The last decade has witnessed the rise of new biologicaltreatments for cancer based on stimulating natural immunereactions against the disease. These treatments, collectivelyreferred to as biological therapy, are beginning to join surgery,radiation therapy, and chemotherapy as effective means fortreating cancer (1, 2). Biological therapy can be denned ascancer treatments that act primarily through natural host defense mechanisms or by the administration of natural mammalian substances. An increased understanding of the cellularimmune system as well as new developments in biotechnologyhave made new approaches to biological therapy feasible. Usingrecombinant DNA technology, many biological compoundshave become available in large amounts for the first time.
In the past decade, however, several cell types have beenidentified that can cause the regression of cancer in somepatients. We began our work in this field with the descriptionof LAK cells which were non-MHC-restricted killer cells capable of lysing fresh tumor but not fresh normal cells in culture.These studies led us to the description of more specific antitu-
mor cells called TIL that were capable of recognizing uniqueantigens on tumor cells. More recently we have begun geneticmodification of these TIL in an attempt to increase theirantitumor reactivity.
1Presented at the Symposium. "Discoveries and Opportunities in CancerResearch: A Celebration of the 50th Anniversary of the Journal Cancer Research,"
May 15, 1991. during the 82nd Annual Meeting of the American Association forCancer Research. Houston, TX.
'The abbreviations used are: LAK, lymphokine-activated killer; MHC, majorhistocompatibility complex; TIL, tumor-infiltrating lymphocytes; IL-2. interleu-kin 2; TNF, tumor necrosis factor.
hormone, originally called T-cell growth factor, which wascapable of causing the growth in culture of T-lymphocytesactivated either by specific antigen or by lectins. This growthfactor, subsequently renamed IL-2, opened new possibilities forexpanding T-lymphocytes with antitumor activity for use inadoptive immunotherapy. In studies attempting to isolate T-cells from growing tumors we noted that lymphocytes exposedto IL-2 developed the ability to kill fresh tumor cells but notfresh normal cells in 4-h chromium release assays (3,4). Furtherstudies revealed that lymphocytes from tumor-bearing as wellas normal hosts in both the mouse and the human developedthis lymphokine-activated killing activity for fresh cancer cells.In vitro these LAK cells showed ubiquitous non-MHC-re
stricted killing of target cells altered either by malignant transformation or by growth in culture.
Our first studies of the in vivo administration of IL-2-de-
pendent cells were performed in three patients with advancedsarcomas who received cells labeled with either MCr or '"In to
monitor their in vivo distribution (4). It was found that theseadoptively transferred IL-2-dependent cells distributed first tothe lung followed by slow clearance to the liver and spleen.Although murine studies demonstrated that the administrationof both IL-2 and LAK cells was necessary for maximal antitumor effects, substantial practical difficulties existed in the application of these findings to humans with advanced cancer.The very tiny amounts of IL-2 that were available precludedthe administration of significant amounts to humans and alsoprecluded the generation of LAK cells in sufficiently largeamounts for use in human treatment. We thus began a seriesof Phase I studies in which naturally derived IL-2 from a highproducer Jurkat cell line was administered to patients (8, 9).We also generated killer cells using exposure to phytohemag-glutinin and administered these cells to patients in Phase Istudies (10).
Table 1 Immunotherapy of murine tumors with IL-2 alone
1. Liver and lung micrometastases (3-day) from a variety of immunogenic andnonimmunogenic sarcomas, melanomas, and adenocarcinomas can be inhibited by IL-2 administration.
2. Lung macrometastases (10-day) from two immunogenic sarcomas (but notfrom two nonimmunogenic sarcomas) can be inhibited by IL-2 administration.
3. A direct relationship exists between the dosage of IL-2 and therapeuticeffect.
4. High dose IL-2 administration leads to in vivo lymphoid proliferation invisceral organs. These cells have LAK activity in vitro.
5. The immunotherapeutic effect of IL-2 on 3-day micrometastases is mediatedby asialo-GMi-positive LAK cells. In immunogenic tumors, Lyt-2-positivecells also participate.
6. The immunotherapeutic effect of IL-2 on 10-day macrometastases is mediated by Lyt-2-positive cells.
8. The sensitivity of macrometastases to therapy involving IL-2 appears to bedirectly related to the expression of MHC antigens (Class I) on the tumor.
9. The administration of IL-2 can enhance the therapeutic effect of concomi-tantly administered LAK cells, TIL, and specifically sensitized T-lympho-cytes.
Table 2 Immunotherapy of murine tumors with LAK cells plus IL-2
1. Liver and lung micrometastases (3-day) from a variety of immunogenic andnonimmunogenic sarcomas, melanomas, and adenocarcinomas can beinhibited by treatment with LAK cells plus IL-2.
