78
Diagnosis and Management
| Date post: | 16-Jul-2015 |
| Category: |
Health & Medicine |
| Upload: | katejohnpunag |
| View: | 266 times |
| Download: | 8 times |

Diagnosis and Management

Topics of Focus
Ulcerative Colitis
Disease Classification
Management:
Mild to moderate
Severe, refractory disease
Crohn’s
Pathogenesis
Diagnosis
Management

UC Definition
Chronic disease characterized by diffuse mucosal inflammation limited to the colon
Rectum involved in majority of cases
Extends proximally and in a circumferential, continuous fashion Hallmark symptoms: Bloody diarrhea, Urgency, Tenesmus
Abdominal pain, fever, weight loss, extraintestinal complications
Potential Triggers: Smoking cessation
Heavy NSAID use
Isotretinoin
Epidemiology Cause unknown
Hypothesis: Combination of genetic, immune, and
environmental factors thought to contribute
Incidence higher in developed countries
Men and women affected equally
Peak age of onset between 15 and 30 years
Second peak in between 50 and 70 years

UC Disease Classification Extensive:
Inflammation that extends beyond splenic flexure and may involve the entire colon (pancolitis)
20-30% of pts
Associated with higher incidence of colectomy/cancer/mortality
Left sided colitis
Inflammation extends to splenicflexure
30-40% of pts
Proctosigmoiditis
Inflammation extends to rectosigmoid colon
30-40% of pts
Ulcerative proctitis
Inflammation confined to rectum
40% of pts


Clinical Severity IndexTruelove and Witts Criteria
Sign/Symptom Mild Severe
Bowel movements
Rectal bleeding
Temperature (°F)
Pulse (beats/minute)
Hematocrit (%)
Sedimentation rate
<4/d
Intermittent
Normal
<90
Normal
<30
>6/d
Frequent
>37.5° C
>90
<75% normal
>30
Truelove SC, Witts LJ. Br Med J. 1955;2:1041-1048.

Severe Ulcerative Colitis
15% of UC patients develop a severe flare
May occur as the initial presentation of UC
Mortality:
1950s (pre-tx era) 25-60%
1960s 7%
Present 1%

Endoscopic Severity IndexModified Sutherland Scale
Mild Moderate Severe
Edema, loss of
vascular pattern,
granular
Friable, coarsely
granular, pinpoint
ulcerations
Ulcerations,
spontaneous
hemorrhage
Modified from Sutherland LR, et al. Gastroenterology. 1987;92:1894-1898.

DDx of IBD
Infectious
E. coli O157: H7
C diff
Syphilis
TB
Chlamydia
Schistosomiasis
Amebiasis
HSV/CMV
Ischemia
Radiation injury
NSAID
Celiac dz/microscopic colitis
Acute self limited colitis
Irritable bowel syndrome

Goals of Therapy Induction of remission of symptoms
Maintenance of remission of symptoms
Reduction in need for long term steroids
Mucosal healing
Prevention of surgery
Prevention and treatment of extraintestinal
complications

