IEE COMPUTING & CONTROL DIVISION: CHAIRMAN'S ADDRESS Some aspects of computers in medicine R.W.Sutton, B.Sc, C.Eng., F.I.E.E. Indexing terms: Computer applications, Instrumentation and measuring science, Microprocessors, Ultrasonics Abstract: The field of medicine is one which offers considerable scope for the application of computers ranging from simple microprocessors to sophisticated array processors. To illustrate these applications a number of examples have been chosen in diagnosis, therapy, patient monitoring and patient mangagement. The first two examples relate to diagnostic equipment, the operation of which would not be possible without an integral computer, namely the now well established X-ray c.t. scanner and the recently developed nuclear magnetic resonance scanner which promises to be an equally important diagnostic tool. From the increasing range of microprocessor applications three examples have been chosen, the kidney machine, Doppler ultra- sound for blood flow measurement, and real-time ultrasound. Images play an important role in medical diagnosis, and it is shown how computer based techniques developed for other applications can be used to improve the quality of these images and so aid diagnosis. Computers are also being used more extensively to maintain patient records, particularly of treatments and their effects, information which is particularly valuable in medical research. Much monitoring equipment in the intensive care situation is now beginning to. incorporate microprocessors allowing more automatic operation and recording. Finally it is indicated how work in the field of expert systems could, by close collaboration between computer scientist and clinician, lead to improved clinical diagnosis. 1 Introduction When commercial digital computers first became available about 30 years ago, it was believed that only relatively few such machines would be required to satisfy the computa- tional needs of the UK. These early machines, which were physically large, used thermionic valves and required regular preventative maintenance. Typical of such machines was the DEUCE computer, which was based on the pilot model ACE developed at the NPL, and which had 384 words of mercury delay-line storage and 8192 words of magnetic-drum storage together with single- and double-word delay lines serving as registers. Since the machine was primarily intended for scientific calculations the word length was 32 bits. These machines were slow and had to be programmed in machine code. They were also expensive, costing around £40 000. Compare this with a typical microcomputer system of today which is contained on a single printed-circuit board and had 32 kbytes of random-access memory and 8192 words of read-only memory for storage of programs and fixed data. Such a system has a word length of only 16 bits but is about three orders of magnitude faster, can be pro- grammed in a high-level language and costs less than £2000. The dramatic decrease in the cost of computer power which has taken place largely over the past few years with the introduction of the microprocessor has opened up potential for the rapid expansion of computer applications. It is unfortunate that by and large the media have concen- trated attention on the likely impact on employment of these developments and ignored the real benefits that can accrue from the availability of low-cost computing power. The field of medicine is one where the whole range of computer power can be, and indeed in many cases is being, used to improve the standards of diagnosis and treatment of disease without decreasing the need for the skills of Paper 996A, delivered before the IEE Computing & Control Division, 7th October 1980 Mr. Sutton is with the Hirst Research Centre, The General Electric Co. Ltd., East Lane, Wembley, Middx. HA9 7PP, England 26 0143-702X/81/010026 + 09 $01-50/0 highly trained clinical and nursing staff. The range of applications is so great that it is possible to deal only with a few examples to illustrate what can be done. From the viewpoint of computer applications in medicine, five key areas can be identified, namely diagnosis (identification of a diseased state), therapy (treatment of disease), prothesis (supply of an artificial part of the body to replace one which is deficient), monitoring and patient management. It is appropriate to start by considering two types of medical diagnostic equipment whose operation would not be possible without the use of a computer as an integral part of the system. 2 X-ray c.t. scanning The first of these, the X-ray c.t. scanner, which was first introduced in 1972 as a result of the work of Godfrey Hounsfield at EMI, enabled X-rays to be used successfully for the first time to study soft tissue, initially in the head. Since that time many other scanners have been developed and their use has proved invaluable particularly in study of tumours in the brain and examination of head injuries. Their use has also been extended to whole-body examina- tions. The basic principle of the scanner is quite simple and is illustrated in Fig. 1. A narrow beam of X-rays is passed through the patient's head or body, and the radiation not absorbed is detected by, for example, a sodium iodide crystal. The detected signal is amplified, digitised and stored in the computer memory. The X-ray source and detector are scanned linearly across the patient, many values of X-ray absorption being stored during this scan. The scanning mechanism is then rotated through a small angle and the linear scan repeated, and so on until the scan has been rotated through 180°. By this time many thousands of values of absorption along the X-ray beams will have been stored, these data relating to an axial slice through the patient of thickness ranging from 5 to 10 mm. Several slices may be required for a complete examination. A grey-scale image, generally of 256 by 256 pixels of IEE PROCEEDINGS, Vol 128, Pt. A, No. 1, JANUARY 1981
Transcript
IEE COMPUTING & CONTROL DIVISION: CHAIRMAN'S ADDRESS
Some aspects of computers in medicineR.W.Sutton, B.Sc, C.Eng., F.I.E.E.
