Identification and Identification and Ablation of Ablation of Epicardial VT Epicardial VT Yi-Gang Li, MD Yi-Gang Li, MD Xinhua Hospital, Shanghai Jiaotong Xinhua Hospital, Shanghai Jiaotong University University
Transcript
Identification and Identification and
Ablation of Epicardial VTAblation of Epicardial VT
• Mapping data inability to identify the reentry circuit isthmus on the endocardium by entrainment mapping• Identification of a focal point of earliest endocardial activation, entrainment indicates an exit or outer loop site, but abl. fails to interrupt VT
Identification of Epicardial VTIdentification of Epicardial VT
Mapping data in absence of SHD (LVOT?)
• Mapping data within CS and accessible LV branches suggest an epicardial VT circuit or focus
Identification of Epicardial VTIdentification of Epicardial VT
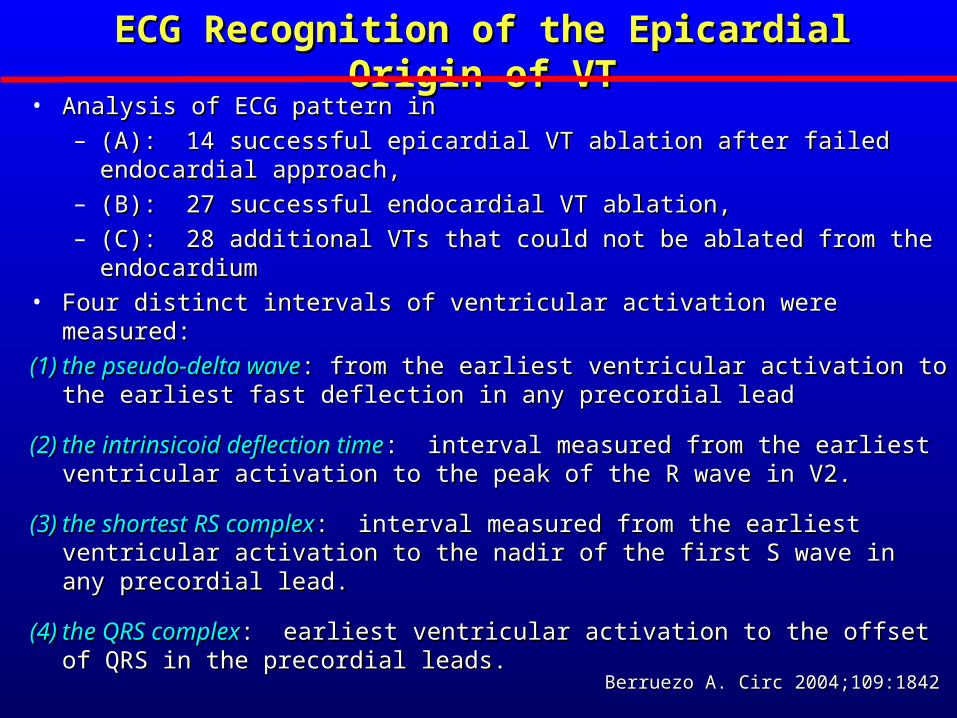
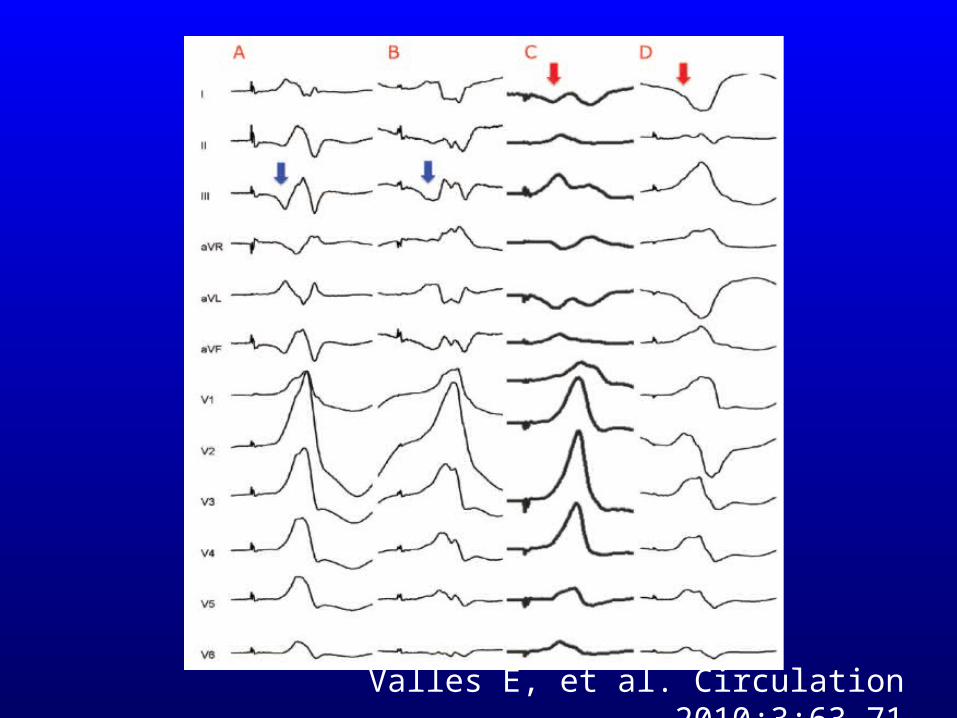
ECG Recognition of the Epicardial Origin of VTECG Recognition of the Epicardial Origin of VT• Analysis of ECG pattern inAnalysis of ECG pattern in
– (A): 14 successful epicardial VT ablation after failed endocardial (A): 14 successful epicardial VT ablation after failed endocardial approach,approach,
– (B): 27 successful endocardial VT ablation,(B): 27 successful endocardial VT ablation,– (C): 28 additional VTs that could not be ablated from the endocardium(C): 28 additional VTs that could not be ablated from the endocardium
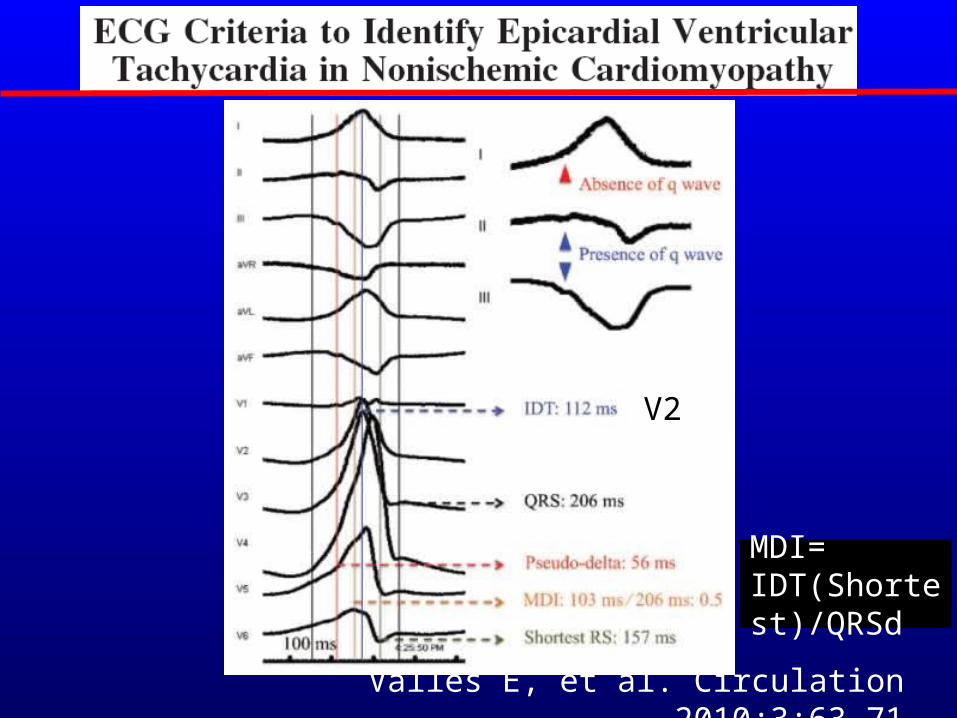
• Four distinct intervals of ventricular activation were measured:Four distinct intervals of ventricular activation were measured:
(1)(1) the pseudo-delta wavethe pseudo-delta wave: from the earliest ventricular activation to the : from the earliest ventricular activation to the earliest fast deflection in any precordial leadearliest fast deflection in any precordial lead
