Immunotherapy is the Preferred Initial Treatment for Most Patients with Metastatic BRAF V600 Mutant Melanoma Michael B. Atkins, M.D. Deputy Director Georgetown-Lombardi Comprehensive Cancer Center
Transcript
Immunotherapy is the Preferred Initial Treatment for Most Patients with
Immunotherapy works as well against BRAFV600 mutant melanoma as WT tumors
Immunotherapy is getting better Better drugs Better patient selection
BRAF inhibitors work as well in patients with prior immune therapy; the converse is not so
High Dose IL-2 Therapy*
RR: 16% (43 / 270) Some large volume and
visceral Most soft tissue and lung
Durable responses Median 8.9 mos CR: not reached
Survival Median 12 mos 11% >@ 5yrs
*Atkins et al JCO, 1999 (N=270)
Pooled data from phase II studies CA184-008 and CA184-022:ipilimumab monotherapy 10 mg/kg (N=227)
mWHO CR/PR/SD = 27.8%
irRC CR/PR/SD with WHO PD = 9.7%
Other PD or unknown = 62.6%
1.0
0.8
0.6
0.4
0.2
0
Pro
po
rtio
n a
live
0 2 4 6 8 10 12 14 16 18 20 22 24 26
Wolchok, Hodi et al
Overall survival for 51-patient cohort Rx’d w/ 10 mg/kg x 4 + maintenance
~26% 2 yr OS estimate also seen in 165-pt cohort from expanded access trial
Kevin Heller, BMS—data presented in part at ESMO 2009, ASCO 2010, 2011 posters
Relationship of MAPKinase pathway mutations and response to HD IL-2
Mutation All CR/PR SD/PD P-value
BRAF 60 14(23%) 46 (77%)
0.05NRAS 15 7 (47%) 8 (53%)
WT 26 3 (12%) 23 (88%)
Joseph, Sullivan et al- JIT 2011
A significantly larger proportion of patients with BRAF or NRAS mutant tumors achieved CR/PR compared to those with WT tumors.
Produces durable unmaintained responses; not restricted by BRAF status
Activity powerful enough to work in the CNS and overcome concurrent immunosuppression
Activity seen in patients with prior IL-2 Activity seen in patients with elevated LDH, liver metastases,
etc Treatment more widely applicable
Ipilimumab Therapy
BRAF inhibitor Therapy - Limitations
Median PFS of only 6-7 months Median OS 13-16 months Forrest plot suggests most of the benefit
confined to patients with M1c disease
Sosman et al NEJM 2012, Chapman et al ASCO 2012Sosman et al NEJM 2012, Chapman et al ASCO 2012
100
90
80
70
60
50
40
30
20
10
0
Ove
rall
surv
ival
(%
)
0 6 12 18 24
Vemurafenib (n=337)
Median f/u 12.5 months
Dacarbazine (n=338)
Median f/u 9.5 months
338
337
173
280
79
178
24
44
0
1
244
326
111
231
50
109
4
7
9.7 13.6
Overall survival (February 01, 2012 cut-off) censored at crossover
Hazard ratio 0.70 (95% CI: 0.57–0.87)p<0.001 (post-hoc)
Time (months)No. at riskDacarbazine
Vemurafenib
15.9
BRIM2
All patients 675
Age: <65 years≥65 years
514161
Sex: FemaleMale
294381
ECOG status: 0 1
459216
Disease stage: IIIc M1a M1b M1c
3374
127441
LDH: Normal Elevated
391284
FactorNumber
of patients
0.2 0.4 0.6 1.0 2 4 106
Favors vemurafenib
Favors dacarbazine
20
Hazard ratio and 95% confidence interval
Overall survival by baseline characteristic (February 01, 2012 cut-off) censored at crossover
BRAF inhibitor Therapy - Limitations
Median PFS of only 6-7 months Median OS 13-16 months Forest plot suggests most of the benefit
confined to patients with M1c disease Combination BRAF-MEK inhibition may offer
some advantages…
Sosman et al ASCO 2012, Chapman et al ASCO 2012Sosman et al ASCO 2012, Chapman et al ASCO 2012
BRAF inhibitor Therapy - Limitations
Median PFS of only 6-7 months Median OS 13-16 months Forest plot suggests most of the benefit
confined to patients with M1c disease Combination BRAF-MEK inhibition may offer
some advantages, but median PFS still only 7-10 months
Sosman et al ASCO 2012, Chapman et al ASCO 2012, Weber et al, ASCO 2012
Sosman et al ASCO 2012, Chapman et al ASCO 2012, Weber et al, ASCO 2012
BRAF inhibitor Therapy - Limitations
Thus, BRAF (+/- MEK) inhibitor treatment postpones but does not prevent the tragedy of metastatic melanoma
Sosman et al ASCO 2012, Chapman et al ASCO 2012, Weber et al, ASCO 2012
Sosman et al ASCO 2012, Chapman et al ASCO 2012, Weber et al, ASCO 2012
Treatment for BRAF Mutant Melanoma
Years after stage IV diagnosis
Pro
por
tion
Sur
vivi
ng
Ipilimumab
0 1 2 3 4 5
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
BRAFi
PRESENTED BY: Michael B. Atkins
Which is preferred?
