18
Improving Outcomes in Colorectal Surgery Dr. Tom Wallace General Surgeon NSQIP Surgeon Champion Enhanced Recovery Lead Royal Inland Hospital Kamloops BC
| Date post: | 22-Jan-2018 |
| Category: |
Healthcare |
| Upload: | bcpsqc |
| View: | 424 times |
| Download: | 0 times |
Improving Outcomes in
Colorectal Surgery Dr. Tom Wallace
General Surgeon
NSQIP Surgeon Champion
Enhanced Recovery Lead
Royal Inland Hospital
Kamloops BC
Royal Inland Hospital (RIH)
245 Beds Kamloops 100,000 population
100 Elective Colon Resections per year

I already do ‘best
practices’
My patients already have great
outcomes.
Challenges
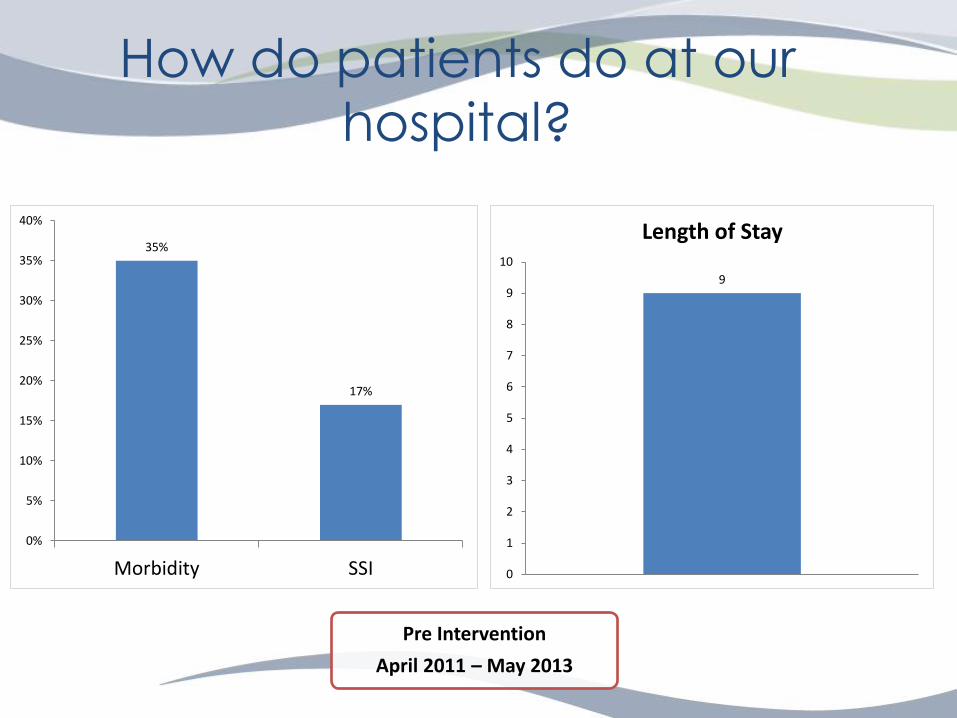
How do patients do at our
hospital?
35%
17%
0%
5%
10%
15%
20%
25%
30%
35%
40%
Morbidity SSI
9
0
1
2
3
4
5
6
7
8
9
10
Length of Stay
Pre Intervention
April 2011 – May 2013

