33
8/19/2018 1 LUNG CANCER SCREENING IMPROVING LUNG CANCER SURVIVAL IN THE COMMUNITY SETTING Scott Skibo, MD, FCCP Haywood Regional Medical Center Duke LifePoint

8/19/2018
1
LUNG CANCER SCREENING
IMPROVING LUNG CANCER SURVIVAL IN THE COMMUNITY SETTING
Scott Skibo, MD, FCCP
Haywood Regional Medical Center
Duke LifePoint

8/19/2018
2
PRACTICE LOCATION
159 Bed Hospital

8/19/2018
3
“At present, lung cancer is recognized late.
Opportunities to improve survival are through earlier
detection, accurate diagnosis, accurate localization,
and curative therapy…”
Carbone, PPNIH ConferenceAnnals of Internal Medicine (1970): 73:1003

8/19/2018
4
1. American Cancer Society: Facts and Figures 2013.
2. SEER Cancer Statistics Review; 1975-2008; National Cancer Institute, Accessed March 2013.
LUNG CANCER
SURVIVAL RATES
BY STAGE
AT DIAGNOSISat 10 years1
at 5 years2
4
|

8/19/2018
5
DIAGNOSING LUNG CANCER EARLY
of new cases have
late-stage cancer.
(Stage III or IV)
of new cases have
Early-stage cancer.
(Stage I or II)
Current State Ideal State

8/19/2018
6
SCREENING FOR LUNG CANCER: EARLY DETECTION MATTERS
• 70% of patients found to have lung cancer in the LDCT arm of the
National Lung Screening Trial (NLST) were diagnosed in the early
stages1
• Only 320 LDCT screenings are needed to prevent one death1
• In the NLST, the mortality for patients at high risk receiving LDCT
screening was reduced by 20% vs. X-ray1
• LDCT screening costs $1631 per person, or $81,0000 per quality-
adjusted year gained in comparison with with no screening2
1. N Engl J Med. 2011;365(5):395-409
2. N Engl J Med. 2014;371:1793-1802

8/19/2018
7
SO HAS THIS HAPPENED?
• USPSTF updated guidelines in 2013 recommending yearly
screening for lung cancer using LDCT
• 2015 Medicare/Insurance reimbursed test
• The importance of detecting lung cancer early and
managing incidental pulmonary nodules is well known and
accepted.

8/19/2018
8
FEWER THAN 4% OF HIGH RISK PATIENTS GET SCREENED FOR LUNG CANCER- AND
NOT CHANGED BY USPSTF GUIDELINES
• 2010 National Health Interview Survey found that only 3.3% of high
risk smokers had been screened by LDCT the previous year
• 2015 National Health Interview Survey found that only 3.9% of high
risk smokers were screened by LDCT
• In 2015, 6.8 million current and former smokers were eligible for CT
screening- only 262,700 were actually screened.
JAMA Oncology 2017;3(9):1278-1281

8/19/2018
9
IN 2016 ONLY 1.9% OF 7.6 MILLION ELIGIBLE PATIENTS UNDERWENT LDCT SCREENING
• Only 1.6% of eligible heavy smokers in the South
underwent LDCT
• Region has the most accredited screening sites
(663/1796)
• Most eligible patients (3,072,095/7,612,975)
• In contrast- 65% of women age 40 or older underwent
mammography for breast cancer screening in 2015
• Pham DC, et al, ASCO 2018, Abstract 6504

8/19/2018
10
WHY IS THE RATE OF SCREENING HIGH RISK PATIENTS SO LOW?
(THIS IS AN EVIDENCE BASED, GUIDELINE RECOMMENDED, AND MEDICARE APPROVED TEST)
WHAT CAN BE DONE TO CHANGE THIS?

8/19/2018
11
WHY IS THE SCREENING RATE SO LOW?
• Are physicians not referring enough?
• Are eligible patients not wanting screening, even if they
know a test is available?

