42
| Date post: | 16-Dec-2015 |
| Category: |
Documents |
| Upload: | dina-charles |
| View: | 218 times |
| Download: | 3 times |

Edward Jenner(1749-1823)
Smallpox (1796)
Sarah Nelmes
James Phipps
Blossom
Immunizations
Vaccines are biologically active agents that induce the production of specific antibodies to render the subject protected (immune) against infectious diseases.
Constituents in a vaccine
Active immunizing agent
Suspending fluid
Preservatives (thimerosal)
Antibiotics (neomycin, streptomycin, polymyxin B)
Adjuvants (aluminum hydroxide, AS04)
Stabilizers (Tween)
Immunizing agents
Live, attenuated organisms
Killed, inactivated organisms
Subparticle (proteins, polysaccharides)

Hepatitis B
Subparticle vaccine (HBsAg)
Recombinant
Aluminum hydroxide
IM, 3 doses: 0, 1, 6 months0, 2, 6 months
No boosters
Hepatitis B
Infants born to HBsAg(+) mothersin addition should receive HBIG 0.5 ml, IM, 1 dose
Injection site pain and low grade fever (1-6%)safe in pregnancy

DTaP
Diphtheria toxoid (protein)Tetanus toxoid (protein)Pertussis acellular (subparticle)
whole cell (killed)
DTaP
Detoxified in formaldehyde, aluminum, Tween, thimerosal, no antibiotics
IM, 0.5 mL
Primary series (3): 2, 4, 6 monthsBooster (2): 12-18 mo, 4-6 years
Efficacy 80%, lasts for ~ 3 years
Boosters q 10 years (Td)
DTaP
Common adverse reactions:fever, redness and swelling at site, fretfulness, anorexia, drowsiness
Precautions for DTaP
Convulsions, with or without fever, within 3 d
Persistent crying for > 3 hrs, within 48 hrs.
Collapse or shock-like state within 48 hrs.
Temperature > 40.5 oC within 48 hrs
Vaccination might be deferred in children with progressive neurological disorder.

Contraindications for DTaP
Anaphylactic reactions
Encephalopathy within 7 days.
Polio vaccines
Injectable IPV
Oral OPV
Inactivated Polio Vaccine
Formalin inactivated
Trivalent (serotype 1, 2, 3)
Trace amounts of neomycin, streptomycin and polymyxin B.
SQ, 0.5 mL
Primary series: 2, 4, 18 monthsBooster: 4-6 yrs
(1 adult booster for travelers)
Inactivated Polio Vaccine
Local reactions 10 %
Low grade temperature 30 %
Precautions/contraindications:allergy to any of the components of the vaccine
Live Polio Vaccine
Vaccine Paralytic Polio:
1 every 3million doses8-10 cases per year in the UStype 3 more frequent (2, 1)usually after first dose1/2 recipients, 1/2 contacts
Precaution: immune suppressed patients or contacts

Hib vaccine
Subparticle vaccines (PRP) conjugated with protein carrier.
Protein carrier allows for:T-cell dependent antigenBetter immunogenicity (infants)Booster effect

Hib vaccines
IM, 0.5 mL
2, 4, 6, 12-15 mo
No boosters
Very safe vaccines. Local injection site reactions occur in 25 % but are very mild. Systemic reactions are very uncommon.
Pneumococcal Conjugate Vaccine
PCV-13
PCV-7
Pneumococcal Conjugate (PCV-13)
• Subparticle (polysaccharide), conjugate
• 13 valent
• IM, , 0.5 mL, 4 doses
• Primary series: 2, 4, 6 months of age
• Booster: 12–15 months
Pneumococcal Conjugate (PCV-13)
Catch-Up (Temporary)
For those who have received PCV-7 partial series, complete series with PCV-13
For those who have completed PCV-7 series, give one extra dose PCV-13 routine up to 5 yr; underlying conditions up to 18 yr

Pneumococcal Polysaccharide Vaccine (PCV-23)
• In addition to PCV-13, children at high risk for severe pneumococcal infection should receive one (or more doses of polysaccharide pneumococcal vaccine (PCV-23) starting at 24 months of age.
Measles, Mumps, Rubella
Live attenuated
Grown in chick embryo,no preservatives,neomycin
SQ, 0.5 mL
Series (2 doses):12-18 mo and 4-6 yrs
Side effects: 5-15% (fever, rash)
P/C: pregnancy, allergies (egg, neomycin), immune globulin, immune suppression, HIV OK except for C3 or CD4<15%
Varicella
Live attenuated, Oka strain
Neomycin, no preservatives
SQ, 0.5 ml
Side effects 5-10% rash
Series: 2 doses at 12-15 m, 4-6 y
P/C: pregnancy, allergies, immune globulin, salycilates, immunodeficiencies (except humoral), HIV: OK for CD4>15%