2. A direct relationship exists between therapeutic effect and the dosage of IL-2 and the dose of LAK cells.
3. The precursor of the LAK cell effective in vivo is Thy-1 negative, immuno-globulin negative, asialo-ASGMi positive.
4. Three-day incubation of splenocytes is optimal for the generation of LAKcells effective in vivo.
5. Immunotherapy of micrometastases with LAK cells and IL-2 is effective inhosts suppressed by total body irradiation or treatment with cyclophosphamide. Therapy is also effective in "B" mice (thymectomized, lethallyirradiated, reconstituted with T-cell-depleted bone marrow).
6. Immunotherapy of micrometastases with allogeneic LAK cells plus IL-2 iseffective.
7. LAK cells effective in immunotherapy can be generated from the splenocytes of tumor-bearing mice.
9. Administration of IL-2 leads to in vivo proliferation of transferred LAKcells.
10. Diffuse i.p. carcinomatosis can be successfully treated with i.p. LAK cellsplus IL-2.
11. LAK cells can mediate antibody-dependent cellular cytotoxicity; thus administration of IL-2 alone or LAK cells plus IL-2 can enhance the invivo therapeutic efficacy of monoclonal antibodies with antitumor reactivity.
The cloning of the gene for IL-2, its insertion into bacteria,and the availability of very large amounts of purified recombinant IL-2, however, opened many new possibilities for thetreatment of patients with these approaches. Phase I studieswere conducted using either natural or recombinant IL-2 alonein 39 patients and using either phytohemagglutinin-activatedkiller cells or LAK cells alone in 27 patients with advancedcancer to determine the safe tolerable doses of each of thesereagents (8-10). These Phase I studies have been reported indetail and served as the basis for the use of combinations of IL-
2 and LAK cells in patients with advanced cancer. None of the66 patients with advanced cancer treated in these Phase I trialsresponded to treatment.
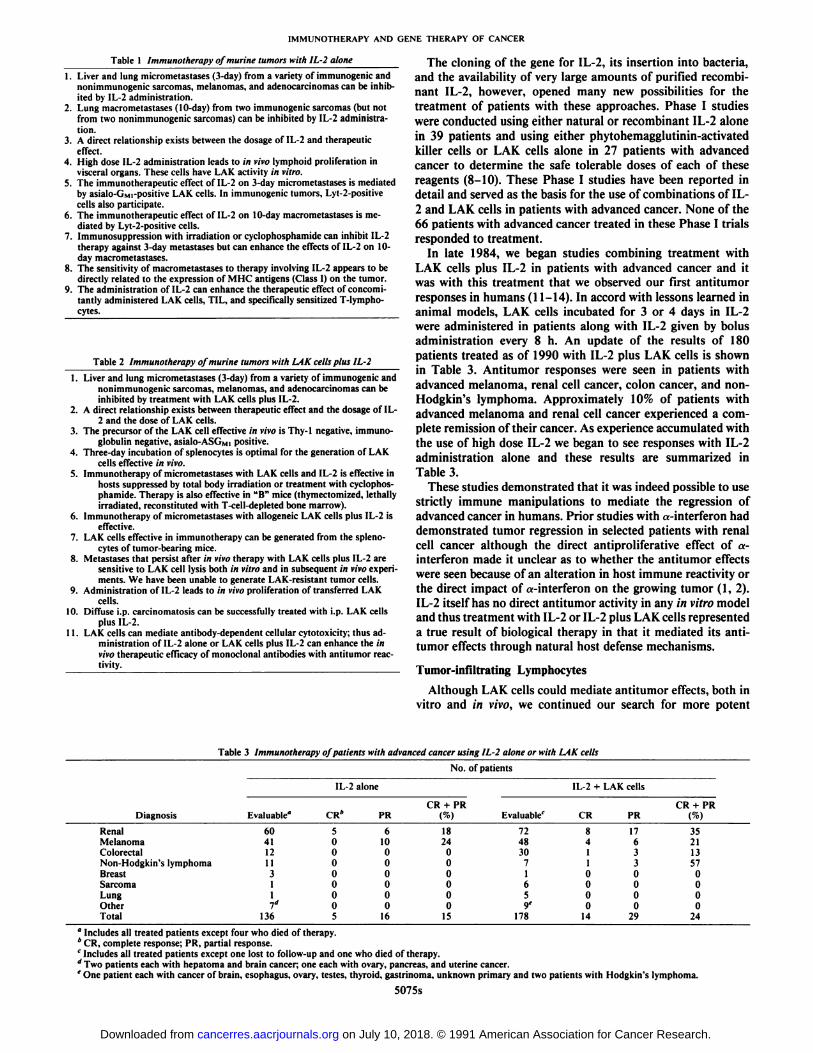
In late 1984, we began studies combining treatment withLAK cells plus IL-2 in patients with advanced cancer and itwas with this treatment that we observed our first antitumorresponses in humans (11-14). In accord with lessons learned inanimal models, LAK cells incubated for 3 or 4 days in IL-2were administered in patients along with IL-2 given by bolusadministration every 8 h. An update of the results of 180patients treated as of 1990 with IL-2 plus LAK cells is shownin Table 3. Antitumor responses were seen in patients withadvanced melanoma, renal cell cancer, colon cancer, and non-Hodgkin's lymphoma. Approximately 10% of patients with
advanced melanoma and renal cell cancer experienced a complete remission of their cancer. As experience accumulated withthe use of high dose IL-2 we began to see responses with IL-2administration alone and these results are summarized inTable 3.
