Ectopic pregnancy is a majorhealth problem for women ofchildbearing age and a leading
cause of pregnancy-related death in thefirst trimester. Untreated, ectopic preg-nancy can lead to massive hemorrhage,infertility and death. With the advent ofhigh-resolution transvaginal sonogra-phy, in conjunction with serum assaysfor the ß-subunit of human chorionicgonadotropin (ß-hCG), rapid and accu-rate diagnosis of this entity is now rou-tinely possible.
Ectopic pregnancy is defined asimplantation of a fertilized ovum out-side the endometrial lining of the uterus.Based on data from the Centers for Dis-ease Control and Prevention, ectopicpregnancy has an incidence of approxi-mately 2% of all reported pregnanciesand accounts for 9% of pregnancy-related deaths.1
First described in the 11th century,ectopic pregnancy was usually fatal.John Bard of New York City, NY, per-formed the first abdominal surgery forectopic pregnancy in 1759. However,the survival rate for surgery was dismalin the 18th century and patients whowere not treated surgically had a greatersurvival rate than those undergoingsurgery.2 With subsequent improve-ments in anesthesia, antibiotics and
blood transfusion during the 20th cen-tury, mortality rates have significantlydeclined. Between 1970 and 1989 therisk of death from ectopic pregnancydropped from 35.5 to 2.6 deaths per10,000 cases despite a fourfold increasein incidence.2
Although ectopic pregnancy canoccur in any woman capable of becom-ing pregnant, certain patient popula-tions are more predisposed to ectopicpregnancy. Risk factors include: historyof prior pelvic inflammatory disease,prior tubal surgery or ligation, presenceof an intrauterine device, infertilitytreatment, history of prior ectopic preg-nancy, and older age. Ectopic preg-nancy has also been found to be morecommon in smokers than nonsmokers,possibly secondary to altered tubalmotility.3,4 These risk factors can be
additive resulting in increased risk forwomen with multiple risk factors.
Ectopic pregnancy most commonlyoccurs in the fallopian tube with 90% to95% occurring in the ampullary or isth-mic portions (Figure 1). Less than 5%of ectopic pregnancies are interstitial inlocation. However, morbidity and mor-tality are higher for interstitial ectopicpregnancies due to later presentationand resultant massive hemorrhage.Cervical, ovarian and intra-abdominalectopic pregnancies are rare andaccount for <1% of all ectopic pregnan-cies.5 Ectopic pregnancies can alsooccur in the scar from a previous cae-sarean section. These ectopic pregnan-cies are also rare, accounting for <1%of ectopic pregnancies. They can pre-sent with vaginal bleeding as early as 5to 6 weeks gestational age and as late as
Imaging of ectopic pregnancy
Jonathan D. Kirsch, MD, and Leslie M. Scoutt, MD
Dr. Kirsch is an A ssistant Professor ofDiagnostic Radiology and Dr. Scoutt is aProfessor of Diagnostic Radiology,Y ale University School of Medicine,New Haven, CT.
16 weeks. These ectopic pregnancies,located in the anterior myometrium ofthe lower uterine segment, may rup-ture—resulting in severe hemorrhageand cardiovascular collapse.6
Clinically, the classic triad of signs/symptoms of ectopic pregnancy consistsof vaginal bleeding, abdominal or pelvicpain, and a tender adnexal mass. Unfor-tunately, this triad is only seen in about50% of women presenting with ectopicpregnancy.7 In many patients, presentingsigns and symptoms are often nonspe-cific and can overlap with findings com-mon to normal early-intrauterinepregnancies or miscarriages. They caninclude nausea, fatigue, lower abdominalpain, cramping and shoulder pain.Because of the overlap with early preg-nancy symptomatology, a high clinicalindex of suspicion for ectopic pregnancyis necessary.
How then does one approach thepregnant patient with pain and vaginalbleeding or the ubiquitous requisitionfor “rule out ectopic” from the Emer-gency Department? The primary differ-ential diagnosis in such cases is fairlystraightforward and includes: normalintrauterine pregnancy (IUP), abnormalIUP or spontaneous abortion, ectopicpregnancy, and molar pregnancy. Theprimary tools used to distinguishbetween these entities are high-resolu-tion transvaginal sonography and serumassays for ß-hCG.
TechniqueTransvaginal sonography is per-
formed at the authors’ institution with acurved 8-4 MHz array or a curved array9-5 MHz endovaginal probe. The uterusis imaged in the sagittal and transverseplanes. Measurement of the endome-trial stripe is obtained on a midlinesagittal image. The cervix is evaluatedto determine if the os is open or closedand whether fluid is present in the endo-cervical canal. The adnexa are carefullyevaluated and measurements of theovaries are obtained in the sagittal andtransverse planes. If a mass is identifiedwithin the adnexa, pressure is appliedwith the probe internally and by the
FIGURE 2. Intradecidual sign. Sagittal trans-vaginal images (A, B) of the uterus demon-strate an eccentrically located smallgestational sac with echogenic rim (arrows).
A B
FIGURE 3. Double decidual sac sign. Transvaginal images (A, B) of the uterus demonstrategestational sac surrounded by 2 hyperechoic curvilinear lines. The inner line (long arrows)represents deciduas capsularis, the outer line (arrowheads) represents deciduas vera (pari-etalis). Also note the yolk sac and small fetal pole.
hand externally on the anterior abdomi-nal wall to determine if the mass is aris-ing from the ovary or is separate fromit. The cul-de-sac is imaged for any evi-dence of free fluid. Color and spectralDoppler waveforms are obtained fromboth ovaries with a resistive index [RI]calculated. Spectral and color Dopplerimaging is also obtained of any abnor-malities seen in the adnexal regionswith calculation of RIs.
Transabdominal imaging of thepelvis is performed if no ectopic preg-nancy is identified transvaginally togive a broader overview of the pelvisand to detect any possible intra-abdominal location of the ectopic preg-nancy. Transabdominal imaging is alsoperformed to evaluate for fluid in thepelvis and in Morison’s pouch. Thearea of the patient’s pain should also beexamined by transabdominal imagingif not adequately visualized on thetransvaginal examination.
