Immunohistological analysis of peptide-induced delayed-type hypersensitivity in advanced melanoma patients treated with melanoma antigen-pulsed mature monocyte-derived dendritic cell vaccination Noriaki Nakai a, *, Norito Katoh a , Wilfred T.V. Germeraad b , Tsunao Kishida c , Eiichiro Ueda a , Hideya Takenaka a , Osam Mazda c , Saburo Kishimoto a a Department of Dermatology, Graduate School of Medical Science, Kyoto Prefectural University of Medicine, 465 Kajii-cho, Kawaramachi Hirokoji, Kamigyo-ku, Kyoto 602-8566, Japan b Department of Internal Medicine, Division of Haematology, University Hospital Maastricht, 6202 AZ Maastricht, The Netherlands c Department of Microbiology, Graduate School of Medical Science, Kyoto Prefectural University of Medicine, 465 Kajii-cho, Kawaramachi Hirokoji, Kamigyo-ku, Kyoto 602-8566, Japan 1. Introduction The incidence and mortality of malignant melanoma is steadily increasing among not only Caucasians, but also other populations including the Asian [1]. Surgical treatment is effective in early stage melanoma, but new strategies are required for patients with advanced melanoma that are highly resistant to conventional chemo- and radiation therapies. One of those new strategies is the active immunotherapy that has been developed in recent years but still needs many improvements. A very attractive option is the development of various vaccination strategies using autologous dendritic cells (DC). In these methods, dendritic cells (DC) are differentiated from peripheral blood monocytes, and after pulsing with tumor antigens, they are administered into patients with the aim to induce an active immune response [2–5]. In melanoma patients this procedure can lead to the induction of an anti-tumor effect [2,3,5] due to the proliferation and activation of melanoma-specific cytotoxic T cells. Potential disadvantages that have been reported may be the induction of tolerance caused by cytokines produced by regulatory T cells [4,6], loss of MHC class I expression [4,5,7] and mutations in or downregulation of tumor antigens [5]. Journal of Dermatological Science 53 (2009) 40–47 ARTICLE INFO Article history: Received 20 February 2008 Received in revised form 1 May 2008 Accepted 27 July 2008 Keywords: Immunohistological analysis Delayed-type hypersensitivity Melanoma Dendritic cell vaccination Melanoma antigen SUMMARY Background: In melanoma patients vaccinated with monocyte-derived melanoma peptide-pulsed dendritic cells (DC), the delayed-type hypersensitivity (DTH) reactions have been examined as a surrogate marker to determine if acquired immunity is induced by DC vaccination. To date, however, only limited information has been reported as for histopathological analyses of DTH. Objective: To evaluate tumor-specific immunomonitoring histopathologically after DC vaccination in melanoma patients. Methods: Seven patients previously vaccinated with monocyte-derived melanoma peptide-pulsed DCs were challenged with recall antigenic peptide injection in the skin of the forearm. Using immunohistochemical techniques, the presence of immune cells and the expression of CD4, CD8, interleukin (IL)-2, IL-4, IL-10, Foxp3, CD1a, CD1d, and interferon (IFN)-g was investigated at the site of injection where a DTH reaction developed. Results: Strong DTH reactions from infiltrated erythema to bullae formation were detected in all 7 cases. Biopsies taken from the DTH site revealed heavy infiltration of mononuclear cells and eosinophils in the dermis and subcutaneous tissue. Cells staining positively for CD4, CD8, IL-2, IL-4, Foxp3, CD1d, and IFN-g were increased at the site 48 h after antigen injection in all cases. Cells positive for IL-10 were never found in any patient. Regulatory T cells appeared 6 h after injection and reached their maximum at day 7. Conclusions: The significant induction of CD8 + T cells as well as both Th1 and Th2-type cells at the site of DTH suggests that effective antigen presentation leading to anti-tumor immune responses has taken place. Inhibitory mechanisms may also develop as the disappearance of the DTH response could be related to an increase in Foxp3+ cells. ß 2008 Japanese Society for Investigative Dermatology. Published by Elsevier Ireland Ltd. All rights reserved. * Corresponding author. Tel.: +81 75 251 5586; fax: +81 75 251 5586. E-mail address: [email protected](N. Nakai). Contents lists available at ScienceDirect Journal of Dermatological Science journal homepage: www.intl.elsevierhealth.com/journals/jods 0923-1811/$30.00 ß 2008 Japanese Society for Investigative Dermatology. Published by Elsevier Ireland Ltd. All rights reserved. doi:10.1016/j.jdermsci.2008.07.013
Transcript
Journal of Dermatological Science 53 (2009) 40–47
Immunohistological analysis of peptide-induced delayed-type hypersensitivityin advanced melanoma patients treated with melanoma antigen-pulsedmature monocyte-derived dendritic cell vaccination
Noriaki Nakai a,*, Norito Katoh a, Wilfred T.V. Germeraad b, Tsunao Kishida c, Eiichiro Ueda a,Hideya Takenaka a, Osam Mazda c, Saburo Kishimoto a
a Department of Dermatology, Graduate School of Medical Science, Kyoto Prefectural University of Medicine, 465 Kajii-cho, Kawaramachi Hirokoji, Kamigyo-ku,
Kyoto 602-8566, Japanb Department of Internal Medicine, Division of Haematology, University Hospital Maastricht, 6202 AZ Maastricht, The Netherlandsc Department of Microbiology, Graduate School of Medical Science, Kyoto Prefectural University of Medicine, 465 Kajii-cho, Kawaramachi Hirokoji, Kamigyo-ku,
Kyoto 602-8566, Japan
A R T I C L E I N F O
Article history:
Received 20 February 2008
Received in revised form 1 May 2008
Accepted 27 July 2008
Keywords:
Immunohistological analysis
Delayed-type hypersensitivity
Melanoma
Dendritic cell vaccination
Melanoma antigen
S U M M A R Y
Background: In melanoma patients vaccinated with monocyte-derived melanoma peptide-pulsed
dendritic cells (DC), the delayed-type hypersensitivity (DTH) reactions have been examined as a
surrogate marker to determine if acquired immunity is induced by DC vaccination. To date, however, only
limited information has been reported as for histopathological analyses of DTH.
