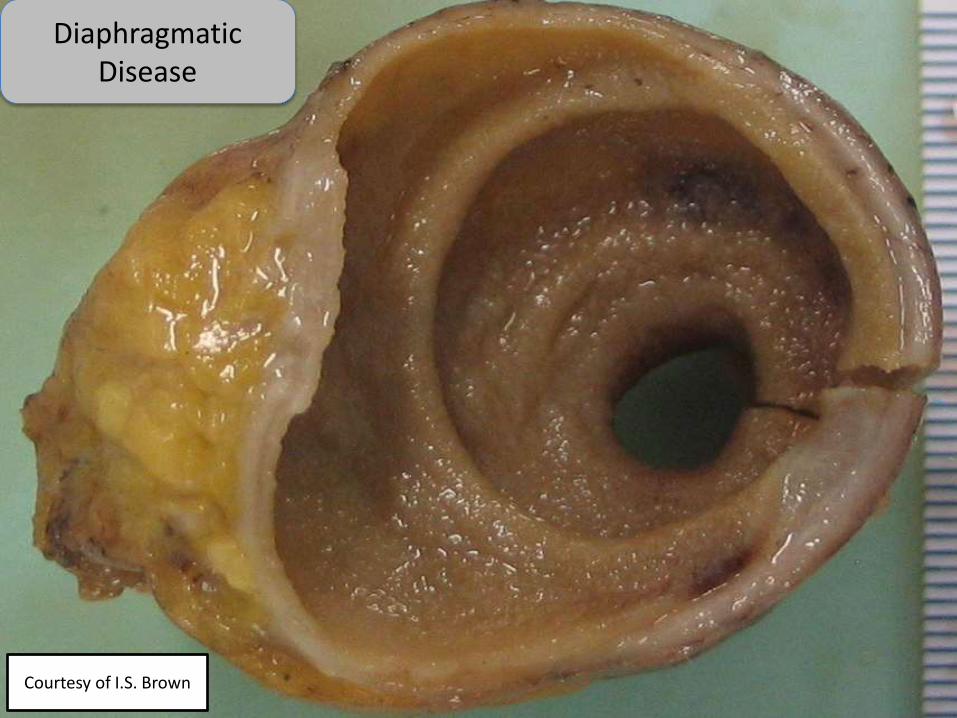
Diaphragmatic Disease
Courtesy of I.S. Brown
Page 29
1 2
3
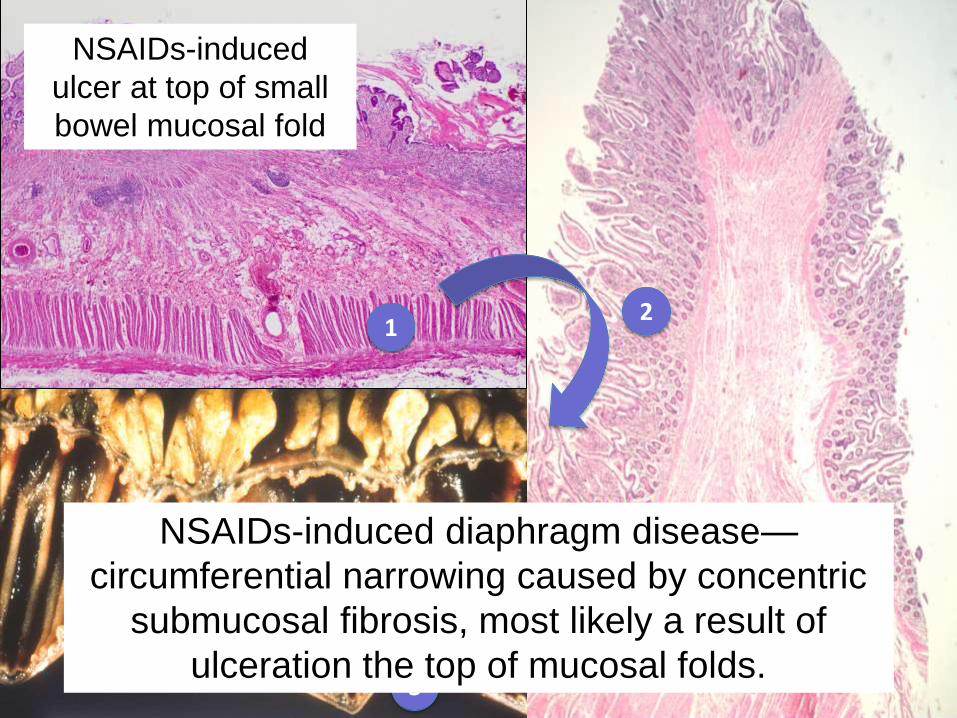
NSAIDs-induced
ulcer at top of small
bowel mucosal fold
NSAIDs-induced diaphragm disease—
circumferential narrowing caused by concentric
submucosal fibrosis, most likely a result of
ulceration the top of mucosal folds.
