THE NATIONAL MEDICAL JOURNAL OF INDIA VOL.2, NO.3 119
IgG ELISA for invasive amoebiasis in endemic areasNANDINI SHETTY, T. PRABHU
ABSTRACTAn IgG ELISA was evaluated as a serological test for thediagnosis of invasive amoebic disease in an endemic area.Sixteen patients with proven amoebic dysentery, 22 withsuspected amoebic dysentery and 21 with amoebic liverabscesses were studied. Control subjects were 26asymptomatic amoebic cyst passers, 13 patients withgiardiasis, 26 with enteric fever and 31 individuals with noevidence of parasitic infestation.
The mean optical density (OD) value of the negativecontrols + 2 standard deviations (SD) was taken as thecut-off point to differentiate seropositive from seronega-tive individuals. It was found that all patients withamoebic liver abscesses had diagnostically raised IgGtitres with specificity and sensitivity rates of 60.5% and100% respectively; 25% of the patients with proven and50% with suspected amoebiasis had positive antibodyvalues with specificity and sensitivity rates of 50% and25% respectively. Among the control subjects only 4(15%) asymptomatic cyst passers, 4 (31%) patients withgiardiasis, 3 (11%) of those with enteric fever and 5(16%) of individuals without parasite infestation wereseropositive.
The results of this study indicate that the IgG ELISAoften provides equivocal results in cases of amoebicdysentery in endemic areas. However, specific IgG titresare significantly raised and of value in the diagnosis ofpatients clinically suspected to have an amoebic liverabscess.
INTRODUCTIONDetection of IgG antibodies against Entamoeba histoLyticaantigens is routinely used to diagnose amoebiasis, particu-larly invasive amoebic diseases. Of the various serologicalmethods used, enzyme-linked immunosorbent assay(ELISA) is the most sensitive and specific. However, itsvalue in the diagnosis of amoebic disease has only beenreported from non-endemic areas. As IgG antibodiestend to persist in the circulation for long periods, theirdetection in patients with symptoms in an endemic zonemay not provide evidence of active infestation. The pre-sent study evaluates the diagnostic efficacy of the IgGELISA test in patients suffering from invasive amoebicdisease in two large hospitals in an endemic area.
St. John's Medical College, Bangalore 560034, IndiaNANDINI SHErrY, T. PRABHU Department of Microbiology
MATERIALS AND METHODSPatientsPatients suspected to have both invasive and non-invasiveamoebic disease admitted to the Victoria Hospital and theSt. John's Medical College Hospital, Bangalore wereincluded in the study. The patients who had amoebicdysentery (n=16) and amoebic liver abscess (n=21)were considered to have invasive amoebic disease whileasymptomatic E. histoLytica cyst passers (n=26) were con-sidered to have non-invasive amoebiasis, Other groups ofpatients included diseased controls, namely, patients whohad cysts of Giardia LambLia detected in their stools(n=13), and patients who had enteric fever (n=26). Inaddition, 31 persons without any overt intestinal diseaseand without any evidence of helminthic infestation(confirmed by microscopic examination of their stools)were also included. Twenty-two patients with clinicallysuspected amoebic dysentery, which could not be sub-stantiated by repeated microscopic examination of thestool, were also included in the study.
Diagnostic criteriaAmoebic Liver abscess (ALA): Patients were diagnosed tohave ALA if they presented with tender hepatomegalywith or without fever, with ultrasonographic demonstra-tion of a space-occupying lesion in the liver from whichsterile pus was aspirated and who responded to standardantiamoebic drugs such as metronidazole.
Amoebic dysentery: Patients with amoebic dysenterywere those who had large bowel diarrhoea, with sigmoido-scopic evidence of colonic or rectal mucosal inflammationand demonstration of haematophagous E. histoLytica inthe stool.
Amoebic cyst passers: Asymptomatic cyst passers werethose who had E. histoLytica cysts in their stools but nointestinal symptoms.
The other patient groups were those in whose stools,cysts or trophozoites of Giardia lamblia weredemonstrated, and patients with enteric fever who had apositive Widal test with or without positive blood culturesfor SaLmonella typhi.
MethodsStooL examination for amoebic trophozoites: Faecal sam-ples from patients suspected to have amoebic dysenterywere subjected to staining techniques to determine thepresence of haematophagous trophozoites as indicators ofinvasive disease. All specimens were initially subjected towet mount screening techniques using 0.85% sodium
120
chloride, D' Antoni's iodine and buffered methyleneblue.' Thereafter all samples were preserved in 10 to 12 mlof a polyvinyl alcohol preservative and fixative solution'and subjected to two permanent staining procedures: thetrichrome stain and the short iron haematoxylin methodof Spencer and Monroe. 1 An average of 4 to 8 permanentstained slides were screened from each faecal specimen.
