Improved Labor Care to Reduce Neonatal Asphyxia Jeffrey M. Smith Maternal Health Team Leader Interventions for Impact in Essential Obstetric and Newborn Care Africa Regional Meeting, 21-25 February, 2011
Transcript
Improved Labor Care to Reduce Neonatal Asphyxia
Jeffrey M. SmithMaternal Health Team Leader
Interventions for Impact in Essential Obstetric and Newborn CareAfrica Regional Meeting, 21-25 February, 2011
2
Afghanistan2002
Maternal Mortality Survey showed an MMR of 1600 MD / 100 000 LB
77% of newborns died if they were born to mothers who died
Newborn mortality and health are directly linked to maternal mortality and health
Bartlett, et al. 2005
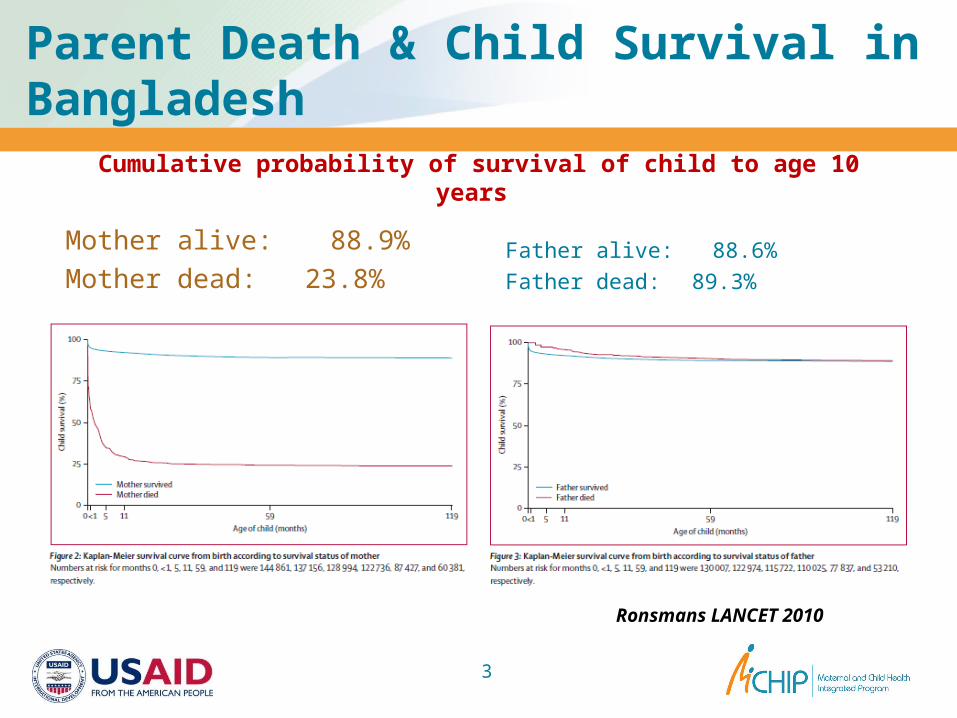
Parent Death & Child Survival in Bangladesh
Cumulative probability of survival of child to age 10 years
Father alive: 88.6%Father dead: 89.3%
3
Mother alive: 88.9% Mother dead: 23.8%
Ronsmans LANCET 2010
4
Improved maternal care will result in improved newborn outcomes
Use of evidence-based labor and delivery practices will achieve: Reduced maternal
and newborn morbidity and mortality
Improved quality of care
Respect for women and newborns
Obstetrics/Midwiferyis watchful waiting
Obstetrics – From the Latin obstare: to stand by To wait, to be vigilant, to be ready
Midwife With women
Watchful waiting • For mother, for newborn • For complications• Interventions when proven and necessary
5
Intrapartum Care to Prevent Asphyxia:
Good maternal and newborn care: Use partograph for vigilant labor
monitoring Allow companionship during labor and birth Ensure supportive 2nd stage management
based on fetal and maternal condition Avoid incorrect practices Manage pre-eclampsia correctly
Ensure skilled attendance at birth to prevent and manage asphyxia
6
Use of thePartograph
Partograph: Drugs provided
• Including oxytocin Amniotic fluid
condition Fetal heart rate
Use of Partograph combines all needed documentation
Ob and Peds leaders should ensure its use
7
Use of the Partograph
How does the Partograph prevent asphyxia? Identify abnormal heart rate
patterns Prevent prolonged labor
• Prevents unnecessary augmentation using oxytocin
Adequate hydration and nutrition during labor essential Dehydration compromises uterine blood
flow Allow women to drink freely and take
small amounts of food during labor
13
Intrapartum care to prevent asphyxia
Labor augmentation
Medical decision based on medical reasons
Use Partograph to diagnose protracted active phase
Provide oxytocin using protocols in MCPC
Do NOT allow uncontrolled oxytocin for augmentation Causes tetanic uterine
contractions Complete restriction of blood
flow to fetus
14
Intrapartum care to prevent asphyxia
Other supportive practices
Clean birthing practices/infection prevention Infected babies don’t breathe well
Doing procedures right! Vacuum extraction and breech delivery Twin delivery – management of 2nd twin
Keep normal births normal!
15
Let Babies Breathe!
Prevent asphyxia Monitor with partographCompanionship, hydration, positionPrevent eclampsia No uncontrolled oxytocin Supportive 2nd stage based on fetal condition















![Basic Emergency Obstetric and Newborn Care (BEMONC) ob part [Compatibility Mode].pdf · Outline Emergency Obstetric and Newborn Care (EmONC) as a strategy in maternal mortality reduction](https://static.documents.pub/doc/80x56/5a73d29f7f8b9ad22a8b90e9/basic-emergency-obstetric-and-newborn-care-bemonc-ob-part-compatibility-modepdfaa.jpg)
















