Implementation and execution of civilian RDCR programs – Minnesota RDCR Donald H Jenkins, MD FACS Associate Professor of Surgery and Director of Trauma Division of Trauma, Critical Care and Emergency General Surgery Saint Marys Hospital, Rochester MN June 2013
Transcript
Implementation and execution of civilian RDCR
programs – Minnesota RDCR
Donald H Jenkins, MD FACS Associate Professor of Surgery and Director of Trauma
Division of Trauma, Critical Care and Emergency General Surgery Saint Marys Hospital, Rochester MN
June 2013
Remote Damage Control: Civilian Experience in
the Pre-Hospital Setting
No Disclosures
Objectives
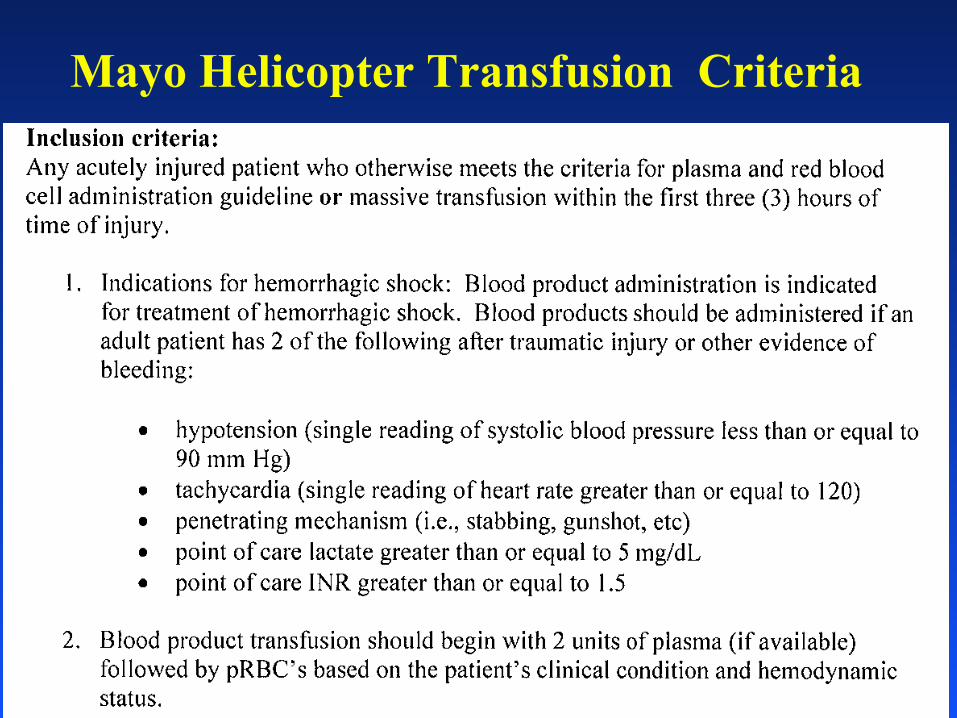
• Indications for treatment with blood products for traumatic hemorrhagic shock in the pre-hospital setting
• Monitoring devices used for coagulopathy and shock • Therapeutics utilized in these patients for pre-hospital
treatment of casualties • Evacuations of long durations compared to rapid ones • Methods of implementation to improve rapid
incorporation of recently initiated changes in practice
Remote Damage Control Resusc
• Austere/rural environment patients • Modified transfusion strategy • Different than those with scene/pre-hospital time < 30
minutes • Limited resources available • Lack of plasma availability • 40% of the population, 60% of the trauma mortality
• Current treatment options for uncontrolled hemorrhage in this environment are very limited
• >75% of combat fatalities occur in the field
Hartford Consensus February 2013
• Leaders in law enforcement, EMS, military and the American College of Surgeons
• Recommendations for civilian organizations to improve survival during active shooter scenarios
• Stress “the importance of early and definitive hemorrhage control to maximize survival in the victims….”
Hartford Consensus THREAT • T - Threat suppression • H - Hemorrhage Control • RE - Rapid Extraction to safety, • A - Assessment by medical providers • T - Transport to definitive care
Coagulopathy on Presentation
• An initial INR ≥ 1.5 reliably predicts those military casualties who will require MT.
• Pts who have a significant injury present with a coagulopathy.
• Severity of injury and mortality is linearly associated with the degree of the initial coagulopathy.
- Schreiber MA, Perkins JP, Kiraly L, Underwood SJ, Wade CE, Holcomb JB. Early Predictors of Massive Transfusion in Combat Casualties. Submitted, J Trauma. - Brohi K, et al. Acute traumatic coagulopathy. J Trauma. 2003.