Serum ß-hCGHuman chorionic gonadotropin is
produced by the placenta and can bedetected in the serum approximately 9
days after conception (23 days afterthe last menstrual period [LMP]). Anegative serum ß-hCG result essen-tially excludes the diagnosis of a livepregnancy. It is important to note thatseveral reference standards are usedin reporting the results of a serum ß-hCG level and it is essential to knowwhich standard is used by your insti-tution. The third international stan-dard (IS) or international referencepreparation (IRP) is now used mostcommonly. However, early studiesand papers on ectopic pregnancy uti-lized the second IS. Conversion fromthe second IS to the IRP can beachieved by multiplying the second ISby a factor of 1.8.
Utilizing the IRP standard, a gesta-tional sac should be seen on transvagi-nal sonography if the serum ß-hCGlevel is 1800 to 2000 mlU/mL.8 Inearly healthy intrauterine pregnancies,the ß-hCG level should double approx-imately every 2 days.
Normal intrauterine pregnancyTo evaluate for an ectopic pregnancy
or abnormal pregnancy, it is necessary
to recognize the ultrasound findings ofan early normal intrauterine pregnancy(IUP). Documentation of an IUP signif-icantly decreases the likelihood for anectopic pregnancy in most patients. Theearliest sonographic finding of an earlyIUP is the intradecidual sign firstdescribed by Yeh et al. in 1986.9 Seen atapproximately 4.5 weeks after theLMP, the intradecidual sign consists ofa small fluid collection with an echo-genic rim eccentrically located adjacentto, but separate from, the central linearechogenic complex (Figure 2). Thepresence of an echogenic rim aids indistinguishing this entity from a decid-ual cyst. The accuracy of this sign isvariable with reported sensitivitiesranging from 48% to 68% and speci-ficities from 66% to 100%.10,11
By 5 weeks gestational age, a moreclearly defined gestational sac shouldbe observed with a double decidual sacsign present. The double decidual sacsign consists of 2 hyperechoic curvilin-ear lines at the margin of the develop-ing gestational sac separated byhypoechoic material (Figure 3). The 2hyperechoic interfaces result from: theinner decidua capsularis, forming the“free” edge of the enlarging gestationalsac; and, the outer decidua vera (Figure4). The hypoechoic region representsfluid between the 2 structures withinthe endometrial canal.5 The doubledecidual sac sign is a highly accurate
FIGURE 4. Early intrauterine pregnancy. The decidua capsularis and decidua parietalisaccount for the hyperechoic lines resulting in the double decidual sac sign. The hypoechoicregion between the hyperechoic lines is secondary to fluid in the uterine cavity.
FIGURE 5. Early intrauterine pregnancy 6 wk 5 d gestational age. Transvaginalimage of the uterus demonstrates fetal pole(calipers) and yolk sac (arrow).
indicator of an early IUP. Absence ofthis sign does not necessarily excludean early IUP. Other characteristics of anormal intrauterine gestational sacinclude: continuous echogenic rim ofat least 2 mm thickness, spherical orovoid shape, location in the upper ormiddle portion of the uterus, andgrowth >1.2 mm per day.
A yolk sac is usually visualized by5.5 weeks and confirms the presence of
an intrauterine pregnancy. The upperlimit for normal size for the yolk sac is5 to 6 mm. By 11 weeks, the yolk sacstarts to involute. By 6 weeks, anembryonic pole should be identifiableand by 6.0 to 6.5 weeks, cardiac activ-ity should be visualized on real-timeimaging (Figure 5).
Concomitant with the developingintrauterine gestational sac is thedevelopment of the corpus luteum.
From the latin meaning “yellowbody,” the corpus luteum forms fromthe ovarian follicle after ovulation.Signaled by hCG from the developingpregnancy, the corpus luteum secretesprogesterone to maintain the preg-nancy until the placenta assumes thisrole. If no pregnancy develops duringthe normal menstrual cycle, the corpusluteum involutes becoming the corpusalbicans.
Sonographically, the corpus luteumcan have a wide range of appearances.The corpus luteum can appear as an ill-defined, hypoechoic, homogeneousstructure, a thick-walled cystic struc-ture; a complex cystic lesion withinternal echoes; and less commonly, asa thin-walled cyst. Color Dopplerimaging generally demonstrates aperipheral ring of flow around the cor-pus luteum (Figure 6). SpectralDoppler interrogation usually demon-strates a low-resistance waveform withan RI of 0.4 to 0.7.12 Unfortunately, aswill be discussed below, the appear-ance of the corpus luteum can mimican ectopic pregnancy. Differentiationof this normal structure from anectopic pregnancy is essential.
tion or abnormal pregnancy is part ofthe differential diagnosis for a preg-nant patient with pain and bleeding.Certain threshold measurements ofmean sac diameter (MSD):
MSD = (L + W + H)/3These measurements can be
employed to aid in diagnosing a failedpregnancy. The literature reports thatthere should be visualization of a yolksac with MSD >8 mm, visualization ofan embryo with MSD >16 mm, andvisualization of cardiac activity by thetime the embryo is 5 mm in length orMSD >18 mm.13 Failure to meet thesethresholds is consistent with a nonvi-able pregnancy in most cases, espe-cially if the ß-hCG level is not risingnormally. To ensure greater specificity,Levine suggests using a higher thresh-old of 13 mm for nonvisualization of a
IMAGING OF ECTOPIC PREGNANCY
FIGURE 6. Sonographic appearances of the corpus luteum on grayscale imaging. Cystic (A),complex cystic lesion (B) with thick wall (arrow), or solid (calipers). Color Doppler flow image(D) demonstrates peripheral vascularity (arrow) and the so-called “ring of fire.”