Indexing terms: Computer applications, Instrumentation and measuring science, Microprocessors, Ultrasonics
Abstract: The field of medicine is one which offers considerable scope for the application of computersranging from simple microprocessors to sophisticated array processors. To illustrate these applications anumber of examples have been chosen in diagnosis, therapy, patient monitoring and patient mangagement.The first two examples relate to diagnostic equipment, the operation of which would not be possible withoutan integral computer, namely the now well established X-ray c.t. scanner and the recently developed nuclearmagnetic resonance scanner which promises to be an equally important diagnostic tool. From the increasingrange of microprocessor applications three examples have been chosen, the kidney machine, Doppler ultra-sound for blood flow measurement, and real-time ultrasound. Images play an important role in medicaldiagnosis, and it is shown how computer based techniques developed for other applications can be used toimprove the quality of these images and so aid diagnosis. Computers are also being used more extensively tomaintain patient records, particularly of treatments and their effects, information which is particularlyvaluable in medical research. Much monitoring equipment in the intensive care situation is now beginning to.incorporate microprocessors allowing more automatic operation and recording. Finally it is indicated howwork in the field of expert systems could, by close collaboration between computer scientist and clinician,lead to improved clinical diagnosis.
1 Introduction
When commercial digital computers first became availableabout 30 years ago, it was believed that only relatively fewsuch machines would be required to satisfy the computa-tional needs of the UK.
These early machines, which were physically large, usedthermionic valves and required regular preventativemaintenance. Typical of such machines was the DEUCEcomputer, which was based on the pilot model ACEdeveloped at the NPL, and which had 384 words of mercurydelay-line storage and 8192 words of magnetic-drumstorage together with single- and double-word delay linesserving as registers. Since the machine was primarily intendedfor scientific calculations the word length was 32 bits.
These machines were slow and had to be programmed inmachine code. They were also expensive, costing around£40 000.
Compare this with a typical microcomputer system oftoday which is contained on a single printed-circuit boardand had 32 kbytes of random-access memory and 8192words of read-only memory for storage of programs andfixed data. Such a system has a word length of only 16 bitsbut is about three orders of magnitude faster, can be pro-grammed in a high-level language and costs less than £2000.
The dramatic decrease in the cost of computer powerwhich has taken place largely over the past few years withthe introduction of the microprocessor has opened uppotential for the rapid expansion of computer applications.It is unfortunate that by and large the media have concen-trated attention on the likely impact on employment ofthese developments and ignored the real benefits that canaccrue from the availability of low-cost computing power.
The field of medicine is one where the whole range ofcomputer power can be, and indeed in many cases is being,used to improve the standards of diagnosis and treatmentof disease without decreasing the need for the skills of
Paper 996A, delivered before the IEE Computing & ControlDivision, 7th October 1980Mr. Sutton is with the Hirst Research Centre, The General ElectricCo. Ltd., East Lane, Wembley, Middx. HA9 7PP, England
26
0143-702X/81/010026 + 09 $01-50/0
highly trained clinical and nursing staff. The range ofapplications is so great that it is possible to deal only with afew examples to illustrate what can be done.
From the viewpoint of computer applications inmedicine, five key areas can be identified, namely diagnosis(identification of a diseased state), therapy (treatment ofdisease), prothesis (supply of an artificial part of the bodyto replace one which is deficient), monitoring and patientmanagement.
It is appropriate to start by considering two types ofmedical diagnostic equipment whose operation would notbe possible without the use of a computer as an integralpart of the system.
2 X-ray c.t. scanning
The first of these, the X-ray c.t. scanner, which was firstintroduced in 1972 as a result of the work of GodfreyHounsfield at EMI, enabled X-rays to be used successfullyfor the first time to study soft tissue, initially in the head.Since that time many other scanners have been developedand their use has proved invaluable particularly in study oftumours in the brain and examination of head injuries.Their use has also been extended to whole-body examina-tions.
