81
Illuminating Hope in the Fight Against Cancer

Illuminating Hope in the Fight Against Cancer

Statements made about Genelux Corporation, other than statements of historical fact, reflect Management’s current beliefs and assumptions founded on the data and information currently available to us. Statements of the company’s progress, results, timing of pre-clinical and clinical trials and projections for product pipelines are examples of forward-looking statements. By definition, such undertakings involve risks, uncertainties and assumptions, and are subject to a number of such factors that could cause actual results to differ substantially from statements made, including but not limited to: risks associated with the success of clinical trials, research and development programs, regulatory approval processes for clinical trials, competitive technologies and products, patents, inception and/or continuation of corporate and other strategic partnerships and the need for additional funding or financing.
The information contained in this presentation does not purport to be all-inclusive or
to contain all of the information that prospective investors may desire. In all cases, interested parties should conduct their own investigation and analysis of Genelux’s business. No representation or warranty is made as to the accuracy or completeness of these materials, and the only representations or warranties that will be made in connection with any further investment will be the representations and warranties as may be set forth in the definitive documentation executed by a duly authorized representative of Genelux.
Genelux Forward Looking Statement
2

OUR COMPANY
3

Research Collaborations
• Memorial Sloan-Kettering Cancer
Center, (New York, New York)
• University of Tuebingen, (Germany)
• Institute of Cancer Research, (UK)
• Univ. California, San Diego
• University of Würzburg, (Germany)
• National Institutes of Health
• University of Leeds (UK)
Contract Manufacturing
Business Office Redlands, CA, USA
Product Analysis Bernried, Germany
Headquarters; Research and Development San Diego, CA, USA
As of Oct. 2014, the Company has 23 employees in the US, and 7 in Germany.
Company Overview

Management
• Tom Zindrick, JD, President & CEO
• Albert Roeder, PhD, COO
• John Prunty, CFO
– Former - Optimer, Gen-Probe
• Paul Scigalla, MD, PhD, CMO
– Former - Pfizer, SUGEN, Boehringer Mannheim, Pharmacia
5
Chief Clinical Advisor • Yuman Fong, MD
– Chairman, Dept. of Surgery, City of Hope
Board of Directors (Majority Independent) • James Tyree, • Thomas Zindrick, JD, - Chairman of the Board - President & CEO – Former – Sugen, Abbott • George Vandeman, JD, Vice Chairman • Ron Simus, DDS – Former – Latham & Watkins, Amgen - First investor • John Thomas, MA, MBA, PhD – Dean, La Sierra University • Billy J. Parrott, BS – President of Private Networks • Dr. Peter Kroll, MD – Founder, Medical Director, CPS
Board and Management

PLATFORM TECHNOLOGY:
ONCOLYTIC VACCINIA VIRUS
6

Most successful biologic in history: safely used in millions of people as the vaccine against smallpox
Genetically stable DNA virus
Replicates in the cell cytoplasm, does not alter the host genome
Infects and kills broad range of cancer cells
Large genetic information carrying capacity - potential inclusion of additional genes to produce therapeutic proteins or improve diagnostic capability
Travels in bloodstream to distant tumors
7
VACCINIA VIRUS’ COMPETITIVE ADVANTAGE

Cowpox & the eradication of smallpox
Milkmaids infected with cowpox (a disease similar to smallpox, but much less virulent)
protected them from smallpox
Observations of natural phenomena
Milkmaids generally immune to smallpox
Hypothesis
Jenner’s vaccine
Jenner's vaccine laid the foundation for contemporary discoveries in immunology. In 1979, the World Health Organization declared smallpox an eradicated disease.
Cowpox vaccine provided protection to smallpox
Vaccinia vaccine

Vaccinia
Modern smallpox vaccine e.g., LIVP strain of vaccinia
A common ancestral virus
Cowpox Vaccinia Variola (the causative agent of smallpox
Jenner’s vaccine

Smallpox has an excellent safe use history
Adverse evens per million vaccinees

Spontaneous remission of leukemia following smallpox vaccination
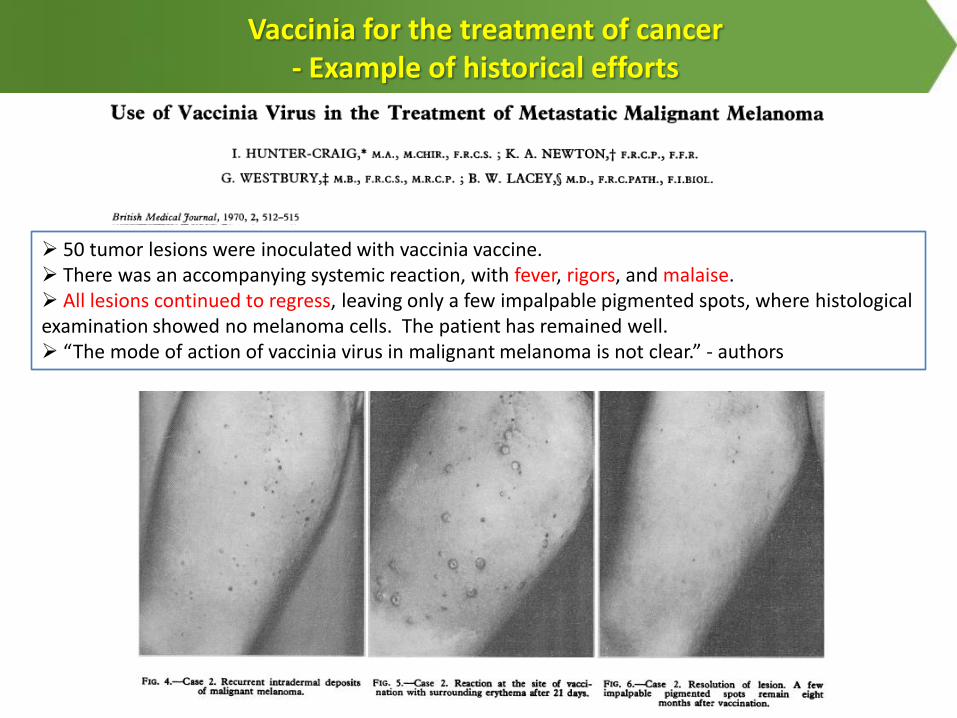
Vaccinia for the treatment of cancer - Example of historical efforts
50 tumor lesions were inoculated with vaccinia vaccine. There was an accompanying systemic reaction, with fever, rigors, and malaise. All lesions continued to regress, leaving only a few impalpable pigmented spots, where histological examination showed no melanoma cells. The patient has remained well. “The mode of action of vaccinia virus in malignant melanoma is not clear.” - authors

Vaccinia for the treatment of cancer - Example of historical efforts
Treating cancers by AS strain of vaccinia in Japan in 1980’s.
I.v. injection of AS strain virus (Case #1: 108 pfu 22 days, 2×108 pfu 20 days; Case #2: 2×108 pfu 3x per wk for 7 wks, then 4×108 pfu & 8×108 pfu for unknown number of times). Antitumor effect against lung & bone mets observed in two cases.
I.v. injection of AS strain virus. Demonstrated significant reductions in patient’s IgA monoclonal protein levels (monoclonal elevations of IgA characterize multiple myeloma).