A B
C D
FIGURE 7. Abnormal IUP. Sagittal grayscale image (A) of the uterus demonstrates anenlarged gestational sac (MSD = 2.2 cm, 7 wk gestation) without evidence of yolk sac or fetalpole. The sac has a distorted nonovoid contour with a thin decidual reaction (arrow). Distorted,enlarged gestational sac (B) with debris and membranes extending from the lower uterine seg-ment into the cervix. The patient was bleeding and undergoing a spontaneous abortion.
yolk sac and 18 mm for nonvisualiza-tion of an embryo.4
In an abnormal pregnancy, the gesta-tional sac may have a distorted non-ovoid contour. Location in the loweruterine segment may be seen in sponta-neous abortion (Figure 7). With a low-lying gestational sac, one should
carefully evaluate for a fundal fibroid,which may displace a viable gesta-tional sac towards the lower uterinesegment. A thin (<2 mm) decidualreaction around a gestational sac is aworrisome sign, as is an enlarged orcalcified yolk sac. An open cervix isconsistent with an impending abortion.
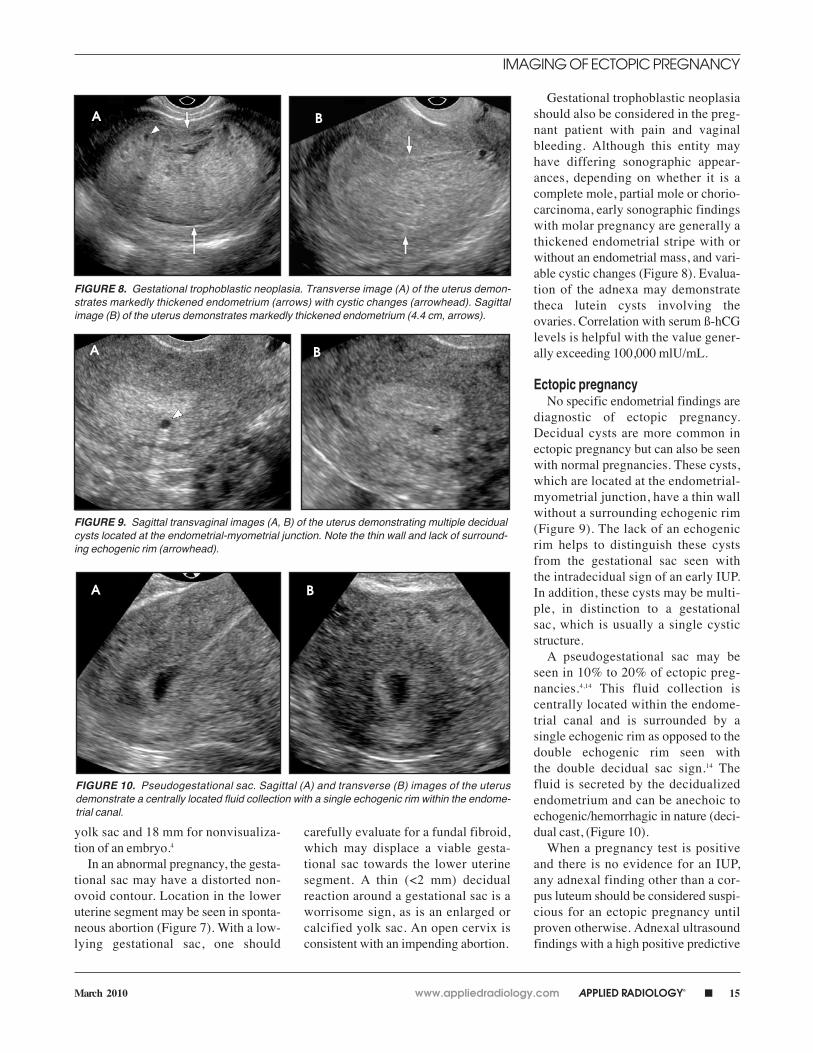
Gestational trophoblastic neoplasiashould also be considered in the preg-nant patient with pain and vaginalbleeding. Although this entity mayhave differing sonographic appear-ances, depending on whether it is acomplete mole, partial mole or chorio-carcinoma, early sonographic findingswith molar pregnancy are generally athickened endometrial stripe with orwithout an endometrial mass, and vari-able cystic changes (Figure 8). Evalua-tion of the adnexa may demonstratetheca lutein cysts involving theovaries. Correlation with serum ß-hCGlevels is helpful with the value gener-ally exceeding 100,000 mlU/mL.
Ectopic pregnancyNo specific endometrial findings are
diagnostic of ectopic pregnancy.Decidual cysts are more common inectopic pregnancy but can also be seenwith normal pregnancies. These cysts,which are located at the endometrial-myometrial junction, have a thin wallwithout a surrounding echogenic rim(Figure 9). The lack of an echogenicrim helps to distinguish these cystsfrom the gestational sac seen with the intradecidual sign of an early IUP.In addition, these cysts may be multi-ple, in distinction to a gestational sac, which is usually a single cysticstructure.
A pseudogestational sac may beseen in 10% to 20% of ectopic preg-nancies.4,14 This fluid collection is centrally located within the endome-trial canal and is surrounded by a single echogenic rim as opposed to thedouble echogenic rim seen with the double decidual sac sign.14 Thefluid is secreted by the decidualizedendometrium and can be anechoic toechogenic/hemorrhagic in nature (deci-dual cast, (Figure 10).
When a pregnancy test is positiveand there is no evidence for an IUP,any adnexal finding other than a cor-pus luteum should be considered suspi-cious for an ectopic pregnancy untilproven otherwise. Adnexal ultrasoundfindings with a high positive predictive
IMAGING OF ECTOPIC PREGNANCY
FIGURE 8. Gestational trophoblastic neoplasia. Transverse image (A) of the uterus demon-strates markedly thickened endometrium (arrows) with cystic changes (arrowhead). Sagittalimage (B) of the uterus demonstrates markedly thickened endometrium (4.4 cm, arrows).
FIGURE 9. Sagittal transvaginal images (A, B) of the uterus demonstrating multiple decidualcysts located at the endometrial-myometrial junction. Note the thin wall and lack of surround-ing echogenic rim (arrowhead).
A B
A B
A B
FIGURE 10. Pseudogestational sac. Sagittal (A) and transverse (B) images of the uterusdemonstrate a centrally located fluid collection with a single echogenic rim within the endome-trial canal.
