37
1 ICT BUSINESS PLAN 2015-2017 A two year plan for IM&T in the Southern Health & Social Care Trust Performance & Reform January 2016

1
ICT BUSINESS PLAN 2015-2017 A two year plan for IM&T in the Southern Health &
Social Care Trust
Performance & Reform January 2016

2
INDEX
1.0 Statement of Purpose Page 3
2.0 ICT Governance Arrangements Page 4
3.0 Meeting the Quality Agenda Page 6
4.0 Resources Page 8
5.0 Summary of 2014/15 ICT Delivery Page 9
6.0 Expenditure 2014/15 Page 16
7.0 Regional E-Health Programme Page 17
8.0 Plans for 2015/16 & 2016/17 Page 19
9.0 Conclusion Page 36

3
1.0 STATEMENT OF PURPOSE
The Southern Health and Social Care Trust employs over 13,000 staff, providing
services for more than 350,000 people across its region, as well as to the whole
of Northern Ireland.
The purpose and vision of the Southern Trust is to deliver safe, high quality health
and social care in a way that respects the needs, individuality and dignity of the
people who use its services. This purpose and vision is underpinned by the
following strategic priorities:
A. To provide safe, high quality care;
B. To maximise independence and choice;
C. To improve health and well-being;
D. To be a great place to work;
E. To make best use of its resources; and
F. To be a good social partner.
ICT plays a pivotal part in achieving these objectives by enabling growth, success
and delivery of service developments through robust technology provision. This
plan recognises that ICT could be used extensively to enable, support and
sustain change and drive efficiency. In this context, it will also help support a
culture of openness, transparency and comparability of information. The Trust is
committed to harnessing information and new technologies to achieve higher
quality care and improve outcomes for patients and service users. Informatics
objectives are as follows:
i. Provide and add value to the Trust business in a strategic and planned way;
ii. Make a real contribution to achieving the Trust objectives above;
iii. Deliver what we say, when we say we will and deliver it right first time; and
iv. Ensure services delivered are value for money.
v. Have secure, timely, resilient and accurate information at the point of care.
These objectives will be monitored through the following performance measures:

4
Financial stability – providing services within budget;
Customer satisfaction;
Monthly monitoring of key performance indicators;
Project plans delivered on time and in budget;
Benchmarking performance with other Trusts; and
Well trained, competent and valued staff.
The purpose of this Business Plan is to identify the IT priorities for investment and
delivery in the financial years 2015/16 and 2016/17 and to agree and
communicate these with key stakeholders including Trust staff, HSC Board, BSO
and 3rd party suppliers This plan has therefore been developed in response to
local E-Health & Care Strategies and is aligned to the Trust TDP.
2.0 ICT GOVERNANCE ARRANGEMENTS
The Trust has established a Technology Enabled Change (TEC) Programme
Board with representation from all project managers who provide a bi-monthly
update on behalf of the SRO of each project. This group makes proposals
relating to ICT investment and these are submitted to SMT for approval in the
form of business cases. The Group reports to the Trust’s Senior Management
Team (SMT) through the Executive Director with responsibility for ICT (Director of
Performance & Reform). The TEC Project Board is responsible for ensuring that
ICT projects are delivered on time and on budget as well as monitoring of joint or
inter-organisational projects such as those Regionally funded. The TEC
Programme Board will assist in ensuring that the ICT Team responds to the
needs of the entire organisation and that investment is objectively prioritised. A
TEC update is provided to:
- Information Governance Forum which reports to Trust Governance Committee
(Quarterly)
- SMT (bi-monthly)
- HSC funded schemes are reported to HSC E-Health Programme Board
(quarterly)
In addition, a monthly Informatics Governance meeting is held to review risk, audit

5
and incidents and any issues are escalated to the Performance & Reform risk
register when appropriate.
Figure 2.1 Informatics Governance Framework
2.2 Information Governance Assurance
The Information Governance agenda currently encompasses the following areas;-
Information Governance Best Practice and Management;
Confidentiality and Data Protection;
Information Security;
Secondary uses of information;
Clinical Information assurance; and
Corporate Information assurance such as FOI.
There is a new Controls Assurance Standard in Northern Ireland for Information
Directional & Representational Information Governance: Operational Information Governance:
Information Governance
Forum
AD Informatics
Head of Information Governance & Head of IT
(IT Security Officer)
Director of Performance & Reform (SIRO) &
Medical Director & Director of CYP (Personal Data Guardians)
Chief Executive Data Controller
Regional Information Governance
Advisory Group
Trust Board
t
SMT FORUM
Governance Committee
Records Management Committee & TEC Programme
Board
Data Protection Sub-Group, Informatics Governance Meeting, DQ Steering Group, Clinical Coding forum
HSC ICT Programme Board

6
Management which is reported annually and monitored on a quarterly basis.
Substantive compliance against this standard is required. The Southern Trust
achieved this standard in 2014/15 and has an action plan to improve the overall
scores for the future.
Ultimate responsibility for Information Governance within the Trust lies with the
Trust Board. However, table 2.1 illustrates that there are personal Data
Guardians and a Senior Information Risk Officers (SIRO) at Board level. The
SIRO acts as an advocate for Information Risk Management on the Board and
provides written assurance to the Department of Health & Social Services in
Northern Ireland on an annual basis. The SIRO is responsible for developing and
encouraging good information handling practice amongst all members of staff
employed or contracted by the Trust.
In summary, the structure & governance arrangements in place in the Southern
Trust comply with the requirements of relevant Controls Assurance Standards
and Audit recommendations.
3.0 MEETING THE QUALITY AGENDA
The Southern Trust places a strong emphasis on quality improvement. Within the
Informatics Division it is recognised that there is a growing appetite with most
staff to embrace technology and use it to improve their working practice; quality of
care given; or help address some of the challenges that they face. Added to that,
there is paramount importance placed on Data Quality and completeness and
timely recording of information to support service delivery and manage clinical
risk. There is also a growing importance on communication and information
sharing between the Trust and all stakeholders in care, including external
partners in Health & Social Care delivery. The NIECR is an excellent example of
how Regionally, information is being shared safely and securely.
Within the Informatics Division the following objectives for improving and
maintaining quality are paramount:

