Implementing PCMH in a Safety Net Implementing PCMH in a Safety Net Clinic by Evolving the Role of RNs at Clinic by Evolving the Role of RNs at Union Square Family Health Union Square Family Health Cambridge Health Alliance Cambridge Health Alliance
Transcript
Implementing PCMH in a Safety Net Implementing PCMH in a Safety Net Clinic by Evolving the Role of RNs at Clinic by Evolving the Role of RNs at
Union Square Family Health Union Square Family Health
Cambridge Health AllianceCambridge Health Alliance
About Union SquareAbout Union Square
Somerville MASomerville MAAll FM MDs, no midAll FM MDs, no mid--levelslevels26,000 patient visits per year26,000 patient visits per year40% Portuguese speaking 40% Portuguese speaking 20% Spanish Speaking 20% Spanish Speaking 8% Haitian Creole Speaking 8% Haitian Creole Speaking smaller populations of Hindi, Nepali and smaller populations of Hindi, Nepali and EnglishEnglish
Union SquareUnion Square’’s Journeys Journey
Level 3 certified Medical HomeLevel 3 certified Medical HomeTeam care structure since 2005Team care structure since 2005
New Clinic ManagerNew Clinic Manager
Observing RN roles, tasks, & daily activities:Observing RN roles, tasks, & daily activities:On 2On 2--3 PCP teams and primarily responsible for Abnl PAPs, Mammos and 3 PCP teams and primarily responsible for Abnl PAPs, Mammos and Depression outreachDepression outreachOverall, RNs pulled away from this kind of work into triage, shoOverall, RNs pulled away from this kind of work into triage, shots, walkts, walk--in visits, in visits, clerical tasks not appropriate to RNs, calling patients with resclerical tasks not appropriate to RNs, calling patients with resultsults
Evolving RN roles to optimize RN skillsEvolving RN roles to optimize RN skillsIdentify the new roles & tasksIdentify the new roles & tasks
–– Training needs for RNs to support new roleTraining needs for RNs to support new role5 part Didactic Diabetic series Training5 part Didactic Diabetic series TrainingMotivational Interview TrainingMotivational Interview Training
75% felt that they know what is expected 75% felt that they know what is expected of them at workof them at work50% agree that they have the opportunity 50% agree that they have the opportunity to do what they do best every dayto do what they do best every day100% felt there was someone at work 100% felt there was someone at work that encourages their developmentthat encourages their development75% felt that their opinion counted75% felt that their opinion counted100% felt that they did not receive 100% felt that they did not receive recognition for good workrecognition for good work
The New Role of the RN at CHAThe New Role of the RN at CHA
Increase the time for RNs to focus on:Increase the time for RNs to focus on:
Care management, specifically with high risk patient groups; Care management, specifically with high risk patient groups; choose first group of High Risk patients to focus on: Diabeticschoose first group of High Risk patients to focus on: Diabetics
Direct patient care time to increase patient engagement, Direct patient care time to increase patient engagement, patient education, etc.patient education, etc.
