maging of Blunt Abdominal Trauma. Luana Stanescu, MD, Joel A. Gross, MD, Michelle Bittle, MD, and F.A. Mann, MD
rdTfhoso
tcmidcsfip(rt
naiIihnrrpnt
IIHliua
solated blunt abdominal trauma (BAT) represents about5% of annual trauma mortality from blunt trauma. As part
f multiple-site injury (polytrauma), BAT contributes an-ther 15% of trauma mortality.1 Exsanguination accounts for0 to 90% of acute deaths from abdominal injury. More than5% of such cases are amenable to surgery, and recent yearsave seen safe extension of nonoperative, image-guidedreatments to most victims of blunt-force trauma.2-21 Earlyecognition and treatment decisions have been greatly im-acted by increasingly sophisticated cross-sectional imagingnd image-guided, minimally invasive therapies.22-32
lunt Disruptionsf the Diaphragm,bdominal Wall, and Flank
he diagnosis of diaphragm rupture is often missed. A highndex of suspicion for diaphragmatic ruptures is warranted inppropriate clinical circumstances, such as lateral impact ve-icle crashes, especially when left-sided, and direct frontal
mpacts. Classical findings are present in less than 40% ofeft-sided and less than 15% of right-sided diaphragm rup-ures.33-37 Diagnostic peritoneal lavage (DPL) is falsely nega-ive in 10 to 15% of cases.37-41
Delayed diagnoses are not uncommon: 10 to 15% of casesresent with more than 24 hours delay,33,35,37,42 especially ifhe commonly associated intrathoracic (�90%) and intraab-ominal (�60%) injuries require endotracheal intubationnd positive-pressure ventilation.37,43 It is believed that theositive intrathoracic pressure prevents or limits herniationf abdominal contents through the diaphragm. New, unilat-ral “elevation” of hemidiaphragm following extubation mayepresent herniation of abdominal contents through a previ-usly unrecognized diaphragm rupture.Conventional radiography (chest radiographs with enteral
ube placement; fluoroscopy) is abnormal in 60 to 90% ofcute traumatic diaphragmatic ruptures, but most findingsre nonspecific and cannot be distinguished from hemotho-
arborview Medical Center, University of Washington, Seattle, Washing-ton.
ax, atelectasis, etc. Sensitivity is 46% in detecting left-sidediaphragm ruptures and only 17% for right-sided ruptures.44
here are two classical chest radiographic findings describedor diaphragmatic rupture: intrathoracical herniation of aollow viscus, with or without a collar sign (narrowed waistf a herniated intraabdominal organ due to compression as itqueezes through the diaphragmatic rupture), and detectionf a nasogastric tube above the left hemidiaphragm.45
In case series reports, diagnostic accuracy of computedomography (CT) was equivalent, but not clearly superior, toonventional radiographic techniques.46 Thin-cut CT withultiplanar reformations is expected to improve sensitiv-
ty.47 At CT, the so-called “dependent viscera” sign (intraab-ominal contents abutting the posterior thoracic wall, espe-ially where the scan level is in the upper third of the liver orpleen) and the “collar” sign are nearly 100% specific. Otherndings, such as the “discontinuous” and thickened dia-hragm signs, show intermediate sensitivity and specificity40 to 75%).46,48 Among reported series in which magneticesonance imaging (MRI) depicted no diaphragmatic disrup-ions, no delayed diagnoses have been reported.49-51
Injuries to the muscles and fascia surrounding the perito-eum may result in three types of injuries: the most commonre type I, small defects, usually located in the lower abdom-nal wall secondary to bicycle handlebar blunt trauma. TypeI includes larger abdominal wall defects after high-energynjuries like motor vehicle accident (MVA) or a fall fromeight, while type III are associated with intraabdominal her-iations in the retroperitoneum following deceleration inju-ies.52 Contained hematomas also occur and do not typicallyequire intervention, but may require embolization for ex-anding hematomas.53-55 High-energy abdominal wall her-ias, open or closed, almost always require surgical interven-ion.56-62
njuries to the Solidntraperitoneal Organsemodynamic instability and evidence of on-going blood
oss are the strongest indicators for the need of interventionn spleen and liver injuries.8,24,63 Among hemodynamicallynstable patients that are not taken immediately to the oper-ting suite, focused abdominal sonography for trauma
FAST) and DPL are diagnostically equivalent in detecting
sot
neht
ldcCt
p(mp
tam
haaPn
.
Imaging of blunt abdominal trauma 197
urgically important intraperitoneal hemorrhage due to solidrgan injury(ie, selecting patients in whom laparotomy isherapeutic).64
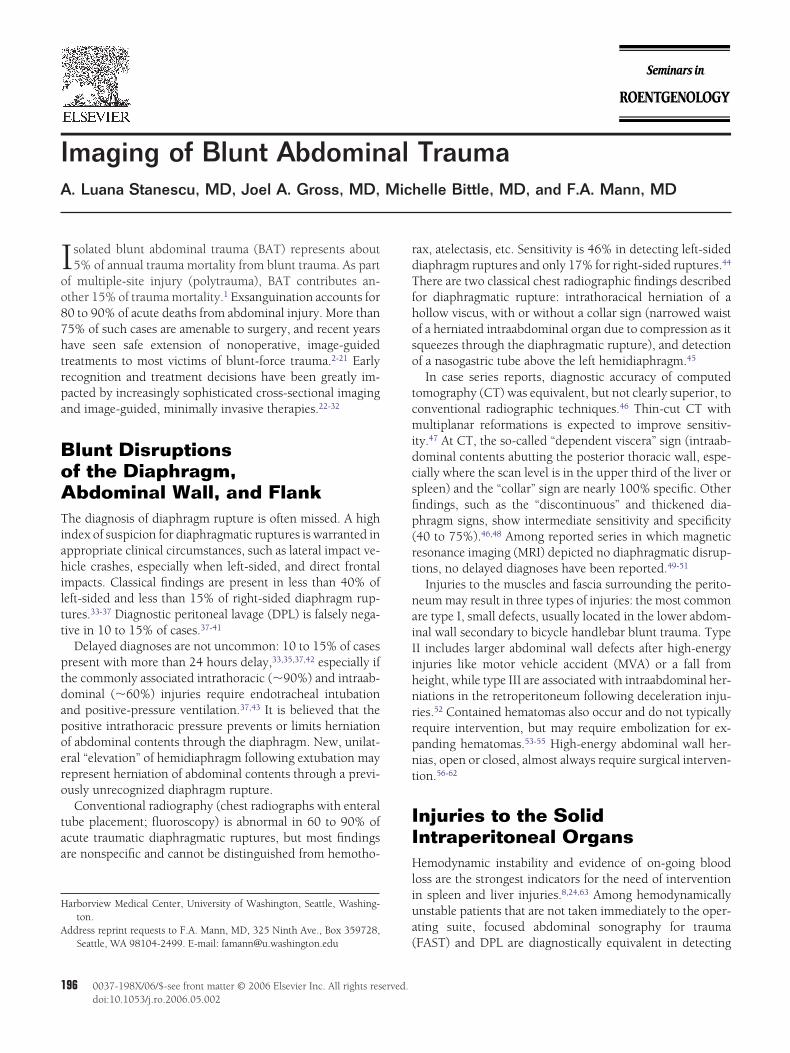
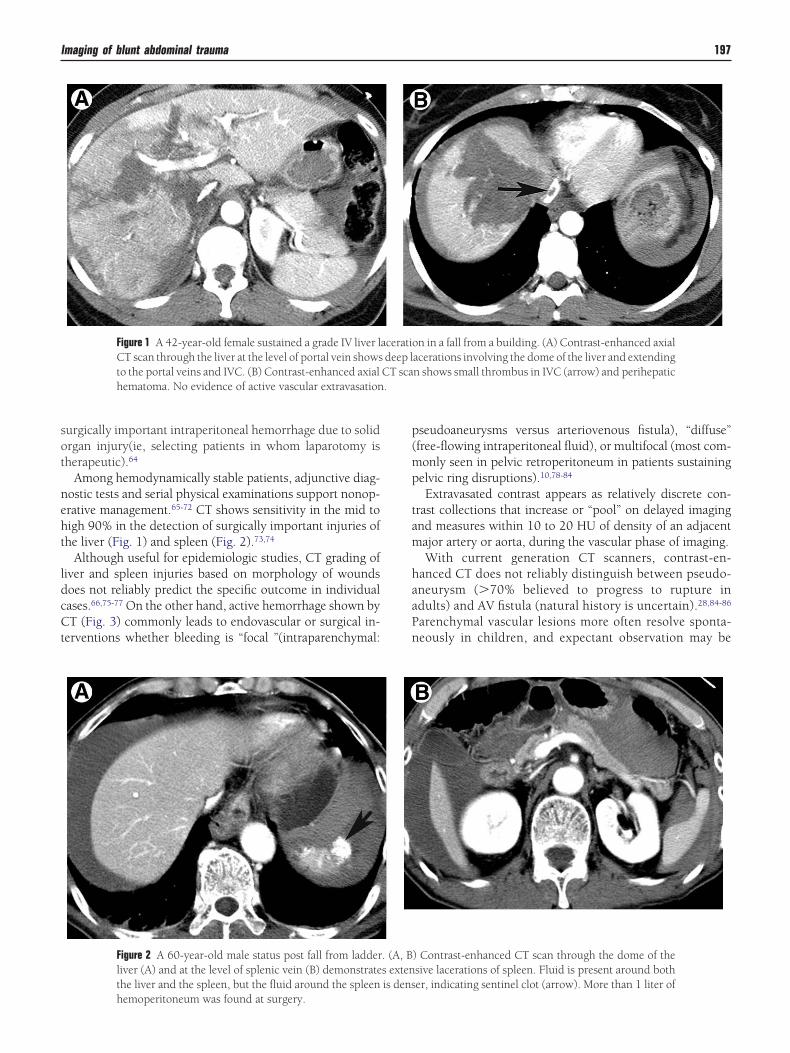
Among hemodynamically stable patients, adjunctive diag-ostic tests and serial physical examinations support nonop-rative management.65-72 CT shows sensitivity in the mid toigh 90% in the detection of surgically important injuries ofhe liver (Fig. 1) and spleen (Fig. 2).73,74
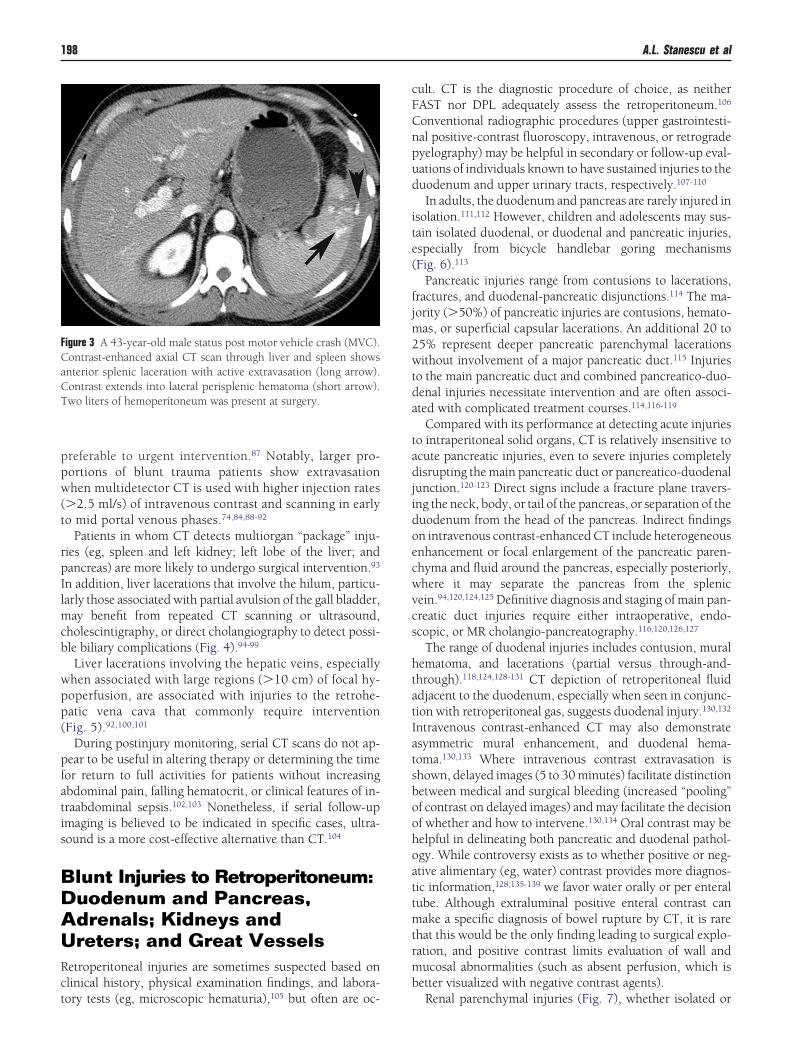
Although useful for epidemiologic studies, CT grading ofiver and spleen injuries based on morphology of woundsoes not reliably predict the specific outcome in individualases.66,75-77 On the other hand, active hemorrhage shown byT (Fig. 3) commonly leads to endovascular or surgical in-
erventions whether bleeding is “focal ”(intraparenchymal:
Figure 1 A 42-year-old female sustained a grade IV liver lCT scan through the liver at the level of portal vein showsto the portal veins and IVC. (B) Contrast-enhanced axialhematoma. No evidence of active vascular extravasation
Figure 2 A 60-year-old male status post fall from ladderliver (A) and at the level of splenic vein (B) demonstratethe liver and the spleen, but the fluid around the spleen
hemoperitoneum was found at surgery.
