2 The Director’s View Dr. Christopher Murray discusses IHME’s work to answer three critical questions 3 Deep Dive The story behind the research to measure global education levels 4 Connections New fellows join IHME; recent outreach events 5 Innovations IHME’s recently published work examines algorithms to assess causes of death, distribution of bed nets, the link between women’s education and child mortality, and trends in chronic diseases 6 Ripple Effect IHME uses social networking to help determine the Global Burden of Disease
5 Innovations IHME’s recently published work examines algorithms to assess causes of death, distribution of bed nets, the link between women’s education and child mortality, and trends in chronic diseases
6 Ripple EffectIHME uses social networking to help determine the Global Burden of Disease
Millions of Americans in the United States have been diagnosed with Type 2 diabetes.
But knowing the nationwide prevalence of diabetes – or any disease – doesn’t help local health officials make decisions about how to allocate money for prevention or treatment in their communities.
Decisions about health care policy and management are made primarily at the local level. And yet, data on risk factors and diseases have mostly been limited to the national and state level.
A new approach by the Institute for Health Metrics and Evaluation (IHME) will change that by putting useful, local data in the hands of the people making the tough choices.
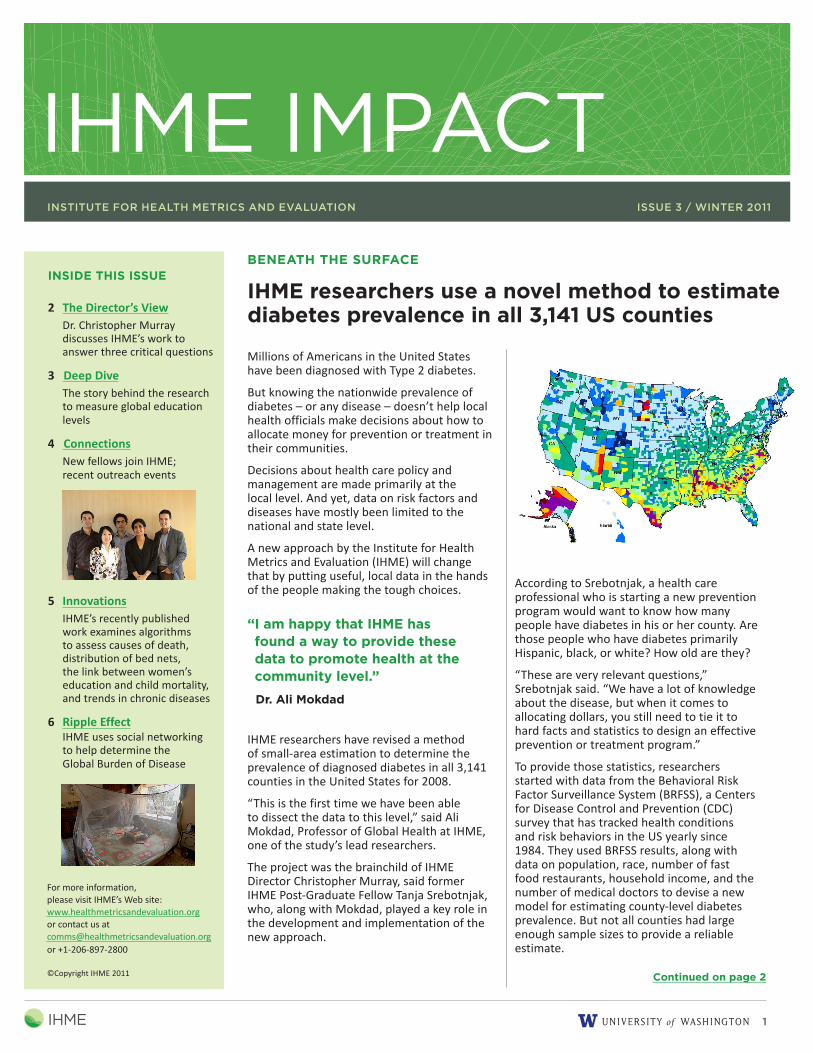
IHME researchers have revised a method of small-area estimation to determine the prevalence of diagnosed diabetes in all 3,141 counties in the United States for 2008.