7
Use of PRINCE methodology in project implementation to ensure that project are
delivered on time and within budget;
An emphasis on developing baseline information and benefits methodology so
that the benefits of IT implementation can be clearly identified during post project
evaluations (PPEs) or at the end of pilots to establish the benefits to be gained
from further implementation; and
Improved collaborative working across HSC Northern Ireland and a ‘once for all’
approach to IT solutions for HSCNI.
The Informatics Division in the Southern Trust is also proud to have been winners
of 3 Regional awards in 2014/15. These were for E-Discharge implementation,
PARIS use across an integrated pathway and video conferencing use by Speech
and Language Therapists for patient therapy following stroke.

8
4.0 RESOURCES
The Informatics structure in the Southern Trust is as follows:
Table 4.1 Informatics Structure
There is a total of 112 WTE staff employed in the Informatics Division. This
includes permanent, temporary and capitalised postholders. There are no
agency staff employed.
Personal Secretary Assistant Director of Informatics
Head of IT
Server & Infrastructure
Support
IT Service Desk Support
Network & Security Support
IT Contracts Manager
Head of Information Governance
FOI/DPA
Information Governance
Closed Records Storage
Head of Information & Data Quality
Clinical Coding Services
Information Analysis
Data Quality
Head of IM&T Project
Management
Business Case
Implementation
PPE
ICT Traininig
Head of PARIS Implementation
IT Innovation
e.g. PARIS Mobile, NIECR Integration
Reporting Development
PARIS Implementation

9
5.0 SUMMARY OF 2014/15 ICT DELIVERY & ACHIEVEMENTS
The table below provides a summary of what was achieved in the last financial
year.
Table 5.1 Summary of ICT Delivery in 2014/15
Infrastructure & Governance
Build new Cisco Infrastructure to improve resilience of network.
Replacement of Core Network in DHH.
Resilient new ether connect link from CAH to DHH.
Installation of Wireless Controllers in Data Centres.
Microsoft Enterprise Agreement for licencing.
Upgrade of Digital Dictation
Latest Anti-Virus Protection and upgrade of firewall as best practice security risk reduction
Monitored and certified destruction processes for old hard drives to government standards.
Replaced all PCs that were more than 4 years old (750 PCs).
Use of Bit Locker and Mobile Device management to secure and control portable devices.
VDI (Virtual Desktop Infrastructure) & iPads.
Medical Devices Business Continuity.
Provision of One View Infrastructure
Replacement of Email Archive
Extension of Storage in Data Centres
Communications
Bedside Entertainment, Mandeville Unit
Rollout of 20 additional VC Units.
Paperless Board (Minute Pad).
Introduction of ‘Skype’ Virtual Patient/Client treatments using Video conferencing.
Voice recognition pilot in Paediatrics.
Roll out of Flow Bed Management electronic whiteboards.
Savience Self Check-In across acute services including language translation.
Wi-Fi in Community Sites (43 sites).
Replacement of Computers on Wheels on wards and additional units to increase ward access to IT.

10
Clinical Systems
Cleanliness Audit system Implementation of 2 way PAS on Flow and allow admissions, discharges and transfers to take place by nurses using the whiteboard
Single Sign-On extension and enhancement.
Endoscopy on-line survey. Anaesthetics Electronic Record.
PARIS continued roll out
Bi-Pacs Digital Breast Screening.
E-rostering implementation in 3 wards
PARIS Mobile.
Regional Systems
BSTP. HRPTS. NIECR maximisation
Table 5.1 provides a very high level summary of the Infrastructure and
Governance elements of the ICT Infrastructure in the Southern Trust which were
upgraded or enhanced in 2014/15. It also provides a very high level summary of
the improvements in Digital Communication in the Trust, as well as the Clinical
Systems that were delivered or upgraded.
The table does not in any way reflect the amount of time, money or resources
involved (in collaboration with suppliers), to deliver this. Some examples of the
tangible achievements are as follows:
5.2 Digital Dictation
Digital Dictation is now the methodology of choice for drafting Clinical Letters in
the Trust. In December 2013 there were around 11,000 digital dictations per
month. This has now grown to over 24,000 dictations per month. This system
not only improves the sound quality for the staff typing the letters but it also gives
a clear indication to managers of where there are dictation backlogs and where
resources need to be diverted to ensure timely communication with GPs.

11
5.3 NIECR Implementation
In December 2013 the Southern Trust had just over 600 NIECR Users. This has
grown to over 3,000 users who collectively access NIECR over 50,000 times per
month.
5.4 Single Sign On
At the commencement of Single Sign-On in February 2014, there were 400 users
of the system who accessed just over 2,000 times per month. There are now
7,760 users of Single Sign-On and on a monthly basis, 400,000 access to
systems are made per month using SSO, minimising the need to remember
passwords for multiple systems. All information systems are now available using
Single Sign on
5.5 Community Information System
Since December 2013, the number of Paris users has grown from 46 to 1,300,
which is around one third of the total planned. There are 100 PARIS Mobile
users who can access a ‘briefcase’ version of PARIS when they are in Patients or
Clients own homes, or outside a Trust facility. Some services, such as
continence, are now completely paperless and have managed to increase clinic
capacity and share admin resources as a result of this. Some PARIS Mobile
users have indicated that they are saving around 40 miles per week in travel cost
and time since the introduction of PARIS Mobile.
5.6 ICT Training
The small (5 WTE) ICT training team continue to provide training for existing
Information Systems in the Trust such as PAS, ED, Theatre systems, for newly
appointed staff to the Trust. As well as existing system support, the Training
team are also involved in the training for new system implementations such as
the Community Information System (PARIS).
Training is delivered using a variety of learning methods such as drop in

12
sessions, classroom training, video clips as well as floor walking to support users
when they first start using the new system in their daily work. In the past 12
months the team have also successfully implemented the NHS skills pathway
solution which is an e-learning solution for the Microsoft suite of products, Word,
Excel, Power Point, Outlook and OneNote. This has been extremely successful
and has resulted in the Southern Trust being the highest user of this product
across the NHS in the UK.
The team continue to investigate innovative training solutions such as short video
clips, virtual classrooms as well as e-learning to support the increasing use of
technology across the Trust and provide the flexibility of learning approaches to
suit the needs of staff. As and when available and required, non-recurrent
funding is used to buy-in additional training sessions, such as basic ICT, to
facilitate HRPTS and BSTP implementation.
The diagram overleaf illustrates the journey of ICT achievements in the Southern
Trust over the past 18 months.