Objective: To evaluate tumor-specific immunomonitoring histopathologically after DC vaccination in
melanoma patients.
Methods: Seven patients previously vaccinated with monocyte-derived melanoma peptide-pulsed DCs
were challenged with recall antigenic peptide injection in the skin of the forearm. Using
immunohistochemical techniques, the presence of immune cells and the expression of CD4, CD8,
interleukin (IL)-2, IL-4, IL-10, Foxp3, CD1a, CD1d, and interferon (IFN)-g was investigated at the site of
injection where a DTH reaction developed.
Results: Strong DTH reactions from infiltrated erythema to bullae formation were detected in all 7 cases.
Biopsies taken from the DTH site revealed heavy infiltration of mononuclear cells and eosinophils in the
dermis and subcutaneous tissue. Cells staining positively for CD4, CD8, IL-2, IL-4, Foxp3, CD1d, and IFN-gwere increased at the site 48 h after antigen injection in all cases. Cells positive for IL-10 were never found
in any patient. Regulatory T cells appeared 6 h after injection and reached their maximum at day 7.
Conclusions: The significant induction of CD8+T cells as well as both Th1 and Th2-type cells at the site of
DTH suggests that effective antigen presentation leading to anti-tumor immune responses has taken
place. Inhibitory mechanisms may also develop as the disappearance of the DTH response could be
related to an increase in Foxp3+ cells.
� 2008 Japanese Society for Investigative Dermatology. Published by Elsevier Ireland Ltd. All rights reserved.
Contents lists available at ScienceDirect
Journal of Dermatological Science
journa l homepage: www. int l .e lsev ierhea l th .com/ journa ls / jods
1. Introduction
The incidence and mortality of malignant melanoma issteadily increasing among not only Caucasians, but also otherpopulations including the Asian [1]. Surgical treatment iseffective in early stage melanoma, but new strategies are requiredfor patients with advanced melanoma that are highly resistant toconventional chemo- and radiation therapies. One of those newstrategies is the active immunotherapy that has been developed
0923-1811/$30.00 � 2008 Japanese Society for Investigative Dermatology. Published b
doi:10.1016/j.jdermsci.2008.07.013
in recent years but still needs many improvements. A veryattractive option is the development of various vaccinationstrategies using autologous dendritic cells (DC). In these methods,dendritic cells (DC) are differentiated from peripheral bloodmonocytes, and after pulsing with tumor antigens, they areadministered into patients with the aim to induce an activeimmune response [2–5]. In melanoma patients this procedure canlead to the induction of an anti-tumor effect [2,3,5] due to theproliferation and activation of melanoma-specific cytotoxic Tcells. Potential disadvantages that have been reported may be theinduction of tolerance caused by cytokines produced byregulatory T cells [4,6], loss of MHC class I expression [4,5,7]and mutations in or downregulation of tumor antigens [5].
N. Nakai et al. / Journal of Dermatological Science 53 (2009) 40–47 41
The in vivo response to treatment can be examined usingimaging to determine the shrinkage and disappearance ofmetastasis of the primary melanoma, while the in vitro evaluationof peripheral blood mononuclear cells (PBMCs) activity can beperformed in ELISPOT [5,8] and ELISA [8] assays. These assaysmeasure cytokine production of cells after proper tumor antigenpresentation by antigen presenting cells to T cells, like IFN-g, or therelease of granzymes by NK cells. Alternatively, a delayed-typehypersensitivity (DTH) test provides a simple approach to studythe in vivo immune response induced by DC vaccination [2,5,9,10].In melanoma patients, the DTH reaction has been examined as asurrogate marker to determine if acquired immunity is induced byDC vaccination loaded with melanoma antigens [2,5,9,10]. Theappearance of DTH reactions correlates with the clinical outcome[11–13], suggesting that evaluation of immune responses at thesite of the DTH is important for understanding the immunologicalmechanism. Some previous studies reported histopathologicalanalyses at sites of DTH following treatment with DC vaccines inmelanoma patients, showing strong perivascular infiltration ofCD4+ and/or CD8+ T cells [2,5,12,14]. Infiltration of Natural Killer(NK) cells and B cells has been looked at only once, but not found[12]. Furthermore information whether Th1 and/or Th2 responsesare predominantly activated and by which cytokines is extremelyimportant, but has never been reported to our knowledge. Ahistopathological assessment of infiltrating cells and cytokinesassociated with tumor immunity may allow tailoring the therapyregimen, including a determination of the therapeutic interval.
In this study, we performed a detailed analysis of DTH skinbiopsies from 7 melanoma patients with acquired immunity due totreatment with a melanoma antigen-pulsed DC vaccine. We alsohistologically examined the time course of the DTH during a weekand focused on the cellular infiltrate as well as cytokineproduction.
2. Patients and methods
2.1. Patients
Seven patients with stages III and IV melanoma were judged tobe eligible for this study. Entry criteria included age over 18-yearold, expression of HLA-A24 on PBMCs, and anticipated survival ofgreater than 3 months. The characteristics of the patients arelisted in Table 1. The study protocol was approved by theInstitutional Ethical Review Board of the Graduate School of
Table 1Characteristics of patients and status before DC vaccination, HLA type, DTH-related inform
Patient Age Sex History Site of
primary
skin tumor
Tumor
thickness
(mm)
Previous
therapya
Stage Site of
metastasis
H
1 61 M – Cheek >4.0 S + C IIIB LN A
2 51 M – Scalp Unknown S IIIB LN A
3 48 M – Forearm >4.0 C IV Lung, LN A
4 45 F – Scalp Unknown S + C IV Lung A
5 67 F – Face 1.7 S + C + T IV Lung,
adrenal
gland
A
6 54 F – Sole >4.0 S + C IV Lung,
bone, LN
A
7 56 F – Vulva 3.0 S + C IV Lung A
Mean follow-up period: 16.9 months; SD, stable disease; PD, progressive disease; NEDa S = Surgery; C = Chemotherapy; T = Thermo-chemotherapy.b This indicates the follow-up duration from the first DC vaccination to the patient’sc These patients had no evidence of disease from the time of entry into the study un
Medical Science, Kyoto Prefectural University of Medicine.Informed consent was obtained from the patients before entryinto the study.