8/19/2018
12
WHY IS THE SCREENING RATE SO LOW?(PROVIDERS)
• Knowledge of, attitudes toward, and use of LDCT for lung cancer
screening among family physicians
• 98% felt LDCT increased odds of detecting cancer at an earlier stage
• 75% felt the benefits outweighed the harms
• 76% discussed risks/benefits of LDCT in some capacity with their
patients
• >50% reported making one or no screening
recommendations in the past year
Cancer 2016;122:2324-31

8/19/2018
13
WHY IS THE SCREENING RATE SO LOW?(PROVIDERS)
• LDCT screening practices and attitudes among primary care providers
at an academic medical center
• Few PCPs ordered lung cancer screening
• 21% X-ray, 12% LDCT, 3% sputum cytology
• <50% of PCPs knew three or more of the six guideline components
for screening, and 24% knew zero
• 30% of providers doubted effectiveness of LDCT in improving
outcomes
• This study was conducted at a medical center that
participated in the NLST
Cancer Epidemiol Biomarkers Prev 2015; 24(4): 664-70

8/19/2018
14
WHY IS THE SCREENING RATE SO LOW?(PROVIDERS)
• What are the factors associated with LDCT screening utilization?
• Lack of knowledge led to a 37% inappropriate referral rate from 2013 to 20151
• Almost 2/3 of physicians are unsure whether CMS covers the cost of LDCT2
• 82% of providers are interested in learning more about lung cancer screening1
1.Prev Med Rep 2017 Jun; 6 :17-22
2. Cancer 2016;122:2324-31

8/19/2018
15
WHAT HAS BEEN LEARNED?(PROVIDERS)
• There is a well documented disconnect in moving clinical research findings into clinical practice (1981 Beta-Blocker Heart attack Trial, etc)1 - This is a evidence based, guideline recommended, Medicare covered test.
• Physician knowledge is not optimal
• Physician belief that LDCT is valuable for early detection, but a lower proportion believe that LDCT reduces lung cancer mortality2
• Physicians believe lung cancer screening to be less efficacious than other cancer screenings2
1. N Engl J Med. 2003;349:868-874
2. Cancer Epidemiol Biomarkers Prev. 2015;24:664-670

8/19/2018
16
WHY IS THE SCREENING RATE SO LOW?(PATIENTS)
• 60% of patients that qualify for LDCT screening adhered to recommendation
• Younger, white, and female patients show a trend towards better adherence1
• No difference for cancer history, residential area, level of education, type of insurance, occupation, or provider location1
• 79% of the patients that did not go through with their prescribed LDCT wanted to do one in the future1
• Fatalistic beliefs, fear of radiation exposure, and anxiety related to CT scans2
• Those who quit smoking or smoke less are more likely to be adherent1
• (smokers are less likely to seek out care for lung cancer)3
1. Prev Med Rep. 2017 Jun;6:17-22
2. Lung Cancer. 2012;77(3):526-531
3. Thorax. 2016 (PubMed PMID: 26911574)

8/19/2018
17
WHY IS THE SCREENING RATE SO LOW (PATIENTS)
Those who quit smoking or smoke less are more likely to be
adherent1
• (smokers are less likely to seek out care for lung cancer)3
• Patients may perceive screening-detected lung cancer as confirmation
of a poor lifestyle choice2
1. Prev Med Rep. 2017 Jun;6:17-22
2. Pham DC et al. ASCO 2018, Abstract 6504
3. Thorax. 2016 (PubMed PMID: 26911574)

8/19/2018
18
WHAT CAN BE DONE TO IMPROVE SCREENING RATE?
• Provider Education
• Most (82%) were interested in learning more about LDCT1
• 59% stated an on-line lecture was the preferred method1
• Focus on mortality reduction, CMS coverage
• In office decision aides
• Patient Education
• Decision aids reduce the proportion of undecided participants and appeared to have a positive effect on patient-clinician communication2
• Community outreach
1. Prev Med Rep. 2017;6:17-22
2. Cochrane Database Syst Rev. 2014;1:CD001431

8/19/2018
19
SHARED DECISION AIDS IMPROVE ADHERENCE TO LDCT SCREENING
Providers who discussed the benefits of LDCT screening with the use of shared decision aids increased screening participation from 10% to 95%1
• 1. Asian Pac. J. Cancer Prev. 2015;16(15):6293-6298