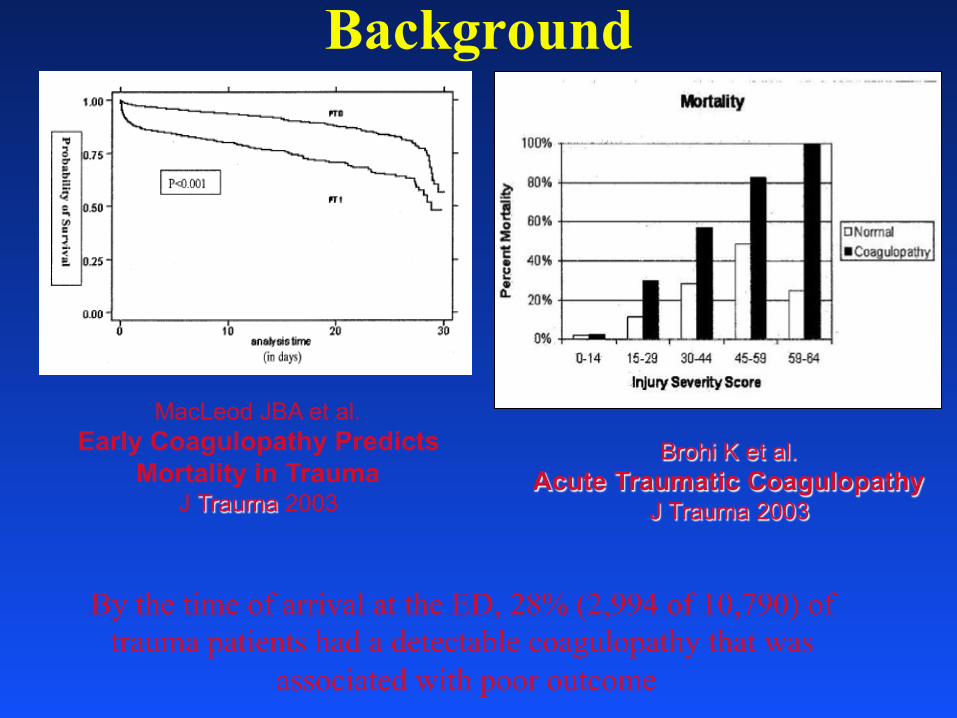
Background
MacLeod JBA et al. Early Coagulopathy Predicts
Mortality in Trauma J Trauma 2003
Brohi K et al. Acute Traumatic Coagulopathy
J Trauma 2003
By the time of arrival at the ED, 28% (2,994 of 10,790) of trauma patients had a detectable coagulopathy that was
associated with poor outcome
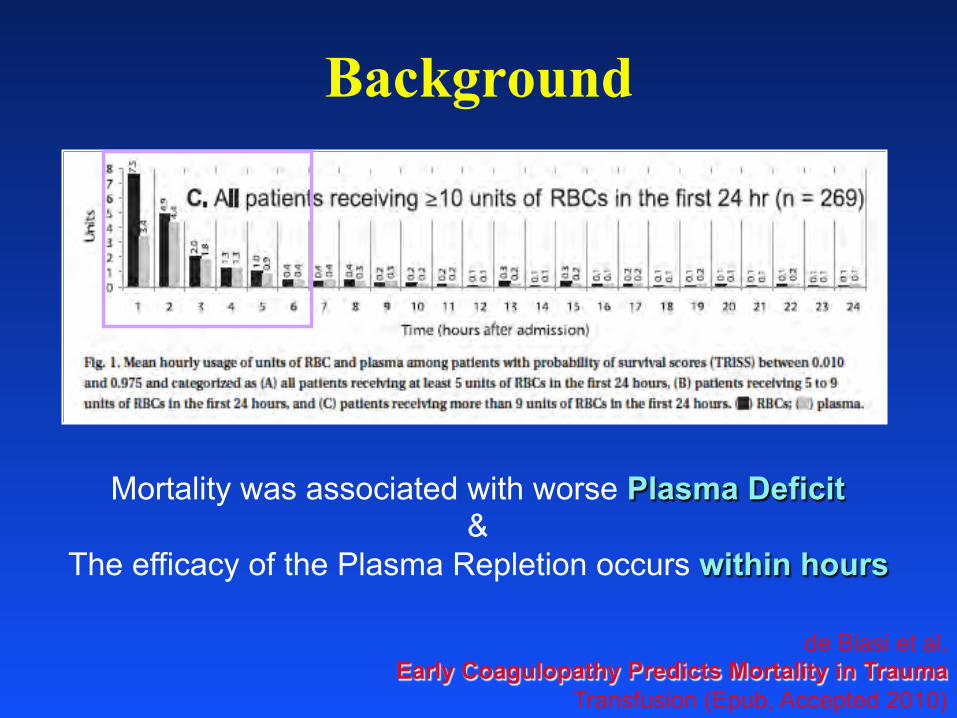
Background
de Biasi et al. Early Coagulopathy Predicts Mortality in Trauma
Transfusion (Epub, Accepted 2010)
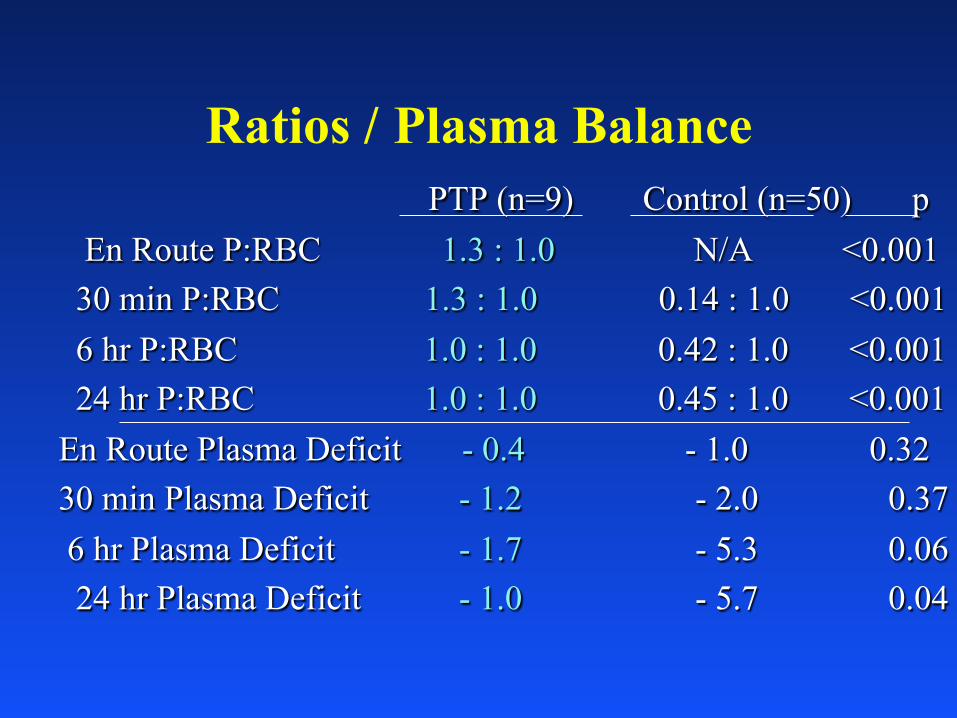
Mortality was associated with worse Plasma Deficit &
The efficacy of the Plasma Repletion occurs within hours
DoD Learned About Thawed Plasma
• Thawed plasma is FFP that is kept for up to 5 days at 4°C • This product should be present upon arrival of the casualty in
the ED • should be used as a primary resuscitative fluid started in the ED
• This approach not only addresses the metabolic abnormality of shock, but initiates reversal of the coagulopathy present in the ED.
• Thawed plasma is used in theater • The DoD Level 1 trauma center uses this product
• Decreases waste by 60-70%
- Malone DL, Hess JR, Fingerhut A. Comparison of practices around the globe and suggestion for a massive transfusion protocol. J Trauma, 2006. - Armand R, Hess JR. Treating coagulopathy in trauma patients. Transfus Med Rev 2003.