Can we do better?
Pre Intervention
April 2011 – May 2013
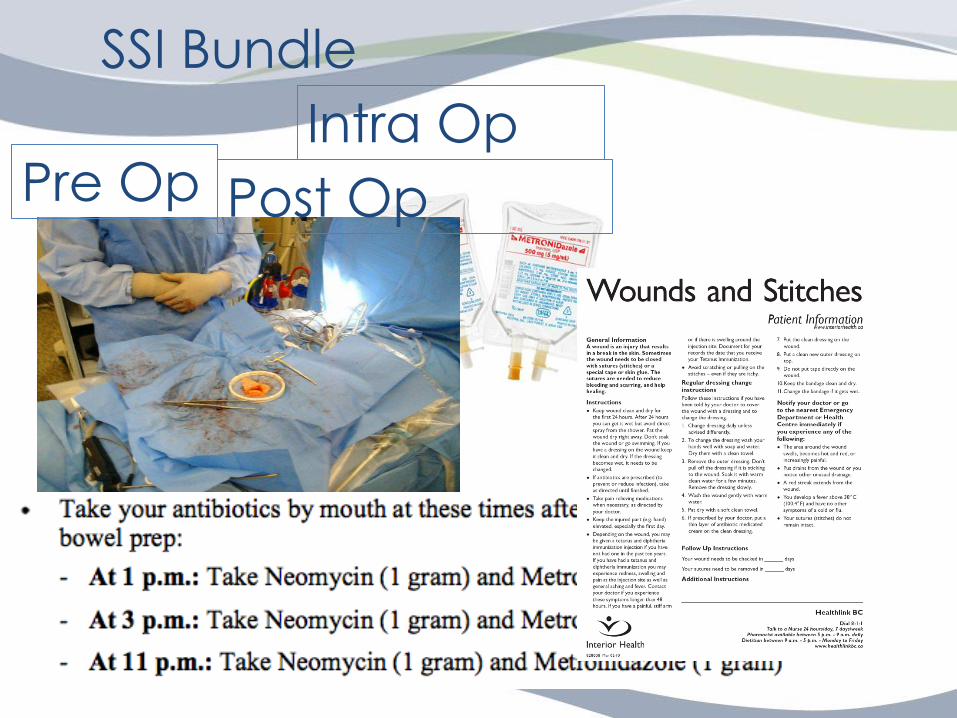
SSI Bundle
May 2013 – May 2014
Pre-Op
Patient received pre op scrub
Optimal Hair Removal (Clippers or None)
Appropriate antibiotic Timing (0-60 min pre cut
time)
Appropriate antibiotic given
Pre Op BGM Value
Pre op Bowel Prep & Oral Antibiotic
Intra- Op
Appropriate Isolation technique
Wound barrier used
Antimicrobial sutures used
Antibiotic re-dosing for surgeries > 4 hrs
Normothermia
Intra Op fluid volume
Intra Op BGM Value
Post - Op
Normothermia
Total Fluid volume in PAR
High O2 for 1 hr in PAR
BGM in PAR
Standardized wound care orders given
(Remove POD 2)
Patient Education Post Op

The Team
Department of Anesthesia
Pre Surgical Screening
NSQIP
Operating Room
Wound/Ostomy Nurses
Daycare Surgery
PAR
Physio
Surgical Ward
Division of General Surgeons
SSI Bundle
Pre Op Intra Op
Post Op

SSI Bundle Compliance June 17, 2013 – October 31, 2015
0% 20% 40% 60% 80% 100%
Dressing removed POD 2
Standardized Wound Care orders
BGM in PAR Taken
High 02 for 1 hr
Normothermia in PAR
Intra Op BGM Taken
Intra Op Warming
Intra Op temp taken
Abx re-dosing > 4 hrs
Antimicrobial Sutures
Wound Barrier
Isolation Technique
Pre op bowel prep
Pre BGM Taken
Appropriate Abx
Appropriate Abx Timing
Appropriate Hair Removal
Pre Op Scrub
Intra Op
Pre Op
Post Op

35%
17%
27%
10%
0%
5%
10%
15%
20%
25%
30%
35%
40%
Morbidity SSI
Pre Intervention (n=94) SSI Bundle (n=95)