2.2. Preparation of monocyte-derived peptide-pulsed DCs for
vaccination
Preparation of monocyte-derived peptide-pulsed DCs and thevaccination protocol have been described previously [5]. In short:monocytes were isolated from peripheral blood, differentiated toDCs with IL-4 and GM-CSF for 7 days followed by maturation withTNF-a and Poly (I:C) for 3 days. Mature DCs were coincubated witha cocktail of MAGE peptides for 6 h. Patients were vaccinated with10 � 106 cells per injection for 10 intradermal injections everyweek or every other week in the groin.
2.3. Evaluation of clinical outcome
The clinical outcome was evaluated based on analysis of wholebody CT images before and after one course of treatment (10vaccinations).
2.4. DTH response
Patients received intradermal injections of 10 mg of a HLA-A24specific melanoma peptide (MAGE-2.156(9); Takara, Otsu, Japan)in 200 ml of PBS or of PBS only (as a control) at separate sites on theforearm. Forty-eight hours later, the DTH was assessed bydetermining the area of erythema and induration using two-dimensional measurements. In patient 1, an assessment of the timecourse of the DTH reaction was performed using measurements at6, 24, 48, and 168 h after application. The DTH response wasconsidered to be positive if the area of erythema and indurationwas greater than 10 mm.
2.5. Histology and immunohistochemistry
Punch biopsies of the skin at the DTH and control sites wereperformed 48 h after injection of MAGE-2 and PBS, respectively.Formaldehyde-fixed, paraffin-embedded specimens were stainedwith hematoxylin and eosin or immunostained with antibodiesagainst CD4 (4B12, Novocastra Laboratories Ltd., Newcastle uponTyne, UK), CD8 (1A5, Novocastra, USA), IFN-g (n/a, Biogenesis Ltd.Oxford, UK), IL-10 (23738, DakoCytomation Co. Ltd. Kyoto, Japan),
ation, and clinical outcome evaluated after 1 treatment course (10 DC vaccinations)
LA-A allotype Antigen pulsed to DC Clinical
outcome
Total no of
vaccines
Survival
periodb
(months)MAGE-1, 2, 3
+ tyrosinase
peptides
MART-1
peptide
+ tumor lysate
2, A24 + + NEDc 76 44
2, A24 + � NEDc 68 36
3, A24 + � PD 14 5
2, A24 + � PD 37 16
11, A24 + � SD 16 9
2, A24 + + PD 15 5
2, A24 + � PD 37 15
, no evidence of disease; LN, lymph nodes.
death.
til completion of one course of treatment (10 vaccinations).
N. Nakai et al. / Journal of Dermatological Science 53 (2009) 40–4742
CD1a (MTB1, Novocastra, USA), and CD1d (NOR3.2, Serotec Ltd.,Oxford, UK), while specimens frozen in liquid nitrogen wereimmunostained with antibodies against IL-2 (ANC7F7, AncellCorporation, Bayport, MN, USA), IL-4 (4D9, Ancell), and Foxp3(236A/E7, eBioscience Inc., San Diego, CA, USA). The details aboutthe concentration or dilution and the incubation time andtemperature for each of the primary antibodies were indicatedas follows: CD4, CD8, and CD1a: 1:30, 60 min at 25 8C; IFN-g:1:300, overnight at 4 8C; CD1d: 1:200, overnight at 4 8C; IL-2, IL-4,IL-10, and Foxp3: 5.0 mg/ml, overnight at 4 8C. All antibodies werebiotin labeled and detected with the HRP–avidin–biotin complexmethod, in each case according to the manufacturer’s protocol.Positive controls were also stained, respectively, according to themanufacturer’s protocol and were evaluated correctly. Positivelystained cells were counted in ten high-power fields (�400)independently by two observers and the mean value wasdetermined [15].
2.6. Statistical analysis
Statistical comparisons were performed using Student t-tests.
3. Results
3.1. Patients’ results
Seven patients with advanced malignant melanoma wereenrolled into our study. Two patients had stage IIIB disease, whilethe others had stage IV disease (Table 1). All patients received oneor more courses of treatments. By completion of one vaccinecourse, one case showed stable disease, four cases showedprogression of disease, and two cases became disease-free. Twostage IIIB patients survived more than 35 months. The mediansurvival period of two stage IV patients with only lung metastaseswas 15.5 months, indicating that they survived longer than thepatients treated by conventional therapies alone (8 months).Median survival period of three stage IV patients with metastasesin lungs and other organs was 6.3 months.