These studies demonstrated that it was indeed possible to usestrictly immune manipulations to mediate the regression ofadvanced cancer in humans. Prior studies with a-interferon haddemonstrated tumor regression in selected patients with renalcell cancer although the direct antiproliferative effect of a-interferon made it unclear as to whether the antitumor effectswere seen because of an alteration in host immune reactivity orthe direct impact of a-interferon on the growing tumor (1, 2).IL-2 itself has no direct antitumor activity in any in vitro modeland thus treatment with IL-2 or IL-2 plus LAK cells representeda true result of biological therapy in that it mediated its anti-tumor effects through natural host defense mechanisms.
Tumor-infiltrating Lymphocytes
Although LAK cells could mediate antitumor effects, both invitro and in vivo, we continued our search for more potent
Table 3 Immunotherapy of patients with advanced cancer using IL-2 alone or with LAK cells
" Includes all treated patients except four who died of therapy.* CR, complete response; PR, partial response.' Includes all treated patients except one lost to follow-up and one who died of therapy.
Two patients each with hepatoma and brain cancer; one each with ovary, pancreas, and uterine cancer.' One patient each with cancer of brain, esophagus, ovary, testes, thyroid, gastrinoma. unknown primary and two patients with Hodgkin's lymphoma.
lymphocytes that might be used in adoptive immunotherapy.Our specific interest was the identification of T-cells that couldrecognize specific tumor antigens in a MHC-restricted fashion.Techniques were developed for isolating TIL from resectedtumors and these cells provided evidence of specific tumorantigen recognition by lymphocytes obtained from a tumor-bearing host (15-18). These cells were isolated by culturingsingle cell suspensions from tumors in IL-2. Infiltrating lymphocytes that bore IL-2 receptors, presumably because of theirreactivity to tumor, grew in the presence of IL-2 and destroyedtumor cells simultaneously growing in the culture. Thus, 2 to 3weeks after initiating cultures pure populations of TIL couldbe established without the presence of contaminating tumorcells. We established techniques for isolating TIL from bothmouse and human tumors and extensively studied these cellsin vitro as well as in tumor models in mice. In the mouse, TILcells were exclusively CD8+ although in the human both CD4+and CD8+ T-cells grew in culture. In the mouse, specificrecognition of tumor antigens could be identified on the basisof specific lysis of target cells as well as by specific cytokinesecretion when TIL were coincubated with the type of tumorcells from which they were derived (19-21). These reactivitieswere MHC restricted and could be inhibited by monoclonalantibodies against Class I antigens.
6. TIL with improved antitumor activity in vivo can be generated from tumorsuspensions by using immunomagnetic beads to isolate lymphocytes followedby incubation of lymphocytes in low dose IL-2.
7. In mice cured of lung micrometastases by administration of TIL. live TILcan be identified in vivo 3 months after injection.
8. The specific secretion of f-interferon by TIL when cultured with tumor is thebest in vitro correlate of the in vivo antitumor effectiveness of TIL. NonlyticTIL that specifically secrete >-interferon can effectively treat established lung
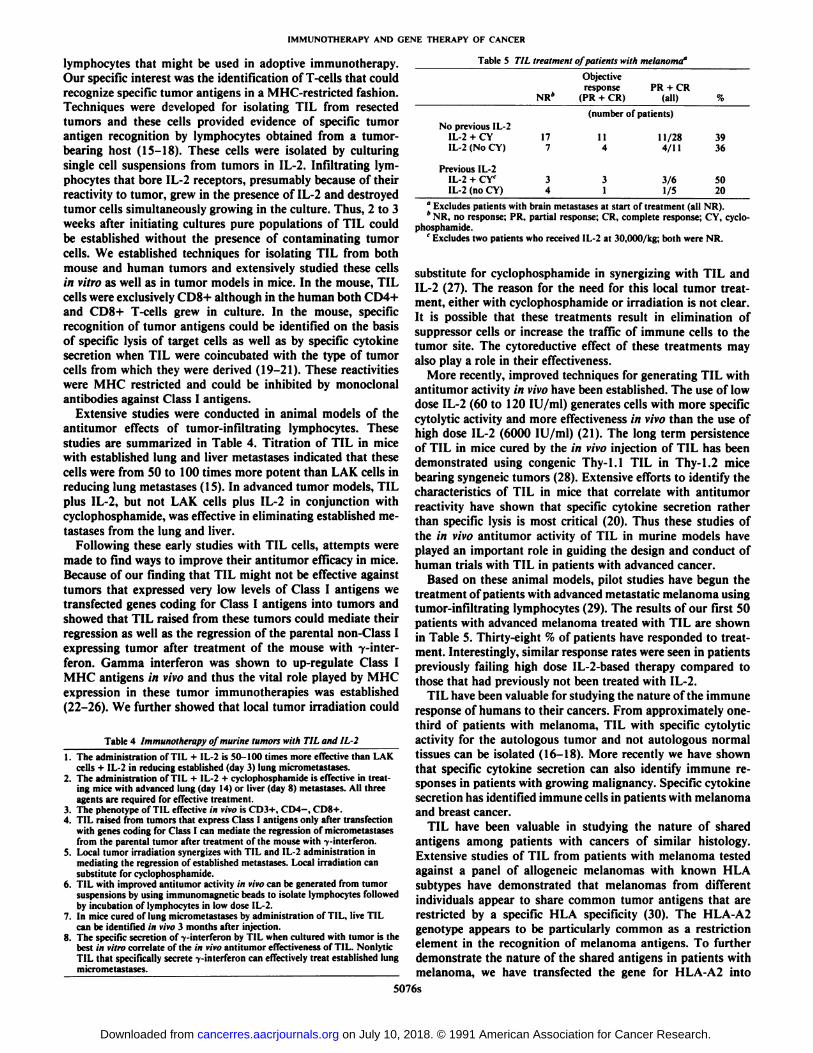
phosphamide.' Excludes two patients who received IL-2 at 30,000/kg; both were NR.