seudoaneurysms versus arteriovenous fistula), “diffuse”free-flowing intraperitoneal fluid), or multifocal (most com-only seen in pelvic retroperitoneum in patients sustainingelvic ring disruptions).10,78-84
Extravasated contrast appears as relatively discrete con-rast collections that increase or “pool” on delayed imagingnd measures within 10 to 20 HU of density of an adjacentajor artery or aorta, during the vascular phase of imaging.With current generation CT scanners, contrast-en-
anced CT does not reliably distinguish between pseudo-neurysm (�70% believed to progress to rupture indults) and AV fistula (natural history is uncertain).28,84-86
arenchymal vascular lesions more often resolve sponta-eously in children, and expectant observation may be
n in a fall from a building. (A) Contrast-enhanced axialacerations involving the dome of the liver and extendingn shows small thrombus in IVC (arrow) and perihepatic
) Contrast-enhanced CT scan through the dome of thesive lacerations of spleen. Fluid is present around bother, indicating sentinel clot (arrow). More than 1 liter of
aceratiodeep lCT sca
. (A, Bs extenis dens
ppw(t
rpIlmcb
wpp(
pfatis
BDAURct
cFCnpud
ite(
fjm2wtda
tadjidoecwvcs
htatIatsboohoattmtrmb
FCaCT
198 A.L. Stanescu et al
referable to urgent intervention.87 Notably, larger pro-ortions of blunt trauma patients show extravasationhen multidetector CT is used with higher injection rates
�2.5 ml/s) of intravenous contrast and scanning in earlyo mid portal venous phases.74,84,88-92
Patients in whom CT detects multiorgan “package” inju-ies (eg, spleen and left kidney; left lobe of the liver; andancreas) are more likely to undergo surgical intervention.93
n addition, liver lacerations that involve the hilum, particu-arly those associated with partial avulsion of the gall bladder,
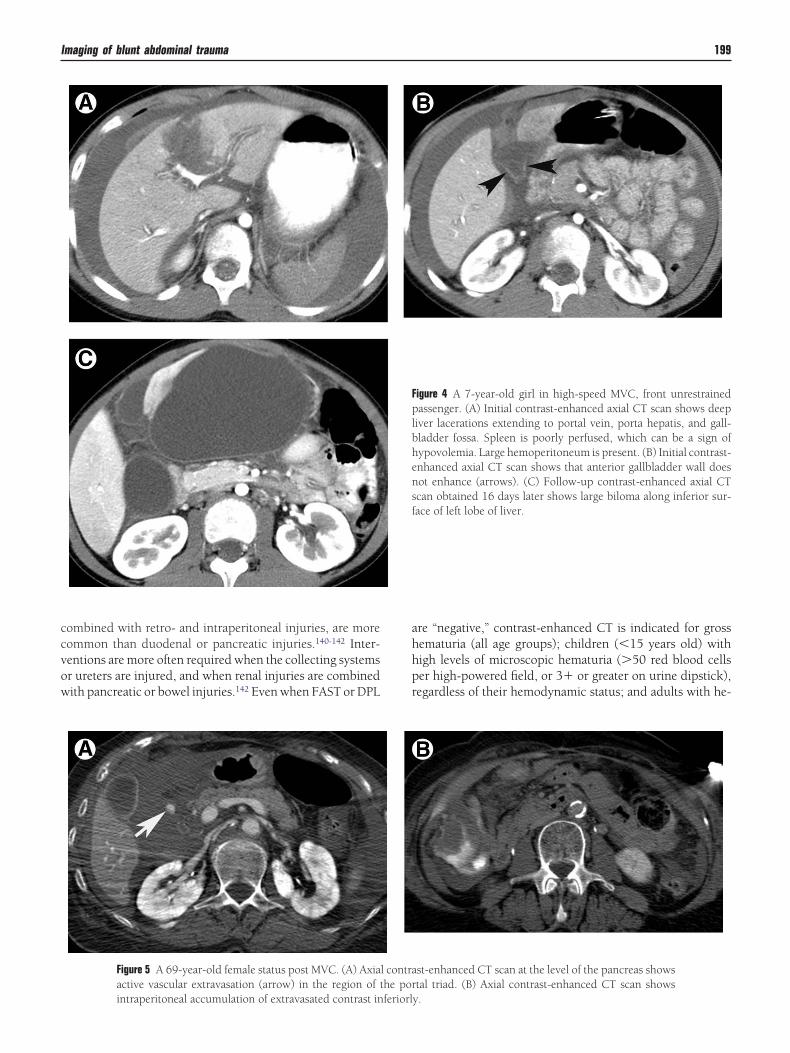
ay benefit from repeated CT scanning or ultrasound,holescintigraphy, or direct cholangiography to detect possi-le biliary complications (Fig. 4).94-99
Liver lacerations involving the hepatic veins, especiallyhen associated with large regions (�10 cm) of focal hy-operfusion, are associated with injuries to the retrohe-atic vena cava that commonly require interventionFig. 5).92,100,101
During postinjury monitoring, serial CT scans do not ap-ear to be useful in altering therapy or determining the timeor return to full activities for patients without increasingbdominal pain, falling hematocrit, or clinical features of in-raabdominal sepsis.102,103 Nonetheless, if serial follow-upmaging is believed to be indicated in specific cases, ultra-ound is a more cost-effective alternative than CT.104
lunt Injuries to Retroperitoneum:uodenum and Pancreas,drenals; Kidneys andreters; and Great Vessels
etroperitoneal injuries are sometimes suspected based onlinical history, physical examination findings, and labora-
igure 3 A 43-year-old male status post motor vehicle crash (MVC).ontrast-enhanced axial CT scan through liver and spleen showsnterior splenic laceration with active extravasation (long arrow).ontrast extends into lateral perisplenic hematoma (short arrow).wo liters of hemoperitoneum was present at surgery.
ory tests (eg, microscopic hematuria),105 but often are oc-
ult. CT is the diagnostic procedure of choice, as neitherAST nor DPL adequately assess the retroperitoneum.106
onventional radiographic procedures (upper gastrointesti-al positive-contrast fluoroscopy, intravenous, or retrogradeyelography) may be helpful in secondary or follow-up eval-ations of individuals known to have sustained injuries to theuodenum and upper urinary tracts, respectively.107-110
In adults, the duodenum and pancreas are rarely injured insolation.111,112 However, children and adolescents may sus-ain isolated duodenal, or duodenal and pancreatic injuries,specially from bicycle handlebar goring mechanismsFig. 6).113
Pancreatic injuries range from contusions to lacerations,ractures, and duodenal-pancreatic disjunctions.114 The ma-ority (�50%) of pancreatic injuries are contusions, hemato-
as, or superficial capsular lacerations. An additional 20 to5% represent deeper pancreatic parenchymal lacerationsithout involvement of a major pancreatic duct.115 Injuries
o the main pancreatic duct and combined pancreatico-duo-enal injuries necessitate intervention and are often associ-ted with complicated treatment courses.114,116-119
Compared with its performance at detecting acute injurieso intraperitoneal solid organs, CT is relatively insensitive tocute pancreatic injuries, even to severe injuries completelyisrupting the main pancreatic duct or pancreatico-duodenal
unction.120-123 Direct signs include a fracture plane travers-ng the neck, body, or tail of the pancreas, or separation of theuodenum from the head of the pancreas. Indirect findingsn intravenous contrast-enhanced CT include heterogeneousnhancement or focal enlargement of the pancreatic paren-hyma and fluid around the pancreas, especially posteriorly,here it may separate the pancreas from the splenicein.94,120,124,125 Definitive diagnosis and staging of main pan-reatic duct injuries require either intraoperative, endo-copic, or MR cholangio-pancreatography.116,120,126,127
The range of duodenal injuries includes contusion, muralematoma, and lacerations (partial versus through-and-hrough).118,124,128-131 CT depiction of retroperitoneal fluiddjacent to the duodenum, especially when seen in conjunc-ion with retroperitoneal gas, suggests duodenal injury.130,132
ntravenous contrast-enhanced CT may also demonstratesymmetric mural enhancement, and duodenal hema-oma.130,133 Where intravenous contrast extravasation ishown, delayed images (5 to 30 minutes) facilitate distinctionetween medical and surgical bleeding (increased “pooling”f contrast on delayed images) and may facilitate the decisionf whether and how to intervene.130,134 Oral contrast may beelpful in delineating both pancreatic and duodenal pathol-gy. While controversy exists as to whether positive or neg-tive alimentary (eg, water) contrast provides more diagnos-ic information,128,135-139 we favor water orally or per enteralube. Although extraluminal positive enteral contrast canake a specific diagnosis of bowel rupture by CT, it is rare
hat this would be the only finding leading to surgical explo-ation, and positive contrast limits evaluation of wall anducosal abnormalities (such as absent perfusion, which is
etter visualized with negative contrast agents).
