IMMUCOTHEL ® – for recurrence prevention of superficial urinary bladder carcinomas Patients appreciate the well-tolerated alternative • practically no side effects • successful alternative to BCG • successful alternative to mitomycin • easy, no-cost disposal we are research
Transcript
IMMUCOTHEL® – for recurrence prevention of superficial urinary bladder carcinomas
Patients appreciate the well-tolerated alternative
• practically no side effects
• successful alternative to BCG
• successful alternative to mitomycin
• easy, no-cost disposal
we areresearch
Therapy scheme
The treatment is divided into pre-sensitization with IMMUCOTHEL® 1 mg and an instillation therapy with IMMUCOTHEL® 10 mg. Subsequent to the pre-sensitization and the weekly instillation therapy over six weeks, the aspired maintenance therapy should be performed once a month for the duration of one year:
IMMUCOTHEL® – therapy scheme for superficial urinary bladder carcinoma
The treatment starts with pre-sensitization with IMMUCOTHEL® 1 mg and continues with instillation therapy of IMMUCOTHEL® 10 mg
Pre-sensitization with IMMUCOTHEL® 1 mg
Start the therapy before TUR if possible, at the latest within six days after TUR
Apply 1 mg s.c. or i.c. in the forearm (positive skin reaction/DTH desired)
Instillation therapy with IMMUCOTHEL® 10 mg
Initial therapy
Start the instillation therapy: Instill 20 ml (2 × IMMUCOTHEL® 10 mg) in the bladder every week over 6 weeks
Maintenance therapy
20 ml (2 × IMMUCOTHEL® 10 mg) intravesically. Instillation every month over 12 months
You will find additional information on our homepages: www.biosyncorp.com, www.biosyn-partnernet.com, www.biosyn.de.Contact: [email protected]
IMMUCOTHEL® is approved for the prevention of recurrent superficial bladder carcinoma (Tis, Ta-T1 (G1-G3)) after transurethral resection as immunotherapy for recurrence prevention
IMMUCOTHEL® is reimbursable as a second-line therapy after standard therapy (yellow Box/RE2) in Austria
The standard therapy with a cytostatic agent or BCG might not be used for all pa-tients. Side effects, intolerances, or limited availability (BCG) often present limiting factors
IMMUCOTHEL® is available as a well-tolerated instillation therapy effective as an immunotherapy for recurrence prevention of superficial urinary bladder carci-nomas. Patients appreciate the advantage of the comparable effectiveness over chemo- or immunotherapy of BCG with significantly fewer side effects [1 – 3]
In contrast to cytostatic agents and BCG, IMMUCOTHEL® can be prepared in ready-to-use form without special personal or product protection
The substance can be disposed of along with normal medical practice waste and does not fall under the cytostatic agent/CMR substance ordinance; this is a logisti-cal advantage in daily medical practice routine
Additional information for KLH/IMMUCOTHEL®: www.biosynpharma.com, www.biosyn-partnernet.com, www.biosyn.de
1. Kälble T, Möhring K, Ikinger U, Riedasch G, Staehler G. Urologe A. 1991 Mar; 30(2): 118-21. [Intravesical prevention of recurrence of super cial urinary bladder cancer with BCG and KLH. A prospective randomized study].
2. Jurincic-Winkler C, Metz KA, Beuth J, Sippel J, Klippel KF. Anticancer Res. 1995 Nov-Dec; 15(6B): 2771-6. Effect of keyhole limpet hemocyanin (KLH) and bacillus Calmette-Guérin (BCG) instillation on carcinoma in situ of the urinary bladder.
3. Lamm DL. J Urol. Urogynäkol 2003; 10(2): 18–21. Laboratory and clinical experience with keyhole limpet hemocyanin (IMMUCOTHEL®) in super cial bladder cancer.
38 Probability of recurrence after sole transurethral resection (TUR)
40 IMMUCOTHEL® for recurrence prevention
44 IMMUCOTHEL® for recurrence prevention of primary tumors
46 IMMUCOTHEL® for recurrence prevention of recurrent tumors
48 IMMUCOTHEL® for recurrence prevention of carcinoma in situ
50 Approval of IMMUCOTHEL® for the following superficial bladder carcinomas
51 Comparison of the immunotherapies IMMUCOTHEL® vs. BCG
59 Comparison of IMMUCOTHEL® vs. Mitomycin C
65Overview: Comparison of recurrence prevention, progression and therapy failure rate of the various therapies
Additional information68 A look at other application areas
72 World-wide first GMP production process for immunocyanin
76 IMMUCOTHEL® products and required text
78 biosyn Arzneimittel GmbH
Contents5
General
Keyhole Limpet Hemocyanin (KLH)
• Isolated from the hemolymph of the sea snail Megathura crenulata
• Cylindrical, with copper-bearing blue protein
• One of the largest known proteins with 8,000 – 32,000 kDa
• Immunocyanin = active component of IMMUCOTHEL®
• KLH stimulates the immune system
• KLH has a direct cytotoxic effect
• Strong KLH immunogenicity is based on the attached oligosaccharides
IMMU COTHEL® General
• No mutagenic potential
• Systemically well tolerated
• No minimum lethal dose could be detected
• Non-toxic over a very large dose range
• Antibody production (IgM, IgG and IgA) against IMMUCOTHEL®
• Detection of antibodies in the mucosa and submucosa of the urinary bladder
• Induces a systemic immune response that also increases after longer treatment-free intervals
• Significantly increases the IgA production and thereby effectively protects the bladder mucosa. Remaining tumor cells can be destroyed
Composition6
• Optimal dose: 10 – 20 mg per instillation
IMMU COTHEL® Clinical
• Bell-shaped dosage response curve
• DTH (delayed-type hypersensitivity reaction) by means of KLH facilitates the immune competence test
• No clear correlation between a DTH and the clinical result
• Between 60 – 70 % of the patients show a positive skin test
• Pre-immunization reduces the probability of recurrence
• Anti-KLH antibodies are not detectable before therapy with IMMUCOTHEL®
• Significant increase of anti-KLH antibody concentration is associated with treatment outcome
Composition 7
IMMUCOTHEL®-treatment for superficial bladder carcinoma
• Probability of recurrence decreases from 70 % (TUR) to 30 %
• 26 % of the recurrences downgrade
• Only 15 % of the recurrences progress
• An IMMUCOTHEL® treatment is best tolerated by patients
Starting from the second recurrence:• The probability of recurrence is 44 %• 10 % of the recurrent tumors downgrade• 17 % of the recurrences progress
Carcinoma in situ (CIS):• The “long-term disease-free rate” for CIS is 49 %• Only 13 % of the recurrent CIS progress• Approval for IMMUCOTHEL® for primary and recurrent
multifocal Ta, singular T1G1 and T1G2 as well as CIS
Recurrence prevention for superficial bladder carcinoma
• TUR (transurethral resection)
• Despite complete removal of the tumor there is a high probability of recurrence after sole TUR (70 %)
Clinical applicationComposition8
• Frequent side effects with BCG therapy result in the discontinuation of BCG therapy treatment in 20 % of cases
BCG treatment for superficial bladder carcinoma
• Recurrence rate for an IMMUCOTHEL® treatment and BCG therapy is comparable
• Minor side effect spectrum for IMMUCOTHEL® vs. severe side effects for BCG
• BCG non-responsive tumors respond well to IMMUCOTHEL® treatment
• Comparable recurrence rate for IMMUCOTHEL® and Mitomycin C therapy
Mitomycin C treatment for superficial bladder carcinoma
• Lower probability of recurrence for recurrent tumors with IMMUCOTHEL® treatment
• Higher “5-year disease free” probability for IMMUCOTHEL® therapy
• Significantly lower progression rate for an IMMUCOTHEL® treatment
• Fewer therapy failures due to medication with an IMMUCOTHEL® treatment
Composition 9
The glycoprotein keyhole Limpet He-mocyanin (KLH) is obtained from the hemolymph of the Californian sea snail Megathura crenulata.
This active ingredient has high thera-peutic potential. Firstly, it lowers the recurrence rate of urinary bladder carci-nomas and is on the market in countries such as Netherlands, Austria, Argentina and South Korea.
Secondly, this high-molecular glycopro-tein acts as a carrier molecule for diverse antigens in new generations of vaccine.
The first success of such a vaccine was demonstrated in a phase III study of Biovest International Company (Worces-
ter, MA, a subsidiary company of Accentia Biopharmaceuticals, Inc., www.biovest.com) on patients with non-Hodgkin lymphoma. The group that was treated with vaccine containing KLH survived significantly longer.
The protein is obtained by the (non-let-hal) puncture of the sea snail in Califor-nia, it is pre-cleaned and subsequently highly purified by Arzneimittel GmbH in Fellbach. In the meantime the gene sequence could be determined and a patent registered. Therefore the genetic engineering manufacture of the recom-binant proteins is also imaginable in the future.
Ecological and innovative: the blue serum of the snailThe sea snails (Megathura crenulata) are up to 15 years old when they are brought on land from the cool sea by specia-lized divers off the Californian coast. The approval of the Californian Fishing Authority is a prerequisite for collecting these snails and acquiring their serum by puncturing.
About 500 keyhole snails per production process are our guests for two weeks at the biosyn Corporation in Carlsbad, California. They live in specialized pools (an expressly developed aquarium faci-lity) for cleaning on a diet, then serum is withdrawn from them after a cold nar-cosis over the iced foot with which they
adhere tightly to substrate and move forward. The missing quantity of liquid is refilled (with what is a company secret). After two weeks, the snails are returned undamaged to the sea.
The immunocyanin (IMMUCOTHEL®) obtained from one snail suffices to treat a patient with urinary bladder carcinoma for one year.
The blue color comes from copper atoms which bind the oxygen to the active cen-ter of the hemocyanin.
In the sea snail, hemocyanin is respon-sible for oxygen transport to the tissues.
Preventive care10
A sea snail delivers the active ingredient – a brief overview of the most important facts
Giant keyhole limpet, a snail from the family of keyhole snails (Megathura crenulata)
Recurrence prevention for superficial bladder carcinomaApprox. 28,750 people are diagnosed with bladder carcinoma every year in the Federal Republic of Germany. Bladder carcinomas occur in men 2.5 times more frequently than in women, whereby the risk increases with age (7th decade of life).
Urinary bladder carcinoma takes 4th pla-ce for tumor localization in males (after prostate, lung, colorectal carcinoma) [1].
Bladder carcinomas are discovered in patients on routine examinations or by blood in the urine and up to 95 % occur as superficial urothelium carcinoma. The standard procedure for a first therapeutic measure is transurethral resection (TUR)
of the malignant tumor of the urinary bladder, which often grows like a papil-loma. 75 – 85 % of bladder carcinomas show the postoperative stage pTa, pT1 or CIS.
Urothelium carcinomas of the urinary bladder frequently tend to return as re-current tumors with deterioration in stage and grading.
70 % of the T1 tumors of the urinary bladder are recurrent within three years after TUR. A therapeutic counteraction is the intravesical instillation of cytostatic or immunologically effective substances.
Significant extension of the recurrence-free intervalThe most frequent variant of KLH consists of 20 subunits that form two connected rings (didecamers) with a molecular weight of about 8 million Dalton.
The dissociated subunits of KLH form the immunocyanin with a molecular weight of about 400 KiloDalton. If one administers immunocyanin to patients, this results in the body's confrontation with hundreds of xenogenic epitopes of this molecule and triggers the activation
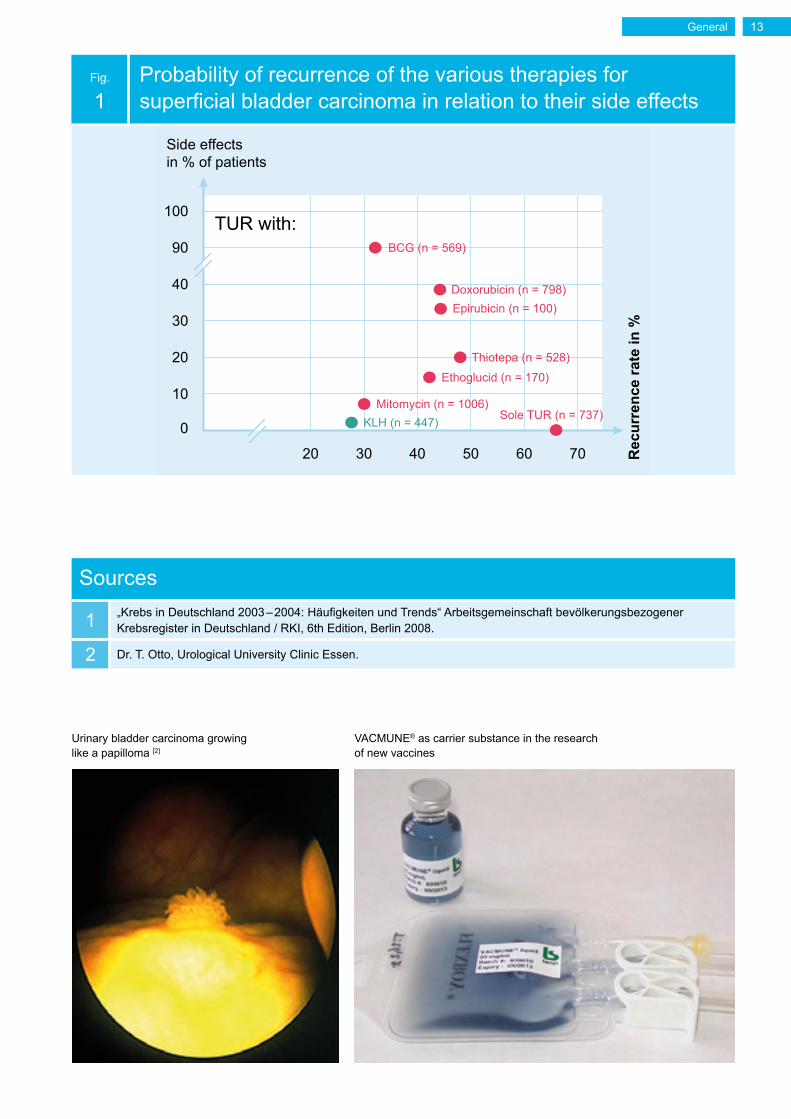
of the patient's immune system. The protein structures of the immunocyanins induce increased activation or syn-thetization of T-helper cells, cytotoxic T-suppressor cells, IFN-α, IFN-γ, IL-1a, and IL-2, macrophages and NK cells are stimulated. For patients with su-perficial urinary bladder carcinoma, the recurrence-free interval is significantly (≥ 100 %) extended by KLH (IMMUCO-THEL®) (Fig. 1).