Oncolytic Vaccinia Virus for Cancer Therapy
Observations of spontaneous cancer remission after virus infection (e.g., remission of leukemia after smallpox vaccination)
Use of natural virus or vaccine virus for cancer treatment (e.g., treating multiple myeloma with AS strain of vaccinia)
1980’s
1900’s -
1970’s
Genetically engineered virus for cancer treatment (e.g., attenuated GL-ONC1 virus for treatment of cancers)
1998 till
now
Recombinant DNA technology
Role of genetic engineering: Attenuation of virus for safety Tumor targeting (e.g., TK mutation) Arming virus w/ additional diagnostic & therapeutic genes
GLV-1h68 (i.e. GL-ONC1)
lacZ PsEL P7.5
ruc-gfp PsEL
gusA rtfr
J2R F14.5L A56R
P11
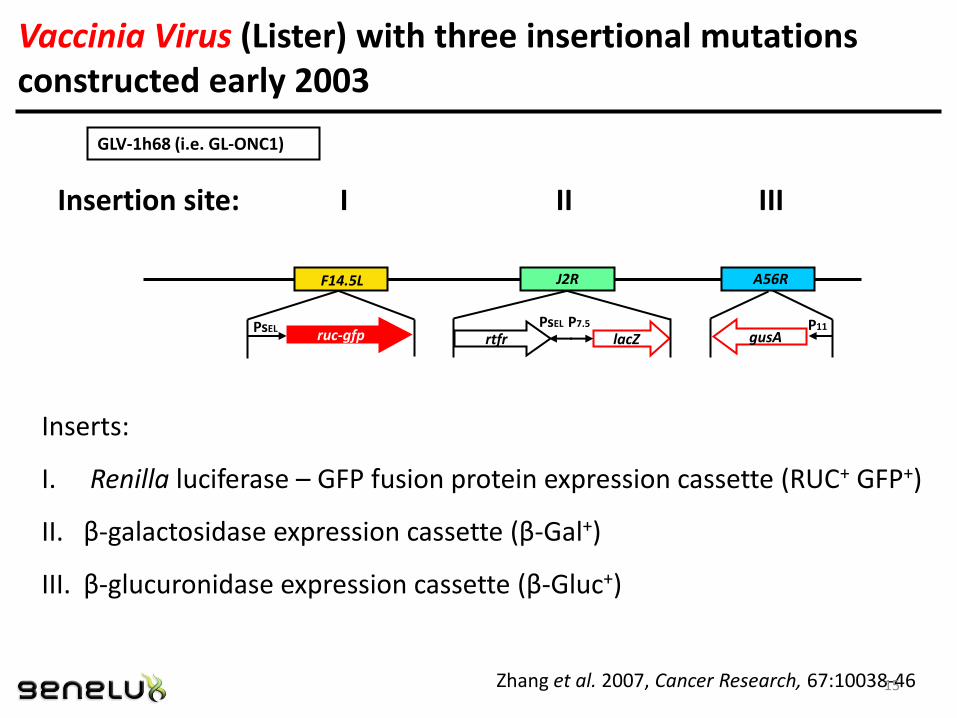
Zhang et al. 2007, Cancer Research, 67:10038-46
Insertion site: I II III
Inserts:
I. Renilla luciferase – GFP fusion protein expression cassette (RUC+ GFP+)
II. β-galactosidase expression cassette (β-Gal+)
III. β-glucuronidase expression cassette (β-Gluc+)
Vaccinia Virus (Lister) with three insertional mutations constructed early 2003
15

Eradication of Solid Human Breast Tumors in Nude Mice with an
Intravenously Injected Light-Emitting Oncolytic Vaccinia Virus
Days after Virus Injection
M
ean T
um
or
Volu
me
Treated Untreated
GLV-1h68 is effective as a monotherapy
Zhang et al. 2007, Cancer Research, 67:10038-46 16
anti-tumor response in 3 phases

Body weight comparison of tumor-bearing mice with and without GLV-1h68 treatment
17

• Analysis of the lungs of 12 PC-3 tumor-bearing mice for the presence of PC-3 cells
• RT-PCR using primers for human β-actin
Lun
gs p
osi
tive
fo
r h
um
an β
-ac
tin
(%
)
GLV-1h68 completely eliminated hematogenous metastases in lungs 21 days after virus injection
GLV-1h68 Colonized & Eradicated Metastases
18

Single injection of GLV-1h68 virus resulted in dramatic reduction of CTCs in the blood of mice bearing metastatic
human prostate (PC-3) tumors
0
200
400
600
800
1000
1200
PBS 1h68
CTC
s/m
l
14 days post treatment
All CTCs detected in 1h68-treated mice were infected tumor cells
19

0
200
400
600
800
1000
1200
1400
1600
30 40 50 60 70 80 90 100
Avera
ge t
um
or
vo
lum
e (
mm
^3)
Time after PANC-1 cell implantation (days)
GLV-1h68 + cisplatin
GLV-1h68
No treatment
cisplatin
GLV-1h68 is effective in Combination with Chemotherapy
Yu et al. 2009, Molecular Cancer Therapy, 8: 141-151 20

Virus + radiotherapy showed synergistic activity against pancreatic cancer
Dai et al., Cancer Letters 344 (2014) 282–290
In vitro synergy Enhanced apoptosis
Enhanced in vivo effect
GLV-1h151
TM: V+XRT synergistically enhance therapy.