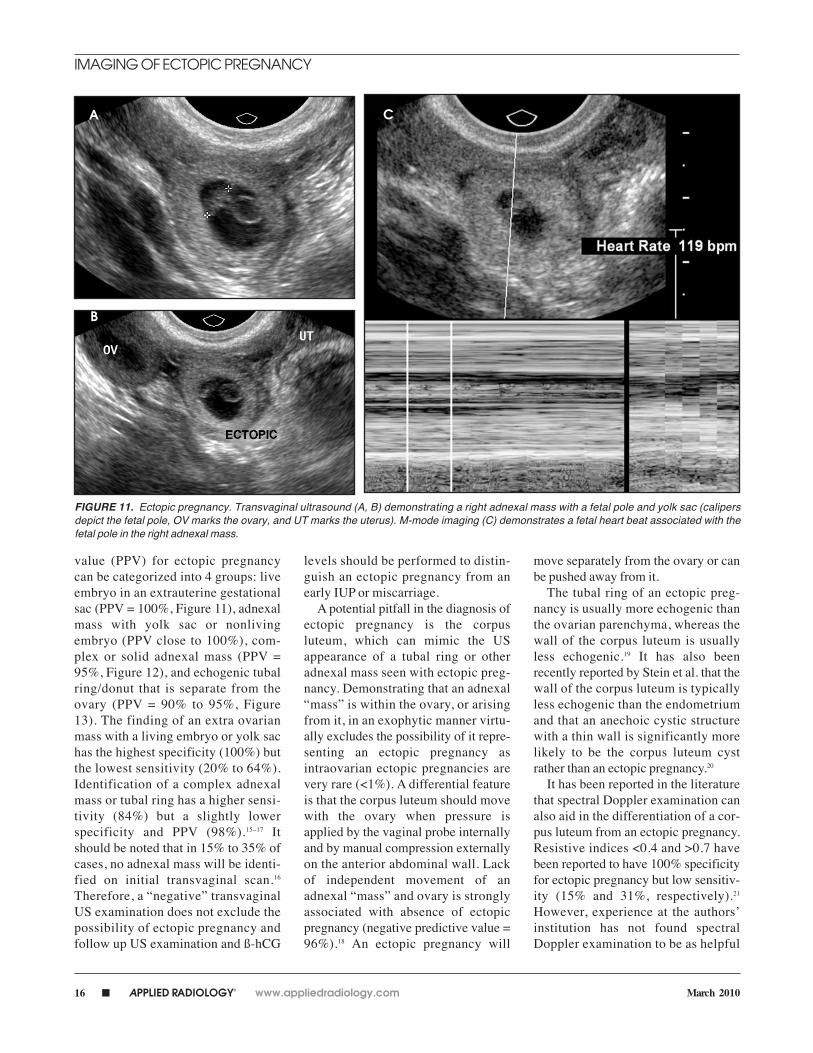
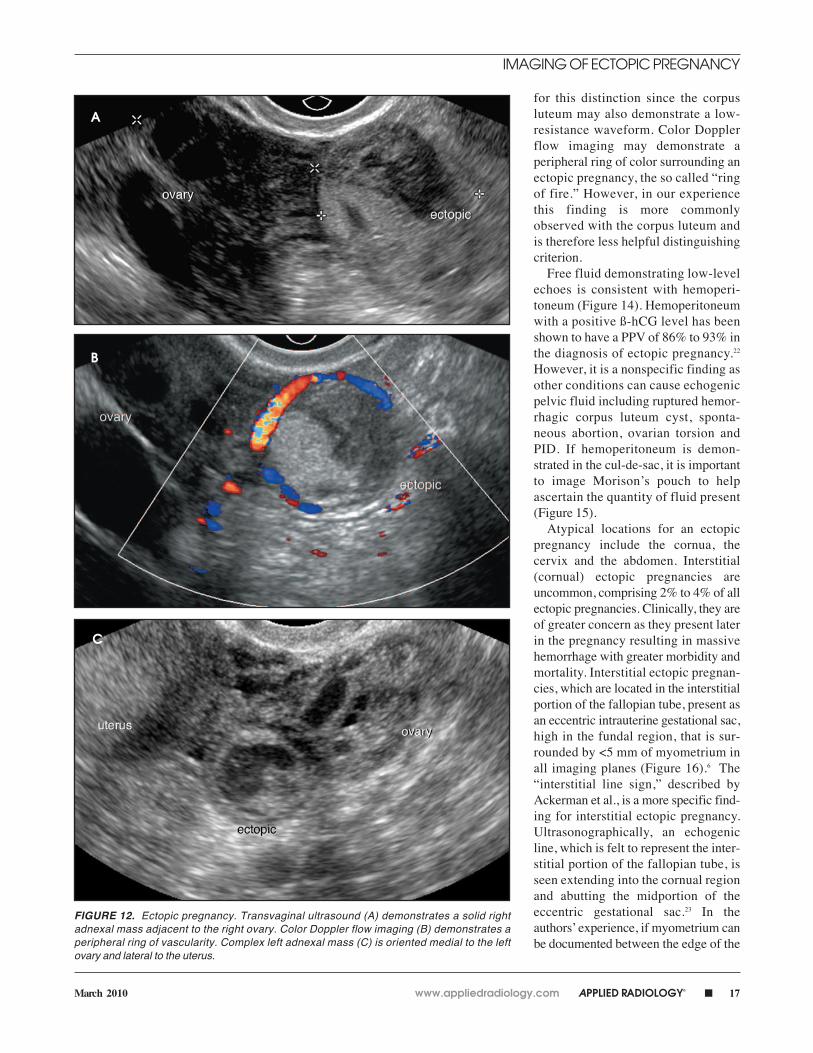
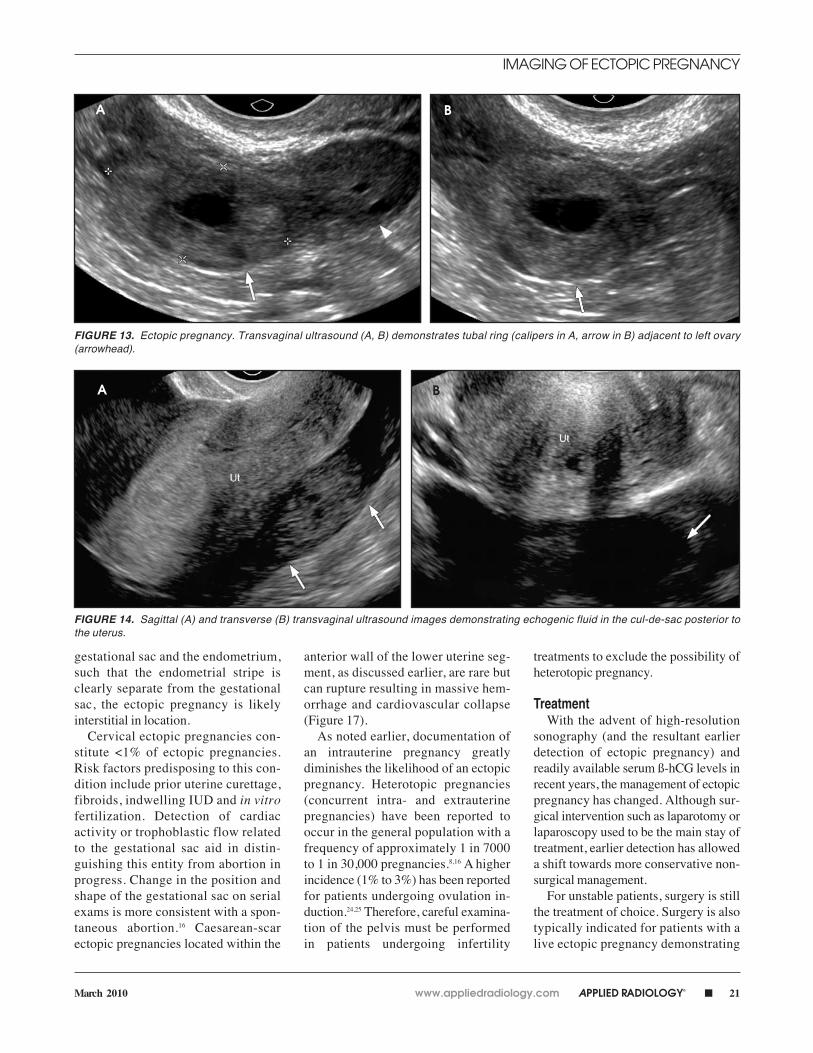
value (PPV) for ectopic pregnancycan be categorized into 4 groups: liveembryo in an extrauterine gestationalsac (PPV = 100%, Figure 11), adnexalmass with yolk sac or nonlivingembryo (PPV close to 100%), com-plex or solid adnexal mass (PPV =95%, Figure 12), and echogenic tubalring/donut that is separate from theovary (PPV = 90% to 95%, Figure13). The finding of an extra ovarianmass with a living embryo or yolk sachas the highest specificity (100%) butthe lowest sensitivity (20% to 64%).Identification of a complex adnexalmass or tubal ring has a higher sensi-tivity (84%) but a slightly lowerspecificity and PPV (98%).15–17 Itshould be noted that in 15% to 35% ofcases, no adnexal mass will be identi-fied on initial transvaginal scan.16
Therefore, a “negative” transvaginalUS examination does not exclude thepossibility of ectopic pregnancy andfollow up US examination and ß-hCG
levels should be performed to distin-guish an ectopic pregnancy from anearly IUP or miscarriage.
A potential pitfall in the diagnosis ofectopic pregnancy is the corpusluteum, which can mimic the USappearance of a tubal ring or otheradnexal mass seen with ectopic preg-nancy. Demonstrating that an adnexal“mass” is within the ovary, or arisingfrom it, in an exophytic manner virtu-ally excludes the possibility of it repre-senting an ectopic pregnancy asintraovarian ectopic pregnancies arevery rare (<1%). A differential featureis that the corpus luteum should movewith the ovary when pressure isapplied by the vaginal probe internallyand by manual compression externallyon the anterior abdominal wall. Lackof independent movement of anadnexal “mass” and ovary is stronglyassociated with absence of ectopicpregnancy (negative predictive value =96%).18 An ectopic pregnancy will
