Immediate dentin sealing improves bond strength of indirect restorations Pascal Magne, DMD, PhD, a Tae Hyung Kim, DDS, b Domenico Cascione, CDT, c and Terence E. Donovan, DDS d Division of Primary Oral Health Care, University of Southern California, School of Dentistry, Los Angeles, Calif Statement of problem. Delayed dentin sealing is traditionally performed with indirect restorations. With this technique, dentin is sealed after the provisional phase at the cementation appointment. It was demonstrated that this chronology does not provide optimal conditions for bonding procedures. Immediate dentin sealing (IDS) is a new approach in which dentin is sealed immediately following tooth preparation, before making the impression. Purpose. The purpose of this study was to determine whether there were differences in microtensile bond strength to human dentin using IDS technique compared to delayed dentin sealing (DDS). Material and methods. Fifteen freshly extracted human molars were obtained and divided into 3 groups of 5 teeth. A 3-step etch-and-rinse dentin bonding agent (DBA) (OptiBond FL) was used for all groups. The control (C) specimens were prepared using a direct immediate bonding technique. The DDS specimens were prepared using an indirect approach with DDS. Preparation of the IDS specimens also used an indirect approach with IDS immediately following preparation. All teeth were prepared for a nontrimming microtensile bond strength test. Specimens were stored in water for 24 hours. Eleven beams (0.9 3 0.9 3 11 mm) from each tooth were selected for testing. Bond strength data (MPa) were analyzed with a Kruskal-Wallis test, and post hoc comparison was done using the Mann-Whitney U test (a=.05). Specimens were also evaluated for mode of fracture using scan- ning electron microscope (SEM) analysis. Results. The mean microtensile bond strengths of C and IDS groups were not statistically different from one another at 55.06 and 58.25 MPa, respectively. The bond strength for DDS specimens, at 11.58 MPa, was sta- tistically different (P=.0081) from the other 2 groups. Microscopic evaluation of failure modes indicated that most failures in the DDS group were interfacial, whereas failures in the C and IDS groups were both cohesive and interfacial. SEM analysis indicated that for C and IDS specimens, failure was mixed within the adhesive and cohesively failed dentin. For DDS specimens, failure was generally at the top of the hybrid layer in the adhesive. SEM analysis of intact slabs demonstrated a well-organized hybrid layer 3 to 5 mm thick for the C and IDS groups. For DDS specimens the hybrid layer presented a marked disruption with the overlying resin. Conclusions. When preparing teeth for indirect bonded restorations, IDS with a 3-step etch-and-rinse filled DBA, prior to impression making, results in improved microtensile bond strength compared to DDS. This tech- nique also eliminates any concerns regarding the film thickness of the dentin sealant. (J Prosthet Dent 2005;94:511-9.) CLINICAL IMPLICATIONS Tooth preparation for indirect bonded restorations such as composite/ceramic inlays, onlays, and veneers can generate significant dentin exposure. The results of this study indicate that freshly cut dentin surfaces may be sealed with a dentin bonding agent immediately following tooth prepa- ration, prior to impression making. A 3-step etch-and-rinse dentin bonding agent with a filled adhesive resin is recommended for this purpose. If a considerable area of dentin has been exposed during tooth preparation for indirect bonded restora- tions, it is suggested that a dentin adhesive be applied strictly according to the manufacturer’s instructions. Successful dentin bonding is of particular clinical im- portance for inlays, onlays, veneers, and dentin-bonded porcelain crowns because the final strength of the tooth- restoration complex is highly dependent on adhesive procedures. Long-term clinical trials by Dumfahrt and Schaffer 1 and Friedman 2 showed that porcelain veneers partially bonded to dentin have an increased risk of fail- ure. Advances in dentin bonding agent (DBA) appli- cation techniques 3-15 suggest that these failures can likely be prevented by changing the application proce- dure of the DBA. In fact, there are principles that should a Associate Professor, Don and Sybil Harrington Foundation Chair of Esthetic Dentistry. b Assistant Professor. c Dental Technologist. d Professor and Co-Chair, Director of Advanced Education in Prosthodontics. DECEMBER 2005 THE JOURNAL OF PROSTHETIC DENTISTRY 511
Transcript
Immediate dentin sealing improves bond strength of indirect restorations
Division of Primary Oral Health Care, University of Southern California, School of Dentistry,Los Angeles, Calif
Statement of problem. Delayed dentin sealing is traditionally performed with indirect restorations. With thistechnique, dentin is sealed after the provisional phase at the cementation appointment. It was demonstratedthat this chronology does not provide optimal conditions for bonding procedures. Immediate dentin sealing(IDS) is a new approach in which dentin is sealed immediately following tooth preparation, before makingthe impression.