(2)(2) the intrinsicoid deflection timethe intrinsicoid deflection time: interval measured from the earliest : interval measured from the earliest ventricular activation to the peak of the R wave in V2.ventricular activation to the peak of the R wave in V2.
(3)(3) the shortest RS complexthe shortest RS complex: interval measured from the earliest ventricular : interval measured from the earliest ventricular activation to the nadir of the first S wave in any precordial lead.activation to the nadir of the first S wave in any precordial lead.
(4)(4) the QRS complexthe QRS complex: earliest ventricular activation to the offset of QRS in the : earliest ventricular activation to the offset of QRS in the precordial leads.precordial leads.
Berruezo A. Circ 2004;109:1842Berruezo A. Circ 2004;109:1842
Groups A & C (unsuccessful endocardial ablation) showed
longer intrinsicoid deflection in V2,
slurred initial part of QRS(pseudo wave)
vs
Group B (endocardially ablated VT)
Berruezo A. Circ 2004;109:1842Berruezo A. Circ 2004;109:1842
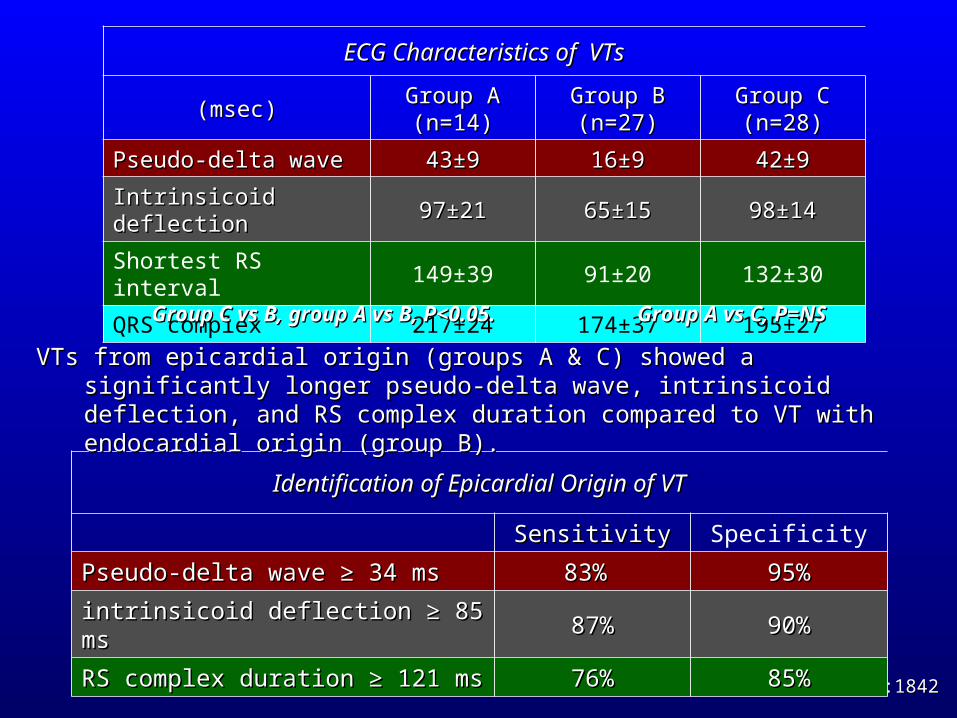
Identification of Epicardial Origin of VTIdentification of Epicardial Origin of VT
SensitivitySensitivity Specificity
Pseudo-delta wave Pseudo-delta wave ≥≥ 34 ms 34 ms 83% 83% 95%95%
intrinsicoid deflection intrinsicoid deflection ≥≥ 85 ms 85 ms 87%87% 90%90%
RS complex duration RS complex duration ≥≥ 121 ms 121 ms 76%76% 85%85%
ECG Characteristics of VTsECG Characteristics of VTs
Group C vs B, group A vs B, P<0.05. Group C vs B, group A vs B, P<0.05. Group A vs C, P=NSGroup A vs C, P=NS
VTs from epicardial origin (groups A & C) showed a significantly longer pseudo-delta VTs from epicardial origin (groups A & C) showed a significantly longer pseudo-delta wave, intrinsicoid deflection, and RS complex duration compared to VT with wave, intrinsicoid deflection, and RS complex duration compared to VT with endocardial origin (group B).endocardial origin (group B).
