389
IBS Daily Journal while on the LOW FODMAP diet

IBS Daily Journal
while on the LOW FODMAP diet

SUZANNE PERAZZINICreator of Strands of My Life
© 2015
Copyright
Designed, Edited and Produced by Suzanne PerazziniAll rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or otherwise, without prior consent from the copyright owner and publisher of this book. This book is sold subject to the conditionsthat it will not, by way of trade or otherwise, be resold, hired out or otherwise circulated without the publisher’s prior consent.
IBS Journal

5 HOW TO USE THIS JOURNAL
6 SLEEP
9 EXERCISE
12 RELAXATION
15 BREAKFAST
16 SNACKS
17 LUNCH
18 DINNER
19 MEDICATION
20 SUPPLEMENTS
21 WATER
22 BOWEL MOVEMENTS
23 BRISTOL STOOL CHART
24 THE JOURNAL
Contents

“Courage doesn’t always roar. Some-times courage is the little voice at the end of the day that says I’ll try again
tomorrow.”
― Mary Anne Radmacher
4

The best way to work out what is happening with your digestive system is to record all the relevant information. Record every single thing that goes into your mouth including medication and supplements. Record your bowel movements, what sort they are and when they happen.
On top of that, record how much sleep you get, how much exercise you do and when you use relaxation techniques. These are essential parts of a balanced lifestyle which supports your IBS.
As time passes, this will be an excellent record to look back on to see what progress you have made. But most of all, it will be a way for you to start seeing patterns and work out what is causing your symptoms.
Assuming you are on a strict low Fodmap diet, this will be a fairly easy process because your symptoms will be minimal. However, there could still be some foods that upset you for reasons which are not Fodmap related. O r maybe you will see that too much of something or too many low Fodmap foods together are causing symptoms.
We are all individuals where Fodmaps are concerned, and it is rare for a person to have issues with all the Fodmap groups so you will be able to create your perfect personalized diet over time, especially once you have undertaken the reintroduction stage of the diet.
Make sure you eat five small meals a day spaced between three and five hours apart with your last meal at least three hours before bedtime. This information is repeated on the dedicated meal pages but it is worth remembering to never overeat, not to graze throughout the day and not to fast. All of these situations will cause your IBS symptoms to reappear or worsen. Follow the diet strictly and you will be amazed at how your IBS symptoms will disappear. Record, learn and adjust. Good luck.
How to use this journal
5

Sleep
Sleep is essential for a person’s health and wellbeing, and lack of good quality sleep is a serious problem which affects many people.
WHAT SLEEP DOES FOR YOU A good night’s sleep improves • learning. While alseep, new pathways are formed in your brain.Sleep helps you pay attention, make • decisions, and be creative.Sleep helps you control your • emotions and behaviour, and to cope with change. Sleep deficiency has been linked to depression, suicide, and risk-taking behaviour.Sleep is involved in healing and repair of your heart and blood vessels. Thus • preventing heart disease, strokes etc.Sleep deficiency increases the risk of obesity because sleep helps maintain a • healthy balance of the hormones that make you feel hungry (ghrelin) or full (leptin). When you don’t get enough sleep, your level of ghrelin goes up and your level of leptin goes down. This makes you feel less hungry when you’re well-rested.Sleep affects how your body reacts to insulin, the hormone that controls your • blood glucose (sugar) level. Sleep deficiency results in a higher than normal blood sugar level, which may increase your risk for diabetes.Sleep supports healthy growth and development. Children grow while they are • asleep.Sleep helps build your immune system and fight common infections.•
6
WHAT HAPPENS IF YOU DON’T GET ENOUGH SLEEP? Irritability, moodiness and disinhibition are some of the first signs a person experiences from lack of sleep followed by apathy, slowed speech and flattened emotional responses, impaired memory and an inability to be creative or multitask. Then finally hypnagogic hallucinations are experienced.
HOW MUCH SLEEP DO YOU NEED?
Everyone’s individual sleep needs vary. In general, most healthy adults are built for 16 hours of wakefulness and need an average of eight hours of sleep a night. However, some individuals are able to function without sleepiness or drowsiness after as little as six hours of sleep. Others can’t perform at their peak unless they’ve slept ten hours.
WHAT CAUSES SLEEPING DIFFICULTIES?
Apart from rarer physiological and psychological disorders that may be involved, the following can be causes:
Stress, for example, school- or job-related pressures, a family or marriage • problem or a serious illness or death in the family. Drinking alcohol or beverages containing caffeine in the afternoon or evening.• Exercising close to bedtime. • Following an irregular morning and night-time schedule.• Working or studying right before getting into bed.• The room being too hot or cold, too noisy or too brightly lit. • Interruptions from children or other family members. • The habits of your sleep partner. • Physical problems like arthritis or having pain, backache, or discomfort.• Medications such as decongestants, steroids and some medicines for high • blood pressure, asthma, or depression.
7

YOUR EXERCISE
Let’s suppose you go to bed at 10.30pm and get up at 6.30am.
No caffeine in the form of tea, coffee or cold drinks after 6.30pm• No food or alcohol of any kind after 7.30pm• At 9.30pm stop all heavy mental activity and relax (preferably no electronic devices • at all)In your bedroom, minimize noise, light and excessive hot or cold temperatures• No non-sleep activities in the bedroom like reading, TV etc.• Try and wake up without an alarm clock after a few days of routine (preferably in •
the weekend if you work).
8 HOURS SLEEP A NIGHT
RECORD
Note in your diary pages how much sleep you have and the quality of that sleep, including if you wake up and how long you stay awake before getting back to sleep.
TIP: If you wake in the night and can’t get back to sleep, go through the alphabet naming one or more countries, mountains, flowers, animals etc. Focusing on something apart from your thoughts will help you to go back to sleep.
8

Exercise
HOW EXERCISE CAN IMPROVE YOUR LIFE
Exercise controls your weight by burning • calories. It’s a simple equation - you gain weight when the calories you burn, including those burned during physical activity, are less than the calories you eat or drink.
Exercise combats heart conditions, stroke, type • 2 diabetes, depression, arthritis, high blood pressure, high cholesterol levels and metabolic syndrome (a condition in which you have some combination of too much fat around the waist, high blood pressure, low HDL cholesterol, high triglycerides, or high blood sugar).
Exercise improves mood by stimulating various • brain chemicals that may leave you feeling happier and more relaxed and reduce your risk of depression. Regular physical activity can help keep your thinking, learning, and judgment skills sharp as you age.
Exercise boosts energy and improves your muscle and bone strength by • delivering oxygen and nutrients to your tissues and helping your cardiovascular system work more efficiently. It can slow the loss of bone density that comes with age.
Exercise helps you fall asleep faster and deepens your sleep. Just don’t exercise •
too close to bedtime.
9