Modern vaccine research: immunocyanin as carrier moleculeTherapeutic vaccines against the great scourges of humanity such as cancer or Morbus Alzheimer are currently the focus of worldwide pharmaceutical research. VACMUNE®, manufactured from im-munocyanin, serves as the carrier ma-
terial for modern vaccines and is thus continually being used in large-scale "big pharma" research projects. The research focusses on brain tumors, general tumors, high blood pressure, and Alzheimer's disease.
General12
Urinary bladder carcinoma growing like a papilloma [2]
Fig.
1Probability of recurrence of the various therapies for superficial bladder carcinoma in relation to their side effects
0
10
20
20 30 40 50 60 70 Rec
urre
nce
rate
in %30
40
90
100TUR with:
Side effects in % of patients
BCG (n = 569)
Doxorubicin (n = 798)Epirubicin (n = 100)
Thiotepa (n = 528)
Ethoglucid (n = 170)
Mitomycin (n = 1006)KLH (n = 447) Sole TUR (n = 737)
Sources
1 „Krebs in Deutschland 2003 – 2004: Häufigkeiten und Trends“ Arbeitsgemeinschaft bevölkerungs bezogener Krebsregister in Deutschland / RKI, 6th Edition, Berlin 2008.
2 Dr. T. Otto, Urological University Clinic Essen.
VACMUNE® as carrier substance in the research of new vaccines
General 13
General
• KLH = Keyhole Limpet Hemocyanin
• Isolated from the hemolymph sea snail Megathura crenulata
• Cylindrical, copper-bearing blue protein
• One of the largest proteins with 8,000 – 32,000 kDa
• Immunocyanin = active component of IMMUCOTHEL®
The active component of IMMUCO-THEL® consists of immunocyanin, a stable modification of the hemoglo-bin hemocyanin (Keyhole Limpet He-mocyanin = KLH), which is isolated from the hemolymph sea limpet Megathura crenulata. The native KLH is a cylindri-cal, copper-bearing blue protein. With a molecular weight of 8,000 – 32,000 kDa, KLH is basically one of the largest exis-ting proteins. In the limpet, this molecule has the function of transporting oxygen to the tissues.
The electronic microscopic image of KLH shows two different aggregation types: didecamers with a molecular weight of 8,000 kDa, and multidecamers with a molecular weight of 12,000 – 32,000 kDa.
The blue color of the hemolymph is caused by 2 copper atoms in the active center of KLH, which is responsible for oxygen transport. The smallest KLH unit is the functional domain (50 kDa), which contains an active center [1, 2].
Eight functional domains form a KLH subunit (400 kDa), which exists in two different forms: KLH 1 and KLH 2 [1]. These two subunits differ both bio- chemically as well as immunologically. Ten KLH subunits form a decamer (4,000 kDa), the basic unit is the dicamer and the multicamer (Fig. 1).
Structure of KLHor active component of IMMUCOTHEL®
Sources
1 Gerbauer W et al. Quaternary structure, subunits and domain patterns of two discrete forms of keyhole limpet hemocyanin: KLH1 and KLH2. Zool 98: 51–68; 1994.
2Söhngen SM, Stahlmann A, Harris JR, Müller SA, Engel A, Markl J. Mass determination, sub-unit organization and control of oligomerization states of keyhole limpet hemocyanin (KLH). Eur J Biochem. 1997 Sep 1; 248(2): 602–614.
3Harris JR, Gebauer W, Söhngen SM, Nermut MV, Markl J. Keyhole limpet hemocyanin (KLH), II: Characteristic reassociation properties of purified KLH1 and KLH2. Micron. 1997 Feb; 28(1): 43–56.
4 Markl J. Evolution of molluscan hemocyanin structures. Biochim Biophys Acta. 2013 Sep; 1834(9): 1840–1852.
5 Dissertation „Strukturelle, enzymkinetische und thermodynamische Untersuchungen am KLH, dem Hämocyanin der Schlüssellochschnecke Megathura crenulata“ Dr. Kay Büchler (2008)
6 Dissertation „3D-Strukturanalyse von Mollusken-Hämocyaninen aus elektronenmikroskopi-schen Bildern“ Dr. Christos Gatsogiannis (2009)
7 Markl J. Blaues Blut – Struktur, Funktion und Evolution der Hämocyanine. Chemie in unserer zeit 1996, 30: 6–18.
As an active ingredient, IMMUCOTHEL® contains immunocyanin, a mixture of the subunits KLH 1 and KLH 2 in a stable modification.
Here the native structure of the subunits is completely preserved.
Both dicamer and multidecamer KLH forms can be rebuilt again in vitro from IMMUCOTHEL® [3] (Fig. 2).
Fig.
2 Composition of the immunocyanin [4, 5, 7]
In vivoIn vitro
MultidecamereDidecamere
Immunocyanin
KLH 1 CN a b c d e f g h
CKLH 2 N a b c d e f g
General16
Mechanism of action
• KLH stimulates the immune system
General• KLH has a direct cytotoxic effect
• Strong KLH immunogenicity is based on the attached oligosaccharides
The exact mechanism of action of KLH is not yet known. KLH itself shows modera-te anti-carcinogenic activity [1]. However, the effect of KLH on superficial bladder
carcinomas is based on its capability of stimulating the immune system [2] (Fig. 1).
Fig.
1The treatment of dendritic cells (DC) with KLH induces the expression of the cytokines IL-10 and IL-12
IL-12
p = 0.003
IL-10
500 100 150 200 250 300pg/ml
1,0000 2,000 3,000 4,000 5,000
p < 0.001
Treated DCsUntreated DCs
General 17
The strong immunogenicity of KLH is probably based on the numerous at-tached oligosaccharides that account for about 4 % of the molecular mass of KLH [3] (Fig. 2). Different mechanisms of action play a role here: on the one hand a non-specific stimulation of the immune system [4], and on the other hand the stimulation of cytotoxic T-cells. The third mechanism of action is the induc-tion of antitumoral antibodies. After an immunization with KLH, mice produced antibodies that bind tumor-associated oligosaccharide antigens [5]. In addition, studies with bladder carcinoma patients
showed an increase of anti-KLH antibo-dies in patients who responded to KLH treatment [6].
An additional study showed that KLH expressed Gal(beta 1-3) GalNAc-bearing oligosaccharides. The immunization of rats with KLH induces the production of anti-Gal(beta 1-3)Gal-NAc antibo-dies. Since bladder carcinomas express cross-reactive Gal(beta 1-3)GalNAc epi-topes (also called Thomsen-Friedenreich antigens), the effectiveness of immuno-therapy with KLH for superficial bladder carcinoma is most likely based on this fact [7].
1McFadden DW, Riggs DR, Jackson BJ, Vona-Davis L. Keyhole limpet hemocyanin, a novel immune stimulant with promising anticancer activity in Barrett’s esophageal adenocarcinoma. Am J Surg. 2003 Nov; 186(5): 552–555.
2Presicce P, Taddeo A, Conti A, Villa ML, Della Bella S. Keyhole limpet hemocyanin induces the activation and maturation of human dendritic cells through the involvement of mannose receptor. Mol Immunol. 2008 Feb; 45(4): 1136–1145.
3Kurokawa T, Wuhrer M, Lochnit G, Geyer H, Markl J, Geyer R. Hemocyanin from the key-hole limpet Megathura crenulata (KLH) carries a novel type of N-glycans with Gal(beta1-6)Man-motifs. Eur J Biochem. 2002 Nov; 269(22): 5459–5473.
4 Tzianabos AO. Polysaccharide immunomodulators as therapeutic agents: structural aspects and biologic function. Clin Microbiol Rev. 2000 Oct; 13(4): 523–533.
5May RJ, Beenhouwer DO, Scharff MD. Antibodies to keyhole limpet hemocyanin cross-react with an epitope on the polysaccharide capsule of Cryptococcus neoformans and other carbo-hydrates: implications for vaccine development. J Immunol. 2003 Nov 1; 171(9): 4905–4912.
6Jurincic-Winkler CD, von der Kammer H, Beuth J, Scheit KH, Klippel KF. Antibody response to keyhole limpet hemocyanin (KLH) treatment in patients with superficial bladder carcinoma. Anticancer Res. 1996 Jul-Aug; 16(4A): 2105–2110.
7Wirguin I, Suturkova-Milosević L, Briani C, Latov N. Keyhole limpet hemocyanin contains Gal(beta 1-3)-GalNAc determinants that are cross-reactive with the T antigen. Cancer Immu-nol Immunother. 1995 May; 40(5): 307–310.
8Gatsogiannis C, Markl J. Keyhole limpet hemocyanin: 9-A CryoEM structure and molecular model of the KLH1 didecamer reveal the interfaces and intricate topology of the 160 functional units. J Mol Biol. 2009 Jan 23; 385(3): 963–983.
• IMMUCOTHEL® is non-toxic over a very large dosing range
The acute and chronic toxicity was tested on various animal species (mouse, rat, rabbit). To check the acute toxicity, the laboratory animals were subcutaneously administered one dose of up to 2,000 mg/kg IMMUCOTHEL®. For rabbit and rats, inflammatory reactions were found at the injection spots. Mice showed an increased production of monocytes and granulocytes. The one-time high admi-nistration of IMMUCOTHEL® caused bone marrow changes and an enlarge-ment of the thymus [1]. In addition, the acute toxicity of IMMUCOTHEL® with an intravesical instillation in rats and rabbit was tested. No histopathological
changes could be determined for a dose range of 0.0025 – 50 mg with and without pre-immunization [2].
The chronic toxicity of IMMUCOTHEL® was examined in rats by means of repeated administration of up to 5 mg/kg, which resulted in an inflammation of the injection point and reversible minor bone marrow changes [3] (Fig. 1 and 2). An inspection of reproduction toxicity in cattle showed no difference between ani-mals treated and untreated with IMMU-COTHEL® with respect to ovulation and pregnancy rate [4].
2Rübben H, Hofstädter F, Küpper W, et al. III. Bericht zum Forschungsvorhaben. Wirkung von Keyhole-Limpet-Haemocyanin (KLH) auf die normale Blasenschleimhaut und chemisch indu-zierte Tumoren. Manuskript (1988).
1Pathological findings for male rats after repeated administration of IMMUCOTHEL® [3]
100%
Inje
ctio
n po
int
phle
gmat
icin
flam
mat
ions
Inje
ctio
n po
int
absc
ess-
form
ing
infla
mm
atio
ns
Per
iphe
ral
fatty
live
r
Incr
ease
dfo
rmat
ion
of m
onoc
ycte
s(b
one
mar
row
)
Incr
ease
d fo
rmat
ion
of e
ryth
rocy
tes
and
gra
nulo
cyte
s (s
plee
n)
5060708090
403020100
Control 0.05 mg/kg 0.5 mg/kg 5 mg/kg
Fig.