13
Figure 5.7 - The Journey of ICT Achievements in SHSCT 2014 & 2015.
Robotics
Touch Screen
Technology (Flow)
Patient Self Check-In
Single Sign-On
VDI (Virtual Desktop
Infrastructure) iPads
NIECR Portal
(Regional)
Digital Dictation &
Voice Recognition
Virtual Clinics using
Video Conference
Paperless Board
Employee Self-Management (Regional
HRPTS, BSTP, E-Rostering)
PARIS Electronic integrated H&CC
record in community based services and
acute mental health.

14
5.8 Accomplishment of ‘Technology Enabled Change’ (TEC) 3 Year Strategy
These achievements are tangible outcomes from the objectives of the Trusts ICT
Strategy - Technology Enabled Change, (TEC) which requires renewal in April
2016. In summary, the accomplishments against TEC have been:
More real time data entry and employee self-service into Regional systems such
as HRPTS, BSTP and local systems such as E-Rostering, E-Discharge and
PARIS.
Paperless or Paper Light working, particularly in community based services
through the implementation of PARIS and excellent pilots of scanning paper
document into the electronic records e.g. Home Treatment Crisis Response
Team.
Improved medical and nursing handover through use of the Regional NIECR
Portal and local systems such as Clinical Noting and Flow.
Greater emphasis on information systems providing patient care and supporting
clinical processes, such as the implementation of the Anaesthetics system.
Greater emphasis on integration of systems such as bi-directional PAS on Flow
electronic whiteboards and TMS Interface with the Anaesthetics Electronic
Record. PAS now interfaces to all of our patient information systems as a single
patient demographic record.
An emphasis on information being recorded only once, duplicate entry minimised
and systems accessed securely but more easily – e.g. single sign on.
Alongside this, ensuring that we develop and maintain a sound, robust, resilient,
secure and reliable information systems infrastructure.
Trust-wide engagement to update our ICT Strategy will commence at the beginning of
2016 and the following engagement methodologies will be used:

15
Figure 5.8.1 – Planned Engagement Methodology ICT Strategy 2016 – 2019
In addition, learning will be applied through:
Feedback from Specialist Exhibitions;
Engagement at a local and National level with other Trusts; and
Use of the Technology Partnership Agreement expertise and learning.
Planned ICT Strategy
Engagement Workshops
Online Survey /
Suggestions
Existing Forums
1:1 Interviews
Regional Stakeholder
Meetings Patient Access Groups
Staff Groups/
Workforce
Ward / Department
Visits
Walk rounds

16
6.0 EXPENDITURE 2014/15
The Trust’s total ICT Expenditure in 2014/15 was as follows:
Table 6.1 – Summary of ICT Expenditure 2014/15
Category Source Expenditure
Capital CRL
Ring-fenced
CIS
£975,981
£5,018,874
£1,683,486
Capital Total £7,678,341
NNR Total £642,326
Salaries £3,376,356
Good &
Services
£626,464
Recurrent Total £4,002,820
Grand Total £12,323,487
6.2 Analysis of 2014/15 Expenditure
Capital
Total capital expenditure increased by £1.2M compared to the previous year. This
was due to £2.6M investment in Microsoft Licencing Agreement to ensure desktop
and data centre licencing compliance for the next 3 years.
Non Recurrent Revenue
NNR investment decreased by £100,000 compared to the previous year.
Recurrent Investment

17
Recurrent investment remained relatively static with an increase of £10,000 due to
incremental rises in salaries.
7.0 REGIONAL E-HEALTH PROGRAMME
2015/16 year to date has been an unusual year in the HSCNI ICT Investment arena.
Firstly, availability of capital funding Regionally has been at an all-time low and
allocated funding at the end of December was £2,860,000, with a circa £4,000,000
shortfall compared to requirements (Trust own priorities – excludes Regional priorities
such as Accelerated Access to ICT). There has been increased Regional interest in
ICT in the following context:
7.1 Regional E-Health & Care Strategy
A Regional E-Health & Care Strategy has been drafted and awaits Ministerial
approval. Fundamentally, the main thrust of this strategy is a ‘Once for NI’
approach to ICT implementation. This is a new direction for HSCNI, where up
until now, commissioning of ICT has encouraged local innovation to help reform
services.
This new approach is inevitably resulting in longer decision making timeframes
and has led to limited investment in local priorities year to date. However, it is
recognised and hoped that this approach will lead to efficiencies and reduce the
Trust boundaries which exist in terms of patient and client information sharing.
7.2 Shared Services ICT & Business Intelligence
A scoping study earlier in the year has led to the appointment of Deliotte to
conduct a feasibility study on the potential for shared ICT and Business
Intelligence services, most likely managed by BSO. Again this has placed new
emphasis and interest in ICT investment decisions and all investment in ICT has
required DHSSPS approval, which has led to delays in business case and service
investment approvals.