Hired LPN to assist in task oriented jobs Hired LPN to assist in task oriented jobs
Enhance protocols and communication between PCP and RN Enhance protocols and communication between PCP and RN around health and treatment goalsaround health and treatment goals
Improve continuity of care: pts able to get appt with their Improve continuity of care: pts able to get appt with their team more quickly since RNs are now an additional providerteam more quickly since RNs are now an additional provider
Position RNs as team leadersPosition RNs as team leaders
Enhanced RN RoleEnhanced RN Role
Enhanced team based chronic and preventive Enhanced team based chronic and preventive care by integrating the redefined RN role with:care by integrating the redefined RN role with:
Social WorkerSocial WorkerClinical PharmacistClinical PharmacistNutritionistNutritionistPlanned Care CoordinatorPlanned Care CoordinatorSoon to comeSoon to come………….Community Outreach Worker.Community Outreach Worker
Goal:Goal:Clearly define resources for RNs to coordinate patient Clearly define resources for RNs to coordinate patient
education and empowermenteducation and empowerment
First Initiative: Diabetic PatientsFirst Initiative: Diabetic Patients
WorkFlow WorkFlow RN reviews Diabetic Patient List with Team Physician and uses RN reviews Diabetic Patient List with Team Physician and uses state Risk Stratification Tool to create High Risk Liststate Risk Stratification Tool to create High Risk ListRN/Team Receptionist outreaches to High Risk Patient via RN/Team Receptionist outreaches to High Risk Patient via phone and sets up a Nurse Visit appointment for meet and phone and sets up a Nurse Visit appointment for meet and greet, assessment of needs, and determine if engageablegreet, assessment of needs, and determine if engageableOr while patient is at clinic, physician does a Or while patient is at clinic, physician does a ““warm handwarm hand--offoff””Nurse Visit is in collaboration with the patient to establish Nurse Visit is in collaboration with the patient to establish patient needs/goals, educational requirement, and discuss patient needs/goals, educational requirement, and discuss return visitsreturn visitsteam meetings weekly with monthly break out of RN/MD/SW to team meetings weekly with monthly break out of RN/MD/SW to discuss HR listdiscuss HR listNutrition, RN, Psych, Pharmacist all on site as neededNutrition, RN, Psych, Pharmacist all on site as needed
MultiMulti--Disciplinary Case ConferencesDisciplinary Case Conferences