Renal parenchymal injuries (Fig. 7), whether isolated or
ccvow
ahhpr
Imaging of blunt abdominal trauma 199
ombined with retro- and intraperitoneal injuries, are moreommon than duodenal or pancreatic injuries.140-142 Inter-entions are more often required when the collecting systemsr ureters are injured, and when renal injuries are combinedith pancreatic or bowel injuries.142 Even when FAST or DPL
Figure 5 A 69-year-old female status post MVC. (A) Axiaactive vascular extravasation (arrow) in the region of t
intraperitoneal accumulation of extravasated contrast inferiorl
re “negative,” contrast-enhanced CT is indicated for grossematuria (all age groups); children (�15 years old) withigh levels of microscopic hematuria (�50 red blood cellser high-powered field, or 3� or greater on urine dipstick),egardless of their hemodynamic status; and adults with he-
igure 4 A 7-year-old girl in high-speed MVC, front unrestrainedassenger. (A) Initial contrast-enhanced axial CT scan shows deep
iver lacerations extending to portal vein, porta hepatis, and gall-ladder fossa. Spleen is poorly perfused, which can be a sign ofypovolemia. Large hemoperitoneum is present. (B) Initial contrast-nhanced axial CT scan shows that anterior gallbladder wall doesot enhance (arrows). (C) Follow-up contrast-enhanced axial CTcan obtained 16 days later shows large biloma along inferior sur-ace of left lobe of liver.
st-enhanced CT scan at the level of the pancreas showstal triad. (B) Axial contrast-enhanced CT scan shows
Fplbhensf
l contrahe por
y.
mct
idptnrprag
uamwatp
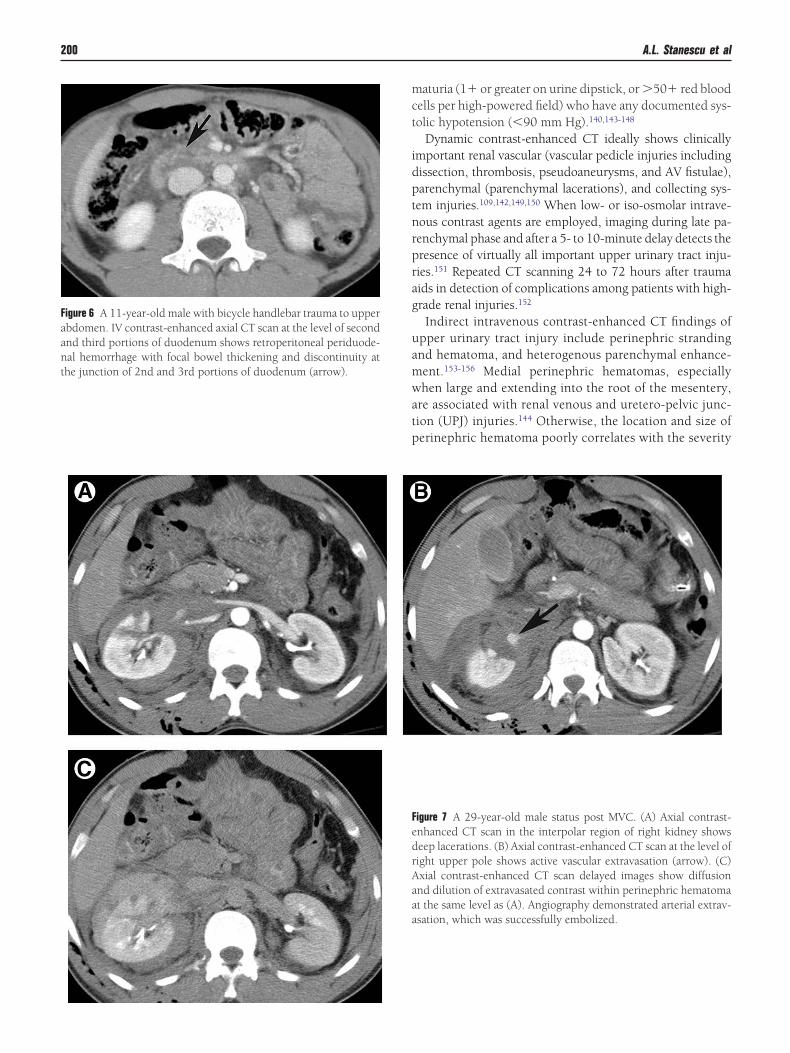
Faanthe junction of 2nd and 3rd portions of duodenum (arrow).
200 A.L. Stanescu et al
aturia (1� or greater on urine dipstick, or �50� red bloodells per high-powered field) who have any documented sys-olic hypotension (�90 mm Hg).140,143-148
Dynamic contrast-enhanced CT ideally shows clinicallymportant renal vascular (vascular pedicle injuries includingissection, thrombosis, pseudoaneurysms, and AV fistulae),arenchymal (parenchymal lacerations), and collecting sys-em injuries.109,142,149,150 When low- or iso-osmolar intrave-ous contrast agents are employed, imaging during late pa-enchymal phase and after a 5- to 10-minute delay detects theresence of virtually all important upper urinary tract inju-ies.151 Repeated CT scanning 24 to 72 hours after traumaids in detection of complications among patients with high-rade renal injuries.152
Indirect intravenous contrast-enhanced CT findings ofpper urinary tract injury include perinephric strandingnd hematoma, and heterogenous parenchymal enhance-ent.153-156 Medial perinephric hematomas, especiallyhen large and extending into the root of the mesentery,
re associated with renal venous and uretero-pelvic junc-ion (UPJ) injuries.144 Otherwise, the location and size oferinephric hematoma poorly correlates with the severity
igure 7 A 29-year-old male status post MVC. (A) Axial contrast-nhanced CT scan in the interpolar region of right kidney showseep lacerations. (B) Axial contrast-enhanced CT scan at the level ofight upper pole shows active vascular extravasation (arrow). (C)xial contrast-enhanced CT scan delayed images show diffusionnd dilution of extravasated contrast within perinephric hematomat the same level as (A). Angiography demonstrated arterial extrav-sation, which was successfully embolized.
igure 6 A 11-year-old male with bicycle handlebar trauma to upperbdomen. IV contrast-enhanced axial CT scan at the level of secondnd third portions of duodenum shows retroperitoneal periduode-al hemorrhage with focal bowel thickening and discontinuity at
FedrAaaa
ols
iuoootafl
cttpcdwa
wumfcil
tmc
ttpicfia
Imaging of blunt abdominal trauma 201
f parenchymal injury or the need to intervene. However,arge subcapsular hematomas can be associated with sub-equent hypertension (Page kidney).157
Direct intravenous contrast-enhanced CT findings of renalnjury include parenchymal lacerations and vascular and/orrinary extravasations; the latter two necessitate interventionr follow-up imaging.144,156,158 The frequency, timing, andptimal methods for follow-up examination remain subjectsf debate. Our practice is to perform a portal venous phase ofhe abdomen and pelvis, followed by 10-minute delayed im-ges in patients with renal injuries or where unexplaineduid is found adjacent to the kidney, ureter, or bladder.Bladder ruptures may be intra- or extraperitoneal, or a
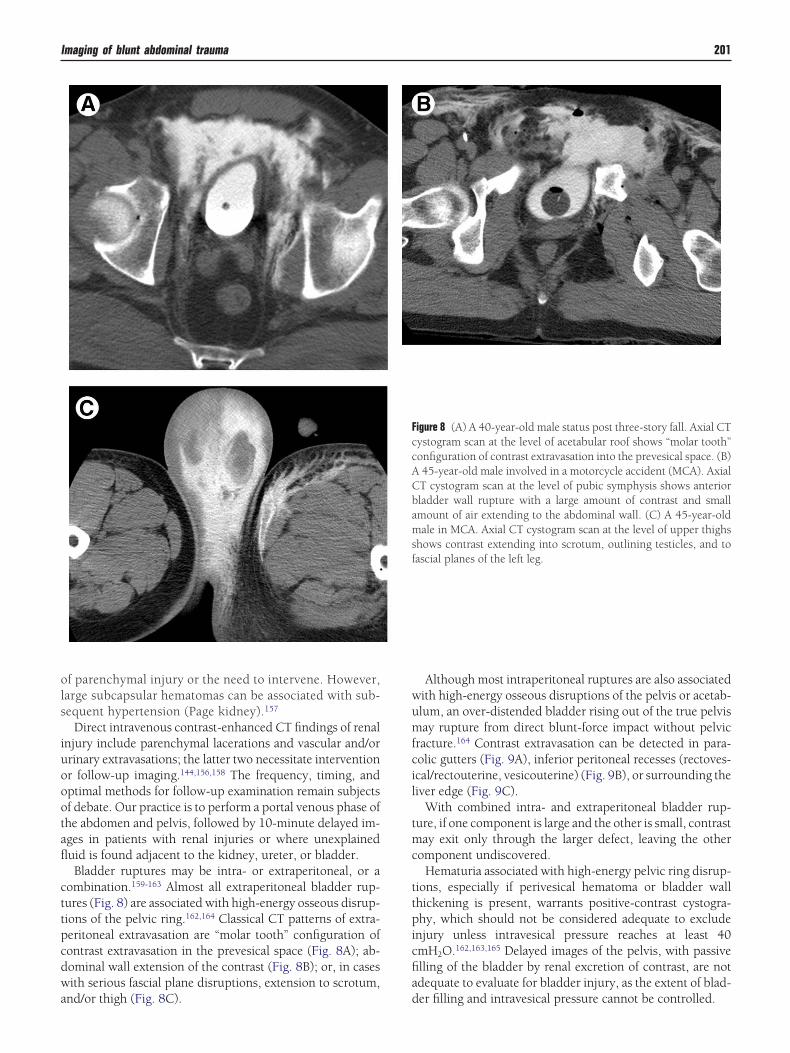
ombination.159-163 Almost all extraperitoneal bladder rup-ures (Fig. 8) are associated with high-energy osseous disrup-ions of the pelvic ring.162,164 Classical CT patterns of extra-eritoneal extravasation are “molar tooth” configuration ofontrast extravasation in the prevesical space (Fig. 8A); ab-ominal wall extension of the contrast (Fig. 8B); or, in casesith serious fascial plane disruptions, extension to scrotum,
nd/or thigh (Fig. 8C). d
Although most intraperitoneal ruptures are also associatedith high-energy osseous disruptions of the pelvis or acetab-lum, an over-distended bladder rising out of the true pelvisay rupture from direct blunt-force impact without pelvic
racture.164 Contrast extravasation can be detected in para-olic gutters (Fig. 9A), inferior peritoneal recesses (rectoves-cal/rectouterine, vesicouterine) (Fig. 9B), or surrounding theiver edge (Fig. 9C).