Viruses with Imaging Genes
Viruses with Therapeutic Genes
Viruses with genes for tissue regeneration & reprogramming
human somatic cells to pluripotency
Optical imaging Immune modulatory molecules Tissue regeneration genes
PET imaging Anti-angiogenic genes Tissue reprogramming genes
MRI imaging Metastasis suppressor genes
Cell matrix-degradative genes
Hormones
microRNAs and many more…
22
NOVEL RECOMBINANT VACCINIA VIRUSES FOR TUMOR DIAGNOSIS & THERAPY
> 500 new recombinant
VACVs produced by Genelux

0
100
200
300
400
500
600
D14 D18 D21 D25 D29 D33 D36 D40
Tu
mo
r v
olu
me (
mm
3)
Day
Virus Iodine Control Virus+Iodine
GLV1h-153 treatment
131I treatment
Virus Expressing hNIS + 131I Eliminated Triple Negative Breast Tumors
Gholami et al. 2014, FASEB J, 28:676-82 23

Intra-pleural treatment with GLV-1h153 eradicates tumor burden
Belin et al. 2013, Surgery, 154:486-93
24

131I-SPECT/CT imaging of hNIS specific uptake of 131I in pleural tumor deposits
Belin et al. 2013, Surgery, 154:486-93 25
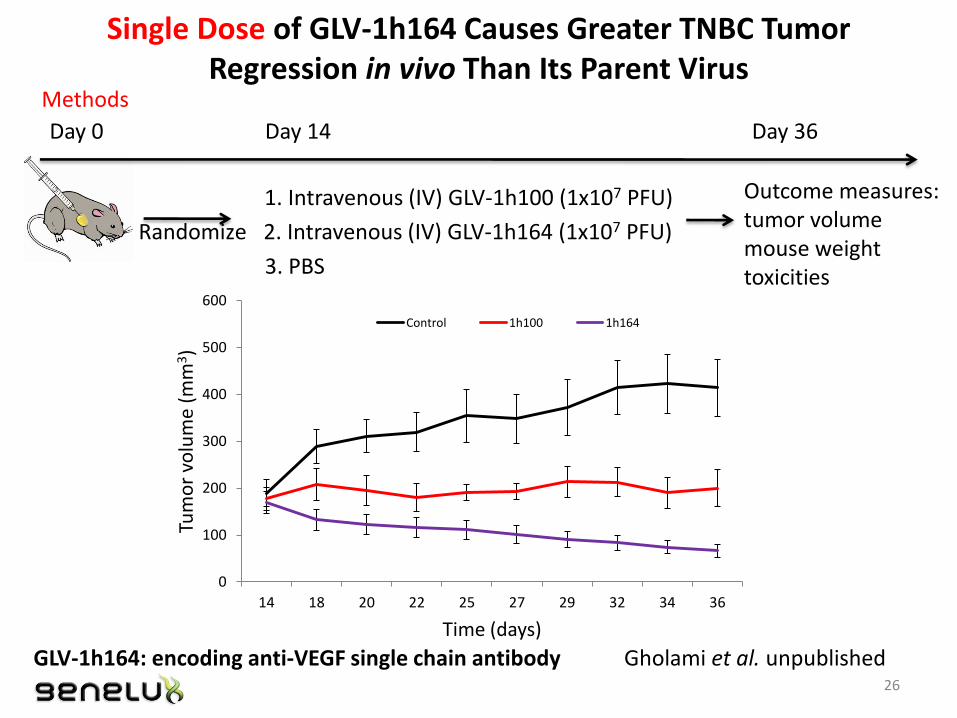
1. Intravenous (IV) GLV-1h100 (1x107 PFU)
Randomize 2. Intravenous (IV) GLV-1h164 (1x107 PFU)
3. PBS
Single Dose of GLV-1h164 Causes Greater TNBC Tumor Regression in vivo Than Its Parent Virus
Methods
Day 14 Day 0
Outcome measures: tumor volume mouse weight toxicities
Day 36
0
100
200
300
400
500
600
14 18 20 22 25 27 29 32 34 36
Tum
or
volu
me
(mm
3)
Time (days)
Control 1h100 1h164
Gholami et al. unpublished 26
GLV-1h164: encoding anti-VEGF single chain antibody

Control
GLV-1h100 GLV-1h164
GLV-1h164 Decreases Vascular Flow to TNBC in vivo A
nim
al 1
A
nim
al 2
27

CLINICAL DEVELOPMENT
28

Well tolerated & specifically targets,
replicates in and lyses tumor cells
•May be delivered via systemic, regional or local routes
•Spares healthy tissues and cells, minimizing toxicity and side effects
•Colonizes and lyses in wide range of tumor types
• Infects free-floating tumor cells (ascites) and circulating tumor cells
Activates patients’ immune response
against tumors
•Harnesses the body’s immune response to recognize and fight against tumor
•Trains body’s immune system to deliver a sustained attack on residual and new cancer cells
Can be armed with transgenes for specific delivery & amplification
in tumor cells
•Enhancing Anti-cancer therapy (targeting, efficacy)
•Enabling real-time optical and/or deep tissue imaging
•Allowing immuno-modulation to improve therapeutic outcomes and quality of life
•> 500 viral vectors with > 110 transgenes
29
GENELUX VACCINIA ONCOLYTIC IMMUNOTHERAPY PLATFORM
GENELUX VACCINIA ONCOLYTIC IMMUNOTHERAPY PLATFORM
Delivering a powerful, targeted and sustained attack on cancer…wherever it may reside

Clinical Site Location
Phase
Disease Indication
Route of Delivery
Combination Therapy
# of Patients Treated
# of Total
Infusions Given
Royal Marsden GL-ONC1-002/MA
I Solid tumors i.v. - 27 129
Royal Marsden/ Surrey GL-ONC1-002/MA
Ib Solid tumors i.v. - 16 104
Tübingen GL-ONC1-004/TUE
I/II Peritoneal carcinomatosis
Intraperitoneal (i.pe.)
- 9 23
UCSD GL-ONC1-005/UCSD
I H & N carcinoma i.v. Cisplatin + radiation
17 24
MSKCC GL-ONC1-003/MSK
I Mesothelioma; Malignant pleural effusion
Intrapleural (i.pl.)
- 14 14
TOTALS 83 294
GL-ONC1
Rationale: - Route of delivery: systemic vs. regional; - Monotherapy vs. combination therapy 30

First-in-Human Phase I & Ib Trial in United Kingdom
A Phase I Open-Label, Dose-Escalating Study of the Safety, Tolerability, and Tumor-Specific Replication of the Intravenous Administration of Green
Fluorescent Protein Encoded Genetically Engineered Attenuated Vaccinia Virus, GL-ONC1, with Real-Time Imaging in Patients with Advanced Solid Organ Cancers
Prof. Kevin Harrington Prof. Johann de Bono
Principal Investigators
Prof. Hardev Pandha
31

GL-ONC1-002/MA Dose-escalation Design
28-day cycle
14-day cycle
14-day cycle
Phase I
Phase Ib
← current 7 to 14-day cycle
5 consecutive days
Cohort 8: 1.667×109 pfu
Cohort 8a: 1.667-3×109 pfu
Cohort 8b: 1.667-5×109 pfu
Cohort 8c: 1.667-5×109 pfu
Cohort 8d: 1.667-5×109 pfu
Phase Ib: 3×109 pfu 28-day cycle
32

