Improving Diabetic Foot Screening Rates in an Academic Primary Care Clinic S Hata, CL Roumie, WM Gregg, J Scott, K Hall, R Follett, P Johnston, C Brown, and GW Garriss Vanderbilt University Medical Center The speaker has no conflicts of interest to disclose pertinent to this presentation.
Transcript
Improving Diabetic Foot Screening
Rates in an Academic Primary Care Clinic
S Hata, CL Roumie, WM Gregg, J Scott, K Hall, R Follett, P Johnston, C Brown, and GW Garriss
Vanderbilt University Medical CenterThe speaker has no conflicts of interest to disclose pertinent to this presentation.
Context
Academic Chronic Care Collaborative sponsored by the AAMC
Promoted health care innovations in academic health centers
22 AHC participated in improving chronic illness care
Vanderbilt addressed diabetes care
Screening Diabetic Foot Exam
The American Diabetes Association recommends a yearly diabetic foot exam.
Early detection and intervention prevent morbidity and amputations.
Locally, our adherence to this guideline has been suboptimal.
What are you trying to accomplish?
Aims Measure our local data on documented foot
exams Improve the proportion of documented 4
element diabetic foot exams (DFE) to greater than 90%, through use of PDSA cycles to implement evidence-based guidelines
Hypothesis Percentage of completed/documented DFEs
would be improved by use of PDSA cycles to institute small tests of change in a year
How will you know a change is an improvement?
Process Measures Percent of foot exams documented
with each method• Templated note• Team DFE• Both• Other (free text writing in a note)
Outcome Measure Proportion of patients with diabetes
who have 4 element DFE documented within the past 12 months
Design and Setting
Study Design: Observational Study with multiple Plan-Do-Study-Act cycles
Setting: Adult Primary Care Clinic Vanderbilt University Medical Center, Nashville, TN
• Weak links in our system• Lost monofilaments• Forgetful, busy providers• Resistance to change
• A team approach can fix problems• Redundancy to prevent missed opportunities• Time saving for providers• “Doctor-proofed”
Summary and Implications
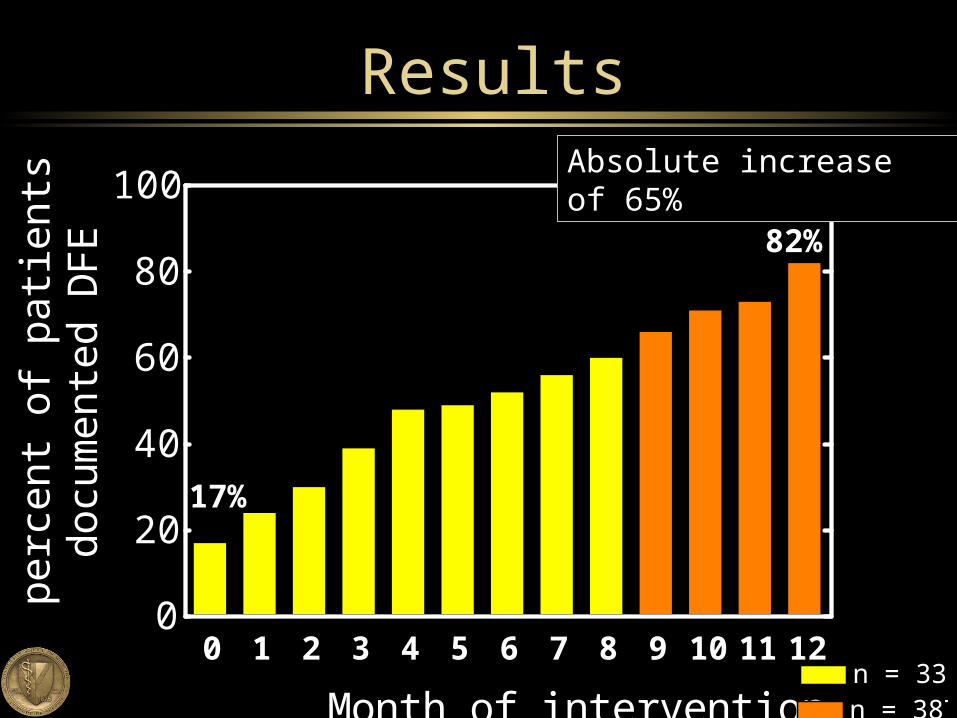
Multi-factorial interventions resulted in an absolute increase of 65% in annual DFE rate
Increased teamwork among physicians, nurses, techs
Improved quality of care for patients with diabetes
Plan to expand these interventions to all primary care clinics at Vanderbilt
Acknowledgements
Susan Hata, MD Christianne Roumie, MD MPH William Gregg, MD, MPH Julie Scott, RN Kara Hall, RN Robert Follett, BS Phil Johnston, Pharm D Charlotte Brown, BS
Excerpt of Note Template (Intervention #3)
“We are what we repeatedly do. Excellence, then, is not




























![Ken Follett - Saginaw Valley State University...Ken Follett From: Daniel Starer [dstarer@researchforwriters.com] Sent: 07 November 2000 16:34 To: Ken Follett Subject: 2of3 Dear Ken,](https://static.documents.pub/doc/80x56/611243a026737230c3353da1/ken-follett-saginaw-valley-state-ken-follett-from-daniel-starer-dstarerresearchforwriterscom.jpg)















![[eBook Ita] Yoga Hata - Sequenza Semplice](https://static.documents.pub/doc/80x56/55cf9a6f550346d033a1b57a/ebook-ita-yoga-hata-sequenza-semplice.jpg)