WHAT EFFECT DOES EXERCISE HAVE ON IBS?
Exercise increases colonic motility, transit time, and transitive • intestinal gas. Exercise doesn’t seem to affect the symptomatic complaints of bloating, but it does change gas transit, so can help.
During exercise, the bowel typically quiets down because blood • is being pumped to other parts of the body. If you exercise regularly and become more physically fit, the bowel may tend to relax even during non-exercise periods.
Exercise helps tackle the psychological origins of stress by • triggering the release of endorphins (brain chemicals that improve mood and promote a sense of well-being).
WHAT EXERCISE SHOULD I DO?
It is best to minimize impact as this can irritate the internal organs including the small and large intestines. Suggestions are: cycling, walking, swimming, yoga, tai chi, pilates, golf, stretching and activities you enjoy.
Also try to schedule your exercise at least a few hours after a meal. It’s important to listen to your body, and if you are having an attack, it may be wise to ease off until you feel better.
10

RECORD
Note in your diary pages how much exercise you have done and what the exercise was. Also include the intensity of it and how you felt afterwards.
YOUR EXERCISE
MorningStretching and strengthening exercises for 15 minutes.
During the Daya) If you are used to exercising, continue doing so for at least 30 minutes, 5 times a week.b) If you usually don’t exercise or exercise sporadically, start with 15 minutes a day of gentle exercise for 5 days a week and increase gradually until you reach 30 minutes. Choose something like in the list above - cycling, walking, swimming, yoga, tai chi, pilates, golf, stretching.
EveningGentle stretching exercises for 5-10 minutes before bed.
20-30 MINUTES A DAY EXERCISE
TIP: In order for exercise to become a habit, you need to attach it to something else in your life which is already a part of your routine. For example: exercise after you put the washing machine on or after you get back from work.
11

Relaxation
There will always be a degree of stress in your life. That’s where relaxation techniques come into play. They can help counter the build-up of adrenaline which is released when under stress and bring you back to a state of calm. Relaxation physically changes the way your body functions. When your body is relaxed, breathing slows, blood pressure and oxygen consumption decrease.
RELAXING KEEPS YOUR HEART HEALTHYRelaxing lowers your heart rate, blood pressure and respiration rate.
RELAXING IMPROVES YOUR MEMORYShort bursts of stress impair the centres of the brain involved in memory and learning.
RELAXING LIFTS YOUR MOODIn humans, the prolonged presence of the stress hormone cortisol can reduce levels of serotonin and dopamine, which are linked to depression.
RELAXING KEEPS OFF THE WEIGHTCortisol (the stress hormone) increases the appetite. Stress makes it harder to resist comfort foods which are high in fat and sugar.
RELAXING REDUCES THE RISK OF STROKEStudies have shown that people who coped with stress the best had a lower risk of
strokes.
12

RELAXATION TECHNIQUES
Guided Imagery
This is a technique which uses guided imagery, creating mental images.Ocean Retreat Trip to the Beach
Progressive Muscle Relaxation
This involves tensing one muscle group at a time and then relaxing it until you have covered all the muscles in the body. This is great for tense, tight muscles.Head to ToeToe to Head
Deep Breathing
This forces you to breathe more deeply, rather than with the short, shallow breaths that stress creates.Deep breathing
13

YOUR EXERCISE
Schedule a time every day for 10 minutes (lengthen the time gradually). Be 1.
consistent, you will see results in a couple of weeks.
Find a quiet place without distractions or noise. If needed use earplugs to block 2.
sound and an eye pillow to block light.
Loosen or remove any jewellery or clothing that could distract you.3.
Sit or lie down (don’t lie down if this tends to send you to sleep) in a comfortable 4.
position.
Choose one of the three techniques above, click on the link and run the tape and 5.
let your body relax and empty your mind. Don’t try too hard though – it will come
with time.
10+ MINS A DAY RELAXATION
RECORD
Note in your diary pages how long you relax for and which exercise you used. Also indicate how you felt afterwards. You could even record when you have needed to use this technique during the day and how effective it was. You should see this become easier as time passes.
TIP: Place this in your schedule as a non-negotiable appointment. Get up 10 minutes early and do your relaxation exercise before your day starts.
14
Breakfast
You should consume your breakfast as soon as you get up or perhaps after a shower. Breakfast, as it says in the word, breaks the fast. And it’s important with IBS to do that as soon as possible. Our digestive systems hate to feel starved and react with symptoms as if we have eaten something high Fodmap. The food arriving into the digestive system will also activate the urge to have a bowel movement, and it is great to get that out of the way before the day fully starts.
WHAT SHALL I EAT?A good choice is a wheat/barley/rye-free cereal like oatmeal [1/4 cup when raw], cornflakes [3/4 cup], rice flakes [3/4 cup] etc., a low Fodmap fruit and lactose-free milk. Weak tea or coffee is optional. If you need more protein that the milk will provide, have an egg prepared how you prefer. If you are on the constipated side of IBS, I suggest oats and a kiwifruit, which has a mild laxative effect.
RECORDTake note in your diary pages, what you eat, how much and when you eat it. Also note how you feel after eating the meal.
TIP: Check the ingredients of any cereal you choose and make sure you recognize all the ingredients as low Fodmap.
15

TIP: The best combination is to have a protein, a carbohydrate and a fruit or vegetable sticks so that you don’t get hungry.
Snacks
You need to have two snacks a day in between your main meals and you need to keep all meals small since our digestive systems don’t like large amounts of food arriving at the same time. Make sure you have the first snack 3-5 hours after your breakfast and keep that same spacing for your meals throughout the day, making sure that your dinner is at least three hours before bedtime. If you get up late, still have your breakfast straightaway and perhaps skip the morning snack if it would be too close to lunchtime. But distribute any important food from the snack into your other meals so you are not eating less.
WHAT SHALL I EAT?Homemade baking, as long as not too starchy would be suitable. But some good alternatives are a few of the following - low Fodmap fruit (2-3 pieces a day), low Fodmap vegetable sticks, cottage cheese, hard cheese, peanut butter, tahini, canned fish, gluten-free crackers, lactose-free yogurt.
RECORDTake note in your diary pages, what you eat, how much and when you eat it. Also note how you feel after eating the meal.
16

Lunch
Lunch is your third meal of the day and should be 3-5 hours after your morning snack. Make sure you stop work or whatever you are doing and take a complete break so you can focus on eating your food. Any kind of stress or tension will affect how the food is received and therefore will determine whether you get symptoms or not. After eating, don’t get up straightaway and start anything physical or stressful. Wait until the food has had time to arrive and the digestive process is well under way. Any stenuous exercise or work should be delayed for an hour or two.
TIP: Before you eat your dinner, put aside your lunch so that it doesn’t get eaten.
WHAT SHALL I EAT?Eating leftover dinner is the easiest way to take care of lunch whether you are eating at home or at work. Most work places have microwaves so you can heat it up. If there are no leftovers or if they are not suitable, a gluten-free sandwich with fresh sliced meat
and low Fodmap salad vegetables would be a good alternative.
RECORDTake note in your diary pages, what you eat, how much and when you eat it. Also note how you feel after eating the meal.
17