Page 30
NSAIDs and colonic damage: a long tale
Possibly increasing due to use of enteric coated or
sustained (slow) release formulation (higher concentrations in
the prox. colon)
• Various types of Colitis
– Focal active colitis and chronic colitis.
– Collagenous colitis and Lymphocytic colitis
– Pseudomembranous colitis (Diclofenac®)
– Eosinophilic colitis (Naproxen®)
– Ulcers (Rt colon)
– Diaphragm disease
– Exacerbation of pre-existing IBD or diverticular disease (or
perforation)
Page 31
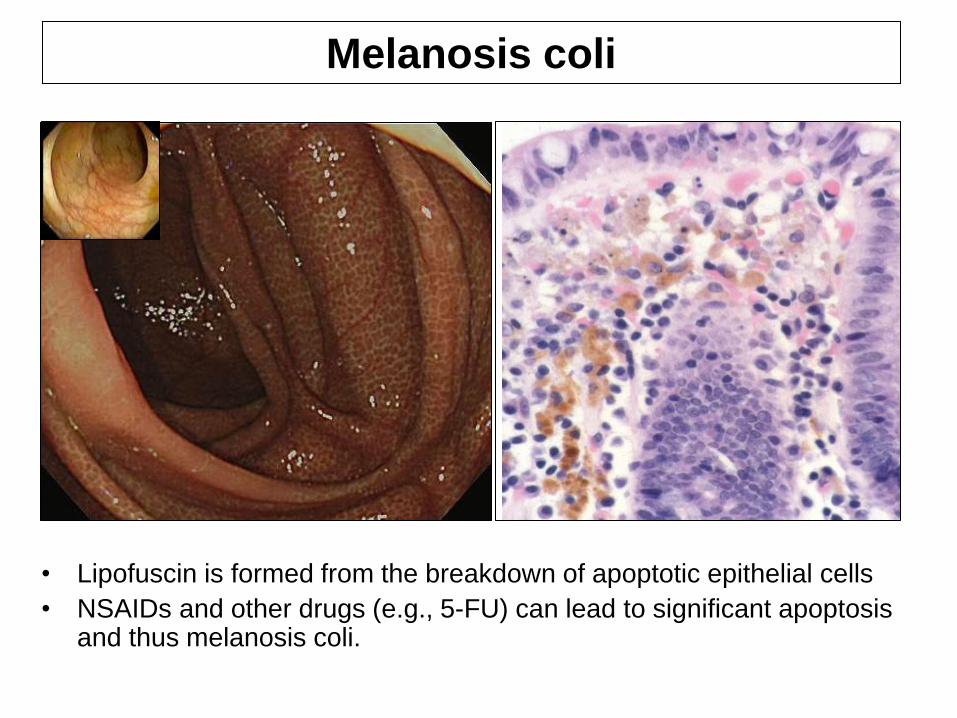
• Lipofuscin is formed from the breakdown of apoptotic epithelial cells
• NSAIDs and other drugs (e.g., 5-FU) can lead to significant apoptosis and thus melanosis coli.