“This is the first time we have been able to dissect the data to this level,” said Ali Mokdad, Professor of Global Health at IHME, one of the study’s lead researchers.
The project was the brainchild of IHME Director Christopher Murray, said former IHME Post-Graduate Fellow Tanja Srebotnjak, who, along with Mokdad, played a key role in the development and implementation of the new approach.
IHME researchers use a novel method to estimate diabetes prevalence in all 3,141 US counties
BENEATH THE SURFACE
Continued on page 2
According to Srebotnjak, a health care professional who is starting a new prevention program would want to know how many people have diabetes in his or her county. Are those people who have diabetes primarily Hispanic, black, or white? How old are they?
“These are very relevant questions,” Srebotnjak said. “We have a lot of knowledge about the disease, but when it comes to allocating dollars, you still need to tie it to hard facts and statistics to design an effective prevention or treatment program.”
To provide those statistics, researchers started with data from the Behavioral Risk Factor Surveillance System (BRFSS), a Centers for Disease Control and Prevention (CDC) survey that has tracked health conditions and risk behaviors in the US yearly since 1984. They used BRFSS results, along with data on population, race, number of fast food restaurants, household income, and the number of medical doctors to devise a new model for estimating county-level diabetes prevalence. But not all counties had large enough sample sizes to provide a reliable estimate.
For more information, please visit IHME’s Web site: www.healthmetricsandevaluation.org or contact us at [email protected] +1-206-897-2800
THE DIRECTOR’S VIEW BENEATH THE SURFACE (continued)
When IHME was created in 2007, it was envisioned as an academic research institute that would fill the gaps in objective evidence about global health.
We use cutting-edge science, not politics, to quantify threats to health worldwide and build evidence about what works and what does not to improve health conditions and health system performance.
Every time we embark upon a new approach to gathering data or begin a groundbreaking study, we have three critical questions in mind: What are the major health problems? How well is society addressing these problems? How do we best dedicate resources to get the maximum impact in improving population health in the future?
To answer these questions, we focus our work on four research areas: measuring health, tracking performance, maximizing impact, and innovative measurement systems.
All of this research is done with one end goal: to improve health through better information. Our work in these four areas provides access to more accurate health information and creates a stronger foundation for strategic decision-making.
This issue of Impact shares some of the ways we are answering these questions
through work in our key research areas.
1. In Beneath the Surface, we look at a method of small-area measurement used by researchers to provide county-level diabetes estimates for every county in the United States – information that will be used by health officials at the local level to make more informed decisions on how to allocate scarce resources.
2. In Deep Dive, we share an exciting discovery about women’s education and child survival and the enormous amount of work required to perform this research.
3. In Connections, we introduce our new Post-Bachelor Fellows and Post-Graduate Fellows, all of whom play key roles in gathering and distilling the information needed to improve upon global health measurement methods. We also share how we used a competition and a food-quality index to generate a record number of donations to a food drive.
4. Innovations provides a summary of our most recent research, including some good news about the distribution and use of bed nets in malaria-prone areas.
5. In Ripple Effect, we look at the launch of Financing Global Health 2010 and the use of social networking tools to gather health measurement surveys from around the world.
I hope you enjoy this issue.
Sincerely,
Christopher J.L. Murray
Institute Director and Professor of Global Health
That’s where small-area measurement comes in. It’s a method that originated in demography and has useful applications beyond the global health field.
“The basic idea is that if you’re interested in drawing any conclusions about a small group of people or a small area, you don’t have enough sample points to draw these conclusions with high enough certainty,” Srebotnjak explained. “Small-area measurement decreases the uncertainty by using information from other population groups that are similar to the one in question.”
The model was tested repeatedly using different population scenarios to ensure its reliability. The researchers ultimately created a model that allowed them to make estimates based on data from 10 people that were as accurate as estimates based on data from 3,000 people.
Local officials will now be able to understand the health of their populations, better allocate resources, track the success of programs, and even apply for state and federal funding that was previously unavailable because of a lack of documentation.
Mokdad, who previously managed and directed the BRFSS at the CDC, says this method gives him an opportunity to provide valuable data to every county in the US.