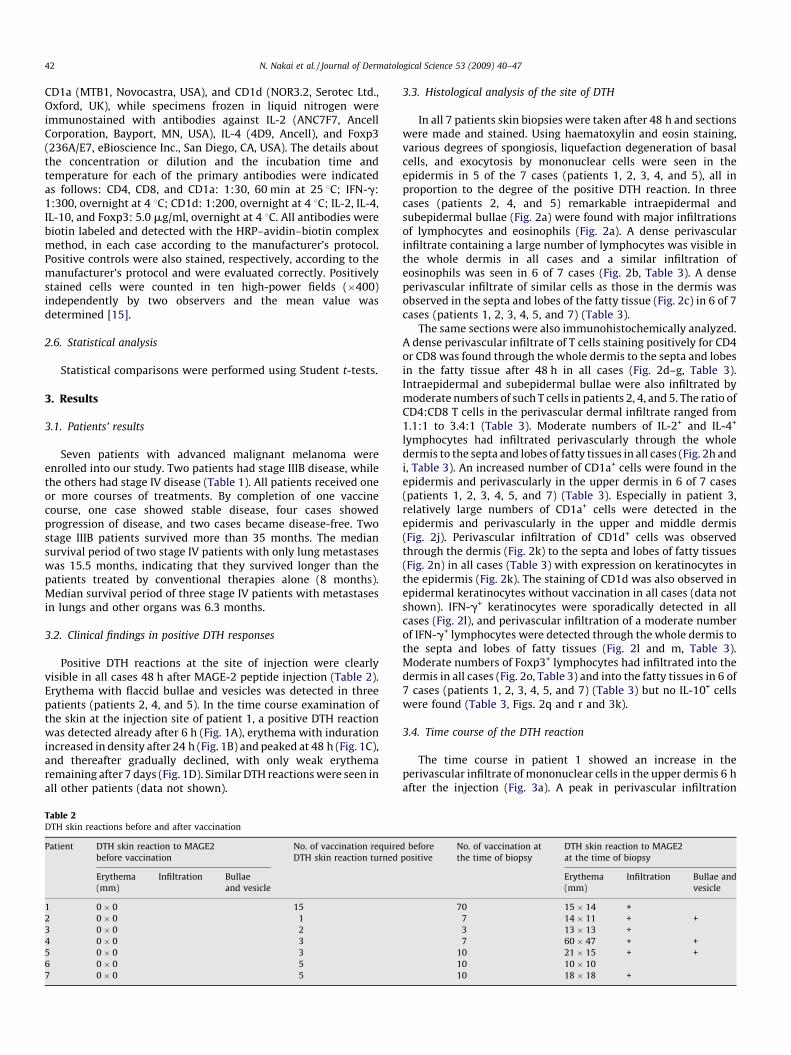
3.2. Clinical findings in positive DTH responses
Positive DTH reactions at the site of injection were clearlyvisible in all cases 48 h after MAGE-2 peptide injection (Table 2).Erythema with flaccid bullae and vesicles was detected in threepatients (patients 2, 4, and 5). In the time course examination ofthe skin at the injection site of patient 1, a positive DTH reactionwas detected already after 6 h (Fig. 1A), erythema with indurationincreased in density after 24 h (Fig. 1B) and peaked at 48 h (Fig. 1C),and thereafter gradually declined, with only weak erythemaremaining after 7 days (Fig. 1D). Similar DTH reactions were seen inall other patients (data not shown).
Table 2DTH skin reactions before and after vaccination
Patient DTH skin reaction to MAGE2
before vaccination
No. of vaccination require
DTH skin reaction turned
Erythema
(mm)
Infiltration Bullae
and vesicle
1 0 � 0 � � 15
2 0 � 0 � � 1
3 0 � 0 � � 2
4 0 � 0 � � 3
5 0 � 0 � � 3
6 0 � 0 � � 5
7 0 � 0 � � 5
3.3. Histological analysis of the site of DTH
In all 7 patients skin biopsies were taken after 48 h and sectionswere made and stained. Using haematoxylin and eosin staining,various degrees of spongiosis, liquefaction degeneration of basalcells, and exocytosis by mononuclear cells were seen in theepidermis in 5 of the 7 cases (patients 1, 2, 3, 4, and 5), all inproportion to the degree of the positive DTH reaction. In threecases (patients 2, 4, and 5) remarkable intraepidermal andsubepidermal bullae (Fig. 2a) were found with major infiltrationsof lymphocytes and eosinophils (Fig. 2a). A dense perivascularinfiltrate containing a large number of lymphocytes was visible inthe whole dermis in all cases and a similar infiltration ofeosinophils was seen in 6 of 7 cases (Fig. 2b, Table 3). A denseperivascular infiltrate of similar cells as those in the dermis wasobserved in the septa and lobes of the fatty tissue (Fig. 2c) in 6 of 7cases (patients 1, 2, 3, 4, 5, and 7) (Table 3).
The same sections were also immunohistochemically analyzed.A dense perivascular infiltrate of T cells staining positively for CD4or CD8 was found through the whole dermis to the septa and lobesin the fatty tissue after 48 h in all cases (Fig. 2d–g, Table 3).Intraepidermal and subepidermal bullae were also infiltrated bymoderate numbers of such T cells in patients 2, 4, and 5. The ratio ofCD4:CD8 T cells in the perivascular dermal infiltrate ranged from1.1:1 to 3.4:1 (Table 3). Moderate numbers of IL-2+ and IL-4+
lymphocytes had infiltrated perivascularly through the wholedermis to the septa and lobes of fatty tissues in all cases (Fig. 2h andi, Table 3). An increased number of CD1a+ cells were found in theepidermis and perivascularly in the upper dermis in 6 of 7 cases(patients 1, 2, 3, 4, 5, and 7) (Table 3). Especially in patient 3,relatively large numbers of CD1a+ cells were detected in theepidermis and perivascularly in the upper and middle dermis(Fig. 2j). Perivascular infiltration of CD1d+ cells was observedthrough the dermis (Fig. 2k) to the septa and lobes of fatty tissues(Fig. 2n) in all cases (Table 3) with expression on keratinocytes inthe epidermis (Fig. 2k). The staining of CD1d was also observed inepidermal keratinocytes without vaccination in all cases (data notshown). IFN-g+ keratinocytes were sporadically detected in allcases (Fig. 2l), and perivascular infiltration of a moderate numberof IFN-g+ lymphocytes were detected through the whole dermis tothe septa and lobes of fatty tissues (Fig. 2l and m, Table 3).Moderate numbers of Foxp3+ lymphocytes had infiltrated into thedermis in all cases (Fig. 2o, Table 3) and into the fatty tissues in 6 of7 cases (patients 1, 2, 3, 4, 5, and 7) (Table 3) but no IL-10+ cellswere found (Table 3, Figs. 2q and r and 3k).
3.4. Time course of the DTH reaction
The time course in patient 1 showed an increase in theperivascular infiltrate of mononuclear cells in the upper dermis 6 hafter the injection (Fig. 3a). A peak in perivascular infiltration
d before
positive
No. of vaccination at
the time of biopsy
DTH skin reaction to MAGE2
at the time of biopsy
Erythema
(mm)
Infiltration Bullae and
vesicle
70 15 � 14 + �7 14 � 11 + +
3 13 � 13 + �7 60 � 47 + +
10 21 � 15 + +
10 10 � 10 � �10 18 � 18 + �
Fig. 1. Observation of DTH on the forearm at different times after intradermal injection of MAGE-2 peptide in patient 1: (A), 6 h; (B), 24 h; (C), 48 h; (D), 7 days after MAGE-2
injection; scale = 1.0 cm.