MMRV
Increase risk of febrile seizures (1‰2 ‰)after 1st dose
1st dose: 1) MMR + V 2) MMRV
2nd dose: 1) MMRV 2) MMR + V
Hepatitis A vaccine
Formalin inactivated virus
Aluminum hydroxide as adjuvant
IM, 2 doses (6-12 months apart)
12 months - 24 months
Can be used for Post-Exposure prophylaxis (within 2w)
Efficacy: 79 - 99 %
Side effects: soreness injection site (56 %)headache (14 %), malaise (7 %)
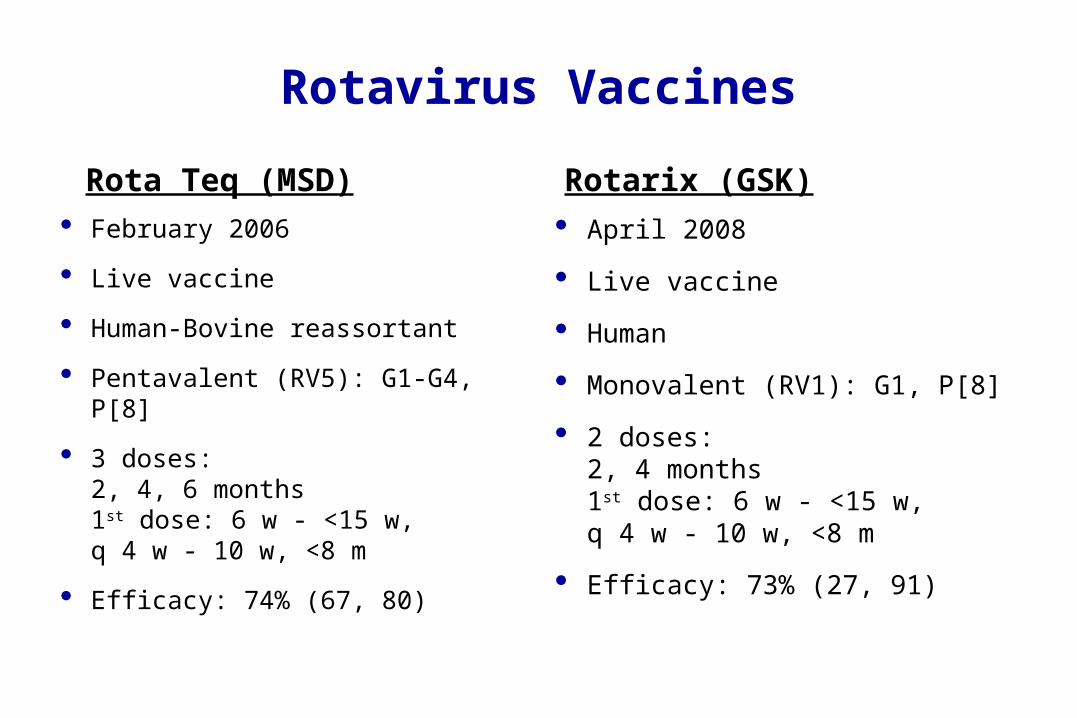
Rotavirus Vaccines
Rota Teq (MSD) February 2006
Live vaccine
Human-Bovine reassortant
Pentavalent (RV5): G1-G4, P[8]
3 doses:2, 4, 6 months1st dose: 6 w - <15 w, q 4 w - 10 w, <8 m
Efficacy: 74% (67, 80)
Rotarix (GSK) April 2008
Live vaccine
Human
Monovalent (RV1): G1, P[8]
2 doses:2, 4 months1st dose: 6 w - <15 w, q 4 w - 10 w, <8 m
Efficacy: 73% (27, 91)

Influenza Vaccines
TIV
Inactivated, split-virus
Chick embryo
Tri-valent (two A, one B), reformulated yearly
IM, 1 or 2 doses
All subjects 6 months and older
LAIV
Live, cold-adapted
Chick embryo
Tri-valent (two A, one B), reformulated yearly
Intranasal, 1 or 2 doses
Healthy, 2-49 years