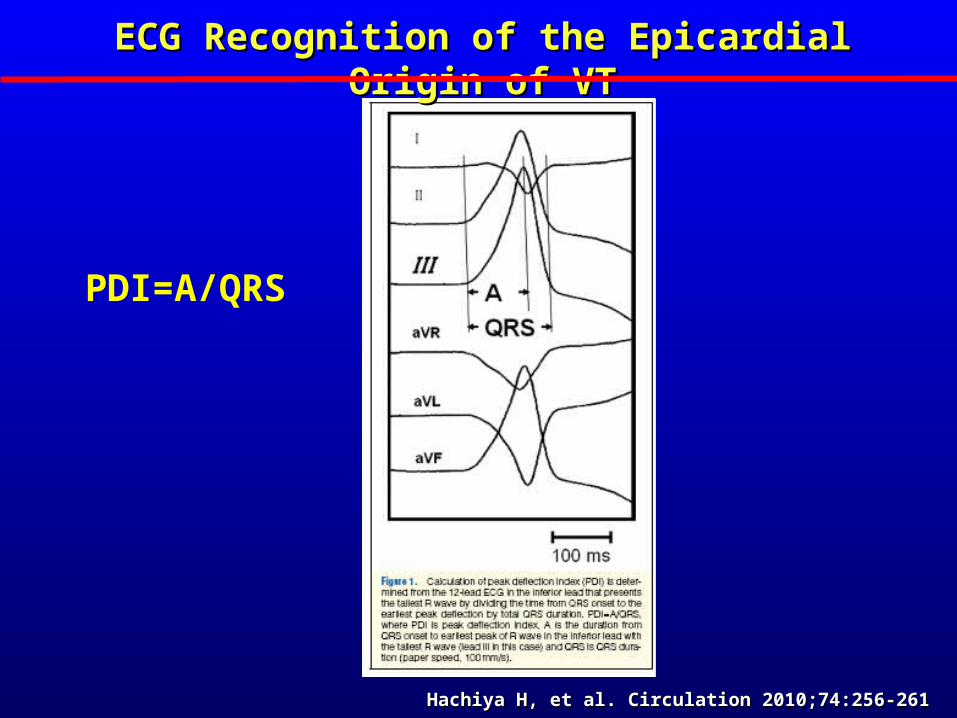
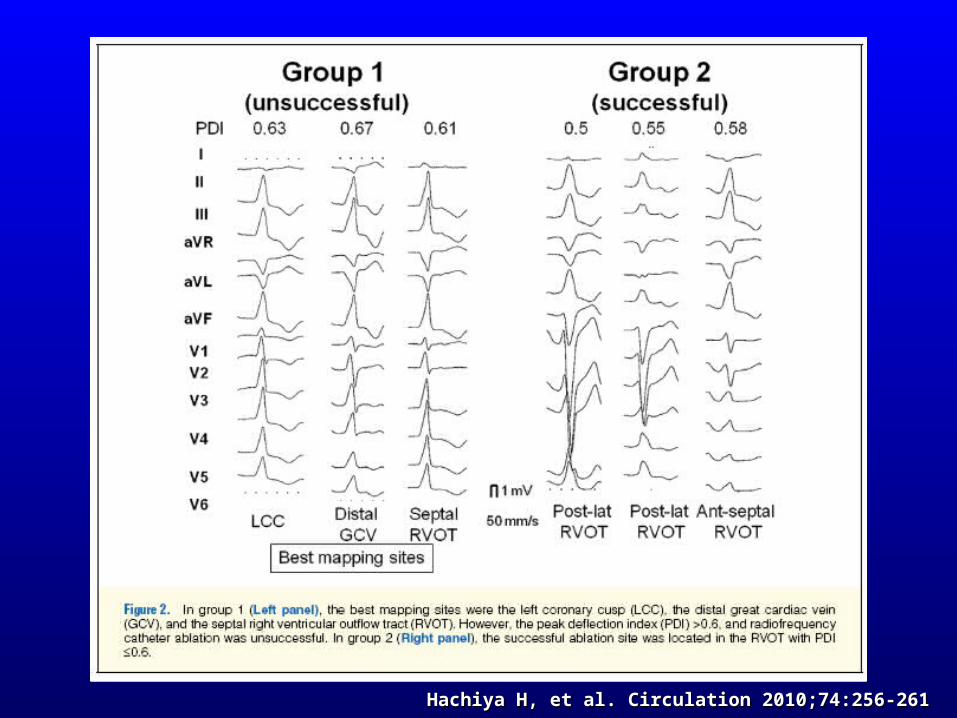
PDI=A/QRS
Hachiya H, et al. Circulation 2010;74:256-261Hachiya H, et al. Circulation 2010;74:256-261
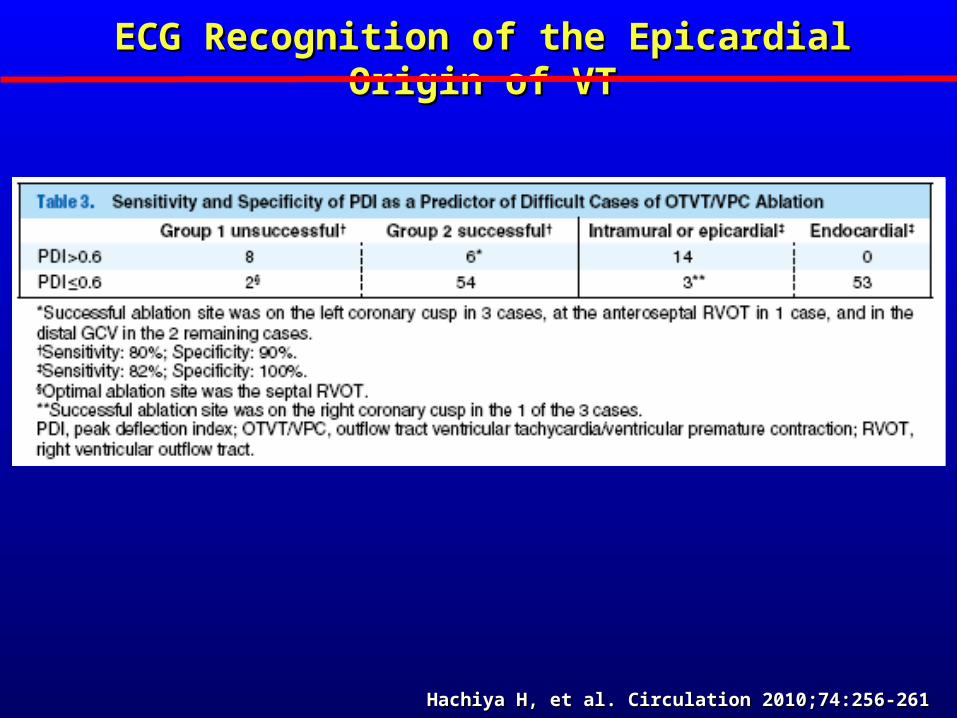
ECG Recognition of the Epicardial Origin of VTECG Recognition of the Epicardial Origin of VT
Hachiya H, et al. Circulation 2010;74:256-261Hachiya H, et al. Circulation 2010;74:256-261
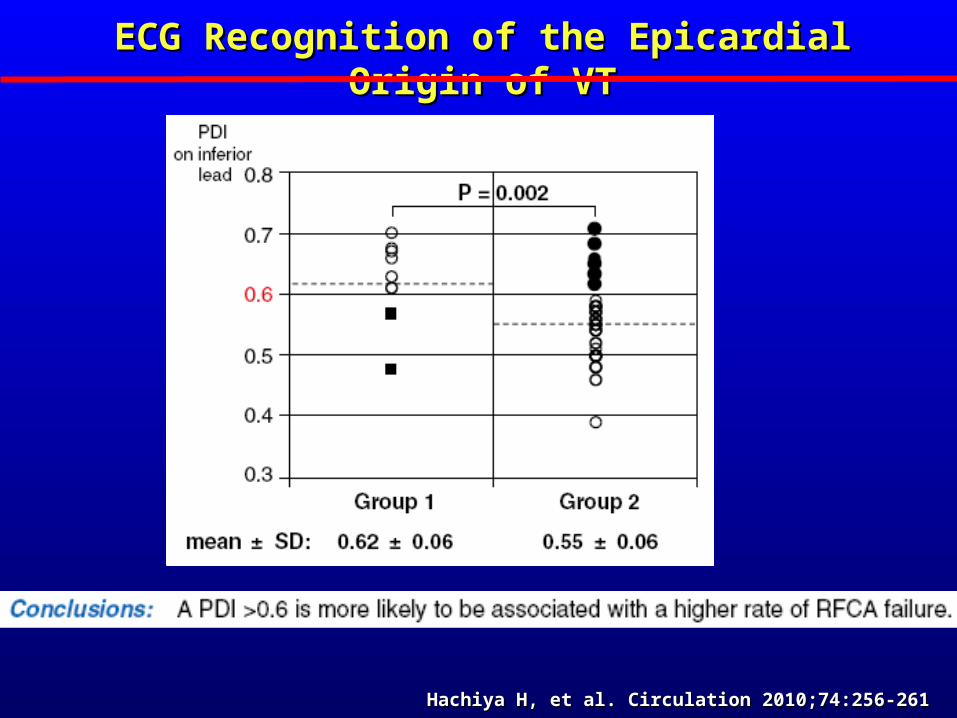