Early Use of Blood in the Pre-hospital Setting
• Mayo Clinic Experience • 1993-96 retrospective review • Criteria: Hgb<10, shock, hypotension after
resuscitation • ~2100 helicopter flights, 94 patients received
PRBC’s (4%, 91% interfacility transfer) • 48% trauma patients, 25% GI bleed, 38% AAA • Hgb increased from 8.9 to 10.2 after 2 PRBC • No transfusion reactions or complications • Average 12 u PRBC after admision • Age of RBC is < 14 days
Air Med J 1998 Zietlow and Berns
Age of Blood and Procoagulant Microparticles
• Historically, PCMP increases with age of blood
• 52 trauma patients vs 22 volunteers • Higher PCMP with injury; no difference
between transfused (n=19)/not transfused • 24 hour PCMP decreased with transfusion
• No decrease if no transfusion • Difference widened with increasing transfusion
Spinella Crit Care 2009 Jy Transfusion 2011 Rubin Transfusion 2010-12
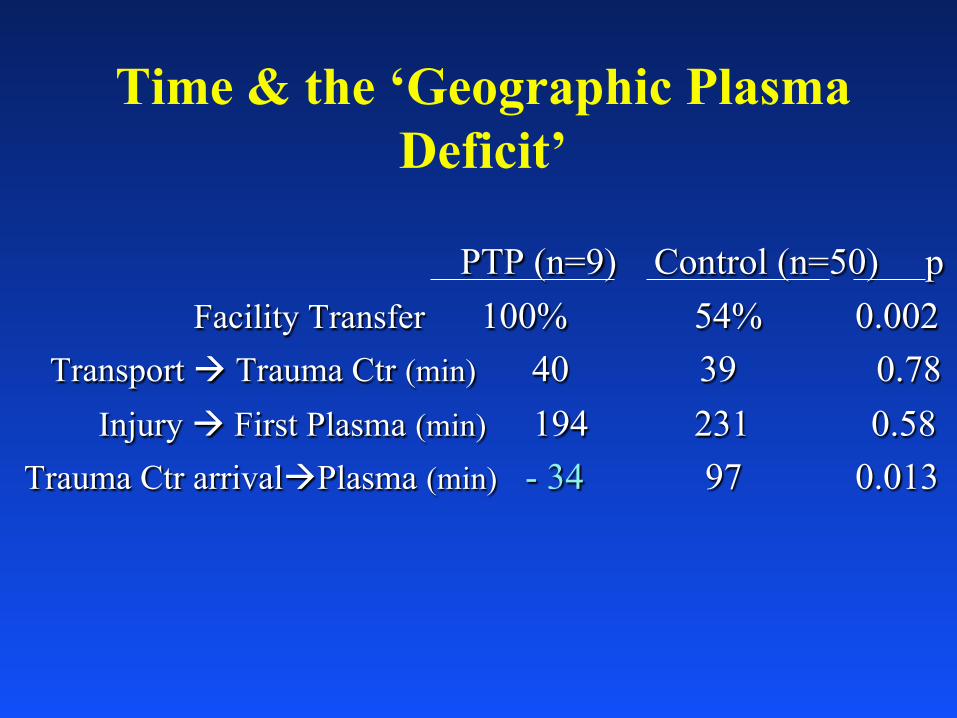
