24
IMPAIRMENT and Disability Claims Sean Kaliski Dept of Psychiatry, UCT Forensic Mental Health Service, W Cape
| Date post: | 14-Dec-2015 |
| Category: |
Documents |
| Upload: | dallas-gateley |
| View: | 223 times |
| Download: | 5 times |

IMPAIRMENT and
Disability Claims
Sean KaliskiDept of Psychiatry, UCT
Forensic Mental Health Service, W Cape

FORENSIC PSYCHIATRY ASSESSMENTS:
1. Determine the specific juridical task that has to be achieved
2. Perform a psychiatric assessment, and determine the degree of impairment
3. Match step 2 to step 14. Comment on:
a. Response to previous interventions / treatmentsb. Prognosis etc
5. Make a recommendation, but try not to decide on the Ultimate Issues
DEFINITION OF CAPACITY• Legal context: “a person’s ability to perform a
specific juristic act”• Is a legal determination, often based on
medical evidence• Two essential (cognitive) elements:– Capacity to assimilate relevant facts– Appreciation/understanding of his/her situation as
it relates to the facts• FUNCTION-BASED CONCEPT
(South African Law Commission; 2004)
Capacity Fluctuates:
• Depends on the demands of the task• Depends on mental state• Depends on the support and assistance
available• Is on a continuum from baseline (minimum) to
optimal abilities in individuals• Therefore determination of the threshold
between Capacity and Incapacity can be difficult to determine (matter of judgement)

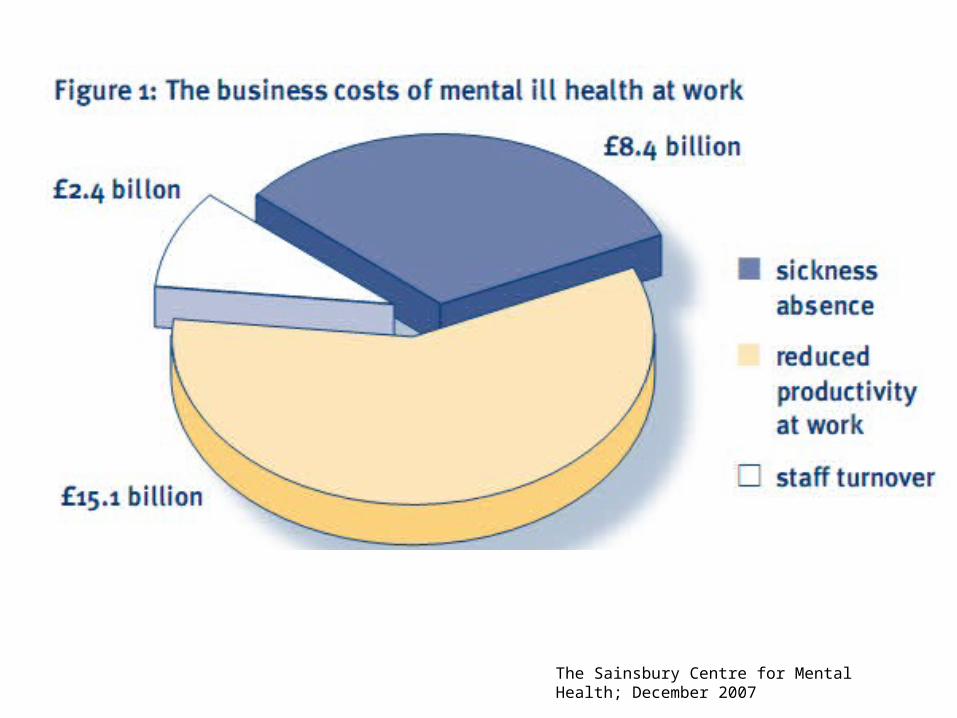
The Sainsbury Centre for Mental Health; December 2007

“J has been exposed to very poor working conditions which have caused him tremendous stress and anxiety. Apart from having to work under a junior manager (at a lower level than he), his working hours have changed and he has limited access to resources such as telephones, radios, forearms, bulletproof vests and roadworthy vehicles.
He has made several appeals to the City Manager to make his post redundant as there was no placement for him in the City. His case has dragged on for more than 4 years with no resolution.
In light of the above, it is evident that his persistent stressful working conditions have impacted significantly on his physical and mental health. It is therefore, strongly recommended that he be medically boarded”
A Recent Local sick note...
Work Phobia and sickness leave certificatesEwart- Smith, M:African J Psych:2009:12(4);249-53
‘Amazingly, several had been receiving full salary while off work on sick leave for 4 or more years, pending final adjudication of their claims. Treatment during these waiting periods typically consisted of marking time with superficial symptom suppression until the desired escape from the noxious work environment was granted..’