Patient Demographics - GL-ONC1-002/MA
TUMOR TYPE TOTALS %
Colorectal 7 17
Melanoma 6 14
Head & Neck 6 14
Parotid 3 7
Cholangiocarcinoma 3 7
Renal cell carcinoma 3 7
Esophagus 3 7
Non-small cell lung cancer 2 5
Rectal carcinoma 2 5
Prostate cancer 2 5
Thyroid 1 2
Myxoid chondrosarcoma 1 2
Pleural carcinoma 1 2
Adenocarcinoma - appendix 1 2
Pleural Mesothelioma 1 2
Ovarian 1 2
TOTALS 43 100
SEX
Male 33 (78%)
Female 10 (22%)
TOTAL NUMBER OF GL-ONC1 INFUSIONS / BOLUS
233
AGE
Range 39-79
Median Age 61
ETHNICITY
Caucasian 41 (95%)
Afro-Caribbean
1 (5%)
Asian 1 (5%)
33

Phase I / II Trial at University Hospital Tübingen
Phase I/II study of intraperitoneal administration of GL-ONC1, a genetically modified vaccinia virus,
in patients with peritoneal carcinomatosis
Prof. Dr. med
Michael Bitzer
Prof. Dr. med.
Ulrich M. Lauer
Principal Investigator Co-Investigator
34

Dose-escalation Design GL-ONC1-004/TUE
Phase I
Phase II
← current
Cohort 2: 1×108 pfu
Cohort 3: 1×109 pfu
Cohort 4: 3×109 pfu
Cohort 5: 5×109 pfu
Cohort 1: 1×107 pfu
Recommended Phase II Dose ?
first i.p. adminstration (107 pfu)
GL-ONC1
35
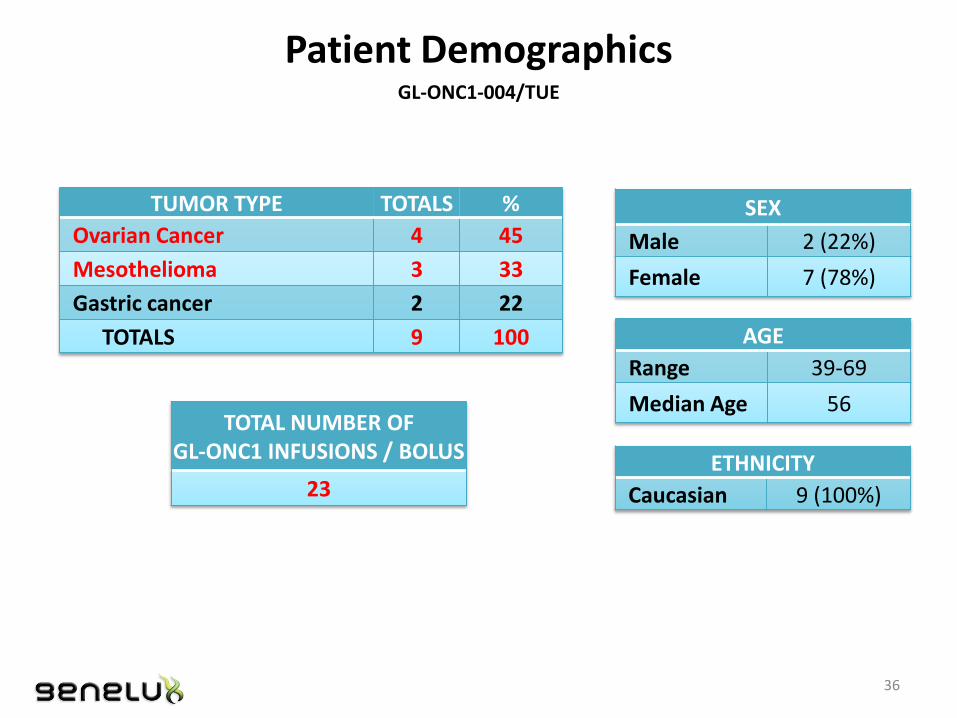
Patient Demographics GL-ONC1-004/TUE
TUMOR TYPE TOTALS %
Ovarian Cancer 4 45
Mesothelioma 3 33
Gastric cancer 2 22
TOTALS 9 100
SEX
Male 2 (22%)
Female 7 (78%)
TOTAL NUMBER OF GL-ONC1 INFUSIONS / BOLUS
23
AGE
Range 39-69
Median Age 56
ETHNICITY
Caucasian 9 (100%)
36

Phase I trial at UCSD Moores Cancer Center
Phase I Trial of Attenuated Vaccinia Virus (GL-ONC1) Delivered Intravenously with Concurrent Cisplatin and Radiotherapy in
Patients with Locoregionally Advanced Head and Neck Carcinoma
Dr. Loren Mell Dr. Sunil Advani Dr. Gregory Daniels
Clinical Investigators
37

Dose-escalation Schedule GL-ONC1-005/UCSD
Phase I
Cohort 1: 3×108 pfu
Cohort 2: 1×109 pfu
Cohort 3: 3×109 pfu
Cohort 4: 3×109 pfu, 2 doses
Cohort -1*: 1×108 pfu
CURRENT
* Necessary only if toxicity is encountered at the initial dose level
Cohort 5: 3×109 pfu, 4 doses
Cohort 6: 3×109 pfu, 6 doses
38

14 Patients (4 Cohorts) Treated GL-ONC1-005/UCSD
TUMOR LOCATION
N %
Larynx 3 21
Hypopharynx 3 21
Base of tongue 2 14
Primary of unknown origin 2 14
Nasopharynx 1 7
Oropharynx 1 7
Adenoid & paranasal sinus 1 7
Parotid gland 1 7
TOTALS 14 100
SEX Male 13
Female 1
AGE
Range 23-77
Median Age 60
ETHNICITY
Caucasian 12 Black or African American
2
TOTAL NUMBER OF GL-ONC1 INFUSIONS / BOLUS
19
39
Phase I Trial at MSKCC
A Phase I Study of intra-pleural administration of GL-ONC1, a genetically modified vaccinia virus, in patients with malignant
pleural effusion: primary, metastases and mesothelioma
Dr. Valerie Rusch Dr. Lee Krug
Clinical Investigators
40

Dose-escalation Schedule GL-ONC1-003/MSK
Phase I
Cohort 1: 1×107 pfu
Cohort 2: 1×108 pfu
Cohort 4: 3×109 pfu
Cohort 3: 1×109 pfu
Cohort -1*: 1×106 pfu
completed
One treatment per cohort
* Necessary only if toxicity is encountered at the initial dose level
41

8 Patients Treated GL-ONC1-003/MSK
TUMOR TYPES
N %
Mesothelioma 9 75
Non-small cell lung cancer 2 17
Breast cancer 1 8
TOTALS 12 100%
SEX
Male 9 (75%)
Female 3 (25%)
TOTAL NUMBER OF GL-ONC1 INFUSIONS
12
42

Safety
Shedding
PK / PD
Infection of tumor tissue/cells
Anti-vaccinia antibody response
Infectivity of baseline tumor biopsy in petri dish
Antitumor response
Key Considerations
43
Is GL-ON1 Viral Therapy Safe?
44