Ulcerative Colitis
Induction Therapies
Mild disease
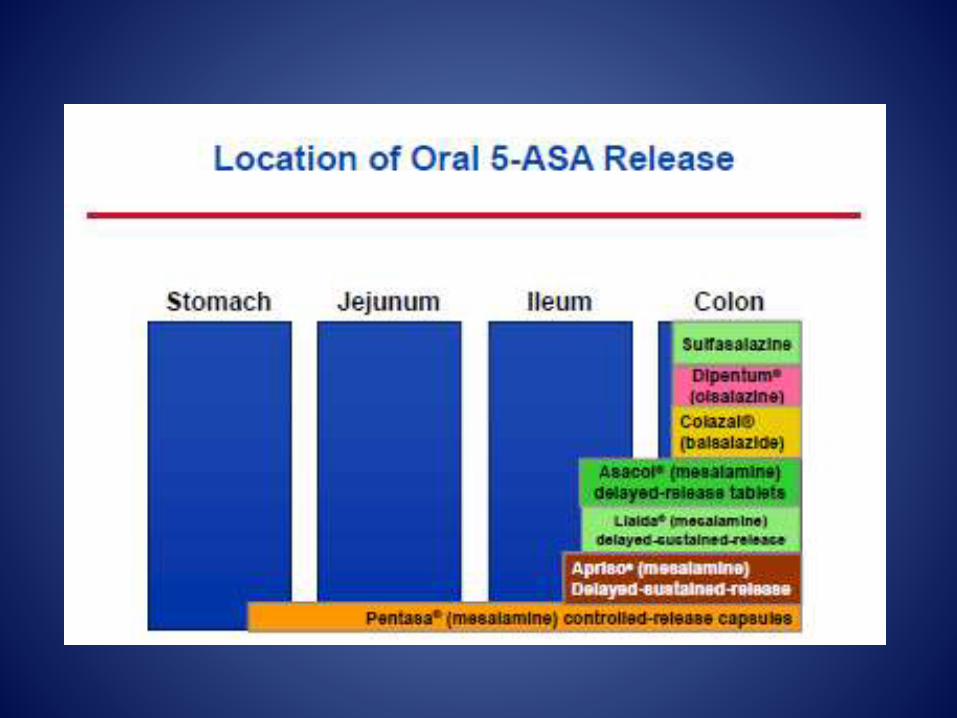
5-ASA
Topical (distal)
Oral (extensive)
Combination
Severe disease
IV steroids
Cyclosporine
Infliximab/Adalimumab
• Moderate disease
– 5-ASA
• Topical (distal)
• Oral (distal)
– Steroid
• Topical (distal)
• Oral (distal/extensive)
Maintenance of Remission
Azathioprine/6-mercaptopurine Immunomodulators inhibit proliferation of T and B
lymphocytes, leading to decreased production of cytotoxicT lymphocytes and plasma cells
Infliximab/Adalimumab Anti-TNF agent neutralizes the biologic activity of TNF-alpha by
inhibiting binding to its receptors. This then leads to decreased cytokine response
Vedolizumab Humanized monoclonal antibody to a4b7 integrin blocks
interaction with MAdCAM-1 and inhibits lymphocyte migration to inflamed tissue
Principles of Corticosteroid
Therapy
Do not under- or overdose corticosteroids:
No benefit with doses > 60 mg prednisone:
Prednisone- 60 mg equivalents:
Solumedrol 4:5 conversion 48 mg
Hydrocortisone 4:1 conversion 240 mg
Use for 3-5 days- if NO response, begin to
consider next step.

Exit Strategies for Severe Steroid Refractory
UC in Hospital…
Cyclosporine
Infliximab
Surgery
Cyclosporine Lipophilic peptide produce by a soil fungus-
Tolypocladium inflatumgams
Blocks production of IL-2 by T-helper lymphocytes
Inhibits T-cell proliferation
Blocks production of B-cell activating factors
Response/remission rates up to 80%

Cyclosporine:
What to check for and how to use it…
Baseline Studies: Creatinine Clearance: >30% dec
GFR is CI
Cholesterol (< 120 mg/dl is CI)
Magnesium (>1.5 mg/dl)
R/O active infection
Therapy protocol: Continue IV steroids
CsA IV 2 mg/kg/day
Prophylactic TMP-SMZ
Monitoring:
CsA levels goal= 200-300 ng/ml
Follow daily labs especially electrolytes
Vitals- may need to tx HTN
Am J Gastroenterol 1997;92:1424