Melanosis coli
Page 32
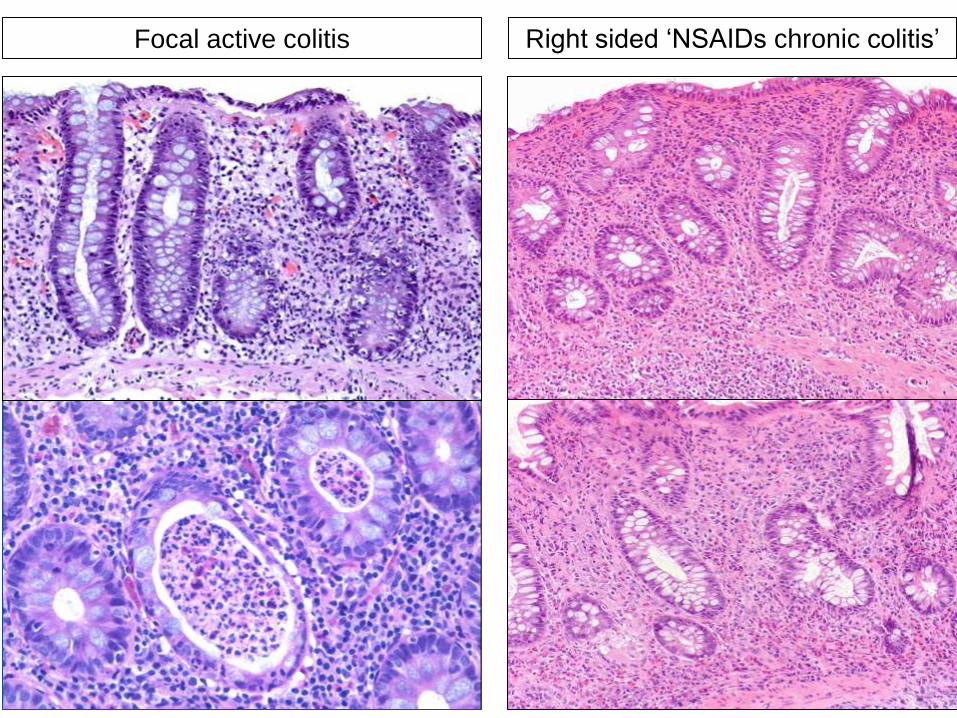
Focal active colitis Right sided ‘NSAIDs chronic colitis’
Page 33
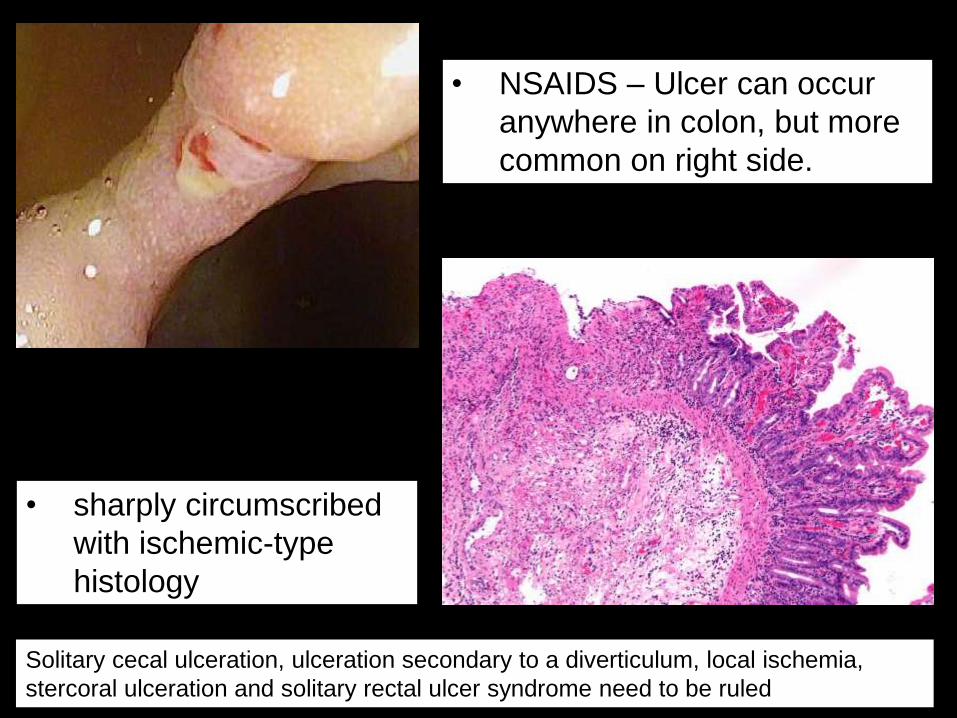
• NSAIDS – Ulcer can occur
anywhere in colon, but more
common on right side.
• sharply circumscribed
with ischemic-type
histology
Solitary cecal ulceration, ulceration secondary to a diverticulum, local ischemia,
stercoral ulceration and solitary rectal ulcer syndrome need to be ruled
Page 34
• Crypt disarray, erosion, cryptitis & crypt abscesses but:
– (no marked cryptic architectural distortion)
– No basal lymphocytic infiltrate
• Reactive epithelial changes
• Apoptosis.