Influenza Vaccine
Recommendations:
Universal immunization for all subjects 6 months and older
Special emphasis to children < 5 y and all household contacts and out-of-home caregivers of children < 5 y of age
TIV to all 6 months-olderLAIV to healthy 2-49 yr
MMWR 2010;vol 59, RR-8
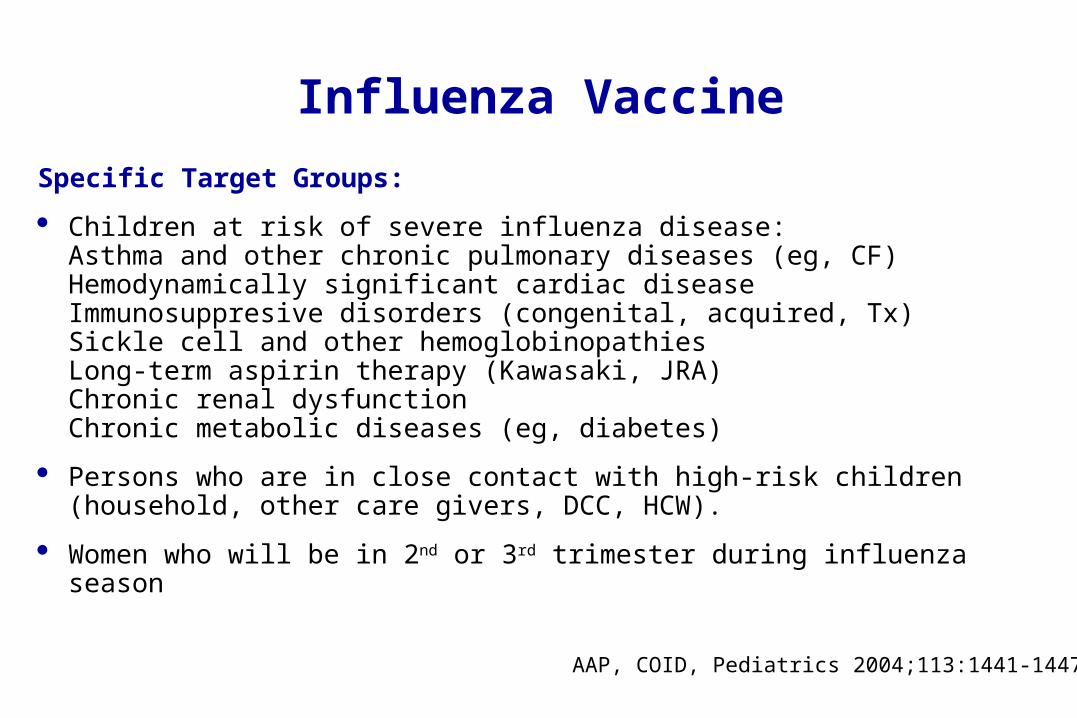
Influenza Vaccine
Specific Target Groups:
Children at risk of severe influenza disease:Asthma and other chronic pulmonary diseases (eg, CF)Hemodynamically significant cardiac diseaseImmunosuppresive disorders (congenital, acquired, Tx)Sickle cell and other hemoglobinopathiesLong-term aspirin therapy (Kawasaki, JRA)Chronic renal dysfunctionChronic metabolic diseases (eg, diabetes)
Persons who are in close contact with high-risk children (household, other care givers, DCC, HCW).
Women who will be in 2nd or 3rd trimester during influenza season
AAP, COID, Pediatrics 2004;113:1441-1447