Infliximab for UC: ACT I and II
Clinical Response
Infliximab
- What to check for and how to use it…
Baseline studies
Check for TB
Check for Hepatitis B
R/o superimposed infection (C
diff and CMV)
Premedication: Diphenhydramine: 25-50 mg
PO/IV
Acetaminophen: 650 mg po
Induction dosing:
5 mg/kg- round to closest 100 mg
3 doses at 0,2, and 6 weeks and
every 8 wks thereafter
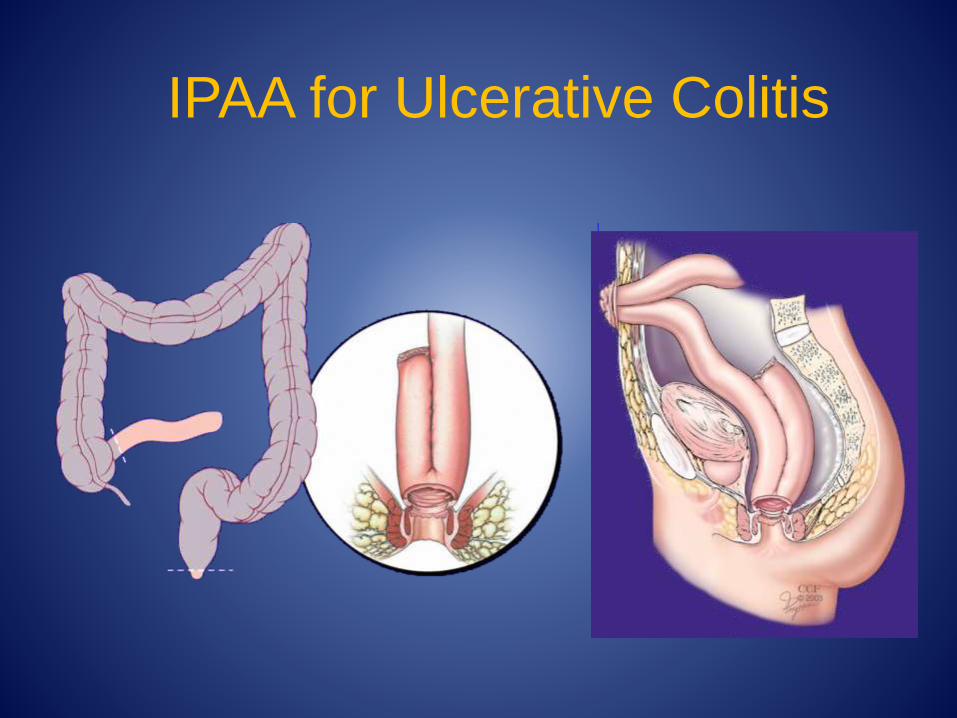
IPAA for Ulcerative Colitis
Putting it all together:
Initial Tx of Severe UC
Daily KUB
IV Solumedrol- 20 mg IV q 8 hrs
NO narcotics, anti-cholinergics
Be wary of superimposed infection:
Stool culture & C. diff
+/- flex sig with biopsy
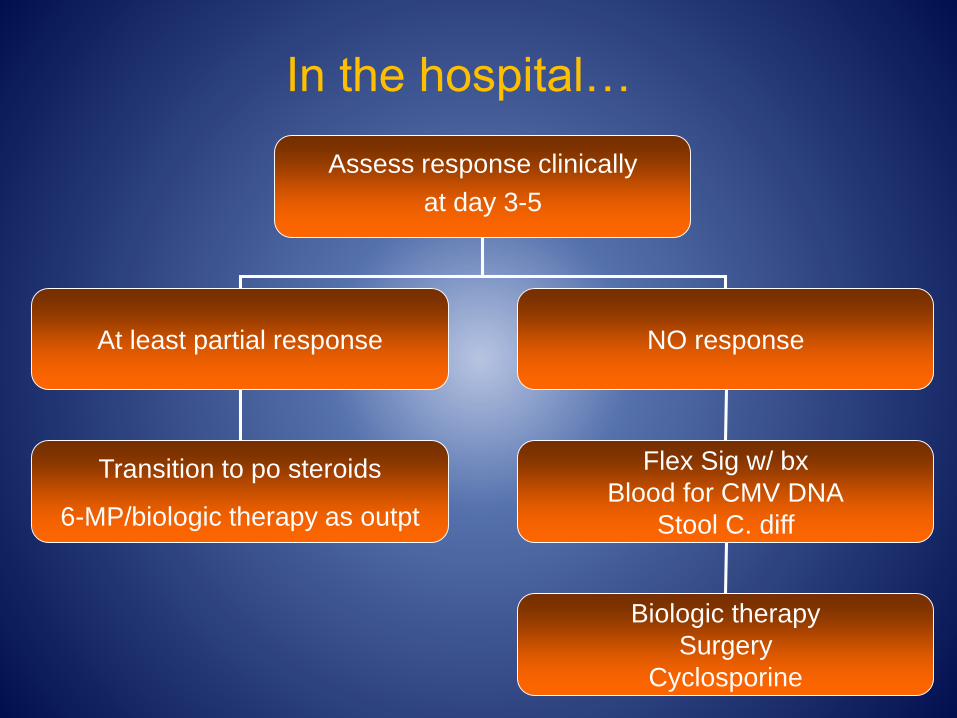
Assess response clinically
at day 3-5
At least partial response NO response
Transition to po steroids
6-MP/biologic therapy as outpt
Flex Sig w/ bx
Blood for CMV DNA
Stool C. diff
Biologic therapy
Surgery
Cyclosporine
In the hospital…
A 37 yo F presents to ED with 2 week history of acute onset bloody diarrhea. Diarrhea has escalated to 15 times/day. She has UC diagnosed 2 years ago and currently takes Azathioprine.
PE: appears ill T 38.9 BP 70/40 P 148 RR 35
Abd: absent bowel sounds; distention, and diffuse marked tenderness with mild palpation
Labs WBC 16.8
KUB as shown
Which of the following is most appropriate management? CT scan
Immediate surgery
Start Infliximab
Start IV Hydrocortisone


Toxic Megacolon Any inflammatory condition of the colon can
predispose to toxic megacolon
Incidence in UC ranges from 8-17%:
Most severe complication associated with UC!
Increased mortality risk:
Range of 19-45%
40% mortality rate in pts undergoing emergent colectomy after a perforation occurred
Hemodynamic instability/progressive abdominal distention/tenderness all indications for immediate surgery
Diagnosis of Toxic Megacolon Diagnosis made on basis of clinical signs and
abdominal plain films
Dilation of transverse or ascending colon > 6 cm
AND at least 1 of the following:
Fever > 38.6° C
Pulse > 120
WBC > 10.5
Anemia