substitute for cyclophosphamide in synergizing with TIL andIL-2 (27). The reason for the need for this local tumor treatment, either with cyclophosphamide or irradiation is not clear.It is possible that these treatments result in elimination ofsuppressor cells or increase the traffic of immune cells to thetumor site. The cytoreductive effect of these treatments mayalso play a role in their effectiveness.
More recently, improved techniques for generating TIL withantitumor activity in vivo have been established. The use of lowdose IL-2 (60 to 120 lU/ml) generates cells with more specificcytolytic activity and more effectiveness in vivo than the use ofhigh dose IL-2 (6000 lU/ml) (21). The long term persistenceof TIL in mice cured by the in vivo injection of TIL has beendemonstrated using congenie Thy-1.1 TIL in Thy-1.2 micebearing syngeneic tumors (28). Extensive efforts to identify thecharacteristics of TIL in mice that correlate with antitumorreactivity have shown that specific cytokine secretion ratherthan specific lysis is most critical (20). Thus these studies ofthe in vivo antitumor activity of TIL in murine models haveplayed an important role in guiding the design and conduct ofhuman trials with TIL in patients with advanced cancer.
Based on these animal models, pilot studies have begun thetreatment of patients with advanced metastatic melanoma usingtumor-infiltrating lymphocytes (29). The results of our first 50patients with advanced melanoma treated with TIL are shownin Table 5. Thirty-eight % of patients have responded to treatment. Interestingly, similar response rates were seen in patientspreviously failing high dose IL-2-based therapy compared tothose that had previously not been treated with IL-2.
TIL have been valuable for studying the nature of the immuneresponse of humans to their cancers. From approximately one-third of patients with melanoma, TIL with specific cytolyticactivity for the autologous tumor and not autologous normaltissues can be isolated (16-18). More recently we have shownthat specific cytokine secretion can also identify immune responses in patients with growing malignancy. Specific cytokinesecretion has identified immune cells in patients with melanomaand breast cancer.
TIL have been valuable in studying the nature of sharedantigens among patients with cancers of similar histology.Extensive studies of TIL from patients with melanoma testedagainst a panel of allogeneic melanomas with known HLAsubtypes have demonstrated that melanomas from differentindividuals appear to share common tumor antigens that arerestricted by a specific HLA specificity (30). The HLA-A2genotype appears to be particularly common as a restrictionelement in the recognition of melanoma antigens. To furtherdemonstrate the nature of the shared antigens in patients withmelanoma, we have transfected the gene for HLA-A2 into
melanomas and have shown that 6 of 6 different melanomastransfected with the gene for HLA-A2 are recognized by asingle HLA-A2-restricted TIL (31). It thus appears that antigens shared among melanomas can be recognized by TIL andpossibilities for the use of these antigens for immunization ofpatients against cancer appear feasible. Using TIL as a recognition system we are currently in the process of attempting toclone the gene that codes for tumor antigens in both the mouseand human by transfection of genes from sensitive to resistantcell lines. Should such genes be cloned they could be insertedinto vaccinia or other viruses for use in the immunization ofpatients against cancer antigens.
Finally studies with TIL have demonstrated that these cellsrecirculate and specifically localize in cancer deposits. Up to0.015% of all injected TIL localized per g of tumor based on invivo studies in humans using TIL labeled with '"In (32, 33).