move separately from the ovary or canbe pushed away from it.
The tubal ring of an ectopic preg-nancy is usually more echogenic thanthe ovarian parenchyma, whereas thewall of the corpus luteum is usuallyless echogenic.19 It has also beenrecently reported by Stein et al. that thewall of the corpus luteum is typicallyless echogenic than the endometriumand that an anechoic cystic structurewith a thin wall is significantly morelikely to be the corpus luteum cystrather than an ectopic pregnancy.20
It has been reported in the literaturethat spectral Doppler examination canalso aid in the differentiation of a cor-pus luteum from an ectopic pregnancy.Resistive indices <0.4 and >0.7 havebeen reported to have 100% specificityfor ectopic pregnancy but low sensitiv-ity (15% and 31%, respectively).21
However, experience at the authors’institution has not found spectralDoppler examination to be as helpful
IMAGING OF ECTOPIC PREGNANCY
FIGURE 11. Ectopic pregnancy. Transvaginal ultrasound (A, B) demonstrating a right adnexal mass with a fetal pole and yolk sac (calipersdepict the fetal pole, OV marks the ovary, and UT marks the uterus). M-mode imaging (C) demonstrates a fetal heart beat associated with thefetal pole in the right adnexal mass.
for this distinction since the corpusluteum may also demonstrate a low-resistance waveform. Color Dopplerflow imaging may demonstrate aperipheral ring of color surrounding anectopic pregnancy, the so called “ringof fire.” However, in our experiencethis finding is more commonlyobserved with the corpus luteum and is therefore less helpful distinguishingcriterion.