PTP (n=9) Control (n=50) p Facility Transfer 100% 54% 0.002 Transport à Trauma Ctr (min) 40 39 0.78 Injury à First Plasma (min) 194 231 0.58 Trauma Ctr arrivalàPlasma (min) - 34 97 0.013
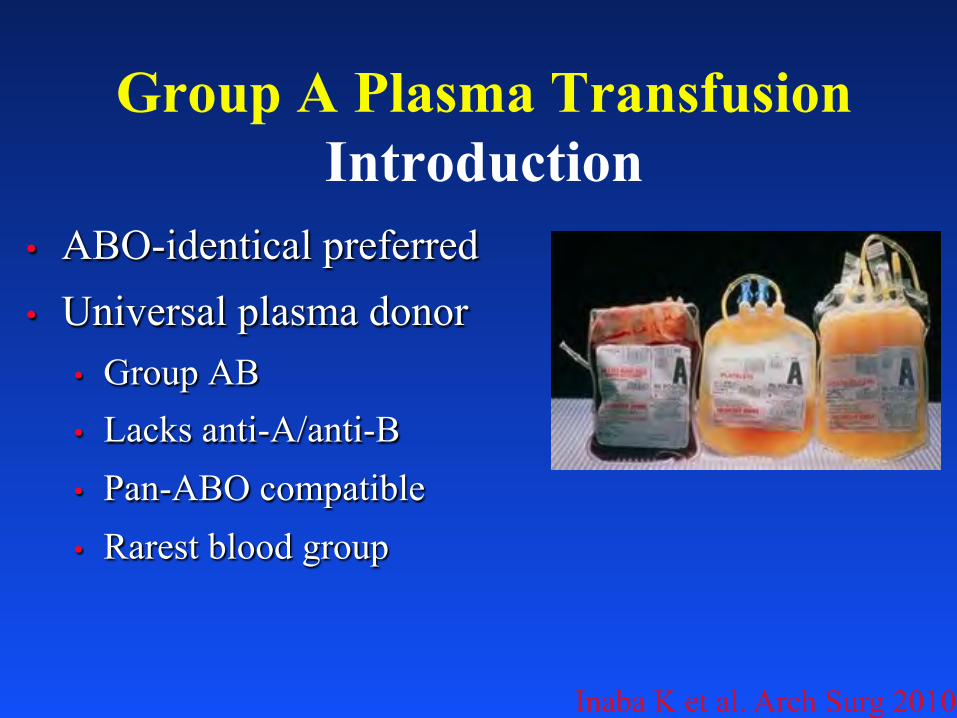
• Group AB • Lacks anti-A/anti-B • Pan-ABO compatible • Rarest blood group
Group A Plasma Transfusion Introduction
Inaba K et al. Arch Surg 2010
Group A Plasma Transfusion Group AB supply
• Recent safety data • ABO incompatible platelets
• 1 – 2 plasma units
• 1 in 9000 hemolysis
• Group O
• Immunosuppression
Isaak EJ et al. Immunohematology 2011 Josephson CD et al. Transfus Apher Sci 2010
• 10,206 patients over study period • Trauma patient • July 2008 – June 2012 • ≥ 1 unit emergency release plasma (group A
plasma) • 258 emergency release plasma (2.5%)
• 4 died prior to blood grouping
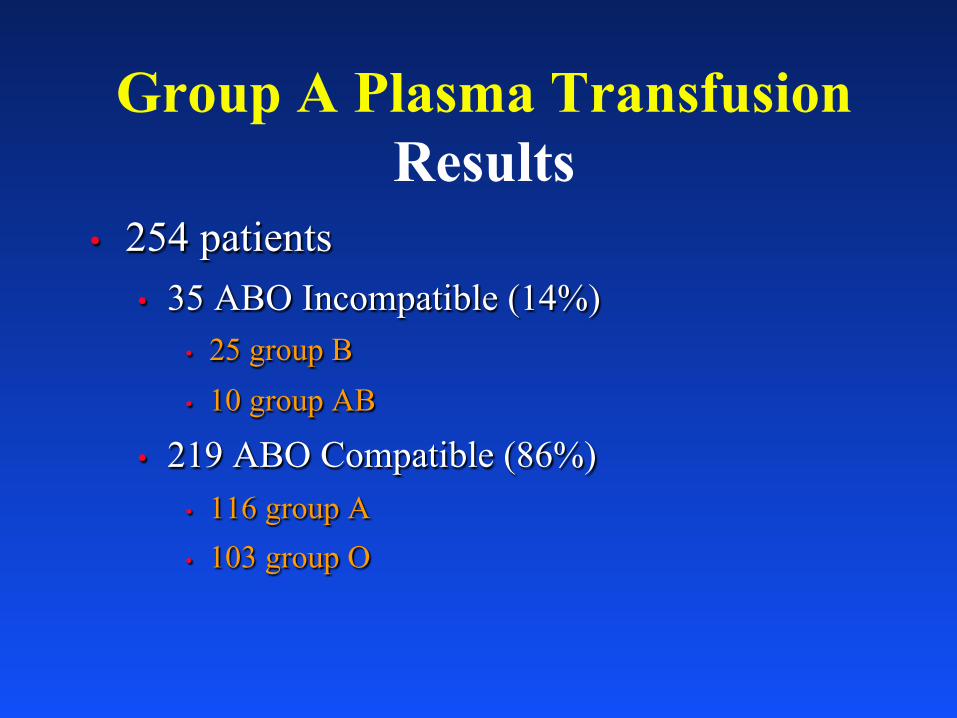
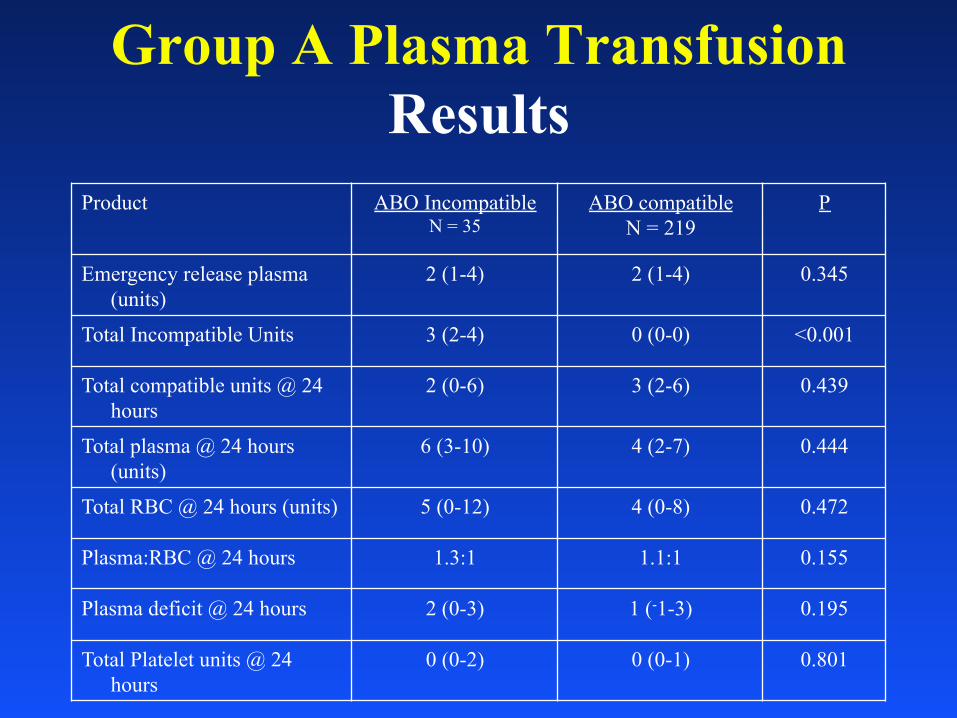
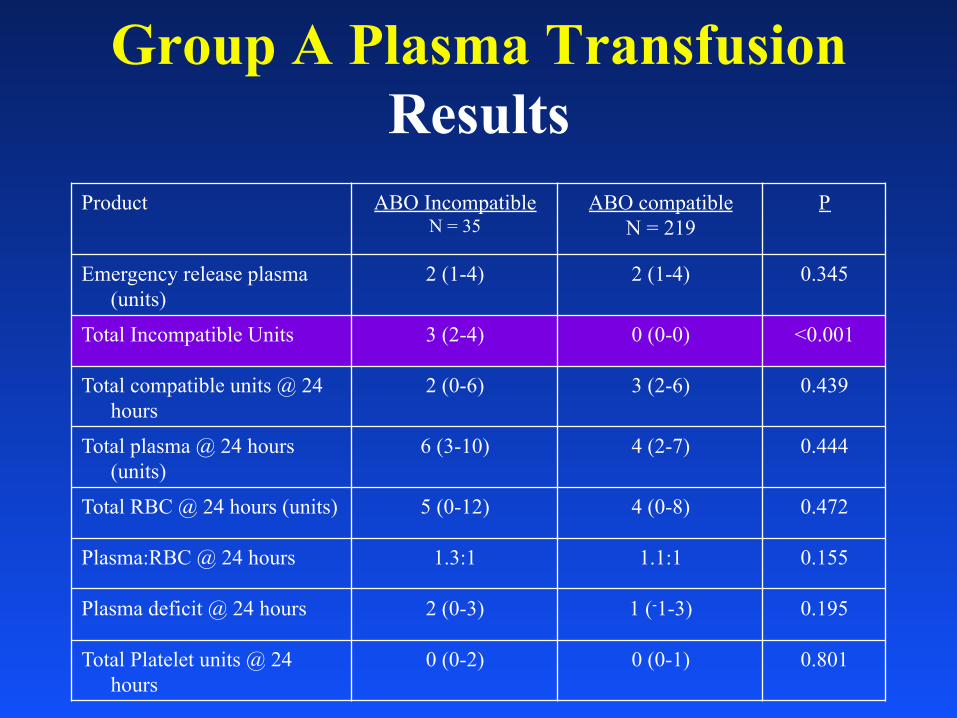
Group A Plasma Transfusion Results
• 254 patients • 35 ABO Incompatible (14%)