ECG Recognition of the Epicardial Origin of VTECG Recognition of the Epicardial Origin of VT
Hachiya H, et al. Circulation 2010;74:256-261Hachiya H, et al. Circulation 2010;74:256-261
Hachiya H, et al. Circulation 2010;74:256-261Hachiya H, et al. Circulation 2010;74:256-261
ECG Recognition of the Epicardial Origin of VTECG Recognition of the Epicardial Origin of VT
Valles E, et al. Circulation 2010;3:63-71
V2
MDI=IDT(Shortest)/QRSd
Valles E, et al. Circulation 2010;3:63-71
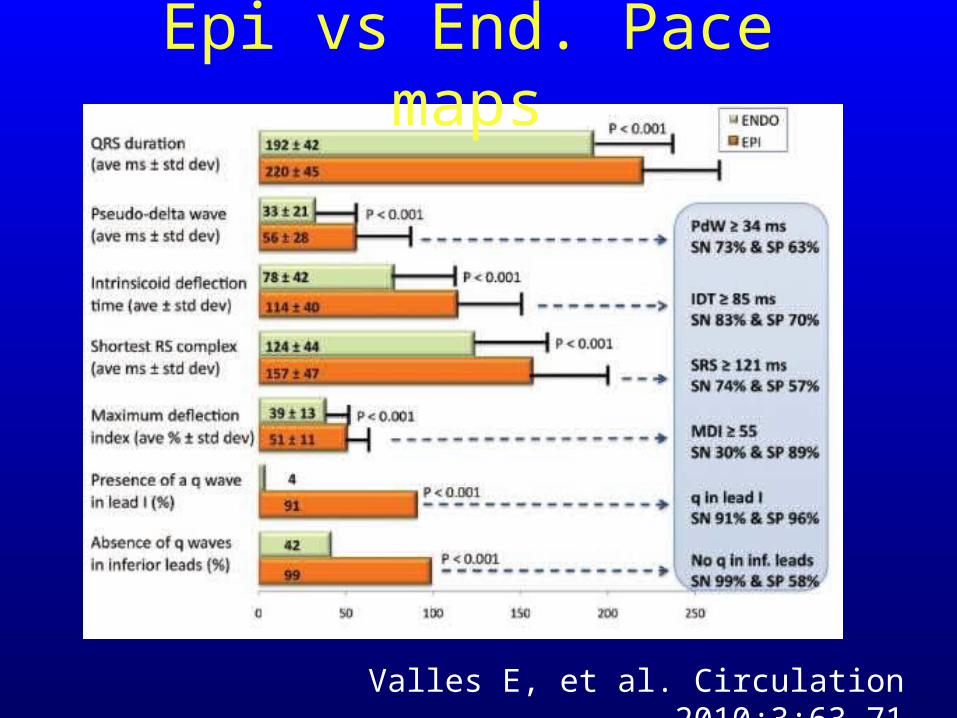
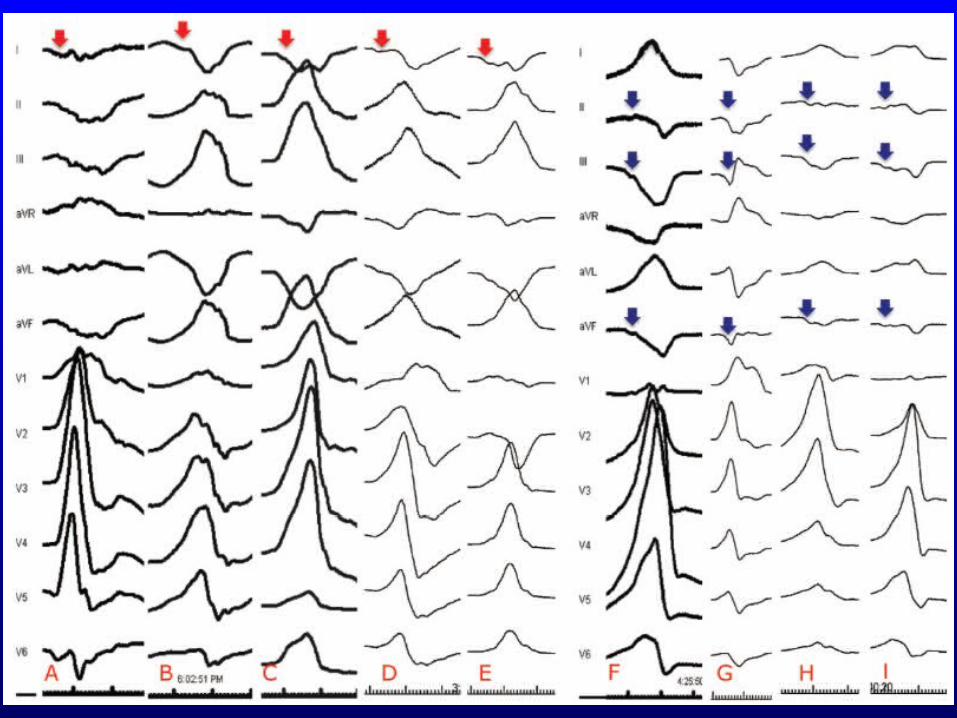
Epi vs End. Pace maps
Valles E, et al. Circulation 2010;3:63-71
Valles E, et al. Circulation 2010;3:63-71
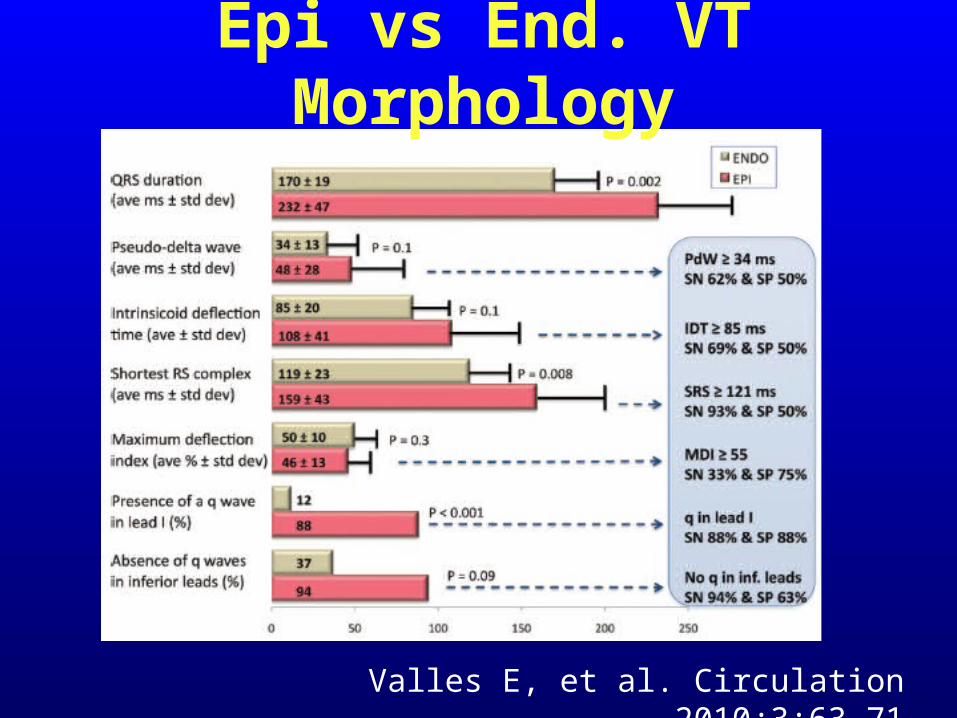
Epi vs End. VT Morphology
11 Pts, 21 VTs
from basal superior or lateral origin
Valles E, et al. Circulation 2010;3:63-71
ECG Recognition of the Epicardial Origin of VTECG Recognition of the Epicardial Origin of VT
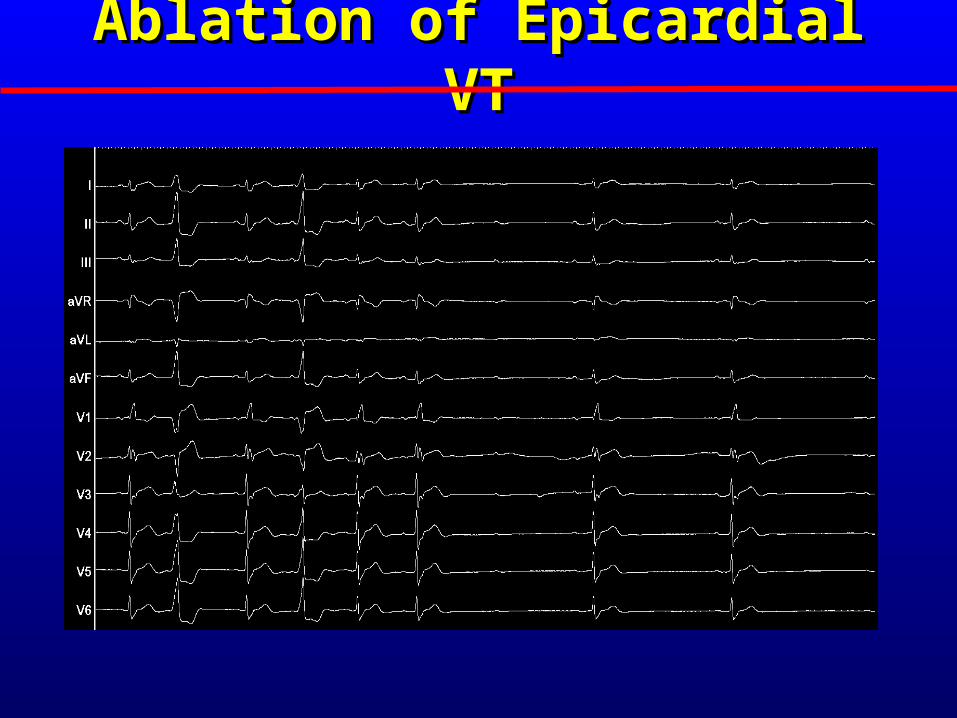