Immunotherapy is getting better
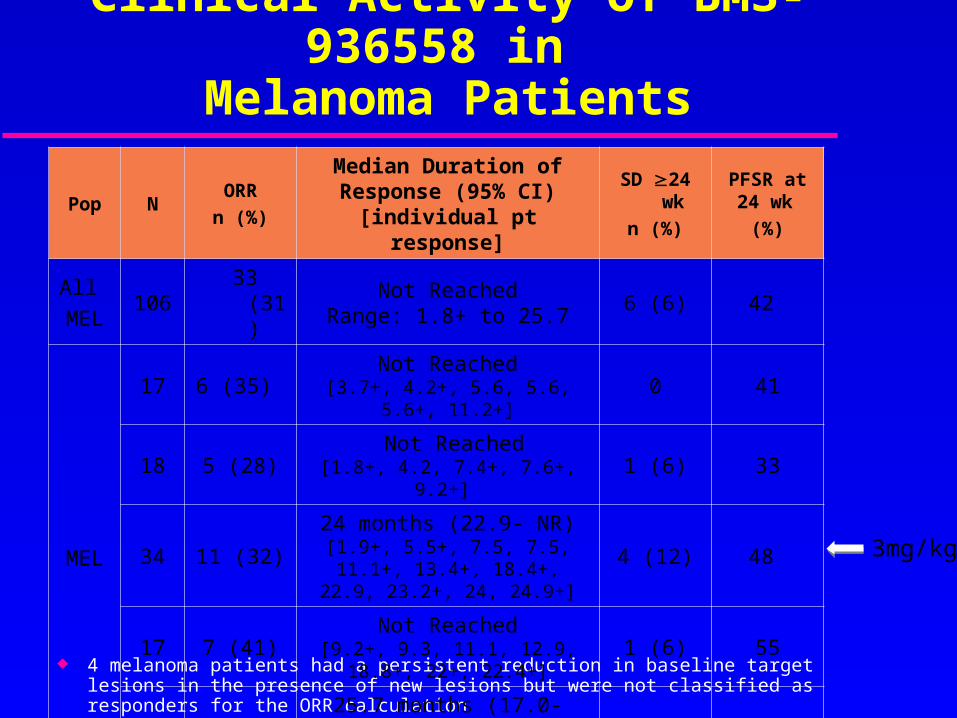
Clinical Activity of BMS-936558 in Melanoma Patients
4 melanoma patients had a persistent reduction in baseline target lesions in the presence of new lesions but were not classified as responders for the ORR calculation
Pop NORR
n (%)
Median Duration of Response (95% CI)
[individual pt response]
SD 24 wk
n (%)
PFSR at 24 wk
(%)
All
MEL106 33 (31)
Not ReachedRange: 1.8+ to 25.7 6 (6) 42
MEL
17 6 (35) Not Reached[3.7+, 4.2+, 5.6, 5.6, 5.6+, 11.2+]
0 41
18 5 (28) Not Reached [1.8+, 4.2, 7.4+, 7.6+, 9.2+]
Changes in Target Lesions Over Time inMelanoma Patients (3mg/kg)
Dose Group: 3mg/kg
+: 1st Occurence of New Lesion
On Study Status(On/Off) Off On
% C
hang
e Fr
om B
asel
ine
In T
arge
t Les
ions
Tum
or B
urde
n
-100
-90
-80
-70
-60
-50
-40
-30
-20
-10
0
10
20
30
40
50
60
Weeks Since Initiation Of Treatment
0 10 20 30 40 50 60 70 80 90 100 110 120 130
Of 33 patients with OR (all dose levels) 29 were treated 1 year (before July 3, 2012) and 14 had responses of 1 year 4 were treated <1 year and 4 had responses ranging from 1.8-5.3 months