/gG Elisa for amoebic antibody: Crude soluble antigen(CSA) was obtained froin a sonicate of the NIH: 200axenic strain of E. histolytica. The antigen was providedby the Department of Parasitology, National Institute ofCholera and Enteric Diseases, Calcutta, India. Theoptimum protein concentration of the antigen used was 20lLg/ml, obtained by a preliminary titration.?
The procedure adopted for the micro ELISA wasessentially that of Yang and Kennedy- with a few modifi-cations. Appropriately diluted CSA of E. histolytica incarbonate-bicarbonate buffer (0.05 M, pH 9.6) was usedto coat polyvinyl ELISA plates (Dynatech, USA). Afterovernight incubation at 4°C the plates were washed with0.85% saline which contained 0.05% Tween20 (SigmaChemicals, USA). Every serum sample was tested induplicate using a single serum dilution of 1:200, thediluent contained bovine serum albumin (BSA) to blocknon-specific protein binding. Each ELISA plate was runwith two wells in which the following reagents had beenomitted-successive pairs of the wells had no antigen,antibody or conjugate and two wells were charged withsubstrate only. These controls served as blanks and werecorrected for non-specific protein binding. Besides these,known positive and negative controls were also incorpo-rated into each plate. Antihuman IgG conjugated horse-radish peroxidase in a 1:1000 dilution (Sigma Chemicals,USA) was used to detect specific human IgG to E. his-tolytica antigen using ortho-phenylene diamine (OPD) asthe substrate. The colour intensity at the end of the assaywas recorded as Ol) at a 492 nm wavelength using a microELISA reader (Dynatech, USA). The mean OD+2SD ofthe non-amoebic individuals was calculated and was takenas the cut-off point to differentiate positive from negativevalues."
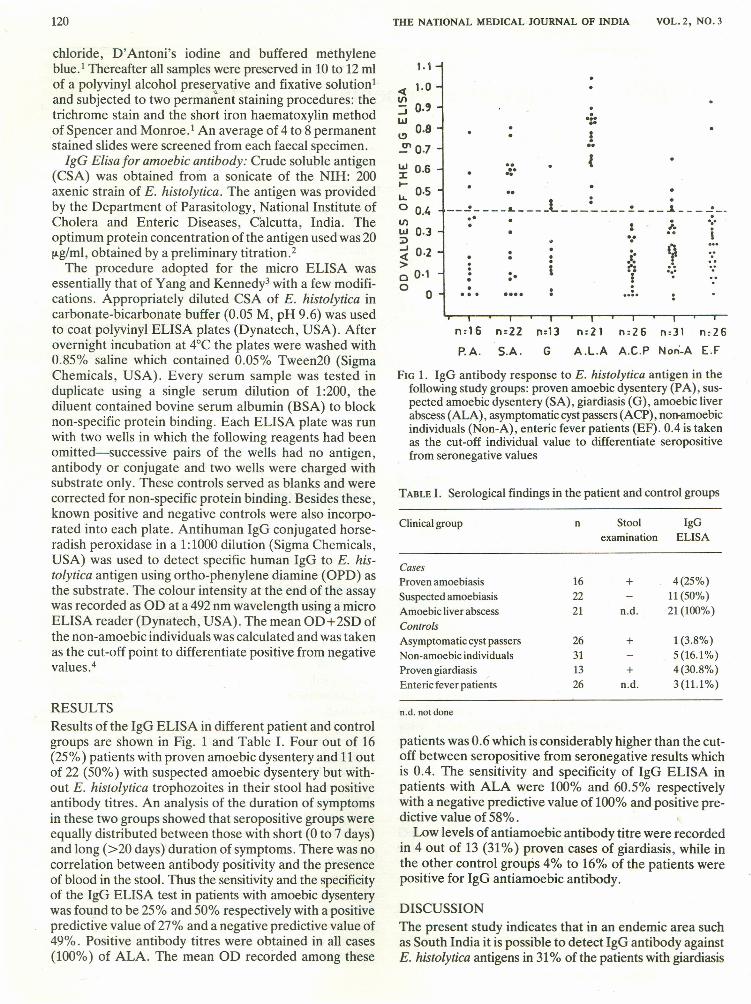
RESULTSResults of the IgG ELISA in different patient and controlgroups are shown in Fig. 1 and Table I. Four out of 16(25%) patients with proven amoebic dysentery and 11 outof 22 (50%) with suspected amoebic dysentery but with-out E. histolytica trophozoites in their stool had positiveantibody titres. An analysis of the duration of symptomsin these two groups showed that seropositive groups wereequally distributed between those with short (0 to 7 days)and long (>20 days) duration of symptoms. There was nocorrelation between antibody positivity and the presenceof blood in the stool. Thus the sensitivity and the specificityof the IgG ELISA test in patients with amoebic dysenterywas found to be 25% and 50% respectively with a positivepredictive value of 27% and a negative predictive value of49%. Positive antibody tit res were obtained in all cases(100%) of ALA. The mean Of) recorded among these
THE NATIONAL MEDICAL· JOURNAL OF INDIA VOL. 2, NO.3
1.1
< 1.0If).J 0.'w 0.8I.!)