Related Adverse Reactions GL-ONC1-002/MA
AE Term G1 (Mild)
G2 (Moderate)
G3 (Severe)
G4 (Life-
threatening)
Total
Fever 34 8 0 0 42
Lymphopenia 1 6 7 2 16
Fatigue 9 4 0 0 13
Nausea 11 1 0 0 12
Chills 9 2 0 0 11
Increased Gamma-glutamyltransferase (GGT)
4 4 3 0 11
Vomiting 8 3 0 0 11
Hypotension 3 6 0 0 9
Rigors 6 2 0 0 8
Increased Alkaline Phosphatase 3 3 2 0 8
TOTALS 88
(62%) 39
(28%) 12
(9%) 2
(1%) 141
(100%)
45

Related Adverse Reactions GL-ONC1-004/TUE
AE Term G1 (Mild)
G2 (Moderate)
G3 (Severe)
G4 (Life-
threatening)
Total
Increased C-reactive Protein 1 15 0 0 16
Fever 13 3 0 0 16
Decrease in lymphocyte count 0 5 3 0 8
Nausea 7 1 0 0 8
Abdominal pain 4 1 1 0 6
Vomiting 4 0 0 0 4
Flatulence 3 0 0 0 3
Leucocytes increased in ascites 0 0 3 0 3
Chills 2 0 0 0 2
Fatigue 0 0 2 0 2
TOTALS 34
(50%) 25
(37%) 9
(13%) 0
(0%) 68
(100%)
46
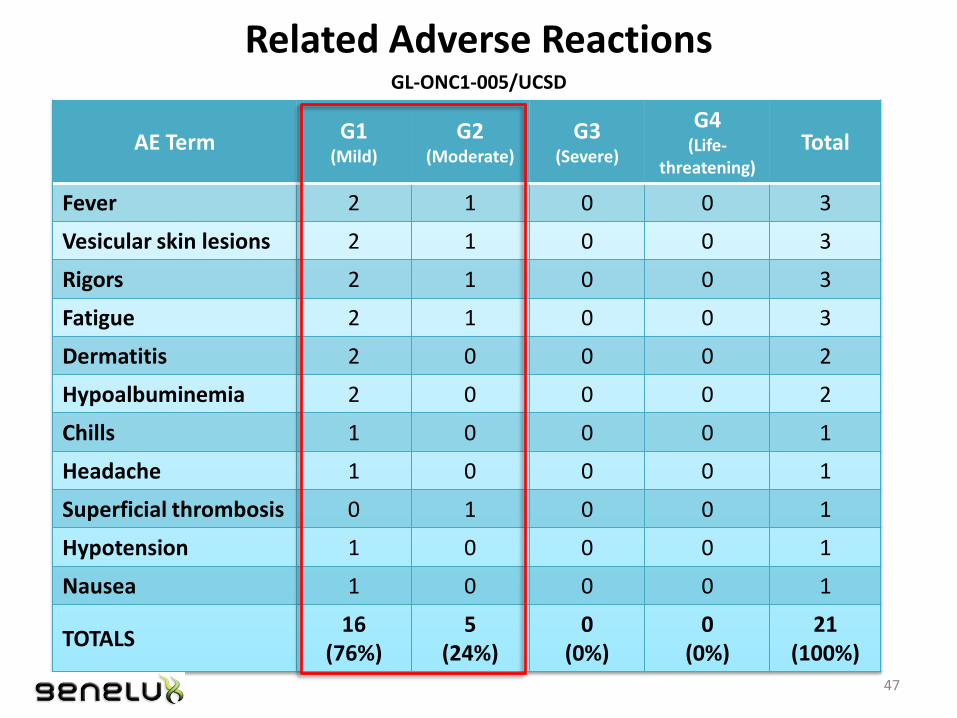
Related Adverse Reactions GL-ONC1-005/UCSD
AE Term G1 (Mild)
G2 (Moderate)
G3 (Severe)
G4 (Life-
threatening)
Total
Fever 2 1 0 0 3
Vesicular skin lesions 2 1 0 0 3
Rigors 2 1 0 0 3
Fatigue 2 1 0 0 3
Dermatitis 2 0 0 0 2
Hypoalbuminemia 2 0 0 0 2
Chills 1 0 0 0 1
Headache 1 0 0 0 1
Superficial thrombosis 0 1 0 0 1
Hypotension 1 0 0 0 1
Nausea 1 0 0 0 1
TOTALS 16
(76%) 5
(24%) 0
(0%) 0
(0%) 21
(100%) 47

Related Adverse Reactions GL-ONC1-003/MSK
Toxicity Definite and Probable G1 G2 G3 G4 # patients
ALT x x 1
Alk phos x x 1
AST x x 1
Chills x 3
Fever x x 4
Flu like symptoms x 3
Headache x 1
Nausea x 1
Pain x 1
Sinus tachycardia x 1
Sweating x 1
48

Does virus shed?
49

Virus Analyses (by VPA) GL-ONC1-005/UCSD
Cohort Patient
Shedding Analysis (by VPA)
Screening Day 4* Day 5* Day 9* Day 10*
U OS U OS U OS U OS U OS
3x108
pfu
501 - - - - - -
502 - - - - - -
503 - - - -
1x109 pfu
504 - - - - - -
506 - - - - - -
507 - - - - - -
3x109
pfu
508 - - - - - -
510 - - - - - -
512 - - - - - -
3x109 pfu
x
2 doses
514 - - - - - -
515 - - - - - - - - - -
516 - - - - - - - - - -
517 - - - - - - - - - -
* Virus treatment on Day 3. U: urine; OS: oral swab Positive values are reported as pfu/300 µL of sample
No shedding of virus in urine or saliva in combination therapy
50

Viral Shedding is Minimal or None
Summary
No to very few viral shedding when delivered i.v., i.pe., or i.pl. No shedding in combination therapy
51

PK / PD
52

GL-ONC1 DNA IN BLOOD DAY(S) AFTER INJECTION - Subsequent Injections Have Similar PK Profile
GL-ONC1-002/MA
Cohorts with multiple doses per cycle
VACV A21L gene.
1
10
Cohort 6
Cohort 7
Cohort 8
Cohort 8a
Co
py N
um
be
r
Cycle 1 Cycle 2
53