MK-3475 (Unconfirmed + Confirmed Responses) in Advanced MEL Patients
Complete Response(N, 95% CI)
Objective Response(N, 95% CI)
Disease Control Rate
(N, 95% CI)
All MELN=83
5%(4; 2%-13%)
47%(39; 34% - 56%)
60%(50; 48%- 70%)
IPI Naïve N=58
7%(4; 2%-18%)
50%(29; 35% -61 %)
67%(39; 51%-76%)
IPI Treated N=25
0 %40%
(10; 17% -59%)44%
(11; 24%-68%)All patients were dosed at 10 mg/kgIncludes all patients who received first dose as of April 25, 2012. Centrally available response information as of Oct 19, 2012Objective response= confirmed and unconfirmed complete and partial responseDisease control rate= objective response + stable disease
Hamid SMR 11/11/12
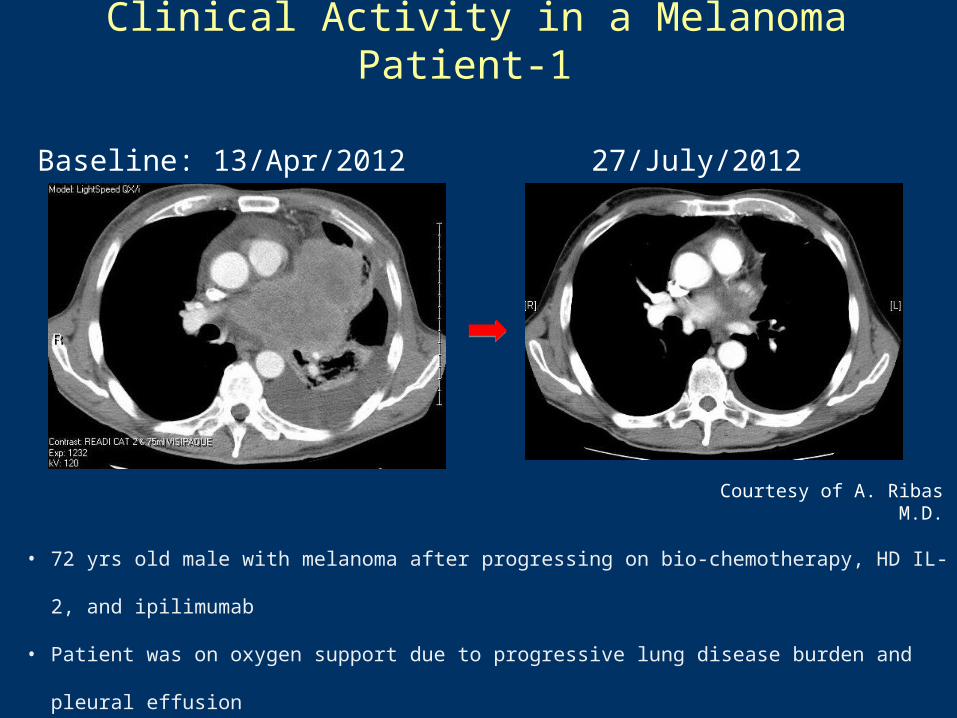
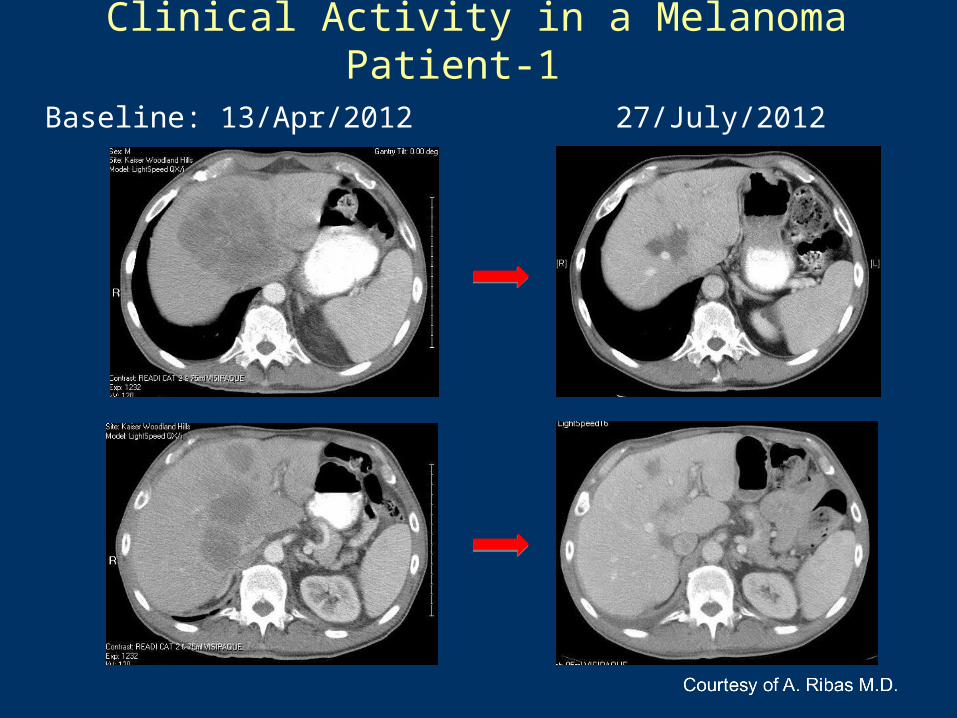
Clinical Activity in a Melanoma Patient-1
Baseline: 13/Apr/2012 27/July/2012
• 72 yrs old male with melanoma after progressing on bio-chemotherapy, HD IL-2, and ipilimumab
• Patient was on oxygen support due to progressive lung disease burden and pleural effusion
• After 3 months of MK-3475, the patient is off the oxygen support and continues to respond
Courtesy of A. Ribas M.D.