A 45 yo M is evaluated for a 1 week history of non-bloody diarrhea that occurs ten times a day and is accompanied by mild abdominal cramping. He has a 5 year history of ulcerative colitis for which he takes mesalamine.
PE T 37.9 C BP 110/80 P 100
Abd: Hyperactive BS; mild diffuse tenderness; no rebound/guarding
WBC 23 H/H/Plt wnl Bun/Creat 15/1 CRP 32 K 2.9
AAS: normal
Which of the following is the most appropriate diagnostic test to perform next?
Abdominal CT
Colonoscopy
RUQ u/s
Stool for C diff
Crohn’s Disease Focal, asymmetrical, transmural, and occasionally
granulomatous inflammation primarily affecting the GI tract
Most commonly affects 2nd and 3rd decades
Incidence 5/100,000 and on the rise
Prevalence 50/100,000 and on the rise
Disease of “Westernized” countries Incidence increasing in Asian countries
Neither medically nor surgically curable
Cost of medical and surgical tx= $2 billion annually
Inflammatory Cascade
Widely accepted theory: Overly aggressive immune response to bacterial antigens in genetically predisposed individuals
Intestinal microbiota activate immune cells leading to dysregulated cytokine production leading to intestinal inflammation
Additional proposed mechanism
Increased cytokines may modulate composition of commensal flora or alter gene expression in specific bacterial subgroups causing increased growth rates and virulence leading to inflammation

To make a diagnosis of IBD…
History
Clinical symptoms

IBD not to be confused with
IBS…
Symptom IBD IBS
Abdominal pain × ×
Diarrhea × ×
Bloating × ×
Constipation × ×
Mucus in stools × ×
Rectal bleeding/urgency ×
Weight loss ×
Nocturnal symptoms ×
Anemia ×
Elevated inflammatory markers ×
Extraintestinal manifestations ×

To make a diagnosis of IBD…
History
Clinical symptoms

What to check if suspicious for
IBD? CBC
CMP Vitamin D, Vitamin B12
ESR/CRP
Stool cultures
Fecal calprotectin/ lactoferrin

To make a diagnosis of IBD…
History
Clinical symptoms

CD- Endoscopic AppearanceNormal Aphthous ulcers
Serpiginous ulcers Cobblestoning of mucosa
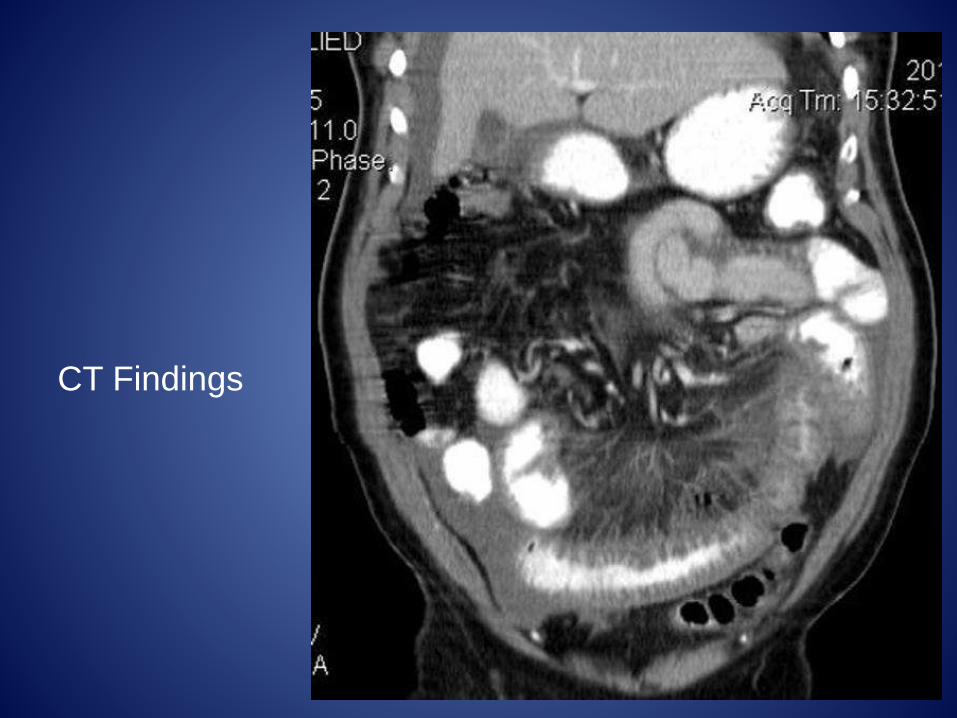
CT Findings