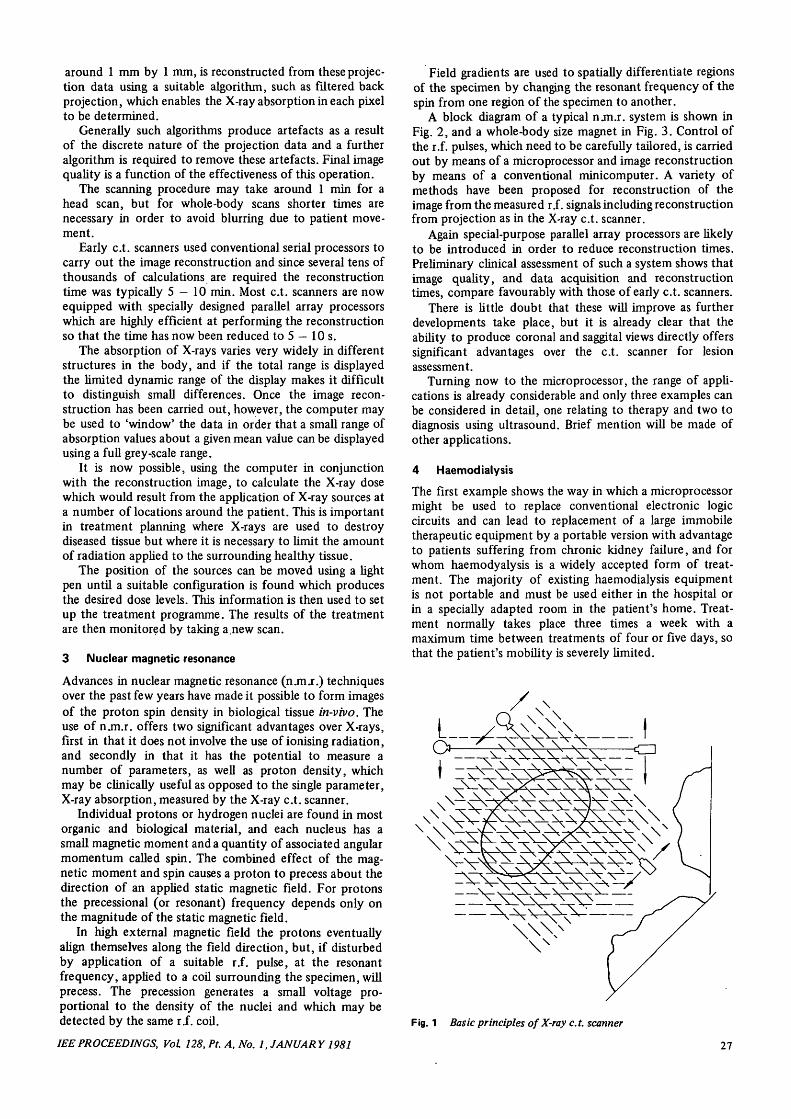
The basic principle of the scanner is quite simple and isillustrated in Fig. 1. A narrow beam of X-rays is passedthrough the patient's head or body, and the radiation notabsorbed is detected by, for example, a sodium iodidecrystal. The detected signal is amplified, digitised andstored in the computer memory. The X-ray source anddetector are scanned linearly across the patient, manyvalues of X-ray absorption being stored during this scan.
The scanning mechanism is then rotated through a smallangle and the linear scan repeated, and so on until the scanhas been rotated through 180°. By this time many thousandsof values of absorption along the X-ray beams will havebeen stored, these data relating to an axial slice through thepatient of thickness ranging from 5 to 10 mm. Several slicesmay be required for a complete examination.
A grey-scale image, generally of 256 by 256 pixels of
IEE PROCEEDINGS, Vol 128, Pt. A, No. 1, JANUARY 1981
around 1 mm by 1 mm, is reconstructed from these projec-tion data using a suitable algorithm, such as filtered backprojection, which enables the X-ray absorption in each pixelto be determined.
Generally such algorithms produce artefacts as a resultof the discrete nature of the projection data and a furtheralgorithm is required to remove these artefacts. Final imagequality is a function of the effectiveness of this operation.
The scanning procedure may take around 1 min for ahead scan, but for whole-body scans shorter times arenecessary in order to avoid blurring due to patient move-ment.
Early c.t. scanners used conventional serial processors tocarry out the image reconstruction and since several tens ofthousands of calculations are required the reconstructiontime was typically 5 — 10 min. Most c.t. scanners are nowequipped with specially designed parallel array processorswhich are highly efficient at performing the reconstructionso that the time has now been reduced to 5 — 10 s.
The absorption of X-rays varies very widely in differentstructures in the body, and if the total range is displayedthe limited dynamic range of the display makes it difficultto distinguish small differences. Once the image recon-struction has been carried out, however, the computer maybe used to 'window' the data in order that a small range ofabsorption values about a given mean value can be displayedusing a full grey-scale range.
It is now possible, using the computer in conjunctionwith the reconstruction image, to calculate the X-ray dosewhich would result from the application of X-ray sources ata number of locations around the patient. This is importantin treatment planning where X-rays are used to destroydiseased tissue but where it is necessary to limit the amountof radiation applied to the surrounding healthy tissue.
The position of the sources can be moved using a lightpen until a suitable configuration is found which producesthe desired dose levels. This information is then used to setup the treatment programme. The results of the treatmentare then monitored by taking a.new scan.
3 Nuclear magnetic resonance
Advances in nuclear magnetic resonance (njnj.) techniquesover the past few years have made it possible to form imagesof the proton spin density in biological tissue in-vivo. Theuse of n jn.r. offers two significant advantages over X-rays,first in that it does not involve the use of ionising radiation,and secondly in that it has the potential to measure anumber of parameters, as well as proton density, whichmay be clinically useful as opposed to the single parameter,X-ray absorption, measured by the X-ray c.t. scanner.
Individual protons or hydrogen nuclei are found in mostorganic and biological material, and each nucleus has asmall magnetic moment and a quantity of associated angularmomentum called spin. The combined effect of the mag-netic moment and spin causes a proton to precess about thedirection of an applied static magnetic field. For protonsthe precessional (or resonant) frequency depends only onthe magnitude of the static magnetic field.
In high external magnetic field the protons eventuallyalign themselves along the field direction, but, if disturbedby application of a suitable xS. pulse, at the resonantfrequency, applied to a coil surrounding the specimen, willprecess. The precession generates a small voltage pro-portional to the density of the nuclei and which may bedetected by the same r.f. coil.