Human Papillomavirus (HPV)
70% sexually active women
Cause of cervical carcinoma especially serotypes 16 and 18 (70%)
Cause of genital warts especially serotypes 6 and 11 (90%)
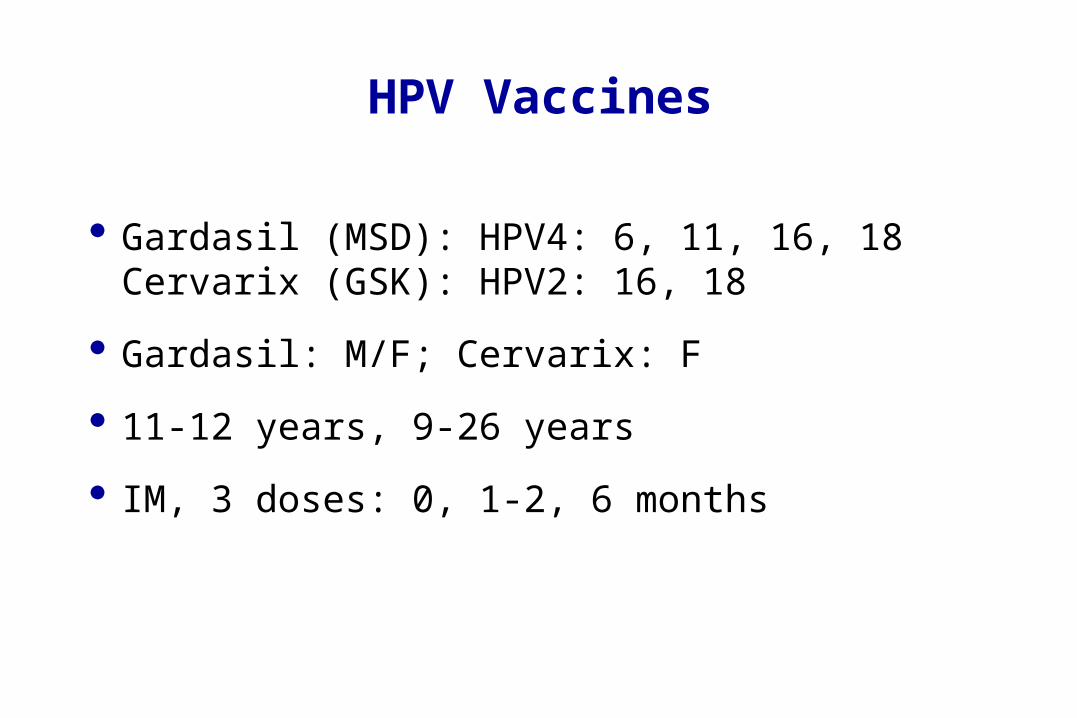
HPV Vaccines
Gardasil (MSD): HPV4: 6, 11, 16, 18Cervarix (GSK): HPV2: 16, 18
Gardasil: M/F; Cervarix: F
11-12 years, 9-26 years
IM, 3 doses: 0, 1-2, 6 months
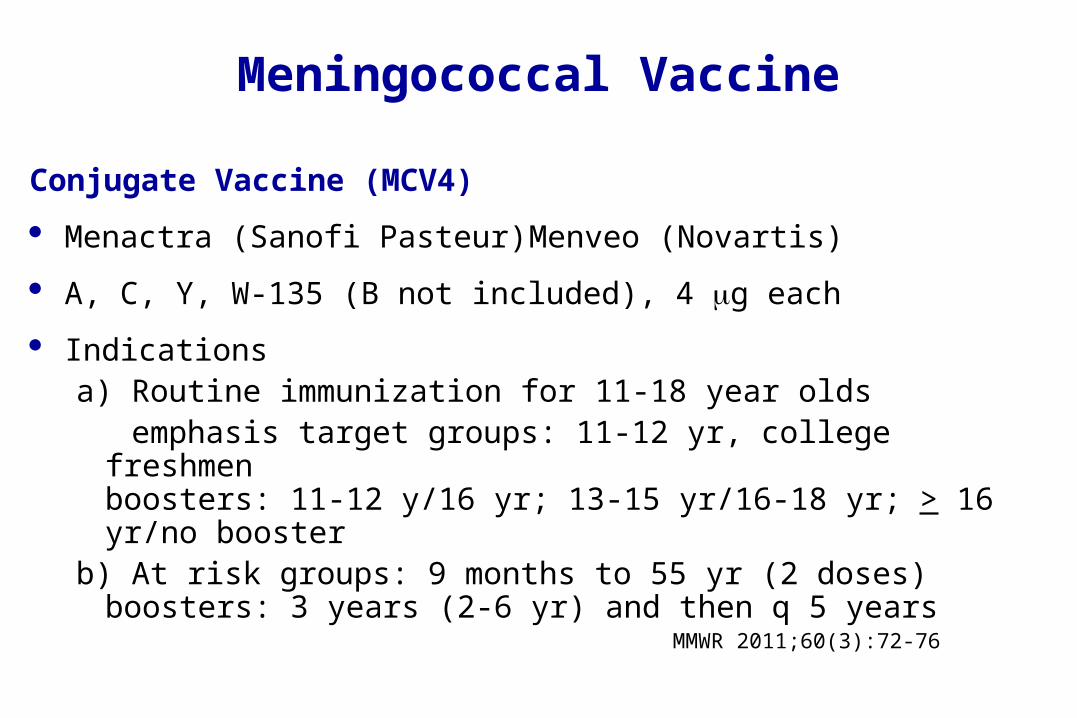
Meningococcal Vaccine
Conjugate Vaccine (MCV4)
Menactra (Sanofi Pasteur) Menveo (Novartis)
A, C, Y, W-135 (B not included), 4 g each
Indicationsa) Routine immunization for 11-18 year olds emphasis target groups: 11-12 yr, college freshmen
boosters: 11-12 y/16 yr; 13-15 yr/16-18 yr; > 16 yr/no boosterb) At risk groups: 9 months to 55 yr (2 doses)
boosters: 3 years (2-6 yr) and then q 5 years
MMWR 2011;60(3):72-76
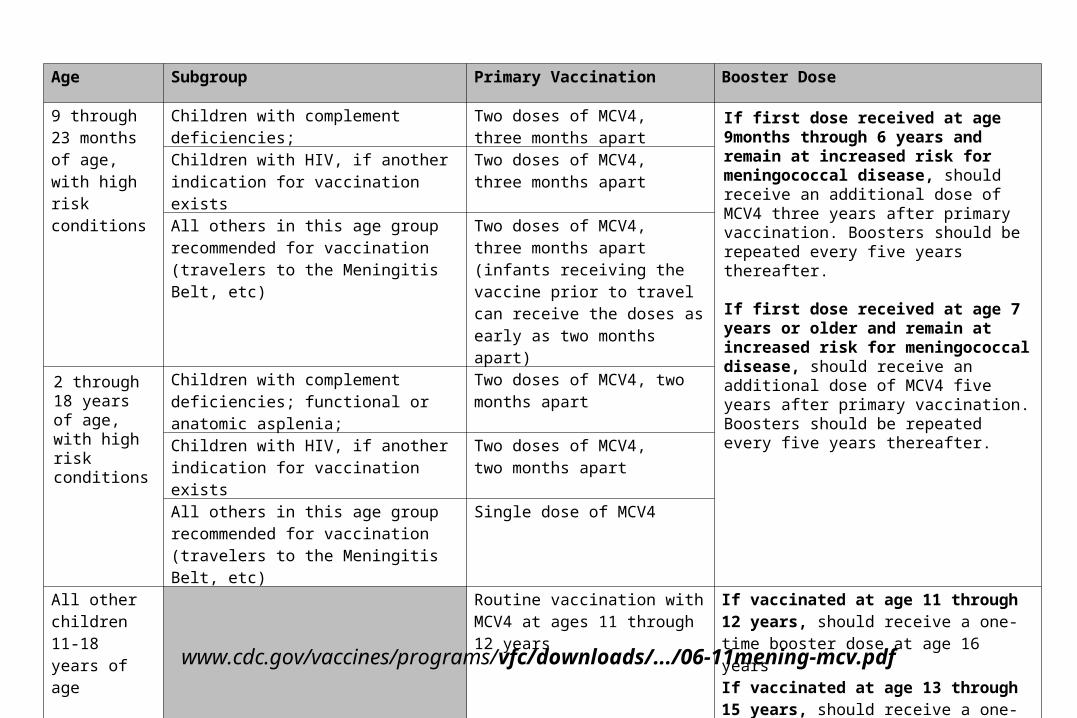
Age Subgroup Primary Vaccination Booster Dose
9 through 23 months of age, with high risk conditions
Children with complement deficiencies; Two doses of MCV4, three months apart
If first dose received at age 9months through 6 years and remain at increased risk for meningococcal disease, should receive an additional dose of MCV4 three years after primary vaccination. Boosters should be repeated every five years thereafter. If first dose received at age 7 years or older and remain at increased risk for meningococcal disease, should receive an additional dose of MCV4 five years after primary vaccination. Boosters should be repeated every five years thereafter.