Current Serologic Markers for Crohn’s
Disease IBD-7 serology
ASCA (anti-Saccaromyces cerevisae)
Anti-OmpC (outer membrane porin type C of E. coli)
CBir1
p-ANCA
ASCA thought to be associated with a more aggressive disease phenotype and a risk for surgery

Disease Phenotype
Inflammatory vs Stricturing vs Fistulizing
Location
Ileocolonic= most common location
Ileal
Colonic
Perianal
Upper GI (jejunoileitis) -> most commonly seen in children
Extraintestinal manifestations
Smoker

Cumulative Probability of Surgical
Intervention in CD
Munkholm P, et al. Gastroenterology. 1993;105:1716.
Years
Pro
bab
ilit
y (
%)
0
20
40
60
80
100
0 2 5 8 11 14 17 20
±2 SD
D

Cumulative incidence of surgical resection over 1
yr in Crohn's disease pts starting corticosteroids
Faubion et al, Gastroenterology 2001; 121: 255
38% of patients required surgery within 12 mos
Predictors: TI, stricturing/penetrating dz, age <40.
n=77 Days
Cumulative probability (%)
30 60 90 182 3650
100
80
60
40
20

Cosnes et al. Inflamm Bowel Dis 2002;8:244
The Evolution of Crohn's Disease:
Inflammation Leads to Structural Damage
24022821620419218016815614413212010896847260483624120
0
20
40
60
80
100
Cumulative probability (%)
Patients at risk: Months2002 552 229 95 37n=
Penetrating
StricturingInflammatory
70%
18%
Over a 20-year period, 88% risk of developing stricturing (18%) or penetrating (70%) disease
Vermiere et al, Aliment Pharmacol Ther 2006; 25: 3
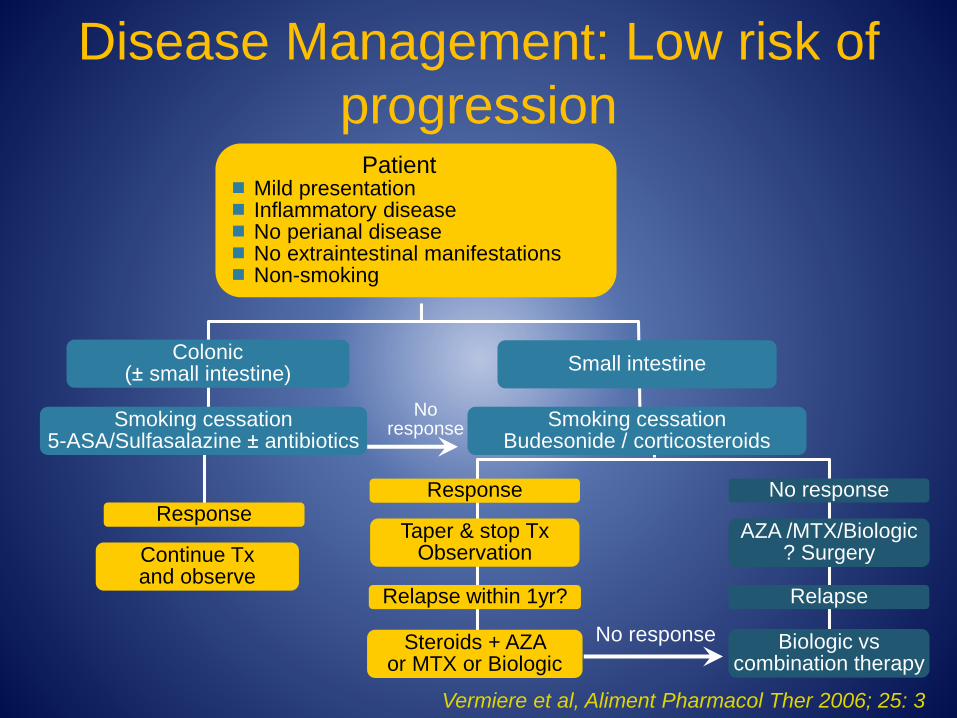
Response
Continue Txand observe
Response
Taper & stop Tx Observation
Relapse within 1yr?
Steroids + AZA or MTX or Biologic
No response
AZA /MTX/Biologic ? Surgery
Relapse
Biologic vscombination therapy
No response
No response
Colonic(± small intestine)
Small intestine
Smoking cessation5-ASA/Sulfasalazine ± antibiotics
Smoking cessationBudesonide / corticosteroids
Patient Mild presentation Inflammatory disease No perianal disease No extraintestinal manifestations Non-smoking
Disease Management: Low risk of
progression