IEEPROCEEDINGS, Vol 128, Pt. A, No. 1, JANUARY 1981
Field gradients are used to spatially differentiate regionsof the specimen by changing the resonant frequency of thespin from one region of the specimen to another.
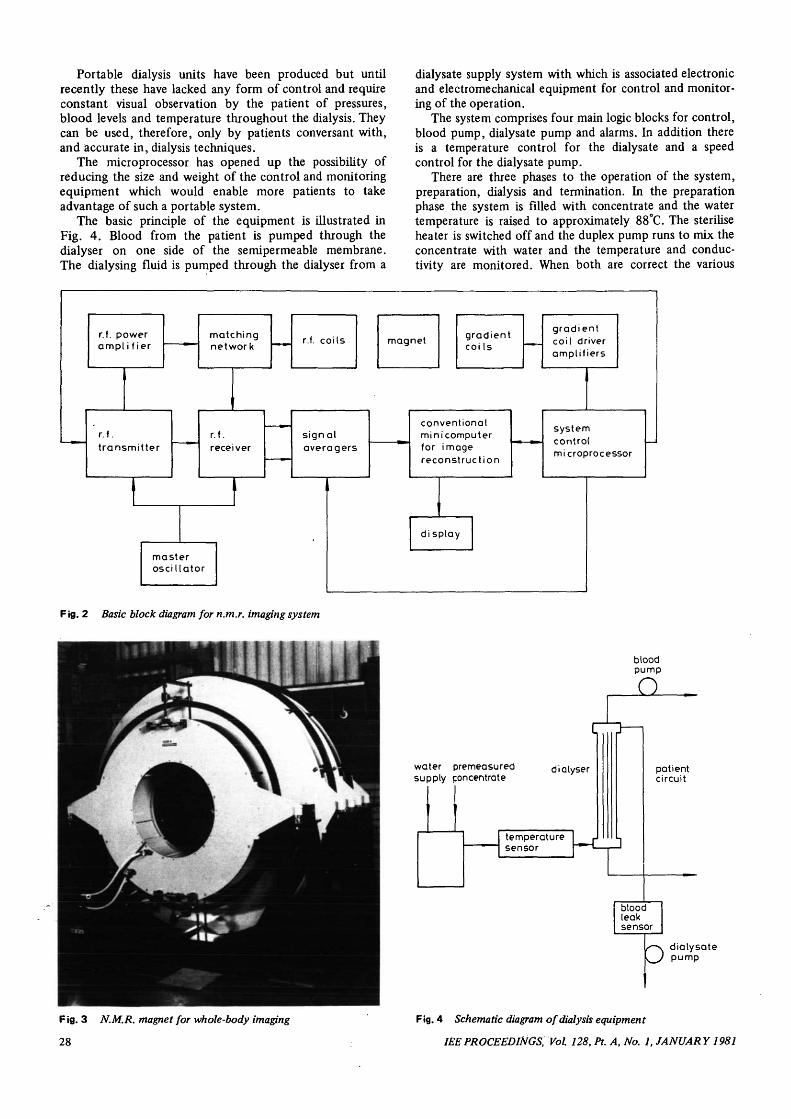
A block diagram of a typical n jn.r. system is shown inFig. 2, and a whole-body size magnet in Fig. 3. Control ofthe r.f. pulses, which need to be carefully tailored, is carriedout by means of a microprocessor and image reconstructionby means of a conventional minicomputer. A variety ofmethods have been proposed for reconstruction of theimage from the measured r.f. signals including reconstructionfrom projection as in the X-ray c.t. scanner.
Again special-purpose parallel array processors are likelyto be introduced in order to reduce reconstruction times.Preliminary clinical assessment of such a system shows thatimage quality, and data acquisition and reconstructiontimes, compare favourably with those of early c.t. scanners.
There is little doubt that these will improve as furtherdevelopments take place, but it is already clear that theability to produce coronal and saggital views directly offerssignificant advantages over the c.t. scanner for lesionassessment.
Turning now to the microprocessor, the range of appli-cations is already considerable and only three examples canbe considered in detail, one relating to therapy and two todiagnosis using ultrasound. Brief mention will be made ofother applications.
4 Haemodialysis
The first example shows the way in which a microprocessormight be used to replace conventional electronic logiccircuits and can lead to replacement of a large immobiletherapeutic equipment by a portable version with advantageto patients suffering from chronic kidney failure, and forwhom haemodyalysis is a widely accepted form of treat-ment. The majority of existing haemodialysis equipmentis not portable and must be used either in the hospital orin a specially adapted room in the patient's home. Treat-ment normally takes place three times a week with amaximum time between treatments of four or five days, sothat the patient's mobility is severely limited.
Fig. 1 Basic principles of X-ray c.t. scanner
27
Portable dialysis units have been produced but untilrecently these have lacked any form of control and requireconstant visual observation by the patient of pressures,blood levels and temperature throughout the dialysis. Theycan be used, therefore, only by patients conversant with,and accurate in, dialysis techniques.
The microprocessor has opened up the possibility ofreducing the size and weight of the control and monitoringequipment which would enable more patients to takeadvantage of such a portable system.