Baseline: 13/Apr/2012 27/July/2012
Clinical Activity in a Melanoma Patient-1
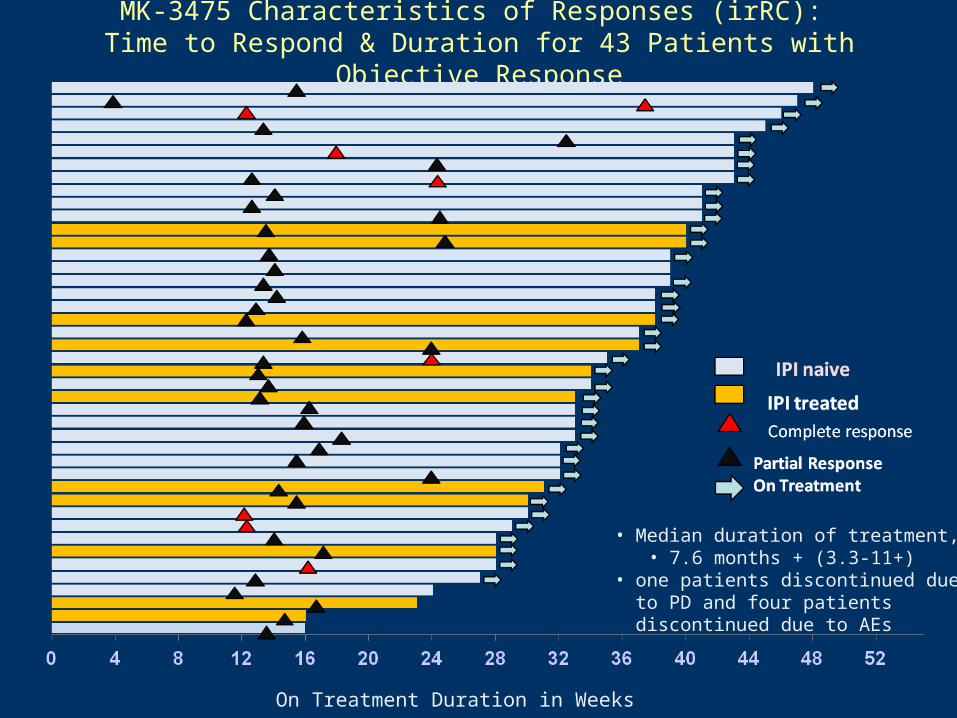
MK-3475 Characteristics of Responses (irRC): Time to Respond & Duration for 43 Patients with Objective
Response
On Treatment Duration in Weeks
• Median duration of treatment, • 7.6 months + (3.3-11+)
• one patients discontinued due to PD and four patients discontinued due to AEs
Immunotherapy for Melanoma
PRESENTED BY: Michael B. Atkins
Years after stage IV diagnosis
Pro
por
tion
Sur
vivi
ng
Ipilimumab
Anti-PD1
Anti PD1 + x
0 1 2 3 4 5
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0 ???
IL-2
Checkpoint blockade vs oncogene-mutation targeted therapy for melanoma
# Annual Cases
Proportion c\ mutation
% RR Median Durability of remission
Pt years
BRAF + cKIT
9000 0.5 0.5 0.6 yrs 1350 pt yrs
Anti-CTLA4/Anti-PD1
9000 N/A 0.33 2 years 6000 pt yrs
Annual pt-years of remission
Adapted from Drew Pardoll
Treatment Selection Opportunities
NSCLC
Melanoma
RCC
**2 pts still under evaluation
42 pts include 18 MEL, 10 NSCLC, 7 CRC, 5 RCC, and 2 CRPC.