BiBi--monthly and attended by site RNs, monthly and attended by site RNs, central CDE, SW, pharmacy, PCP, central CDE, SW, pharmacy, PCP, Ambulatory RNs in rotation (spread to Ambulatory RNs in rotation (spread to other sites)other sites)Single case presented; the team helps the Single case presented; the team helps the RN Care Manager with any challenging or RN Care Manager with any challenging or outstanding issuesoutstanding issues
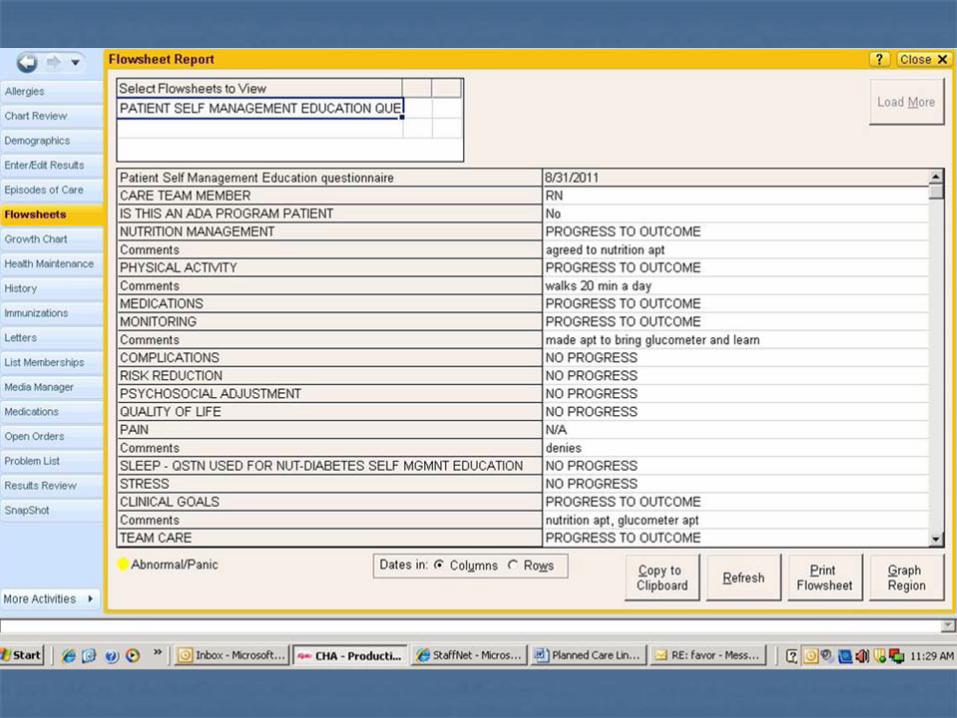
Tools for RN to provide Tools for RN to provide EducationEducation
Involve IT to help the RNInvolve IT to help the RN’’s work s work more efficientmore efficient
Results & AchievementsResults & Achievements
Outcomes of USFH Diabetes Pilot Outcomes of USFH Diabetes Pilot From July 2011 to Nov 2011From July 2011 to Nov 2011
Improved RN confidence in managing diabetes and Improved RN confidence in managing diabetes and high risk patientshigh risk patientsTotal 140 high risk patients being cared for by 4 RNs, Total 140 high risk patients being cared for by 4 RNs, 100 diabetic visits over 6 months100 diabetic visits over 6 monthsImproved diabetes outcomes over 6 month period:Improved diabetes outcomes over 6 month period:--13% increase in percent of A1c levels < 7% 13% increase in percent of A1c levels < 7% --20% decrease in percent of A1c levels > 9%20% decrease in percent of A1c levels > 9%
18% more patients engaged as active in the registry18% more patients engaged as active in the registry
Increase in Diabetic PatientsIncrease in Diabetic Patients
0
50
100
150
200
250
300
350
2010-07
2010-08
2010-09
2010-10
2010-11
2010-12
2011-01
2011-02
2011-03
2011-04
2011-05
2011-06
2011-07
2011-08
2011-09
2011-11
2011-12
2012-01
Num
ber
Time
Numbers of Diabetics at USFH
# of Diabetic Patients
# of Diabetic Patients
RN Care Mgmt
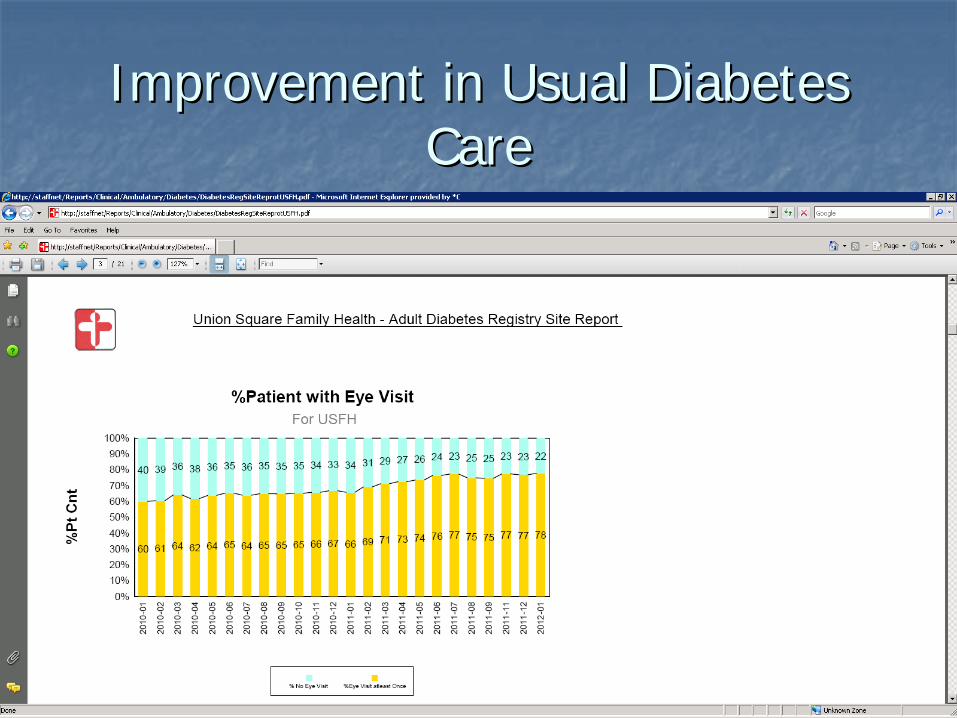
Improvement in Usual Diabetes Improvement in Usual Diabetes CareCare
USFH Depression Outreach USFH Depression Outreach (Sustaining Past Initiatives while adding on (Sustaining Past Initiatives while adding on
New Initiatives)New Initiatives) Goal: 3 Goal: 3 ““ContactsContacts”” within 16 week periodwithin 16 week period
0%
10%
20%
30%
40%
50%
60%
Sep-
09
Oct
-09
Nov
-09
Dec
-09
Jan-
10
Feb-
10
Mar
-10
Apr
-10
May
-10
Jun-
10
Jul-1
0
Aug
-10
Sep-
10
Oct
-10
Nov
-10
Dec
-10
Jan-
11
Feb-
11
Mar
-11
Apr
-11
May
-11
Jun-
11
Jul-1
1
Aug
-11
Sep-
11
Oct
-11
Nov
-11
Dec
-11
Jan-
12
Feb-
12
Mar
-12
Apr
-12
May
-12
Jun-
12
Jul-1
2
Aug
-12
Sep-
12
Oct
-12
Nov
-12
Dec
-12
CHA Goal
USFH
What has this meant for patients?What has this meant for patients?