2Pathological findings for female rats after repeated administration of IMMUCOTHEL® [3]
100%
Inje
ctio
n po
int
phle
gmat
icin
flam
mat
ions
Inje
ctio
n po
int
absc
ess-
form
ing
infla
mm
atio
ns
Per
iphe
ral
fatty
live
r
Incr
ease
dfo
rmat
ion
of m
onoc
ycte
s(b
one
mar
row
)
Incr
ease
d fo
rmat
ion
of e
ryth
rocy
tes
and
gra
nulo
cyte
s (s
plee
n)
5060708090
403020100
Control 0.05 mg/kg 0.5 mg/kg 5 mg/kg
General 21
Humoral and cellular immune response
General
• Production of antibodies (IgM, IgG and IgA) against IMMUCOTHEL®
• Detection of antibodies against IMMUCOTHEL® in the mucosa and submucosa of the urinary bladder
• IMMUCOTHEL® induces a systemic immune response that also increases after longer treatment-free intervals
• IMMUCOTHEL® significantly increases the IgA production and thereby effectively protects the bladder mucosa. Remaining tumor cells can be destroyed
General22
Fig.
1Simplified representation of the immune response with a KLH treatment
Macrophage
Antigen presentation
Lysis of the tumor cell
Lysis of the tumor cell
Anti-KLH antibody
production
Antigen-antibodyreaction
Activation of T-cells
Cytotoxic T-cell
1. IgM
2. IgA
3. IgG
Phagocytosis and dissolution ofthe tumor cell
Activation of B-cells
+ Cytokines
Activity of natural killer cells
Phagocytosis Phagocytosisand dissolutionof the tumor cell
IMMUCOTHEL®
U
U
In humans, KLH triggers a strong immune reactionThanks to its size and the large number of oligosaccharides, KLH is a strong an-tigen. When an immune system comes into contact with KLH for the first time, the macrophages are activated. They immediately act directly against tumor cells. Secondly, macrophages increase
the activity of natural killer cells and gra-nulocytes by means of cytokines. Thirdly, macrophages present the antigen with T- and B-lymphocytes for information transfer and at the same time stimulate them by means of cytokines (Fig. 1).
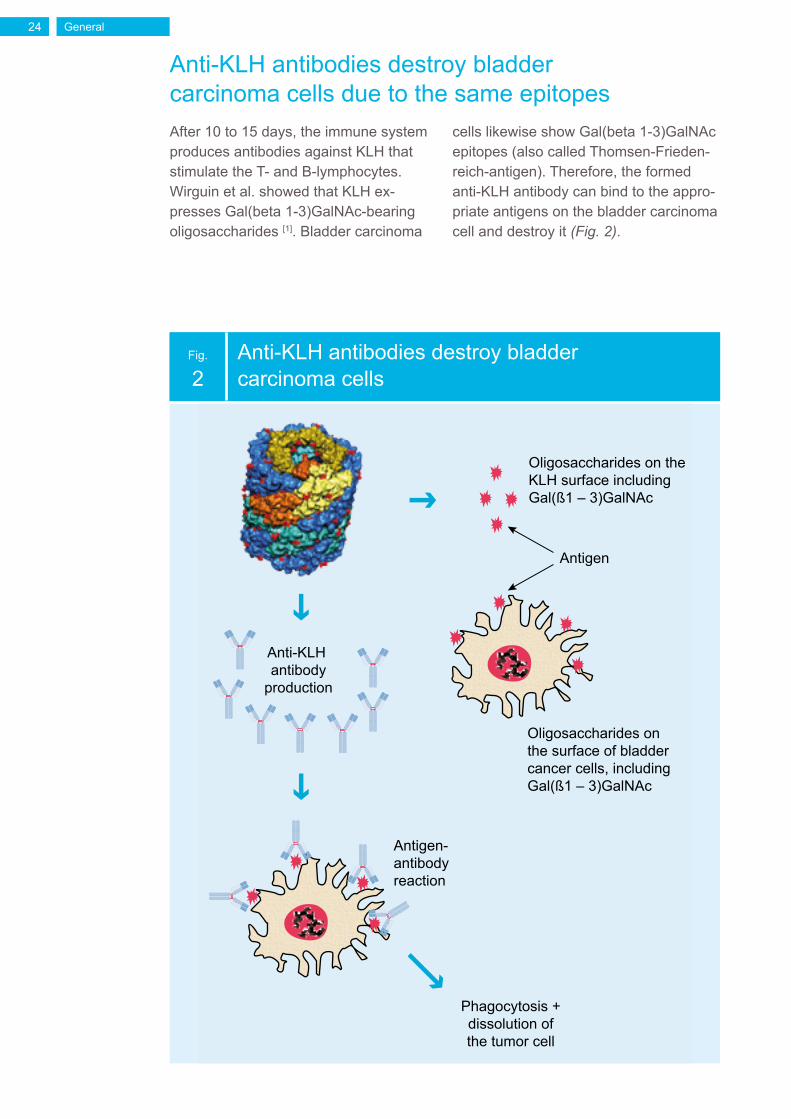
Oligosaccharides on the surface of bladder cancer cells, includingGal(ß1 – 3)GalNAc
Antigen
Anti-KLH antibody
production
Antigen-antibody reaction
Oligosaccharides on the KLH surface including Gal(ß1 – 3)GalNAc
Anti-KLH antibodies destroy bladder carcinoma cells due to the same epitopesAfter 10 to 15 days, the immune system produces antibodies against KLH that stimulate the T- and B-lymphocytes. Wirguin et al. showed that KLH ex-presses Gal(beta 1-3)GalNAc-bearing oligosaccharides [1]. Bladder carcinoma
cells likewise show Gal(beta 1-3)GalNAc epitopes (also called Thomsen-Frieden-reich-antigen). Therefore, the formed anti-KLH antibody can bind to the appro-priate antigens on the bladder carcinoma cell and destroy it (Fig. 2).
General24
Anti-KLH antibody formation in the mucosa and submucosa of the urinary bladderImmunohistochemical examinations of urinary bladder biopsies detected an-ti-KLH antibodies in the mucosa and submucosa after an IMMUCOTHEL® tre-atment (Fig. 3). Anti-KLH antibodies were
increased both in patients with additional intracutaneous immunization as well as exclusively intravesical immunization [2].
Fig.
3Anti-KLH antibody in the mucosa and submucosa [2]
a) CD8-positive cells in the tumor tissue and in the submucosa before KLH therapy.
b) CD8-positive cells in the Lamina propria before KLH therapy.c) An increase of the number of CD8-positive cells (c1) and CD4-positive cells (c2)
after a 6-week IMMUCOTHEL® treatment. 200x magnification
General 25
In humans, KLH triggers a systemic immune responseA sub- and intracutaneous administrati-on of KLH triggers a systemic immune response with KLH-specific IgM- and IgG-antibodies, as a study by Peters and Fauci already showed in 1983 [3]. After an immunization with 5 mg KLH, the hig-
hest titer of anti-KLH IgM was detected after two weeks, which declined in the following months. No anti-KLH IgM was traceable after 3 and 6 months. However, anti-KLH IgG were only detectable after 3 months.
IMMUCOTHEL® induces a systemic immune response that also increases after longer treatment-free intervals In a study from 2004, the immunological response to an intravesical treatment with IMMUCOTHEL® (KLH) for superfici-al bladder carcinoma was investigated [4]. Different immunological parameters were repeatedly measured. The first measu-rement took place before the immuniza-tion (day 14), the second measurement before the first intravesical treatment (day 1), the third measurement during the 6-times-a-week intravesical treatment (day 36), and the fourth and fifth mea-surement during the treatment after the third and twelfth months respectively.
The most common immunoglobulin, immunoglobulin G (IgG), is produced at a primary infection only after about three weeks. As anticipated, a signifi-cant increase of IgGs against KLH for the measurement on day 36 could be detected. Anti-KLH IgGs also elevated significantly further after three and twelve months (Fig. 4). This demonstrates that a systemic immune response is also present or is still increasing after longer treatment-free intervals.
IMMUCOTHEL® protects the bladder mucosa and remaining tumor cells can be destroyed Apart from the blood plasma, immuno-globulin A (IgA) is specifically secreted from mucous membranes and forms an important defense barrier against patho-gens. The IgA concentration against KLH in the blood plasma significantly increa-ses during the weekly intravesical treat-ment with IMMUCOTHEL® and declines after prolonging the treatment-free intervals, but continues to remain sig-
nificantly higher than the original value (Fig. 5). These results demonstrate that IMMUCOTHEL® effectively protects the healthy parts of the bladder mucosa by increased IgA production during the enti-re treatment time period and can destroy remaining tumor cells.
General26
Fig.
4IgG concentration in the course of a one-year IMMUCOTHEL® treatment [4]
Day -14 Day -1 Day 36 Month 3 Month 12
3.0
Ant
i KLH
IgG
(10l
og A
.U./l
)
4.0
3.5
4.5
5.5
5.0
6.0
p = 0.001
p = 0.001 p = 0.03
Fig.
5IgA concentration in the course of a one-year IMMUCOTHEL® treatment [4]
0
Ant
i KLH
IgA
(A.U
./l)
Day -14 Day -1 Day 36 Month 3 Month 12
1,000
500
1,500
3,000
2,500
2,000
4,000
3,500
p = 0.001
p = 0.001p = 0.002
General 27
Sources
1Wirguin I, Suturkova-Milosević L, Briani C, Latov N. Keyhole limpet hemocyanin contains Gal(beta 1-3)-GalNAc determinants that are cross-reactive with the T antigen. Cancer Immu-nol Immunother. 1995 May; 40(5): 307–310.
2Jurincic CD, Stöcker W, Klippel KF, et al. Immunhistochemische Untersuchung von Harnbla-senbiopsien nach Immunotherapie des oberflächlichen Blasenkarzinoms mit Keyhole Limpet Haemocyanin (KLH). In: Stiefel T., Porcher H., (eds.) IMMUCOTHELWorkshop II. Avignon, 25.–27. November 1988; Walter Druck GmbH Stuttgart (1989), 45–55.
3Peters M, Fauci AS. Selective activation of antigen-specific human B cells in recently im-munized individuals by nonspecific factors in the absence of antigen. J Immunol. 1983 Feb;130(2): 678–680.
4Kurth KH, De Boer EC, De Reijke TM, 2004 Amsterdam, Immunological response following intravesical treatment with Immucothel (KLH) for superficial bladder carcinoma. Persönliche Mitteilung.
Concentration profile of various immunoglobulins during an IMMUCOTHEL® treatmentFigure 6 shows an overview of the concentration profile of immunoglobu-
lins IgG, IgM and IgA during a one-year IMMUCOTHEL® treatment.
Fig.
6Activation of the immunoglobulin in the course of a one-year IMMUCOTHEL® treatment [4]
1 Lamm DL. J Urol. Urogynäkol 2003; 10 (2): 18-21. Laboratory and clinical experience with keyhole limpet hemocyanin (Immucothel®) in superficial bladder cancer.
Dose-response relationship
• Optimal dose: 10 – 20 mg per instillationGeneral
• Bell-shaped dose-response curve for IMMUCOTHEL®
For immunologically effective substances like IMMUCOTHEL® and BCG, there is no linear dose-response relationship, but a comparable effect can be achieved over a certain dosing range. The admi-nistration scheme for IMMUCOTHEL® was therefore empirically adopted from BCG.
In a phase I/II clinical study, a dose escalation was evaluated with KLH for patients with residual papillary urinary bladder carcinoma and in situ carcinoma.
Two weeks before the intravesical instil-lation, all patients received percutaneous treatment of 1 mg KLH and subsequently intravesical treatment with 0.4, 2, 10 and 50 mg KLH. For all doses, this resulted in complete remissions. In addition, there was no significant difference in the com-plete remission rate in the high dosage range. The complete remission rate for IMMUCOTHEL® in the range from 2 – 10 MG was highest with 42 %, while the remission rate was stable at 30 % for BCG at 2 – 50 mg.
General 29
DTH (delayed-type hypersensitivity reaction)
General• DTH by means of KLH is used to test the immune competence
• No clear correlation between a DTH and the clinical result
• Between 60 – 70 % of the patients show a positive skin test
A DTH (delayed-type hypersensitivity reaction) is a hypersensitivity reaction at the injection point that only manifests 48 – 72 hours after contact with the anti-gen and which is mediated by T-cells or macrophages (Fig. 1). This reaction is an important defense mechanism against diverse intracellular pathogens, and additionally occurs in the event of tumor immunity.
The immune response against intracellu-lar pathogens is strongly impaired by the loss of CD4+T cells. Therefore the im-mune competence has been determined with the help of KLH for decades.
The relationship between a DTH and the clinical result is notclear. In 1974, Olsen et al. determined that after a positive DTH, bladder carcinoma patients sho-wed significantly lower recurrence rates when tested for immune competence [1]. Also Jurincic-Winkler et al. demonstrated a positive correlation between a positi-ve DTH and a lower recurrence rate [2]. However, the results of Lammers et al. were inconsistent. While a positive skin test appeared to be a prognostic factor for recurrence in the phase III study, at the same time a negative skin test was associated with progression [3].