• 25 group B • 10 group AB
• 219 ABO Compatible (86%) • 116 group A • 103 group O
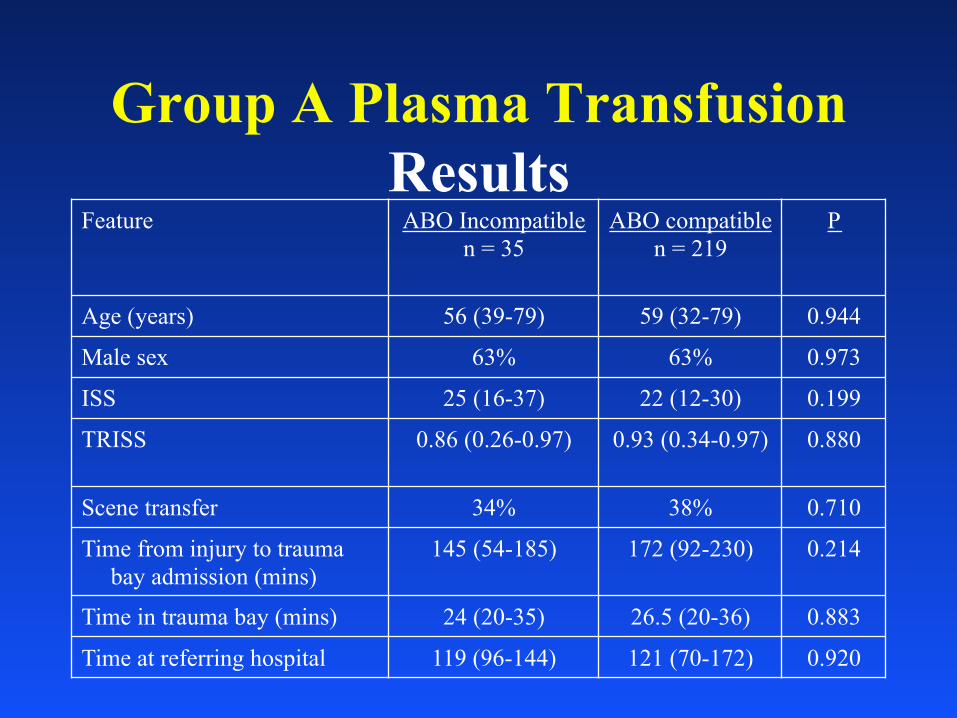
Group A Plasma Transfusion Results
Feature ABO Incompatible n = 35 ABO compatible
n = 219 P
Age (years) 56 (39-79) 59 (32-79) 0.944 Male sex 63% 63% 0.973 ISS 25 (16-37) 22 (12-30) 0.199 TRISS 0.86 (0.26-0.97) 0.93 (0.34-0.97) 0.880 Scene transfer 34% 38% 0.710 Time from injury to trauma
bay admission (mins) 145 (54-185) 172 (92-230) 0.214 Time in trauma bay (mins) 24 (20-35) 26.5 (20-36) 0.883 Time at referring hospital 119 (96-144) 121 (70-172) 0.920
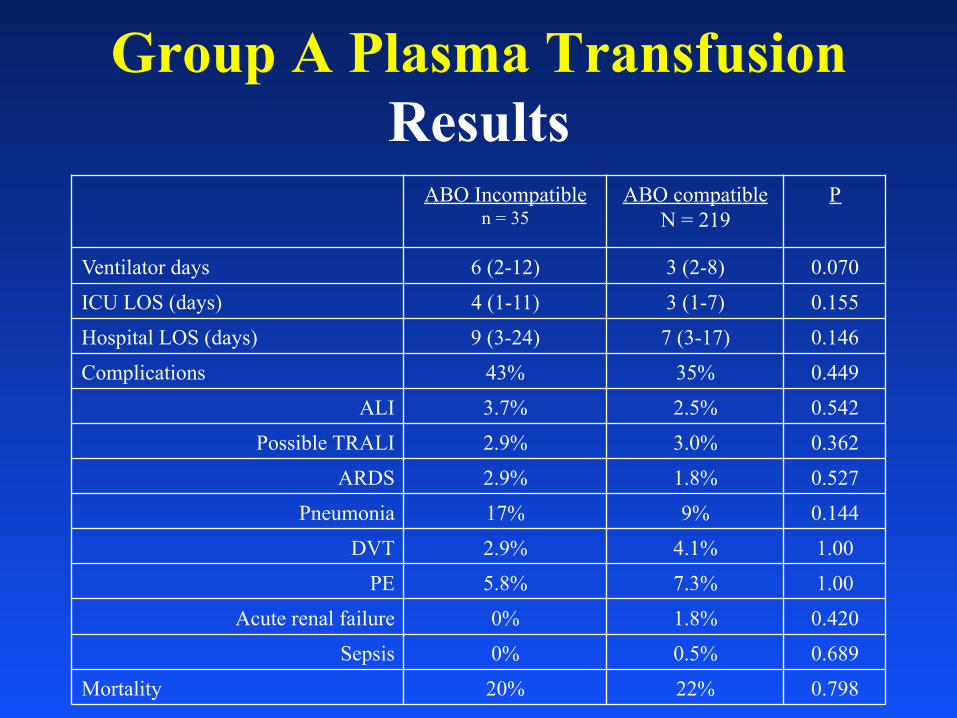
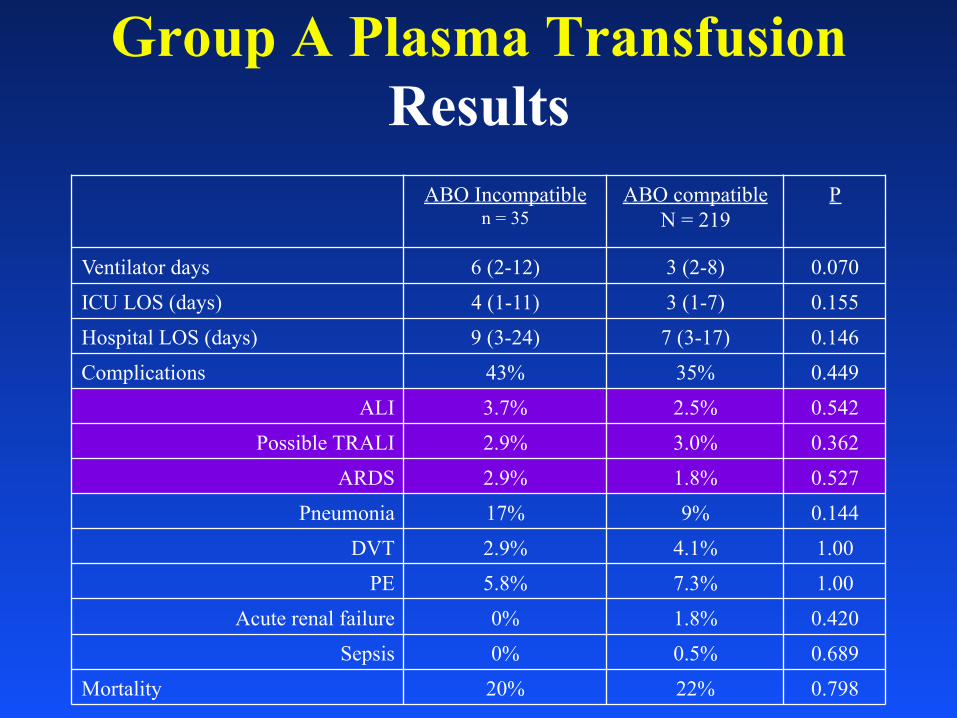
Group A Plasma Transfusion Results
Group A Plasma Transfusion Results
ABO Incompatible n = 35 ABO compatible
N = 219 P
Ventilator days 6 (2-12) 3 (2-8) 0.070 ICU LOS (days) 4 (1-11) 3 (1-7) 0.155 Hospital LOS (days) 9 (3-24) 7 (3-17) 0.146 Complications 43% 35% 0.449
ALI 3.7% 2.5% 0.542 Possible TRALI 2.9% 3.0% 0.362