Children with HIV, if another indication for vaccination exists
Two doses of MCV4, three months apart
All others in this age group recommended for vaccination (travelers to the Meningitis Belt, etc)
Two doses of MCV4, three months apart (infants receiving the vaccine prior to travel can receive the doses as early as two months apart)
2 through 18 years of age, with high risk conditions
Children with complement deficiencies; functional or anatomic asplenia;
Two doses of MCV4, two months apart
Children with HIV, if another indication for vaccination exists
Two doses of MCV4, two months apart
All others in this age group recommended for vaccination (travelers to the Meningitis Belt, etc)
Single dose of MCV4
All other children 11-18 years of age
Routine vaccination with MCV4 at ages 11 through 12 years
If vaccinated at age 11 through 12 years, should receive a one-time booster dose at age 16 years If vaccinated at age 13 through 15 years, should receive a one-time booster dose at age 16 through 18 years
www.cdc.gov/vaccines/programs/vfc/downloads/.../06-11mening-mcv.pdf
Meningococcal Vaccine
Polysaccharide (MPSV4):
Menomune (Sanofi Pasteur)
A, C, Y, W-135 (B not included), 50 g each, SC
Children > 2 years at risk
– asplenia, complement deficiency, HIV (opt), outbreak, traveler to an endemic area
– In all cases MCV4 is prefered over MPSV4)