The ability to introduce and express foreign genes in eu-karyotic cells has opened new possibilities for the therapy ofcancer. Our first attempts at the gene therapy of cancer involvedmodification of TIL by the insertion of marker genes (35, 36).More recently genes coding for cytokines have been introducedinto TIL.
In the first phase of these studies we inserted into TIL abacterial gene coding for neomycin phosphotransferase whichcould induce resistance to the antibiotic neomycin and enableus to differentiate adoptively transferred TIL from endogenoushost lymphocytes (35, 36). The goal of these studies was todemonstrate the feasibility and safety of using retroviral mediated gene transfer to introduce genes into humans and tostudy the long term distribution and survival of autologous TIL.
Because of the practical, safety, and ethical issues involvedwith human gene transfer and the possible consequences ofusing a modified retrovirus derived from the Moloney murineleukemia retrovirus randomly integrating a new gene into thehuman genome, our clinical studies utilizing human TIL transduced with the gene coding for neomycin resistance (NeoR)were preceded by extensive in vitro studies and were extensivelyreviewed by a variety of review groups composed of clinicians,scientists, ethicists, and lay people. In these studies we demonstrated that the gene could be successfully inserted intohuman TIL, that the properties of human TIL were not altered,that the gene was expressed in TIL, and that these procedurescould be performed with little risk to the patient and no risk tohealth care personnel and the public. Retroviral mediated genetransduction of TIL was selected because of the high efficiency
Table 6 Experimental leads for improving immunotherapy
\. Enhancing in vivo effectiveness of TILa. Combination with other cytokinesb. Combination with local radiation therapy
2. Generating more effective TILa. Lymphocyte subpopulations or clonesb. Repeated in vitro stimulationc. Low-dose IL-2d. Culture in IL-2 + IL-4e. Modify TIL by gene transfer
3. Immunize with gene-modified tumora. Cytokine genesb. MHC antigen genes
4. Application of new cytokinesa. IL-6b. Cytokine combinations
of gene transfer using this technique (37, 38).Studies performed on TIL from multiple cancer patients as
well as the 10 patients who have now received NeoR gene-modified TIL demonstrated that the NeoR gene could be inserted into human TIL, that it was satisfactorily expressed, andthat the general properties of the TIL were not changed (35,36). Semiquantitative Southern blots indicated that approximately one viral genome copy was present in the gene-transduced TIL. The phenotype and cytotoxicity of the transducedand nontransduced cells were similar. Analyses of T-cell receptor gene rearrangements revealed the oligoclonal nature of theTIL population and no major changes in the DNA rearrangement patterns or the level of mRNA expression of theßand 7 chains following transduction and selection of TIL inthe neomycin analogue G418 (35). Similarly, cytokine mRNAexpression was not significantly altered following the transduction of TIL.
Transduced TIL consistently showed resistance to G418, aneomycin analogue lethal to all eukaryotic cells. The polymer-ase chain reaction technique was utilized to detect the NeoRgenome. Approximately one transduced cell in 10s normal cells
could be consistently detected (36).Safety considerations were paramount in our consideration
of the use of this gene transduction technique for introducinggenes into TIL for use in patient therapy. Extensive safetystudies were performed on all transduced TIL including testsfor aerobic and anaerobic bacteria, fungi, and Mycoplasma andtests using sarcoma-positive, leukemia-negative assays for eco-tropic, xenotropic, and amphotropic infectious viruses. Amplification tests using NIH 3T3 cells were performed and wereshown to be capable of detecting a single viral particle per mlof solution. All safety tests performed on TIL in preclinicalstudies as well as on TIL from the patients who received thegene-modified cells were negative and no safety problems ofany kind were detected (36). Gene-modified cells could bedetected in the circulation up to 189 days and in tumor depositsup to 64 days after the infusion of gene-modified TIL (36).
Laboratory and clinical studies using TIL transduced withthe gene for neomycin resistance demonstrated that retroviralmediated gene transduction was a feasible and safe means forintroducing genes into humans. Because of the accumulation ofTIL at tumor deposits we have conducted studies attemptingto modify human TIL with genes that can improve the antitu-mor effectiveness of these cells. The first gene that we haveselected for these studies is the gene for TNF.
Extensive animal research in the Surgery Branch, NationalCancer Institute, and in many other groups have demonstrated
that the injection of recombinant TNF can mediate the necrosisand regression of a variety of established murine cancers. However, tumor-bearing mice can tolerate up to 400 Mg/kg TNFand these doses are required to mediate tumor regression; theadministration of less TNF is far less effective. In contrast, themaximum tolerated dose of TNF in humans in both SurgeryBranch, National Cancer Institute, and other studies is approximately 8 /¿g/kgday O)- Thus when given i.v. injections humanscan tolerate only 2% of the TNF dose required to mediateantitumor effects in the mouse and this appears to explain whyantitumor effects have not been seen when TNF was administered systemically to humans.