18
7.3 EHCR for HSCNI
Due to the urgent need to replace the HSCNI PAS System, a Regional scoping
study has led to investigation of a potential single Electronic Health & Care
Record for Northern Ireland. A business case is being produced to identify the
preferred option and cost. However, local investment decisions are being
delayed in this context, to avoid any investment being counter strategic.
It is acknowledged by the Trust that these are 3 important factors and
considerations and the Trust continues to engage with DHSSPS, HSCB and BSO
to help inform Regional business cases and scoping studies.
7.4 Tele-Health & Telecare
The Regional Tele-monitoring contract is due to expire and a review of the
service outcomes is underway, alongside a planning workshop which will take
place in January 2016. Tele-health is likely to play a key part in future HSCNI
service delivery in the future.
7.5 CAWT
The CAWT project is already starting to acknowledge the huge part that
technology can play in terms of cross boundary service delivery. It is anticipated
that CAWT initiatives are likely to include ICT investment in the future to share
services and information.

19
8.0 PLANS FOR 2015/16 & 2016/17
This section will outline the following:
ICT Procurements undertaken in 2014/15, which are currently being
implemented in 2015/16;
Technical Infrastructure Refresh requirements for 2015-2017 including
costs.
Service Development aspirations in the Trust which are dependent upon
funding availability and also Regional Strategic Direction, as outlined in
Section 7 of this Plan.
Projects which have not progressed, as they have been deemed
Regionally as counter strategic.
Ongoing assessments of best practice technologies which may bring
service improvements in the Southern Trust.
Summary of Funding Gaps.
8.1 ICT Procurements Undertaken in 2014/15 – Implementation Progress
Update
Anaesthetic Record Keeping
This system was procured from OxygenCare in 2014/15. It is the system of
Regional choice and has been in use for some time in the South Eastern Trust.
This system creates an electronic Anaesthetic Record and went live on 20th July
2015 in Theatres 1-8 in Craigavon Area Hospital. The Southern Trust has
enhanced the system through interfacing with the Regional Theatre Management
System (TMS) which means that the Theatres lists are automatically populated.
The Southern Trust has also made a further enhancement through an interface
with PAS to automatically download patient demographics. This fits in with the
Trust Technology Enabled Change Strategy by ensuring that data is entered only
once and minimises duel entry thus saving time and reducing errors.
In addition,, the Trust is making best use of this system and is piloting a Pre-
Operative Assessment Module. Learning from this pilot is being shared

20
Regionally. The pilot is testing the proof of concept of patients completing
electronic assessment forms using an iPad device, which means that the
information is available for Anaesthetists, Surgeons and also ward or Day
Surgery staff. The current model for Pre-Operative Assessment is very paper
dependent and there have been occasions where not all of the documentation is
available at the point of care. This system therefore manages this risk.
It is a challenging project implementation as it requires all Theatre staff to move
from papers to electronic processes. However, there has been excellent
leadership within the Theatres and Anaesthetics Department and as a result,
excellent progress has been made. It is expected that roll out will be completed
Trust-wide by 31st March 2016.
Multi-Functional Device (MfD) Retendering
The Trust’s contract for Multi-Functional Devices is now end of life. A re-
procurement was completed in 2015/16 and Konica Minolta have been appointed
as the preferred supplier. A project plan is now being drafted to replace all
existing Multi-Functional Devices with new state of the art functionality. Some of
the enhancements to the new devices include the Trust’s ability to meet ISO
standards for scanning which will enable the Trust’s scanned documents to meet
legal admissibility requirements. All Multi-Functional Devices should be replaced
by 30th June 2016.
Cleanliness Audit System
The Southern Trust participated in a Regional procurement of a Cleanliness Audit
System. Two other Trusts have worked with the Southern Trust to implement this
and the system is now in use.
Single Sign-On
Single Sign-On Functionality continues to be developed. There are now 7,760
active users in the Trust and over 400,000 system accesses per month. Single
Sign-On cards are now being offered as a replacement to staff identity cards.
Proximity readers to allow staff to swipe their Single Sign-On Card to access the

21
systems that they are entitled to, are currently in use in two departments in the
Trust. Further roll-out is planned this year.
Implementation of Community Information System
Roll-out continues and there are now 1,300 users. The majority of Mental Health
Services are now working digitally with Support & Recovery services now in
progress. Significant progress also continues within Integrated Care Teams in
the OPPC Directorate. Paris development was required for Child & Family
Functionality which has delayed aggressive roll out in this area, although services
such as CAHMS and Autisim are making excellent use of the system. Some
progress has been made to interface PARIS with NIECR which when complete,
will significantly assist staff in Acute Care and Non-Acute hospitals in facilitating
early discharge through having the right community based information to assist
with discharge decisions and home care packages.
Funding will be required to continue will roll-out of PARIS for a further 3 years.
An optimum bias paper has been submitted to the Department of Health & Social
Services. It is hoped that this bid will be successful and has Commissioner
support.
Capital cost £750,000 per annum for 3 year period
PARIS Mobile Pilot
50 staff are now using PARIS Mobile functionality. A Consultant from the
Beeches Management Centre has been appointed to undertake focus groups
with PARIS Mobile Users to provide baseline information and indications of
benefits from this.
Based on user feedback, development work continues with Civica and their
partner Total Mobile to add more functionality into the PARIS Mobile Solution,
which is a ‘briefcase’ or off-line version of Paris which can be used when staff
don’t have a wifi or 3/4G connection.
Costs for further roll out of Paris Mobile are included in the Regional Accelerated