Sources
1 Olsson CA, Chute R, Rao CN. J Urol. 1974 Feb; 111(2): 173-6. Immunologic reduction of bladder cancer recurrence rate.
2Jurincic-Winkler C, Metz KA, Beuth J, Sippel J, Klippel KF. Anticancer Res. 1995 Nov-Dec; 15(6B): 2771-6. Effect of keyhole limpet hemocyanin (KLH) and bacillus Calmette-Guérin (BCG) instillation on carcinoma in situ of the urinary bladder.
3Lammers RJ, Witjes WP, Janzing-Pastors MH, Caris CT, Witjes JA. J Clin Oncol. 2012 Jun 20; 30(18): 2273-9. Intracutaneous and intravesical immunotherapy with keyhole limpet hemocyanin compared with intravesical mitomycin in patients with non-muscle-invasive blad-der cancer: results from a prospective randomized phase III trial.
1Simplified process of a DTH (delayed-type hypersensitivity reaction)
Subcutaneous administration of the antigen KLH leads
to KLH being processed by the local antigen
presenting cells in the surrounding tissue
24 hours 48 hours 72 hours
T-helper cells (TH1) recognize the antigen and release cytokines, which trigger a reaction
in blood vessels
Increased amount of T-cells, phagocytes,
liquid and proteins at the site of the
antigen KLH injection induces visible skin
changes
KLH
TH1 Bloodvessel
Cytokines
Clinical application 31
Pre-immunization
General • Pre-immunization reduces the probability of recurrence
In animal experiments, numerous studies demonstrated the necessity of a pre-im-munization in order for IMMUCOTHEL® to develop its full effectiveness.
Swerdlow et al. found significantly fewer tumors in a bladder carcinoma mouse model after pre-immunization with KLH compared to mice without a pre-immu-nization [1]. Also in an animal experiment
study by Lamm et al., pre-immuniza-tion with IMMUCOTHEL® reduced the tumor incidence and tumor volume (p < 0.001) [2]. At the same time, pre-im-munization significantly increased the survival probability to 75 % (p < 0.0001) (Table 1).
Sources
1Swerdlow RD, Ratliff TL, La Regina M, Ritchey JK, Ebert RF. Immunotherapy with keyhole limpet hemocyanin: efficacy and safety in the MB-49 intravesical murine bladder tumor model. J Urol. 1994 Jun; 151(w6): 1718–1722.
2 Lamm DL, Dehaven JI, Riggs DR. Keyhole limpet hemocyanin immunotherapy of bladder cancer: laboratory and clinical studies. Eur Urol. 2000; 37 Suppl 3: 41–44.
Tab.
1Pre-immunization increases the efficiency of IMMUCOTHEL®
• Anti-KLH antibodies are not detectable prior to therapy with IMMUCOTHEL®
• Significant increase of the anti-KLH antibody concentration is associated with treatment outcome
Exact determination of the anti-KLH antibody titers using quantitative human anti-KLH-ELISA assaysAs already described in detail, IMMU-COTHEL® induces a systemic immune response.
With the help of a new quantitative human anti-KLH ELISA assay, a study in 2012 showed the exact concentrati-on profile of the various immunoglobu-lins after an immunization with KLH [1]. Older studies demonstrated that the IgM concentration increases with the initial immunization, and then subsequently the KLH-specific IgGs.
In the treatment-free interval interval, the IgG titer significantly declines. Howe-ver the drop in the IgG- and IgA concen-tration reduces after every immunization and results in a sustained anti-KLH titer (Fig. 1).
This study furthermore was able to show that KLH was not detectable in any of the 35 investigated patients before treatment (Fig. 2).
Clinical application34
Fig.
1Evolution of anti-KLH antibody concentration after multiple immunization with KLH [1]
1,200
800
1,000
600
400
200
0
300
200
250
150
100
50
0200
KLH
IgG
(mg/
l)
KLH
IgA and IgM
(mg/l)
0 400 600
Time in days800
ImmunizationIgG IgA IgM
Fig.
2Anti-KLH antibody concentration before and after a KLH treatment (n = 35) [1]
Ant
i-KLH
ant
ibod
y (m
g/l) 1,000
100
10
1Before
KLH treatment
n.d.n.d. n.d.
AfterKLH treatment
IgG
IgA
IgM
Clinical application 35
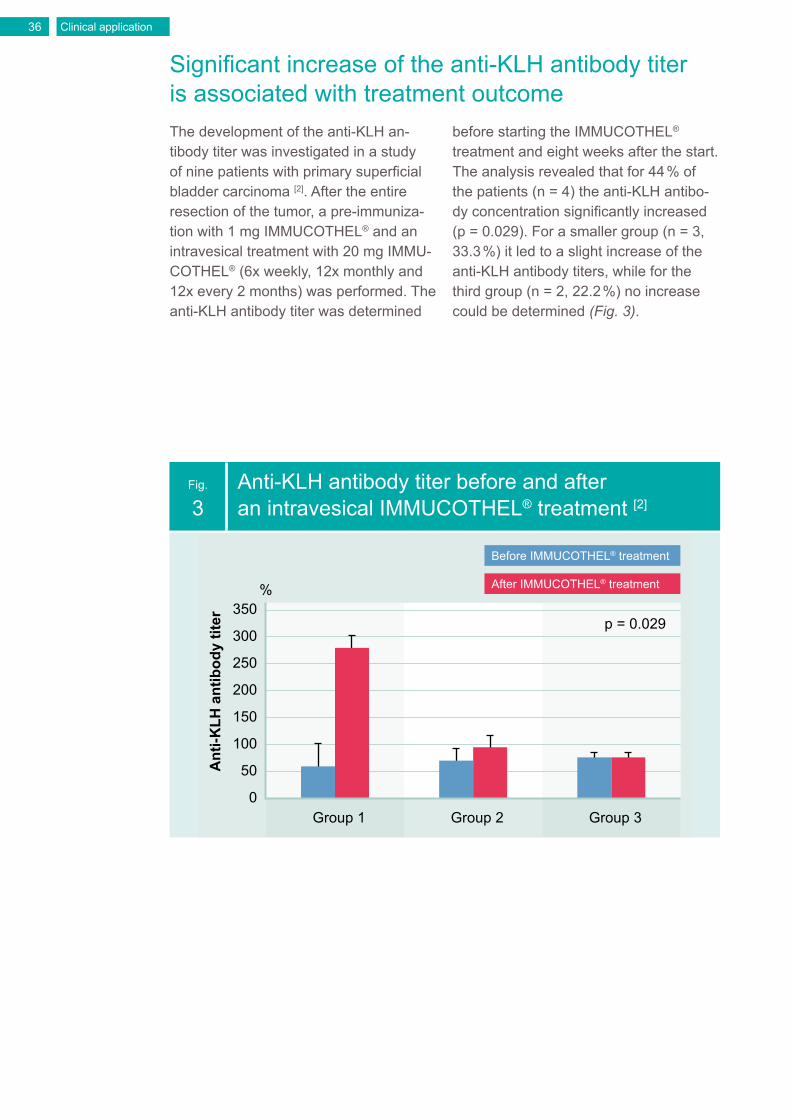
Significant increase of the anti-KLH antibody titer is associated with treatment outcomeThe development of the anti-KLH an-tibody titer was investigated in a study of nine patients with primary superficial bladder carcinoma [2]. After the entire resection of the tumor, a pre-immuniza-tion with 1 mg IMMUCOTHEL® and an intravesical treatment with 20 mg IMMU-COTHEL® (6x weekly, 12x monthly and 12x every 2 months) was performed. The anti-KLH antibody titer was determined
before starting the IMMUCOTHEL® treatment and eight weeks after the start. The analysis revealed that for 44 % of the patients (n = 4) the anti-KLH antibo-dy concentration significantly increased (p = 0.029). For a smaller group (n = 3, 33.3 %) it led to a slight increase of the anti-KLH antibody titers, while for the third group (n = 2, 22.2 %) no increase could be determined (Fig. 3).
Fig.
3Anti-KLH antibody titer before and after an intravesical IMMUCOTHEL® treatment [2]
350%
Group 1
p = 0.029
Ant
i-KLH
ant
ibod
y tit
er
Group 2 Group 3
250
300
200
150
100
50
0
Before IMMUCOTHEL® treatment
After IMMUCOTHEL® treatment
Clinical application36
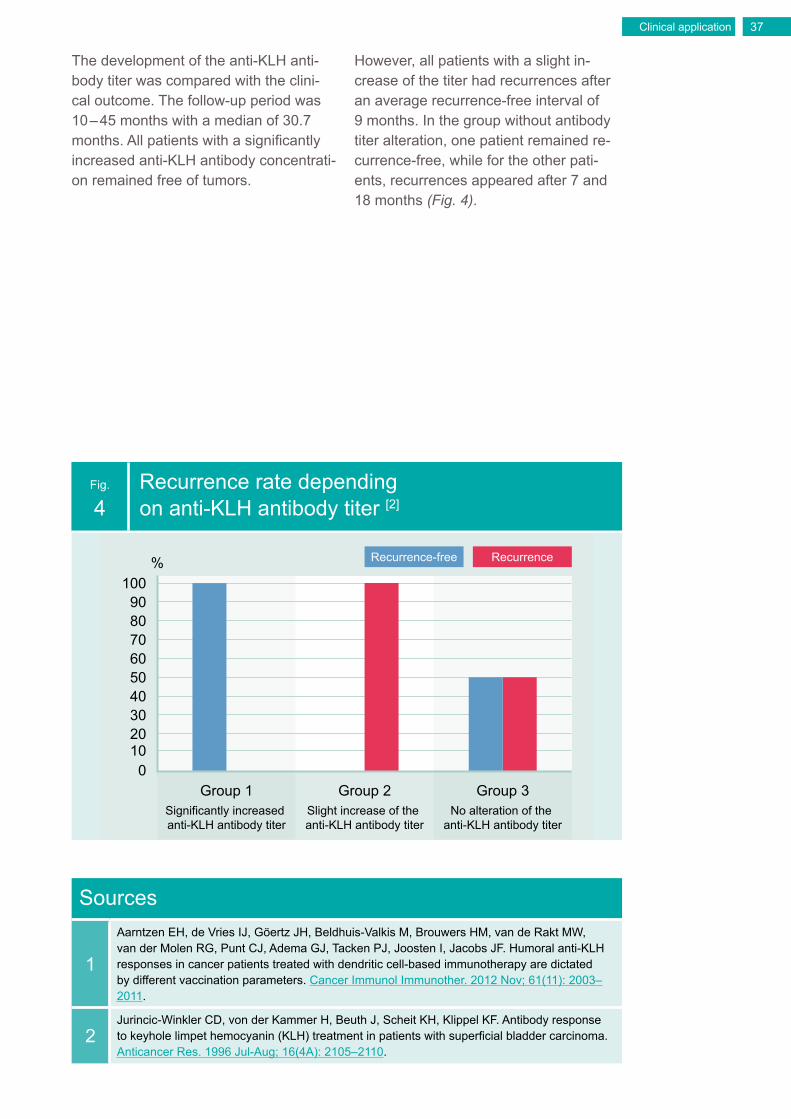
The development of the anti-KLH anti-body titer was compared with the clini-cal outcome. The follow-up period was 10 – 45 months with a median of 30.7 months. All patients with a significantly increased anti-KLH antibody concentrati-on remained free of tumors.
However, all patients with a slight in-crease of the titer had recurrences after an average recurrence-free interval of 9 months. In the group without antibody titer alteration, one patient remained re-currence-free, while for the other pati-ents, recurrences appeared after 7 and 18 months (Fig. 4).
Fig.
4Recurrence rate depending on anti-KLH antibody titer [2]
100%
Group 1 Group 2 Group 3
5060
40
8090
70
3020100
Recurrence-free Recurrence
Significantly increased anti-KLH antibody titer
Slight increase of the anti-KLH antibody titer
No alteration of the anti-KLH antibody titer
Sources
1
Aarntzen EH, de Vries IJ, Göertz JH, Beldhuis-Valkis M, Brouwers HM, van de Rakt MW, van der Molen RG, Punt CJ, Adema GJ, Tacken PJ, Joosten I, Jacobs JF. Humoral anti-KLH responses in cancer patients treated with dendritic cell-based immunotherapy are dictated by different vaccination parameters. Cancer Immunol Immunother. 2012 Nov; 61(11): 2003–2011.
2Jurincic-Winkler CD, von der Kammer H, Beuth J, Scheit KH, Klippel KF. Antibody response to keyhole limpet hemocyanin (KLH) treatment in patients with superficial bladder carcinoma. Anticancer Res. 1996 Jul-Aug; 16(4A): 2105–2110.
1Prognosis for superficial urinary bladder carcinomas [1]
Stage N Progression Survival rate after 5 years
pTa G1-2 1685 4.1 % 96 %
pT1 G1-2 596 18.8 % 81 %
pT1 G3-4 437 31.4 % 64 %
Sources
1 Rübben H, Otto T. In: Rübben H (publisher): Uroonkologie. 6. complete edition Berlin/Heidel-berg/New York, Springer Verlag 2014; 415–502. Harnblasenkarzinome.