• Mild/marked (inflammation:
– lymphocytes, plasma cells, neutrophils
NSAIDs colitis
Goldstein Am J Clin Pathol 1998
Page 35
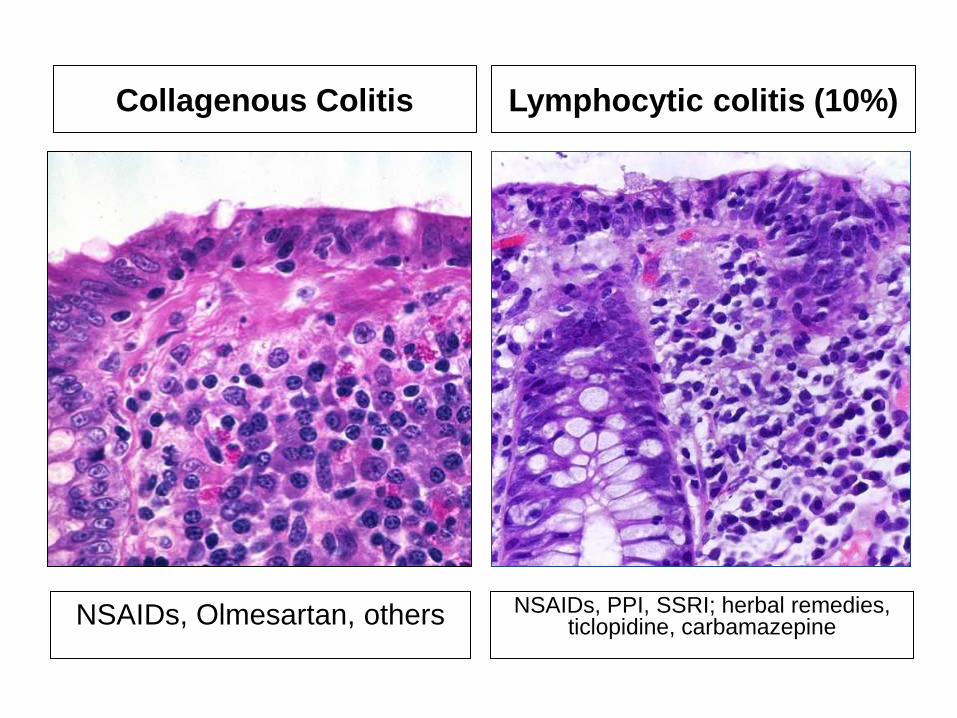
Collagenous Colitis Lymphocytic colitis (10%)
NSAIDs, PPI, SSRI; herbal remedies, ticlopidine, carbamazepine
NSAIDs, Olmesartan, others
Page 36
NSAIDS and ‘microscopic colitis’
Collagenous colitis
• Case control study of 31
pts w/ collagenous colitis
– 19 patients using NSAIDs
(vs. 4 controls)
– All developed diarrhea after
beginning NSAID therapy
– 3 improved with
discontinuation of NSAIDs
– 1 re-challenged: recurrence
of diarrhea
• 40 pts w/ lymphocytic
colitis
– Half taking NSAIDs
– Patients on NSAIDs had
higher intraepithelial
lymphocyte counts
– However, no correlation
between NSAID use and
clinical course
Riddell et al. Gut 1992 Wang N, et al. Am J Surg Pathol 1999
Lymphocytic colitis
Page 37
NSAIDs,Digoxin, Cocaine,
Pseudoephedrine
vasopressors
OCP/estrogenic compounds
Eosinophilic colitis Ischemic colitis
Am J Gastroenterol 2004:1175 Aliment Pharmacol Ther 2009;29:535-541
NSAIDs, Gold, L-Tryptophan,
Carbamazepine, Methotrexate,
Tacrolimus, Azothioprine,
Rifampicin, Clozapine
Page 38
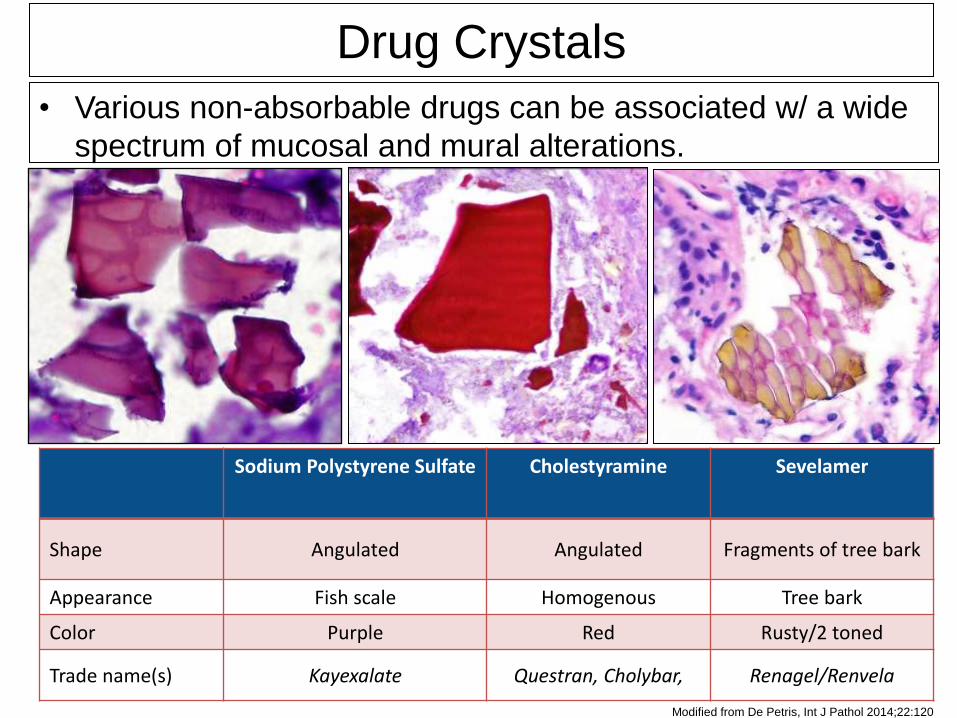
Sodium Polystyrene Sulfate Cholestyramine Sevelamer
Shape Angulated Angulated Fragments of tree bark
Appearance Fish scale Homogenous Tree bark
Color Purple Red Rusty/2 toned
Trade name(s) Kayexalate Questran, Cholybar, Renagel/Renvela
Modified from De Petris, Int J Pathol 2014;22:120
• Various non-absorbable drugs can be associated w/ a wide
spectrum of mucosal and mural alterations.