N. Nakai et al. / Journal of Dermatological Science 53 (2009) 40–47 43
through the whole dermis into the septa and lobes of fatty tissuesoccurred after 48 h (P < 0.0005 for mononuclear cells after 48 h,antigen (+) vs. antigen (�)) (Fig. 3a). Thereafter, infiltration ofmononuclear cells gradually decreased, but was still detectableafter 7 days (Fig. 3a). Interestingly, no infiltrate of eosinophils wasfound after 6 h (Fig. 3b); however, increased perivascularinfiltration of eosinophils in the dermis and in the septa andlobes of fatty tissues was detected after 24 h (P < 0.05, antigen (+)after 24 h vs. antigen (+) after 6 h) (Fig. 3b) and a peak occurredafter 7 days (P < 0.0005, antigen (+) after 7 days vs. antigen (+) after6 h) (Fig. 3b). In this patient, CD4+ and CD8+ T cells first appearedperivascularly in the upper dermis after 6 h (Fig. 3c and d). Thenumber of CD4+ and CD8+ T cells increased and reached a peakafter 48 h (P < 0.0005 for CD4+ T cells after 48 h, antigen (+) vs.antigen (�); P < 0.0005 for CD8+ T cells after 48 h, antigen (+) vs.antigen (�)) (Fig. 3c and d), before declining until day 7 (Fig. 3c andd). Cells staining positively for IL-2 and IL-4 were first observedperivascularly in the upper dermis after 6 h (Fig. 3e and f);thereafter, these cells increased in number and were still present inhigh amounts on 7 day (P < 0.0005 for IL-2+ after 48 h, antigen (+)vs. antigen (�); P < 0.005 for IL-4+ cells after 48 h, antigen (+) vs.antigen (�)) (Fig. 3e and f). An increased infiltration of CD1a+ cellsin the epidermis and upper dermis was first seen after 6 h and highnumbers of these cells were still present on day 7 (P < 0.05 forCD1a+ cells after 48 h, antigen (+) vs. antigen (�)) (Fig. 3g). An in-and efflux of CD1d+ cells was detected perivascularly through thewhole dermis to the septa and lobes of the fatty tissues over time:CD1d+ cells reached a peak after 48 h (P < 0.005 for CD1d+ cellsafter 48 h, antigen (+) vs. antigen (�)) (Fig. 3h) and then declineduntil day 7 (Fig. 3h). IFN-g+ cells were first seen perivascularly inthe upper dermis after 6 h (Fig. 3i); thereafter, these cells increasedacross the whole dermis to the septa and lobes of fatty tissues andreached a peak at 48 h (P < 0.0001 for IFN-g+ cells after 48 h,antigen (+) vs. antigen (�)) (Fig. 3i) and then declined until day 7(Fig. 3i) (P < 0.05 for IFN- g+ cells, antigen (+) after 7 days vs.antigen (+) after 48 h). Foxp3+ lymphocytes first appeared
perivascularly in the upper dermis after 6 h (Fig. 3j); thereafter,the numbers increased and Foxp3+ cells were still present in largeamounts on day 7 (P < 0.001 for Foxp3+ cells after 48 h, antigen (+)vs. antigen (�)) (Figs. 2p and 3j). Again, never during the DTHreaction, IL-10+ cells were found (Figs. 2r and 3k).
4. Discussion
In the current study we analyzed the development of a DTHresponse in the skin against a tumor associated antigen with which7 melanoma patients had previously been vaccinated using adendritic cell vaccine to investigate the local immune response.
DTH is often used as surrogate readout system in phase I/II trialsfor immune responses induced by DC vaccines given to cancerpatients. DTH is divided into the classical DTH and an allergen-induced DTH. The classical DTH was originally used for thediagnosis of tuberculosis [16,17] in which a purified proteinderivative (PPD) from cultures of M. bovis or M. avium was injectedin the skin of a suspected patient. This process was shownimmunologically to be a similar process as typical cell-mediatedimmunity, involving Th1 cells and Th1 cytokines. On the otherhand, the allergen-induced DTH is also referred to as an allergen-induced late phase skin reaction (LPR) [18–20] and occurs in atopicpatients. Although accumulation of evidence shows that LPR is aprocess similar to that of the classical DTH, in the clinicalappearance of the DTH and LPR at the site of antigen injection,some differences have been reported [19,20]. DTH results inerythema with strong induration, whereas the LPR is associatedwith erythema with edema and slight induration. Furthermore, thepeak of the reaction following antigen injection is seen 6–10 h inthe LPR, whereas this is at 24–48 h in DTH. Finally, anaccumulation of predominantly CD4+ T cells occurs at both DTHand LPR sites, but the infiltrate is denser and more dispersed inDTH [19,20].
In the present study, increased numbers of cells stainingpositively for CD4, CD8, IL-2, IL-4 and IFN-g+ were observed during
Fig. 2. Hematoxylin/eosin and immunohistochemical staining of skin biopsies taken from sites of DTH 48 h or 7 days after intradermal MAGE-2 injection. (a) Marked
intraepidermal and subepidermal bullae were seen with considerable infiltration of lymphocytes and eosinophils after 48 h (patient 4, �400, H&E). (b and c) A dense
perivascular infiltrate of a large number of lymphocytes and eosinophils was seen in the whole dermis (b) and in the septa and lobes of fatty tissues (c) after 48 h (patient 1,
�200, H&E). (d–g) A dense perivascular infiltrate of cells staining for CD4 (d and e) or CD8 (f and g) was found through the dermis to the septa and lobes of fatty tissues after
48 h (patient 1, �200, CD4, dermis (d) and subcutis (e); CD8, dermis (f) and subcutis (g)). (h and i) Moderate numbers of IL-2+ (h) and IL-4+ (i) lymphocytes had infiltrated
perivascularly through the whole dermis after 7 days (patient 1,�200). (j) Relatively large numbers of CD1a+ cells were detected in the epidermis, as well as perivascularly, in
the upper and middle dermis after 48 h (patient 3, �200). (k and n) Perivascular infiltration of CD1d+ cells increased through the dermis (k) to the septa and lobes of fatty
tissues (n) with expression on keratinocytes in the epidermis (k) after 48 h (patient 1, �200). (l and m) A moderate number of IFN-g+ lymphocytes with perivascular
infiltration were detected through the whole dermis (l) to the septa and lobes of fatty tissues (m) after 48 h (patient 1, �200). (o) Moderate numbers of Foxp3+ lymphocytes
had infiltrated into the dermis after 48 h (o) and increased with time until day 7 (p) (patient 1, �400). (q) No IL-10+ cells were found at any time (dermis, after 48 h (q) and 7
days (r), patient 1, �400). (s) A control normal lymph node (�400, IL-10).
