37
Improving nutritional care in our hospitals 4 th May 2017 BAPEN Scotland Denise Deas & Elisabeth Waterhouse Project Dietitians (Practice Development)

Improving nutritional care in our hospitals
4th May 2017 BAPEN Scotland
Denise Deas & Elisabeth Waterhouse Project Dietitians (Practice
Development)

• Nutritional care • Project over view • Study days • Facilitation • Sustained approach
Good nutritional care?
https://www.youtube.com/watch?v=w1QaThLJi_0

Good nutritional care is dependent on a co-ordinated approach to the delivery of food and fluid by all healthcare professionals. This process takes into account the individuals requirements, preferences and cultural needs. Illness, disease and/or lifestyle can have a significant impact on nutritional status by altering nutritional requirements
(NHSGGC Nutrition Resource Manual)

Background • The provision of adequate nutrition and
hydration is a fundamental cornerstone of compassionate care and a basic nursing task which is frequently overlooked (Francis, 2013)
• Good nutritional care improves disease outcomes and patients quality of life (BAPEN, 2010).
• Maximising opportunities for individuals to eat and drink and maximising quality and choice of food and fluids offered are considered to be fundamental to improving intakes (Scottish Government, 2010)

• ‘This is the challenge, but one that can be met through clear communication and coordinated actions between all those involved in the food chain including input from the patients themselves. This will be central to the success of the wider nutritional care of patients’ (Scottish Government, 2010)
Overview of project • Money from Scottish Government in 2015 • 12 month secondment ending in May
2017 • Support good nutritional care within acute
ward areas • Support evidence for Care Assurance
Standards (CAS)

Project aim By May 2017, facilitated wards within NHSGGC will demonstrate 95% compliance with safe, effective and person centred nutritional care processes in relation to Care Assurance System (CAS) standard 8.

Project Objectives • Improve staff knowledge and
understanding in basic nutrition and hydration and its impact on adult acute patients whilst in hospital
• Support accurate and meaningful nutritional screening and assessment at ward level
• Improve care planning and evaluation in relation to nutrition
• Improve compliance with the meal time bundle
Aim To improve CAS Link Nurses (standard 8) and nominated HCSW knowledge and understanding of the impact of nutrition on patient care through education and training to support improvements in nutritional care at ward level.

Content • Basic principles of nutrition and hydration
including LBM and fluid balance monitoring
• Mealtime processes/bundle including TMD and tasting session of patient meals
• Signposting to specialist nutrition related services e.g. RD, NNS and SLT
• Scenario based nutritional screening with MUST and care planning

Nutrition • Major function of food is to provide the
body with energy • Imbalance = malnutrition • 25-34% hospital admissions are at risk
(BAPEN, 2016)
• Consequences of poor nutritional intake = lean body mass (LBM)

LBM Functions
Digestion
Skin integrity
and healing
mobility
Generation
of heat
Immune function
Organ function
Hydration • Water is essential for life and maintaining the
correct balance of fluid in the body is crucial to health (RCN 2007)
• Good hydration can assist to prevent or treat many conditions including constipation, cognitive impairment, pressure ulcers and UTI’s (RCN 2007)
• There must be provision to ensure patients are able to access a minimum of 1.5 litres of fluid per day (Food in Hospitals 2010)

Mealtimes and food provision • NHS GGC Mealtime bundle
- Mealtime coordinator - Meal choice sheet - Mealtime observation tool - Patient and staff questionnaires - Identifying assistance levels

Food first approach
• Communication • Ward provisions • Promote patient experience • need for supplements