The initial therapy form for all urinary bladder tumors is transurethral resection (TUR). With TUR, the infiltration depth and histological differentiation on which the further therapy steps depend can be relatively precisely diagnosed. The surgi-cal technique plays a large role, since a cut depth that is too low poses the risk of understaging superficial urinary bladder tumors. The objective of every TUR is complete resection.
Crucial for the prognosis of superficial urinary bladder carcinoma is not only the tumor stage, but also the degree of malignity. For a urinary bladder carci-noma with tumor stage Ta, after a TUR the likelihood of a superficial recurrence is 70 %. Progression to a higher tumor stage is about 4 % for TaG1 tumors, 20 % for TaG2 and 56 % for TaG3 (Table 1). Overall survival after 5 years is reduced from 96 % for a TaG1 tumor to 81 % for a T1G1 tumor. The probability of progres-sion increases from 4 % for TaG1 tumors to 19 % for T1G1 tumors [1].
Probability of recurrence after sole transurethral resection (TUR)
General• Primary therapy for superficial bladder carcinoma: TUR
• Despite complete removal of the tumor, high probability of recurrence after sole TUR
Clinical application38
Clinical application 39
IMMUCOTHEL®
for recurrence prevention
General
• With IMMUCOTHEL®, the probability of recurrence decreases from 70 % (TUR) to 30 %
• Only 15 % of recurrences progress
• For 26 % of the recurrent tumors downgrade
• IMMUCOTHEL® treatment is the best-tolerated therapy for patients
Lower probability of recurrence with an IMMUCOTHEL® treatmentAlready in 1974 Olsson et al. reported that for patients with a recurrent urinary bladder carcinoma, the recurrence fre-quency after a KLH treatment declined from 70 % to 30 % [1]. Numerous studies followed, both controlled as well as un-controlled, which confirmed the recurren-ce prevention effect of IMMUCOTHEL®.
In an analysis of 6 studies (mainly Ta- and T1 bladder carcinomas) with compa-rable appraisal criteria, the probability of
recurrence was 30 % [2–7]. Only a small proportion of the recurrences (15 %) in-dicated progression, while downgrading was determined for 26 % of the tumors (Fig. 1). In many studies, no distinction was made between primary and recur-rent tumors for the effectiveness assess-ment of IMMUCOTHEL®. The probability of recurrence of 30 % is therefore inde-pendent of the risk assessment of the Ta- and T1 bladder carcinomas.
Minimal side effects with an IMMUCOTHEL® treatmentApart from the good recurrence preventi-on effect of IMMUCOTHEL® both for pri-mary as well as for recurrent tumors, the great advantage of an IMMUCOTHEL® treatment is its very good patient tole-rance. An analysis of eight studies (n = 279), in which the side effects are listed in detail, only showed slight side effects
(Fig. 2), that never led to a discontinua-tion of therapy [2, 4–10]. Compared to all other therapies used to treat superficial urinary bladder carcinoma, an IMMUCO-THEL® treatment is tolerated best by patients.
Clinical application40
Fig.
1
Probability of recurrence and development of recurrences with an IMMUCOTHEL® treatment [2–7] (Summary of 6 studies, n = 346)
100%
Recurrence-free
Recurrence Downgrading Stable Progression
5060
40
8090
70
3020100
Fig.
2
Side effects with an IMMUCOTHEL® treatment [2, 4–10] (Summary of 8 studies, n = 279)
25%
Side effectsoverall
Mildcystitis
Fever< 38 °C
Severeside
effects
Dis-continuation
of therapy
15
10
20
5
0
Clinical application 41
Sources
1 Olsson CA, Chute R, Rao CN. Immunologic reduction of bladder cancer recurrence rate. J Urol. 1974 Feb; 111(2): 173–176.
2 Jurincic CD, Engelmann U, Gasch J, Klippel KF. Immunotherapy in bladder cancer with key-hole-limpet hemocyanin: a randomized study. J Urol. 1988 Apr; 139(4): 723–726.
3Weymann H, Ergebnisse einer Phase-II-Studie beim Harnblasenkarzinom mit IMMUCO-THEL® (KLH). IN: Kurth KH (Hrsg): IMMUCOTHEL®-Workshop III. Istanbul, 1. – 3. Dezember 1989; Schönaich, Papierhaus Mach (1992), pp. 101–107.
4Jurincic-Winkler C, Engelmann U, Beuth J, Klippel KF. Efficacy of local Bacillus Calmette-Guérin treatment in superficial bladder cancer relapsing under Keyhole-Limpet Hemocyanin immunotherapy. Zentralbl Bakteriol. 1995 Oct; 282(4): 409–415.
5Flamm J, Bucher A, Höltl W, Albrecht W. Recurrent superficial transitional cell carcinoma of the bladder: adjuvant topical chemotherapy versus immunotherapy. A prospective randomized trial. J Urol. 1990 Aug; 144(2 Pt 1): 260–263.
6 Flamm J, Bucher A. Adjuvant topical chemotherapy versus immunotherapy in primary superfi-cial transitional cell carcinoma of the bladder. Br J Urol. 1991 Jan; 67(1): 70–73.
7Kälble T, Möhring K, Ikinger U, Riedasch G, Staehler G. [Intravesical prevention of recurrence of superficial urinary bladder cancer with BCG and KLH. A prospective randomized study]. Urologe A. 1991 Mar; 30(2): 118–121.
8Jurincic-Winkler C, Metz KA, Beuth J, Sippel J, Klippel KF. Effect of keyhole limpet hemocy-anin (KLH) and bacillus Calmette-Guérin (BCG) instillation on carcinoma in situ of the urinary bladder. Anticancer Res. 1995 Nov-Dec; 15(6B): 2771–2776.
9Jurincic-Winkler CD, von der Kammer H, Beuth J, Scheit KH, Klippel KF. Antibody response to keyhole limpet hemocyanin (KLH) treatment in patients with superficial bladder carcinoma. Anticancer Res. 1996 Jul-Aug; 16(4A): 2105–2110.
10Echarti C, Jurincic-Winkler CD, Klippel KF. Efficacy of prophylactic Immucothel in patients pretreated with conventional drugs to prevent recurrence of superficial bladder carcinoma. Eur Urol. 2000; 37 Suppl 3: 50–53.
IMMUCOTHEL® for recurrence prevention of primary tumors
General• The probability of recurrence for primary tumors is 34 %
• 8 % of primary tumors downgrade
• Only 10 % the primary tumors progress
Sources
1 Flamm J, Bucher A. Adjuvant topical chemotherapy versus immunotherapy in primary superfi-cial transitional cell carcinoma of the bladder. Br J Urol. 1991 Jan; 67(1): 70–73.
2Jurincic-Winkler C, Engelmann U, Beuth J, Klippel KF. Efficacy of local Bacillus Calmette-Guérin treatment in superficial bladder cancer relapsing under Keyhole-Limpet Hemocyanin immunotherapy. Zentralbl Bakteriol. 1995 Oct; 282(4): 409–415.
3Jurincic-Winkler CD, von der Kammer H, Beuth J, Scheit KH, Klippel KF. Antibody response to keyhole limpet hemocyanin (KLH) treatment in patients with superficial bladder carcinoma. Anticancer Res. 1996 Jul-Aug; 16(4A): 2105–2110.
4Kurth KH, De Boer EC, De Reijke TM, 2004 Amsterdam, Immunological response following intravesical treatment with Immucothel (KLH) for superficial bladder carcinoma. Persönliche Mitteilung.
Probability of recurrence and development of recurrences for primary tumors with an IMMUCOTHEL® treatment [1–4] (summary of 4 studies, n = 150)
100%
Recurrence-free
Recurrence Downgrading Stable Progression
5060
40
8090
p < 0.05
p < 0.05
70
3020100
Due to the low number of patients with superficial urinary bladder carcinoma, only a few studies have investigated the effect of IMMUCOTHEL® on primary tu-mors [1–4]. Compared to studies that make no difference between primary and recur-rent tumors, the prevention of recurrence effect for primary tumors is comparable (Fig. 1). Despite the smaller number of studies (n = 4) and hence also fewer patients (n = 150), the differences bet-ween the studies are minor, as demons-trated by the smaller standard deviations. Especially the high standard deviations
in combined studies for downgrading of recurrences or a stable recurrence are considerably reduced. Therefore there is also a significant difference between the results for both of these parameters with primary tumors compared to com-bined studies, whereby the likelihood for downgrading decreases significantly (8 %; p = 0.01) and the likelihood for a stable recurrence increases significantly (82 %; p = 0.0059). Primary tumors show with 10 % a lower non-significant rate of progression.
Clinical application 45
Due to the low number of patients inves-tigated, only a few studies have evalua-ted the effect of IMMUCOTHEL® on recurrences of superficial urinary bladder carcinoma [1–4]. The analysis of 4 studies (n = 113) shows that the recurrence prevention effect for already recurrent tumors is significantly higher than in studies that made no difference between primary and recurrent tumors (44 %; p = 0.0081).
Here as well, despite the smaller number of studies and hence also fewer patients, there are fewer differences between the studies or accordingly smaller standard deviations.
Recurrences have a significantly lower likelihood for downgrading of a further recurrence compared to those in com-bined studies (10 %; p = 0.0424) (Fig. 1).
IMMUCOTHEL® for recurrence prevention of recurrent tumors
General• The probability of recurrent tumors is 44 %
• 10 % of the recurrent tumors downgrade
• 17 % of the recurrences progress
Clinical application46
Fig.
1
Probability of recurrence and development of recurrences in recurrent tumors with an IMMUCOTHEL® treatment [1–4] (Summary of 4 studies, n = 113)
100%
Recurrence-free
Recurrence Downgrading Stable Progression
5060
40
8090
p < 0.05
p < 0.05
70
3020100
Sources
1Flamm J, Bucher A, Höltl W, Albrecht W. Recurrent superficial transitional cell carcinoma of the bladder: adjuvant topical chemotherapy versus immunotherapy. A prospective randomized trial. J Urol. 1990 Aug; 144(2 Pt 1): 260–263.
2 Olsson CA, Chute R, Rao CN. Immunologic reduction of bladder cancer recurrence rate. J Urol. 1974 Feb; 111(2): 173–176.
3Echarti C, Jurincic-Winkler CD, Klippel KF. Efficacy of prophylactic Immucothel in patients pretreated with conventional drugs to prevent recurrence of superficial bladder carcinoma. Eur Urol. 2000; 37 Suppl 3: 50–53.
4Bassi, P.; Spinadin, R.; Saraeb, S.; Carando, R.; Balta, G.; Iannello, A. R., 2000: KLH im-munotherapy of BCG resistant carcinoma in situ of the bladder A phase II trial. European Urology. 37(suppl. 2): 113.
A special case of the superficial bladder carcinoma is the carcinoma in situ (CIS). After a TUR, progression to a muscle-in-vasive bladder tumor with CIS without further treatment is 54 %.
In comparison, only 2 % of the patients with a Ta grade 1 tumor progress to a muscle-invasive bladder carcinoma. Also after treatment with BCG or che-motherapy, the recurrence rate is 34 % or 50 %, whereby Mitomycin C is more effective in the treatment of CIS than
other chemotherapeutics. The "long-term disease-free rate" with a Mitomycin C tre-atment is 36 %, for BCG it is 46 % [1].
Several studies (n = 86) have specifically investigated the efficacy of IMMUCO-THEL® for CIS [2–5]. The recurrence rate with an IMMUCOTHEL® treatment is 48 %. Progression also declines to 20 % (Fig. 1). Especially relevant is that the "long-term disease-free rate" for an IM-MUCOTHEL® treatment is about 49 %.
IMMUCOTHEL® for recurrence prevention of carcinoma in situ
General• The "long-term disease-free rate" with an IMMUCOTHEL ®
treatment is 49 %
• Only 13 % of the recurrences progress
Clinical application48
Fig.
1
Comparison of conventional therapies with an IMMUCOTHEL® treatment of CIS shows that the highest long-term likelihood of not developing any further recurrences is given with an IMMUCOTHEL® treatment [1–5]
60%
Long-termrecurrence-free
Recurrence Progression
50
40
30
20
10
0
BCGIMMUCOTHEL® Mitomycin C
Sources
1Sylvester RJ, van der Meijden AP, Witjes JA, Kurth K. Bacillus calmette-guerin versus che-motherapy for the intravesical treatment of patients with carcinoma in situ of the bladder: a meta-analysis of the published results of randomized clinical trials. J Urol. 2005 Jul; 174(1): 86–91; discussion 91–92.
2Jurincic-Winkler C, Metz KA, Beuth J, Sippel J, Klippel KF. Effect of keyhole limpet hemo-cyanin (KLH) and bacillus Calmette-Guérin (BCG) instillation on carcinoma in situ of the urinary bladder. Anticancer Res. 1995 Nov-Dec; 15(6B): 2771–2776.