2' 0.7
....,.,!..
...."~ 0.6
t- 0.5u,o 0.4If)w 0.3:;)
~ 0·2>o 0·1o 0
- .__ ~ L l ~ .! ~ .s __.. . .•.
• : I. :•• I'.'. . .i: ~?· . : "0· t ,.0 :. .( '.'• . ..• ..
• • 0 .... ....
n:16 n:22 n:13 n:21 n:26 n:31 n:26
P.A. S.A. G A.l.A A.C.P Nori-A E.F
FIG 1. IgG antibody response to E. histolytica antigen in thefollowing study groups: proven amoebic dysentery (PA), sus-pected amoebic dysentery (SA), giardiasis (G), amoebic liverabscess (ALA), asymptomatic cystpassers (ACP), non-amoebicindividuals (Non-A), enteric fever patients (EF). 0.4 is takenas the cut-off individual value to differentiate seropositivefrom seronegative values
TABLE I. Serological findings in the patient and control groups
patients was 0.6 which is considerably higher than the cut-off between seropositive from seronegative results whichis 0.4. The sensitivity and specificity of IgG ELISA inpatients with ALA were 100% and 60.5% respectivelywith a negative predictive value of 100% and positive pre-dictive value of 58%.
Low levels of anti amoebic antibody titre were recordedin 4 out of 13 (31 %) proven cases of giardiasis, while inthe other control groups 4% to 16% of the patients werepositive for IgG anti amoebic antibody.
DISCUSSIONThe present study indicates that in an endemic area suchas South India it is possible to detect IgG antibody againstE. histolytica antigens in 31% of the patients with giardiasis
SHErrY, PRABHU : IgG ELISA FOR AMOEBIASIS IN ENDEMIC AREAS
and 16% of individuals without any intestinal disease.Further, even in patients with frank amoebic dysentery thespecificity and sensitivity of the IgG ELISA is unacceptablylow. However, in patients with ALA the test is sensitiveand specific with a high negative predictive value althoughthe positive predictive value is low. Thus IgG ELISA canbe used to help in the diagnosis of patients with amoebicliver abscess but cannot be used as a confirmatory testbecause of its low specificity rate (60%) and positive pre-dictive value (58%). Similar conclusions have beenreported previously= from other countries.
The diagnostic efficacy of IgG ELISA in amoebicdysentery in the present series remains extremely poor incontrast to the experience of others in non-endemicareas.v' However, other reports from endemic areas havealso shown a persistent antibody response from previousE. histolytica infection which interferes with its diagnosticefficacy.s? Contrary to the pattern of antibody responsepreviously described, positive antibody levels in the presentseries were detected in only a few (4/16) proven patientswith amoebic dysentery in spite of demonstrable tissueinvasion by the E. histolytica trophozoites. On the otherhand 50% (11122)of patients with non-amoebic dysenteryhad a positive antibody titre. It is possible that the anti-body response may vary according to the E. histolyticastrain and its degree of invasion. This has been suggestedpreviously by Healy et al.8 The particular strain causingamoebic dysentery or the inadequate host immune systemmight be responsible for such a poor antibody response.It is possible that a greater degree of invasion is necessaryfor an adequate antibody response to occur. This has beenuniformly seen in patients with ALA in endemics-? as wellas non-endemic areas.t-
In the patients in whom E. histolytica trophozoites weredemonstrated the presence of amoebic antibody in 50%might be explained by E. histolytica trophozoites beingmissed in their stools or because they had a previoussubclinical infection. Under these circumstances thedetection of amoebic antigen in the stool describedrecently will be of considerable value.t!' We thereforeconclude that the IgG ELISA is of little diagnostic valuein amoebic dysentery, but is more useful in patients withamoebic liver abscesses.