“At the CDC, I had many requests for local data from local health departments,” Mokdad says. “I am happy that IHME has found a way to provide these data to promote health at the community level.”
IHME has already used this method to estimate life expectancy in US counties, and researchers plan to release local data for other risk factors, such as health insurance coverage, smoking, blood pressure, and obesity.
Link between women’s education and child survival makes international headlines, but grueling work to quantify education levels is the unsung hero
Women are advancing further in school than at any time in recent history, a trend that is having a tremendous impact on child mortality, according to IHME research. These findings were part of an IHME study that revealed the impact of increased levels of education in reproductive-age women on child mortality rates. The research article, “Increased educational attainment and its effect on child mortality in 175 countries between 1970 and 2009: a systematic analysis,” was published in The Lancet in September 2010.
The relationship between a mother’s education and child mortality made headlines in Japan, Panama, and Malaysia and has been quoted by CBS News and Al Jazeera. But what many people don’t realize is the enormous amount of work that went into simply locating and accessing the data that made this analysis possible.
As IHME Post-Bachelor Fellow Krycia Cowling, one of the study’s authors, explained, “Unfortunately, we couldn’t just look on the Internet for the data we needed, because much of this historical information is only found in statistical and demographic yearbooks.”
According to Cowling, when Emmanuela Gakidou, the study’s lead author, found out that Harvard University
had some of the data she needed in books that were only available on that campus, she persuaded a researcher there to photocopy individual pages of demographic tables published in the books and send them to IHME. Each data point was then manually entered into the project spreadsheets.
“We used a total of 915 censuses and surveys from 219 different countries,” Cowling said. “That’s a lot of data points.”
“The punch line of the paper is the effect of the increased education levels on child mortality,” said Cowling. “But the bulk of time we spent on the research – about three-quarters of the total time – was quantifying the levels of education everywhere.”
The study showed that mortality in children under age 5 dropped from 16 million to 7.8 million annually between 1970 and 2009, and IHME researchers estimate that 51% of the reduction can
be linked to increased education among women of reproductive age.
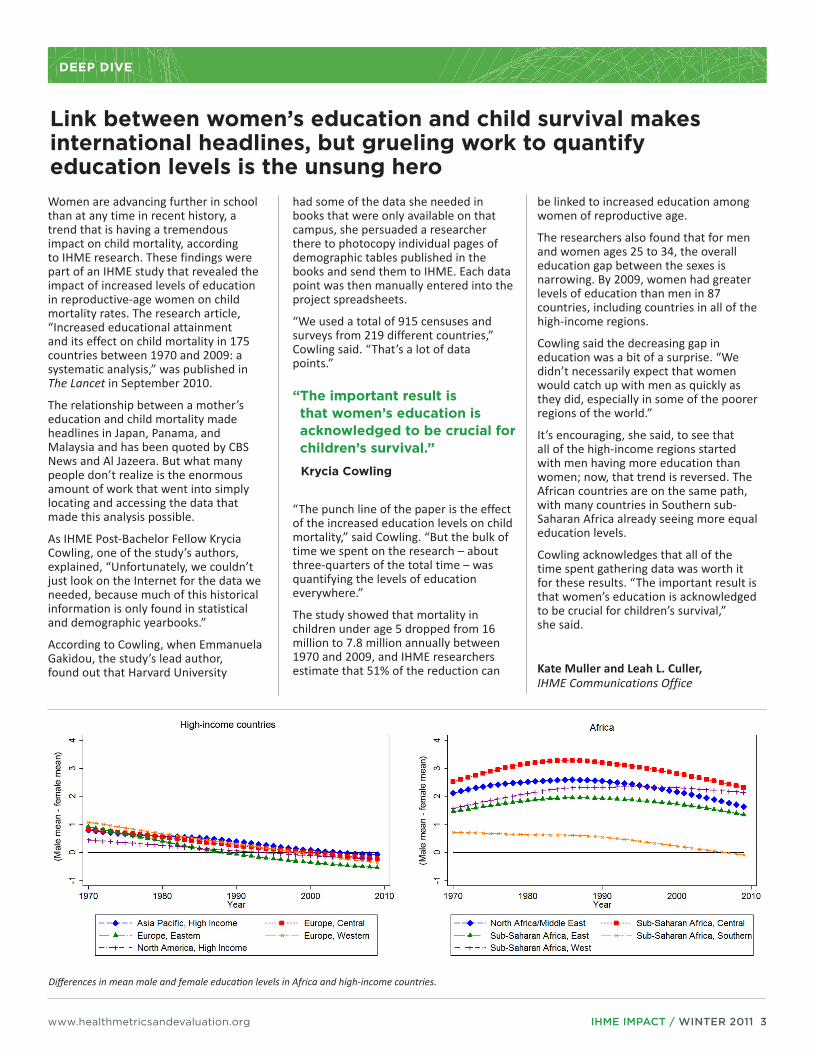
The researchers also found that for men and women ages 25 to 34, the overall education gap between the sexes is narrowing. By 2009, women had greater levels of education than men in 87 countries, including countries in all of the high-income regions.