22
Access to IT business case bid.
ECR Maximisation
The Trust continues to encourage use of the NIECR and throughout the PARIS
Implementation, staff are also being given access and advice on NIECR during
their PARIS training session. The Trust now has over 1,800 regular users and
3,000 registered users. The Trust is enthusiastic about developments on the
NIECR including electronic triage of outpatient Referrals and awaits a timeframe
for implementation from the BSO.
Use of iPads
The Trust procured iPads and VDI (Virtual Desktop Infrastructure) to enable staff
to access IT in a more portable way. An iPad survey was issued and 12
recommendations were made on the basis of this. Work continues on iPad
configuration and some examples of improvements are that the email App has
been extended to include 30 days of emails and instructions have also been
issued to iPad users on how to use these devices outside Trust sites. Work is
on-going to enable access to Apps securely on Trust iPads..
PC Replacement
The Trust continues to refresh its PC Estate. Desktop refresh has now been
completed and all PCs and laptops within the Trust are now a maximum of 4
years old. This minimises user hardware problems and ensures that the Trust
can make best use of any new available software as operating systems are up to
date. This is an annual rolling programme. £450,000 funding has been secured
to replace 750 PCs in 2015/16 to ensure that this hardware remains refreshed.
Continued Implementation of Flow & Note in Acute
The Flow Electronic White Boards were fully implemented across the Trust Acute
and Non-Acute Wards in 2014/15. However, further significant development has
been achieved in 2015/16. A Bi-Directional PAS link has been included in Flow
which means that Nursing Staff and Doctors can use the Electronic Touch Screen

23
to discharge and transfer patients in real time. In addition, a suite of reports has
now been developed on Flow which better enables Bed Managers to have a
more accurate picture of actual bed availability across the Trust. Like every
significant transformational change where there are a range of multi-disciplinary
shift and bank staff workers, further engagement is on-going to ensure maximum
use of this system.
Electronic Patient Centre Documents to GPs
The Southern Trust is leading a Regional project to make discharge letters and
clinic letters available directly into GP Systems. This has the advantage from the
Trust perspective in that letters do not have to be printed and sorted by
secretarial and audio typist staff. It has the advantage for GPs in that they get an
immediate copy of the letter as soon as it has been typed. This has been a major
transformational change and will reduce letters generated across the HSC by
18,000 per week. A roll-out plan is in draft and will be approved at project board
in January 2016. It is anticipated that all GPs will be able to access their letters
electronically by the end of the financial year.
Pilot of Voice Recognition Software in Acute Paediatrics
Diagnostic teams in Laboratory and Radiology have been using Voice
Recognition Software for some time. However, as diagnostic reports tend to be
relatively short and succinct, there has been less voice training requirement for
the software than in other specialities. The Paediatrics Department volunteered
to lead on a pilot for Voice Recognition and software was procured last year. The
Informatics division has been working with the Paediatrics Department since
then. It has proven to be very time consuming for the Data Dictionaries to be
developed for such detailed and diverse letters and language, however, there is
some success with individual clinicians who have had the patience to continue to
train the software. Evaluation and feedback continues with users.
Extension of Savience Patient Self Check-In
14 new self-check-in kiosks were procured last year based on the success of
24
pilots in Craigavon Area Hospital and Daisy Hill Hospital. These kiosks are
primarily targeted in areas where there are no receptionists on duty. The new
measured term contract for cabling delayed the installation of these kiosks but
this is being addressed in 2015/16 and usage is being monitored by the Assistant
Director of Support Services in Acute Care.
Document Scanning
In 2014/15 the Continence Service agreed to pilot scanning of records attached
to the PARIS record. A post project evaluation has been undertaken in 2015/16
and was presented to the CIS Programme Board in December 2015. The
recommendations from this pilot are that originals of the scanned documents can
be destroyed as the scanned documents are legally admissible and no
documents could not be retrieved digitally in a 12 month period of the pilot. It will
be recommended to SMT that this model is rolled forward with all further PARIS
roll-out and this should bring both efficiencies and improved information
governance.
8.2 Technical Infrastructure Refresh Requirements for 2015/17
The Southern Trust has an extremely complex ICT Infrastructure, linking to BSO
Regional Data Centres to bring access to the Trust to the Regional, private,
Secure HSCNI Network, as well as important Regional Applications such as
NIECR, BSTP, HRPTS, Laboratory System and PACs Radiology System. The
Southern Trust Infrastructure delivers these Regional systems and network to
over 8,000 IT users in the Trust, across 100+ sites. In addition, the Trust hosts
100+ local Applications such as PARIS, email, Flow bed management and E-
Discharge. We also manage cyber security, firewalls, data storage and business
continuity.
The nature of the Trust’s business means that data security is of paramount
importance and there is huge emphasis on ensuring that data is not intercepted
or lost. This is not without a high level of investment.
25
This section details the necessary investment in the Trust’s ICT Infrastructure to
ensure the following:
Highly available ICT across the Trust;
Minimum disruption to staff from ICT outages;
Optimum security of data; and
Minimisation of the risk of data loss.
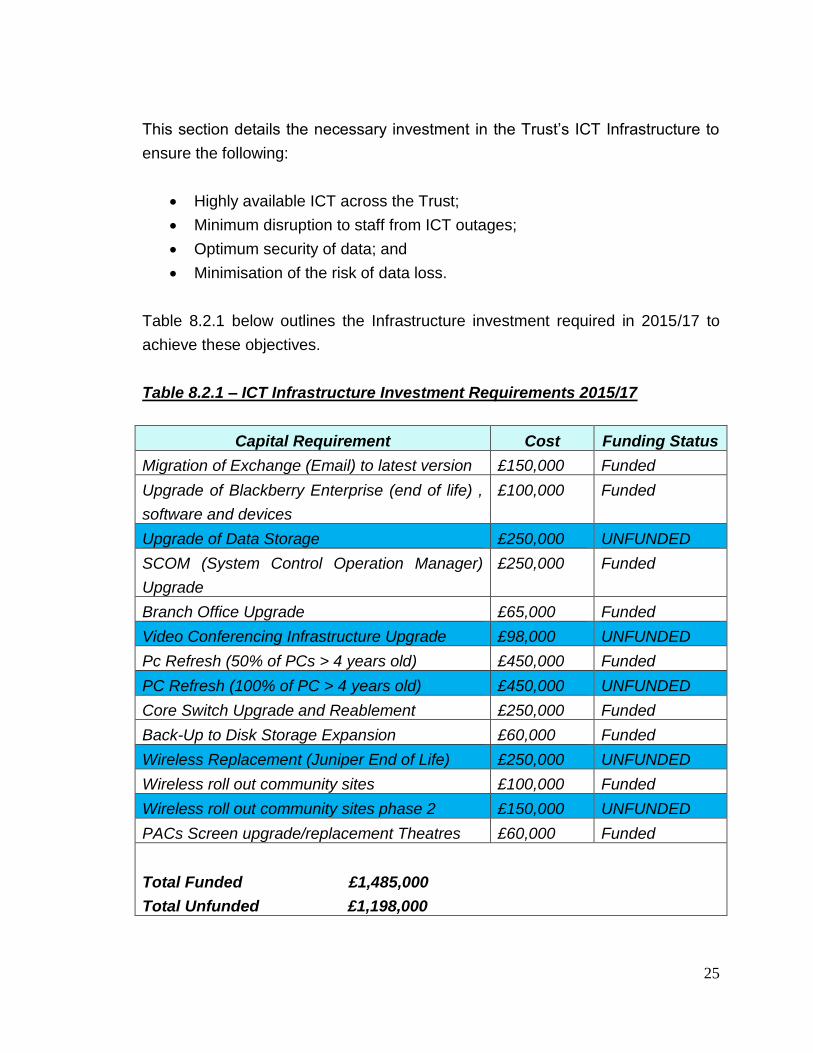
Table 8.2.1 below outlines the Infrastructure investment required in 2015/17 to
achieve these objectives.
Table 8.2.1 – ICT Infrastructure Investment Requirements 2015/17
Capital Requirement Cost Funding Status
Migration of Exchange (Email) to latest version £150,000 Funded
Upgrade of Blackberry Enterprise (end of life) ,
software and devices
£100,000 Funded
Upgrade of Data Storage £250,000 UNFUNDED
SCOM (System Control Operation Manager)
Upgrade
£250,000 Funded
Branch Office Upgrade £65,000 Funded
Video Conferencing Infrastructure Upgrade £98,000 UNFUNDED
Pc Refresh (50% of PCs > 4 years old) £450,000 Funded
PC Refresh (100% of PC > 4 years old) £450,000 UNFUNDED
Core Switch Upgrade and Reablement £250,000 Funded
Back-Up to Disk Storage Expansion £60,000 Funded
Wireless Replacement (Juniper End of Life) £250,000 UNFUNDED
Wireless roll out community sites £100,000 Funded
Wireless roll out community sites phase 2 £150,000 UNFUNDED
PACs Screen upgrade/replacement Theatres £60,000 Funded
Total Funded £1,485,000
Total Unfunded £1,198,000