Serological investigation of the patients with amoebicliver abscess in the present study indicates that the IgGELISA is of particular diagnostic value in endemic areas.If a serological diagnosis is not available, clinical diagnosisis usually achieved by recovery of typical anchovy saucefluid which is bacteriologically sterile. Bacterial infectionof the abscess, however, could lead to aspiration of foulsmelling, contaminated pus which might originally havebeen sterile. 12,13 In other cases where overt abscess forma-tion has not occurred or micro-abscesses cannot bedetected, and there are no immediate indications for
121
drainage, hepatic amoebiasis is purely an unproven butwell-recognized clinical entity.f Serological tests aretherefore of immense value in these cases.
It is apparent that a stool examination remains the firstline of investigation for intestinal amoebiasis. Whiledetection of IgM antibodies and faecal antigen assaysrequire further evaluation, the IgG ELISA is to be recom-mended as a useful adjunct to the diagnosis of suspectedcases of hepatic amoebiasis particularly in endemic areas.
ACKNOWLEDGEMENTSWe are grateful to Dr S. C. Pal and Dr P. Das of the NationalInstitute of Cholera and Enteric Diseases, Calcutta, for supply-ing us the antigen and providing us training facilities. We alsothank Dr M. J. G. Farthing, Consultant Gastroenterologist,St. Bartholomew's Hospital, London for advice and assistance,the Karnataka State Council for Science and Technology for fund-ing this project and Mrs. Lakshmi Menon for secretarial help.
REFERENCESGarcia LS. Laboratory diagnosis of parasitic infections. In:Finegold SM, Martin WJ (eds). Diagnostic Microbiology. St.Louis:C. V. Mosby Co, 1982:457-530.
2 Lowry PH, Rosebrough NJ, Farr AL, Randall RJ. Protein measure-ment with the folin phenol reagent.T Bioi Chem 1951;193:265-7.
3 Yang J, Kennedy MT Evaluation of enzyme-linked immunosorbentassay for the serodiagnosis of amoebiasis. } Clin Microbiol1979;10:778--85.
4 Das P, Pal S, Pal Sc. Evaluation of the micro enzyme-linkedimmunosorbent assay, indirect haemagglutination and indirectfluorescence antibody techniques for the serodiagnosis ofamoebiasis. I Diarrhoeal Dis Res 1984;1984;2:238--42.
5 Bos HJ, Eijk AA, Steerenberg PA. Application of ELISA-theenzyme-linked immunosorbent assay-in the serodiagnosis ofamoebiasis. Trans R Soc Trop Med Hyg 1975;69:440.
6 Knobloch J, Mannweiler E. Development and persistence ofantibodies to Entamoeba histolytica in patients with amoebic liver
Iabscess. Analysis of216 cases. Am} Trop Med Hyg 1983;32:727-32.7 Healy GR, Visvesvara GS, Kagan IG. Observations on the persistence
of antibodies to E. histolytica. Arch Invest Med 1974;5:495-500.8 Healy GR, Kagan IG, Gleason NN. Use of the indirect haemagglutina-
tion test in some studiesof seroepidemiologyof amoebiasisin the westernhemisphere. Health Lab Sci 1970;7:109--16.
9 Grundy MS, Voller A, Warhurst D. An enzyme-linked immunosorbentassay for the detection of E. histolytica antigens in faecal material. TransR Soc Trop Med Hyg 1987;81:627-32.
10 Anand P, Malviya B, Das P, Mateen MA, Habibullah CM, Das SR.Multilayer-enzyme-linked immunosorbent assay (ML-ELISA) for thedetection of E. histolytica trophozoite coproantigen. Immunol Invest1985;14:443-53.
11 Mahajan RC, Ganguly NK. Amoebic antigen in immunodiagnosisand prognosis of amoebic liver abscess. Trans R Soc Trop Med Hyg1980;74:300--2.
12 Healy GR. Laboratory diagnosis of amoebiasis. Bull NY Acad Med1971;47:478--93.
13 Cahill KM, Elsdon-Dew R, Juniper K, Neal RA, Powell SJ, HealyGR. Symposium on amoebiasis. Bull NY Acad Med 1971;47:435-507.
14 Prakash 0, Tandon BN, Bhalla I, Ray AK, Vinayak VK. Indirecthaemagglutination and amoeba-immobilisation tests and theirevaluation in intestinal and extra intestinal amoebiasis. Am} TrapMed 1969;18:670--5.