dTap
Booster
Adolescents (11-12 yr, 13-18 yr)
GlaxoSmithKline (Boostrix)Sanofi Pasteur (Adacel)
Special Situations
Prematurity (HBV)
Immune suppressed:self: MMR, VZVfamily contact: (OPV)
Pregnancy: MMR, VZV
Full doses
Multiple vaccines
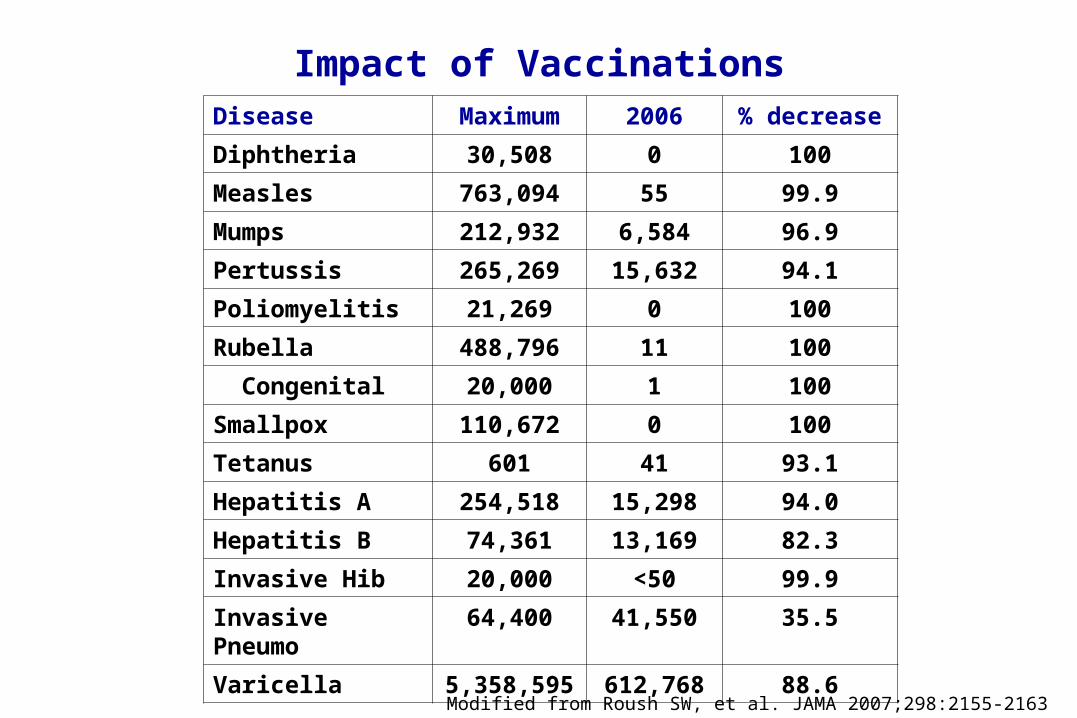
Impact of VaccinationsDisease Maximum 2006 % decrease
Diphtheria 30,508 0 100
Measles 763,094 55 99.9
Mumps 212,932 6,584 96.9
Pertussis 265,269 15,632 94.1
Poliomyelitis 21,269 0 100
Rubella 488,796 11 100
Congenital 20,000 1 100
Smallpox 110,672 0 100
Tetanus 601 41 93.1
Hepatitis A 254,518 15,298 94.0
Hepatitis B 74,361 13,169 82.3
Invasive Hib 20,000 <50 99.9
Invasive Pneumo 64,400 41,550 35.5
Varicella 5,358,595 612,768 88.6
Modified from Roush SW, et al. JAMA 2007;298:2155-2163

QUESTIONS?