With combined intra- and extraperitoneal bladder rup-ure, if one component is large and the other is small, contrastay exit only through the larger defect, leaving the other
omponent undiscovered.Hematuria associated with high-energy pelvic ring disrup-
ions, especially if perivesical hematoma or bladder wallhickening is present, warrants positive-contrast cystogra-hy, which should not be considered adequate to exclude
njury unless intravesical pressure reaches at least 40mH2O.162,163,165 Delayed images of the pelvis, with passivelling of the bladder by renal excretion of contrast, are notdequate to evaluate for bladder injury, as the extent of blad-
igure 8 (A) A 40-year-old male status post three-story fall. Axial CTystogram scan at the level of acetabular roof shows “molar tooth”onfiguration of contrast extravasation into the prevesical space. (B)45-year-old male involved in a motorcycle accident (MCA). AxialT cystogram scan at the level of pubic symphysis shows anteriorladder wall rupture with a large amount of contrast and smallmount of air extending to the abdominal wall. (C) A 45-year-oldale in MCA. Axial CT cystogram scan at the level of upper thighs
hows contrast extending into scrotum, outlining testicles, and toascial planes of the left leg.
FccACbamsf
er filling and intravesical pressure cannot be controlled.
nTaArsqan
ha
oitoM
F
202 A.L. Stanescu et al
With the advent of CT, adrenal injuries are now recog-ized as the most common retroperitoneal injury.166,167
he right adrenal is injured much more often than the left,nd bilateral adrenal hemorrhage is relatively rare.167,168
n association also exists between right adrenal hemor-hage and liver lacerations involving the bare area.169 De-pite their frequency, adrenal hemorrhages very rarely re-uire treatment. Embolization may be done for large,ctive extravasations associated with ongoing hemody-amic consequences.170,171
Adrenocortical replacement therapy may be needed forypoadrenalism, a very infrequent consequence of bilateraldrenal hemorrhage.172
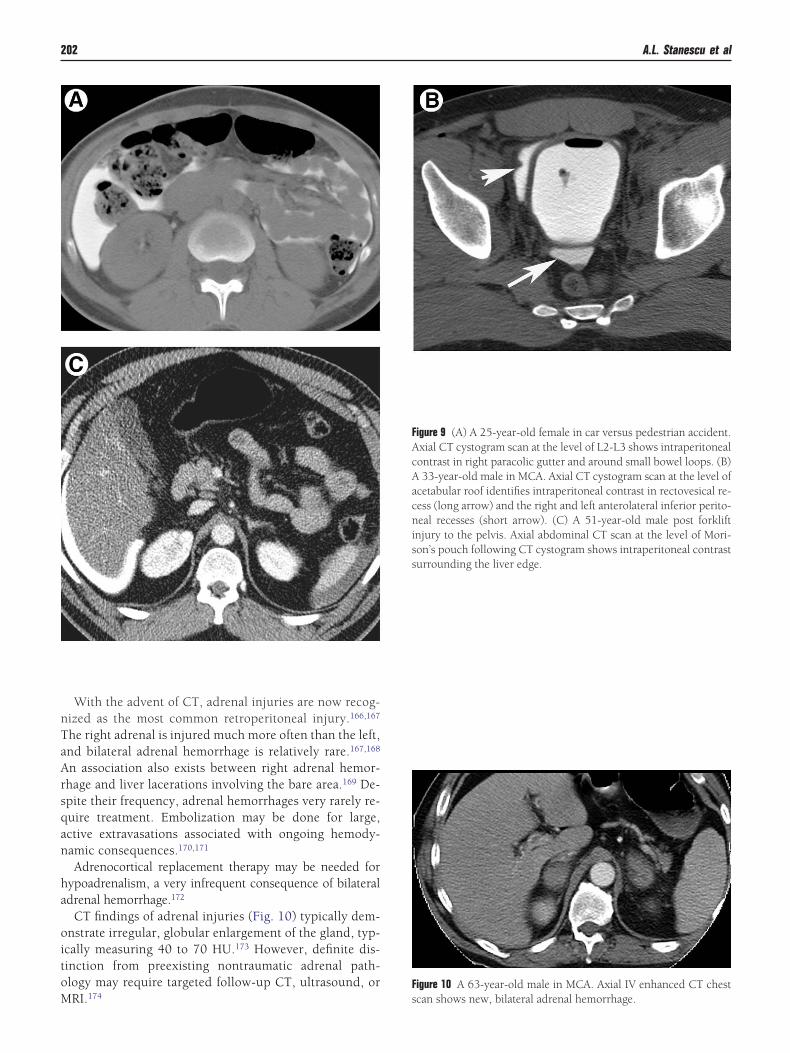
CT findings of adrenal injuries (Fig. 10) typically dem-nstrate irregular, globular enlargement of the gland, typ-cally measuring 40 to 70 HU.173 However, definite dis-inction from preexisting nontraumatic adrenal path-logy may require targeted follow-up CT, ultrasound, or
Figure 9 (A) A 25-year-old female in car versus pedestrian accident.Axial CT cystogram scan at the level of L2-L3 shows intraperitonealcontrast in right paracolic gutter and around small bowel loops. (B)A 33-year-old male in MCA. Axial CT cystogram scan at the level ofacetabular roof identifies intraperitoneal contrast in rectovesical re-cess (long arrow) and the right and left anterolateral inferior perito-neal recesses (short arrow). (C) A 51-year-old male post forkliftinjury to the pelvis. Axial abdominal CT scan at the level of Mori-son’s pouch following CT cystogram shows intraperitoneal contrastsurrounding the liver edge.
RI.174 s
igure 10 A 63-year-old male in MCA. Axial IV enhanced CT chest can shows new, bilateral adrenal hemorrhage.
he small bowel sustains surgically important blunt injuryore frequently than the colon.175 The spectrum of bowel
njuries includes wall contusions, serosal injuries (“desero-alization”), perforations and transections, mesenteric rents,nd hematomas.176,177 When mural disruption occurs in theroximal gastrointestinal tract (stomach through proximal
ejunum), leakage of alimentary tract contents into the peri-oneum induces acute chemical peritonitis and related clini-al findings.178 Distal small bowel and colon spillage tend toresent later as peritoneal sepsis.177 Delays in diagnosis ofowel injury are associated with complicated clinical coursesnd increased mortality.179,180 Serial physical evaluation ofhe abdomen alone (ie, without adjunctive diagnostic tests,uch as CT, ultrasound or US, DPL) may be associated with24-hour delay in diagnosis of surgically important bowel
njuries in 10 to 15% of individuals with distracting injuries,uch as femur fractures.181 DPL remains a somewhat moreensitive test than CT for isolated hollow viscus injury, evenith intravenous and alimentary contrast enhancement,
hin-sections, and multidetector technologies.180,182,183 How-ver, less than 1% of surgically important blunt-force hollowisceral injuries occurring in adults are found in the absencef other, often more obvious and clinically immediate, intra-bdominal injuries.176 Conventional radiography, ultra-ound, and MRI have little or no role in the routine diagnosisf bowel injuries.184
CT performed without oral or intravenous contrast en-ancement may show intramural hematoma as focal, asym-etric hyperdensity within bowel wall with adjacent mesen-
eric edema (“misty mesentery”).128,185 Bowel contusion maye suggested on intravenous contrast-enhanced CT by focalFig. 11) or multifocal (Fig. 12) bowel thickening and mural
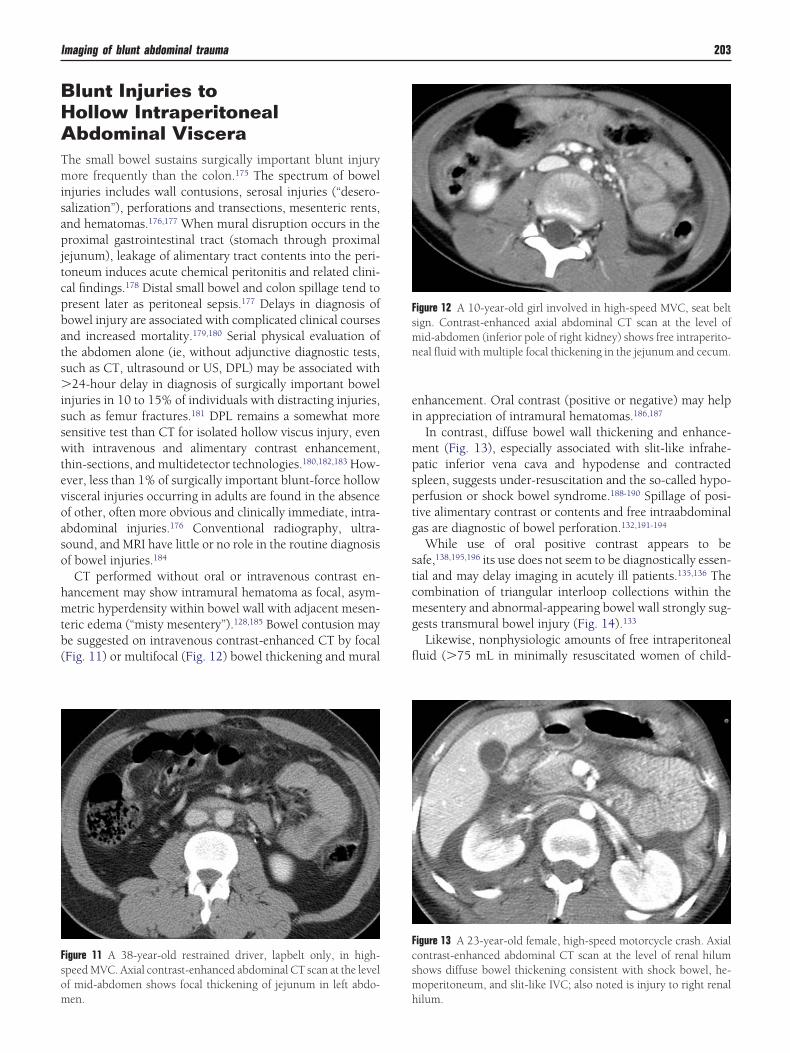
igure 11 A 38-year-old restrained driver, lapbelt only, in high-peed MVC. Axial contrast-enhanced abdominal CT scan at the levelf mid-abdomen shows focal thickening of jejunum in left abdo-
en. h
nhancement. Oral contrast (positive or negative) may helpn appreciation of intramural hematomas.186,187
In contrast, diffuse bowel wall thickening and enhance-ent (Fig. 13), especially associated with slit-like infrahe-atic inferior vena cava and hypodense and contractedpleen, suggests under-resuscitation and the so-called hypo-erfusion or shock bowel syndrome.188-190 Spillage of posi-ive alimentary contrast or contents and free intraabdominalas are diagnostic of bowel perforation.132,191-194
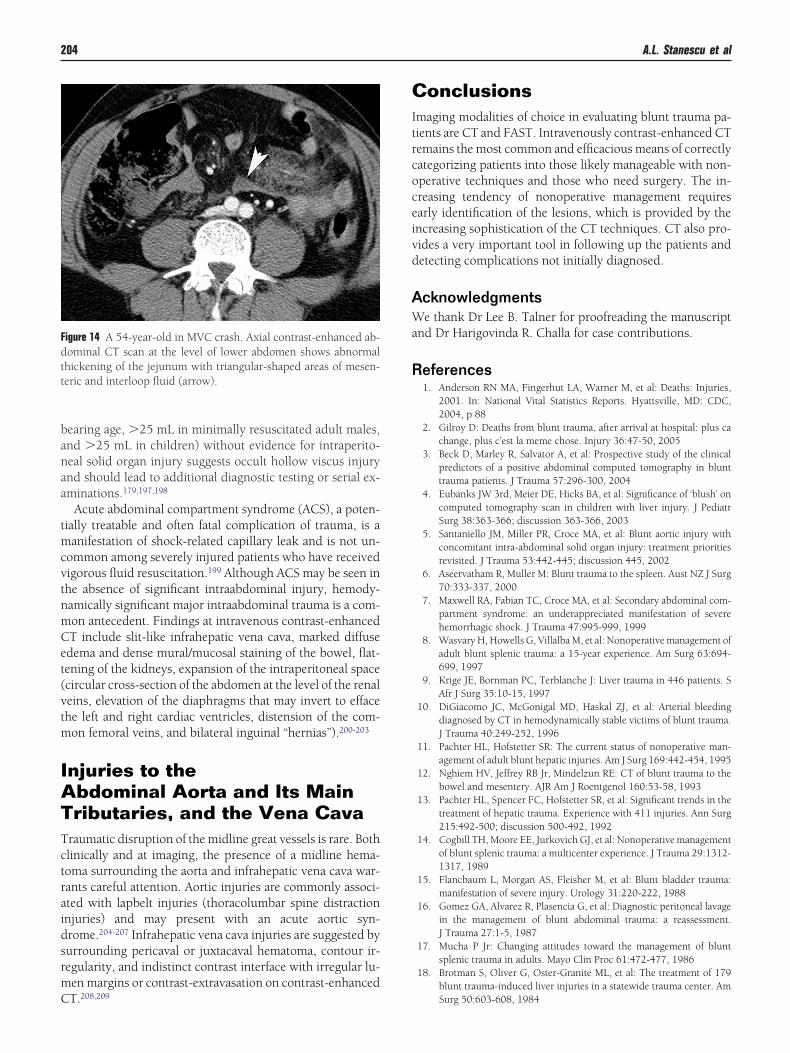
While use of oral positive contrast appears to beafe,138,195,196 its use does not seem to be diagnostically essen-ial and may delay imaging in acutely ill patients.135,136 Theombination of triangular interloop collections within theesentery and abnormal-appearing bowel wall strongly sug-
ests transmural bowel injury (Fig. 14).133
Likewise, nonphysiologic amounts of free intraperitonealuid (�75 mL in minimally resuscitated women of child-
igure 12 A 10-year-old girl involved in high-speed MVC, seat beltign. Contrast-enhanced axial abdominal CT scan at the level ofid-abdomen (inferior pole of right kidney) shows free intraperito-eal fluid with multiple focal thickening in the jejunum and cecum.
igure 13 A 23-year-old female, high-speed motorcycle crash. Axialontrast-enhanced abdominal CT scan at the level of renal hilumhows diffuse bowel thickening consistent with shock bowel, he-operitoneum, and slit-like IVC; also noted is injury to right renal
ilum.
banaa
tmcvtnmCet(vtm
IATTctraidsrmC
CItrcoceivd
AWa
R
Fdtt
204 A.L. Stanescu et al
earing age, �25 mL in minimally resuscitated adult males,nd �25 mL in children) without evidence for intraperito-eal solid organ injury suggests occult hollow viscus injurynd should lead to additional diagnostic testing or serial ex-minations.179,197,198
Acute abdominal compartment syndrome (ACS), a poten-ially treatable and often fatal complication of trauma, is aanifestation of shock-related capillary leak and is not un-
ommon among severely injured patients who have receivedigorous fluid resuscitation.199 Although ACS may be seen inhe absence of significant intraabdominal injury, hemody-amically significant major intraabdominal trauma is a com-on antecedent. Findings at intravenous contrast-enhancedT include slit-like infrahepatic vena cava, marked diffusedema and dense mural/mucosal staining of the bowel, flat-ening of the kidneys, expansion of the intraperitoneal spacecircular cross-section of the abdomen at the level of the renaleins, elevation of the diaphragms that may invert to effacehe left and right cardiac ventricles, distension of the com-on femoral veins, and bilateral inguinal “hernias”).200-203