Purpose. The purpose of this study was to determine whether there were differences in microtensile bondstrength to human dentin using IDS technique compared to delayed dentin sealing (DDS).
Material and methods. Fifteen freshly extracted human molars were obtained and divided into 3 groups of 5teeth. A 3-step etch-and-rinse dentin bonding agent (DBA) (OptiBond FL) was used for all groups. The control(C) specimens were prepared using a direct immediate bonding technique. The DDS specimens were preparedusing an indirect approach with DDS. Preparation of the IDS specimens also used an indirect approach with IDSimmediately following preparation. All teeth were prepared for a nontrimming microtensile bond strength test.Specimens were stored in water for 24 hours. Eleven beams (0.93 0.93 11 mm) from each tooth were selectedfor testing. Bond strength data (MPa) were analyzed with a Kruskal-Wallis test, and post hoc comparison wasdone using the Mann-Whitney U test (a=.05). Specimens were also evaluated for mode of fracture using scan-ning electron microscope (SEM) analysis.
Results. The mean microtensile bond strengths of C and IDS groups were not statistically different from oneanother at 55.06 and 58.25 MPa, respectively. The bond strength for DDS specimens, at 11.58 MPa, was sta-tistically different (P=.0081) from the other 2 groups. Microscopic evaluation of failure modes indicated thatmost failures in the DDS group were interfacial, whereas failures in the C and IDS groups were both cohesiveand interfacial. SEM analysis indicated that for C and IDS specimens, failure was mixed within the adhesive andcohesively failed dentin. For DDS specimens, failure was generally at the top of the hybrid layer in the adhesive.SEM analysis of intact slabs demonstrated a well-organized hybrid layer 3 to 5 mm thick for the C and IDSgroups. For DDS specimens the hybrid layer presented a marked disruption with the overlying resin.
Conclusions. When preparing teeth for indirect bonded restorations, IDS with a 3-step etch-and-rinse filledDBA, prior to impression making, results in improved microtensile bond strength compared to DDS. This tech-nique also eliminates any concerns regarding the film thickness of the dentin sealant. (J Prosthet Dent2005;94:511-9.)
CLINICAL IMPLICATIONS
Tooth preparation for indirect bonded restorations such as composite/ceramic inlays, onlays, andveneers can generate significant dentin exposure. The results of this study indicate that freshly cutdentin surfaces may be sealed with a dentin bonding agent immediately following tooth prepa-ration, prior to impression making. A 3-step etch-and-rinse dentin bonding agent with a filledadhesive resin is recommended for this purpose.
If a considerable area of dentin has been exposedduring tooth preparation for indirect bonded restora-tions, it is suggested that a dentin adhesive be appliedstrictly according to the manufacturer’s instructions.
aAssociate Professor, Don and Sybil Harrington Foundation Chair ofEsthetic Dentistry.
bAssistant Professor.cDental Technologist.dProfessor and Co-Chair, Director of Advanced Education in
Prosthodontics.
DECEMBER 2005