Dinner
Eat you dinner 3-5 hours after your afternoon snack and at least three hours before bed. When planning your dinner, make sure it has protein, carbohydrate and vegetables. Carbohydrate gives you instant energy which doesn’t last long while the energy from protein takes a little longer to kick in but lasts longer. Combining the two at all five meals is
ideal for keeping away hunger, which is your enemy. Eat in a calm situation and don’t allow any heavy discussions with family during meals. You can schedule a family meeting for such matters. Keeping your digestive system happy is your first priority.
WHAT SHALL I EAT?This will depend on your preferences and whether you follow a particular eating regime like vegetarianism. However, as above, make sure you balance your meal well with all food groups while staying low Fodmap. This is the largest meal of the day in many cultures, but you have to cut back on what you would usually eat because now your food is being distributed between five meals instead of the traditional three.
RECORDTake note in your diary pages, what you eat, how much and when you eat it. Also note how you feel after eating the meal.
TIP: Vary your proteins between red meat, chicken, fish, tofu etc. throughout the week.
18

Medication
Those on the low Fodmap diet sometimes forget that everything that is swallowed affects your gut, and that includes medication.Some medication like insulin for diabetics or high blood pressure pills are lifesaving and can’t be stopped. But that medication may contain high Fodmap inactive ingredients so do have a chat with your doctor and ask about all the ingredients in the medicine you are taking and not just the active ones. It can be possible to make a change if it is found that a certain medication is increasing your gastrointestinal problems.Many with IBS are on anti-depressant or anti-anxiety medication because they haven’t been absorbing tryptophan, which plays a part in regulating a person’s moods. This situation will gradually change as you start to actually absorb the nutrients in your food for the first time in ages. And so those medicines can be reduced under the careful supervision of your doctor – because many of them are habit-forming and the withdrawal from them has to be done with care.Many medicines have common side effects that affect the gut and so it’s almost impossible to know if it is food or pills that are causing symptoms. This is a very tricky situation and has to be handled with care.
TIP: Having a doctor who fully understands your personal situation and understands the concepts of the low Fodmap diet will go a long way to helping you resolve these problems together. If your doctor is uncooperative and doesn’t listen to your concerns, change doctor.
19
Supplements
Many people with IBS are taking a whole raft of supplements in an attempt to get better. And that is very understandable. But most of them will be unnecessary once you are eating a diet which is healthy for you because you will finally be absorbing all the nutrients in your food.
Some supplements contain high Fodmaps, and it takes some work to find the very best supplements which won’t hurt your gut. Regard every single thing that goes down into your gut with suspicion and do your research into them all. Google the ingredients and side effects of these things, become informed about what you are consuming and talk to your doctor or chemist about any doubts you have.
RECORDRecord on your diary pages all the supplements you are taking. If you are still having symptoms on a strict low Fodmap diet, then you have to start looking at your supplements.
TIP: Look for an ingredient ending in “ol” - it could be one of the Fodmap groups, a Polyol.
20

Water
Water is needed by every sytem in our body and makes up 60% of our body weight. Even mild dehydration will make us listless and tired.
HOW MUCH WATER DO YOU NEED?That depends on a variety of things:
How much exercise you do. A serious athlete will • require considerably more fluid than someone who walks for 20 minutes a day.
Location is important. Hot temperatures cause • loss of fluids through perspiration. Even heated interiors dry out your skin. Higher altitudes also cause a greater loss of hydration through increased respiration and urination.
Some illnesses like a bladder infection or a tummy • bug with diarrhea cause dehydration.
On average a man requires 3 litres and a woman needs 2.2 litres of fluid a day. Making sure that your urine is light yellow is a good test.
RECORDMake note of how many glasses you drink in a day and when you drank them.
TIP: Drink a glass of water with each of your 5 meals and a glass in between each meal.
21

Bowel Movements
During the elimination and reintroduction stages of the diet, it is important to monitor your bowel movements carefully and make adjustments to your diet according to your stools that day. On the next page you will see the Bristol Stool Chart. This is the generally accepted measure of a person’s stools. Our aim is to have a number 3 or 4 stool on a regular basis. This means that we are neither constipated nor have diarrhea. The average person has one to three bowel movements a day. But some people have one every two days or four movements a day. You have to find what is right for you. Create a routine that your body comes to recognize but the very best time to go is staright after breakfast before starting your day. If you need a second visit, make it just before bedtime so that you can have a good settled night’s sleep. A third time, if necessary, could be straight after lunch.
RECORDRecord any bowel movement you have during the day with the time and the type.
TIP: Don’t ignore an urge to visit the toilet especially if you are constipated. That can make the condition worse.
22

Bristol Stool Chart
Type 1 Separate hard lumps, like nuts - hard to pass
Type 2 Sausage-shaped but lumpy
Type 3 Like a sausage but with cracks on the surface
Type 4 Like a sausage or snake, smooth and soft
Type 5 Soft blobs with clear-cut edges
Type 6 Fluffy pieces with ragged edges, a mushy stool
Type 7 Watery, no solid pieces. Entirely liquid
23

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Personal Challenge Tell someone close to you that you love them
Date: ___/___/___
24
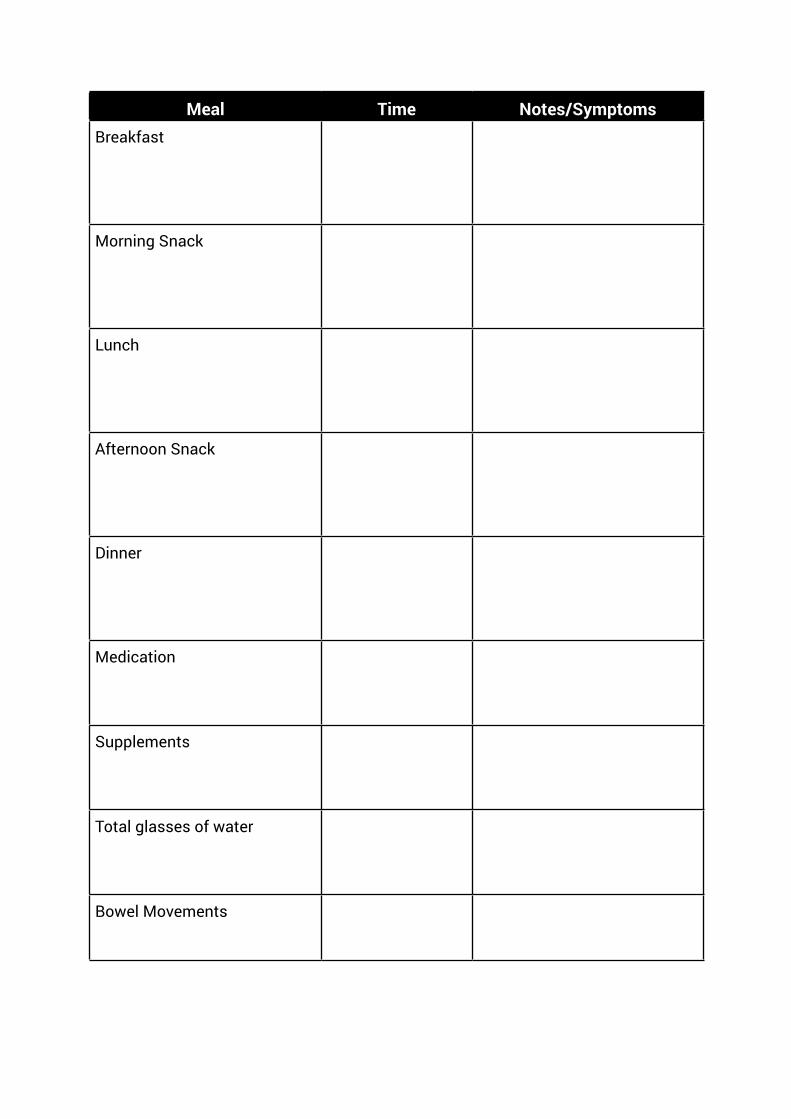
Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements
Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Quote “Don’t compare your beginning to someone else’s
middle.”
Jon Acuff