njuries to thebdominal Aorta and Its Mainributaries, and the Vena Cava
raumatic disruption of the midline great vessels is rare. Bothlinically and at imaging, the presence of a midline hema-oma surrounding the aorta and infrahepatic vena cava war-ants careful attention. Aortic injuries are commonly associ-ted with lapbelt injuries (thoracolumbar spine distractionnjuries) and may present with an acute aortic syn-rome.204-207 Infrahepatic vena cava injuries are suggested byurrounding pericaval or juxtacaval hematoma, contour ir-egularity, and indistinct contrast interface with irregular lu-en margins or contrast-extravasation on contrast-enhanced
igure 14 A 54-year-old in MVC crash. Axial contrast-enhanced ab-ominal CT scan at the level of lower abdomen shows abnormalhickening of the jejunum with triangular-shaped areas of mesen-eric and interloop fluid (arrow).
T.208,209
onclusionsmaging modalities of choice in evaluating blunt trauma pa-ients are CT and FAST. Intravenously contrast-enhanced CTemains the most common and efficacious means of correctlyategorizing patients into those likely manageable with non-perative techniques and those who need surgery. The in-reasing tendency of nonoperative management requiresarly identification of the lesions, which is provided by thencreasing sophistication of the CT techniques. CT also pro-ides a very important tool in following up the patients andetecting complications not initially diagnosed.
cknowledgmentse thank Dr Lee B. Talner for proofreading the manuscript
nd Dr Harigovinda R. Challa for case contributions.
eferences1. Anderson RN MA, Fingerhut LA, Warner M, et al: Deaths: Injuries,
2001. In: National Vital Statistics Reports. Hyattsville, MD: CDC,2004, p 88
2. Gilroy D: Deaths from blunt trauma, after arrival at hospital: plus cachange, plus c’est la meme chose. Injury 36:47-50, 2005
3. Beck D, Marley R, Salvator A, et al: Prospective study of the clinicalpredictors of a positive abdominal computed tomography in blunttrauma patients. J Trauma 57:296-300, 2004
4. Eubanks JW 3rd, Meier DE, Hicks BA, et al: Significance of ‘blush’ oncomputed tomography scan in children with liver injury. J PediatrSurg 38:363-366; discussion 363-366, 2003
5. Santaniello JM, Miller PR, Croce MA, et al: Blunt aortic injury withconcomitant intra-abdominal solid organ injury: treatment prioritiesrevisited. J Trauma 53:442-445; discussion 445, 2002
6. Aseervatham R, Muller M: Blunt trauma to the spleen. Aust NZ J Surg70:333-337, 2000
7. Maxwell RA, Fabian TC, Croce MA, et al: Secondary abdominal com-partment syndrome: an underappreciated manifestation of severehemorrhagic shock. J Trauma 47:995-999, 1999
8. Wasvary H, Howells G, Villalba M, et al: Nonoperative management ofadult blunt splenic trauma: a 15-year experience. Am Surg 63:694-699, 1997
9. Krige JE, Bornman PC, Terblanche J: Liver trauma in 446 patients. SAfr J Surg 35:10-15, 1997
10. DiGiacomo JC, McGonigal MD, Haskal ZJ, et al: Arterial bleedingdiagnosed by CT in hemodynamically stable victims of blunt trauma.J Trauma 40:249-252, 1996
11. Pachter HL, Hofstetter SR: The current status of nonoperative man-agement of adult blunt hepatic injuries. Am J Surg 169:442-454, 1995
12. Nghiem HV, Jeffrey RB Jr, Mindelzun RE: CT of blunt trauma to thebowel and mesentery. AJR Am J Roentgenol 160:53-58, 1993
13. Pachter HL, Spencer FC, Hofstetter SR, et al: Significant trends in thetreatment of hepatic trauma. Experience with 411 injuries. Ann Surg215:492-500; discussion 500-492, 1992
14. Cogbill TH, Moore EE, Jurkovich GJ, et al: Nonoperative managementof blunt splenic trauma: a multicenter experience. J Trauma 29:1312-1317, 1989
15. Flancbaum L, Morgan AS, Fleisher M, et al: Blunt bladder trauma:manifestation of severe injury. Urology 31:220-222, 1988
16. Gomez GA, Alvarez R, Plasencia G, et al: Diagnostic peritoneal lavagein the management of blunt abdominal trauma: a reassessment.J Trauma 27:1-5, 1987
17. Mucha P Jr: Changing attitudes toward the management of bluntsplenic trauma in adults. Mayo Clin Proc 61:472-477, 1986
18. Brotman S, Oliver G, Oster-Granite ML, et al: The treatment of 179blunt trauma-induced liver injuries in a statewide trauma center. Am
Surg 50:603-608, 1984
Imaging of blunt abdominal trauma 205
19. DuPriest RW Jr, Rodriguez A, Khaneja SC, et al: Open diagnosticperitoneal lavage in blunt trauma victims. Surg Gynecol Obstet 148:890-894, 1979
20. Alho A, Karaharju O, Kallio E: Blunt hepatic injury. Ann Chir Gynae-col 67:66-69, 1978
21. Gill W, Champion HR, Long WB, et al: Abdominal lavage in blunttrauma. Br J Surg 62:124-124, 1975
22. Yoon W, Jeong YY, Kim JK, et al: CT in blunt liver trauma. Radio-graphics 25:87-104, 2005
23. Madoff DC, Denys A, Wallace MJ, et al: Splenic arterial interventions:anatomy, indications, technical considerations, and potential compli-cations. Radiographics 25:S191-S211, 2005 (suppl 1)
24. Balogh Z, Caldwell E, Heetveld M, et al: Institutional practice guide-lines on management of pelvic fracture-related hemodynamic insta-bility: do they make a difference? J Trauma 58:778-782, 2005
25. Labori KJ, Raeder MG: Diagnostic approach to the patient with jaun-dice following trauma. Scand J Surg 93:176-183, 2004
27. Peitzman AB, Harbrecht BG, Rivera L, et al: Failure of observation ofblunt splenic injury in adults: variability in practice and adverse con-sequences. J Am Coll Surg 201:179-187, 2005
28. Haan JM, Bochicchio GV, Kramer N, et al: Nonoperative managementof blunt splenic injury: a 5-year experience. J Trauma 58:492-498,2005
29. Wahl WL, Ahrns KS, Chen S, et al: Blunt splenic injury: operationversus angiographic embolization. Surgery 136:891-899, 2004
30. Tsugawa K, Koyanagi N, Hashizume M, et al: New insight for man-agement of blunt splenic trauma: significant differences betweenyoung and elderly. Hepatogastroenterology 49:1144-1149, 2002
31. Mizzi A, Shabani A, Watt A: The role of follow-up imaging in paedi-atric blunt abdominal trauma. Clin Radiol 57:908-912, 2002
32. Minarik L, Slim M, Rachlin S, et al: Diagnostic imaging in the fol-low-up of nonoperative management of splenic trauma in children.Pediatr Surg Int 18:429-431, 2002
33. Patselas TN, Gallagher EG: The diagnostic dilemma of diaphragminjury. Am Surg 68:633-639, 2002
35. Shackleton KL, Stewart ET, Taylor AJ: Traumatic diaphragmatic inju-ries: spectrum of radiographic findings. Radiographics 18:49-59,1998
36. Murray JG, Caoili E, Gruden JF, et al: Acute rupture of the diaphragmdue to blunt trauma: diagnostic sensitivity and specificity of CT. AJRAm J Roentgenol 166:1035-1039, 1996
37. Voeller GR, Reisser JR, Fabian TC, et al: Blunt diaphragm injuries. Afive-year experience. Am Surg 56:28-31, 1990
38. Hammond JS, Yudd A, Schwartz LB, et al: Peritoneoscintigraphy inthe diagnosis of traumatic diaphragmatic rupture. Am Surg 62:1055-1059, 1996
39. Baron BJ, Scalea TM, Sclafani SJ, et al: Nonoperative management ofblunt abdominal trauma: the role of sequential diagnostic peritoneallavage, computed tomography, and angiography. Ann Emerg Med22:1556-1562, 1993
40. Feliciano DV: Diagnostic modalities in abdominal trauma. Peritoneallavage, ultrasonography, computed tomography scanning, and arte-riography. Surg Clin North Am 71:241-256, 1991
41. Hawkins ML, Bailey RL Jr, Carraway RP: Is diagnostic peritoneal la-vage for blunt trauma obsolete? Am Surg 56:96-99, 1990