Successful dentin bonding is of particular clinical im-portance for inlays, onlays, veneers, and dentin-bondedporcelain crowns because the final strength of the tooth-restoration complex is highly dependent on adhesiveprocedures. Long-term clinical trials by Dumfahrt andSchaffer1 and Friedman2 showed that porcelain veneerspartially bonded to dentin have an increased risk of fail-ure. Advances in dentin bonding agent (DBA) appli-cation techniques3-15 suggest that these failures canlikely be prevented by changing the application proce-dure of the DBA. In fact, there are principles that should
THE JOURNAL OF PROSTHETIC DENTISTRY 511
THE JOURNAL OF PROSTHETIC DENTISTRY MAGNE ET AL
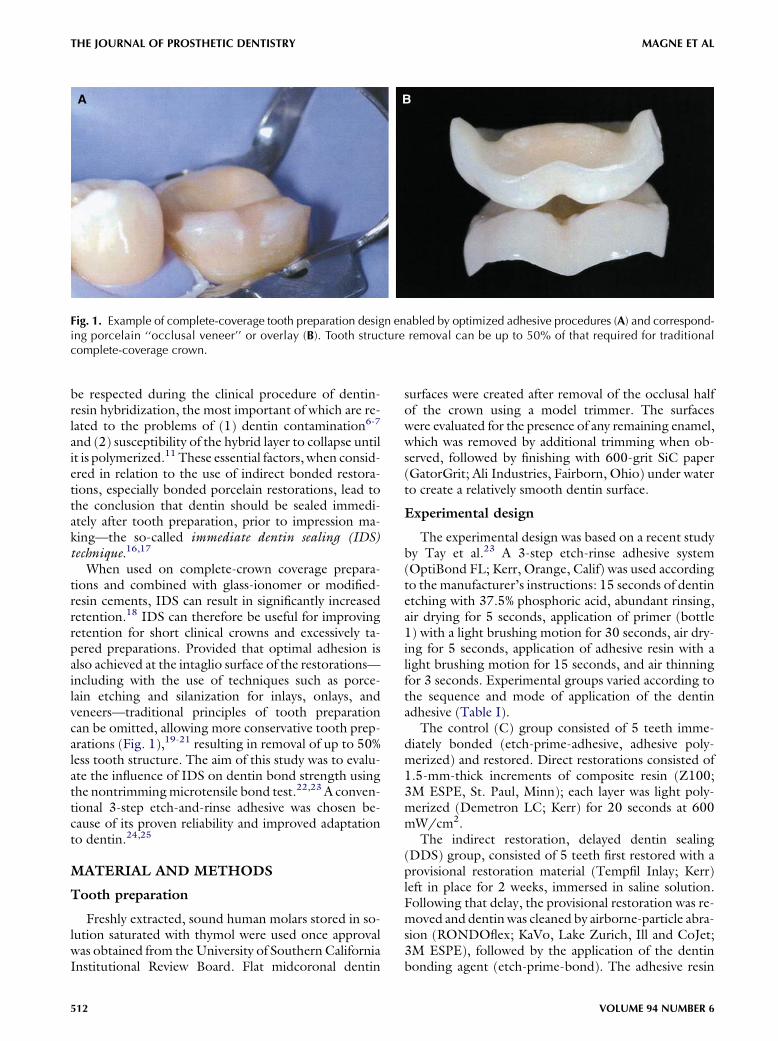
Fig. 1. Example of complete-coverage tooth preparation design enabled by optimized adhesive procedures (A) and correspond-ing porcelain ‘‘occlusal veneer’’ or overlay (B). Tooth structure removal can be up to 50% of that required for traditionalcomplete-coverage crown.
be respected during the clinical procedure of dentin-resin hybridization, the most important of which are re-lated to the problems of (1) dentin contamination6-7
and (2) susceptibility of the hybrid layer to collapse untilit is polymerized.11 These essential factors, when consid-ered in relation to the use of indirect bonded restora-tions, especially bonded porcelain restorations, lead tothe conclusion that dentin should be sealed immedi-ately after tooth preparation, prior to impression ma-king—the so-called immediate dentin sealing (IDS)technique.16,17
When used on complete-crown coverage prepara-tions and combined with glass-ionomer or modified-resin cements, IDS can result in significantly increasedretention.18 IDS can therefore be useful for improvingretention for short clinical crowns and excessively ta-pered preparations. Provided that optimal adhesion isalso achieved at the intaglio surface of the restorations—including with the use of techniques such as porce-lain etching and silanization for inlays, onlays, andveneers—traditional principles of tooth preparationcan be omitted, allowing more conservative tooth prep-arations (Fig. 1),19-21 resulting in removal of up to 50%less tooth structure. The aim of this study was to evalu-ate the influence of IDS on dentin bond strength usingthe nontrimmingmicrotensile bond test.22,23 A conven-tional 3-step etch-and-rinse adhesive was chosen be-cause of its proven reliability and improved adaptationto dentin.24,25
MATERIAL AND METHODS
Tooth preparation
Freshly extracted, sound human molars stored in so-lution saturated with thymol were used once approvalwas obtained from theUniversity of Southern CaliforniaInstitutional Review Board. Flat midcoronal dentin
512
surfaces were created after removal of the occlusal halfof the crown using a model trimmer. The surfaceswere evaluated for the presence of any remaining enamel,which was removed by additional trimming when ob-served, followed by finishing with 600-grit SiC paper(GatorGrit; Ali Industries, Fairborn, Ohio) under waterto create a relatively smooth dentin surface.
Experimental design
The experimental design was based on a recent studyby Tay et al.23 A 3-step etch-rinse adhesive system(OptiBond FL; Kerr, Orange, Calif) was used accordingto the manufacturer’s instructions: 15 seconds of dentinetching with 37.5% phosphoric acid, abundant rinsing,air drying for 5 seconds, application of primer (bottle1) with a light brushing motion for 30 seconds, air dry-ing for 5 seconds, application of adhesive resin with alight brushing motion for 15 seconds, and air thinningfor 3 seconds. Experimental groups varied according tothe sequence and mode of application of the dentinadhesive (Table I).