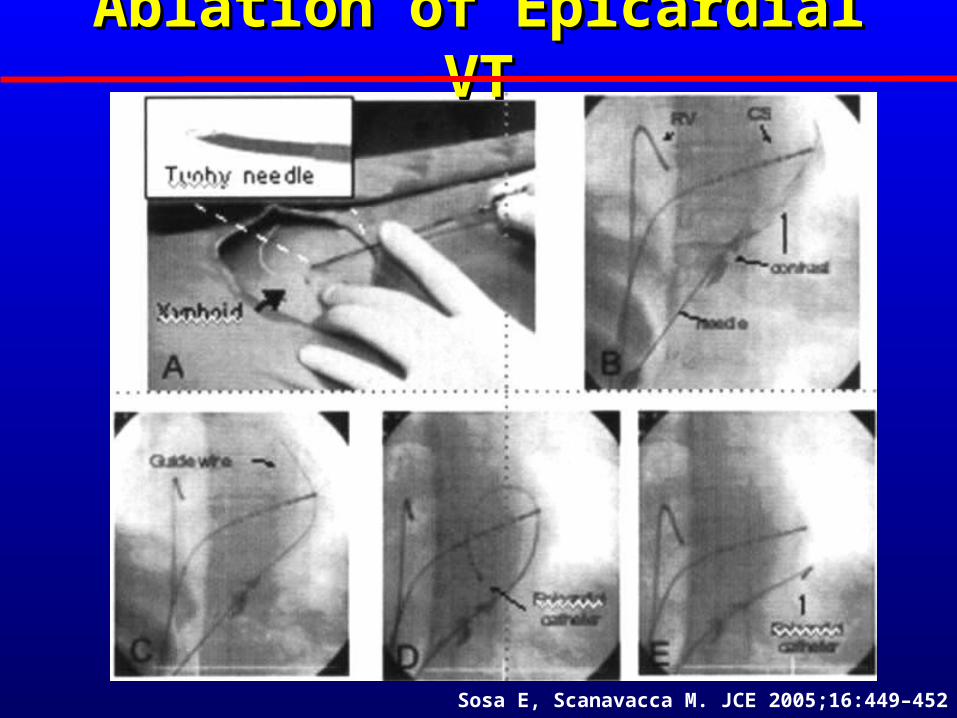
Ablation of Epicardial VTAblation of Epicardial VT
Sosa E, Scanavacca M. JCE 2005;16:449–452
Ablation of Epicardial VTAblation of Epicardial VT
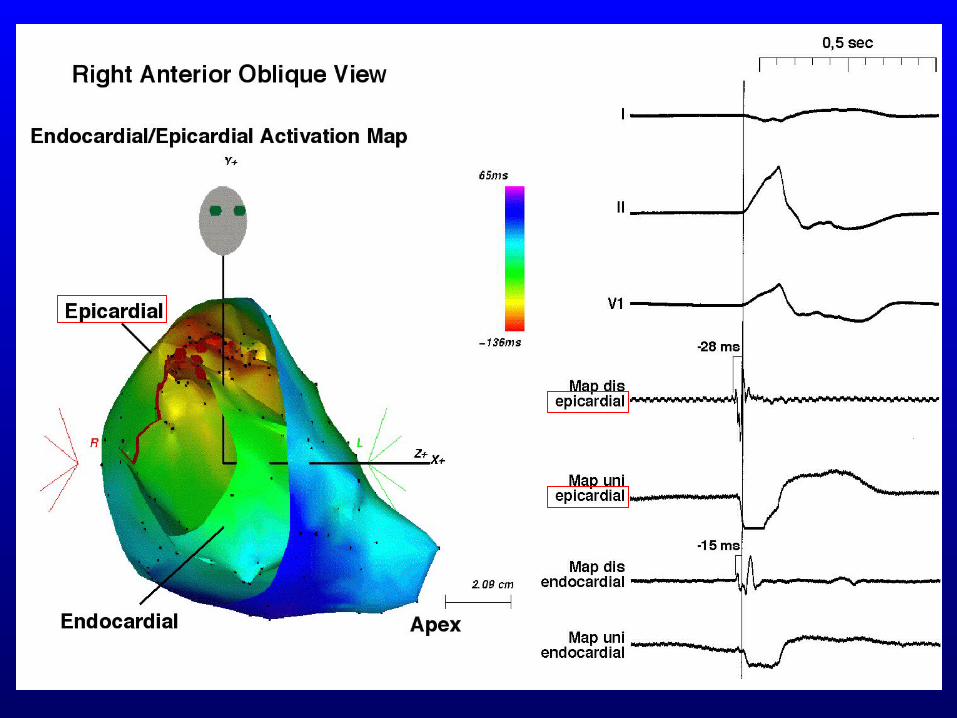
• Mapping of the epicardium can be performed
using fluoroscopy and/or CARTO system.
• Areas of infarction or scar have low amplitude
electrograms similar to findings during
endocardial mapping.
• Epicardial fat may create low amplitude
regions.