Cowling said the decreasing gap in education was a bit of a surprise. “We didn’t necessarily expect that women would catch up with men as quickly as they did, especially in some of the poorer regions of the world.”
It’s encouraging, she said, to see that all of the high-income regions started with men having more education than women; now, that trend is reversed. The African countries are on the same path, with many countries in Southern sub-Saharan Africa already seeing more equal education levels.
Cowling acknowledges that all of the time spent gathering data was worth it for these results. “The important result is that women’s education is acknowledged to be crucial for children’s survival,” she said.
Kate Muller and Leah L. Culler,IHME Communications Office
Differences in mean male and female education levels in Africa and high-income countries.
“The important result is that women’s education is acknowledged to be crucial for children’s survival.”
Post-Bachelor Fellows(pictured above, left to right):
Brendan DeCenso is from Cincinnati, OH, and received his Bachelor of Science in Business Administration and Bachelor of Arts in Economics, both from the University of North Carolina at Chapel Hill. At IHME, he is on the Monitoring Costs research team.
David Chou is from Oak Brook, IL, and received his Bachelor of Arts in Public Policy from Duke University. He is on the Health Financing research team.
Rashmi Jasrasaria is from Boxborough, MA, and received her Bachelor of Arts in Social Studies from Harvard University. She is a member of the Effective Intervention Coverage research team.
Katrina Ortblad, from Seattle, earned her Bachelor of Arts in Human Biology modified with Environmental Studies from Dartmouth College. She is on the Causes of Death research team.
Miriam Alvarado is from Santa Clara, CA. She received Bachelor of Arts degrees in Economics and Development Studies, both from the University of California, Berkeley. She is on the Social Determinants research team.
Samuel Masters is from Friday Harbor, WA, and received his Bachelor of Science in Economics from the University of Washington. He is on the Health Service Delivery Constraints research team.
Ben Campbell is from Pittsburgh, PA, and received his Bachelor of Arts in Anthropology from Dartmouth College. He is on the Verbal Autopsy research team.
Thomas Roberts is from Mechanicsville, VA. He received his Bachelor of Arts in Sustainability Studies from the University of Virginia. He is on the Risk Factors and Cost Effectiveness research teams at IHME.
Nicole Johns is from Sudbury, MA, and received her Bachelor of Arts in Sociology from Dartmouth College. She is working on the Burden of Disease research team.
Michael Freeman is from Denver, CO, and received his Bachelor of Arts in Sociology and International Affairs from Colorado College. He is on the Risk Factors research team.
Emily Carnahan is from Edina, MN, and received her Bachelor of Arts in Economics from Northwestern University. She is on the US County Performance research team.
Katherine Lofgren is from Denver, CO, and received her Bachelor of Arts in Biology from Smith College. She is on the Demographics: Mortality and Population research team.
Post-Graduate Fellows(pictured above, left to right):
Andres Vecino-Ortiz is from Bogota, Colombia. He earned his MD from Universidad Javeriana and his Master of Economics from Universidad de los Andes. He is on the Cost Effectiveness research team.