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Gratitude AffirmationI gratefully accept all the good that manifests in
my life.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Health TipBananas are rich in potassium which can be good
for keeping your blood pressure healthy.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Personal Challenge Smile at 3 strangers today

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements
Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Quote “We have to live life with a sense of urgency so
not a minute is wasted.”
Les Brown

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Gratitude AffirmationMy gratitude is sincere and constant.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Health TipA red pepper has nine times more vitamin C than a
green one.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Personal Challenge Don’t complain for an entire day

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Quote“Don’t fear death, fear the un-lived life.”
Natalie Babbitt
Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Gratitude AffirmationThere are more blessings in my life than I can count.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Health TipStretching when you wake up boosts circulation and
digestion.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Personal Challenge Carve your name on a tree in your garden.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements
Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Quote“Live as big as you can, with what you’ve got.”
Jill Shalvis

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Gratitude AffirmationWith every breath I take, I am bringing more and
more gratitude into my life.
Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Health Tip Peppermint tea improves the flow of bile which
moves food through the gut more quickly

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Personal Challenge Sing in the shower at the top of your voice

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Quote “Be determined enough to live for your dreams.”
Lailah Gifty Akita
Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Gratitude AffirmationI am grateful for all my material possessions

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Health TipNever skip breakfast. An IBS gut hates fasting
through the day.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Personal Challenge Do something you used to love doing when you
were a small child

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Quote“Live with passion. Live with enthusiasm.
Live your best life.”
Lailah Gifty Akita
Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Gratitude AffirmationI find it easy to maintain an attitude of gratitude
even in difficult situations

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Health TipPlace ice cubes in your glass before pouring in dry wine. That way you can have two glasses
instead of one.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Personal Challenge Do something that scares you

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Quote“A heart can no more be forced to love than a
stomach can be forced to digest food by persuasion.”
Alfred Nobel

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Gratitude AffirmationI am so grateful for every person and every thing in
my life.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Health Tip20 minutes of sunshine covers your daily vitamin D needs or eat plenty of fatty fish, eggs, beef liver
and cheese

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Personal Challenge Show someone how much you love them.
Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Quote“We must live life and treasure every moment on
Earth.”
Lailah Gifty Akita

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Gratitude AffirmationMy life is singular, unique and wondrous. For this I
am profoundly thankful.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Health TipRev up your metabolism by alternating your speed
and intensity during aerobic workouts.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements
Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Personal Challenge Brush your teeth with your non-dominant hand.
This is excellent for exercising the brain.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements
Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Quote“Celebrate your life, this is your only life.”
Lailah Gifty Akita

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Gratitude AffirmationMy thoughts are focused on positivity and
thankfulness
Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements
Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Health TipLaughter boosts the immune system and helps
the body shake off allergic reactions. It heals bodies as well as broken hearts.
Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements
Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Personal Challenge Hold the door open for two people today

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Quote“Worry is the stomach’s worst poison.”
Alfred Nobel

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Gratitude AffirmationI am grateful for my family

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Health TipCalm a queasy stomach by pressing down on the
groove between the tendons that run from the base of your palm to your wrist.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Personal Challenge Don’t lie for a week.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Quote“Sometimes there is a 36-piece orchestra going off
in my stomach.”
Willie Nelson

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements
Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Gratitude AffirmationI am grateful for the sun as it warms my skin and
brightens my life.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Health TipBlueberries contain high quantities of resveratrol
– an antioxidant compound found in red wine that is believed to help protect against heart disease
and cancer.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements
Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Personal Challenge Say yes to everything today.
Within reason.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Quote“If your stomach disputes you, lie down and pacify
it with cool thoughts.”
Satchel Paige

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Gratitude AffirmationI am grateful for the rain because it makes the
plants that feed us grow.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Health TipFolic acid can help with cancer prevention. It is found in green leafy vegetables, liver and fruit.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements
Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Personal Challenge Let someone else be right today.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Quote“When I repress my emotion my stomach
keeps score.”
Enoch Powell

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Gratitude AffirmationAt the close of every day, I count my blessings and
give thanks for all that I have.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Health TipGet out of the bus a stop early and walk the extra
distance to work each day.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements
Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Personal Challenge Give a stranger a compliment.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Quote“If you slow it down, eat in courses, your body,
mind, stomach will catch up with this full feeling and you won’t eat as much.”
Guy Fieri
Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Gratitude AffirmationI am eternally grateful for all the pleasure my
senses bring me.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Health TipIf you are sure you don’t have SIBO, take a
probiotic, preferably lactobacillus pantarium 299v and bifidobacterium align longum.
Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Personal Challenge Go to bed at the same time each night for two
weeks.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Quote“All the food that is put into the stomach that the system cannot derive benefit from, is a burden to
nature in her work.”
Ellen G. White

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Gratitude AffirmationI am deeply grateful for each experience life
brings me.
Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements
Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Health TipTo make sure that you don’t eat too much at a meal, choose a smaller plate and don’t refill it.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Personal Challenge Start a conversation with a stranger today.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Quote“Peace in the head, peace in the stomach.”
Jean-Bertrand Aristide

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Gratitude AffirmationI accept all gifts graciously and with
deep gratitude.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Health TipHot, spicy foods containing chillies or cayenne
pepper trigger endorphins, the feel-good hormones. However, don’t overdo it. Your gut may
be sensitive to spicy food.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Personal Challenge Leave your cell phone at home today.
Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Quote“To change one’s life: Start immediately. Do it
flamboyantly. No exceptions.”
William James

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Gratitude AffirmationMy needs and desires are generously met.
For this I am thankful.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Health TipMake sure you get the equivalent of 2 glasses of milk a day to get enough calcium. You will also
need Vitamin D and magnesium to make sure it is absorbed.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Personal Challenge Go for a walk in the park or on the beach alone.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Quote“Be happy for this moment. This moment is your
life.”
Omar Khayyam

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Gratitude AffirmationMy mind is always effortlessly focused on
positivity and thankfulness

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Health TipYour favourite drink has to be water. It contains no
Fodmaps unlike almost every other drink.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Personal Challenge Focus on a single task at a time, without
multi-tasking.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Quote“Don’t compromise yourself. You are all you got.”
Janis Joplin

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements
Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Gratitude AffirmationI am grateful for the soft bed I sleep in each night.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Health TipAvoid processed foods. Check all labels and if you don’t recognize all ingredients as food, put it back on the shelf. Eat as close to the source of the food
as possible.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Personal Challenge Buy a small gift for yourself.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Quote“Good health and good sense are two of life’s
greatest blessings.”
Publilius Syrus

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Gratitude AffirmationGratitude brings me into a harmonious relation-
ship with the good in everyone that surrounds me.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Health TipEat fatty fish like salmon and sardines at least once a week to get a good hit of omega-3 fatty
acids. But don’t eat too much at once because fat is a gut irritant if you consume too much.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Personal Challenge Write all your bad memories on paper, burn this
paper afterwards. Let go.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Quote“To enjoy the glow of good health, you
must exercise.”
Gene Tunney

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Gratitude AffirmationEvery day I say Thank You for what I want
to see more of in my life..