““JoeJoe”” is a 72yo gentleman with poorly controlled diabetesis a 72yo gentleman with poorly controlled diabetesHomeless, disabled veteran, bad arthritis in his knees, used Homeless, disabled veteran, bad arthritis in his knees, used to eat ice cream every night, 1 lb pasta weekly, Dunkin to eat ice cream every night, 1 lb pasta weekly, Dunkin Donuts Donuts –– 1 donut/day, drank regularly1 donut/day, drank regularly
Autumn, RN, engaged him, educated him, worked on Autumn, RN, engaged him, educated him, worked on increasing his motivation. His goal was to no longer be increasing his motivation. His goal was to no longer be diabetic. First steps: ice cream every other day and to get diabetic. First steps: ice cream every other day and to get his questions about nutrition answered.his questions about nutrition answered.Referred him to nutrition, went 3x Referred him to nutrition, went 3x –– found very helpfulfound very helpfulConnected him to Senior Care Options with assistance of Connected him to Senior Care Options with assistance of Social WorkerSocial Worker
Joe, 6 months laterJoe, 6 months laterA1C 10.3 A1C 10.3 7.8 7.8 5.85.8, LDL 159 , LDL 159 90; weight 230 90; weight 230 200 lbs 200 lbs over a 3month periodover a 3month period
Now he has a home, goes to AA twice a week, connected to Now he has a home, goes to AA twice a week, connected to community servicescommunity services
With his weight loss, his knees no longer hurt With his weight loss, his knees no longer hurt –– he walks he walks everywhere. His transportation issues are no longer a everywhere. His transportation issues are no longer a barrier for him.barrier for him.
No longer needs his diabetes medicines No longer needs his diabetes medicines –– A1C down to 6.0.A1C down to 6.0.
Autumn: Autumn: ““It was so good for me as a nurse to learn not to It was so good for me as a nurse to learn not to have any judgments about what patients can accomplish. have any judgments about what patients can accomplish. It has been so amazingly rewarding and inspiring for me to It has been so amazingly rewarding and inspiring for me to follow up with him and to see that this was somebody who follow up with him and to see that this was somebody who might not have been able to make those changes without might not have been able to make those changes without that support.that support.””
Spreading to other CHA sites: Spreading to other CHA sites: Lessons Learned Lessons Learned
Keep the focus on the patient to facilitate changeKeep the focus on the patient to facilitate change
Importance of constant communicationImportance of constant communication
Coaching Coaching
AdvocatingAdvocating
Caution: too much change at one time = STAFF ANXIETYCaution: too much change at one time = STAFF ANXIETY
LeadershipLeadership’’s role in spreads role in spread
Invest in trainingInvest in training
Next Steps for Union SquareNext Steps for Union Square
Assess training needs of all staff for further growth in Assess training needs of all staff for further growth in the Medical Home Initiativethe Medical Home Initiative
First Call Resolution with Receptionist; Accountability to complFirst Call Resolution with Receptionist; Accountability to complete work ete work requests sent to themrequests sent to them
Medical Assistant outreach on nonMedical Assistant outreach on non--emergent Emergency Room visitsemergent Emergency Room visits
RN Chronic Care Management training needs: HTN, AntiRN Chronic Care Management training needs: HTN, Anti--Coagulation, Coagulation, CHF training and protocolsCHF training and protocols
Physician culture change of delegating work to appropriate deparPhysician culture change of delegating work to appropriate department tment for outreach/clerical workfor outreach/clerical work
ReRe--assess RN job satisfaction surveyassess RN job satisfaction surveyClinic WorkflowsClinic WorkflowsEmergency Room Visit and Hospital Discharge OutreachEmergency Room Visit and Hospital Discharge OutreachKeep the momentum and excitement for this work and Keep the momentum and excitement for this work and sustain it!!!!!!sustain it!!!!!!
CONTACTCONTACT
Aimee ChevalierAimee ChevalierClinical Manager of Union Square Family Clinical Manager of Union Square Family