- Inability to capture during epicardial
pacing
- High pacing tresholds: Epicardial fat;
difficult catheter stability
Mapping of Epicardial VTMapping of Epicardial VT
• Mapping using conventional or Navi-Star Catheter
(Biosense-Webster)
• Internally or externally irrigated catheter can be
used for RF ablation to avoid high impedance
• Power limit of 50 W with temperature limit of 45ºC,
infusion rate of 17 ml/min and duration of 110 sec
• Aspiration of pericardial fluid after 5 RF
applications to prevent fluid accumulation
Mapping and Ablation of Mapping and Ablation of Epicardial VTEpicardial VT
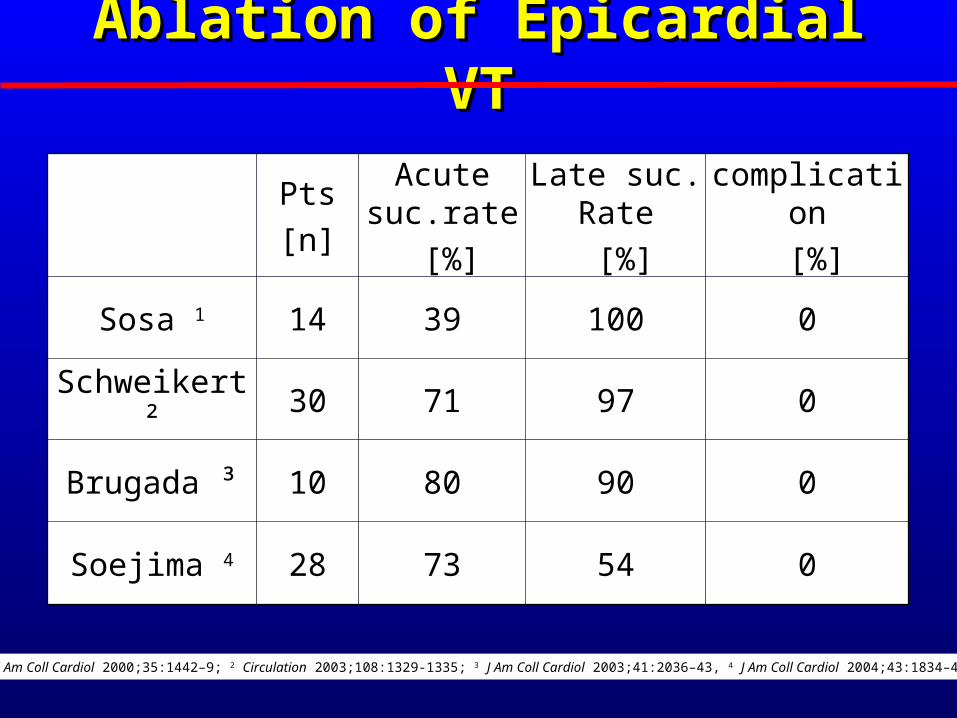
Ablation of Epicardial VTAblation of Epicardial VT
Pts
[n]
Acute suc.rate
[%]
Late suc. Rate
[%]
complication
[%]
Sosa 1 14 39 100 0
Schweikert ² 30 71 97 0
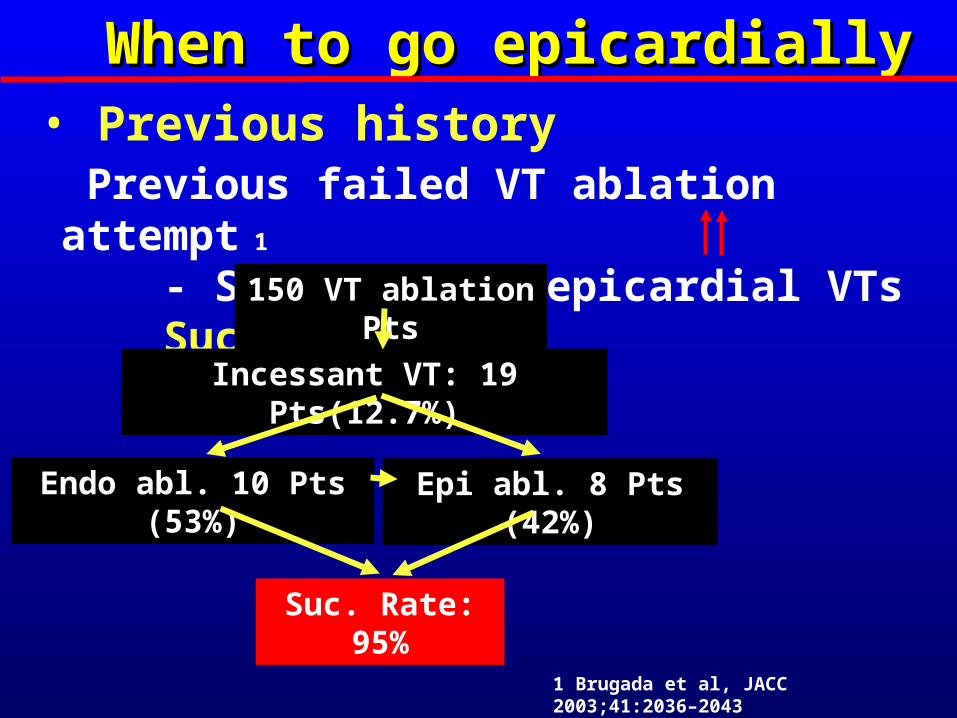
Brugada ³ 10 80 90 0
Soejima 4 28 73 54 0
1 J Am Coll Cardiol 2000;35:1442–9; 2 Circulation 2003;108:1329-1335; 3 J Am Coll Cardiol 2003;41:2036–43, 4 J Am Coll Cardiol 2004;43:1834–42
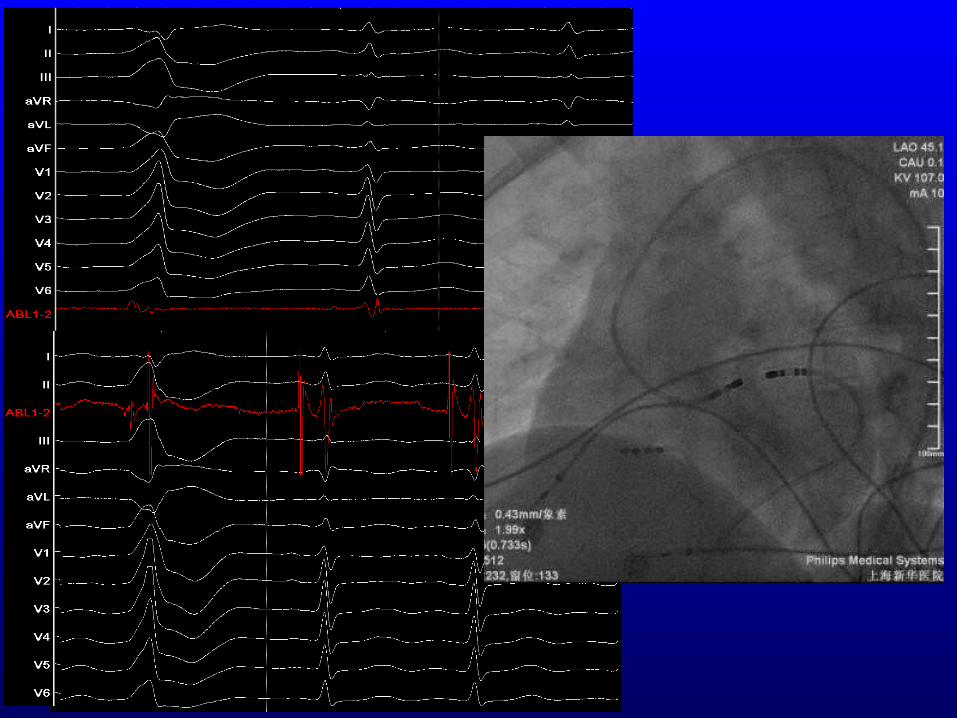
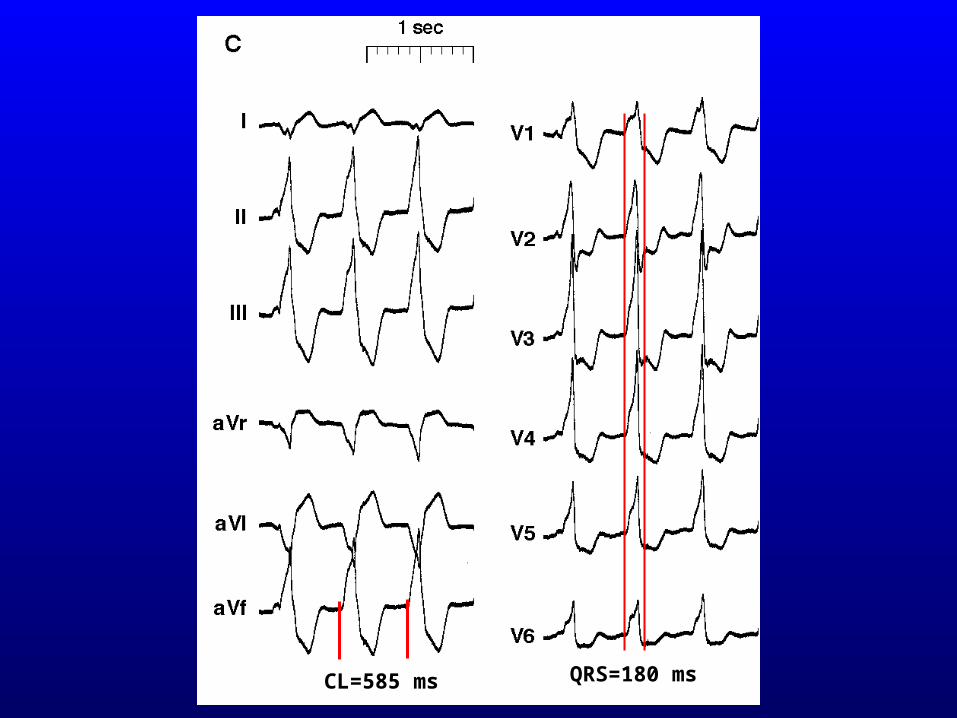
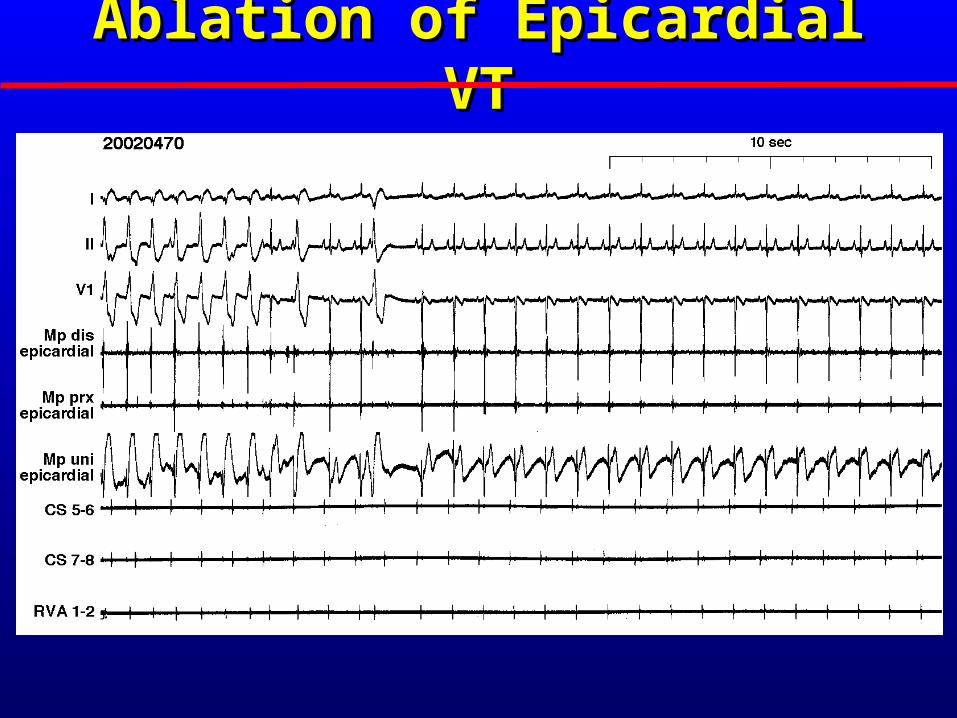
QRS=180 msCL=585 ms
Ablation of Epicardial VTAblation of Epicardial VT
Phrenic nerve injury
• Pacing shoud be performed before energy
delivery to indenify phrenic nerve capture,
indicating where ablation might cause
diaphragmatic paralysis.
• phrenic nerve injury can be avoided by:
- interposing a sheath,baloon, or even air in the
pericardium between the abl. Site and the
nerve.
ComplicationsComplications
• Coronary nerve injury
- Coronary angiography before RF ablation
- Requiring a minimum of 4 mm between
epicardial coronary vessels and the ablation
catheter.
- the catheter is not touching the vessel at any
point of cardiac cycle
• Pericartitis
- mild, limited duration, often responds well to
anti-inflammatory medication
ComplicationsComplications
• Epicardial mapping will not prevent all VT abl.
failures.
- Tachycardia circuits can originate from deep
within the ventricular septum/myocardium, may
require transcoronary ethanol ablation, or
irrigated needle catheters.
• Ablaion can be limmited by
- epicardial fat,
- proximity to coronary arteries and other other
stuctures
Problems in eProblems in epicardial ablation ablation
Conclusion
• Epicardial VT can be identify by previous history, present clinical data and surface ECG
• Mapping data and cardiac Image facilitate VT ablation
• Epicardial VT is rare, but it can be either focal