Knowledge and understanding
60
65
70
75
80
85
90
Knowledge Understanding
PErc
enta
ge
Health Care Support Workers (HCSW) mean score of knowledge and understanding pre and post study day
Pre
Post
Knowledge and understanding
70
75
80
85
90
95
Knowledge Understanding
Perc
enta
ge
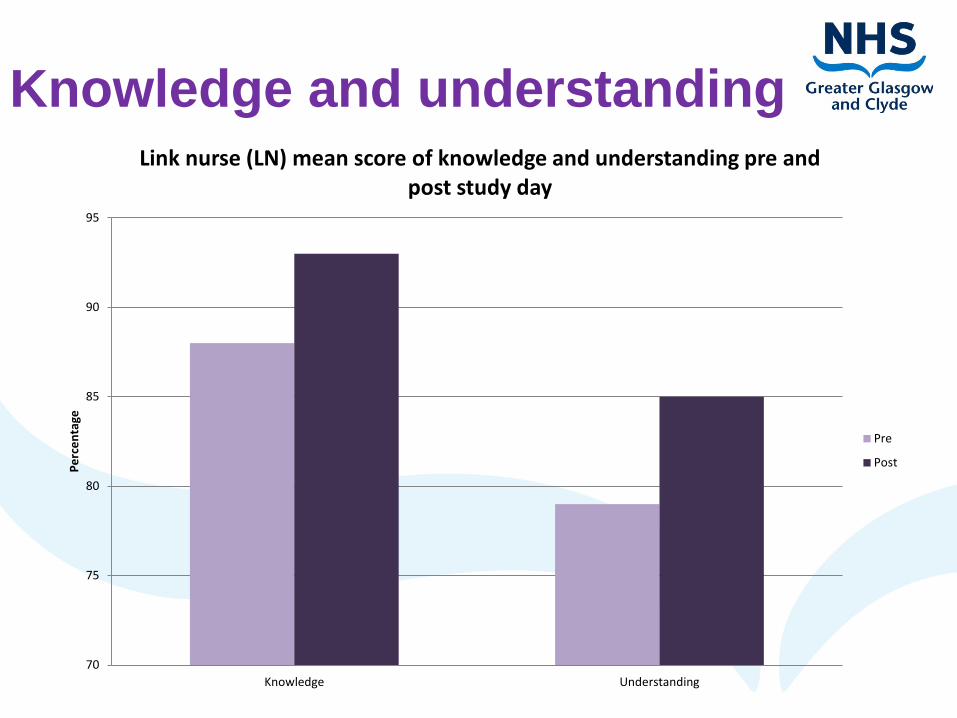
Link nurse (LN) mean score of knowledge and understanding pre and post study day
Pre
Post

Knowledge and understanding results
• 12% increase in knowledge of the link between malnutrition LBM was demonstrated by LN post study day.
• HCSW demonstrated an increased knowledge of the use of alternative measurements to obtain weights and heights pre (8%) and post study day (27%).

Confidence
0
1
2
3
4
5
6
7
8
9
10
Pre confidence in K and U Post confidence in K and U Pre confidence to championnutrition
Post confidence to championnutrition
Aver
age
con
fiden
ce le
vels
(0=
not c
nfid
ence
, 10=
ver
y co
nfid
ent)
Link nurse(LN) and health care support worker (HCSW) average confidence in nutritional knowledge and understanding and ability
to champion nutrition in practice, pre and post study day
HCSW
LN

Tasting
• Taster menu of patients food provided (produced by one of the two Central Food Production Units)
• Standardised meal choices • Choice of Soup, 3 main courses and a hot
pudding • 160 candidates who took part in the
survey

Tasting results
• >80% felt the quality of food provided was very good or excellent
• ~70% thought the quality was better than expected
• ~80% had positively changed there opinion of hospital food

Facilitation • Promoting hospital food and food first
approach • Promoting communication through
nutritional screening, care planning and catering staff
• Promoting compliance with mealtime bundle
• Promoting online training using learnpro and digital routes

Data collection results Q1 Has the patient been screened using MUST
within 24 hours of admission to hospital? • 44% (8 out of 18) of wards showed
improvement • 50% showed <10% improvement • 13% showed 10-20% improvement • 37% showed >20% improvement

Data collection results Q7 Has the patient been screened every 7
days from initial screen during hospital stay? • 33% (6 out of 18) of wards showed
improvement • 16% showed <10% improvement • 50% showed 10-20% improvement • 34% showed >20% improvement
Data collection results Q10 Is the MUST score accurate on the
current screen? • 61% (11 out of 18) of wards showed
improvement • 36% showed 10-20% improvement • 64% showed >20% improvement

Data collection results Q13 Does the patient has an appropriate
current documented nursing plan of care? • 50% (9 out of 18) of wards showed
improvement • 11% showed <10% improvement • 33% showed 10-20% improvement • 56% showed >20% improvement

Meal time observation results • 67% (12 out of 18) wards showed
mealtime improvements • Main areas of improvement - Patient hand washing - Choice of drinks with meal - Mealtime brief - Use of RAG system - Mealtime without interruptions

Meal time observation results
0
1
2
3
4
5
6
7
8
9
10
<10% 10-20% >20%
Num
ber o
f war
ds
% improvement
Number of facilitated wards showing improvements in compliance with the meal time observation tool

Sustainability • Patient centred care • Leadership • Culture change
• https://www.youtube.com/watch?v=V74AxCq
OTvg


Websites • http://www.rcgp.org.uk/policy/rcgp-policy-
areas/francis-report.aspx • http://www.bapen.org.uk/ • http://www.gov.scot/Resource/Doc/229423/0
062185.pdf • https://www.rcn.org.uk/




