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Health TipBalance looking after others with some self-love or you will get run down and burnt out. That kind of neglect will have a negative effect on your gut.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements
Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Personal Challenge Avoid elevators and escalators. Take the
stairs instead.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Quote“Happiness is nothing more than good health and a
bad memory.”
Albert Schweitzer

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Gratitude AffirmationI am grateful for all the teachers in my life.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Health TipTomatoes contain lycopene, a powerful cancer fighter. They’re also rich in vitamin C. Cooked tomatoes are also nutritious, so use them in
pasta, soups and casseroles, as well as in salads.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements
Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Personal Challenge Get something you have been struggling with for a
while off your chest. Talk to someone you trust.
Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Quote“As for butter versus margarine, I trust cows more
than chemists.”
Joan Gussow

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Gratitude AffirmationI am grateful for every moment that I
spend in silence.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Health TipMindful living - by slowing down and
concentrating on basic things, you’ll clear your mind of everything that worries you.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Personal Challenge Go see a family member you have been
meaning to see

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Quote“A fit, healthy body-- that is the best
fashion statement.”
Jess C. Scott

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements
Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Gratitude AffirmationI appreciate everything I have and I show my
sincerest gratitude to my loved ones.
Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Health TipDo your weights workout before your cardio.
The cardio increases blood flow to the muscles, flushing out lactic acid, which builds up in the
muscles while you’re weight training.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Personal Challenge Smile at yourself in the mirror for at least
10 seconds.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements
Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Quote“Success is getting what you want, happiness is
wanting what you get.”
W.P. Kinsella

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Gratitude AffirmationI clearly see the beauty of life that flourishes
around me.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Health TipIBS is connected to hormonal fluctuations so women will feel their cycles more acutely than
someone without IBS.
Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Personal Challenge Pick up a piece of litter and place it in a bin. If we
all did that every day, our streets would be much cleaner.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements
Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Quote“It’s not who you are that holds you back, it’s who
you think you’re not.”
Unknown

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Gratitude AffirmationMy thoughts are focused on positivity
and thankfulness