N. Nakai et al. / Journal of Dermatological Science 53 (2009) 40–4744
Table 3Summary of data for the DTH response 48 h after intradermal injection of MAGE-2 peptide
Positively stained cells were counted in ten high-power fields (�400) independently by two observers and the mean value is shown. The ++, + and � symbols indicate a two-
fold increase, a one- to two-fold increase, and a less than one-fold increase, respectively, in cell numbers at the DTH site, compared to a control site receiving a PBS injection.
ND, not done.
N. Nakai et al. / Journal of Dermatological Science 53 (2009) 40–47 45
the DTH reaction. The number of CD4+, CD8+ and IFN-g+ cellspeaked at 48 h, whereas IL-2+ and IL-4+ cells increased con-tinuously over 7 days. We have previously shown an increase inpeptide-specific IFN-g-producing T cells among peripheral bloodmononuclear cells in the same patients as are examined in thisstudy, using an ELISPOT assay [5]. These findings strongly suggestthat the reaction may be predominantly mediated throughclassical DTH rather than LPR, which is consistent with the factthat none of the patients had a history of atopic diathesis.Moreover, the T cell kinetics and intensity, as well as the clinicalappearance and peak of reaction also resemble those of a classicalDTH than LPR [19,20].
Although the presence of IL-4+ cells at the DTH site is anintriguing finding suggesting that a Th2-like response may also beinvolved in the tumor antigen-specific immune response, it hasalso been reported that IL-4 may promote Th1 anti-tumor immuneresponses together with IFN-a by attracting granulocytes [21].Either way, induction should have occurred in vivo by the DCvaccine.
The ratio of CD4+:CD8+ infiltrating cells in the dermis wasapproximately 1:1 to 3:1, similar to the ratios found for classicalDTH reactions [22–24], LPR [19], and in lymph nodes andperipheral blood of humans [25]. The results are consistent withthe findings of De Vries et al. [26] and Nestle et al. [2], rather thanthose of Bedrosian et al. [14] who reported minimal infiltration ofCD4+ cells. This discrepancy may be due to differences in theprotocols of DC induction, antigen pulsation, and/or vaccination.
CD1a and CD1d are the main markers for Langerhans cells anddermal DCs, respectively [27]. We detected an increase in the
numbers of these cells, which strongly suggests that Langerhanscells and dermal DCs proliferated and/or accumulated at the DTHsite. It is well known that the CD1-mediated interaction between aDC and a Natural Killer T (NKT) cell can provoke NKT cells toproduce IFN-g and IL-4, which can subsequently contribute to theactivation of immature DCs, NK cells, and T cells [28]; in fact, asignificant infiltrate including IL-4+ and IFN-g+ cells was observedin our study.
A dense perivascular influx of eosinophils was detected in 6 of 7cases, which is not widely considered as a typical feature ofconventional DTH, as accumulation of eosinophils is morefrequently seen at sites of LPR than DTH [19]. As a possiblesuggestion, eosinophils may also influence cytokine production byDCs and T cells and thus promoting anti-tumor immunity.Although eosinophils are pivotal effector cells in allergies suchas asthma and atopic dermatitis, they also may play a role ingeneral inflammation, including anti-tumor immunity, due to theirproduction of inflammatory proteins such as major basic protein(MBP), eosinophil-derived neurotoxin (EDN), and eosinophilcationic protein (ECP). Especially EDN affects the function ofDCs and may thereby modulate tumor immunology. EDN convertsimmature DCs to mature DCs allowing production of IL-6, IL-12and TNF-a [29] and causes DC to migrate to the regional lymphnodes [30]. Eosinophils themselves also produce Th1 cytokinesincluding IL-12 [31], IL-2 [32] and IFN-g [32] as well as Th2cytokines such as IL-4 and IL-13 [33,34]. Other cytokines producedby eosinophils include IL-3 and GM-CSF that may act oneosinophils in autocrine manners [35]. For all these reasons,eosinophils may regulate DC-T interactions and subsequent T cell-
Fig. 3. Numbers of mononuclear cells (a), eosinophils (b) and cells staining for CD4 (c), CD8 (d), IL-2 (e), IL-4 (f), CD1a (g), CD1d (h), IFN-g (i), Foxp3 (j), and IL-10 (k) expressed
as means � S.D. measured over ten high-power fields (400�) in the dermis at various times after intradermal injection of MAGE-2 peptide in patient 1. The counting was performed
independently by two observers. A skin biopsy taken from a site of PBS injection 48 h after the injection is shown as a control.
N. Nakai et al. / Journal of Dermatological Science 53 (2009) 40–4746
mediated responses. Actually, six of 6 evaluable cases exceptpatient 6 also showed increase of eosinophils in blood temporarilywhen DTH expressed positive (data not shown). However, the ratiowas normalized in a short time in spite of continuation of DCvaccination.