42. Shreck GL, Toalson TW: Delayed presentation of traumatic rupture ofthe diaphragm. J Okla State Med Assoc 96:181-183, 2003
43. Orsi P, Rollo S, Montanari M, et al: [Rupture of the diaphragm causedby closed thoraco-abdominal trauma. Case contribution andanatomo-clinical considerations]. G Chir 19:13-17, 1998
44. Gelman R, Mirvis SE, Gens D: Diaphragmatic rupture due to blunttrauma: sensitivity of plain chest radiographs. AJR Am J Roentgenol156:51-57, 1991
45. Iochum S, Ludig T, Walter F, et al: Imaging of diaphragmatic injury: a
46. Rees O, Mirvis SE, Shanmuganathan K: Multidetector-row CT of righthemidiaphragmatic rupture caused by blunt trauma: a review of 12cases. Clin Radiol 60:1280-1289, 2005
47. Larici AR, Gotway MB, Litt HI, et al: Helical CT with sagittal andcoronal reconstructions: accuracy for detection of diaphragmatic in-jury. AJR Am J Roentgenol 179:451-457, 2002
48. Bergin D, Ennis R, Keogh C, et al: The “dependent viscera” sign in CTdiagnosis of blunt traumatic diaphragmatic rupture. AJR Am J Roent-genol 177:1137-1140, 2001
49. Tsuda M, Ichiki K, Doki Y, et al: [Thoracic surgical approach fortraumatic diaphragmatic hernia]. Kyobu Geka 57:949-952, 2004
50. Barbiera F, Nicastro N, Finazzo M, et al: The role of MRI in traumaticrupture of the diaphragm. Our experience in three cases and review ofthe literature. Radiol Med (Torino) 105:188-194, 2003
51. Shanmuganathan K, Mirvis SE, White CS, et al: MR imaging evalua-tion of hemidiaphragms in acute blunt trauma: experience with 16patients. AJR Am J Roentgenol 167:397-402, 1996
53. Lefere P, Gryspeerdt S, Van Holsbeeck B, et al: Diagnosis and treat-ment of expanding haematoma of the lateral abdominal wall afterblunt abdominal trauma. Eur Radiol 9:1553-1555, 1999
54. Klingler PJ, Wetscher G, Glaser K, et al: The use of ultrasound todifferentiate rectus sheath hematoma from other acute abdominaldisorders. Surg Endosc 13:1129-1134, 1999
55. Zainea GG, Jordan F: Rectus sheath hematomas: their pathogenesis,diagnosis, and management. Am Surg 54:630-633, 1988
56. Hardcastle TC, Du Toit DF, Malherbe C, et al: Traumatic abdominalwall hernia—four cases and a review of the literature. S Afr J Surg43:41-43, 2005
57. Aguirre DA, Santosa AC, Casola G, et al: Abdominal wall hernias:imaging features, complications, and diagnostic pitfalls at multi-de-tector row CT. Radiographics 25:1501-1520, 2005
58. Mancel B, Aslam A: Traumatic abdominal wall hernia: an unusualbicycle handlebar injury. Pediatr Surg Int 19:746-747, 2003
59. Lane CT, Cohen AJ, Cinat ME: Management of traumatic abdominalwall hernia. Am Surg 69:73-76, 2003
60. Hickey NA, Ryan MF, Hamilton PA, et al: Computed tomography oftraumatic abdominal wall hernia and associated deceleration injuries.Can Assoc Radiol J 53:153-159, 2002
61. Killeen KL, Girard S, DeMeo JH, et al Using CT to diagnose traumaticlumbar hernia. AJR Am J Roentgenol 174:1413-1415, 2000
63. Toutouzas KG, Karaiskakis M, Kaminski A, et al: Nonoperative man-agement of blunt renal trauma: a prospective study. Am Surg 68:1097-1103, 2002
64. Bode PJ, Edwards MJ, Kruit MC, et al: Sonography in a clinical algo-rithm for early evaluation of 1671 patients with blunt abdominaltrauma. AJR Am J Roentgenol 172:905-911, 1999
65. Romano L, Giovine S, Guidi G, et al: Hepatic trauma: CT findings andconsiderations based on our experience in emergency diagnostic im-aging. Eur J Radiol 50:59-66, 2004
66. Poletti PA, Wintermark M, Schnyder P, et al: Traumatic injuries: roleof imaging in the management of the polytrauma victim (conservativeexpectation). Eur Radiol 12:969-978, 2002
67. Ravera M, Cocozza E, Reggiori A: Blunt splenic rupture—experiencein a preserving non-operatively orientated care team in a tropicalhospital. S Afr J Surg 37:41-44, 1999
68. Becker CD, Mentha G, Terrier F: Blunt abdominal trauma in adults:role of CT in the diagnosis and management of visceral injuries. Part 1:liver and spleen. Eur Radiol 8:553-562, 1998
69. Van Etten EP, van Popta T, Van Luyt PA, et al: Changes in the diag-nosis and treatment of traumatic splenic rupture: a retrospective anal-ysis of 99 consecutive cases. Eur J Emerg Med 2:196-200, 1995
70. Tricarico A, Sicoli F, Calise F, et al: Conservative treatment in splenic
72. Wolf Y, Vinograd I, Katz S, et al: Non-operative management of trau-matized spleen in children: the role of open abdominal tap. Z Kinder-chir 42:23-25, 1987
73. Mirvis SE, Shanmuganathan K: Trauma radiology: part I. Computer-ized tomographic imaging of abdominal trauma. J Intensive Care Med9:151-163, 1994
74. Shanmuganathan K. Multi-detector row CT imaging of blunt abdom-inal trauma. Semin Ultrasound CT MR 25:180-204, 2004
75. Barquist ES, Pizano LR, Feuer W, et al: Inter- and intrarater reliabilityin computed axial tomographic grading of splenic injury: why somany grading scales? J Trauma 56:334-338, 2004
76. Hackam DJ, Potoka D, Meza M, et al: Utility of radiographic hepaticinjury grade in predicting outcome for children after blunt abdominaltrauma. J Pediatr Surg 37:386-389, 2002
77. Shapiro MJ, Krausz C, Durham RM, et al: Overuse of splenic scoringand computed tomographic scans. J Trauma 47:651-658, 1999
78. Mohr AM, Lavery RF, Barone A, et al: Angiographic embolization forliver injuries: low mortality, high morbidity. J Trauma 55:1077-1081;discussion 1081-1072, 2003
79. Kushimoto S, Arai M, Aiboshi J, et al: The role of interventional radi-ology in patients requiring damage control laparotomy. J Trauma54:171-176, 2003
80. Willmann JK, Roos JE, Platz A, et al: Multidetector CT: detection ofactive hemorrhage in patients with blunt abdominal trauma. AJR Am JRoentgenol 179:437-444, 2002
81. Okamoto K, Norio H, Kaneko N, et al: Use of early-phase dynamicspiral computed tomography for the primary screening of multipletrauma. Am J Emerg Med 20:528-534, 2002
82. Fang JF, Chen RJ, Wong YC, et al: Classification and treatment ofpooling of contrast material on computed tomographic scan of blunthepatic trauma. J Trauma 49:1083-1088, 2000
83. Taylor GA, Kaufman RA, Sivit CJ: Active hemorrhage in children afterthoracoabdominal trauma: clinical and CT features. AJR Am J Roent-genol 162:401-404, 1994
84. Shanmuganathan K, Mirvis SE, Sover ER: Value of contrast-enhancedCT in detecting active hemorrhage in patients with blunt abdominalor pelvic trauma. AJR Am J Roentgenol 161:65-69, 1993
85. Gavant ML, Schurr M, Flick PA, et al: Predicting clinical outcome ofnonsurgical management of blunt splenic injury: using CT to revealabnormalities of splenic vasculature. AJR Am J Roentgenol 168:207-212, 1997
88. Pinto A, Magliocca M, Grassi R, et al: [Role of computerized tomog-raphy in the diagnosis of peritoneo-intestinal lesions resulting fromclosed trauma. Experience at 2 emergency departments]. Radiol Med(Torino) 101:177-182, 2001
89. Miller LA, Shanmuganathan K: Multidetector CT evaluation of ab-dominal trauma. Radiol Clin North Am 43:1079-1095, viii, 2005
90. Shanmuganathan K, Mirvis SE: CT scan evaluation of blunt hepatictrauma. Radiol Clin North Am 36:399-411, 1998
91. Shanmuganathan K, Mirvis SE, Reaney SM: Pictorial review: CT ap-pearances of contrast medium extravasations associated with injurysustained from blunt abdominal trauma. Clin Radiol 50:182-187,1995
92. Shanmuganathan K, Mirvis SE: CT evaluation of the liver with acuteblunt trauma. Crit Rev Diagn Imaging 36:73-113, 1995
93. Peiper HJ: Significance of traumatology in abdominal and vascularsurgery. Jpn J Surg 15:93-102, 1985
94. Gupta A, Stuhlfaut JW, Fleming KW, et al: Blunt trauma of the pan-creas and biliary tract: a multimodality imaging approach to diagnosis.