Sustained survival & production of virus confirmed GL-ONC1-004/TUE
1,00E-01
1,00E+01
1,00E+03
1,00E+05
1,00E+07
1,00E+09
tota
l p
ful
total pfu of GL-ONC1 in peritoneal fluid of pt 401 (titration assay)
inoculation dosage = 1.0 E+07 pfu
peak >> 1.0 E+08 pfu
lavageascites
> 3 weeks of progeny virus production
viral
Viral output
(intraperitoneal virus replication)
54
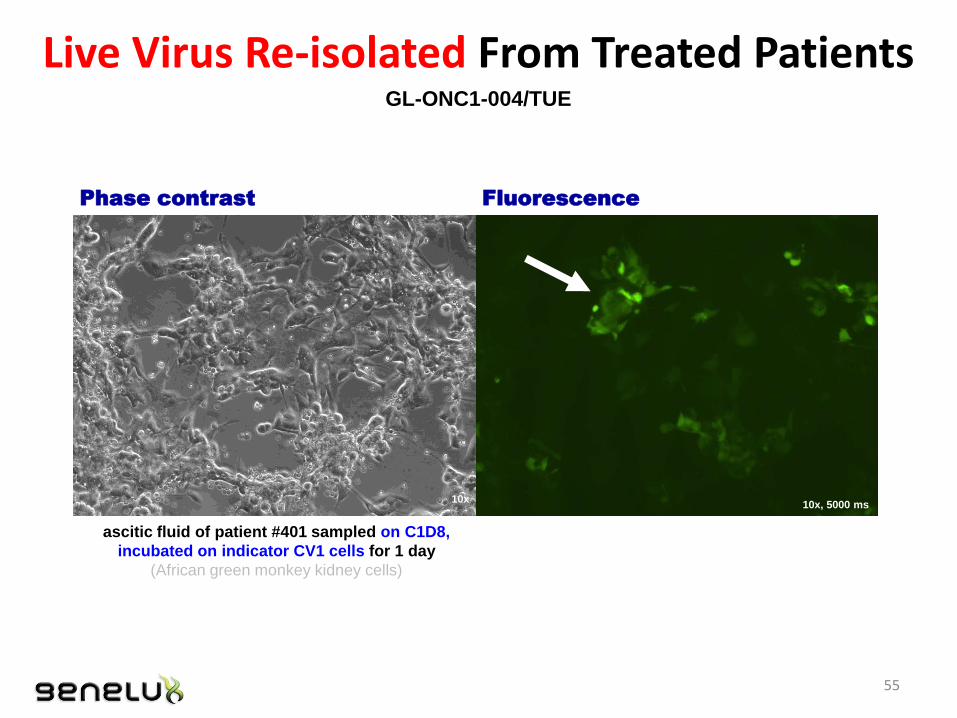
Live Virus Re-isolated From Treated Patients GL-ONC1-004/TUE
ascitic fluid of patient #401 sampled on C1D8,
incubated on indicator CV1 cells for 1 day
(African green monkey kidney cells)
Phase contrast Fluorescence
10x, 5000 ms 10x
55
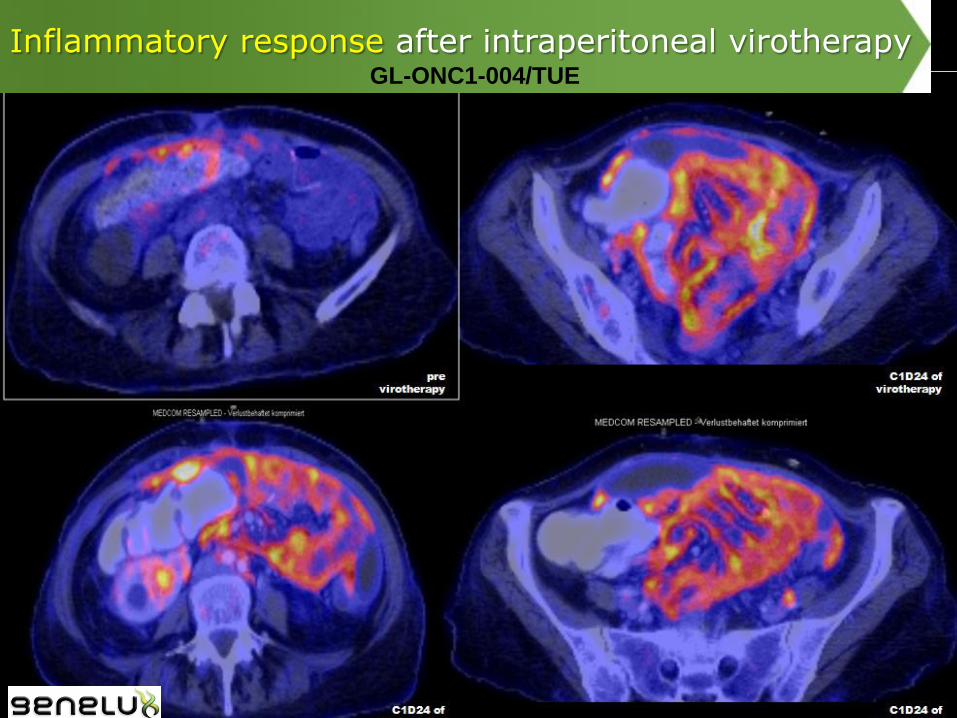
Inflammatory response after intraperitoneal virotherapy GL-ONC1-004/TUE
Cohorts with single dose per cycle Cohorts with multiple doses per cycle
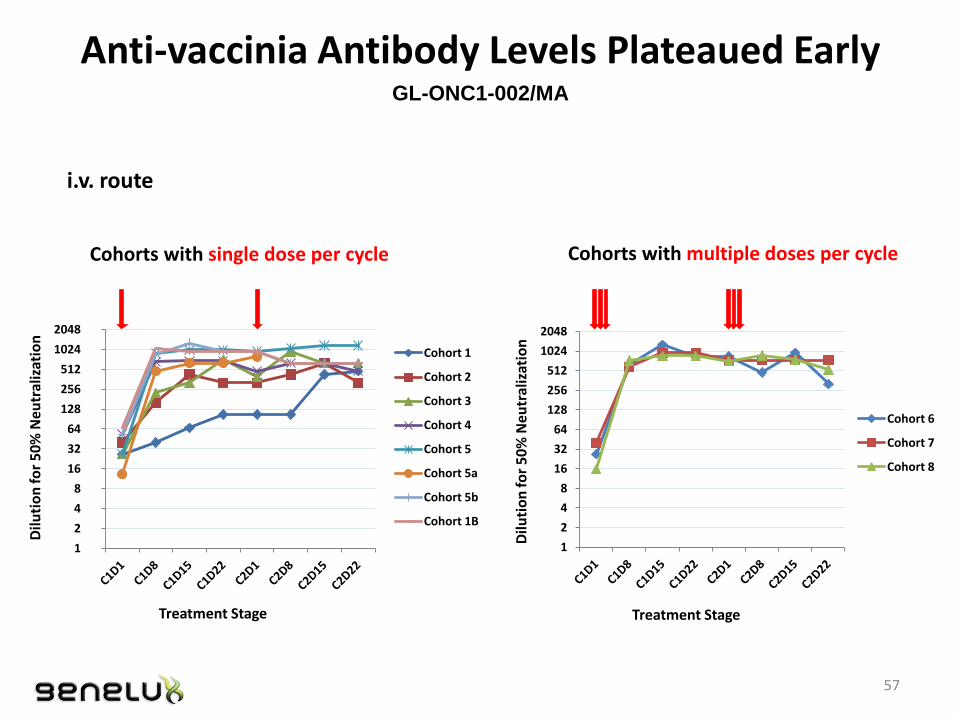
Anti-vaccinia Antibody Levels Plateaued Early GL-ONC1-002/MA
i.v. route
1
2
4
8
16
32
64
128
256
512
1024
2048
Dilu
tio
n fo
r 5
0%
Neu
tral
izat
ion
Cohort 1
Cohort 2
Cohort 3
Cohort 4
Cohort 5
Cohort 5a
Cohort 5b
Cohort 1B
1
2
4
8
16
32
64
128
256
512
1024
2048
Dilu
tio
n fo
r 5
0%
Ne
utr
aliz
atio
n
Cohort 6
Cohort 7
Cohort 8
Treatment Stage Treatment Stage
57