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Health TipMake sure you get enough vitamin C to keep your immune system strong. Eat citrus fruits, kiwifruit ,
tomatoes, papaya and red peppers.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Personal Challenge Don’t say anything negative today. Focus on
the positive.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Quote“Motivation will almost always beat mere talent.”
Norman R. Augustine
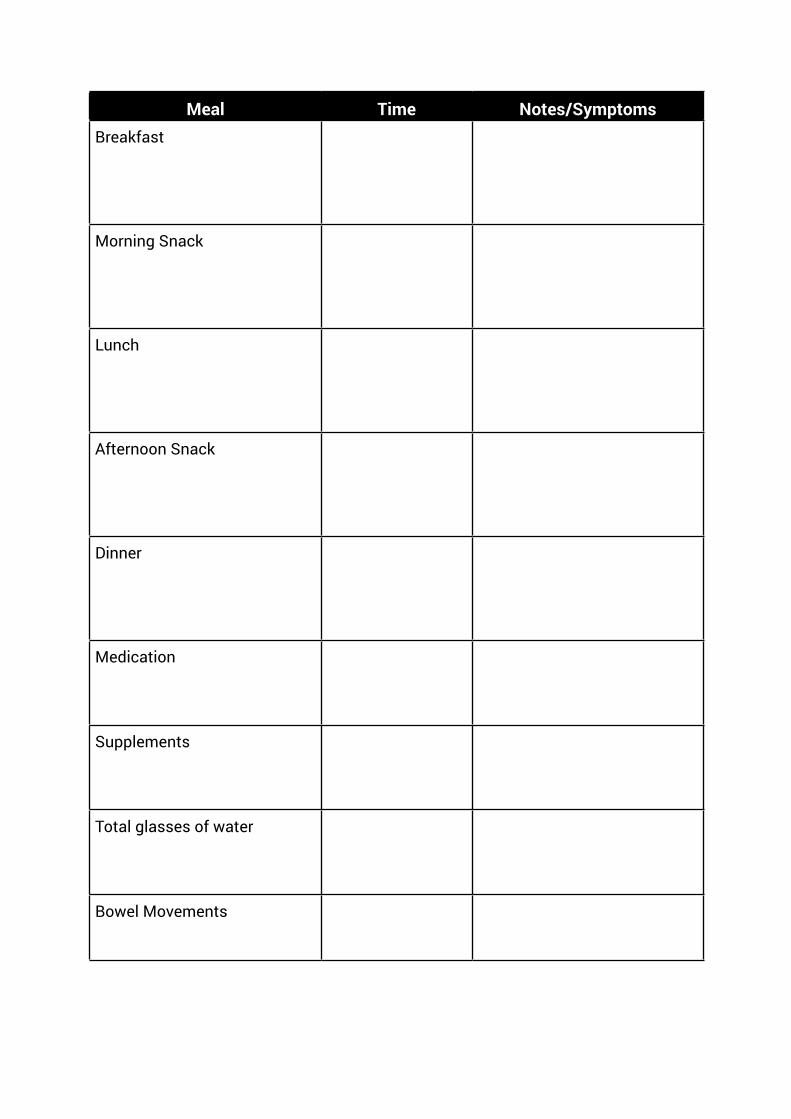
Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements
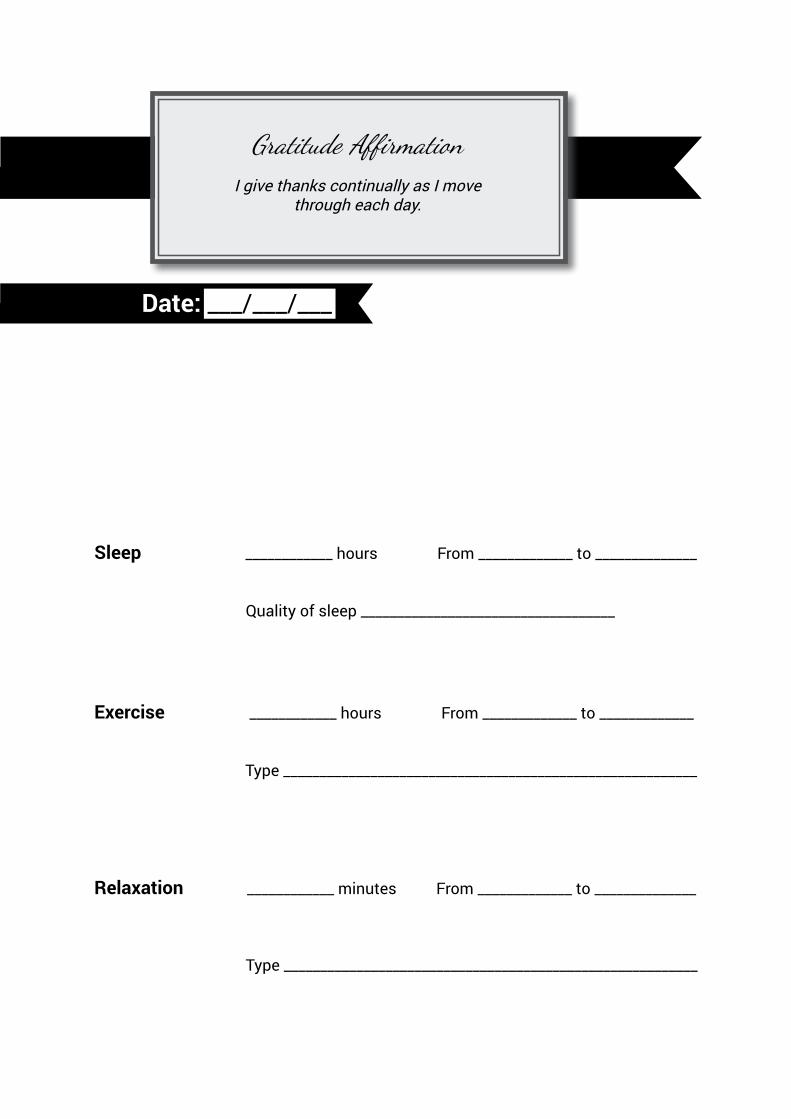
Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Gratitude AffirmationI give thanks continually as I move
through each day.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Health TipHunger is the enemy of someone with IBS so
always keep low Fodmap snacks on hand in case you get held up somewhere without low Fodmap
food when your next meal time arrives.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements
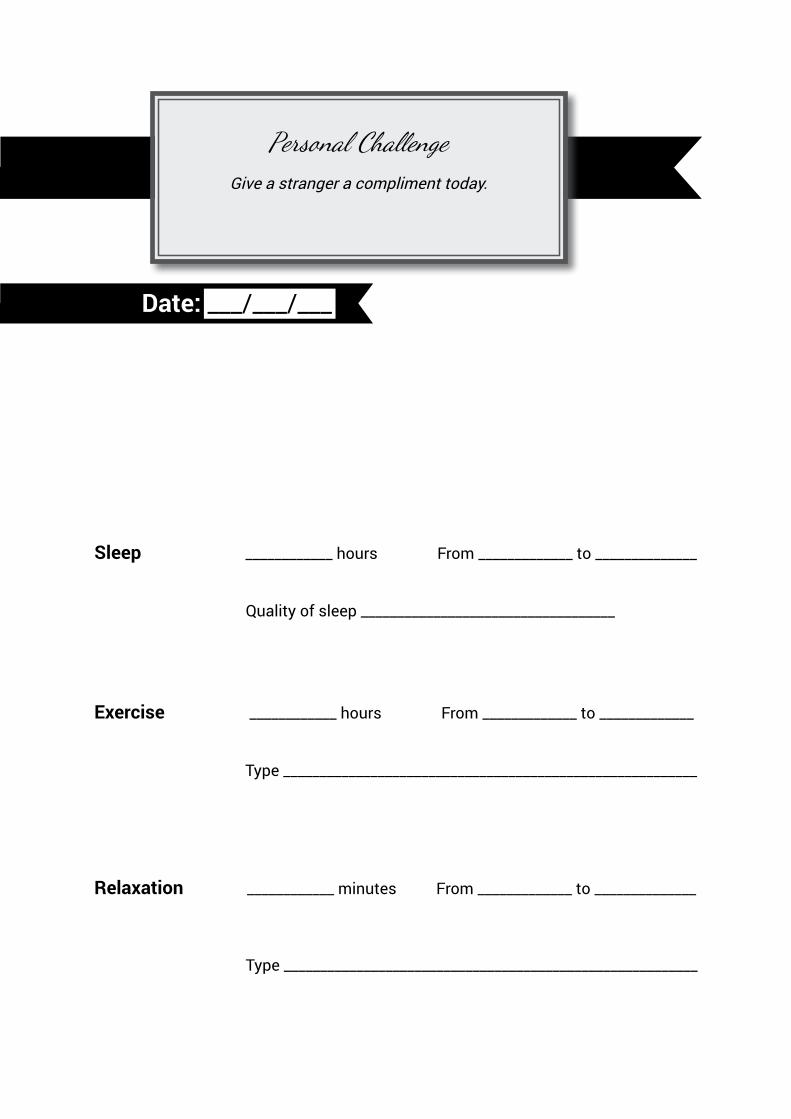
Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Personal Challenge Give a stranger a compliment today.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Quote“Winners make it happen, losers let it happen.”
Unknown

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Gratitude AffirmationAn attitude of gratitude is the key to manifesting a
better life for myself.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Health TipIf you have reflux, avoid tomatoes, citrus fruits, spicy food, oily food, caffeine, mint and alcohol.
Also don’t lie down after eating, and eat at least 3 hours before bed.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Personal Challenge Spend a few minutes deleting unnecessary
contacts from your phone.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Quote“A goal is a dream with a deadline.”
Unknown