Enhanced cell aggregation and production of cytokines suggestthat the anti-tumor immune response against the melanoma witha single course of DC vaccination containing a single peptideepitope can last for at least 7 days in vivo. However, the prognosisdiffered among patients with a positive DTH reaction, as shown inTable 1. This result may be due to differences in the degree of theDTH reaction, particularly, the differences in the degree of activity
of Th1 and Th2 cells that work for inducing an anti-tumorimmunity and regulatory T cells that work for restricting an anti-tumor immunity, the expression level of this particular epitope onthe tumor, and thus the sensitivity, in the levels of cytokinesrelated to tolerance, such as TGF-b [4,36–38], and finally also totumor escape phenomena caused by loss of MHC class I [4,5,9,39]and mutations in or downregulation of tumor antigens [5]. In ourpatients only moderate clinical responses were measured. One ofthe mechanisms might be a limited and short-lived immunologicalactivity that can be visualized by the downmodulation of the DTHreaction due to the time-dependent increase in Foxp3+ (Treg) cellsover 7 days despite the absence of IL-10+ cells. Already many years
N. Nakai et al. / Journal of Dermatological Science 53 (2009) 40–47 47
ago it was shown that DTH responses could be upregulated andlonger lasting by adding cyclophosphamide analogues that weresupposed to eliminate some cells with immunosuppressiveactivities [40], cells that we now call Treg. The use of lowconcentrations of such drugs to limit the effects of Tregs couldenhance the effects of DC vaccines, which is worthwhileinvestigating. Alternatively, co-administration of IL-6 may alsoelevate anti-tumor efficacy of DC vaccine, because IL-6 suppressesTreg induction by TGF-b while promoting generation of Th17 incombination of TGF-b [41].
In conclusion, a DTH examination to assess the time course ofantigen expression on immunocytes after DC vaccination increasesthe understanding of the immunological anti-tumor response invivo. The present study suggests that this method is safe for thepatients, non time consuming, and potentially offers valuableindicators to estimate the outcome of each new variable, like doseof peptide, vaccine cell number, interval and number of inocula-tions, in the vaccine regimen. Based on our results, strengtheningof antigen-specific anti-tumor immunity and analysis of tumormechanism(s) of immunological regulatory functions are requiredto improve the efficacy of DC vaccination.
Acknowledgment
This work was supported in part by a Grant-in-Aid for CancerResearch from the Ministry of Health, Labour and Welfare.
References
[1] Ishihara K, Saida T, Yamamoto A, Otsuka F. Nationwide survey of malignantskin tumors (1997–2001). Skin Cancer (Japan) 2004;19:147–55.
[2] Nestle FO, Alijagic S, Gilliet M, Sun Y, Grabbe S, Dummer R, et al. Vaccination ofmelanoma patients with peptide- or tumor lysate-pulsed dendritic cells. NatMed 1998;4:328–32.
[3] Morisaki T, Matsumoto K, Onishi H, Kuroki H, Baba E, Tasaki A, et al. Dendriticcell-based combined immunotherapy with autologous tumor-pulsed dendri-tic cell vaccine and activated T cells for cancer patients: rationale, currentprogress, and perspectives. Hum Cell 2003;16:175–82.
[4] Mazda O, Germeraad WTV. Tumor immunity and immuno-gene therapy ofmalignancies. In: Mazda O, editor. Frontiers in immuno-gene therapy. Tri-vandrum: Research Signpost; 2004. p. 1–30.
[5] Nakai N, Asai J, Ueda E, Takenaka H, Katoh N, Kishimoto S. Vaccination ofJapanese patients with advanced melanoma with peptide, tumor lysate or bothpeptide and tumor lysate-pulsed mature, monocyte-derived dendritic cells. JDermatol 2006;33:462–72.
[6] Chakraborty NG, Chattopadhyay S, Mehrotra S, Chhabra A, Mukherji B. Reg-ulatory T-cell response and tumor vaccine-induced cytotoxic T lymphocytes inhuman melanoma. Hum Immunol 2004;65:794–802.
[7] Berger TG, Haendle I, Schrama D, Luftl M, Bauer N, Pedersen LO, et al.Circulation and homing of melanoma-reactive T cells to both cutaneousand visceral metastases after vaccination with monocyte-derived dendriticcells. Int J Cancer 2004;111:229–37.
[8] Shu S, Cochran AJ, Huang RR, Morton DL, Maecker HT. Immune responses in thedraining lymph nodes against cancer: implications for immunotherapy. Can-cer Metastasis Rev 2006;25:233–42.
[9] Jager E, Jager D, Knuth A. CTL-defined cancer vaccines: perspectives for activeimmunotherapeutic interventions in minimal residual disease. Cancer Metas-tasis Rev 1999;18:143–50.
[10] Jager D, Jager E, Knuth A. Vaccination for malignant melanoma: recentdevelopments. Oncology 2001;60:1–7.
[11] Jager D, Jager E, Knuth A. Immune responses to tumour antigens: implica-tions for antigen specific immunotherapy of cancer. J Clin Pathol2001;54:669–74.
[12] de Vries IJ, Bernsen MR, Lesterhuis WJ, Scharenborg NM, Strijk SP, GerritsenMJ, et al. Immunomonitoring tumor-specific T cells in delayed-type hyper-sensitivity skin biopsies after dendritic cell vaccination correlates with clinicaloutcome. J Clin Oncol 2005;23:5779–87.
[13] van den Eertwegh AJ. Active specific immunotherapy in colon cancer. RecentResults Cancer Res 2005;165:260–7.
[14] Bedrosian I, Mick R, Xu S, Nisenbaum H, Faries M, Zhang P, et al. Intranodaladministration of peptide-pulsed mature dendritic cell vaccines results insuperior CD8+ T-cell function in melanoma patients. J Clin Oncol 2003;21:3826–35.
[15] Roosje PJ, van Kooten PJ, Thepen T, Bihari IC, Rutten VP, Koeman JP, et al.Increased numbers of CD4+ and CD8+ T cells in lesional skin of cats withallergic dermatitis. Vet Pathol 1998;35:268–73.
[16] Dannenberg Jr AM. Roles of cytotoxic delayed-type hypersensitivity andmacrophage-activating cell-mediated immunity in the pathogenesis of tuber-culosis. Immunobiology 1994;191:461–73.