Does virus infect tumor tissue/cells?
58

Pt. # Tumor type Cohort GFP IHC Viral Plaque Assay
1 MPM1 epithelioid 1 (-) (+) (+)
2 NSCLC2 1 (-) (-) (-)
3 MPM epithelioid 1 (-) (+) (-)
4 MPM epithelioid 1 (-) N/A (-)
5 MPM epithelioid 2 (-) (-) (-)
6 MPM epithelioid 2 (+) (-) (-)
7 NSCLC 2 (-) N/A
8 MPM epithelioid 3 (-) (-) (+)
9 MPM epithelioid 3 (+) (+) (-)
10 MPM epithelioid 3 (+) (+) (-)
11 MPM sarcomatoid 4 (-) (-) (-)
12 Breast cancer 4 (-) Pending (-)
1 MPM: Malignant pleural mesothelioma 2 NSCLC: Non-small cell lung cancer
GL-ONC1 Effectively Infects Mesothelioma Tumors
59
GL-ONC1-003/MSK

Positive virus-encoded GFP in Mesothelioma biopsy
Positive IHC of GL-ONC1 in Mesothelioma biopsy
GL-ONC1 Effectively Infects Mesothelioma Tumors
60
GL-ONC1-003/MSK

H & N squamous cell carcinoma biopsy (Pt. 204 - C4D15)
Viral Colonization in Tumor Biopsy Confirmed by IHC GL-ONC1-002/MA
i.v. route
61

UDA= User defined Assay. GFP signal detection.
Virus-infected CTC
Virus-infected CTC
Patient 127 - C1D8 Colorectal cancer with liver metastases
GFP+ CTCs were also found in pt. #129, 135, 136, & 305
CTCs were Infected by GL-ONC1 Virus - Confirmed by GFP imaging (real-time monitoring of therapy)
GL-ONC1-002/MA
62

Evidence of antitumor activities & clinical benefits
63

Diagnosis Cohort
#
Dose Conc. in
pfu/cycle
# of
Cycles
# of Known
Wks of Stable
Disease (SD)
Met. Hurtle cell carcinoma thyroid, lung 1 1 × 105 6 24
Parotid adenocystic tumor, lung mets 2 1 ×106 6 12
H & N squamous cell carcinoma, lung mets 3 1 ×107 8 24
Esophageal carcinoma 5 1 × 109 6 24
Colorectal carcinoma, lung mets 5 1 × 109 5 12
H & N squamous cell carcinoma, lung mets 6 5 × 107 5 12
Myxoid chondrosarcoma, multiple lung mets 7 5 × 108 6 48
Colorectal cancer (adenocarcinoma), liver
metastases 5a 1 × 109 1 8
Metastatic renal cell carcinoma, lung mets 5b 3 × 109 5 12
Cholangiocarcinoma 8 5 × 109 5 12
NSCLC 8 5 × 109 5 12
Adenocarcinoma of the appendix 8b 5 × 109 8 13
Esophageal carcinoma, lung mets 8c 5 × 109 6 13
13 of 27 Evaluable Pts with Stable Disease
SD based on CT scans 64
GL-ONC1-002/MA

Pre-treatment
Post-treatment
GL-ONC1 (Ch 8) Cholangiocarcinoma
Tumor growth slowed
Treatment Benefit / Preliminary evidence of tumor response
65

Pt. 133 Tumor sizes
0
10
20
30
40
50
60
01/04/
2012
01/05/
2012
01/06/
2012
01/07/
2012
01/08/
2012
01/09/
2012
01/10/
2012
01/11/
2012
Tum
or
lon
gest
dia
me
ters
(m
m)
Pre-treatment
Post-treatment
MAPPING study (Pazopinib vs placebo)
GL-ONC1 (Ch 8)
NSCLC
Tumor growth slowed
Treatment Benefit / Preliminary evidence of tumor response
66

• 43-yr old man; metastatic mucinous adenocarcinoma of the appendix and progressive peritoneal bowel disease;
• Tolerated 8 cycles of viral treatment (4 × 1010 pfu of GL-ONC1 total);
• Clinical signs of treatment benefit reported by Patient & Physician:
Reduction in abdominal pain: 6-8 hrs 2-3 hrs;
Reduced pain medication;
Soften of abdominal mass by palpation.
• Additional GL-ONC1 treatment given:
Dr. Mazhar Ajaz to UK’s GTAC: “The patient has been desperate to continue
beyond his scheduled six cycles of treatment because of the perceived benefit.”
Patient is still alive at last time of contact.
Cohort 8b Pt. 307: Treatment benefit observed
- 5 x 109 pfu: Highest dose of single i.v. infusion
67

Overall survival of patients in SD vs. PD group GL-ONC1-002/MA
0.00
5.00
10.00
15.00
20.00
25.00
30.00
35.00
40.00
Nu
mb
er o
f M
on
ths
Evaluable Patients in Phase I, Phase IB & 8
Overall Survival in months as of 12-Feb-14
PD
SD
OS (mons)
PD Mean 7.73 Median 7.82
SD Mean 14.40 Median 10.99
Remission
0 5 10 15 20 25 30 35 40
0
20
40
60
80
100
OS Time in Months
Su
rviv
al p
rob
ab
ility
(%
)
Group
PD
SD
68