Free fluid demonstrating low-levelechoes is consistent with hemoperi-toneum (Figure 14). Hemoperitoneumwith a positive ß-hCG level has beenshown to have a PPV of 86% to 93% inthe diagnosis of ectopic pregnancy.22
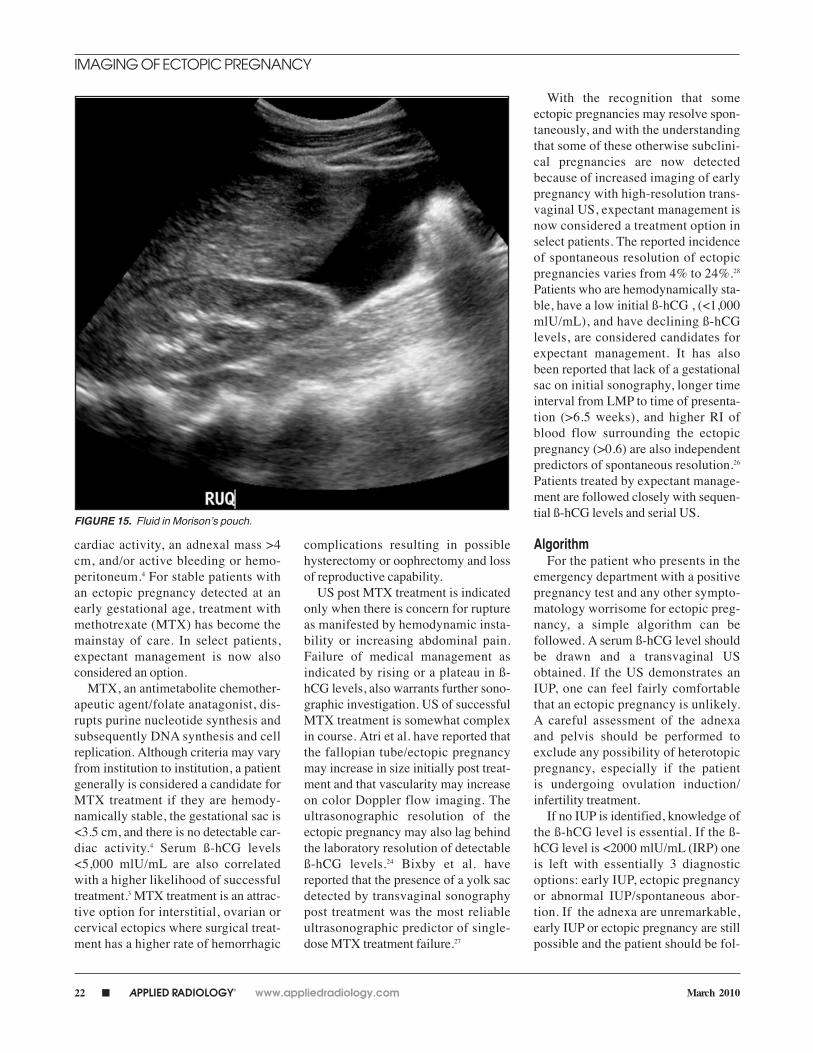
However, it is a nonspecific finding asother conditions can cause echogenicpelvic fluid including ruptured hemor-rhagic corpus luteum cyst, sponta-neous abortion, ovarian torsion andPID. If hemoperitoneum is demon-strated in the cul-de-sac, it is importantto image Morison’s pouch to helpascertain the quantity of fluid present(Figure 15).
Atypical locations for an ectopicpregnancy include the cornua, thecervix and the abdomen. Interstitial(cornual) ectopic pregnancies areuncommon, comprising 2% to 4% of allectopic pregnancies. Clinically, they areof greater concern as they present laterin the pregnancy resulting in massivehemorrhage with greater morbidity andmortality. Interstitial ectopic pregnan-cies, which are located in the interstitialportion of the fallopian tube, present asan eccentric intrauterine gestational sac,high in the fundal region, that is sur-rounded by <5 mm of myometrium inall imaging planes (Figure 16).6 The“interstitial line sign,” described byAckerman et al., is a more specific find-ing for interstitial ectopic pregnancy.Ultrasonographically, an echogenicline, which is felt to represent the inter-stitial portion of the fallopian tube, isseen extending into the cornual regionand abutting the midportion of theeccentric gestational sac.23 In theauthors’ experience, if myometrium canbe documented between the edge of the
IMAGING OF ECTOPIC PREGNANCY
FIGURE 12. Ectopic pregnancy. Transvaginal ultrasound (A) demonstrates a solid rightadnexal mass adjacent to the right ovary. Color Doppler flow imaging (B) demonstrates aperipheral ring of vascularity. Complex left adnexal mass (C) is oriented medial to the leftovary and lateral to the uterus.
gestational sac and the endometrium,such that the endometrial stripe isclearly separate from the gestationalsac, the ectopic pregnancy is likelyinterstitial in location.
Cervical ectopic pregnancies con-stitute <1% of ectopic pregnancies.Risk factors predisposing to this con-dition include prior uterine curettage,fibroids, indwelling IUD and in vitrofertilization. Detection of cardiacactivity or trophoblastic flow relatedto the gestational sac aid in distin-guishing this entity from abortion inprogress. Change in the position andshape of the gestational sac on serialexams is more consistent with a spon-taneous abortion.16 Caesarean-scarectopic pregnancies located within the
anterior wall of the lower uterine seg-ment, as discussed earlier, are rare butcan rupture resulting in massive hem-orrhage and cardiovascular collapse(Figure 17).
As noted earlier, documentation ofan intrauterine pregnancy greatlydiminishes the likelihood of an ectopicpregnancy. Heterotopic pregnancies(concurrent intra- and extrauterinepregnancies) have been reported tooccur in the general population with afrequency of approximately 1 in 7000to 1 in 30,000 pregnancies.8,16 A higherincidence (1% to 3%) has been reportedfor patients undergoing ovulation in-duction.24,25 Therefore, careful examina-tion of the pelvis must be performed in patients undergoing infertility
treatments to exclude the possibility ofheterotopic pregnancy.
TreatmentWith the advent of high-resolution
sonography (and the resultant earlierdetection of ectopic pregnancy) andreadily available serum ß-hCG levels inrecent years, the management of ectopicpregnancy has changed. Although sur-gical intervention such as laparotomy orlaparoscopy used to be the main stay oftreatment, earlier detection has alloweda shift towards more conservative non-surgical management.