The basic principle of the equipment is illustrated inFig. 4. Blood from the patient is pumped through thedialyser on one side of the semipermeable membrane.The dialysing fluid is pumped through the dialyser from a
dialysate supply system with which is associated electronicand electromechanical equipment for control and monitor-ing of the operation.
The system comprises four main logic blocks for control,blood pump, dialysate pump and alarms. In addition thereis a temperature control for the dialysate and a speedcontrol for the dialysate pump.
There are three phases to the operation of the system,preparation, dialysis and termination. In the preparationphase the system is filled with concentrate and the watertemperature is raised to approximately 88°C. The steriliseheater is switched off and the duplex pump runs to mix theconcentrate with water and the temperature and conduc-tivity are monitored. When both are correct the various
r.f. powerampl i f ier
matchingnetwork
r.f.transmitter
r.f. coils magnet gradientcoi Is
gradientcoil driveramplifiers
r.f.receiver
signalaveragers
masteroscillator
conventionalminicomputerfor imagereconstruction
systemcontrolmicroprocessor
display
Fig. 2 Basic block diagram for n.m.r. imaging system
bloodpump
O
water premeasuredsupply concentrate
diatyser patientcircuit
bloodleaksensor
3 dialysatepump
Fig. 3 N.M.R. magnet for whole-body imaging
28
Fig. 4 Schematic diagram of dialysis equipment
IEE PROCEEDINGS, Vol. 128, Pt. A, No. 1, JANUAR Y1981
alarms are tested and the patient is connected to the bloodlines.
The machine can then enter the dialysis phase duringwhich the dialysate pressure, conductivity and temperatureare monitored together with venous and arterial pressures.Checks are also made to ensure that there are no air bubblesin the blood line and that blood is not leaking through thedialyser. The emphasis throughout is on the safety of thepatient and should any problems arise with air bubbles orblood leaks the blood pump is stopped and dialysis dis-continued.
After dialysis the machine is put in the terminate modeduring which the blood is washed back into the patientusing a saline solution and the machine then rinsed out withwater at about 88°C.
In collaboration with the Renal Unit at the Royal FreeHospital, the four main logic blocks on a standard dialysatesupply system have been replaced with a single-board 8-bitmicrocomputer with associated analogue to digital convertorand a suitable interface. Similarly control of temperatureand of dialysate pump speed could be carried out in themicroprocessor. This equipment has been successfullydemonstrated in a short clinical trial.
The computer program to execute the necessary logicfunctions occupies 3 kbytes of programmable read-onlymemory. A significant reduction in physical size is achieved,but there is probably very little cost reduction over theconventional digital logic. The programmable capabilitydoes, however, allow greater flexibility in matching themachine to patient requirements and makes possible theaddition of new control and logic functions.
5 Diagnostic ultrasound
5.1 Blood-flow measurement
The Doppler principle can be used to monitor the flow ofblood in major veins and arteries. The simplest Dopplerdevice, a continuous wave device, is shown in block diagramform in Fig. 5. A continuous beam of ultrasound is pro-jected into the body from a transducer on the end of aprobe. Ultrasound backscattered from within the body isreceived on a second transducer mounted in the same probe.The ultrasound from moving scatterers such as blood cellsis shifted in frequency by an amount proportional to thevelocity of the cells.
The Doppler shift frequency is extracted by mixing thereceived and transmitted signals and since this frequency isnormally in the audio range it is usual to listen to this signalon headphones or loudspeaker. The frequency can also beindicated on a frequency meter.
oscillator amplifier
probe
/ / blood cell
loudspeakerorheadphones
frequencymeter
beam f = 2 v ">s9
F ig. 5 Block diagram of continuous-wave flow detector
IEEPROCEEDINGS, Vol 128, Pt. A, No. 1, JANUARY 1981
F ig. 6 Doppler ultrasound equipmen t for blood-flow measuremen t
Two difficulties arise with this type of instrument.First it is not possible to determine the blood velocityquantitatively since the relationship between frequency andvelocity is dependent on the angle between the ultrasoundbeam and the direction of blood flow which is normallyparallel to the vessel axis.
Secondly the c.w. instrument is sensitive to blood flowat all points within the ultrasound beam. If, as is frequentlythe case, there are two vessels within the beam, the Dopplersignal is a mixture of signals from both. It is often difficult,therefore, to obtain signals from an artery without con-tamination by signals from an accompanying vein.
Even the Doppler signal from a single vessel is a mixtureof signals of different frequencies corresponding with thedifferent streamline velocities that exist within the vessel.
To resolve these difficulties it is necessary to obtaininformation at different distances along the beam, and thisis achieved by using a pulsed or range-gated system in whichshort bursts of ultrasound are transmitted periodically.
Furthermore, since the flow in arteries is pulsatile innature, it is necessary to determine the Doppler frequenciesat intervals throughout the cardiac cycle.
An instrument has been developed which enables thenecessary calculations to be carried out, and this is shownin Fig. 6. Originally designed to utilise the Doppler principlein order to image veins and arteries, this equipment hasbeen extended by the addition of two microprocessorsystems to provide quantitative data on blood flow.