Length of Stay
9
7
0
1
2
3
4
5
6
7
8
9
10
Pre Intervention (n=94) SSI Bundle (n=95)
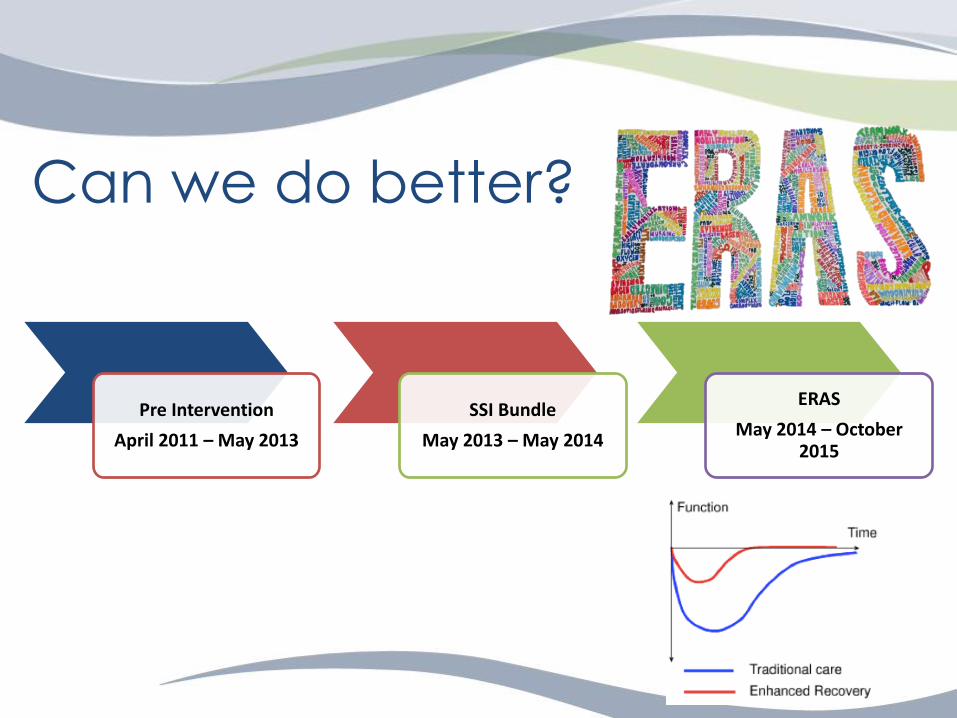
Pre Intervention
April 2011 – May 2013
SSI Bundle
May 2013 – May 2014
ERAS
May 2014 – October 2015
Can we do better?

ERAS Pre-Operative Elements
ERAS Intra-Operative Elements
ERAS Post-Operative Elements
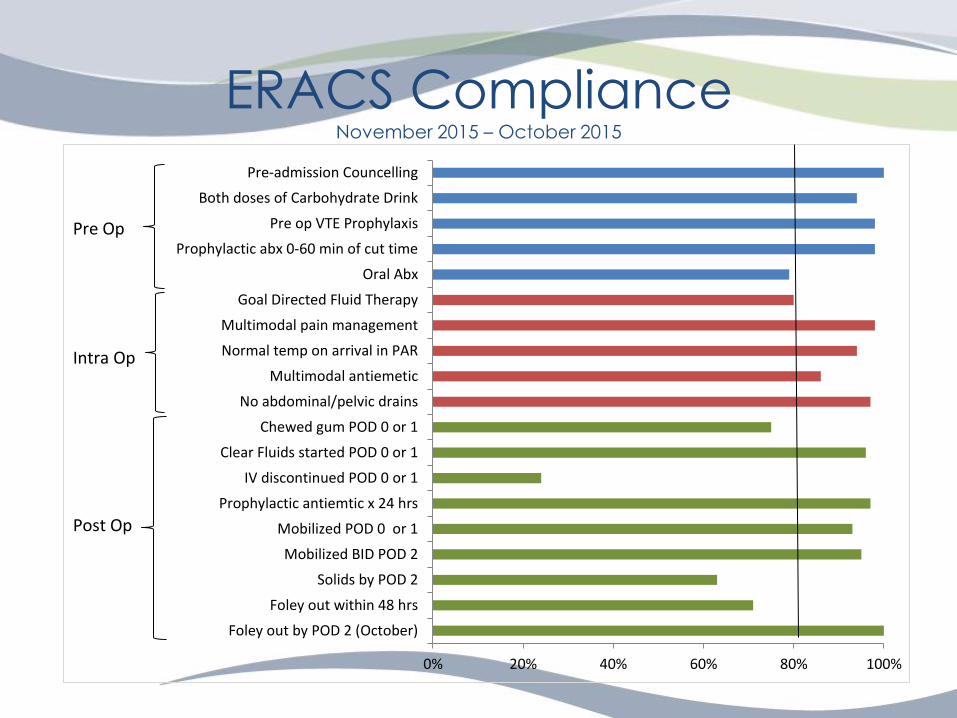
ERACS Compliance November 2015 – October 2015
0% 20% 40% 60% 80% 100%
Foley out by POD 2 (October)
Foley out within 48 hrs
Solids by POD 2
Mobilized BID POD 2
Mobilized POD 0 or 1
Prophylactic antiemtic x 24 hrs
IV discontinued POD 0 or 1
Clear Fluids started POD 0 or 1
Chewed gum POD 0 or 1
No abdominal/pelvic drains
Multimodal antiemetic
Normal temp on arrival in PAR
Multimodal pain management
Goal Directed Fluid Therapy
Oral Abx
Prophylactic abx 0-60 min of cut time
Pre op VTE Prophylaxis
Both doses of Carbohydrate Drink
Pre-admission Councelling
Intra Op
Pre Op
Post Op