For unstable patients, surgery is stillthe treatment of choice. Surgery is alsotypically indicated for patients with alive ectopic pregnancy demonstrating
FIGURE 13. Ectopic pregnancy. Transvaginal ultrasound (A, B) demonstrates tubal ring (calipers in A, arrow in B) adjacent to left ovary(arrowhead).
FIGURE 14. Sagittal (A) and transverse (B) transvaginal ultrasound images demonstrating echogenic fluid in the cul-de-sac posterior tothe uterus.
cardiac activity, an adnexal mass >4cm, and/or active bleeding or hemo-peritoneum.4 For stable patients withan ectopic pregnancy detected at anearly gestational age, treatment withmethotrexate (MTX) has become themainstay of care. In select patients,expectant management is now alsoconsidered an option.
MTX, an antimetabolite chemother-apeutic agent/folate anatagonist, dis-rupts purine nucleotide synthesis andsubsequently DNA synthesis and cellreplication. Although criteria may varyfrom institution to institution, a patientgenerally is considered a candidate forMTX treatment if they are hemody-namically stable, the gestational sac is<3.5 cm, and there is no detectable car-diac activity.4 Serum ß-hCG levels<5,000 mlU/mL are also correlatedwith a higher likelihood of successfultreatment.3 MTX treatment is an attrac-tive option for interstitial, ovarian orcervical ectopics where surgical treat-ment has a higher rate of hemorrhagic
complications resulting in possiblehysterectomy or oophrectomy and lossof reproductive capability.
US post MTX treatment is indicatedonly when there is concern for ruptureas manifested by hemodynamic insta-bility or increasing abdominal pain.Failure of medical management asindicated by rising or a plateau in ß-hCG levels, also warrants further sono-graphic investigation. US of successfulMTX treatment is somewhat complexin course. Atri et al. have reported thatthe fallopian tube/ectopic pregnancymay increase in size initially post treat-ment and that vascularity may increaseon color Doppler flow imaging. Theultrasonographic resolution of theectopic pregnancy may also lag behindthe laboratory resolution of detectableß-hCG levels.24 Bixby et al. havereported that the presence of a yolk sacdetected by transvaginal sonographypost treatment was the most reliableultrasonographic predictor of single-dose MTX treatment failure.27
With the recognition that someectopic pregnancies may resolve spon-taneously, and with the understandingthat some of these otherwise subclini-cal pregnancies are now detectedbecause of increased imaging of earlypregnancy with high-resolution trans-vaginal US, expectant management isnow considered a treatment option inselect patients. The reported incidenceof spontaneous resolution of ectopicpregnancies varies from 4% to 24%.28
Patients who are hemodynamically sta-ble, have a low initial ß-hCG , (<1,000mlU/mL), and have declining ß-hCGlevels, are considered candidates forexpectant management. It has alsobeen reported that lack of a gestationalsac on initial sonography, longer timeinterval from LMP to time of presenta-tion (>6.5 weeks), and higher RI ofblood flow surrounding the ectopicpregnancy (>0.6) are also independentpredictors of spontaneous resolution.26
Patients treated by expectant manage-ment are followed closely with sequen-tial ß-hCG levels and serial US.
AlgorithmFor the patient who presents in the
emergency department with a positivepregnancy test and any other sympto-matology worrisome for ectopic preg-nancy, a simple algorithm can befollowed. A serum ß-hCG level shouldbe drawn and a transvaginal USobtained. If the US demonstrates anIUP, one can feel fairly comfortablethat an ectopic pregnancy is unlikely.A careful assessment of the adnexa and pelvis should be performed toexclude any possibility of heterotopicpregnancy, especially if the patient is undergoing ovulation induction/ infertility treatment.
If no IUP is identified, knowledge ofthe ß-hCG level is essential. If the ß-hCG level is <2000 mlU/mL (IRP) oneis left with essentially 3 diagnosticoptions: early IUP, ectopic pregnancyor abnormal IUP/spontaneous abor-tion. If the adnexa are unremarkable,early IUP or ectopic pregnancy are stillpossible and the patient should be fol-
lowed up with repeat US in 5 to 7 daysand serial ß-hCG levels obtained. His-tory and physical exam findings are alsohelpful as lack of vaginal bleeding makesthe diagnosis of miscarriage less likely,whereas a large amount of vaginal bleed-ing is more consistent with spontaneousabortion. If any abnormality is identifiedin the adnexal regions, ectopic preg-nancy should be the presumptive diagno-sis until proven otherwise.
If the ß-hCG level is >2000 mlU/mL,an intrauterine gestational sac shouldbe seen. If no intrauterine gestationalsac is identified, ectopic pregnancyshould be strongly considered. If an adnexal abnormality is identified,the presumptive diagnosis is ectopic
pregnancy until proven otherwise. Ifno adnexal abnormality is seen, closefollow-up US and serial ß-hCG levelsshould be performed.
Patients with an abnormal IUP orwho are undergoing a spontaneousabortion should demonstrate abnormalfindings within the endometrial cavity.Findings include abnormal gestationalsac or avascular heterogenous materialconsistent with blood clot. Heteroge-neous material/endometrial thickeningwith trophoblastic flow is consistentwith retained products of conception.
ConclusionTransvaginal sonography and serum
ß-hCG level assays have changed
the course and management of ectopicpregnancy. Once considered to be a surgical emergency, earlier and more expeditious diagnosis with trans-vaginal sonography has changed themanagement approach to ectopic preg-nancy, such that maintaining fertilitywith medical and expectant manage-ment is now possible. Knowledge of the US findings of normal early IUP, abnormal intrauterine pregnancy/ spontaneous abortion, and ectopicpregnancy is essential. Correlation withserum ß-hCG levels and physical find-ings allows the radiologist to formulatea quick and accurate diagnosis and recommend the appropriate follow-upand treatment.
FIGURE 17. Sagittal grayscale (A) and color Doppler (B) transvaginal images demonstrate an ectopic pregnancy in the wall of the myometriumin the lower uterine segment at the site of previous ceasarean-section scar.