26
A significant amount of non-recurrent revenue has also been invested in ICT in
2015/16, to address licencing and support gaps in the Southern Trust as follows:
Table 8.2.2 – Non Recurrent Investment Requirements 2015/17
Purpose Cost Funding
Data Protector Licence for backup £13,500 Funded
MS Terminal Services Licences £14,050 Funded
Sharepoint Configuration £19,580 Funded
Cisco Support £45,000 Funded
Office Pro Plus £2,620 Funded
Apple Mobility £10,000 Funded
HP Technical Support £24,986 Funded
Adobe Pro Licences £1,378 Funded
Capita Operations Support £56,683 Funded
HP Hardware Support £11,652 Funded
3rd Party ICT Basic Training Support £9,992 Funded
Team Training Up skilling £8,500 Funded
QoS Operational Support £6,700 Funded
IP Routing Operational Support £2,257 Funded
Network Security Admin Licences £3,360 Funded
TOTAL £230,260 Funded
8.3 Service Development Aspirations Dependent on Funding Availability
This section outlines the service development requests and aspirations which
have been raised by employees of the Trust. These are very dependent on
available funding but also Regional strategic direction and approval, due to the
on-going discussions about an EHCR for Northern Ireland (see section 7).
Electronic Solution for Scanned Records for HR
Belfast Trust have implemented a solution known as Automated Intelligence
which has enabled them to scan HR Records but also anotate the scanned

27
version to add notes to them electronically. The Southern Trust had initially
anticipated that this functionality would be available on HRPTS but it is not. The
Director of HR is keen to pursue this solution as HR Records are now required to
be retained for 100 years. A demo has been requested with Belfast Trust and a
business case is being prepared to avail of slippage funding.
Capital cost estimated £200,000.
Health & Safety Risk Assessment System
The HR Department are keen to implement an electronic system to conduct
health and safety assessments. This is based on an audit recommendation.
Discussions are on-going in relation to this, as this would be another system and
password for staff which may be difficult to embrace given the magnitude of
change for staff across the Southern Trust using BSTP and HRPTS Systems as
well, as systems such as Datix and any other clinical systems.
Capital cost £17,000 Recurrent Revenue £6,000 per annum
Paperless IT Requests and Tracking
The Trust currently uses INFRA for logging of IT support requests and equipment
requests. This system is not fit for purpose as it does not allow users to track
their requests for either IT support or equipment. In addition, it does not provide
the data analytics required to effectively run and manage a wide geographically
spread IT service desk, for example highlighting recurrent user issues or area
wide faults.
Capital requirement £150,000 Recurrent Revenue £10,000 per annum
Electronic Ordering Solution
Based on the successes of Flow Electronic Whiteboards, Acute Services
colleagues have indicated that it would be extremely beneficial for the screens to
have a portal ordering system. This exists in areas such as Physio requests, or