Xiaoyue “Maggie” Niu is from Beijing, China and earned a PhD in Statistics from the University of Washington. She works on the Demographics: Mortality and Population research team.
Alireza Vahdatpour is from Tehran, Iran, and earned his PhD in Computer Science from the University of California, Los Angeles. Alireza works on the Verbal Autopsy and Optimal Resource Allocation research teams.
Nalina Varanasi is from Mumbai, India, and she received her PhD in Economics from the University of Washington. She works on the Health Service Delivery Constraints research team.
Lahn Straney is from Brisbane, Australia and earned his PhD in Epidemiology and Biostatistics from the University of Queensland. He is on the Effective Intervention Coverage research team.
IHME draws from metrics expertise while raising record amount of money, food for charity
CONNECTIONS
IHME staff rallied to support the University of Washington’s effort to raise money for the 2010 Combined Fund Drive, helping the school raise a record $2,044,404, despite a year of budget cuts and dismal economic news.
Every faculty, fellow, and staff member at IHME participated in some way, either contributing money through a payroll deduction to their favorite charity, donating to the food drive, or participating in one of three fundraising events: a chili cook-off, a scavenger hunt, and a raffle. Proceeds from the events alone totaled more than $1,000 and went to FareStart,the nonprofit program aimed at training the homeless to work in restaurants.
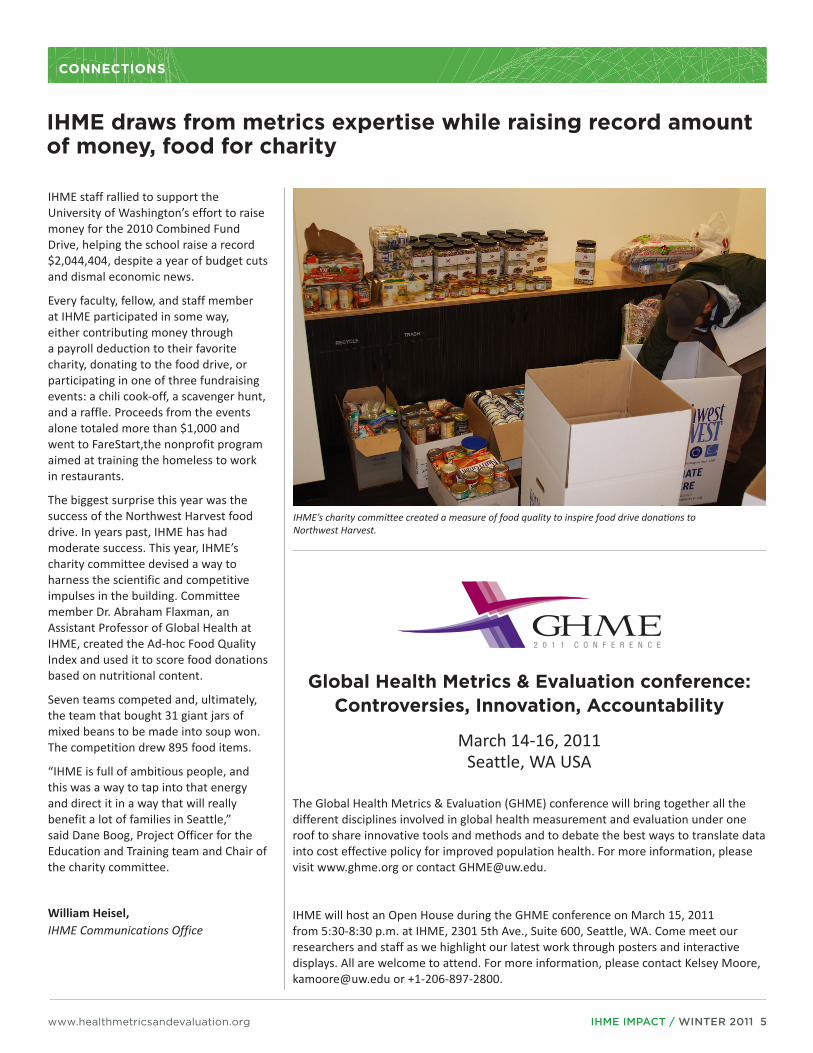
The biggest surprise this year was the success of the Northwest Harvest food drive. In years past, IHME has had moderate success. This year, IHME’s charity committee devised a way to harness the scientific and competitive impulses in the building. Committee member Dr. Abraham Flaxman, an Assistant Professor of Global Health at IHME, created the Ad-hoc Food Quality Index and used it to score food donations based on nutritional content.