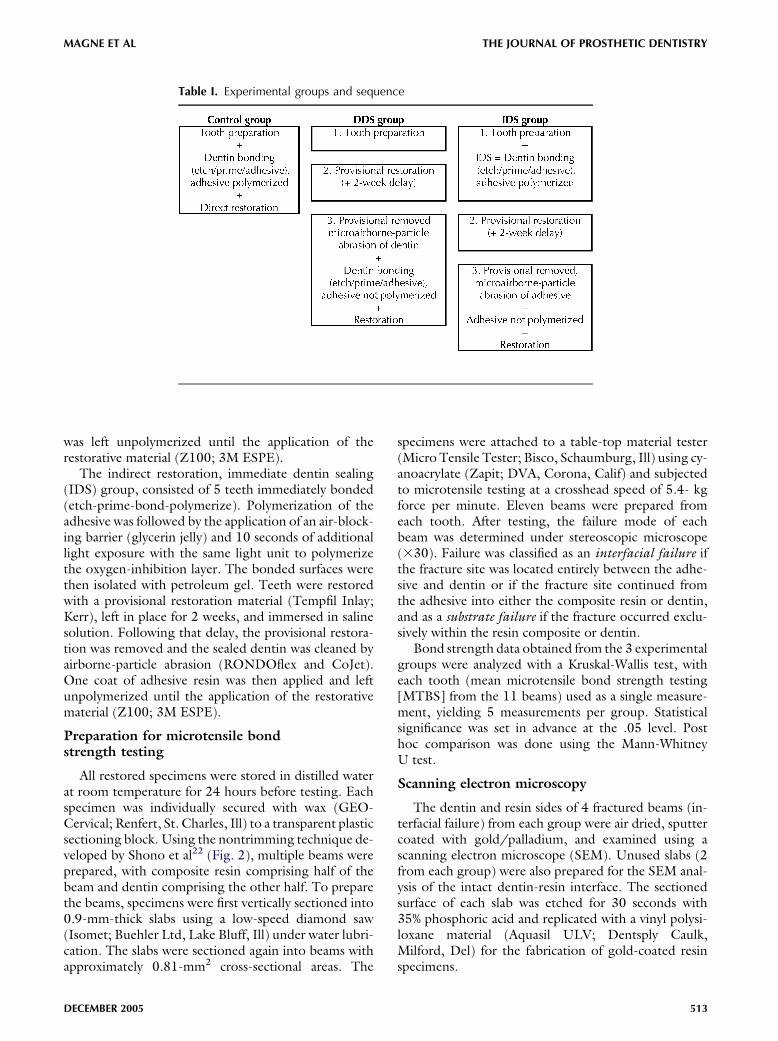
The control (C) group consisted of 5 teeth imme-diately bonded (etch-prime-adhesive, adhesive poly-merized) and restored. Direct restorations consisted of1.5-mm-thick increments of composite resin (Z100;3M ESPE, St. Paul, Minn); each layer was light poly-merized (Demetron LC; Kerr) for 20 seconds at 600mW/cm2.
The indirect restoration, delayed dentin sealing(DDS) group, consisted of 5 teeth first restored with aprovisional restoration material (Tempfil Inlay; Kerr)left in place for 2 weeks, immersed in saline solution.Following that delay, the provisional restoration was re-moved and dentinwas cleaned by airborne-particle abra-sion (RONDOflex; KaVo, Lake Zurich, Ill and CoJet;3M ESPE), followed by the application of the dentinbonding agent (etch-prime-bond). The adhesive resin
VOLUME 94 NUMBER 6
THE JOURNAL OF PROSTHETIC DENTISTRYMAGNE ET AL
DECEM
Table I. Experimental groups and sequence
was left unpolymerized until the application of therestorative material (Z100; 3M ESPE).
The indirect restoration, immediate dentin sealing(IDS) group, consisted of 5 teeth immediately bonded(etch-prime-bond-polymerize). Polymerization of theadhesive was followed by the application of an air-block-ing barrier (glycerin jelly) and 10 seconds of additionallight exposure with the same light unit to polymerizethe oxygen-inhibition layer. The bonded surfaces werethen isolated with petroleum gel. Teeth were restoredwith a provisional restoration material (Tempfil Inlay;Kerr), left in place for 2 weeks, and immersed in salinesolution. Following that delay, the provisional restora-tion was removed and the sealed dentin was cleaned byairborne-particle abrasion (RONDOflex and CoJet).One coat of adhesive resin was then applied and leftunpolymerized until the application of the restorativematerial (Z100; 3M ESPE).