This equipment, which uses pulsed Doppler and has 30range gates enabling information to be obtained at depthintervals of less than 1 mm, is shown in block-diagram formin Fig. 7. The ultrasound probe is attached to the arm of aposition resolving mechanism. A position computer com-bines the information from the position resolver with thesample volume depth information from the pulse Doppler
29
system. When the sample volume is within a blood vesseland a Doppler signal is present, a correctly positioned imageof the sample volume is intensified and stored on the screenof a colour monitor. The direction of flow is also detectedand the image is coloured red for flow in one direction andblue for flow in the other direction. The position gives thethree Cartesian co-ordinates of each sampling volume, anytwo of which can be selected for display on the monitor.This enables cross-section, lateral or anterior/posteriorviews to be displayed.
The angle between the ultrasound beam and the vessel isdetermined by collecting data from two cross-sectionalscans taken a short distance on either side of the point ofinterest as shown in Fig. 8. From this the co-ordinates ofthe centroids of the two scans can be calculated and theorientation of the vessel determined. A third cross-sectionalscan taken at the point of interest is used to determine theorientation of the beam, thus enabling the beam/vesselangle to be computed.
A bit-slice microprocessor is used to process the datafrom the different range-gates in order to obtain the firstmoment integral and power of the Doppler spectra whichare used to calculate the mean Doppler frequency. Thisprocess is carried out over a number of time intervals
probepositionresolver
probey c// y
imoqes ofskin
vein s'(£/' / ^ ^ v e i n
, / ultrasound beam arteryartery '
F ig. 7 Block diagram of imaging system
storage c.r.t.
v e s s e l a x i s
d e t e c t e d f l o w p o i n t s
F ig. 8 Illustration of method of beam/vessel angle measurement
30
— Skin
F ig. 9 Typical results from carotid artery scan
throughout the cardiac cycle, and the e.c.g. R-wave is usedto control the timing of the data acquisition which alsoneeds to be averaged over a number of cardiac cycles.
The calculations associated with angle measurement arecarried out in a single board microprocessor which alsoperforms several other functions, principally to calculatethe velocity from mean frequency and angle, the flow byintegration of the velocity profile over the vessel diameter,the vessel width from the Doppler power profile and meanblood velocity.
These calculations are performed for the data in eachtime slot throughout the cardiac cycle in order to givecomplete information on the flow.
In addition to these basic calculations, a number ofimportant corrections have to be applied to the raw data,and the final data have to be smoothed before display. Theseprocedures are also performed by the same microprocessor.
A typical result obtained from a carotid artery examina-tion is shown in Fig. 9. The procedure can be used as ameans of screening for potential stroke since ultrasound hasno harmful effects at the power levels required.
5.2 Ultrasonic imaging
Ultrasonic pulse echo equipment is used increasingly invarious areas of medical diagnosis because it is cheap,compact, safe and very effective for visualising soft tissueand its motion. It is now widely used in obstetrics to avoidX-ray hazard, in cardiology, tumour diagnosis, cardiovascu-lar investigations and paediatrics.
Until recent years ultrasonic images have been formedusing static B-mode (brightness mode) scanning withpulse-echo information in the forms of range and brightness,to represent the amplitude of the echoes. The component
IEEPROCEEDINGS, Vol 128, Pt. A, No. 1, JANUARY 1981
parts of such a system are shown in Fig. 10. As the ultra-sonic transducer is moved to scan different paths within thepatient, the direction of the scan line on the display ismoved to correspond with the direction of the ultrasonicbeam, as derived from a mechanical position sensing scanarm. The echoes received at the transducer are amplifiedwith a swept gain to compensate for the increasing attenua-tion of echoes from deeper structures. Demodulation of thereceived rS. signal produces the amplitude of the echowhich is used to brightness-modulate the scan line. Thecomplete B-mode scan is built up by storing all the lines toform a 2-dimensional display or 'slice' through the patient(tomogram). The time to make a scan is long, comparedwith the heart cycle for example, and blurring can thereforeoccur.
In obstetrics it is usual to measure the biparietaldiameter and the crown-rump length using a system ofelectronically controlled calipers. These parameters providemeasures of foetal growth. The introduction of micro-processors will enable additional information on growth tobe obtained from measures of circumference, area andvolume, which will enable the weight of the foetus to beestimated. This type of measurement could also be usefulin staging tumour masses and in determination of heartchamber volumes.
Thus the microprocessor enables clinically usefulquantitative data to be obtained directly, and this can bedisplayed to the clinician alongside the image and recordedwith it by photographing the display.
t.v. monitor
storage
control
transmitter
Fig. 10 Schematic diagram of typical static B-mode scanner
Real-time is a variant of B-mode scanning with themanual scan replaced by a rapid mechanical or electronicscan. The advantages are two-dimensional visualisation ofmoving structures, rapid location of the organ of interest,no mechanical linkage and reduced image-storage require-ments. The essential features of an electronic linear real-time scanner are shown in Fig. 11. The transducer consistsof a large number of small transducer elements arranged ina linear array. The elements are operated in a small subgroupas shown, and scanningis achieved by electronically steppingthis subgroup, one element at a time, along the completearray. Increasing the number of elements in the subgroupimproves the lateral resolution in the far field of the trans-ducer but degrades it in the near field. Electronic focusingof the transmitted beam, by introducing appropriate delaysinto the pulsing circuits of elements of the subgroup, canbe used to improve near-field lateral resolution.