Seven teams competed and, ultimately, the team that bought 31 giant jars of mixed beans to be made into soup won. The competition drew 895 food items.
“IHME is full of ambitious people, and this was a way to tap into that energy and direct it in a way that will really benefit a lot of families in Seattle,” said Dane Boog, Project Officer for the Education and Training team and Chair of the charity committee.
William Heisel,IHME Communications Office
IHME’s charity committee created a measure of food quality to inspire food drive donations to Northwest Harvest.
Global Health Metrics & Evaluation conference: Controversies, Innovation, Accountability
March 14-16, 2011Seattle, WA USA
The Global Health Metrics & Evaluation (GHME) conference will bring together all the different disciplines involved in global health measurement and evaluation under one roof to share innovative tools and methods and to debate the best ways to translate data into cost effective policy for improved population health. For more information, please visit www.ghme.org or contact [email protected].
IHME will host an Open House during the GHME conference on March 15, 2011 from 5:30-8:30 p.m. at IHME, 2301 5th Ave., Suite 600, Seattle, WA. Come meet our researchers and staff as we highlight our latest work through posters and interactive displays. All are welcome to attend. For more information, please contact Kelsey Moore, [email protected] or +1-206-897-2800.
Algorithms developed by IHME researchers reassign causes of death; each color represents a different cause of death code.
Researchers from IHME developed new algorithms to redistribute cause of death coding for deaths that have been improperly assigned and classified, allowing for more effective large-scale comparisons of cause of death trends across countries and time.
Innovation: Comparable assessments of cause of death trends are limited by a number of factors. Changes in cause of death coding over time make it difficult to compare deaths assigned with different versions of coding systems. In addition, deaths are frequently assigned codes that are not useful for public health analyses, often called garbage codes. Researchers reduced the number of garbage codes by mapping causes of death over six decades and consulting with health experts to identify likely causes to which garbage codes should be reassigned. They developed algorithms to redistribute those deaths into a database with 700 million deaths.
Naghavi M, Makela S, Foreman K, O’Brien J, Pourmalek F, Lozano R. Algorithms for enhancing public health utility of national causes-of-death data. Population Health Metrics, May 2010
African countries rapidly distribute bed nets to fight malaria
The number of households that own an insecticide-treated bed net in countries susceptible to malaria has grown 16 times over the past decade, according to new research from IHME and its collaborators. Countries that received the most health aid for malaria programs had the fastest scale-up of bed net distribution. Use of the nets has also grown significantly. In 1999, only 1.5% of children at risk slept under a
net. By 2008, more than a quarter – 26.6% – of children slept under a net.
Innovation: The method IHME developed to track bed nets has broad application to help study the scale-up of other global health interventions, including vaccines and medications. The new method is an adaptation of a “stock and flow model” that has been used in the past by companies to track products, such as appliances and pharmaceuticals. IHME matched the model to the wide array of information available about bed nets, estimating trends in ownership and use, even in countries that have sparse data.
Flaxman AD, Fullman N, Otten MW Jr., Menon M, Cibulskis RE, Ng M, Murray CJL, Lim SS. Rapid scaling-up of insecticide-treated bed net coverage in Africa and its relationship with development assistance for health: a systematic synthesis of supply, distribution, and household survey data. PLoS Medicine, August 2010
Rising education levels among women save children’s lives worldwide
IHME research found that women are advancing further in school than at any time in recent history, a trend that is having a tremendous impact on child mortality. Between 1970 and 2009, mortality in children under age 5 dropped from 16 million to 7.8 million annually, and IHME researchers estimate that 51% of the reduction can be linked to increased education among women of reproductive age.
Innovation: Researchers at IHME gathered data from 915 censuses and national surveys worldwide to create a time series of education levels for 175 countries.