Preparation for microtensile bondstrength testing
All restored specimens were stored in distilled waterat room temperature for 24 hours before testing. Eachspecimen was individually secured with wax (GEO-Cervical; Renfert, St. Charles, Ill) to a transparent plasticsectioning block. Using the nontrimming technique de-veloped by Shono et al22 (Fig. 2), multiple beams wereprepared, with composite resin comprising half of thebeam and dentin comprising the other half. To preparethe beams, specimens were first vertically sectioned into0.9-mm-thick slabs using a low-speed diamond saw(Isomet; Buehler Ltd, Lake Bluff, Ill) under water lubri-cation. The slabs were sectioned again into beams withapproximately 0.81-mm2 cross-sectional areas. The
BER 2005
specimens were attached to a table-top material tester(Micro Tensile Tester; Bisco, Schaumburg, Ill) using cy-anoacrylate (Zapit; DVA, Corona, Calif) and subjectedto microtensile testing at a crosshead speed of 5.4- kgforce per minute. Eleven beams were prepared fromeach tooth. After testing, the failure mode of eachbeam was determined under stereoscopic microscope(330). Failure was classified as an interfacial failure ifthe fracture site was located entirely between the adhe-sive and dentin or if the fracture site continued fromthe adhesive into either the composite resin or dentin,and as a substrate failure if the fracture occurred exclu-sively within the resin composite or dentin.
Bond strength data obtained from the 3 experimentalgroups were analyzed with a Kruskal-Wallis test, witheach tooth (mean microtensile bond strength testing[MTBS] from the 11 beams) used as a single measure-ment, yielding 5 measurements per group. Statisticalsignificance was set in advance at the .05 level. Posthoc comparison was done using the Mann-WhitneyU test.
Scanning electron microscopy
The dentin and resin sides of 4 fractured beams (in-terfacial failure) from each group were air dried, sputtercoated with gold/palladium, and examined using ascanning electron microscope (SEM). Unused slabs (2from each group) were also prepared for the SEM anal-ysis of the intact dentin-resin interface. The sectionedsurface of each slab was etched for 30 seconds with35% phosphoric acid and replicated with a vinyl polysi-loxane material (Aquasil ULV; Dentsply Caulk,Milford, Del) for the fabrication of gold-coated resinspecimens.
513
THE JOURNAL OF PROSTHETIC DENTISTRY MAGNE ET AL
Table II. Mean microtensile bond strength values (MPa) and SDs of OptiBond FL
Group 55.06a 6.69 Group 11.58b 11.19 Group 58.25a 3.28
Values for each tooth obtained from 11 measurements (11 beams). Groups identified with different superscripts are significantly different (P,.05).
Fig. 2. Schematic representation of preparation of composite resin-dentin beams in ‘‘nontrimming’’ version of microtensile bondtest.
RESULTS
Microtensile bond strength
Table II lists the MTBS values of OptiBond FL todentin in the control (C) and experimental (DDS andIDS) groups. The mean MTBS varied from 12 to 58MPa. The Kruskal-Wallis test indicated a significantdifference among the 3 groups (P=.0081). The Mann-Whitney U test applied to the C and IDS groups didnot show a difference. The mean bond strength of theDDS group, 11.58 MPa, was significantly lower(P=.008) than that of the 2 other groups (55.06 and58.25 MPa for the C and IDS groups, respectively).The large variation within the DDS group (group withthe smallest mean and the largest standard deviation)is explained by the numerous failures at ‘‘near-0’’ loaddue the very low bond strength. Such failures did notoccur in the other groups. Results of the failure modesdetermined by optical microscopic evaluation are shownin Table III. Failures were either interfacial or cohesivein dentin for the C and IDS groups, whereas most ofthe failures in the DDS group were interfacial.Obvious cohesive failure in the restorative compositeoccurred only in 3 beams.