Static B-scanners originally used analogue scan convertortubes, but these are now being superseded by microproces-sor-controlled digital scan convertors. Microprocessors arebeing introduced into real-time B-scanners for control ofthe scan, replacing digital logic and giving greater flexibilityof operation, and for simple image-processing operationswhich will be discussed later.
IEEPROCEEDINGS, Vol. 128, Pt. A, No. 1, JANUARY 1981
demodulatorultrasoundbeampath
display
raster
controlvideo
demodulator
transmitter
electronicallycontrolled switches
multielementtransducermm
| active group
Iultrasound beampath
Fig. 11 Schematic diagram of electronic real-time scanner system
Typical scans of the foetal skull obtained using a real-time B-scanner are shown in Figs. 12 and 13.
6 Image processing
The use of data windowing described above is one form ofimage processing that has been successfully applied tomedical diagnostic equipment. A wide range of techniqueshave been developed, particularly for military and space
F ig. 13 Digitised image of foetal skull at 30 weeks, clearly showingeye sockets and other facial features
Fig. 14 Smoothing to remove noise
applications, and very spectacular results have been achievedin the processing of pictures from the moon.
These include edge enhancement, pattern recognition,texture analysis, feature extraction and smoothing toreduce high-frequency noise. Although these techniquescan, in principle, be applied to medical images derived fromultrasound, X-ray or similar equipment there is always thedanger that they may introduce artefacts or unduly enhancefeatures which detract from the clinical value of the originaldata.
However a texture analysis approach to chest X-radio-graphs has permitted the successful diagnosis of lung disease,and it is possible that the technique could be more widelyapplied, for example, to ultrasound images.
Medical images generally have a low signal/noise ratioand are of poor quality. The noise may result from eitherthe detection process or be generated in the associatedelectronic equipment, and as a result important diagnosticfeatures may be obscured. The effects of high-frequencynoise may be reduced by means of smoothing or by addingtogether several noisy images of the same object.
An example of the way in which smoothing improvesimage quality is shown in Fig. 14. In this example theoriginal object has a uniform intensity and the noise has amean of 0-75 and a standard deviation of 0-354 comparedwith the original object intensity. After smoothing thenoise mean it is reduced to 0-625 with a standard deviationof 0-228.
The effect of adding together four frames of a noisypicture is illustrated in Fig. 15. In each frame the noisehas a mean level of 1 -5 compared with the wanted signal,and it is quite difficult to identify the image from anysingle frame. After summation the noise has a mean levelof 1-0 and the image becomes quite clear. Adding framestogether in this way reduces the noise by a factor of yJNwhere N is the number of frames, this reduction resultingfrom the random nature of the noise as compared with thefixed image.
A further problem with medical images, which wasimportant in early c.t. scanners due to the long scan timesinvolved, is blurring of the image owing to movementeither as a result of the patient's breathing or, in the case ofcardiovascular studies, owing to the action of the heart.
The nature of the problems involved can be furtherillustrated by an example of edge detection applied to anultrasound scan of the carotid artery. Image discontinuities
32 IEEPROCEEDINGS, Vol 128, Pt. A, No. 1, JANUARY 1981
F ig. 15 Removal of noise by adding frames
are accentuated by means of a spatial operator and theedge-enhanced picture thresholded to produce a binarydisplay. The original carotid artery scan is first smoothedby interpolating between lines and between points alonglines and then the edge-detection algorithm applied withthe result shown in Fig. 16.
It is seen that, although the technique works well in anideal case, when it is applied to a noisy image many spuriousedge points result and further 'cleaning' is required toproduce a satisfactory edge picture.
As is the case with the c.t. scanner very large amounts ofdata have to be processed in order to carry out any image-processing procedure, and this is very time consuming on asequential computer. It is likely, therefore, that parallel-array processing will be necessary if reasonable computationtimes are to be achieved.
Even so the present cost of such systems mean that theycan only be used in conjunction with higher-cost equipmentand will not find their way into ultrasonic equipment unlessor until the same dramatic cost reductions occur in arrayprocessors that resulted from the introduction of the micro-processor.
7 Patient management
Computers have been widely applied to the problems ofpatient management and record keeping in hospitals. Someof the earliest systems, implemented on large expensivemultiuser machines proved unsuccessful and were aban-doned. Not only were these systems costly to acquire, runand maintain, they suffered also from being overambitiousattempts at integrated hospital computing.
In spite of these early setbacks many useful systems arenow in use, and these will undoubtedly grow as more atten-tion is paid to the needs of the user. These are, basically,first that it should be easy to enter data and to look upstored information, and secondly that the system shallrespond rapidly to requests.
Development in word-processing equipment with easy touse features for modification of data by correction, insertionor deletion; the exploitation of the tree structure of view-data which gives access to substantial databases usingsimpler single-key instructions; special keyboards allowingeasy entry of key words or the use of light pens, trackerballs or touch wires to select from a 'menu'; and, in the
Fig. 16 Edge-extraction process
longer term, developments in voice and optical-characterrecognition can all lead to computer-based systems whichare more acceptable to the medical profession.