Vermiere et al, Aliment Pharmacol Ther 2006; 25: 3
Patient Young age at onset (<18 yr) Non-inflammatory disease behavior Extensive disease (small/large bowel) Early steroid need Extraintestinal manifestations Active smoker
Response
Taper and stop steroids and continue
immunosuppressants
Smoking cessationSteroids+ AZA or MTX or Biologic therapy
No response
Anti-TNF or combination therapy
Response
Maintenance
No response
Switch therapies
Surgery
Disease Management:
Intermittent to High Risk of Progression

Azathioprine/6-MP
Metabolism
AZA 6-MP
6-MMP
6-TGN
HPRT
6-MMPR
6-TIMP
TPMTTPMT
IMPDH/GMPS
Dosing of 6-MP: 1.5 mg/kg
Dosing of Azathioprine: 2.5 mg/kg
Two Methods of Starting Therapy: Dose escalation to target weight
calculated dose vs starting immediately at weight calculated dose
Check TPMT Enzyme Activity prior to starting therapy

Lab monitoring while on therapy
CBC
Q week for 1 month
Q 2 wks for 1 month
Q 1 month for 3 months
Q 3 months
May need to adjust monitoring parameters if dose escalate
LFTs
Q 3 months
Leukopenias
Pancreatitis
Nausea/vomiting
If occurs with 6-MP, can switch to AZN or vice versa
Allergic reactions
Infections
Hepatotoxicity
Malignancy
Methotrexate
Induction: 25 mg IM/SQ weekly
Maintenance: 15 mg/week
Daily Folic acid supplementation
Adverse reactions:
Nausea/vomiting
Infections
Interstitial or hypersensitivity pneumonitis Check baseline CXR
Potential for myelosuppression and hepatotoxicity
Monitor CBC and especially LFTs closely (Q 1-3 months)

A 19 yo woman is evaluated for a 3 month history of progressively worsening diarrhea, abdominal pain, and weight loss. Her brother was diagnosed with Crohn’s disease at age 16.
PE: T 37.4 BP 110/65 RR 20 P 90
Abd Exam: RLQ tenderness; no rebound/guarding. Rectal exam: normal
C-scope: moderately to severely active CD involving TI with diagnosis confirmed histologically.
MRE: active inflammation involving the distal 20 cm w/o abscess/phlegmon/obstruction
Which of the following is the most effective maintenance treatment:
Ciprofloxacin + Metronidazole
Infliximab
Mesalamine
Prednisone
Surgical Resection

Anti-TNF Quick Review…
Infliximab
Certolizumab pegol
Adalimumab


Anti-TNF agents Check PPD, CXR and Hep B surf antigen prior to initiating
therapy
Immunogenicity
Infusion/ Injection site reactions
Class Effect: Delayed hypersensitivity reactions
Infections
Non-Hodgkin’s lymphoma (including hepatosplenic T-cell
lymphoma in children receiving infliximab + azathioprine)
Other malignancies
Drug-induced lupus
Demyelinating disease
Worsening Heart failure

Sonic Trial!
Randomized, double-blind trial evaluating the efficacy of monotherapy vs combined immunosuppression therapy
508 pts w/ CD immunosuppressive therapy naïve randomized to: Infliximab + placebo capsule
Azathioprine + placebo infusion
Infliximab + Azathioprine
Received medications till week 30 and were given the option to continue in a blinded study extension through week 50
Primary End point: Steroid free remission at week 26
Colombel et al. NEJM ‘10

Primary End Point

Secondary End Point
A 37 yo M is evaluated for a 1 month history of stool leakage. In the past week he has developed perianalpain and low-grade fevers. He was diagnosed 4 years ago with Crohn’s disease involving the small bowel and colon. He is on 6-MP.
PE VSS; normal abdominal exam
Rectal: 2 fistula orifices right anterolateral to the anus with expression of white material with gentle palpation. A fluctuant, tender region that is 1.5 cm diameter is noted left posterolateral to the anus.
In addition to EUA and surgical debridement of abscess cavities and fistula tracts, which is the most appropriate management?
Ciprofloxacin
Corticosteroids
Infliximab
Metronidazole

Perianal fistula
Adequate evaluation of patients with perianal
fistula includes
endoscopy to assess extent of rectal disease and
presence of proximal disease
pelvic floor imaging with magnetic resonance imaging
or anal endoscopic ultrasound
examination under anesthesia
Anti-TNF agents are useful in treating non-
complicated peri-anal fistula
Don’t wait too long, call the colorectal surgeon