SEM observations
The fractured beams for both the C and IDS groupsdemonstrated interfacial failure that was typically mixed,with both areas of failed adhesive resin and areas of
514
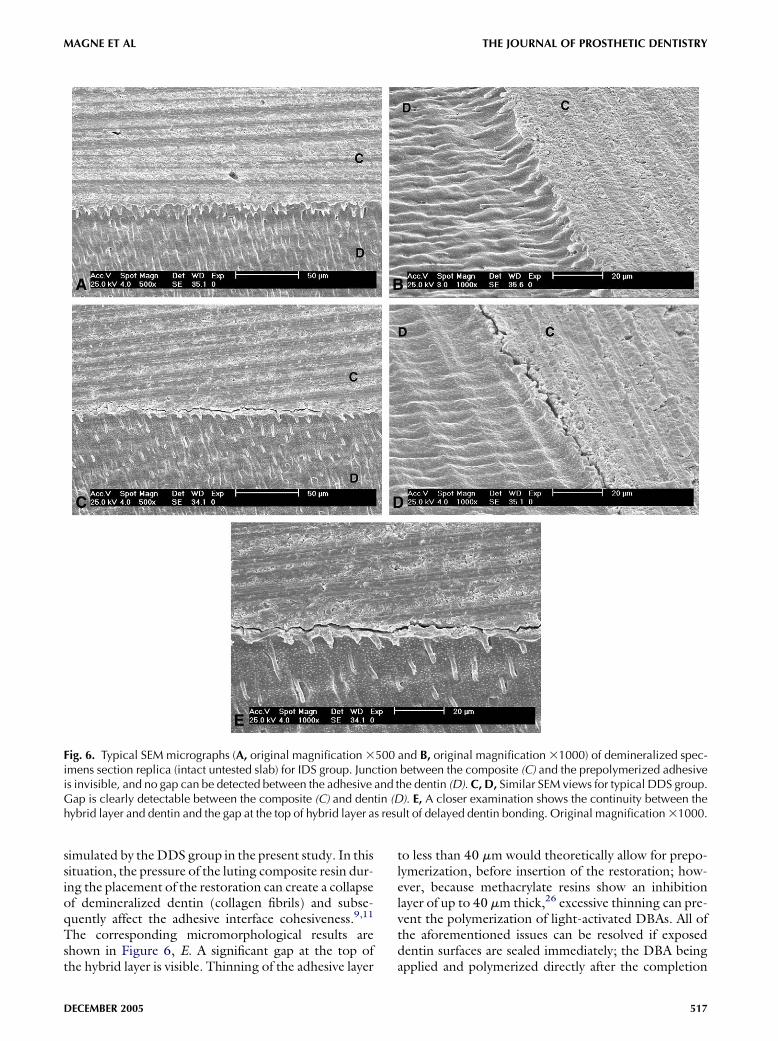
cohesively failed dentin (‘‘islands’’) showing numeroushybridized smear plugs and ‘‘torn’’ (irregular) intertu-bular dentin (Figs. 3 and 4). For DDS specimens, itwasmore difficult to determine the exact nature of inter-facial failure because of the similar nature of the filled ad-hesive and hybrid layer: Figure 5 suggests failure at thetop of the hybrid layer and in the adhesive, as therewere no exposed dentin tubules. The intact slabs forall groups generated a well-organized hybrid layer of3- to 5-mm thickness and resin tags. For the C andIDS groups, this ‘‘interdiffusion zone’’ was usually incontinuity with the dentin underneath (Fig. 6, A andB). For DDS specimens, gaps were frequently observedbetween the hybrid layers and systematically presented amarked disruption with the overlying composite resin(Fig. 6, C and E). In contrast, C and IDS specimensshowed rare discontinuities either in the dentin-resin in-terface or between the prepolymerized adhesive and theluting composite.
DISCUSSION
The results of the present study strongly favor imme-diate dentin sealing using OptiBond FL. Although earlybond strength of the adhesive was measured andno inference with respect to the durability of the bondcan be made, there are several rational motives andother practical and technical reasons confirming the val-idity of sealing dentin immediately, before makingimpressions.17
VOLUME 94 NUMBER 6
THE JOURNAL OF PROSTHETIC DENTISTRYMAGNE ET AL
First, freshly cut dentin is the ideal substrate for den-tin bonding.3,6,8 Significant reductions in bond strengthcan occur when simulating dentin contamination withvarious provisional cements compared to freshly cutdentin. In practice, freshly cut dentin is present only atthe time of tooth preparation, prior to impressionmaking.
Secondly, prepolymerization of the DBA results inimproved bond strength. In studies evaluating DBAbond strength, the infiltrating resin and adhesive layerare usually polymerized first (prepolymerization), priorto placing composite increments, which appears to gen-erate improved bond strength when compared to spec-imens in which DBA and the overlying composite arepolymerized together.4,9 These results can be explainedby the collapse of the unpolymerized dentin-resin hy-brid layer caused by pressure during composite resinor restoration placement,9,11 which correlate well withthe impaired bond strength and SEM observationsfor the DDS group in the present study. Prepolymeriz-ing the DBA is compatible with the direct application ofcomposite restorations; however, prepolymerizing theadhesive resin raises several issues when applied duringthe luting of indirect bonded restorations. PolymerizedDBA thicknesses can vary significantly according to sur-face geometry—on average, 60 to 80 mm on a smoothconvex surface and up to 200 to 300mmon concave sur-faces such as marginal chamfers.3,11 As a result, applyingand polymerizing the DBA immediately before the in-sertion of an indirect composite resin or porcelain resto-ration could interfere with the complete seating of therestoration. Practically speaking, it is therefore recom-mended that the adhesive resin be kept unpolymerizedbefore the restoration is fully seated, which was
Table III. Distribution of failure modes as observed byoptical microscopy
Failure mode Control group DDS group IDS group
Interfacial (%) 62 98 49
Dentin substrate (%) 34 2 49
Composite substrate (%) 4 0 2
Fig. 3. A, Typical SEM micrograph of composite side of frac-tured beam from control group, which failed at 47.1 MPa.Note mixed interfacial failure, mainly in dentin (D) and, inpart, in filled adhesive (A). Original magnification 380.B, Higher magnification of dentin-adhesive transition areaon composite side. Original magnification 32000. C, Corre-sponding view from tooth side suggests cohesive fracture indentin beneath hybrid layer (note blocked hybridized resinplugs and ragged collagen fibrils between). There is very tightrelationship between filled adhesive (A) and dentin (D). Orig-inal magnification 32000.