Work Phobia and sickness leave certificatesEwart- Smith, M:African J Psych:2009:12(4);249-53
• ‘..during long periods of absence from work, the psychiatrist issues a monthly off work certificate, a lot of certificates when the patient has been off for years.
• Or treating psychiatrist issues certificate stating patient must have 6 or 12 months off, and then medical boarding
• Internationally, anyone off for more than 6 months is unlikely to return to the open labour market
• Sick benefits are generous, and therefore there is no incentive to return to the ‘noxious workplace’.
• Prolonged sick leave is associated with 6 fold increase in suicide, decrease in psychological and physical health, breakdown in interpersonal relationships and financial hardship, ie. Deterioration in quality of life

Employment Equity Act
• Companies have to employ people with disabilities
• Companies have to accommodate people with disabilities
• Paradoxically many employees who develop a disability apply for boarding and pensions
IMPAIRMENT VS DISABLITY
• “Impairment is the alteration of normal functional capacity due to a disease, is assessed by medical means after a diagnosis has been established, and appropriate and optimal treatment applied”
• “Disability is the alteration of capability to meet the personal, social or occupational demands due to an impairment, and is assessed by non-medical means”
» (Coetzer, Emsley et al; 2001)

ASSESSMENT OF IMPAIRMENT
• Differentiate between impairment and incompetence
• Impairment should represent a change in the person’s previous level of functioning
• Can be specific for the actual demands of that job, or global (eg. Psychiatrist now not even fit to serve tea at La Perla)
• Equivalence between ADL and demands of job
• Occupational Therapy evaluation is usually useful to establish the precise deficits and to provide recommendations for accommodating the employee
TREATMENT-RESISTANCE
• All accepted methods of treatment have failed to produce an adequate response
• Each method has been given reasonable period to be effective (about 8-12 weeks)
• The longer the overall period, the more convincing: Two years is yardstick period for most psychiatric disorders!

CONFOUNDERS THAT ARE NOT ROUTINELY CONSIDERED !!
• Personality Disorder (or strong traits)– Narcissistic, Dependent, Borderline, Avoidant
• Alcohol & Substance Abuse• Disciplinary problems at work – Often advised by HR to apply for boarding or else be fired
• Person is just plain INCOMPETENT• Sociopolitical factors– Equity, Racism, perception that pension is better than
salary • Treatment is inappropriate, excessive (eg.
Polypharmacy), enhances sick role

ETHICAL RULE:
• The treating doctor should not apply for disability
• The treating physician should refer to a colleague for this purpose, or advise the employer / insurer that an non-involved psychiatrist should assess and advise on impairment, prognosis, and management.


A 33 yr Old Teacher
• Nababeep High school 1998: – Had been working there for 2 years– problems with colleagues bcs of integration of race
groups– They questioned his qualifications– Drives to CT to consult with well known
Boardiologist– After 3 consultations psychiatrist recommends
boarding bcs of depression and anxiety– Boarded in that year.

• No further consultations with psychiatrist, and stops medication
• 1999 enrolls at Technikion to do mechanical engineering, leaves course when wife injured in MVA
• For next 6 years has own restaurant in Springbok• Builds a shop: sells food • Assists friend with his local newspaper• Wants to work as teacher on contract, but wants to
be appointed • Returns to Boardiologist in 2008 who issues
certificate that he has recovered from his illness and is fit to return to teaching

Case: 39 yr old Medical Technologist
• 20 yrs of treatment for OCD– Checking behaviour: takes half an hour to get of car, 1
hour to get to bed, checks windows, doors etc repeatedly. Sleeps from exhaustion
– At work can only do one slide in about half an hour as checks the case number and culture result over and over and over and over and over and over
– Has had every antidepressant etc at heroic doses– Deep Brain stimulation suggested, but medical aid
refuses as it is considered experimental procedure• Treatment resistant and cannot work (& barely
living)
Recommendations:• Keep people at work, almost at all costs
• If the pt’s major cause of distress / stress is due to circumstances in the workplace• Refer to OT for job coaching / supported employment• Advise resignation, and possibly re-training• Do not give certificate for more than 1-2 weeks
• If pt has a serious mental illness– Provide limited sick certificate – not longer than 1 month– Advise PILAR process for longer – independent psychiatrist. Provide
latter with information about course, treatment (and response)– Assist in trying to return person to work when better– Only after at least 2 years of optimal treatment (unless has serious
illness that will deteriorate) advise assessment for permanent disability


