A B
A B
FIGURE 16. Interstitial ectopic pregnancy. Transverse (A) and sagittal (B) transvaginal ultrasound images demonstrate a gestational sac in thecornual (interstitial) region of the uterus/fallopian tube. Note the lack of surrounding myometrium around the gestational sac (arrow).
REFERENCES1. Centers for Disease Control. Ectopic pregnancy–United States, 1988–1989. Morbid Mortal WeeklyRep. 1992;41:591–594.2. Speroff L, Fritz M. Clinical GynecologicEndocrinology and Infertility. Philadelphia: Lippin-cott, Williams, and Wilkins; 2004:1275–12773. Sepilian VP, Wood E. Ectopic Pregnancy. Emed-icine (online). August 2007. 4. Levine D. Ectopic Pregnancy. Radiology.2007;245:385–397.5.Atri M, Leduc C, Gillett P, et al. Role of endovagi-nal sonography in the diagnosis and managementof ectopic pregnancy. Radiographics. 1996;16:755–774.6. Lin EP, Bhatt S, Dogra VS. Diagnostic clues toectopic pregnancy. Radiographics. 2008;28:1661–1671.7. Schwartz RO, Di Pietro DL. Beta-hCG as a diag-nostic aid for suspected ectopic pregnancy. ObstetGynecol. 1980;56:197–203.8. Scoutt LM. Sonographic evaluation of acutepelvic pain in women. 2008 ARRS CategoricalCourse Syllabus:p.1–5.9. Yeh HC, Goodman JD, Carr L, Rabinowitz JG.Intradecuidual sign: A US criterion of early intrauter-ine pregnancy. Radiology. 1999;161:463–467.10. Chiang G, Levine D, Swire M, et al. The intrade-cidual sign: Is it reliable for diagnosis of earlyintrauterine pregnancy? AJR Am J. Roentgenol.2004;183:725–731.11. Laing FC, Brown DL, Price JF, et al. Intradecid-ual sign: Is it effective in diagnosis of an early
intrauterine pregnancy? Radiology. 1997;204:665–660.12. Durfee SM, Frates MC. Sonographic spectrumof the corpus luteum in early pregnancy: Grayscale, color, and pulsed Doppler appearance. JClin Ultrasound. 1999;27:55–59.13. Levi CS, Lyons EA, Lindsay DJ. Early diagnosisof nonviable pregnancy with endovaginal US. Radi-ology. 1988;167:383–385.14. Fleischer A, Pennell RG, McKee MS, et al.Ectopic pregnancy: Features at transvaginalsonography. Radiology. 1990;174:375–378.15. Brown DL, Doubilet PM. Transvaginal sonogra-phy for diagnosing ectopic pregnancy: Positivity cri-teria and performance characteristics. J UltrasoundMed. 1994;13:259–266.16. Frates MC, Laing FC. Sonographic evaluationof ectopic pregnancy: An update. AJR Am J.Roentgenol. 1995;165:251–259.17. Nyberg DA, Hughes MP, Mack LA, Wang KY.Extrauterine findings of ectopic pregnancy at trans-vaginal US: Importance of echogenic fluid. Radiol-ogy. 1991;178:823–826.18. Blaivas M, Lyon M. Reliability of adnexal massmobility in distinguishing possible ectopic preg-nancy from corpus luteum cysts. J Ultrasound Med.2005;24:599–603. 19. Frates MC, Visweswaran A, Laing FC. Compar-ison of tubal ring and corpus luteum echogenicities:A useful differentiating characteristic. J UltrasoundMed. 2001;20:27–31.20. Stein MW, Ricci ZJ, Novak L, et al. Sonographiccomparison of the tubal ring of ectopic pregnancy
with the corpus luteum. J Ultrasound Med. 2004;23:57–62.21. Atri M. Ectopic pregnancy versus corpus luteumcyst revisited: Best Doppler predictors. J Ultra-sound Med. 2003;22:1181–1184.22. Russell SA, Filly RA, Damato N. Sonographicdiagnosis of ectopic pregnancy with endovaginalprobes: What really has changed? J UltrasoundMed. 1993;12:145–151.23. Ackerman TE, Levi CS, Dashefsky SM, et al.Interstitial line: Sonographic findings in interstitial(cornual) ectopic pregnancy. Radiology. 1993;189:83–87.24. Rizk B, Tan SL, Morcos S, et al. Heterotopicpregnancies after in vitro fertilization and embryotransfer. Am J Obstet Gynecol. 1991;164:161–164.25. Fernandez H, Gervaise A. Ectopic pregnanciesafter infertility treatment: Modern diagnosis andtherapeutic strategy. Human Reprod Update.2004;10:503–513.26. Atri M, Bret P, Tulandi T, Senterman MK.Ectopic pregnancy: Evolution after treatment withtransvaginal methotrexate. Radiology. 1992;185:749–753.27. Bixby S, Tello R, Kuligowska E. Presence of ayolk sac on transvaginal sonography is the mostreliable predictor of single-dose methotrexate treat-ment failure in ectopic pregnancy. J UltrasoundMed. 2005;24:591–598.28. Atri M, Chow CM, Kintzen G, et al. Expectanttreatment of ectopic pregnancies: Clinical andsonographic predictors. AJR Am J. Roentgenol.2001;176:123–127.













![Case Report Laparoscopic Management of Cornual Ectopic ... · ectopic pregnancies [1-14]. In general, risk factors for CEP are similar to those for ectopic pregnancy, and ipsilateral](https://static.documents.pub/doc/80x56/603719f53ca964727a5a9df3/case-report-laparoscopic-management-of-cornual-ectopic-ectopic-pregnancies-1-14.jpg)









![Recurrent Ectopic Pregnancies: A ra þtý m Analysis of Risk ... · ectopic pregnancy increases the risk of consequent ectopic pregnancies [2]. In the literature, there are few studies](https://static.documents.pub/doc/80x56/5e7ed4ffeeff774ac9229124/recurrent-ectopic-pregnancies-a-ra-t-m-analysis-of-risk-ectopic-pregnancy.jpg)