donor resulted in 97.6% reduction in AB plasma use
Group A Plasma Transfusion Discussion
• Group A plasma has equivalent outcomes to group AB • Incompatible transfusions occurred • No hemolytic reactions • Similar mortality • Similar immunogenic complications
• Limitations
• Small comparison group
• Type II error potential
• Post-hoc analysis
43
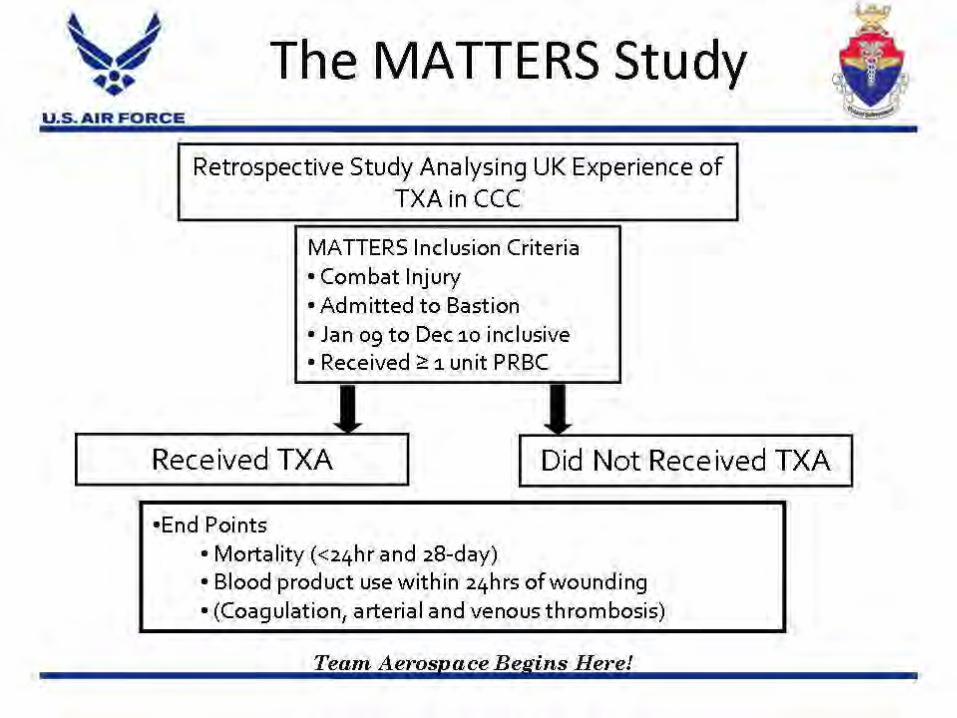
CRASH-2 Study Lancet, Online Article, 2010
• Prospective, randomized controlled trial • 20,211 patients • TXA significantly reduced all cause mortality from 16.0% to
14.5% • TXA significantly reduced death due to bleeding from 5.7% to
4.9% 43
44
45
StO2
Beilman Study • Over a 15-month period, seven Level I trauma centers in
the USA enrolled 383 patients, 50 of whom developed MODS
• StO2 below 75% indicates serious hypoperfusion in trauma patients
• 78% of patients who developed MODS, and 91% of patients who died, had StO2 below 75% in the first hour