Drug Crystals
Page 39
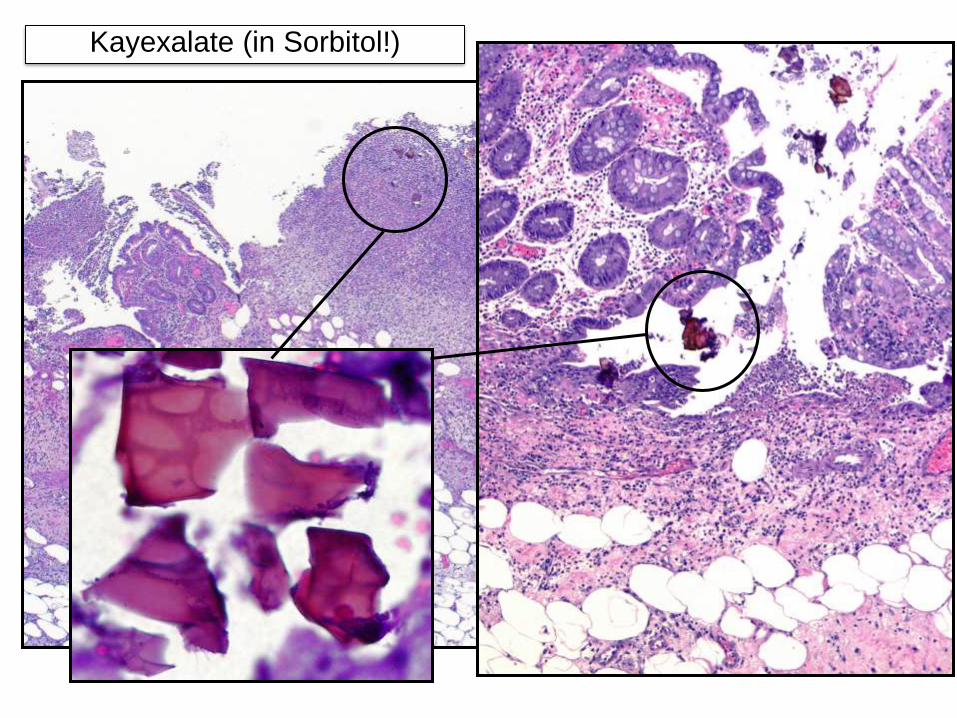
Kayexalate (in Sorbitol!)
• Cation exchange resin used to treat
hyperkalemia
• Administered w/ sorbitol an hyperosmotic
agent to prevent impaction
– Colonic necrosis
– Injury reported in upper GIT but commonly
milder.
Page 40
Kayexalate (in Sorbitol!)
Page 41
DIAGNOSIS OF DRUG INDUCED INJURY IS
(CAN BE) DIFFICULT
• Some compounds are associated w/
characteristic patterns of injury (many
don’t)
• Since the gut has a limited set of response
patterns to injuries
– overlapping features with primary GI
pathology
– clinical correlation is always important (clinical
adverse reaction?).
Page 42
DIAGNOSIS OF DRUG INDUCED INJURY IS
(CAN BE) DIFFICULT
• ….when little or no clinical information is
usually provided!
• Always consider in atypical “itis”.
• Pointers:
– Marked nuclear pleomorphism / cytologic
atypia.
– Atypical mitoses.
– Apoptosis.
– Withering crypts.