As of Oct.9, 2014
GL-ONC1-005/UCSD: BEST OVERALL RESPONSES
Ch Pt. # Disease Type HPV Stage BOR at Wk 23
(PET/CT)
Duration of BOR
(mos)
Current Status
OS Time in mos as of Oct.9, 2014
1
501 Base of tongue, squamous carcinoma Negative IV A CR 28.1 CR 28.1 mos & ong. 502 Hypopharynx, squamous carcinoma Negative IV A CR 13 PD 26.6 mos & ong.
503 Paranasal sinus, adenoid cystic carcinoma
Negative IV B PR @ 6m 23.7 Min. disease 23.7 mos & ong.
2
504 Glottic larynx Negative IV A CR 21.7 CR 21.7 mos & ong
506 Nasopharynx Negative IV B CR 18.9 CR 18.9 mos & ong.
507 Hypopharynx Negative IV A PD 4 Deceased 17.5 mos & ong.
3 508 Hypopharynx, squamous carcinoma Positive IV A CR 18.8 CR 18.8 mos & ong. 510 Hypopharynx, squamous carcinoma Negative IV A CR 16.7 CR 16.7 mos & ong. 512 Supraglottic larynx, squamous carcinoma Negative IV A CR 16.3 CR 16.3 mos & ong.
4
514 Larynx Negative IV A PR 4 Deceased 8 mos 515 Neck mass of unknown primary origin Positive IV A CR 15.4 CR 15.4 mos & ong. 516 Oropharynx carcinoma Positive IV B CR 13.8 CR 13.8 mos & ong. 517 Neck mass of unknown primary origin Positive IV A PR 9.1 PR 9.1 mos & ong.
518 Cancer of parotid gland Negative IV B N/A 4.9 Deceased 4.9 mos
519 Tongue, squamous carcinoma Negative IV B PR at W 15 In FU (D 150) PR 5.0 mos & ong.
5 521 Supraglottic larynx, squamous Negative IV A Pending In FU (D 129) Pending 4.4 mos & ong.
522 Tongue, squamous carcinoma Negative IV A Pending In Tx (D 24) Pending 0.9 mos & ong.
Red - Pending Green – CR (complete response) HPV – Human papillomavirus PR – partial response Black - PD (progressive disease) BOR – best overall response

Clinical Response – 501 (Base of Tongue)
Baseline 3 Mo Post-Treatment
Baseline 4 Mo Post-Treatment
Endoscopy
Imaging
70

Clinical Response – 502 (Hypopharynx)
Baseline 3 Mo Post-Treatment
Baseline 4 Mo Post-Treatment
Endoscopy
Imaging
71

Patient 503: ● 77 yr-old woman; ● diagnosed on 9/11/12 with adenoid cystic carcinoma, paranasal sinus; ● Stage IVB, HPV–; T4B N0 M0.
Treatment:
• Received first RT+Cisplatin on October 29, 2012.
• 3 × 108 pfu GL-ONC1 i.v. on October 31, 2012.
• Completed the trial per protocol on April 3, 2013.
• Week 23 CT on April 3, 2013 showed partial response (PR)
72
CASE STUDY: UCSD PATIENT (503) – HPV NEGATIVE: CONVERSION FROM PARTIAL TO COMPLETE RESPONSE
Baseline
4-mo PET/CT
Tumor

Baseline PR @ Week 23
Minimal Disease @ Month 16.5
March 5, 2014: 16.5 mo. from enrollment, and no further treatment, patient showed only minimal disease. Conversion from Partial to Complete Response
CASE STUDY: UCSD PATIENT (503) – HPV NEGATIVE: CONVERSION FROM PARTIAL TO COMPLETE RESPONSE

Cohorts & Pt. #
Mesothelioma subtype
Baseline Disease Status (prior Tx)
Post-GL-ONC1 Other Anti-cancer
Survival Status
OS since Date of Diagnosis (Mos)
1
001 epithelioid Newly diagnosed Surgery; RT + Chemo Alive 21.5
003 epithelioid Newly diagnosed None Alive 20.8
004 epithelioid Newly diagnosed Chemo + RT; Surgery Alive 17.3
2
005 epithelioid Newly diagnosed Surgery;
Chemo + RT Alive 16.6
006 epithelioid Newly diagnosed Surgery; Chemo
Alive 17.3
3
008 epithelioid Newly diagnosed Chemo + RT Alive 15.5
009 epithelioid Newly diagnosed Chemo + RT Alive 14.6
010 epithelioid SD
(Carboplatin, Pemetrexed)
None Alive 14.6
Median For epithelioid
17.0
4 011 sarcomatoid Newly diagnosed N/A Deceased 3.7
014 biphasic Newly diagnosed None Deceased 6.1
Survival of Mesothelioma Pts
As of Oct.23, 2014 74

Antitumor activity shown in “fluid” biopsy - Analyses of ascites or peritoneal lavage
% of total cells Day 4 Day 8 Day 22 Day 59
Tumor cells 5 % < 2 % 0 % 0 %
Virus-infected tumor cells 5-10 % 90 % 0 % 0 %
At C1D8 significant reduction of ascitic malignant cells; increased % of GL-ONC1 infected tumor cells
Following C1D22 no longer detection of tumor cells in peritoneal lavage
GL-ONC1-004/TUE
Example:
75

Summary of Key Considerations (all human trials)
Safety:
Multiple doses of GL-ONC1 treatments delivered by different routes are well tolerated (294 infusions in 83 patients)
5 × 109 pfu single i.v. dose in human pt. well tolerated
MTD not reached in any of the trials
Shedding: Minimal to none
Systemic & regional delivery: Yes
Infection of tumor tissue/cells: Yes
Antibody response: Yes; plateau rapidly (i.v.)
Infectivity of baseline tumor biopsy in petri dish: Yes
Antitumor response: Yes, clinical benefit also observed
76

GL-ONC1
Oncolysis
Innate & Adaptive Immune
Activation
Dual-Mechanism of Action: Tumor cell lysis and activation of antitumor immunity
77

The Potential of Immunotherapy
Has the potential to achieve complete, long-lasting remissions and cancer cures, with few or no side effects, and for any cancer patient, regardless of their cancer type. - www.cancerresearch.org
78

Cancer Immunotherapy - the New Movement
Cancer immunotherapy—treatments that harness and enhance the innate powers of the immune system to fight cancer—represents the most promising new cancer treatment approach since the development of the first chemotherapies in the late 1940s. - www.cancerresearch.org
“Immunotherapies will likely become the treatment backbone in up to 60% of cancers over the next 10 years compared with <3% today.” Andrew Baum, MD Citigroup Global Health
Immunotherapy -The Beginning of the End for Cancer: Transforming Cancer into Chronic Disease
79
• Sophisticated clinical trial design
• Rich discovery and pre-clinical pipeline
• Robust intellectual property portfolio
• Diversified strategic opportunities
Genelux is Poised for Success
Our mission is to deliver a powerful, targeted and sustained attack on cancer …wherever it may reside
80

Illuminating Hope in the Fight Against Cancer
Thank You!
38
















![ORIGINAL RESEARCH Open Access Effects of internal low-dose … · 2017. 8. 24. · Iodine-131 [131I] is part of the uranium decay scheme and may be released into the environment by](https://static.documents.pub/doc/80x56/610237ef10574120875471d1/original-research-open-access-effects-of-internal-low-dose-2017-8-24-iodine-131.jpg)