We have thus sought means to selectively increase the localconcentration of TNF at the tumor site. Because TIL can trafficdirectly to tumor deposits and concentrate at those sites (32,33) we have hypothesized that TIL that are genetically modifiedto produce large amounts of TNF may generate high TNFconcentrations in the local tumor microenvironment and thusexhibit an increased antitumor effect compared to normal TIL.
The retroviral vector construct selected for insertion of theTNF gene into human TIL contains the TNF gene promotedby the murine long terminal repeat and the neomycin resistancegene promoted by the SV40 early promoter region. The two-gene retroviral construct was introduced into the PA317 producer cell line and the supernatant from this line was used totransduce the TIL from patients with advanced metastaticmelanoma.
Although it has been relatively easy to express cytokine genesin tumor cells and demonstrate production of large amounts ofTNF, difficulties exist in the expression of cytokine genes inlymphocytes. It has been difficult to achieve consistently highlevels of cytokine production in lymphocytes using these retro-viral vectors probably because regulatory mechanisms exist forcytokine transcription, translation, and/or secretion in lymphocytes that do not exist in other cell types. We have, however,been able to achieve the expression of TNF genes in lymphocytes from selected patients and have achieved cytokine secretion in excess of 100 pg/106 cells/24 h.
We have begun clinical studies using these TNF gene-modified TIL in patients with advanced cancer. Increasing numbersof TNF-transduced TIL are being administered, first in theabsence of IL-2 and then when safely tolerated doses areachieved, in conjunction with IL-2. To the present time fourpatients with advanced melanoma have been treated with theTNF gene-modified TIL. No side effects have been seen at celldoses which have ranged up to 10" cells in a single infusion. Alarge series of patients treated with gene-modified TIL plus IL-2 will be required to know whether or not this approach givesimproved results compared to the use of unmodified TIL. Wecurrently have permission to treat up to 50 patients with TNFgene-modified TIL utilizing this approach.
Additional genes being studied for insertion into TIL toimprove their antitumor activity include 7-interferon, IL-2, IL-6, and genes for chimeric T-cell receptors.
More recently we have begun studies investigating the use ofgenetic modification of tumor cells to increase their immuno-genicity. We and others have demonstrated that insertion ofcytokine genes can increase the immune recognition of tumorcells and can lead to the production by the host of cytolyticcells that are not produced in response to the parental non-modified tumor (39-43). These experiments have been conducted by a variety of groups and include insertion of genes forIL-4, IL-2, tumor necrosis factor, 7-interferon, and granulo-
cyte-macrophage-colony-stimulating factor. In related experiments we have shown that insertion of the gene for Class Imajor histocompatibility antigens can also increase the immu-nogenicity of tumors and lead to the generation of TIL thatcannot be produced from low MHC-expressing tumors (26).
This approach to gene therapy, by genetically modifying tumorsfor use in immunization, holds promise not only for activeimmunotherapy but also for the development of immune cellsthat might be used in adoptive immunotherapy.
In the last decade biological therapy has been shown to becapable of mediating the regression of established cancers insome patients with advanced malignancy. The continued development of these biological approaches offers the hope that theycan lead to the development of effective, safe, and practicaltreatments for patients with cancer.
References
1. Rosenberg, S. A.. Longo. D. L., and Lotze. M. T. Principles and applicationsof biologic therapy. In: V. T. DeVita, S. Hellman, and S. A. Rosenberg (eds.).Cancer, Principles and Practices of Oncology, Ed. 3, pp. 1342-1398. Philadelphia: J. B. Lippincott Co., 1989.
2. DeVita, V., Hellman, S., and Rosenberg, S. A. (eds.). Biologic Therapy ofCancer. Philadelphia: J. B. Lippincott Co., 1991.
3. Yron, !.. Wood. T. A., Spiess, P. J., and Rosenberg, S. A. In vitro growth ofmurine T cells. V. The isolation and growth of lymphoid cells infiltratingsyngeneic solid tumors. J. Immunol., 125: 238-245, 1980.
4. Lotze, M. T., Line, B. R.. Mathisen. D. J., and Rosenberg, S. A. The in vivodistribution of autologous human and murine lymphoid cells grown in T cellgrowth factor (TCGF): implications for the adoptive immunotherapy oftumors. J. Immunol.. 125: 1487-1493, 1980.
6. Papa, M. Z., Mule, J. J., and Rosenberg, S. A. The anti-tumor efficacy oflymphokine-activated killer cells and recombinant interleukin-2 in vivo: immunogenic and nonimmunogenic murine tumors of three distinct histologietypes. Cancer Res.. 46: 4973-4978. 1986.
8. Lotze, M. T., Frana, L. W., Sharrow, S. O.. Robb. R. J., and Rosenberg, S.A. In vivo administration of purified human interleukin-2. 1. Half life andimmunologie effects of the Jurkat cell line derived IL-2. J. Immunol., 134:157-166, 1985.