28
social work request, but would require extension to enable a request for
cardiology diagnostics or referrals to another speciality. At present all of this is
done on paper which creates time delays and also means that the orders are not
traceable and trackable. A business case is being prepared for this to avail of
slippage if available.
Capital cost £250,000 Recurrent Revenue £60,000 per annum
ICU Live Monitoring System
The Southern Trust is the only ICU Department which does not have a live
monitoring system. Visits have been made to other Trusts and Consultant
Intensives are keen to progress this. This would assist in managing risk and is a
once for all solution for Northern Ireland. A business case has been prepared to
avail of slippage funding.
Capital costs £203,000 Recurrent Revenue £38,000 per annum
Electronic NEWS Alerting
The Southern Trust has piloted Electronic NEWS. This involves nursing staff
inputting vital signs onto an iPod other portable device and these being displayed
in a NEWS Score on the Electronic White Boards. A business case is being
prepared to avail of slippage funding for this.
Capital Cost £250,000 Recurrent Revenue £24,000 per annum
Regional Access to IT Business Case
The HSC Board has prepared a business case for improved access to IT. The
costs associated with providing 3,000 additional users with mobile devices and
access to the appropriate applications such as PARIS, NIECR, Equipment
Ordering, BSTP and HRPTS are to included in the business case. The costs are
as follows and would have to be met through a Regionally approved business
case:

29
£7,140,510 Capital £1,601,850 Recurrent Revenue
Patient or Guest Wi-Fi in Hospitals
SMT have approved a business case to implement patient and guest Wi-Fi in
hospitals. This will bring benefits to patients in hospital beds but also those
waiting for outpatients/ED and also strategically enables tools such as ‘survey
monkey’ to be sent to patient’s smart phones or devices, which will make gaining
valuable user feedback easier.
Capital Cost £15,000 Revenue Cost £20,000 per annum
Document Management System on PARIS
Roll-out of PARIS has identified a significant issue for users. Users are scanning
documents to the PARIS Record but as this record grows, a document
management system is required to organise these so that it is clear which
documents are required for direct patient or client care at that time. The Trust
has offered to pilot this on behalf of the HSCNI and share learning on naming
conventions and processes.
Capital cost £200,000 (funding approved by HSCB)
Video Conferencing Units
There is a request for 6 further Video Conferencing Units in Paediatrics, Stroke,
Support & Recovery, Mental Health, Palliative Care and OPPC. The
implementation of these Video Conferencing Units is not only dependent on
funding for the units, but is also dependent on funding identified in the Technical
Infrastructure requirements (Table 8.2.1) to increase the capacity of Video
Conferencing across the Trust. At present, the Trust has used its full capacity for
Video Conferencing and the Infrastructure upgrade is a pre-requisite for any
additional units.
Capital cost £60,000

30
Call Recording in the ED Department
Following a SAI, it is recommended that calls are recorded in the ED Department.
Capital cost £8,000. Recurrent Revenue £650.00 per annum
Bluestone Mobile Connectivity
Following an SAI, it is recommended that mobile phone connectivity is boosted in
the Bluestone Unit.
Capital cost £150,000
Conference Me iPads
One of the recommendations from a recent iPad survey was that it would be
useful to be able to use Conference Me on their iPads. Some staff have
indicated that if this functionality was available, they would be able to forfeit their
laptops or PCs.
Capital Cost £250,000
Admin Licences for HRPTS
It has been established that due to capacity shortfalls, some Senior Managers are
sharing passwords with secretarial staff to undertake HRPTS functions and BSTP
functions. It is recommended that the Trust invests in administrative licences to
mitigate this risk.
Capital cost £172,800 Recurrent Revenue £40,000 per annum
Speech Recognition Point & Click
Following a recent pilot, some staff who have very poor typing skills, have

31
requested licences for speech recognition to point and click into the PARIS
Application and a speech recognition software to recognise and type their
dictation.
Capital cost £50,000
Direct Access for EEG Reporting
In order to improve EEG Reporting turnaround, software can be installed in the
Royal Victoria Hospital, to allow colleagues remote access to EEG images to
enable digital reporting, thus improving turnaround of results.
Capital cost £22,000
Data Analytics
There are a range of Data Analytics projects which are on-going across the Trust.
These include;
Availability of PARIS Data in the Regional Data Warehouse
Making best use of the Microsoft Enterprise Agreement to utilise Microsoft
licences for Data Analytics for Acute Information to present a dashboard.
Department led work on changes on risk adjusted mortality indicator
reporting to new SHIMI. The Trust is working with the Department of
Health to better understand the logic and analytics around this.
M&M (Mortality and Morbidity) reporting. The Trust is working with the
Department to share learning on M&M processes and reporting to facilitate
the specification and development of a Regional system.
Clinical coding improvements in turnaround continue. The Trust is
achieving the Regional 3 month target and now 97% of all Trust FCEs are
coded within 60 days. The importance of timely and accurate clinical
coding to improve data analytics is recognised and a priority for the Trust.
Whilst none of these projects have direct capital costs, they are on-going
investments in staff time to better improve availability of complex information

32
across the Trust.
Patient Self Check in Using Paris
Mental Health and OPPC teams are keen to avail of existing self check in kiosks
across the Trust for users to self check in using Paris. At present, the kiosks are
only linked to PAS, but CIVICA (Paris supplier) have done integration work to
facilitate use.
Capital cost £79,000 Recurrent Revenue Cost £3,500 per annum
As indicated in previous sections at this stage in 2015/16, none of these service
developments proposals have attracted any funding with the exception of a
document management system for Paris. However, it is useful to have this list
available for budget planning for 2016/17 and also to avail of slippage as all
projects can be procured at short notice due to business cases being in place,
procurement avenues being secured and the fact that the majority of the
requirements are licenced based which means that they can become Trust
assets very quickly. In summary, the deficit costs are as follows:
Table 8.3.1 Funding Deficit Relating To Requested ICT Service
Developments
Project Capital Cost Revenue Cost
Automated Intelligence (HR record
scanning)
£200,000 None known
Health & Safety Risk Assessment £17,000 £6,000
IT Paperless Requests and Tracking £150,000 £10,000
Electronic Ordering £250,000 £60,000
ICU Live Monitoring £203,000 £38,000
Electronic News Alerting £250,000 £24,000
Regional Access To IT
(excluded from total costs as needs to be
Regionally Funded)
£7,140,510 £1,601,850
Guest Wifi £15,000 £20,000