Another area of patient management where computer-based systems are proving of value is in research. One suchsystem based on the use of ANSI standard MUMPS hasbeen in use for about two years for the study of breast-cancer patients at the Royal Marsden Hospital. A detailedfile is created which includes information about bio-chemistry, radiotherapy, haematology, histopathology,nuclear medicine, pharmacology, diagnostic radiology,surgery and a general clinical file, the data being entered viaa standard v.d.u.
It is possible to collate data about diagnosis, therapy,aetiology and prognosis for any required group of patients.Analyses of patient data are now becoming possible whichwere previously ruled out by the sheer work of extractingfrom notes which are often incomplete, unintelligible oreven missing.
8 Intensive care
Another area where microprocessors are finding increasingapplication is in units devoted to coronary care andresuscitation where heart rate, respiration, fluid intake,urine output, blood gases etc. have to be continuouslymonitored and controlled. Traditionally, specialised instru-ments have only been able to provide indication ofabnormally high or abnormally low conditions.
The addition of microprocessors to such instrumentationenables more sophisticated criteria of abnormality to beintroduced by indicating trends as well as absolute values,and by correlation of more than one parameter.
Much undoubtedly needs to be done in order to determinewhich information is of the greatest clinical value, but thebasic tools are now available at a cost which makes theiradoption an economically viable proposition.
9 Expert systems
Developments have been taking place over the past decadeor so in so called 'expert systems', as a result of researchinto artificial intelligence.
A number of examples exist of the application of suchsystems in medical diagnosis as well as in the interpretationof mass spectra, and in oil exploration. As yet there does
IEEPROCEEDINGS, Vol 128, Pt. A, No. 1, JANUARY 1981 33
not appear to be very widespread acceptance of such sys-tems, but they will undoubtedly play an increasinglyimportant role.
Such expert systems may be regarded as being essentiallyrule driven, the rules being of the IF . . . . THEN . . . . form.Typical examples are the work of Shortliffe Medical Schoolwhich resulted in MYCIN, and of Feigenbaum at StanfordUniversity on PUFF.tions and meningitis injections and the recommendation ofdrug treatment. PUFF is concerned with the diagnosis ofpulmonary function disorders, and uses the shell of theMYCIN system.
Both PUFF and MYCIN are relatively simple backward-chaining inference systems which, in the case of MYCIN,enables the user to ask questions such as 'why' and 'how'in order to expose the line of reasoning.
The key feature of such systems is that they are de-veloped from a close liaison between the specialist clinicianor group of clinicians and computer scientists. The know-ledge bearing rules originate from and are tested by theclinician. Much of this knowledge is often largely heuristicand is private to the expert in the sense that he may beunable readily to share it with others. The role of thecomputer scientist is a twofold one. First to help the expertto uncover his knowledge in the form of rules, and secondlyto provide the basic computer language, an 'advice language'which must be designed for the 'manipulation of rule-oriented knowledge bases in such a way as to enable non-computer-minded clinical experts freely to exchangedescriptive concepts with the system and thus to improvethe quantity and quality of its stored knowledge'.
The state-of-the-art is such that languages of the MYCINtype are being reimplemented to be usable on relativelysmall minicomputer systems. Even so such systems arestill likely to have a cost which limits their general availa-bility.
Furthermore the applications so far studied have dealtwith relatively small diagnostic areas and there is at presentlittle indication that a more widely based diagnostic systemis feasible, and the time taken to produce a system may notbe trivial for overworked clinicians. The development of
PUFF took about 50 h of interaction with the clinicalexpert and 10 man-weeks of effort by computer scientists.
We are clearly in the early stages of the development ofsuch systems but they do appear to offer considerableadvantages over other types of computer based system withrespect of their ease of use.
10 Conclusion
It has only been possible to consider a few examples of theway in which computers are leading towards improved andmore reliable medical diagnosis. Many more could havebeen cited which will have an important role to play inthe advancement of medical techniques.
Whatever the role of the computer, be it in instrumenta-tion, in patient management or as an aid in decision making,one thing is abundantly clear, i.e. that the system must beacceptable to medical personnel. For this reason it isessential that all such developments take place in closeliaison with the medical profession, for without this thecleverest and most sophisticated system will fail.
This is particularly so in the case of the aids to decisionmaking where the great attraction of the expert systemapproach is that it lends itself to implementation andenhancement of the system by the doctor and not by thecomputer expert.
At least one major obstacle seems to remain to widerapplication of computers other than in instruments, andthis is the vexed question of input and output. Operatingsystems requiring sophisticated commands typed on con-ventional keyboards present untold difficulties to themedical profession whose time is valuable and who areoften working under extreme pressure.
In the case of patient management simple structuressuch as that used by viewdata could help in reducing theproblem, as could special keyboards which provide alimited vocabulary of key words.
In the somewhat longer term it is possible that voiceinput could be developed to the point where it providesa cheap and accurate method of inputting clinical data.
34 TEE PROCEEDINGS, Vol 128, Pt. A, No. 1, JANUARY 1981