Radiographics 24:1381-1395, 2004
95. Benedict MD, Rafal R: Finding of CT and MR evaluation of gallbladderhemobilia. Emerg Radiol 10:46-48, 2003
96. Kohler R, Millin R, Bonner B, et al: Laparoscopic treatment of anisolated gallbladder rupture following blunt abdominal trauma in aschoolboy rugby player. Br J Sports Med 36:378-379; discussion 379,2002
98. Colletti PM, Barakos JA, Ralls PW, et al: Hepatobiliary scintigraphyand scintiangiography in abdominal trauma. Clin Nucl Med 12:901-909, 1987
99. Harrell DJ, Vitale GC, Larson GM: Selective role for endoscopic ret-rograde cholangiopancreatography in abdominal trauma. Surg En-dosc 12:400-404, 1998
00. Hewett JJ, Freed KS, Sheafor DH, et al: The spectrum of abdominalvenous CT findings in blunt trauma. AJR Am J Roentgenol 176:955-958, 2001
01. Taga S, Ezaki T, Yano K, et al: Hepatic venous injury; a case report ofatriocaval shunt by a centrifugal pump. Hepatogastroenterology 44:1219-1221, 1997
02. Mehall JR, Ennis JS, Saltzman DA, et al: Prospective results of a stan-dardized algorithm based on hemodynamic status for managing pe-diatric solid organ injury. J Am Coll Surg 193:347-353, 2001
03. Allins A, Ho T, Nguyen TH, et al: Limited value of routine followupCT scans in nonoperative management of blunt liver and splenicinjuries. Am Surg 62:883-886, 1996
04. Luks FI, Lemire A, St-Vil D, et al: Blunt abdominal trauma in children:the practical value of ultrasonography. J Trauma 34:607-610; discus-sion 610-611, 1993
05. Maull KI, Rozycki GS, Vinsant GO, et al: Retroperitoneal injuries:pitfalls in diagnosis and management. South Med J 80:1111-1115,1987
06. Al-Salamah SM, Mirza SM, Ahmad SN, et al: Role of ultrasonography,computed tomography and diagnostic peritoneal lavage in abdominalblunt trauma. Saudi Med J 23:1350-1355, 2002
07. Shah P, Applegate KE, Buonomo C: Stricture of the duodenum andjejunum in an abused child. Pediatr Radiol 27:281-283, 1997
08. Kunin JR, Korobkin M, Ellis JH, et al: Duodenal injuries caused byblunt abdominal trauma: value of CT in differentiating perforationfrom hematoma. AJR Am J Roentgenol 160:1221-1223, 1993
10. Savage C, Reabe S, Goldman SM, et al: Imaging of bilateral uretero-pelvic junction laceration from blunt trauma. Emerg Radiol 10:99-101, 2003
11. Beyrouti MI, Beyrouti R, Kchaou I, et al: [Duodeno-pancreatic trauma.About 14 cases]. Tunis Med 83:73-82, 2005
12. Ludwig K, Petermann J, Lorenz D: [Diagnosis and therapy of trau-matic injury of the pancreas]. Zentralbl Chir 123:245-250, 1998
13. Wales PW, Shuckett B, Kim PC: Long-term outcome after nonopera-tive management of complete traumatic pancreatic transection in chil-dren. J Pediatr Surg 36:823-827, 2001
14. Lucas CE, Ledgerwood AM: Factors influencing outcome after bluntduodenal injury. J Trauma 15:839-846, 1975
15. Nowak MM, Baringer DC, Ponsky JL: Pancreatic injuries. Effective-ness of debridement and drainage for nontransecting injuries. AmSurg 52:599-602, 1986
17. Kim HS, Lee DK, Kim IW, et al: The role of endoscopic retrogradepancreatography in the treatment of traumatic pancreatic duct injury.Gastrointest Endosc 54:49-55, 2001
18. Sekino Y, Kobayashi A, Takagi S, et al: Successful treatment for com-bined pancreatoduodenal injury by a second-stage pancreatojejunos-tomy following pancreatoduodenectomy. Hepatogastroenterology51:1674-1675, 2004
19. Yeung CY, Lee HC, Huang FY, et al: Pancreatitis in children—expe-
rience with 43 cases. Eur J Pediatr 155:458-463, 1996
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Imaging of blunt abdominal trauma 207
20. Bigattini D, Boverie JH, Dondelinger RF. CT of blunt trauma of thepancreas in adults. Eur Radiol 9:244-249, 1999
21. Coppola V, Vallone G, Verrengia D, et al: [Pancreatic fractures: therole of CT and the indications for endoscopic retrograde pancreatog-raphy]. Radiol Med (Torino) 94:335-340, 1997
22. Lane MJ, Mindelzun RE, Sandhu JS, et al: CT diagnosis of bluntpancreatic trauma: importance of detecting fluid between the pan-creas and the splenic vein. AJR Am J Roentgenol 163:833-835, 1994
23. Sivit CJ, Eichelberger MR, Taylor GA, et al: Blunt pancreatic trauma inchildren: CT diagnosis. AJR Am J Roentgenol 158:1097-1100, 1992
24. Jayaraman MV, Mayo-Smith WW, Movson JS, et al: CT of the duode-num: an overlooked segment gets its due. Radiographics 21(SpecNo.):S147-S160, 2001
25. Becker CD, Mentha G, Schmidlin F, et al: Blunt abdominal trauma inadults: role of CT in the diagnosis and management of visceral inju-ries. Part 2: Gastrointestinal tract and retroperitoneal organs. EurRadiol 8:772-780, 1998
26. Rescorla FJ, Plumley DA, Sherman S, et al: The efficacy of early ERCPin pediatric pancreatic trauma. J Pediatr Surg 30:336-340, 1995
27. Fulcher AS, Turner MA, Yelon JA, et al: Magnetic resonance cholan-giopancreatography (MRCP) in the assessment of pancreatic ducttrauma and its sequelae: preliminary findings. J Trauma 48:1001-1007, 2000
28. Scaglione M, de Lutio di Castelguidone E, Scialpi M, et al: Blunttrauma to the gastrointestinal tract and mesentery: is there a role forhelical CT in the decision-making process? Eur J Radiol 50:67-73,2004
29. Holmes JF, Offerman SR, Chang CH, et al: Performance of helicalcomputed tomography without oral contrast for the detection of gas-trointestinal injuries. Ann Emerg Med 43:120-128, 2004
30. Timaran CH, Daley BJ, Enderson BL: Role of duodenography in thediagnosis of blunt duodenal injuries. J Trauma 51:648-651, 2001
31. Ciftci AO, Tanyel FC, Salman AB, et al: Gastrointestinal tract perfora-tion due to blunt abdominal trauma. Pediatr Surg Int 13:259-264,1998
32. Kim HC, Shin HC, Park SJ, et al: Traumatic bowel perforation: anal-ysis of CT findings according to the perforation site and the elapsedtime since accident. Clin Imaging 28:334-339, 2004
34. Taylor GA, Sivit CJ: Computed tomography imaging of abdominaltrauma in children. Semin Pediatr Surg 1:253-259, 1992
35. Stuhlfaut JW, Soto JA, Lucey BC, et al: Blunt abdominal trauma:performance of CT without oral contrast material. Radiology 233:689-694, 2004
36. Halsted MJ, Racadio JM, Emery KH, et al: Oral contrast agents for CTof abdominal trauma in pediatric patients: a comparison of dilutehypaque and water. AJR Am J Roentgenol 182:1555-1559, 2004
37. Allen TL, Mueller MT, Bonk RT, et al: Computed tomographic scan-ning without oral contrast solution for blunt bowel and mesentericinjuries in abdominal trauma. J Trauma 56:314-322, 2004
38. Federle MP, Yagan N, Peitzman AB, et al: Abdominal trauma: use oforal contrast material for CT is safe. Radiology 205:91-93, 1997
39. Federle MP, Peitzman A, Krugh J: Use of oral contrast material inabdominal trauma CT scans: is it dangerous? J Trauma 38:51-53,1995
40. Rathaus V, Pomeranz A, Shapiro-Feinberg M, et al: Isolated severerenal injuries after minimal blunt trauma to the upper abdomen andflank: CT findings. Emerg Radiol 10:190-192, 2004
41. Noor MA, Ather MH: Difference in the outcome of patients managedwith isolated renal injury and co-existent abdominal organ injury. JAyub Med Coll Abbottabad 15:29-32, 2003
42. Baverstock R, Simons R, McLoughlin M: Severe blunt renal trauma: a7-year retrospective review from a provincial trauma centre. CanJ Urol 8:1372-1376, 2001
43. Santucci RA, Langenburg SE, Zachareas MJ: Traumatic hematuria inchildren can be evaluated as in adults. J Urol 171:822-825, 2004
44. Smith JK, Kenney PJ. Imaging of renal trauma. Radiol Clin North Am
41:1019-1035, 2003
45. Brown SL, Haas C, Dinchman KH, et al: Radiologic evaluation ofpediatric blunt renal trauma in patients with microscopic hematuria.World J Surg 25:1557-1560, 2001
46. Morey AF, Bruce JE, McAninch JW: Efficacy of radiographic imagingin pediatric blunt renal trauma. J Urol 156:2014-2018, 1996
47. Miller KS, McAninch JW: Radiographic assessment of renal trauma:our 15-year experience. J Urol 154:352-355, 1995
48. Stein JP, Kaji DM, Eastham J, et al: Blunt renal trauma in the pediatricpopulation: indications for radiographic evaluation. Urology 44:406-410, 1994
49. Ihara N, Yashiro N, Itoh K, et al: Early ureteral luminal enhancementon computed tomography in a renal trauma patient: a characteristicsign of communication between artery and collecting system. RadiatMed 22:272-274, 2004
50. Brandes SB, McAninch JW: Urban free falls and patterns of renalinjury: a 20-year experience with 396 cases. J Trauma 1999;47:643-649; discussion 649-650, 1999
51. Titton RL, Gervais DA, Hahn PF, et al: Urine leaks and urinomas:diagnosis and imaging-guided intervention. Radiographics 23:1133-1147, 2003