A 29 yo F is evaluated for painful red spots on her shins and a recent increase in the frequency of loose stools with some bleeding. She has no other symptoms and was diagnosed with ulcerative colitis 4 years ago. Her only medication is mesalamine.
Exam: few tender, erythematous subcutaneous nodules, each measuring about 1 to 3 cm in diameter, are noted on the anterior surfaces of the legs.
Labs: WBC 9200
Which of the following is the most appropriate therapy for the skin lesions? Broad spectrum antibiotics
Intensified therapy for UC
NSAIDs
Topical steroid cream
Common Extraintestinal manifestations
of IBD Joints
Peripheral arthritis Ankylosing spondylitis and sacroileitis
Skin Pyoderma gangrenosum Erythema nodosum
Eyes Episcleritis Iritis Uveitis
Hepato-biliary Primary sclerosing cholangitis Gallstones
Other Hypercoagulable state Renal stones Aphthous stomatitis

EIMs of IBD: The Facts
EIMs are most commonly associated with colonic disease, extensive disease and family history1
Although virtually every organ system can be involved the most commonly involved organs are skin, eyes, joints and biliary tract
Studies have reported ranges of 6-40% of patients with IBD have at least one EIM2,3
1-6% of patients have more than one EIM
1Extracolonic diagnosis in UC: an epidemiological study. Monsen AU, Am J Gastroent, 1990; 85(6): 711-6
2The prevalence of EID in IBD: population-based study. Bernstein A, Gastro, 2001: 96(4): 1116-22
3Autoimmune disorders and EIM in 1st degree familial and sporadic IBD: case-controlled study. Ricart A, IBD. 2004: 10(3):
207-14

EIMs of IBD: more Facts
EIMs may precede, parallel, or be independent of
intestinal disease activity
Musculoskeletal diseases are the most common
EIMs found in patients with IBD
Cutaneous disorders associated with IBD occur in
about 15% of patients
Rare extraintestinal manifestations of IBD. Hoffman R, Inflamm Bowel Dis, 2004; 10: 140-147

Skin manifestations of IBD: oral lesions
Aphthous Ulcer

Skin manifestations of IBD
Courtesy of J-F Colombel, MD.
Erythema nodosum

Erythema Nodosum
Prevalence of EN in IBD 10-20%
more common in women
most commonly occurs on extensor surfaces -
usually on shins, but can appear on calves, trunk
and face
usually associated with colonic involvement
commonly associated with disease activity but
not necessarily severity or extent
can rarely precede diagnosis of IBDImportant cutaneous manifestations of IBD. Trost L, Postgrad Med J 2005; 81:580-585
EIMs in IBD. Danese S, World Jl of Gastro 2005; 11 (46): 7227-7236
Erythema Nodosum characterized by sudden onset multiple, red, warm
and painful nodules
systemic symptoms --fever, malaise and especially
peripheral joint involvement-- can occur
self-limiting
typical course lasts 3-6 weeks, but residual bruise-like
lesions (should not scar) and arthralgias can last for
months
resolves with control of IBD and often recurs with
exacerbations

Skin manifestations of IBD
Pyoderma gangrenosum

Pyoderma gangrenosum (PG) PG occurs in 1-10% patients with IBD
more common in UC than CD
most common in young to middle aged adults
more common in women than men
can occur anywhere but most commonly found on
extensor surfaces of lower extremities
Relationship of Extraintestinal involvements in IBD. Das K, Dig Dis Sci; 1999 44(1): 1-13
Important cutaneous manifestations of IBD. Trost L, Postgrad Med J, 2005; 81:580-585
Rare extraintestinal manifestations of IBD. Hoffman R, Inflamm Bowel Dis, 2004; 10: 140-147
EIM of IBD. Kethu, S, J Clinical Gastro, 2006; 40(6): 467-475
Pyoderma gangrenosum (PG) Diagnosis usually made clinically
biopsy of lesions can extend ulcers and lead to poor
wound healing
Need to exclude underlying infectious etiology
approx 50% patients with PG develop large ulcers in
response to minor trauma (pathergy)
surgical trauma i.e. scar or adjacent to ileostomy can
be site of PG1
Relationship of Extraintestinal involvements in IBD. Das K, Dig Dis Sci; 1999 44(1): 1-13
Important cutaneous manifestations of IBD. Trost L, Postgrad Med J, 2005; 81:580-585
Rare extraintestinal manifestations of IBD. Hoffman R, Inflamm Bowel Dis, 2004; 10: 140-147
EIM of IBD. Kethu, S, J Clinical Gastro, 2006; 40(6): 467-475
Pyoderma gangrenosum (PG) can occur before, during, or after onset of IBD
and may or may not parallel disease activity
PG has been reported years after proctocolectomy2
Treatment: usually with systemic steroids (high doses), but sulfa
drugs, CYA, tacrolimus, 6-MP and dapsone have been used
Remicade has been used successfully in refractory PG
preventing secondary infections is crucial
1Relationship of Extraintestinal involvements in IBD. Das K, Dig Dis Sci; 1999, 44(1): 1-13
2PG in IBD. Levitt MD, Br J Surg; 1991, 78(6): 676-78