9. Lotze, M. T., Matory, Y. L., Ettinghausen, S. E., Rayner, A. A., Sharrow,S. O., Seipp, C. A., Custer, M. C., and Rosenberg, S. A. In rivo administrationof purified human interleukin-2. II. Half life and immunologie effects andexpansion of peripheral lymphoid cells in vivo with recombinant IL-2. J.Immunol., 135: 2865-2875, 1985.
10. Rosenberg, S. A. Immunotherapy of cancer by the systemic administrationof lymphoid cells plus interleukin-2. J. Biol. Response Modif., 3: 501-511,1984.
11. Rosenberg. S. A., Lotze, M. T., Muul, L. M., Leitman, S., Chang, A. E.,Ettinghausen, S. E., Matory, Y. L.. Skibber. J. M., Shiloni, E., Seipp, C. A.,Simpson, C., and Reichert, C. M. Observations on the systemic administration of autologous lymphokine-activated killer cells and recombinant interleukin-2 in patients with metastatic cancer. N. Engl. J. Med.. 313: 1485-1492, 1985.
12. Rosenberg, S. A., Lotze, M. T., Muul, L. M., Chang. A. E.. Avis, F. P.,Leitman, S., Linehan, W. M., Robertson, C. N., Lee, R. E., Rubin, J. T.,Seipp. C. A.. Simpson, C. G., and White. D. E. A progress report on thetreatment of 157 patients with advanced cancer using lymphokine activatedkiller cells and interleukin-2 or high dose interleukin-2 alone. N. Engl. J.Med., 316: 889-905. 1987.
13. Rosenberg, S. A. Immunotherapy of patients with advanced cancer usinginterleukin-2 alone or in combination with lymphokine activated killer cells.In: V. DeVita, S. Hellman. and S. A. Rosenberg (eds.). Important Advancesin Oncology, pp. 217-257. Philadelphia: J. B. Lippincott Co., 1988.
14. Rosenberg. S. A., Lotze, M. T.. Yang, J. C.. Aebersold, P. A., Linehan, W.M., Seipp, C. A., and White, D. E. Experience with the use of high-doseinterleukin-2 in the treatment of 652 patients with cancer. Ann. Surg., 210:474-485, 1989.
15. Rosenberg. S. A.. Spiess, P., and Lafreniere. R. A new approach to theadoptive immunotherapy of cancer with tumor-infiltrating lymphocytes. Science (Washington DC). 223: 1218-1321. 1986.
16. Muul, L. M., Spiess, P. J., Director, E. P., and Rosenberg, S. A. Identification
of specific cytolytic immune responses against autologous tumor in humansbearing malignant melanoma. J. Immunol., 104: 366-376, 1987.
17. Topalian, S. L.. Muul. L. M., Solomon. D.. and Rosenberg. S. A. Expansionof human tumor infiltrating lymphocytes for use in immunotherapy trials. J.Immunol. Methods, 102: 127-141, 1987.
18. Topalian, S. L., Solomon, D., and Rosenberg, S. A., Tumor-specific cytolysisby lymphocytes infiltrating human melanomas. J. Immunol., 142: 3714-2725, 1989."
21. Vang. J. C., Perry-Lalley, D.. and Rosenberg. S. A. An improved method forgrowing murine tumor infiltrating lymphocytes with in vivo antitumor activity. J. Biol. Response Modif.. 9: 149-159. 1990.
22. Cohen. P. J.. Lotze, M. T.. Roberts. J. R., Rosenberg, S. A., and Jaffe. E. S.The immunopathology of sequential tumor biopsies in patients treated withinterleukin-2. Correlation of response with T-cell infiltration and HLA-DRexpression. Am. J. Pathol.. 129: 208-216. 1987.
23. Rubin, J. T., Elwood. L. T., Rosenberg, S. A., and Lotze, M. T. Immunohis-tochemical correlates of response to recombinant interleukin-2 based immunotherapy in human. Cancer Res., 49: 7086-7092. 1989.
24. Weber. J. S., Jay. G.. and Rosenberg. S. A. Immunotherapy of a murinetumor with interleukin-2; increased sensitivity after MHC Class I genetransfection. J. Exp. Med.. 166: 1716-1733. 1987.
25. Weber. J. S., and Rosenberg, S. A. Modulation of murine tumor majorhistocompatibility antigens by cytokines in vivoand in vitro. Cancer Res., 48:5818-5824, 1988.
26. Weber. J. S., and Rosenberg. S. A. Effects of murine tumor MHC class Iexpression on the anti-tumor activity of tumor infiltrating lymphocytes. J.Nati. Cancer Inst., 82: 755-761. 1990.
27. Cameron, R. B.. Spiess. P. J.. and Rosenberg, S. A. Synergistic antitumoractivity of tumor infiltrating lymphocytes, interleukin-2. and local tumorirradiation: studies on the mechanism of action. J. Exp. Med., 171: 249-263. 1990.