3Bassi, P.; Spinadin, R.; Saraeb, S.; Carando, R.; Balta, G.; Iannello, A. R., 2000: KLH im-munotherapy of BCG resistant carcinoma in situ of the bladder A phase II trial. European Urology. 37(suppl. 2): 113.
4Lamm DL, Morales A, Grossman HB, et al: Keyhole limpet hemocyanin (KLH) immunother-apy of papillary and in situ transitional cell carcinoma of the bladder: A multicenter phase I–II clinical trial. J Urol 155: A1405, 1996.
5 Lamm DL, Dehaven JI, Riggs DR. Keyhole limpet hemocyanin immunotherapy of bladder cancer: laboratory and clinical studies. Eur Urol. 2000; 37 Suppl 3: 41–44.
Superficial urinary bladder tumors are classified into risk groups that dictate the treatment recommendation (Table 1).
IMMUCOTHEL® is approved for the follo-wing superficial urinary bladder tumors:
• Primary and recurrent multifocal Ta • Singular T1G1 and T1G2 • Carcinoma in situ (CIS)
An IMMUCOTHEL® treatment is appro-ved for high-risk tumors as second-line treatment or in the event of failure or contraindication of BCG.
Approval of IMMUCOTHEL® for the following superficial urinary bladder carcinomas
General• Primary and recurrent multifocal Ta
• Singular T1G1 and T1G2
• Carcinoma in situ (CIS)
Sources
1Babjuk M, Burger M, Zigeuner R, Shariat SF, van Rhijn BW, Compérat E, Sylvester RJ, Kaasinen E, Böhle A, Palou Redorta J, Rouprêt M; European Association of Urology. EAU guidelines on non-muscle-invasive urothelial carcinoma of the bladder: update 2013. Eur Urol. 2013 Oct; 64(4): 639–653.
Tab.
1Risk groups for superficial urinary bladder tumors [1]
Risk group Definition
Low-risk tumors • Primary, solitary Ta, low grade/G1, < 3 cm, no CIS
Intermediate-risk tumors
• All tumors that are not in the low-risk or high-risk group
High-risk tumors • T1 tumor• High Grade/G3 tumor• CIS• Multiple, recurrent and large (> 3 cm) Ta-, G1-, G2
tumors
Clinical application50
Comparison of the immunotherapies IMMUCOTHEL® vs. BCG
• Frequent side effects result in a discontinuation of therapy with BCG treatment in 20 % of the cases
General
• Recurrence rate with an IMMUCOTHEL® treatment and a BCG treatment is comparable
• Minor side effect spectrum for IMMUCOTHEL® vs. severe side effects for BCG
• BCG-non-responsive tumors respond well to IMMUCOTHEL® treatment
Clinical application 51
Probability of recurrence with a BCG therapyBacillus Calmette-Guérin (BCG) is a we-akened live vaccine against tuberculosis developed in the early 20th century. In the 1980s it was shown that an instillation of BCG in the urinary bladder provides an effective form of immunotherapy for a urinary bladder carcinoma. The ex-act therapeutic action of BCG is not yet known, but is based on the activation of the immune system, as is the case with IMMUCOTHEL®.
Numerous meta-analyses have mean-while confirmed that treatment with BCG significantly reduces the recurrence rate of superficial urinary bladder tumors from 76 % to 24 %, compared with a sole TUR (Fig. 1) [1–9].
Severe side effects with BCG treatmentA treatment with BCG is frequently accompanied by sometimes severe side effects. The most frequent local side effects are cystitis, disorders in voiding from the urinary bladder and hematu-ria, which occur in approx. 75 % of the patients.
Systemic side effects such as flu-like symptoms, general malaise and fever oc-cur with approx. 40 % of the patients. It is recommended to discontinue subsequent instillations in the event of side effects.
This leads to sometimes only 16 % of the patients receiving all planned instillations [10]. Local and systemic side effects result in the discontinuation of the BCG therapy in approx. 20 % of the cases [1].
To reduce the occurrence of side effects, the following contraindications were com-piled for a BCG therapy [3]:
• TUR within the last 2 weeks• Traumatic catheter examination• Macroscopic hematuria• Urethral stenosis• Active tuberculosis• Prior BCG sepsis• Immunosuppression• Urinary tract infection
A BCG treatment is considered to have failed if one or more of the following occurs [1]:
1. Occurrence of a muscle-invasive bladder carcinoma
2. Occurrence of severe papillary tumors and/or CIS after 3 and 6 months
3. Progression during the BCG treatment4. BCG-intolerance5. Severe side effects due to the BCG
therapy
Clinical application52
Fig.
1
BCG significantly reduces the rate of recurrence and progression for superficial urinary bladder carcinomas compared to TUR [1–9]
100%
Recurrence-free Recurrence Progression
5060
40
8090
70
3020100
TUR BCG
Clinical application 53
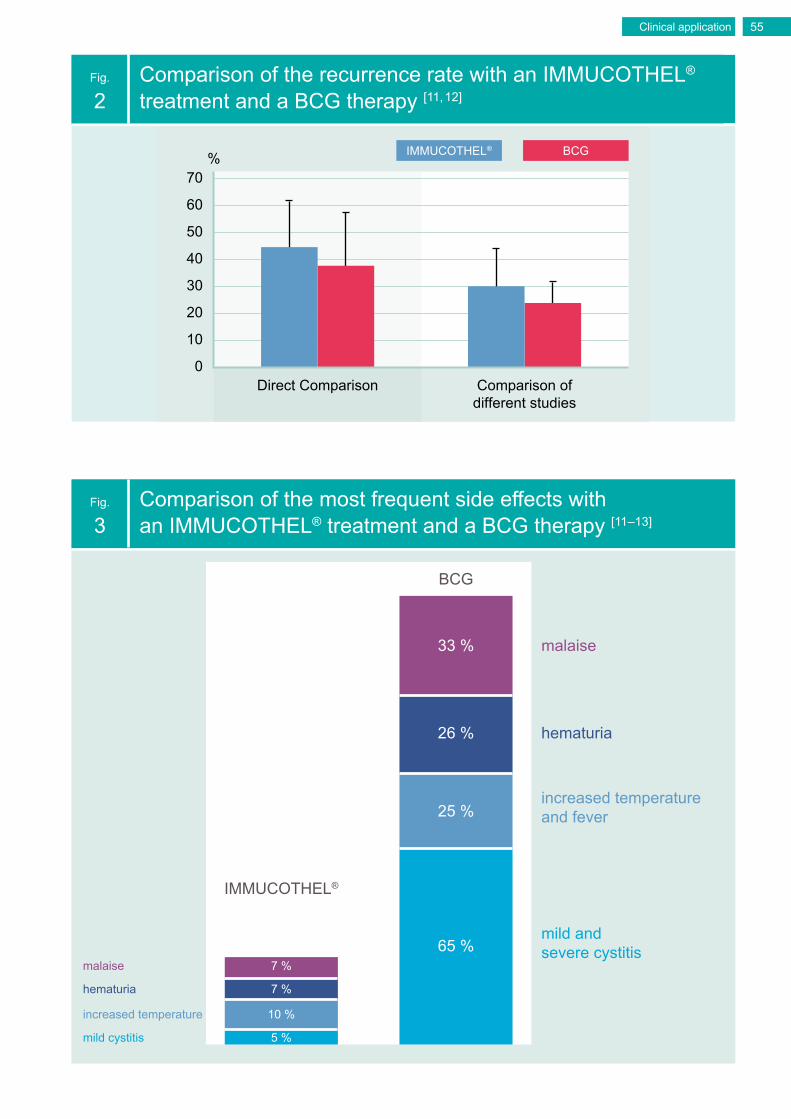
Comparable recurrence rate with significantly lower side effects with an IMMUCOTHEL® treatmentOnly in two studies (n = 212) was the recurrence rate for an IMMUCOTHEL® treatment and a BCG therapy compared directly [11, 12]. These studies showed a slightly increased recurrence rate with an IMMUCOTHEL® treatment, but without statistical significance (44 % vs. 38 %; p = 0.4988). A comparison with other studies in which either IMMUCOTHEL® or BCG was investigated also reveals a slightly increased, non-significant probability of recurrence. The greater number of total patients increases the significance of these values, which is also reflected in the lower standard deviation (Fig. 2).
Apart from the two already mentioned studies, another study compared the side effects of an IMMUCOTHEL® treatment and BCG therapy for superficial bladder carcinoma [11–13]. Side effects associated with an IMMUCOTHEL® treatment were overall markedly less frequent (p < 0.0001) (Fig. 3). In addition, the severity of the side effects with a BCG therapy is significantly higher. Whereas no serious side effects have developed with an IMMUCOTHEL® treatment until now, in the case of BCG therapy < 5 % of the patients developed serious side effects [1]. Ten patients have since died after an intravesical BCG therapy [14].
Clinical application54
Fig.
2Comparison of the recurrence rate with an IMMUCOTHEL® treatment and a BCG therapy [11, 12]
70%
Direct Comparison Comparison ofdifferent studies
50
60
40
30
20
10
0
BCGIMMUCOTHEL®
Fig.
3Comparison of the most frequent side effects with an IMMUCOTHEL® treatment and a BCG therapy [11–13]
IMMUCOTHEL®
BCG
malaise
hematuria
increased temperatureand fever
mild and severe cystitis
mild cystitis
increased temperature
hematuria
malaise
33 %
25 %
65 %
5 %
10 %
7 %
7 %
26 %
Clinical application 55
Effective treatment outcome with IMMUCOTHEL® on patients who do not respond to a BCG therapyIf a CIS does not respond to a BCG therapy or if there is progression of other superficial urinary bladder carcinomas, usually a radical cystectomy is recom-mended, since there is little likelihood that patients will react positively to a further BCG treatment. Furthermore, se-veral studies with conservative therapies such as chemotherapeutics have only delivered disappointing results.
Two studies have investigated the effect of an IMMUCOTHEL® treatment on su-perficial urinary bladder carcinomas that did not respond to a BCG therapy [15, 16]. 97 % of the tumors were a carcinoma in situ (CIS). It was found that an IMMUCO-THEL® treatment is positive for these pa-tients in two respects. Firstly, only 45 % of the patients had a recurrence with the IMMUCOTHEL® treatment (Fig. 4). Se-condly, in the case of these recurrences, only 21 % of the tumors showed progres-sion.
A comparison of these results with the probability of recurrence and progression with a BCG treatment of CIS or non-pri-mary tumors shows that the probability of recurrence with CIS does not differ (45 % vs. 45 %), whereby in the study of Kaasinen et al. no significant difference in the probability of recurrence between primary and secondary CIS could be determined [17]. Mitrakas et al. investiga-ted the recurrence rate of non-primary bladder carcinomas with a BCG therapy, of which about one third were CIS [18]. Here it was shown that there was a signi-ficant advantage for an IMMUCOTHEL® treatment after a failed BCG therapy and a further BCG therapy (45 % vs. 71 %; p = 0.0074). The comparison of the probability of progression for non-primary urinary bladder carcinomas, that were further treated with BCG, to non-primary BCG non-responsive CIS, that were tre-ated with IMMUCOTHEL®, shows a clear advantage for IMMUCOTHEL® vs. BCG (21 % vs. 43 %; p = 0.0174) (Fig. 5).
Clinical application56
Fig.
5
Significant advantage in the recurrence rate or likelihood of progression with an IMMUCOTHEL® treatment of BCG non-responsive non-primary CIS [18]
90
p < 0.05
p < 0.05%
Recurrence Progression
50607080
403020100
BCG with primary + non-primary CIS
IMMUCOTHEL® with BCG non-responsive non-primary CIS
Repeated BCG therapy of non-primary superficial urinary bladder tumors
Fig.
4
Recurrence rate or likelihood of progression when new recurrences occur with an IMMUCOTHEL® treatment of CIS that does not respond to a BCG therapy (n = 31) [15, 16]
60%
Recurrence-free Recurrence Progression
50
40
30
20
10
0
Clinical application 57
Sources
1Babjuk M, Burger M, Zigeuner R, Shariat SF, van Rhijn BW, Compérat E, Sylvester RJ, Kaasinen E, Böhle A, Palou Redorta J, Rouprêt M; European Association of Urology. EAU guidelines on non-muscle-invasive urothelial carcino-ma of the bladder: update 2013. Eur Urol. 2013 Oct; 64(4): 639–653.
2 Schenkman E, Lamm DL. Superficial bladder cancer therapy. ScientificWorldJournal. 2004 Jun 28; 4 Suppl 1: 387–399.
3 Sylvester RJ. Bacillus Calmette-Guérin treatment of non-muscle invasive bladder cancer. Int J Urol. 2011 Feb; 18(2): 113–120.
5Herr HW, Schwalb DM, Zhang ZF, Sogani PC, Fair WR, Whitmore WF Jr, Oettgen HF. Intravesical bacillus Calmette-Guérin therapy prevents tumor progression and death from superficial bladder cancer: ten-year follow-up of a prospective randomized trial. J Clin Oncol. 1995 Jun; 13(6): 1404–1408.