Skin manifestations of IBD
Sweet’s syndrome
Sweet’s syndrome Described first in 1964; less than 40 cases
associated with IBD in literature
associated with malignancies (leukemias), CTD or post-URI
Four cardinal features
fever
leukocytosis
tender red plaques
histologic findings of neutrophilic infiltrate with leukocytoclasis
Rare extraintestinal manifestations of IBD. Hoffman R, Inflamm Bowel Dis, 2004; 10: 140-147
Sweet’s Syndrome – An EIM in IBD. Digestion, Ytting H, 2005; 72: 195-200
Acute febrile neutrophilic dermatosis

Sweet’s syndrome More common in women (one study cited 86%)1
Cutaneous lesions involve arms, legs,
trunk, hands & face
Associated with
arthralgias/arthritis (>60%)
fever (50-80%)
eye involvement (conjunctivitis or iridocyclitis in 40%)
1Sweet’s syndrome: A clinicopathologic review of 29 cases. Kemmett D, J Am Acad Derm, 1990; 23:503-507
Rare extraintestinal manifestations of IBD. Hoffman R, Inflamm Bowel Dis, 2004; 10: 140-147
Sweet’s Syndrome – An EIM in IBD. Digestion, Ytting H, 2005; 72: 195-200
Sweet’s syndrome Usually parallels IBD disease activity, but there have
been cases where it precedes IBD or occurs later in its course
Treatment based on uncontrolled non-randomized studies
most cases have responded to systemic steroids
in a review of 29 cases, oral prednisone for average of 6 weeks resolved skin lesions
other options for refractory lesions include dapsone, colchicine, potassium iodide, cyclosporine
Sweet’s syndrome: A clinicopathologic review of 29 cases. Kemmett D, J Am Acad Derm, 1990; 23:503-507
Rare extraintestinal manifestations of IBD. Hoffman R, Inflamm Bowel Dis, 2004; 10: 140-147

EIM of IBD: peripheral
arthropathy
Joint complications were seen in 16% UC and 33%
CD patients
Several studies have shown that peripheral arthritis
is more common in extensive UC and colonic CD
Most patients developed the joint complications after
diagnosis of IBD, but in a modest group of patients it
either predated the diagnosis of IBD or was present
at time of diagnosis
Peripheral arthropathies in IBD: articular distribution and natural history. Orchard T, Gut, 1998: 42: 387-391

EIM of IBD: axial involvement Axial involvement varies from asymptomatic
sacroiliitis to inflammatory LBP to ankylosingspondylitis (AS)
Sacroiliitis is hallmark of AS but under-reported due to insidious onset and asymptomatic nature (ranging from 10-52% in various studies)
radiographic evidence present in 20-25% patients
Diagnosis of inflammatory LBP includes presence of pain during night and at rest which improves with movement
Peripheral arthropathies in IBD: articular distribution and natural history. Orchard T, Gut, 1998: 42: 387-391
Review article: joint involvement in IBD. Devos M, Aliment Pharmacol Thera, 2004; 20(4) 36-42
Arthritis or vasculitis as presenting symptoms of CD. Mader R, Rheumatol Int, 2005: 25: 401-405

Ankylosing Spondylitis AS is present in 3-10% IBD patients
Diagnosis of AS made using modified NY criteria (combines clinical parameters with radiological sacroiliitis)
LBP and morning stiffness for >3 mos, improves with exercise
Associated decreased mobility of lumbar spine and limitation in chest expansion and radiological criteria
Sacroiliitis of at least grade 2 bilaterally or grade 3 unilaterally
Review article: joint involvement in IBD. Devos M, Aliment Pharmacol Thera, 2004; 20(4) 36-42

Treatment of IBD-arthropathies NSAIDS or COX-2 inhibitors
Intra-articular/systemic steroids
sulfasalazine (greater benefit with peripheral arthropathy)
mesalamine (two small studies in AS patients showed improvement)
MTX (scarce data , but benefit with peripheral arthropathy)
Infliximab (great success with both GI and joint -axial and peripheral- symptoms in several studies)
PhysiotherapyReview article: joint involvement in IBD. Devos M, Aliment Pharmacol Thera, 2004; 20(4) 36-42
Arthritis or vasculitis as presenting symptoms of CD. Mader R, Rheumatol Int, 2005: 25: 401-405
EIMs of CD. Juillerat P, Digeston, 2005; 71: 31-36

EIM Take home points…. EIMs may precede, parallel, or be independent of
intestinal disease activity
in most cases, erythema nodosum, aphthous
stomatitis, peripheral arthritis and episcleritis parallel
activity of intestinal disease
Most commonly involved organs are joints, skin,
eyes, and biliary tract
EIMs can occur after proctocolectomy in UC patients
so be aware…

