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Gratitude AffirmationI am grateful for my house which shelters me from
the elements.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Health TipDon’t take digestive enzymes if you have IBS.
Most of them contain high Fodmap ingredients and/or substances which have not yet been
tested for their Fodmap content.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Personal Challenge Take a walk today and find one object for each
letter of the alphabet, from A to Z.
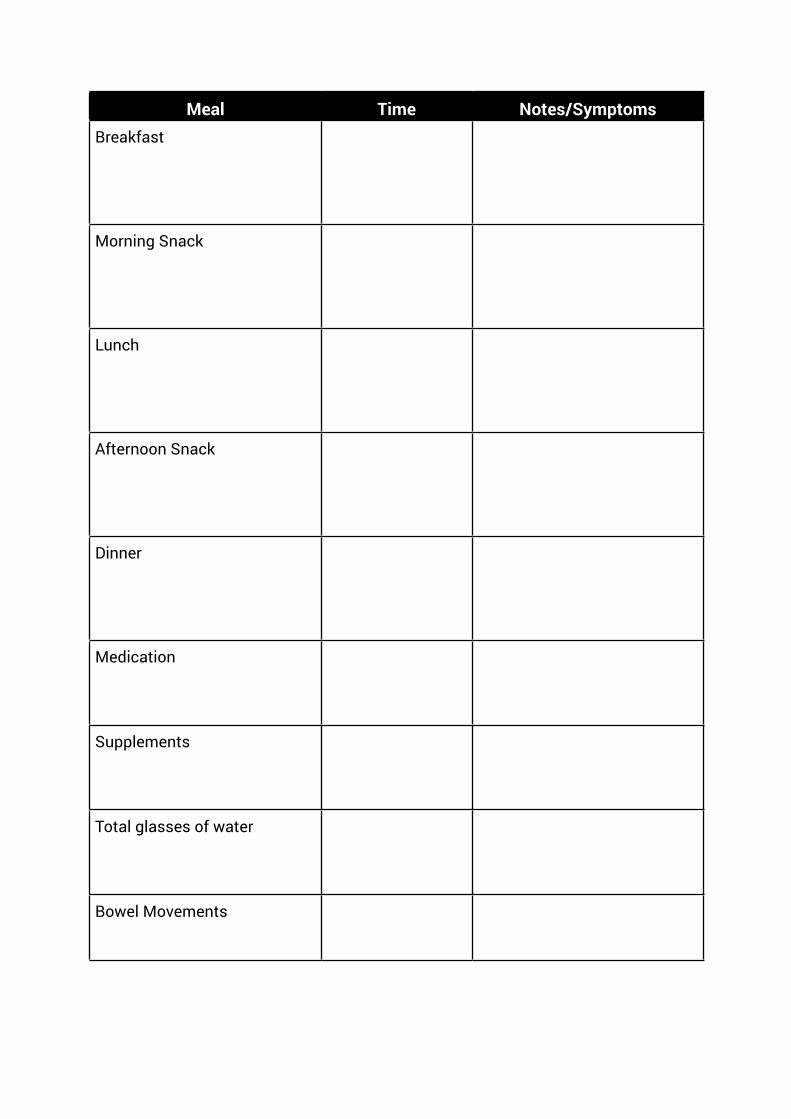
Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Quote“Don’t suffer from insanity, enjoy every
minute of it.”
Unknown

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements
Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Gratitude AffirmationI am forever grateful for being able to contribute to
the lives of others.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements
Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Health TipFor constipation, drink 8 glasses of water and
exercise daily. Also make sure you have an adequate intake of fibre and fats/oil.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Personal Challenge Create your own dance for your happy moments.
Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Quote“If you obey all the rules you miss all the fun.”
Katherine Hepburn

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements
Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Gratitude AffirmationI am grateful for being able to hear my intuition.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements
Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Health TipYou can only have 5gms of fructose a day so
make sure the major part of that is in the form of fruit and vegetables and not added sugar.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Personal Challenge Find out your blood type.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Quote“The greatest wealth is health.”
Virgil

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Gratitude AffirmationI am grateful for my wonderful life.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Health TipBe aware of how many Fodmaps you are
consuming during the day and don’t eat too many in any one meal or you could get symptoms.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements
Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Personal Challenge Take some time to watch the sunset or sunrise.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements
Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Quote“Eat right, exercise regularly, die anyway.”
Unknown

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements
Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Gratitude AffirmationI am truly grateful for the support I receive from
my family and friends.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Health TipAdd spices and herbs to your meals to create
tasty food that doesn’t make you feel deprived.
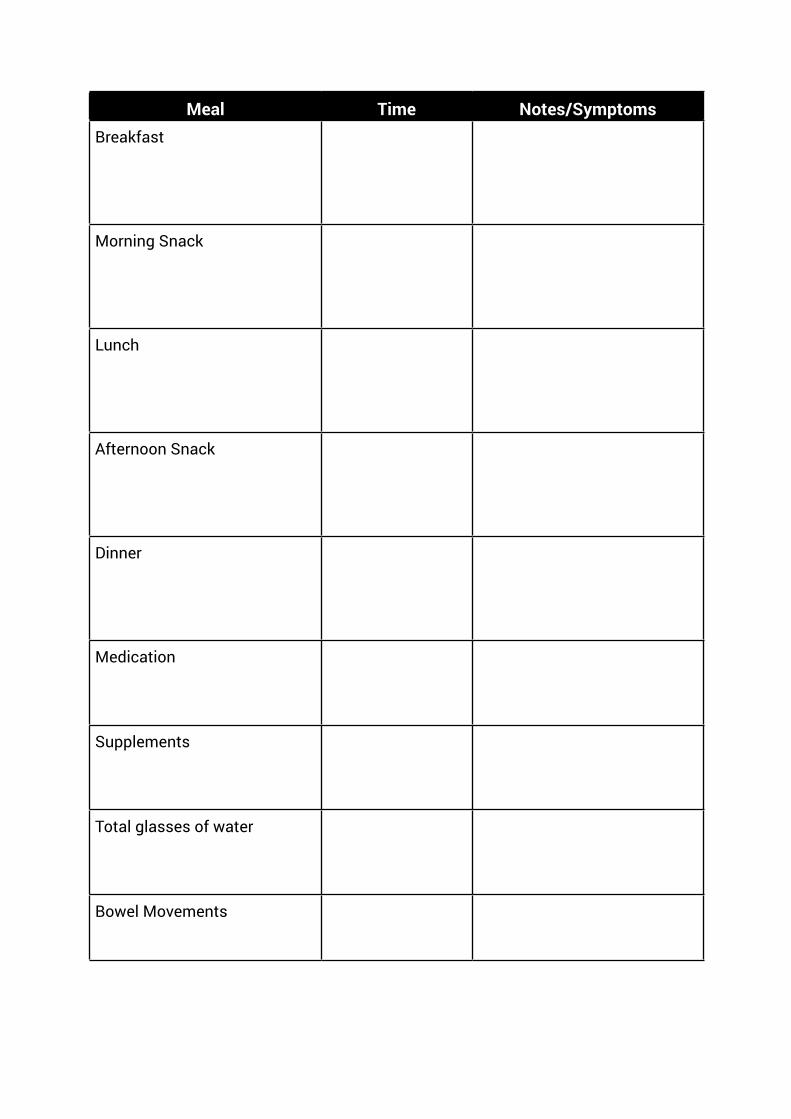
Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Personal Challenge Buy your mum or sister flowers.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements
Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Quote“In order to change we must be sick and tired of
being sick and tired.”
Unknown

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Gratitude AffirmationI cherish each and every moment in my life.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Health TipMake sure that your weight stays stable while on
the elimination diet because your body already has enough to deal with without the strain of
weight loss or gain.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements
Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Personal Challenge Change your name for the day.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Quote“A sad soul can kill you quicker than a germ.”
John Steinbeck

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Gratitude AffirmationThankfulness keeps me connected to universal
abundance.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Health TipWhen you start the elimination diet, if you have
been used to a certain amount of sugar and caffeine, you could have withdrawal headaches.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Personal Challenge Write down at least 10 things you’re grateful for
and hang the sheet of paper in your room.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Quote“He who takes medicine and neglects to diet
wastes the skill of his doctors.”
Chinese Proverb