28. Alexander. R. B.. and Rosenberg, S. A. Adoptively transferred tumor infiltrating lymphocytes can cure established metastatic tumor in mice andpersistent long term in vivo as functional memory T lymphocytes. J. Immu-nother., in press, 1991.
29. Rosenberg, S. A.. Packard, B. S., Aebersold, P. M., Solomon, D., Topalian,S. L., Toy, S. T., Simon, P., Lotze, M. T., Yang, J. C., Seipp, C. A., Simpson,C., Carter, C., Bock, S.. Schwartzentruber, D., Wei, J. P., and White, D. E.Immunotherapy of patients with metastatic melanoma using tumor infiltrating lymphocytes and interleukin-2: preliminary report. N. Engl. J. Med.,319: 1676-1680. 1988.
30. Horn. S. A.. Topalian, S. L., Simon, S. T., Mancini, M. J., and Rosenberg.S. A. Common expression of melanoma tumor-associated antigens recognized by human tumor-infiltrating lymphocytes: analysis by HLA restriction.J. Immunother. 10: 153-164. 1991.
31. Kawakami. Y.. Zakut. R., Topalian, S. L., Stotter. H.. and Rosenberg, S. A.Shared human melanoma antigens: recognition by tumor infiltrating lymphocytes in HLA-A2.1 transfected melanomas, submitted. 1991.
32. Fisher. B., Packard. B. S., Read, E. J., Carrasquillo, J. A., Carter. C. S.,Topalian, S., Yang, J. C., Volles, P., Larson, S. M., and Rosenberg, S. A.Tumor localization of adoptively transferred indium-111 labeled tumor infiltrating lymphocytes in patients with metastatic melanoma. J. Clin. Oncol.,7:250-261, 1989.
33. Griffith. K. D.. Read, E. J., Carrasquillo. J. A.. Carter, C. S., Yang, J. C.,Fisher, B., Aebersold. P.. Packard. B. S., Yu, M. V.. and Rosenberg, S. A.In vivo distribution of adoptively transferred indium-Ill labeled tumorinfiltrating lymphocytes and peripheral blood lymphocytes in patients withmetastatic melanoma. J. Nail. Cancer Inst., 81: 1709-1717, 1989.
35. Kasid, A., Morecki. S.. Aebersold. P.. Cornetta, K.. Culver. K., Freeman, S.,Director, E., Lotze, M. T., Blaese, R. M., Anderson. W. F.. and Rosenberg,S. A. Human gene transfer: characterization of human tumor infiltratinglymphocytes as vehicles for retroviral mediated gene transfer in man. Proc.Nati. Acad. Sci. USA. 87: 473-477. 1990.
36. Rosenberg, S. A., Aebersold, P., Cornetta, K., Kasid. A.. Morgan, R. A.,Moen, R., Karson, E. M., Lotze. M. T., Yang. J. C., Topalian, S. L., Merino,M. J., Culver, K., Miller, A. D. E., Blaese, R. M., and Anderson. W. F. Genetransfer into humans: immunotherapy of patients with advanced melanomausing tumor-infiltrating lymphocytes modified by retrieval gene transduction.N. Engl. J. Med., 8: 323:570-578, 1990.
37. Bender, M. A., Palmer. T. D.. Gelinas, R. E., and Miller, A. D. Evidencethat the packaging signal of Moloney murine leukemia virus extends into thegag region. J. Viro!.. 61: 1639-1646, 1987.
38. Armentano, D., Yu, S. F., Kantoff. P. S., von Rüden,T., and Anderson, W.F. Effect of internal viral sequences on the utility of retroviral vectors. J.Virol., 61: 1647-1650. 1987.
39. Fearon, E. R.. Pardoll. D. M., Itaya, T.. Golumbek. P., Levitsky, H. I..Simons, J. W., Karasuyama, H., Vogelstein, B., and Frost, P. Interleukin-2production by tumor cells bypasses T helper function in the generation of anantitumor response. Cell. 60: 397-403. 1990.
40. Gansbacher. B.. Zier, K.. Daniels, B., Cronin, K., Bannerji. R., and Gilboa.E. Interleukin 2 gene transfer into tumor cells abrogates tumorigenicity andinduces protective immunity. J. Exp. Med., 172: 1217-1224, 1990.
41. Gansbacher, B., Bannerji. R.. Daniels, B.. Zier, K., Cronin, K., and Gilboa,E. Retroviral vector-mediated -y-interferon gene transfer into tumor cellsgenerates potent and long lasting antitumor immunity. Cancer Res., SO:7820-7825, 1990.
43. Colombo, M. P., Ferrari, G., Stoppacciaro, A., Parenza, M., Rodolfo, M.,Mavilio, F., and Parmiani. G. Granulocyte colony-stimulating factor genetransfer suppresses tumorigenicity of a murine adenocarcinoma in vivo. J.Exp. Med.. 173: 889-897. 1991. "