Gakidou E, Cowling K, Lozano R, Murray CJL. Increased educational attainment and its effect on child mortality in 175 countries between 1970 and 2009: a systematic analysis. The Lancet, September 2010
New methods allow estimates of diabetes at county level
Using a new approach, researchers at IHME have estimated the prevalence of diagnosed diabetes in all counties in the United States for 2008. The method allows local policymakers to compare different health needs and set priorities to use scarce resources efficiently.
Innovation: Data on prevalence of risk factors and diseases have previously been mostly limited to the state level. IHME researchers used data on population, race, number of fast food restaurants, household income, and the number of medical doctors to devise a new model for estimating risk factors and disease prevalence. They also used those data to create county-level estimates, ultimately creating a model that allowed them to make estimates based on data from 10 people that were of the same quality as estimates based on data from 3,000 people.
Srebotnjak T, Mokdad AH, Murray CJL. A novel framework for validating and applying standardized small area measurement strategies. Population Health Metrics, September 2010
Just published this month:
Roth GA, Fihn SD, Mokdad AH, Aekplakorn W, Hasegawae T, Lim SS. High total serum cholesterol, medication coverage and therapeutic control: an analysis of national health examination survey data from eight countries. Bulletin of the World Health Organization, February 2011
Danaei G, Finucane MM, Lin JK, Singh GM, Paciorek CJ, Cowan MJ, Farzadfar F, Stevens GA, Lim SS, Riley LM, Ezzati M, on behalf of the Global Burden of Metabolic Risk Factors of Chronic Diseases Collaborating Group (Blood Pressure). National, regional, and global trends in systolic blood pressure since 1980: systematic analysis of health examination surveys and epidemiological studies with 786 country-years and 5.4 million participants. The Lancet, February 2011
Gakidou E, Mallinger L, Abbott-Klafter J, Guerrero R, Villalpando S, Lopez-Ridaura R, Aekplakorn W, Naghavi M, Lim SS, Lozano R, Murray CJL. Management of diabetes and associated cardiovascular risk factors in seven countries: a comparison of data from national health examination surveys. Bulletin of the World Health Organization. March 2011
IHME uses social networking to help determine the Global Burden of Disease
RIPPLE EFFECT
common metric for quantifying losses of years of healthy life. A group of scientists, including Dr. Christopher Murray, IHME Director, created this concept in the early nineties by generating comprehensive and consistent estimates of morbidity and mortality for eight regions of the world.
This online outreach provides IHME the potential to directly measure the pulse of the entire world.
A contest on Facebook boosted responses by appealing to people’s competitiveness, Cooley said. “We were posting the number of responses per country to see if we could get countries to rally and increase their numbers.”
Regular updates of the number of responses from various countries are posted on Twitter, and the survey is being promoted by global health blogs worldwide. One writer recently posted on Twitter, “C’mon, Aussies! Make 15 minutes count for global health.” And Karen Grepin, a well-regarded blogger and New York University professor, wrote recently, “I have not had this much geeky fun in ages.”
IHME has posted the survey in Spanish and is working on a Mandarin translation.
Researchers hope to get at least another 8,000 responses. Data from the online survey, along with information gathered through household surveys in Peru, Bangladesh, South Africa, Indonesia, and Tanzania and from phone surveys in the US will help shape the new health state severity weights.
Make your next 15 minutes count for global health – please take the Global Burden of Disease 2010 Health Measurement Survey: http://gbdsurvey.org
Leah L. Culler,IHME Communications Office
Researchers at IHME, in conjunction with 800 collaborators around the globe, are trying to improve the understanding of global health by asking citizens worldwide to take an online survey, and the Institute is using Facebook, Twitter, and blogs to promote the cause.
“The point of the survey is to add to our understanding of global health problems and ultimately enable policymakers and health care leaders to make better decisions on how to improve population health,” said Rebecca Cooley, the Global Burden of Disease Project Officer at IHME.