33
Video Conferencing Units £60,000 none
Call Recording in ED £8,000 £650
Mobile phone connectivity Bluestone
Unit
£150,000 none
Conference Me on iPADs £250,000 None known
Admin Licences for HRPTS £172,800 £40,000
Speech Recognition point and click pilot
in Paris
£50,000 None known
Direct Access EEG Reporting £22,000 None known
Patient Self Check-in Paris £79,000 £3,500
TOTAL (excludes Regional Access To IT
business case)
£1,876,800 £202,150
8.4 Projects Which Have Not Progressed As They Have Been Deemed Counter
Strategic
This sections outlines a number of Trust aspirations which have not been
progressed as the HSCB E-Health Programme Board have indicated that they
are counter strategic, due to on-going considerations of a Regional EHCR (see
Section 7). These are as follows:
Microbiology Information System
The Trust Microbiology Consultant is particularly keen to improve Microbiology
Reporting and alerts and it is not possible to do this on the existing Laboratory
system. A preferred Information System was identified by the Southern Trust but
this is not being pursued as it is deemed counter strategic in the context of an
EHCR for Northern Ireland.
Clinical Noting Development
The Trust planned to further develop its Clinical Noting System which is linked to
the Flow Electronic Whiteboards and provides some handover and task
management solutions. The Trust had hoped to develop electronic forms with
some snomed coding and data analytics, so that Clinical noting could be used as

34
an alternative to continuation notes in paper case notes, or as an alternative for
completion of paper forms which are currently filed in casenotes. This has been
considered counter strategic in the context of EHCR.
E-Prescribing
The Trust was keen to pursue a digital solution for outpatient prescribing. At
present when a Consultant wishes to change a medication this is handwritten on
a triplicate proformas, with a copy given to the patient to give to the GP. This
leads to issues with legibility and queries from GP practices in relation to dosage
etc. The Trust had planned to develop its Clinical Noting Solution with E-Forms
to overcome this but this is deemed counter strategic.
In addition, Regional plans for a Regional E-Prescribing Module have been halted
whilst discussions continue regarding an EHCR.
8.5 Ongoing Assessments of Best Practice Technologies Which May Bring
Service Improvements in the Southern Trust.
This section outlines the ongoing work with professional teams across the Trust
to establish best practice ICT innovation and potential technology enabled
innovation.
Stroke Service
A visit is planned to University College Hospital, London, to see Stroke Pad in
use. This system has been designed and developed to capture all stroke related
information and seamlessly present the data required for SSNAP reporting. The
visit is scheduled for February 2016 and dependent upon Clinicians views of the
system, may be business case and bid for 2016/17.
RFID
Western Trust is exploring installation of RFID to improve tracking of paper

35
records and equipment. A feasibility study is ongoing will be shared with other
Trusts. This may be a business case and bid for 2016/17
Clinical Communication Gateway (CCG)
Southern Trust is keen to be able to receive electronic referrals made by GPs
directly into the Paris application. At present this is only feasible in PAS for acute
services and the Southern Trust has not yet been provided with the software by
BSO – it is still in pilot in Northern Trust. Southern Trust will work with BSO to
influence Paris integration which will minimise data entry of information provided
in a GP referral for community and mental health based services.
Electronic Triage
NIECR includes functionality for electronic triage of acute referrals. This is being
piloted by Northern Trust. The Southern Trust will work with BSO, aiming to be
an early adopter of paperless referrals and triage when the software is signed off
by Northern Trust. This will minimise referral printing, scanning and filing and
also data entry on PAS.
Project Echo
The Trust will continue to invest in Video Conferencing infrastructure and Units
(subject to funding) to facilitate multi-disciplinary learning meetings such as
Cancer and Cardiology MDM and Project Echo.
Emergency Departments
The Emergency Departments in the Southern Trust continue to face exponential
pressure. Best practice in other EDs across the UK is being researched and
there may be potential for technology enabled improvements such as patient self
triage, data control rooms and patient tracking. These investigations continue in
collaboration with the ED Management team. This may require a business case
and funding support in 2016/17.
GP Out of Hours

36
Like ED, GP OOH continue to face significant pressure. Investigations continue
with telephony and video conferencing to try to facilitate consultations from GPs
own homes, or across Trust sites. Conceptual ideas are being discussed with
OPPC Directorate. This may require a business case and funding support in
2016/17.
8.6 Summary of Funding Confirmed & Funding Gaps
In summary, the funding confirmed at December 2015, for 2015/16 for ICT is as
follows:
Table 8.6.1 ICT Funding Confirmed
Capital Funding Source Amount Confirmed
CRL £340,000
HSCB Ring fenced Tranche 1 £1,280,000
HSCB Ring fenced Tranche 2 £340,000
HSCB Ring fenced Tranche 3 £900,000
TOTAL £2,860,000
In summary, the funding gaps which exist and will be pursued for either slippage
or new funding opportunities in 2016/17 are as follows:
Table 8.6.2 ICT Funding Gap
Category Capital funding
gap
Revenue
Requirement
Extension of PARIS Community
Information System implementation
(business case submitted to DHSSPS)
£750,000 per
annum for 3
years
None
ICT Infrastructure £1,198,000 None

37
Service Development Proposals £1,876,800 £202,150
Regional Access To IT (excluded -
Regional business case)
£7,140,510 £1,601,850
TOTAL £3,824,800 £202,150
This excludes the potential Electronic Health and Care Record (EHCR) and also
those potential ICT service improvements outlined in section 8.5. Every
opportunity will be taken to bid for slippage funding or against 2016/17 budgets to
address this gap.
9.0 CONCLUSION
The financial context in the HSCNI continues to bring challenges for ICT
implementation and support in the Southern Trust. This Business Plan identifies
these challenges but also outlines the significant progress that has been made in
progressing ICT improvements, despite this. It also provides an opportunity to
bid for slippage funding for service developments that have not yet been funded
and prepares us for bidding against new budgets in 2016/17.

