8/19/2018
20
SHARED DECISION MAKING MATERIALS

8/19/2018
21
PHYSICIAN OUTREACH/EDUCATION
= Individual practices visited

8/19/2018
22
COMMUNITY OUTREACH/EDUCATIONNEWSPAPERS
8/19/2018
23
COMMUNITY OUTREACH/EDUCATIONLOCAL TV

8/19/2018
24
COMMUNITY OUTREACH/EDUCATIONCOMMUNITY EVENTS
8/19/2018
25
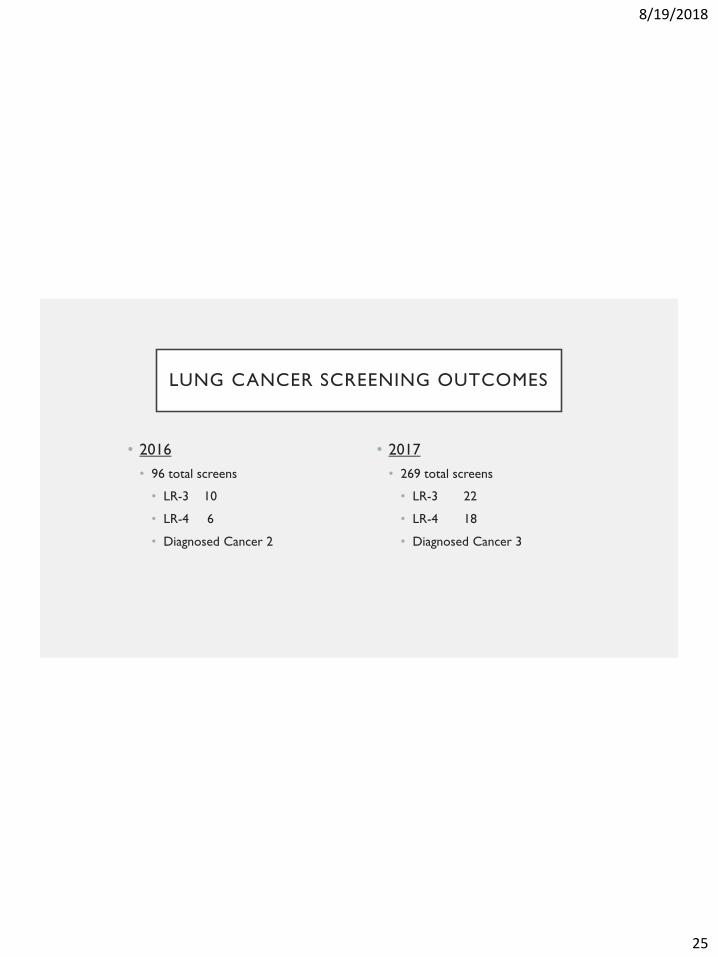
LUNG CANCER SCREENING OUTCOMES
• 2016
• 96 total screens
• LR-3 10
• LR-4 6
• Diagnosed Cancer 2
• 2017
• 269 total screens
• LR-3 22
• LR-4 18
• Diagnosed Cancer 3

8/19/2018
26
0
5
10
15
20
25
30
35
40
2016 & 2017 LDCT Screenings
2016 2017
January December
8/19/2018
27
2018 – THROUGH JULY WE HAVE SCREENED 277 PATIENTS
96 269 474

8/19/2018
28
LUNG CANCER DIAGNOSED BEFORE AND AFTER PROGRAM DEVELOPMENT (SYSTEM
WIDE)
• 2014 (Pre- ENB) • 2015 (Post-ENB)
10%
10%
32%
48%
N= 31 (20% Stage 1 and 2)
Stage 1
Stage 2
Stage 3
Stage 4
29%
27%18%
26%
N=92 (56% Stage 1 and 2)
Stage 1
Stage 2
Stage 3
Stage 4

8/19/2018
29
54% OF OUR PATIENTS DIAGNOSED
WITH NSCLC IN 2017 EITHER UNDERWENT SURGICAL RESECTION OR STEREOTACTIC RADIOSURGERY (SBRT)

8/19/2018
30
NEXT STEPS
• Improve adherence to LDCT
• QI program launched to improve efficiency of scheduling
process (automation)
• Piloting a program for same day screening.
• Revisiting primary care programs/improved shared
decision making materials
• Expand availability of LDCT screening exams beyond our
immediate market

8/19/2018
31
DIAGNOSING LUNG CANCER EARLY
56%of new cases have
early-stage cancer.
(Stage I or II)
85%of new cases have
Early-stage cancer.
(Stage I or II)
Current State Ideal State

8/19/2018
32
POLICY CHANGE IS NEEDED TO IMPROVE ADHERENCE NATIONALLY
• Make lung cancer screening a national quality health
measure for healthcare systems by CMS to optimize
reimbursement
• In 2008 CMS made mammograms for breast cancer and
colonoscopies for colorectal cancer national areas of
improvement

8/19/2018
33
QUESTIONS?

