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Gratitude AffirmationAt the end of each day, I take a moment to
reflect and be grateful.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Health TipMake sure you get enough fibre on the low
Fodmap diet but not too much because fibre is a gut irritant. Good sources are quinoa, oats, brown
rice, oat and rice bran, fruit and vegetables.
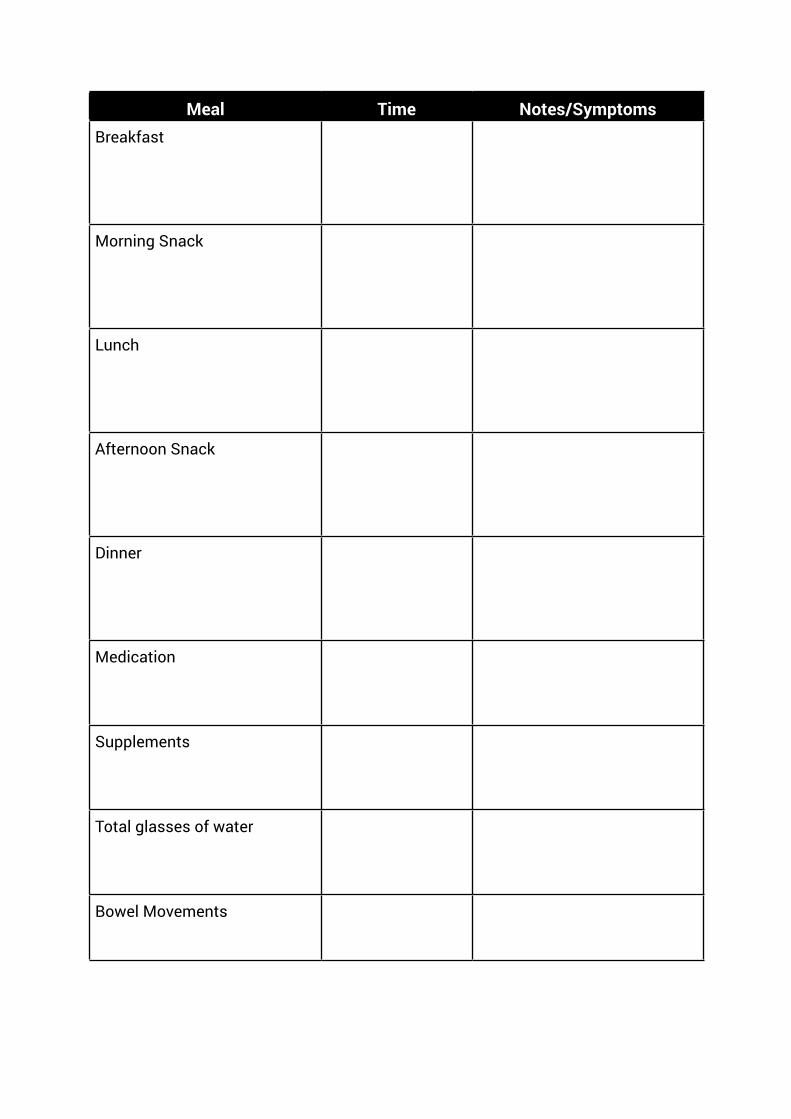
Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Personal Challenge Do something impulsive.
Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Quote“Be careful about reading health books. You may
die of a misprint.”
Mark Twain

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Gratitude AffirmationEvery day I thank the universe for showing me the
way to my dreams.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Health TipA adequate iron intake is important and your needs can be met by all meats, especially red meat, shellfish and sardines. Tofu also has a
decent amount of iron as do iron-enriched cereals.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements
Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Personal Challenge Actively listen to someone’s concerns
and problems.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Quote“Diseases of the soul are more dangerous and
more numerous than those of the body.”
Cicero

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Gratitude AffirmationI am so grateful to be alive and well.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Health TipEat as many different coloured fruits and
vegetables as possible in order to get a wide variety of nutrients.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Personal Challenge Make plans to visit someone who does not live
close to you.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements
Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Quote“A good laugh and a long sleep are the best cures
in the doctor’s book.“
Irish Proverb

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Gratitude AffirmationI am thankful for the trees that provide the planet
with oxygen.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements
Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Health TipThe best milk for the low Fodmap diet is either
oat, rice or lactose-free. Soya milk must be made from the protein of the bean to be acceptable.
Avoid almond milk until it has been tested.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Personal Challenge Loan or buy someone your favourite book.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Quote“Fresh air impoverishes the doctor.“
Danish Proverb

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Gratitude AffirmationI am thankful for every spark of insight
that inspires me.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Health TipInstead of onion, use the green part of spring onions or leeks. Instead of garlic, use garlic-
infused oil. The Fodmaps in garlic and onion are not soluble in oil but they are soluble in liquids.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Personal Challenge Make someone laugh today.
Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Quote“My own prescription for health is less paperwork
and more running barefoot through the grass.”
Terri Guillemets

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Gratitude AffirmationI have a wonderful life and for that I give my
unending gratitude.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Health TipIf you have trapped gas, try some appropriate
yoga poses or other gentle exercise like walking to relax the muscles. You can also use heat in the
form of a warm bath or a heat pack.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Personal Challenge Get someone you love a small gift.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Quote“In a disordered mind, as in a disordered body,
soundness of health is impossible.”
Cicero

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Gratitude AffirmationI take the time to appreciate the simple
things in life.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Health TipIf you do go off track on the diet and symptoms
return, get straight back on the diet and expect the upset to last for up to two days. Don’t give up at
this stage but hang tough.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Personal Challenge Watch your favourite movie.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements
Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Quote“Gold that buys health can never be ill spent.”
Thomas Dekker, Westward Ho, 1604

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Gratitude AffirmationEach Morning I give thanks for another day of life.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Health TipCaffeine is a gut irritant and should be avoided as much as possible though weak tea or coffee once or twice a day should be acceptable, depending on
your individual tolerance.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Personal Challenge Do the thing you would do if it were your
last day on earth.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Quote“Natural forces within us are the true healers of
disease.”
Hippocrates
Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Gratitude AffirmationBeing grateful for what I have brings more
abundance into my life.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements
Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Health TipIf your IBS symptoms don’t go away on a strict
low Fodmap diet, it is possible that you have SIBO (small intestinal bacterial overgrowth) and you will
need antibiotics to rectify that.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Personal Challenge This evening when you get home, keep only one
light on in your house at a time.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements
Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Quote“To avoid sickness eat less; to prolong life
worry less.”
Chu Hui Weng

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Gratitude AffirmationI am eternally grateful for my mind which can
solve problems.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements
Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Health TipAvoid carbonated drinks since carbonation is
a gut irritant. Smoothies are also questionable since they have air pumped into them during the
making.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Personal Challenge Do something your future self will thank you for,
like starting a savings plan.
Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements
Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Quote“If I’d known I was going to live so long, I’d have
taken better care of myself.“
Leon Eldred
Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

Sleep ____________ hours From _____________ to ______________
Quality of sleep ___________________________________
Exercise ____________ hours From _____________ to _____________
Type _________________________________________________________
Relaxation ____________ minutes From _____________ to ______________
Type _________________________________________________________
Date: ___/___/___
Gratitude AffirmationI am forever grateful for the miraculous life
energy in my body.

Meal Time Notes/SymptomsBreakfast
Morning Snack
Lunch
Afternoon Snack
Dinner
Medication
Supplements
Total glasses of water
Bowel Movements

