Correlation of PD-L1 expression in pretreatment tumor biopsies with clinical outcomes in Anti-PD-1 Therapy
Association Between Pretreatment Tumor PD-L1 Expression and Clinical Response
Response Status PD-L1 Positive no. (%)
PD-L1 Negative no. (%)
Totalno. (%)
CR/PR 9 (36) 0 9 (21)
Nonresponder 16* (64) 17 (100) 33 (79)
All Patients 25 17 42
Topalian S, et al. NEJM 2012;366:2443-2454.
Prop
ortio
n of
pati
ents
p=0.006
0
0.2
0.4
0.6
0.8
1
PD-L1(+) PD-L1(-)
PD-L1(+)PD-L1(-)9/25
16*/25
17/17
0/17† analysis not pre-planned and based on subset of subjects'.
†
Sequencing of Treatment
Baseline characteristics
Ove
rall
resp
on
se r
ate
(%)
30
40
50
70
60
80
BRIM2- ORR by pre-defined subgroups
20
0
Age
<65 65Alltreatedpatients
Alltreatedpatients
Sex
F M
LDH at enrollment
1.0–1.5xULN
>1.5xULN
Normal
ECOG PS
0 1
Stage
M1a/M1b
M1c
# priortherapies
1 >1
Previous IL-2
Yes No
10
Overall ORR of 53% (IRC)
RR (size proportional to the number of patients in the subgroup)
95% Confidence intervals
Ribas et al ASCO 2011Ribas et al ASCO 2011
BRAF inhibition +/- prior immunotherapy
MAPKi PFS
IT initially PFS 6.7 mo (CI 4.3-9.1 mo)MAPKi initially PFS 5.6 mo (CI 4.7-6.8 mo)
p-value 0.43, log rank
MAPKi OS
IT initially OS 19.6 mo (CI 10.0- mo)MAPKi initially OS 13.4 mo (CI 10.1-17 mo)
p-value 0.40, log rank
OS
(pr
obab
ility
)
Time (mo)
Ackerman/Sullivan-BIDMC/MGH-SITC 2012
Immunotherapy following MAPKI: DFHCC/MIA Retrospective Data
– 193 patients discontinued MAPKi therapy (176 with disease progression)
• Median OS 2.9 mos (CI 1.8-4.4 mos) from last dose of MAPKi
• Single agent ipilimumab treatment (n=34 pts) No tumor responses (2 SD)Median PFS 2.7 mos, median OS 5 mos50% of patients received < 4 doses All Pts alive > 1 year- are back on MAPK inhibitors inhibitors
– Summary: • Patients progressing on BRAFi appear unlikely to respond to
ipilimumab• Those alive either had slow growing disease and short period
of RAFi treatment due to toxicity or are back on a RAFi
Ackerman/Sullivan-BIDMC/MGH-SITC 2012
OS 5.0 mo (CI 3.0-8.8 mo)
long term survivors all treated with additional MAPKi
OS
(pr
obab
ility
)
Time (mo)
PFS 2.7 mo (CI 1.8-3.1 mo)
Ipilimumab following BRAF inhibitor Therapy
Ackerman/Sullivan-BIDMC/MGH-SITC 2012
Treatment Selection in Patients with BRAF Mutant Melanoma: Conclusions
Current data suggests that for many patients with BRAFV600E melanoma (asymptomatic, immune infiltrate), starting with immunotherapy offers them a chance for longterm benefit without compromising their benefit from subsequent BRAFi therapy
Two shots on goal are better than one
E1612: Ipi vs Vemurafenib
ECOG PS1. 02. 1
Stage 1. St III or
M1a/b2. M1c
Prior therapy1. No prior Rx2. Prior Rx
RANDOMIZE
Arm 1:
Ipi 3 or 10mg/kg q 3wks x 4 +/- maint q12 wks
Arm 2:
Vemurafenib 960mg BID
ECOG and SWOG protocol – Atkins, ChmielowskiTumor measurements q12 wks
ECOG and SWOG protocol – Atkins, ChmielowskiTumor measurements q12 wks
Ipi 3 or 10mg/kg q 3wks x 4 +/- maint q12 wks
Vemurafenib 960mg BID
PD
PD
Treatment Selection in Patients with BRAF Mutant Melanoma: Conclusions
Current data suggests that for many patients with BRAFV600E melanoma (asymptomatic, immune infiltrate), starting with immunotherapy offers them a chance for longterm benefit without compromising their benefit from subsequent BRAFi therapy
Newer immunotherapies are approaching the efficacy (RR and PFS) of BRAFi with more durability