[17] Adams LG. In vivo and in vitro diagnosis of Mycobacterium bovis infection. RevSci Tech 2001;20:304–24.
[18] Frew AJ, Varney VA, Gaga M, Kay AB. Immunohistology of human allergic late-phase skin reactions. Skin Pharmacol 1991;4(Suppl. 1):71–8.
[19] Gaga M, Frew AJ, Varney VA, Kay AB. Eosinophil activation and T lymphocyteinfiltration in allergen-induced late phase skin reactions and classical delayed-type hypersensitivity. J Immunol 1991;147:816–22.
[20] Tsicopoulos A, Fahy O, Tonnel AB. Delayed-type hypersensitivity reactions tonominal protein antigens and to environmental allergens: similarities anddifferences. Eur J Dermatol 1999;9:261–8.
[21] Eguchi J, Hiroishi K, Ishii S, Baba T, Matsumura T, Hiraide A, et al. Interleukin-4gene transduced tumor cells promote a potent tumor-specific Th1-typeresponse in cooperation with interferon-alpha transduction. Gene Ther2005;12:733–41.
[22] Poulter LW, Seymour GJ, Duke O, Janossy G, Panayi G. Immunohistologicalanalysis of delayed-type hypersensitivity in man. Cell Immunol 1982;74:358–69.
[23] Platt JL, Grant BW, Eddy AA, Michael AF. Immune cell populations in cutaneousdelayed-type hypersensitivity. J Exp Med 1983;158:1227–42.
[24] Chu CQ, Field M, Andrew E, Haskard D, Feldmann M, Maini RN. Detection ofcytokines at the site of tuberculin-induced delayed-type hypersensitivity inman. Clin Exp Immunol 1992;90:522–9.
[25] Janossy G, Panayi G, Duke O, Bofill M, Poulter LW, Goldstein G. Rheumatoidarthritis: a disease of T-lymphocyte/macrophage immunoregulation. Lancet1981;2:839–42.
[26] De Vries IJ, Bernsen MR, van Geloof WL, Scharenborg NM, Lesterhuis WJ,Rombout PD, et al. In situ detection of antigen-specific T cells in cryo-sectionsusing MHC class I tetramers after dendritic cell vaccination of melanomapatients. Cancer Immunol Immunother 2007.
[27] Gerlini G, Hefti HP, Kleinhans M, Nickoloff BJ, Burg G, Nestle FO. Cd1d isexpressed on dermal dendritic cells and monocyte-derived dendritic cells. JInvest Dermatol 2001;117:576–82.
[28] Seino K, Motohashi S, Fujisawa T, Nakayama T, Taniguchi M. Natural killer Tcell-mediated antitumor immune responses and their clinical applications.Cancer Sci 2006;97:807–12.
[29] Yang D, Chen Q, Rosenberg HF, Rybak SM, Newton DL, Wang ZY, et al. Humanribonuclease A superfamily members, eosinophil-derived neurotoxin andpancreatic ribonuclease, induce dendritic cell maturation and activation. JImmunol 2004;173:6134–42.
[30] Yang D, Rosenberg HF, Chen Q, Dyer KD, Kurosaka K, Oppenheim JJ. Eosinophil-derived neurotoxin (EDN), an antimicrobial protein with chemotactic activ-ities for dendritic cells. Blood 2003;102:3396–403.
[31] Grewe M, Czech W, Morita A, Werfel T, Klammer M, Kapp A, et al. Humaneosinophils produce biologically active IL-12: implications for control of T cellresponses. J Immunol 1998;161:415–20.
[32] Woerly G, Roger N, Loiseau S, Dombrowicz D, Capron A, Capron M. Expressionof CD28 and CD86 by human eosinophils and role in the secretion of type 1cytokines (interleukin 2 and interferon gamma): inhibition by immunoglo-bulin a complexes. J Exp Med 1999;190:487–95.
[33] Bandeira-Melo C, Sugiyama K, Woods LJ, Phoofolo M, Center DM, CruikshankWW, et al. IL-16 promotes leukotriene C(4) and IL-4 release from humaneosinophils via CD4- and autocrine CCR3-chemokine-mediated signaling. JImmunol 2002;168:4756–63.
[34] Gessner A, Mohrs K, Mohrs M. Mast cells, basophils, and eosinophils acquireconstitutive IL-4 and IL-13 transcripts during lineage differentiation that aresufficient for rapid cytokine production. J Immunol 2005;174:1063–72.
[35] Kita H, Ohnishi T, Okubo Y, Weiler D, Abrams JS, Gleich GJ. Granulocyte/macrophage colony-stimulating factor and interleukin 3 release from humanperipheral blood eosinophils and neutrophils. J Exp Med 1991;174:745–8.
[36] Shurin MR, Lu L, Kalinski P, Stewart-Akers AM, Lotze MT. Th1/Th2 balance incancer, transplantation and pregnancy. Springer Semin Immunopathol1999;21:339–59.
[37] Ronger-Savle S, Valladeau J, Claudy A, Schmitt D, Peguet-Navarro J, Dezutter-Dambuyant C, et al. TGFbeta inhibits CD1d expression on dendritic cells. JInvest Dermatol 2005;124:116–8.
[38] Zou W, Regulatory. T cells, tumour immunity and immunotherapy. Nat RevImmunol 2006;6:295–307.
[39] Kageshita T, Wang Z, Calorini L, Yoshii A, Kimura T, Ono T, et al. Selective loss ofhuman leukocyte class I allospecificities and staining of melanoma cells bymonoclonal antibodies recognizing monomorphic determinants of class Ihuman leukocyte antigens. Cancer Res 1993;53:3349–54.
[40] Limpens J, Garssen J, Germeraad WT, Scheper RJ. Enhancing effects of locallyadministered cytostatic drugs on T effector cell functions in mice. Int JImmunopharmacol 1990;12:77–88.
[41] Bettelli E, Carrier Y, Gao W, Korn T, Strom TB, Oukka M, et al. Reciprocaldevelopmental pathways for the generation of pathogenic effector TH17 andregulatory T cells. Nature 2006;441:235–8.