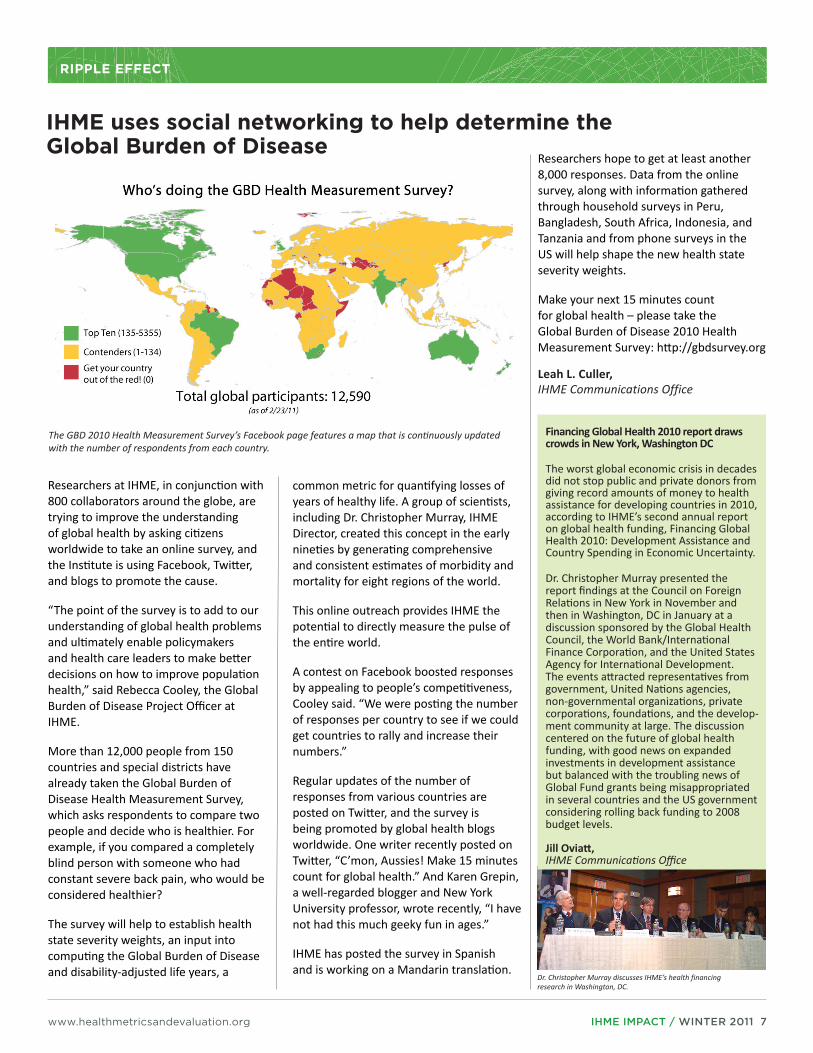
More than 12,000 people from 150 countries and special districts have already taken the Global Burden of Disease Health Measurement Survey, which asks respondents to compare two people and decide who is healthier. For example, if you compared a completely blind person with someone who had constant severe back pain, who would be considered healthier?
The survey will help to establish health state severity weights, an input into computing the Global Burden of Disease and disability-adjusted life years, a
The GBD 2010 Health Measurement Survey’s Facebook page features a map that is continuously updated with the number of respondents from each country.
Financing Global Health 2010 report draws crowds in New York, Washington DC
The worst global economic crisis in decades did not stop public and private donors from giving record amounts of money to health assistance for devel oping countries in 2010, according to IHME’s second annual report on global health funding, Financing Global Health 2010: Development Assistance and Country Spending in Economic Uncertainty.
Dr. Christopher Murray presented the report findings at the Council on Foreign Relations in New York in November and then in Washington, DC in January at a discussion sponsored by the Global Health Council, the World Bank/International Finance Corpora tion, and the United States Agency for International Development. The events attracted representa tives from government, United Nations agencies, non-governmental organizations, private corporations, foundations, and the develop-ment community at large. The discussion centered on the future of global health funding, with good news on expanded investments in development assistance but balanced with the troubling news of Global Fund grants being misap propriated in several countries and the US government considering rolling back funding to 2008 budget levels.
Jill Oviatt, IHME Communications Office
Dr. Christopher Murray discusses IHME’s health financing research in Washington, DC.