DECEMBER 2005
515
THE JOURNAL OF PROSTHETIC DENTISTRY MAGNE ET AL
Fig. 4. A, Typical SEM micrograph of fractured beam fromIDS group, which failed at 57.4 MPa. Note mixed interfacialfailure, mainly in dentin (D) and, in part, in filled adhesive(A). B, Higher magnification of dentin area on tooth sidealso suggests cohesive fracture in dentin beneath hybrid layerwith blocked hybridized resin plugs. Original magnification32000.
Fig. 5. A, Typical SEM micrograph of composite side of frac-tured beam from DDS group, which failed at 12.7 MPa. Noteadhesive failure with 2 distinct areas. Original magnification380. B, Higher magnification on composite side reveals fail-ure both in adhesive (A) and at top of hybrid layer (HL). Noteabsence of exposed dentin tubules. Original magnification32000. C, Corresponding view from tooth side suggestssame conclusions. Original magnification 32000.
516
VOLUME 94 NUMBER 6
THE JOURNAL OF PROSTHETIC DENTISTRYMAGNE ET AL
Fig. 6. Typical SEM micrographs (A, original magnification 3500 and B, original magnification 31000) of demineralized spec-imens section replica (intact untested slab) for IDS group. Junction between the composite (C) and the prepolymerized adhesiveis invisible, and no gap can be detected between the adhesive and the dentin (D). C, D, Similar SEM views for typical DDS group.Gap is clearly detectable between the composite (C) and dentin (D). E, A closer examination shows the continuity between thehybrid layer and dentin and the gap at the top of hybrid layer as result of delayed dentin bonding. Original magnification 31000.
simulated by theDDS group in the present study. In thissituation, the pressure of the luting composite resin dur-ing the placement of the restoration can create a collapseof demineralized dentin (collagen fibrils) and subse-quently affect the adhesive interface cohesiveness.9,11
The corresponding micromorphological results areshown in Figure 6, E. A significant gap at the top ofthe hybrid layer is visible. Thinning of the adhesive layer
DECEMBER 2005
to less than 40 mm would theoretically allow for prepo-lymerization, before insertion of the restoration; how-ever, because methacrylate resins show an inhibitionlayer of up to 40 mm thick,26 excessive thinning can pre-vent the polymerization of light-activated DBAs. All ofthe aforementioned issues can be resolved if exposeddentin surfaces are sealed immediately; the DBA beingapplied and polymerized directly after the completion
517
THE JOURNAL OF PROSTHETIC DENTISTRY MAGNE ET AL
of tooth preparations, before making the definitive im-pression, was confirmed to generate superior bondstrength13,14 and fewer gap formations.11,15 The result-ing interphase, simulated in the IDS group of thepresent study, could potentially better withstandlong-term exposure to thermal and functional loadscompared to the same adhesive being applied and poly-merized together with the restoration.