52. Blankenship JC, Gavant ML, Cox CE, et al: Importance of delayedimaging for blunt renal trauma. World J Surg 25:1561-1564, 2001
54. Fanney DR, Casillas J, Murphy BJ: CT in the diagnosis of renal trauma.Radiographics 10:29-40, 1990
55. Sebastia MC, Rodriguez-Dobao M, Quiroga S, et al: Renal trauma inoccult ureteropelvic junction obstruction: CT findings. Eur Radiol9:611-615, 1999
56. Harris AC, Zwirewich CV, Lyburn ID, et al: CT findings in blunt renaltrauma. Radiographics 21(Spec No.):S201-S214, 2001
57. Sufrin G: The Page kidney: a correctable form of arterial hypertension.J Urol 113:450-454, 1975
58. Sofocleous CT, Hinrichs C, Hubbi B, et al: Angiographic findings andembolotherapy in renal arterial trauma. Cardiovasc Intervent Radiol28:39-47, 2005
59. Morey AF, Iverson AJ, Swan A, et al: Bladder rupture after blunttrauma: guidelines for diagnostic imaging. J Trauma 51:683-686,2001
60. Deck AJ, Shaves S, Talner L, Porter JR: Current experience with com-puted tomographic cystography and blunt trauma. World J Surg 25:1592-1596, 2001
61. Pao DM, Ellis JH, Cohan RH, et al: Utility of routine trauma CT in thedetection of bladder rupture. Acad Radiol 7:317-324, 2000
62. Morgan DE, Nallamala LK, Kenney PJ, et al: CT cystography: radio-graphic and clinical predictors of bladder rupture. AJR Am J Roent-genol 174:89-95, 2000
63. Deck AJ, Shaves S, Talner L, et al: Computerized tomography cystog-raphy for the diagnosis of traumatic bladder rupture. J Urol 164:43-46, 2000
64. Festini G, Gregorutti S, Reina G, et al: Isolated intraperitoneal bladderrupture in patients with alcohol intoxication and minor abdominaltrauma. Ann Emerg Med 20:1371-1372, 1991
65. Rehm CG, Mure AJ, O’Malley KF, et al: Blunt traumatic bladder rup-ture: the role of retrograde cystogram. Ann Emerg Med 20:845-847,1991
66. Schwarz M, Horev G, Freud E, et al: Traumatic adrenal injury inchildren. Isr Med Assoc J 2:132-134, 2000
68. Pinto A, Scaglione M, Pinto F, et al: Adrenal injuries: spectrum of CTfindings. Emerg Radiol 10:30-33, 2003
69. Patten RM, Spear RP, Vincent LM, et al: Traumatic laceration of theliver limited to the bare area: CT findings in 25 patients. AJR Am JRoentgenol 160:1019-1022, 1993
70. Yao DC, Jeffrey RB Jr, Mirvis SE, et al: Using contrast-enhanced helical
CT to visualize arterial extravasation after blunt abdominal trauma:
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
208 A.L. Stanescu et al
incidence and organ distribution. AJR Am J Roentgenol 178:17-20,2002
71. Tixedor N, Lesnik A, Vernhet H, et al: [Embolization treatment of atraumatic adrenal hemorrhage]. J Radiol 80:733-735, 1999
72. Lewis JV: Bilateral adrenal hemorrhage after blunt trauma: diagnosisby computed tomography. South Med J 87:1269-1271, 1994
74. Dueck A, Poenaru D, Kamal I: Hypertension following minor trauma:a rare presentation of pheochromocytoma. Pediatr Surg Int 15:508-509, 1999
75. Longo WE, Degutis LC, Baker CC: Blunt hollow viscus injuries of thedigestive tract: a poorly recognized phenomenon. Conn Med 53:451-454, 1989
76. Watts DD, Fakhry SM: Incidence of hollow viscus injury in blunttrauma: an analysis from 275,557 trauma admissions from the Eastmulti-institutional trial. J Trauma 54:289-294, 2003
77. Munns J, Richardson M, Hewett P: A review of intestinal injury fromblunt abdominal trauma. Aust NZ J Surg 65:857-860, 1995
78. Moss RL, Musemeche CA: Clinical judgment is superior to diagnostictests in the management of pediatric small bowel injury. J Pediatr Surg31:1178-1181; discussion 1181-1172, 1996
79. Brownstein MR, Bunting T, Meyer AA, et al: Diagnosis and manage-ment of blunt small bowel injury: a survey of the membership of theAmerican Association for the Surgery of Trauma. J Trauma 48:402-407, 2000
80. Neugebauer H, Wallenboeck E, Hungerford M: Seventy cases of inju-ries of the small intestine caused by blunt abdominal trauma: a retro-spective study from 1970 to 1994. J Trauma 46:116-121, 1999
81. Ferrera PC, Verdile VP, Bartfield JM, et al: Injuries distracting fromintraabdominal injuries after blunt trauma. Am J Emerg Med 16:145-149, 1998
82. Menegaux F, Tresallet C, Gosgnach M, et al: Diagnosis of bowel andmesenteric injuries in blunt abdominal trauma: a prospective study.Am J Emerg Med 24:19-24, 2006
83. Pikoulis E, Delis S, Psalidas N, et al: Presentation of blunt small intes-tinal and mesenteric injuries. Ann R Coll Surg Engl 82:103-106, 2000
84. Shih HC, Wen YS, Ko TJ, et al: Noninvasive evaluation of blunt ab-dominal trauma: prospective study using diagnostic algorithms tominimize nontherapeutic laparotomy. World J Surg 23:265-269; dis-cussion 269-270, 1999
85. Halvorsen RA Jr, McKenney K: Blunt trauma to the gastrointestinaltract: CT findings with small bowel and colon injuries. Emerg Radiol9:141-145, 2002
86. Killeen KL, Shanmuganathan K, Poletti PA, et al: Helical computedtomography of bowel and mesenteric injuries. J Trauma 51:26-36,2001
88. Mirvis SE, Shanmuganathan K, Erb R: Diffuse small-bowel ischemia inhypotensive adults after blunt trauma (shock bowel): CT findings andclinical significance. AJR Am J Roentgenol 163:1375-1379, 1994
89. Sivit CJ, Taylor GA, Bulas DI, et al: Posttraumatic shock in children:CT findings associated with hemodynamic instability. Radiology 182:
723-726, 1992
90. Taylor GA, Fallat ME, Eichelberger MR: Hypovolemic shock in chil-dren: abdominal CT manifestations. Radiology 164:479-481, 1987
91. Sharma OP, Oswanski MF, Singer D, et al: The role of computedtomography in diagnosis of blunt intestinal and mesenteric trauma(BIMT). J Emerg Med 27:55-67, 2004
92. Butela ST, Federle MP, Chang PJ, et al: Performance of CT in detectionof bowel injury. AJR Am J Roentgenol 176:129-135, 2001
93. Brody JM, Leighton DB, Murphy BL, et al: CT of blunt trauma boweland mesenteric injury: typical findings and pitfalls in diagnosis. Ra-diographics 20:1525-1536; discussion 1536-1527, 2000
94. Strouse PJ, Close BJ, Marshall KW, et al: CT of bowel and mesenterictrauma in children. Radiographics 19:1237-1250, 1999
95. Nastanski F, Cohen A, Lush SP, et al: The role of oral contrast admin-istration immediately prior to the computed tomographic evaluationof the blunt trauma victim. Injury 32:545-549, 2001
96. Tsang BD, Panacek EA, Brant WE, et al: Effect of oral contrast admin-istration for abdominal computed tomography in the evaluation ofacute blunt trauma. Ann Emerg Med 30:7-13, 1997
97. Eanniello VC 2nd, Gabram SG, Eusebio R, et al: Isolated free fluid onabdominal computerized tomographic scan: an indication for surgeryin blunt trauma patients? Conn Med 58:707-710, 1994
98. Rathaus V, Zissin R, Werner M, et al: Minimal pelvic fluid in bluntabdominal trauma in children: the significance of this sonographicfinding. J Pediatr Surg 36:1387-1389, 2001
99. Miller PR, Meredith JW, Johnson JC, et al: Prospective evaluation ofvacuum-assisted fascial closure after open abdomen: planned ventralhernia rate is substantially reduced. Ann Surg 239:608-614; discus-sion 614-606, 2004
00. Goldman R, Zilkoski M, Mullins R, et al: Delayed celiotomy for thetreatment of bile leak, compartment syndrome, and other hazards ofnonoperative management of blunt liver injury. Am J Surg 185:492-497, 2003
01. Laffargue G, Taourel P, Saguintaah M, et al: CT diagnosis of abdom-inal compartment syndrome. AJR Am J Roentgenol 178:771-772,2002
02. Epelman M, Soudack M, Engel A, et al: Abdominal compartmentsyndrome in children: CT findings. Pediatr Radiol 32:319-322, 2002
03. Pickhardt PJ, Shimony JS, Heiken JP, et al: The abdominal compart-ment syndrome: CT findings. AJR Am J Roentgenol 173:575-579,1999
04. Lin PH, Barr V, Bush RL, et al: Isolated abdominal aortic rupture in achild due to all-terrain vehicle accident—a case report. Vasc Endovas-cular Surg 37:289-292, 2003
05. Berthet JP, Marty-Ane CH, Veerapen R, et al: Dissection of the abdom-inal aorta in blunt trauma: Endovascular or conventional surgicalmanagement? J Vasc Surg 38:997-1003; discussion 1004, 2003
06. Roth SM, Wheeler JR, Gregory RT, et al: Blunt injury of the abdominalaorta: a review. J Trauma 42:748-755, 1997
07. Michaels AJ, Gerndt SJ, Taheri PA, et al: Blunt force injury of theabdominal aorta. J Trauma 41:105-109, 1996
08. Duncan IC, Sher BJ, Fingleson LM: Blunt injury of the infrarenalinferior vena cava—imaging and conservative management. S AfrJ Surg 43:20-21, 2005
09. Parke CE, Stanley RJ, Berlin AJ: Infrarenal vena caval injury followingblunt trauma: CT findings. J Comput Assist Tomogr 17:154-157,