6Shahin O, Thalmann GN, Rentsch C, Mazzucchelli L, Studer UE. A retrospective analysis of 153 patients treated with or without intravesical bacillus Calmette-Guerin for primary stage T1 grade 3 bladder cancer: recurrence, pro-gression and survival. J Urol. 2003 Jan; 169(1): 96–100.
7Orsola A, Trias I, Raventós CX, Español I, Cecchini L, Búcar S, Salinas D, Orsola I. Initial high-grade T1 urothe-lial cell carcinoma: feasibility and prognostic significance of lamina propria invasion microstaging (T1a/b/c) in BCG-treated and BCG-non-treated patients. Eur Urol. 2005 Aug; 48(2): 231–238.
8Lee JY, Joo HJ, Cho DS, Kim SI, Ahn HS, Kim SJ. Prognostic Significance of Substaging according to the Depth of Lamina Propria Invasion in Primary T1 Transitional Cell Carcinoma of the Bladder. Korean J Urol. 2012 May; 53(5): 317–323.
9Kilinc MF, Sonmez NC, Dalkilic A, Arisan S, Guney S. Analysis of results of recurrence and progression rates of high-grade Ta bladder cancer and comparison with results of high-grade T1. Urologia. 2014 Oct-Dec; 81(4): 237–241.
10Lamm DL, Blumenstein BA, Crissman JD, Montie JE, Gottesman JE, Lowe BA, Sarosdy MF, Bohl RD, Grossman HB, Beck TM, Leimert JT, Crawford ED. Maintenance bacillus Calmette-Guerin immunotherapy for recurrent TA, T1 and carcinoma in situ transitional cell carcinoma of the bladder: a randomized Southwest Oncology Group Study. J Urol. 2000 Apr; 163(4): 1124–1129.
11 Kälble T, Möhring K, Ikinger U, Riedasch G, Staehler G. [Intravesical prevention of recurrence of superficial urinary bladder cancer with BCG and KLH. A prospective randomized study]. Urologe A. 1991 Mar; 30(2): 118–121.
12Jurincic-Winkler C, Metz KA, Beuth J, Sippel J, Klippel KF. Effect of keyhole limpet hemocyanin (KLH) and bacil-lus Calmette-Guérin (BCG) instillation on carcinoma in situ of the urinary bladder. Anticancer Res. 1995 Nov-Dec; 15(6B): 2771–2776.
13 Lamm DL. Laboratory and clinical experience with keyhole limpet hemocyanin (IMMUCO THEL®) in superficial blad-der cancer. J Urol. Urogynäkol 2003; 10(2): 18–21.
14 Lamm DL. Complications of bacillus Calmette-Guérin immunotherapy. Urol Clin North Am. 1992 Aug; 19(3): 565–572.
15 Bassi, P.; Spinadin, R.; Saraeb, S.; Carando, R.; Balta, G.; Iannello, A. R., 2000: KLH immunotherapy of BCG resis-tant carcinoma in situ of the bladder A phase II trial. European Urology. 37(suppl. 2): 113.
16 Echarti C, Jurincic-Winkler CD, Klippel KF. Efficacy of prophylactic Immucothel in patients pretreated with conven-tional drugs to prevent recurrence of superficial bladder carcinoma. Eur Urol. 2000; 37 Suppl 3: 50–53.
17Kaasinen E, Wijkström H, Malmström PU, Hellsten S, Duchek M, Mestad O, Rintala E; Nordic Urothelial Cancer Group. Alternating mitomycin C and BCG instillations versus BCG alone in treatment of carcinoma in situ of the urinary bladder: a nordic study. Eur Urol. 2003 Jun; 43(6): 637–645.
18Mitrakas LP, Zachos IV, Tzortzis VP, Gravas SA, Rouka EC, Dimitropoulos KI, Vandoros GP, Karatzas AD, Melekos MD, Papavassiliou AG. Previous Bladder Cancer History in Patients with High-Risk, Non-muscle-invasive Blad-der Cancer Correlates with Recurrence and Progression: Implications of Natural History. Cancer Res Treat. 2014 Sep 11.
• Comparable recurrence rate with an IMMUCOTHEL® and Mitomycin C treatment
General
• Lower probability of recurrence of recurrent tumors with an IMMUCOTHEL® treatment
• Higher likelihood of "5-years disease free" with an IMMUCOTHEL® treatment
• Significantly lower rate of progression with an IMMUCOTHEL® treatment
• Fewer discontinuations of therapy due to medication with an IMMUCOTHEL® treatment
Comparable recurrence rate with an IMMUCOTHEL® and Mitomycin C treatmentThree studies were conducted that direc-tly compared the efficacy of a Mitomycin C treatment with an IMMUCOTHEL® treatment for superficial bladder carcino-ma [1–3]. In all studies, no distinction was made between primary and recurrent tu-mors. Furthermore, the studies involved almost exclusively pTa and pT1 tumors grade 1 to 3 (only 1 % CIS).
Whereas two studies involved randomi-zed controlled tests, the study by Lam-mers et al. was a prospective, rando-mized phase III study that included ten times as many patients.
If one compares the two small phase I studies, the results for the probability of recurrence in both therapy groups are very similar ((IMMUCOTHEL®) 14.65 % ± 0.5 vs. 33.85 % ± 7.43 (Mitomycin C)), whereby in total there is a significantly lower probability of recurrence with an IMMUCOTHEL® treatment (p = 0.0463); despite the small number of patients (total n = 85; n (IMMUCOTHEL®) = 41; n (Mitomycin C) = 44) [1, 2].
Clinical application 59
Significant impact of the TUR on the subsequent treatmentThe evaluation of the study by Lammers et al. [3] presents greater difficulties, since the analysis showed that the TUR had a significant impact on the probability of recurrence in both therapy groups in a third of the involved institutes (Table 1). In the treatment of a not entirely removed urinary bladder carcinoma, a chemo-therapeutic agent such as Mitomycin C has a significant advantage, since the
mechanisms of action of a chemothera-peutic agent differ fundamentally from an immunotherapy's therapeutic action. The effect of an immunotherapeutic treat-ment is time-delayed, since the immune system must first be activated. Therefore the main impact of an immunotherapy is the prevention of recurrence and not the destruction of a residual tumor.
Lower probability of recurrence of recurrent tumorsIMMUCOTHEL® is approved as se-cond-line treatment or in the event of failure or contraindication of BCG for the following superficial urinary bladder tumors
• Primary and recurrent multifocal Ta• Singular T1G1 and T1G2• Carcinoma in situ (CIS)
The study by Lammers et al. included exactly the counted recurrent tumors with exception of the CIS. If one compares
the probability of recurrence in the pati-ents who were already pre-treated and therefore the treatment within the study represented a second-line treatment, it shows that an IMMUCOTHEL® treatment has a lower probability of recurrence (53 %) compared to a Mitomycin C the-rapy (64 %) [3]. Furthermore, the "5-years disease free" probability with a treatment of a second or further recurrence is higher with an IMMUCOTHEL® therapy (17 % vs. 9 %) (Fig. 1).
Clinical application60
Fig.
1
Comparison of the probability of recurrence and "5-years disease free" probability with an IMMUCOTHEL® and Mitomycin C therapy for recurrent tumors (n = 52)
70%
Recurrence "5-years disease free"
50
60
40
30
20
10
0
Mitomycin CIMMUCOTHEL®
Tab.
1 Comparison of the two clinical groups
Treatment Significance (p-value)
Recurrence rate Recurrence-free interval
IMMUCOTHEL® 0.003 0.004
Mitomycin C 0.050 0.051
Clinical application 61
Significantly lower rate of progression with an IMMUCOTHEL® therapyProgression did not frequently occur in the study by Lammers et al., since the patients were observed until the first recurrence and not until the first progres-sion. A total of 20 patients experienced
progression. The likelihood of progres-sion with an IMMUCOTHEL® treatment was 3.1 %, and 17.2 % with a Mitomy-cin C therapy, corresponding to a signifi-cance of p = 0.0003 (Fig. 2) [3].
Fewer discontinuations of therapy due to the medi-cation with an IMMUCOTHEL® treatmentBased on its size, the study by Lammers et al. provides significant conclusions about the side effects of an IMMUCO-THEL® or Mitomycin C treatment [3]. Out of a total of 523 patients, 168 pati-ents experienced no side effects, with no difference between the two thera-pies (33 %, 31 %). Whereas the number
of occuring side effects did not differ in connection with the treatment, the oc-currence of moderate and severe side effects with a Mitomycin C treatment was 10 % higher, which was not significant, but displayed a trend (p = 0,0819).
Clinical application62
Fig.
3
Comparison of the probability of therapy failure with an IMMUCOTHEL® and Mitomycin C treatment [3]
Mitomycin CIMMUCOTHEL®
12%
Discontinuation of therapy triggered by the medication
10
8
6
4
2
0
p < 0.0001
Fig.
2Comparison of the rate of progression with an IMMUCOTHEL® and Mitomycin C treatment [3]
Mitomycin CIMMUCOTHEL®
20%
Progression
1012
8
1618
14
6420
p = 0.0003
Clinical application 63
Fig.
4
Comparison of the likelihood of an allergic reaction to the medication with an IMMUCOTHEL® and Mitomycin C treatment [3]
Mitomycin CIMMUCOTHEL®
10%
Allergic reaction triggered by the medication
56
4
89
7
3210
p < 0.0001
Sources
1 Jurincic CD, Engelmann U, Gasch J, Klippel KF. Immunotherapy in bladder cancer with key-hole-limpet hemocyanin: a randomized study. J Urol. 1988 Apr; 139(4): 723–726.
2 Al-Naieb Z, Shubber H, Shalli A. Treatment of metaplastic carcinoma of the bladder: 2-years follow-up with keyhole limpet hemocyanin (KLH). Uroskop 1990; 3/90: 18–20.
3Lammers RJ, Witjes WP, Janzing-Pastors MH, Caris CT, Witjes JA. Intracutaneous and intra-vesical immunotherapy with keyhole limpet hemocyanin compared with intravesical mitomycin in patients with non-muscle-invasive bladder cancer: results from a prospective randomized phase III trial. J Clin Oncol. 2012 Jun 20; 30(18): 2273–2279.
A discontinuation of therapy triggered by the medication occured with 25 patients (10 %) undergoing Mitomycin C treat-ment, whereby half of the patients sho-wed an allergic reaction to Mitomycin C (Fig. 3). A total of 6.3 % of the cases had an allergic reaction to Mitomycin C, whereas there were no allergic to IMMU-COTHEL® (Fig. 4).
A discontinuation of therapy in connec-tion with the IMMUCOTHEL® treatment occurred in 3 cases (1 %). This data shows that both the probability of thera-py failure due to the medication as well as the occurrence of an allergic reaction with an IMMUCOTHEL® treatment is sig-nificantly lower (respectively p < 0.0001).
Overview of the probability of recurrence of non-invasive superficial bladder carcinoma [1]
80%
BCG (n = 689)
IMMU-COTHEL®
(n = 447)
Mito-mycin C
(n = 1,006)
Ethoglucid(n = 170)
Doxo-rubicin
(n = 798)
50
60
40
70
30
20
10
0Epi-
rubicin(n = 100)
Thiotepa(n = 528)
TUR (n = 737)
Probability of recurrence
OverviewComparison of recurrence prevention, progression, and therapy failure rate of the various therapies
Clinical application 65
Comparison of the therapy failure rate due to the medication
Overview for the probability of therapy failure for non-invasive superficial bladder carcinoma [3, 4]
25%
IMMUCOTHEL® Mitomycin C BCG
15
20
10
5
0
Rate of discontinuation of therapy
Comparison of the rate of progression
Overview of the probability of progression of non-invasive superficial bladder carcinoma [2]
16%
IMMUCOTHEL® BCG Mitomycin C
1412
68
10
420
Rate of progression
Clinical application66
Comparison of the side effects of the respective treatment
Overview of the occurrence of the most frequent side effects with an IMMUCOTHEL®, BCG and Mitomycin C treatment [5, 6]
70%
Cystitis Hematuria Fever Malaise Allergicreaction
50
60
40
30
20
10
0
IMMUCOTHEL® 5 % 5 % 10 % 7 % 0 %
BCG 54 % 32 % 20 % 36 % 2 %
Mitomycin C 40 % 30 % 4 % 14 % 5 %
Sources
1 Schenkman E, Lamm DL. Superficial bladder cancer therapy. ScientificWorldJournal. 2004 Jun 28; 4 Suppl 1: 387–399.
2Sylvester RJ, van der MEIJDEN AP, Lamm DL. Intravesical bacillus Calmette-Guerin reduces the risk of progres-sion in patients with superficial bladder cancer: a meta-analysis of the published results of randomized clinical trials. J Urol. 2002 Nov; 168(5): 1964–1970.