Thirdly, IDS allows stress-free dentin bond develop-ment. Dentin bond strength develops progressively overtime. In directly placed adhesive restorations, the weakerearly dentin bond is immediately challenged by the over-lying composite resin shrinkage and subsequent occlusalforces. However, when using IDS and indirect bondedrestorations, because of the delayed placement of therestoration (intrinsic to indirect techniques) and post-poned occlusal loading, the dentin bond can increaseover time and residual stresses can dissipate,27 resultingin significantly improved restoration adaptation as dem-onstrated by Dietschi et al.12
Finally, IDS protects dentin against bacterial leakageand sensitivity during the provisional phase of treat-ment. Based on the fact that provisional restorationsmay permit microleakage of bacteria and, subsequently,dentin sensitivity, Pashley et al3 proposed sealing dentinduring crown preparation. This idea proves even moreuseful when using bonded porcelain restorations, giventhe specific difficulty of obtaining sealed and stable pro-visional restorations. An in vivo study confirmed theability of different primers to prevent sensitivity andbacterial penetration when preparing for porcelainveneers.6
The potential exposure of the polymerized adhesiveto the oral fluids, permitting water sorption,28 couldcompromise the bond between the existing adhesiveand the new restoration. Considering the results of thepresent study (group IDS versus group C), placementof a provisional restoration for a period up to 2 weeksdid not seem to affect this bond, whichmay be explainedby remaining free radicals, van der Waals interactions(intermolecular forces), and micromechanical interlock-ing. As a matter of fact, just prior to restoration place-ment in the IDS group, the existing adhesive layer wasmeticulously cleansed by microairborne-particle abra-sion. Using pumice or roughening with a coarsediamond rotary cutting instrument at low speed canalso promote the bond to the sealed dentin.11,16,17
Clinically, the entire tooth preparation surface couldthen be considered and conditioned as it would be inthe absence of dentin exposure: H3PO4 etch (30 sec-onds), rinse, then dry and coat with adhesive resin. Atthis time, no prepolymerization of the adhesive is indi-cated because it would prevent the complete seating ofthe restoration. As demonstrated by the bond strengthresults and SEM analysis of the IDS group in the presentstudy, bonding to the existing adhesive was sufficient to
518
generate cohesive failures in dentin, and no gaps wereobserved between the prepolymerized adhesive andthe new restoration (Figs. 6, A and B). The success ofthis procedure might also be attributed to the dentinbonding system, especially the filled adhesive. OptiBondFL (Kerr) is particularly indicated for IDS because of itsability to form a consistent and uniform layer, as well asits cohesiveness with the final luting composite resin.11
Although there is a tendency to simplify bonding proce-dures, recent data confirm that conventional 3-stepetch-and-rinse adhesives still perform most favorablyand are most reliable in the long term.24,25 Especiallyfor posterior bonded restorations, OptiBond FL al-lows both dentin hybridization and the formation ofa low elastic modulus liner (stress absorber) with signif-icantly improved adaptation to dentin.12 There are nodata, however, suggesting that IDS cannot be appliedsuccessfully in conjunction with other adhesive systems.
Several practical and clinical facts support the use ofIDS. Patients experience improved comfort during theprovisional restoration stage, limited need for anesthesiaduring definitive insertion of the restorations, and re-duced postoperative sensitivity.3,6 When applying IDS,owing to the direct and immediate polymerizationmode, light-activated DBAs can be used. WithoutIDS, the use of dual-polymerizingDBAs to ensure com-plete polymerization through the restoration may be re-quired. As IDS is performed primarily on exposeddentin surfaces, the clinician can focus on the ‘‘wetbonding’’ to dentin (for total etching situations),whereas enamel conditioning can be performed sepa-rately at the stage of definitive restoration placement.
Caution must be applied during the provisional res-toration stage because sealed dentin surfaces have thepotential to bond to resin-based provisional materialsand cements. As a result, retrieval and removal of directprovisional restorations can be difficult. Tooth prepara-tions must be rigorously isolated with a separating me-dium, such as a thick layer of petroleum jelly, duringfabrication of the provisional restoration. Therefore, itis suggested the clinician consider fabricating provi-sional restorations indirectly, avoiding resin-based pro-visional cements and providing mechanical retentionand stabilization instead, such as locking the restorationon the tooth through addition of liquid resin in palatalembrasures. Splinting multiple restorations can also sig-nificantly enhance the primary stability of the provisionalrestoration. The results of the present study indicatedthat clinical trials using immediate dentin sealing shouldbe initiated.
CONCLUSIONS
Tooth preparation for indirect bonded restorationssuch as composite/ceramic inlays, onlays, and veneerscan generate significant dentin exposure. The results
VOLUME 94 NUMBER 6
THE JOURNAL OF PROSTHETIC DENTISTRYMAGNE ET AL
of this study indicate that to improve dentin bondstrength, these freshly cut dentin surfaces shouldbe sealed with a DBA immediately following toothpreparation, before making impressions. A 3-stepetch-and-rinse DBA with a filled adhesive resin is sug-gested for this specific purpose.
The authors thank Byoung Suh (President, Bisco Dental Products)
for providing the microtensile tester, Jenny Wang (Senior Research
Chemist, Bisco Dental Products) and Marie-Claude Bijon (Depart-
ment of Cariology, Endodontology and Pediatric Dentistry, School
of Dental Medicine, University of Geneva) for their assistance and
for SEM analysis, Tina Jaskoll (Professor Developmental Genetics,
School of Dentistry, University of Southern California) for assistance
with the optical microscope, and Charles Shuler (Associate Professor,
Associate Dean, Student Life & Academic Affairs, School of Dentis-
try, University of Southern California) for guidance with the statistical
analysis presented in this study.
REFERENCES
1. Dumfahrt H, Schaffer H. Porcelain laminate veneers. A retrospective eval-
uation after 1 to 10 years of service: part II—clinical results. Int J Prostho-
dont 2000;13:9-18.
2. Friedman MJ. A 15-year review of porcelain veneer failure—a clinician’s