35%
17%
27%
10%
20%
4%
0%
5%
10%
15%
20%
25%
30%
35%
40%
Morbidity SSI
Pre Intervention (n=94) Post SSI Bundle (n=95) Post ERACS (n=165)
Morbidity and SSI
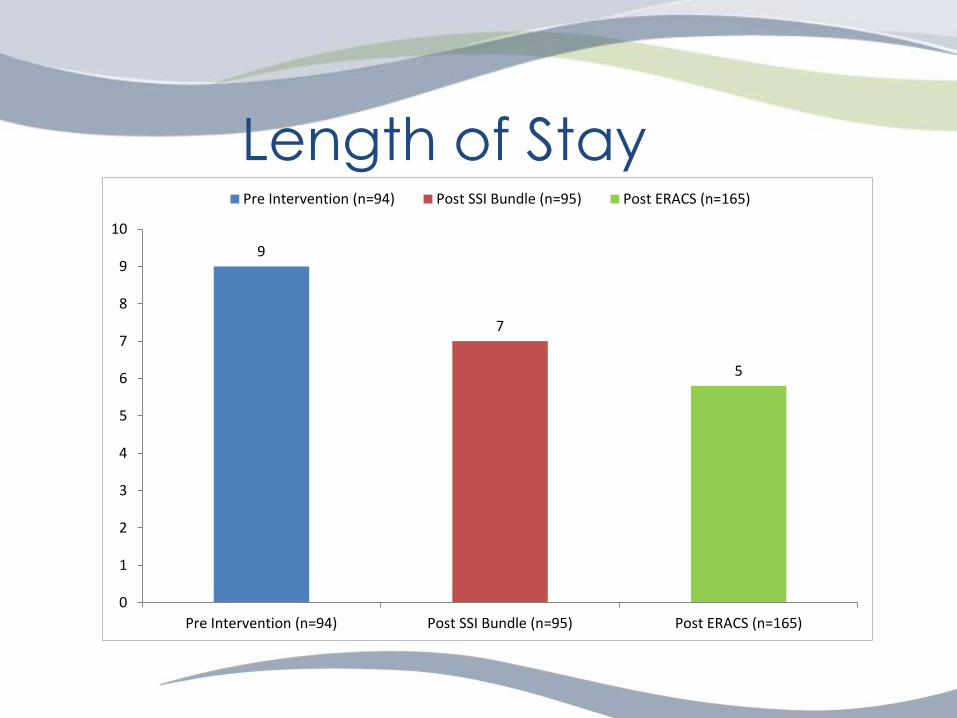
9
7
5
0
1
2
3
4
5
6
7
8
9
10
Pre Intervention (n=94) Post SSI Bundle (n=95) Post ERACS (n=165)
Pre Intervention (n=94) Post SSI Bundle (n=95) Post ERACS (n=165)
Length of Stay

Conclusions
Successful Implementation of an SSI Bundle and
ERAS has led to:
• Length of Stay
• Adverse Events
• Patient Satisfaction
• Culture / Teamwork
• Sustained Improvements

