• Trauma patients who maintained StO2 above 75% within the first hour had an 88% chance of MODS-free survival
J Trauma 2006
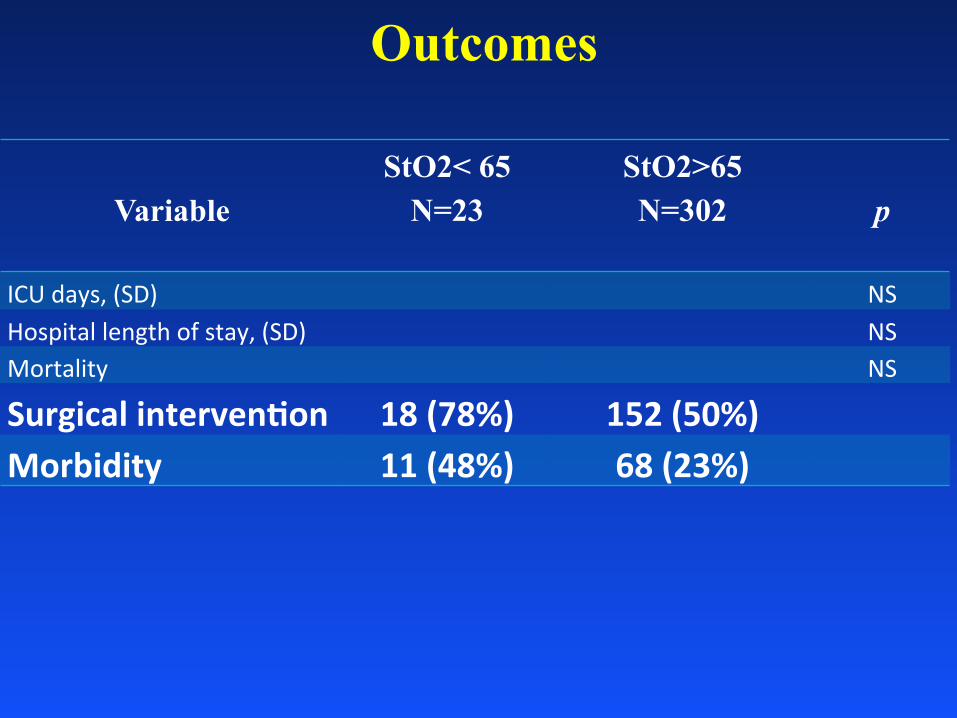
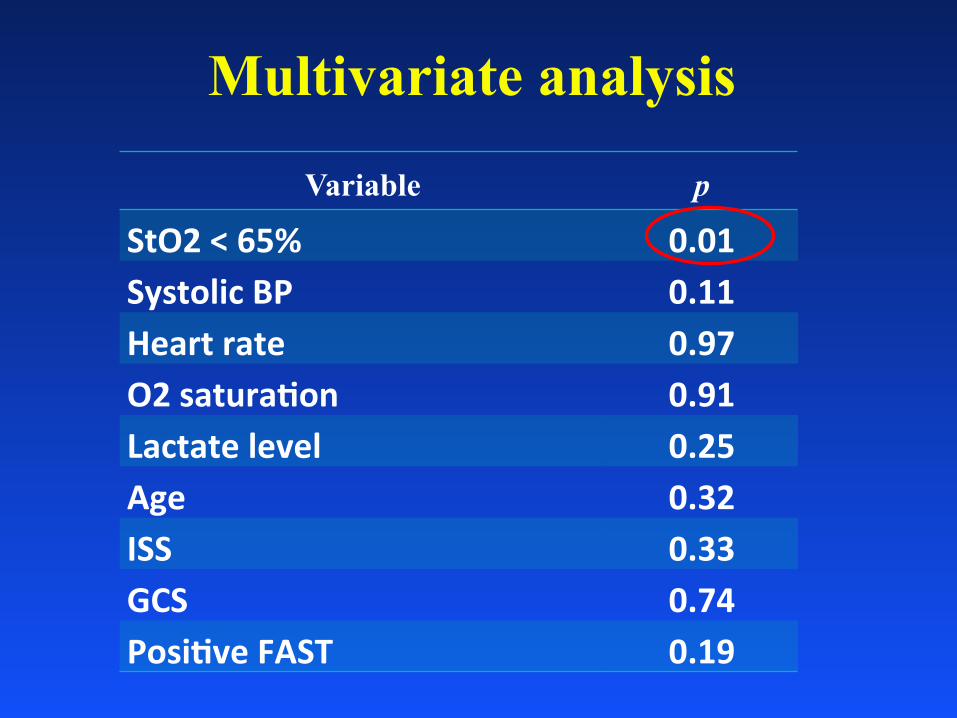
Can early StO2 predict the need of blood product requirement in trauma
population?
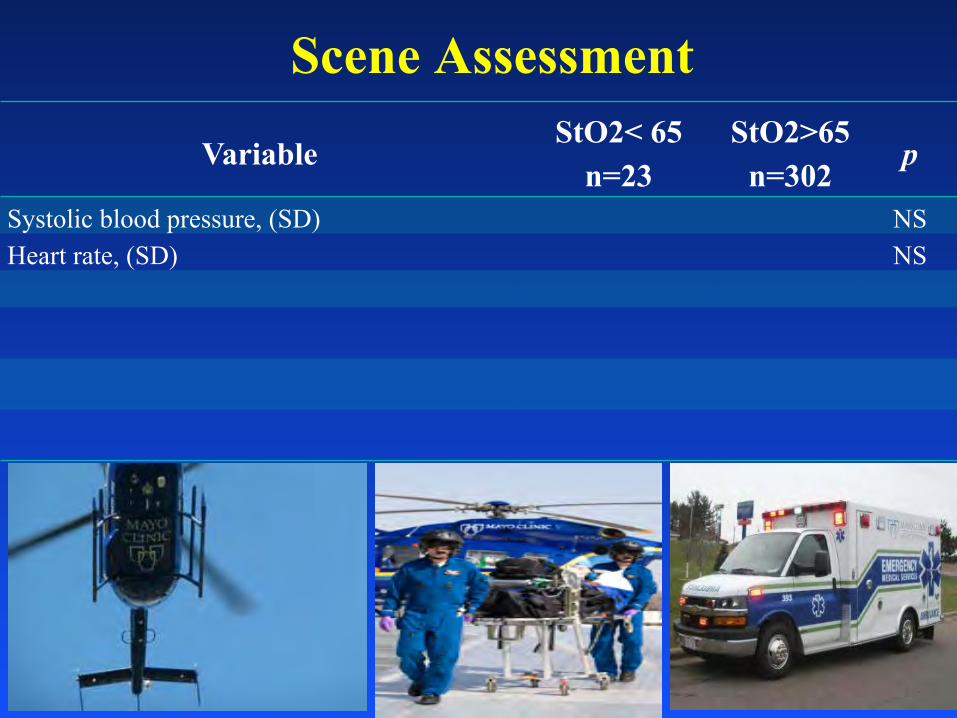
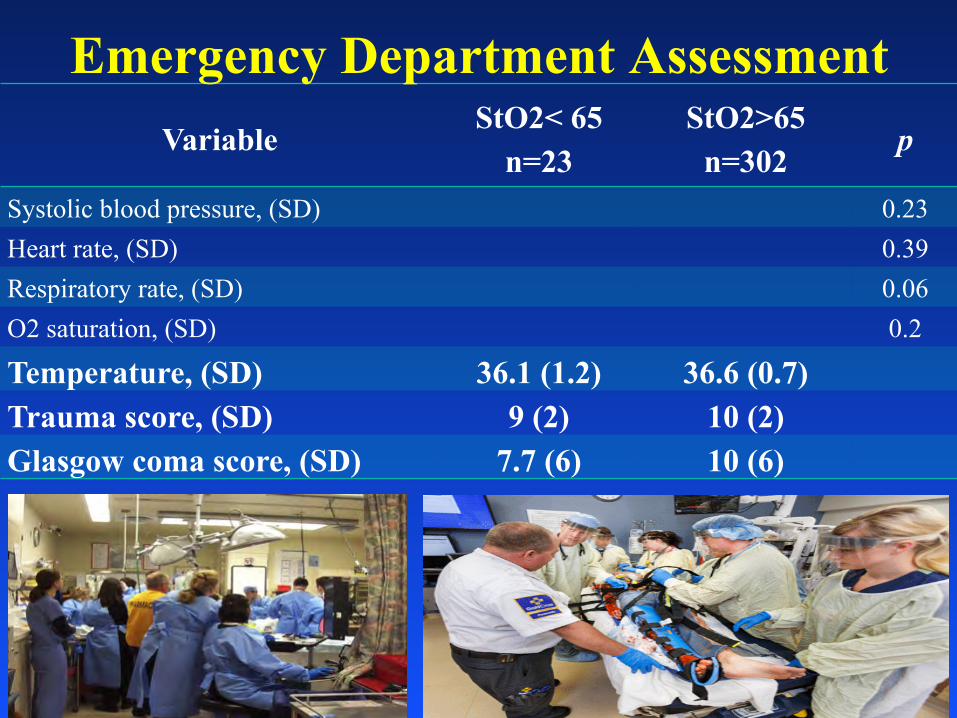
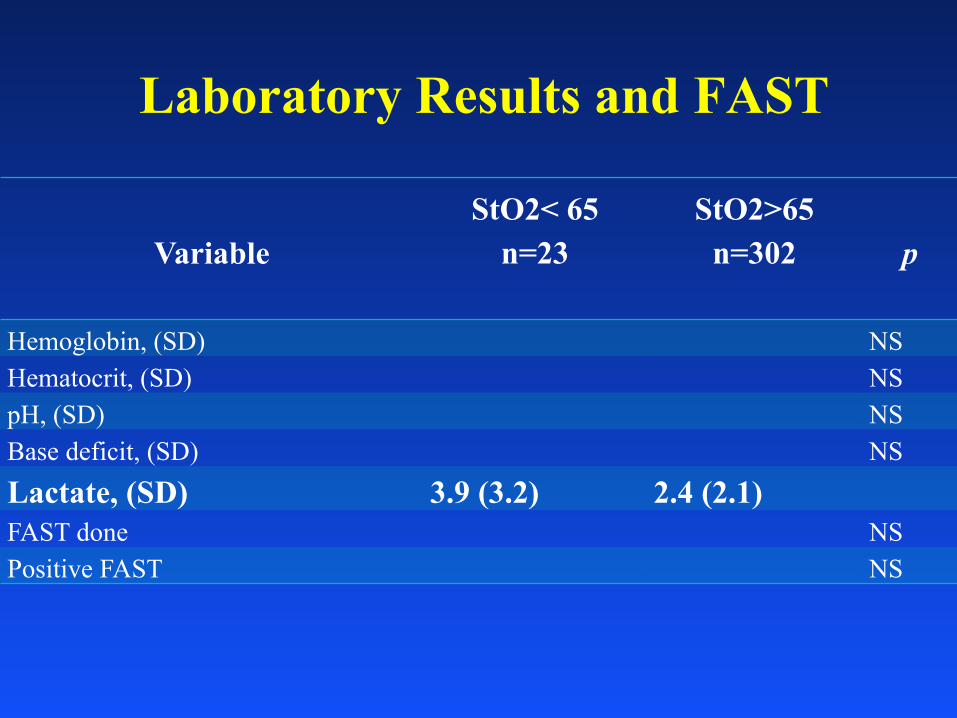
Total 632 level 1 trauma 325 patients with recorded StO2
StO2 < 65% 0.01 Systolic BP 0.11 Heart rate 0.97 O2 satura.on 0.91 Lactate level 0.25 Age 0.32 ISS 0.33 GCS 0.74 Posi.ve FAST 0.19
Current Status • All 3 Mayo helicopter bases carrying 3 PRBC
and 3 thawed plasma • All 3 use same transfusion triggers • All 3 use i-Stat INR and ABG cartridges • All 3 carry TXA; uses similar triggers but has
some limitations for use • Just added StO2 as a trigger • Limited waste at all 3 sites • No crystalloid for those with hemorrhage • Tourniquets and Combat Gauze on all 3 ships
Implementation of Change • Consensus • Review of the literature and our own data • Practicality and safety are first order of
business with best interest of patient in mind • Continuous monitoring of program • Education of all health care providers • Willingness of blood bank and transfusion
medicine to consider novel use of products
Overall System Results • Current era (2011) compared to the era
before pre-hospital plasma • Referrals up (838 vs 998*) • ISS up (9 vs 12*) • Mortality same (2.5% vs 2.2%) • Observed decline open abdomen (under study) • Observed decline in massive tx (under study) • Arrival TEG improved? (under study)
Summary • Trauma patients die from shock • Our job is to limit preventable trauma death • First, identify the patient in shock • Pre-hospital resuscitation with plasma can
prevent the trauma induced coagulopathy and limit the risk of death due to hemorrhage
• Making dried plasma available in the rural and pre-hospital/austere environment will save lives