3Babjuk M, Burger M, Zigeuner R, Shariat SF, van Rhijn BW, Compérat E, Sylvester RJ, Kaasinen E, Böhle A, Palou Redorta J, Rouprêt M; European Association of Urology. EAU guidelines on non-muscle-invasive urothelial carcino-ma of the bladder: update 2013. Eur Urol. 2013 Oct; 64(4): 639–653.
4Lammers RJ, Witjes WP, Janzing-Pastors MH, Caris CT, Witjes JA. Intracutaneous and intravesical immunotherapy with keyhole limpet hemocyanin compared with intravesical mitomycin in patients with non-muscle-invasive bladder cancer: results from a prospective randomized phase III trial. J Clin Oncol. 2012 Jun 20; 30(18): 2273–2279.
5 Gontero P, Bohle A, Malmstrom PU, O’Donnell MA, Oderda M, Sylvester R, Witjes F. The role of bacillus Calmette-Guérin in the treatment of non-muscle-invasive bladder cancer. Eur Urol. 2010 Mar; 57(3): 410–429.
6 Böhle A, Jocham D, Bock PR. Intravesical bacillus Calmette-Guerin versus mitomycin C for superficial bladder cancer: a formal meta-analysis of comparative studies on recurrence and toxicity. J Urol. 2003 Jan; 169(1): 90–95.
General• KLH as additive of immunotherapeutic agents in treating cancer
• KLH as carrier protein for tumor vaccines
KLH increases the effect of a standard immunotherapeutic treatment of melanomasMcFadden et al were able to demons-trate in an in vitro study, that KLH has an antiproliferative effect on melanomas or an additive effect in combination with alpha-interferon and interleukin-2 [1]. Al-pha-interferon and interleukin-2 are both standard immunotherapeutic treatments for melanomas. Studies conducted on mice have substantiated these results in vivo [2]. A combination of KLH and inter-leukin-2 reduced the tumor volume by
30 % (p = 0.014). With KLH and alpha-in-terferon, the tumor volume was reduced by 28 % (p = 0.031).
In contrast, an individual treatment only showed a significant reduction (30 %; p = 0.022) with interleukin-2, whereas KLH and alpha-interferon reduced the tumor insignificantly by 18 % and 16 % respectively (Fig. 1).
Additional information68
Fig.
1
KLH increases the effect of alpha-interferon, a standard immunotherapeutic treatment against melanoma, in vivo [2]
35%
Alpha-interferon
Interleukin-2 KLH Alpha-interferon
+ KLH
Interleukin-2+ KLH
25
30
20
p = 0.022 p = 0.031 p = 0.014
15
10
5
0
Reduction of the tumor volume
Additional information 69
Immunostimulating properties of KLH as the basis for tumor vaccinesIn the rapidly-growing area of tumor vaccines, KLH has special significance. A large number of important carcinoge-nic antigens show poor immunogenicity when injected into humans.
However, the immunogenicity of these antigens increases significantly when they are conjugated on highly immuno-genic protein carriers such as KLH. A large number of cancer antigens have meanwhile been coupled to KLH, crea-ting very promising tumor vaccine candi-dates, among others against follicular or non-Hodgkin lymphomas, glioblastomas, melanomas, breast and ovarian carcino-mas [3].
Phase I and II studies are meanwhile available for several cancer types [4–6]. A phase II study with glioblastoma pati-ents is of particular interest here. Glioblastomas are highly aggressive brain tumors that until now have always ended fatally and non-responsive to available conventional therapies. One of the most frequent genetic changes in glioblastomas is the amplification of the EGFR gene, whereby most changes concern the mutant EGFR gene EGFRvI-II. EGFRvIII is expressed in approx. 30 % of newly diagnosed glioblastoma patients and is a negative prognostic fac-tor for long-term survival. Eighteen pati-ents were treated with a vaccine against EGFRvIII (PEPvIII-KLH/CDX-110) [5]. In contrast to the routinely applied che-motherapeutics, the vaccine showed only a minimum toxicity. The duration until progression was significantly prolonged from 6.3 to 14.2 months among the vac-cinated patients (p = 0.0102).
The survival time was likewise prolonged from 15 to 26 months (p < 0.0001). In addition, the effect of the vaccination on the standard chemotherapy with te-mozolomide was investigated. The time period until progression increased from 6.4 to 15.2 months (p = 0.0004) or for survival from 15.2 to 23.2 months. Based on these encouraging results, a larger phase II-study is already running, and a phase III-study is in planning.
Phase III studies for breast cancer pati-ents with metastases are already availa-ble in which the tumor-associated anti-gen Sialyl-Tn, whose expression is also associated with a poor prognosis among other things for breast cancer, is coupled to KLH. The study comprised 1,028 wo-men and compared Sialyl-Tn-KLH with KLH alone [7]. Although the Sialyl-Tn-KLH vaccine was well tolerated, there was no significant advantage in the time period until progression (3.4 vs. 3.0 months) or survival (23.1 vs. 22.3 months). Ho-wever, the authors posed the question whether the clinical advantage had been distorted by using a KLH control group instead of a placebo control group, due to a non-tumor-specific immune respon-se to KLH. Significantly higher anti-KLH antibody titers in the KLH control group support this statement.
A retrospective blinded review of the data from this study also showed that women, who had additionally received a conco-mitant endocrine therapy, had a longer time period until progression or survival in the Sialyl-Tn-KLH group (36.5 vs. 30.7 months) [8].
Additional information70
Sources
1 McFadden DW, Riggs DR, Jackson BJ, Ng A, Cunningham C. Keyhole limpet hemocyanin potentiates standard immunotherapy for melanoma. Am J Surg. 2007 Feb; 193(2): 284–287.
2 Rizvi I, Riggs DR, Jackson BJ, McFadden DW. Keyhole limpet hemocyanin: an effective adjunct against melanoma in vivo. Am J Surg. 2007 Nov; 194(5): 628–632.
3Kantele A, Häkkinen MP, Zivny J, Elson CO, Mestecky J, Kantele JM. Humoral immune response to keyhole limpet haemocyanin, the protein carrier in cancer vaccines. Clin Dev Immunol. 2011; 2011:614383.
4
Curti A, Tosi P, Comoli P, Terragna C, Ferri E, Cellini C, Massaia M, D’Addio A, Giudice V, Di Bello C, Cavo M, Conte R, Gugliotta G, Baccarani M, Lemoli RM. Phase I/II clinical trial of sequential subcutaneous and intravenous delivery of dendritic cell vaccination for refractory multiple myeloma using patient-specific tumour idiotype protein or idiotype (VDJ)-derived class I-restricted peptides. Br J Haematol. 2007 Nov; 139(3): 415–424.
6Baek S, Kim YM, Kim SB, Kim CS, Kwon SW, Kim Y, Kim H, Lee H. Therapeutic DC vaccina-tion with IL-2 as a consolidation therapy for ovarian cancer patients: a phase I/II trial. Cell Mol Immunol. 2015 Jan; 12(1): 87–95.
7Miles D, Roché H, Martin M, Perren TJ, Cameron DA, Glaspy J, Dodwell D, Parker J, Mayor-domo J, Tres A, Murray JL, Ibrahim NK; Theratope® Study Group. Phase III multicenter clinical trial of the sialyl-TN (STn)-keyhole limpet hemocyanin (KLH) vaccine for metastatic breast cancer. Oncologist. 2011; 16(8): 1092–1100.
8Ibrahim NK, Murray JL, Zhou D, Mittendorf EA, Sample D, Tautchin M, Miles D. Survival Advantage in Patients with Metastatic Breast Cancer Receiving Endocrine Therapy plus Sialyl Tn-KLH Vaccine: Post Hoc Analysis of a Large Randomized Trial. J Cancer. 2013 Aug 22; 4(7): 577–584. eCollection 2013.
Worldwide first GMP production processAt first a GMP production process had to be developed in order to be able to use the KLH in pharmaceutical research. The active substance immunocyanin, a preparation made of subunits of the hemocyanin, is isolated from the he-molymphs of the Californian sea snail Megathura crenulata.
The first phase – obtaining the he-molymphs – is performed in the GMP production facility in Carlsbad, California.
The cleaning and processing activities involved in manufacturing the drug pro-duct are carried out in the production line (likewise GMP-compliant) in Fellbach near Stuttgart, Germany.
biosyn has invested millions of euros and over two decades of research and development in the transatlantic project and in the sea snail.
Worldwide first GMP production process for immunocyanin
General
• Extraction of the hemolymphs in a GMP production facility
• Two decades of biosyn research and investment of millions of euros
• The keyhole limpets are returned undamaged to the sea after the serum has been removed
• The VACMUNE® manufactured from immunocyanin serves as carrier material for modern vaccines
Additional information72
Sea-water acquaria for keeping keyhole limpets
Sea-water cleaning system of the self-developed aquaria
Additional information 73
Preparation of the chromatographic cleaning of keyhole limpet hemocyanin
The blue color comes from copper atoms that bind to the active center of the glycoprotein hemocyanin of the oxygen. Hemocyanin is responsible for the oxygen transport in the sea snail.
Additional information74
Sterile puncture of the sea limpet Megathura crenulata under laminar flow. (GMP class 10,000 cleanroom)
Additional information 75
IMMUCOTHEL 1 mg, powder for solution for injection / IMMUCOTHEL 10 mg, powder for solution for intravesical use Active ingredient: ImmunocyaninIndications: Prevention of bladder carcinoma recurrence after transurethral resection and after failure of established therapies for this indication.Composition: IMMUCOTHEL® 1 mg: 1 vial with 54.63 mg powder for injections contains 1 mg biotechnically obtained, chromatographically uniform, molecularly standardized immu-nocyanin. Each vial is accompanied by 1 ampoule with 1 ml solvent. IMMUCOTHEL® 10 mg: 1 vial with 546.3 mg powder for intravesical instillations contains 10 mg of biotechnically obtained, chromatographically uniform, molecularly standardized immunocyanin. Each vial is accompanied by 1 ampoule with 10 ml solvent. Excipients: Powder: Glycine, sodium hydroxide, sodium chloride, sucrose. Solvent: Water for injections.Contra-indications: Immunosuppression. Known hypersensitivity to proteins foreign to the body.Undesirable effects: Hepatobiliary disorders Rare (1/10,000 to <1/1,000): increase of γ-glutamyl transferase and of glutamate pyruvate transaminase. Renal and urinary disorders Rare (1/10,000 to <1/1,000): Urgency,feeling of pressure or pain. Not known (cannot be estimated from the available data): Allergic reactions of the bladder manifesting as sterile leukocyturia.General disorders and administration site conditions Uncommon (1/1,000 to <1/100): Subfebrile temperatures are sometimes reported but are reversible after 3 days. Interactions: Specific interactions were not observed. The immunostimulating effect of IMMUCOTHEL® may be impaired by concurrent immunosuppressive radio- or chemotherapy or by simultaneous administration of corticosteroids.Packages: IMMUCOTHEL® 1 mg / 10 mg: 1 vial of 1 mg / 10 mg immunocyanin and 1 ampoule with 1 ml / 10 ml solvent.Subject to prescription 03/15 e Marketing authorization holder: biosyn Arzneimittel GmbH, Schorndorfer Strasse 32, 70734 Fellbach, Germany, Tel. + 49 - 711 - 575 32 00, Fax + 49 - 711 - 575 32 99, www.biosyn.de, E-Mail: [email protected]
CompositionIMMUCOTHEL® 1 mg
1 vial with 54.63 mg powder for injections contains 1 mg biotechnically obtained, chromatographically uniform, molecularly standardized immunocyanin. Each vial is accompanied by 1 ampoule with 1 ml solvent.
PZN: 2434955
IMMUCOTHEL® 10 mg
1 vial with 546.3 mg powder for intra-vesical instillations contains 10 mg of biotechnically obtained, chromatographi-cally uniform, molecularly standardized immunocyanin. Each vial is accompanied by 1 ampoule with 10 ml solvent.
GMP production of sodium selenite at biosyn: Vacuum drying facility for the selective crystallization
of metal salts with defined hydrate percentages
Die biosyn Arzneimittel GmbH
World market leader for high-dose selenium injections
biosyn Arzneimittel GmbH is a pharmaceutical and biotech company based in Fellbach, Germany. It specializes in trace elements, is a world market leader for high-dose selenium injections, developer and operator of two unique GMP manufacturing operations for producing active ingre-dients, and in the biotech sector, is actively involved in the production of glycoprotein isolated from the Megathura crenulata, a sea snail found in California. 70 percent of our sales turnover is realized outside of Germa-ny – in 26 countries all around the world.
With products geared to the areas of intensive care, oncology and en-docrinology, biosyn is a partner to hospitals and physicians in private practice, as well as to naturopathic physicians and holistic health practi-tioners. We pursue research and development and evaluate the current medical- scientific literature as well as engage in modern online marketing. Our mid-sized family enterprise places great value on an open, engaged and customer-oriented corporate culture.
78
79
IMMUCOTHEL® – for recurrence prevention of superficial urinary bladder carcinomas