IN ORTHOMOLECULAR RESEARCH IN ORTHOMOLECULAR RESEARCH VOLUME 3 • ISSUE 2 research-driven botanical integrative orthomolecular breakthrough ADVANCES Cancer Cancer: Growth for the Sake of Growth AHCC and Cancer: A Prospectus EGCG: The Key to Green Tea Fucoidan - From the Ocean to your Cells HMR Lignan - Getting the Balance Right
Transcript
I N O R T H O M O L E C U L A R R E S E A R C HI N O R T H O M O L E C U L A R R E S E A R C H
Cancer: Growth for the Sake of GrowthAHCC and Cancer: A Prospectus
EGCG: The Key to Green TeaFucoidan - From the Ocean to your CellsHMR Lignan - Getting the Balance Right
Advances in Orthomolecular Researchis published and distributed through integrative physicians, health carepractitioners, and progressive health food retailers.
PrintingMcAra Printing Inc.Calgary, Alberta Canada
1
Digital version of this magazine and all back issues are available online at www.AOR.ca
8
A D VA N C E SI N O R T H O M O L E C U L A R R E S E A R C H VOLUME 3 • ISSUE 2
12
Cover Picture: Cancer Cells
16
21
1 Cancer: Growth for the sake of Growth8 AHCC and Cancer: A Prospectus
12 EGCG: The Key to Green Tea16 Fucoidan: From the Ocean to your Cells21 HMR Lignan: Getting the Balance Right26 Q & A
1ADVANCES in orthomolecular researchVolume 3, Issue 2
CCaanncceerrCancer is rust... When metal is exposed to water and oxygen, it slowlystarts to change. The iron is corroded and transformed frommetallic iron to iron oxide. The rust replaces the "healthy"metallic iron and eats away at the metal, weakening itsstructure. Paint, oil and protective coatings are all effectiveways to guard metal against corrosion, but rusting occurs ifthe paint is damaged, if the oil dissipates or if the finish isscratched - exposing the metal to oxidants. Corrosives canalso encourage rust formation, salt being a good example.
Figure 1: Initiation, promotion and progression of cancer.
Rust is "metallic" cancer. Like rust, cancer is a space-occupying lesion - cancerous cells occupy the space that waspreviously inhabited by healthy cells. Cancer slowly eatsaway at healthy tissues, monopolizes resources andeventually weakens organ function.
As corrosive agents promote the rusting of metal, specificchemicals cause damage to DNA and increase the risk ofdeveloping cancer - such chemicals are known ascarcinogens.
Cancer arises from DNA damage to a specific cell. In acancer cell, several consecutive cellular mutations haveinactivated the tumor suppressor genes responsible forinducing the cellular death of old or abnormal cells - aprocess known as apoptosis. Abnormal cells typically die topreserve the rest of the organism. However, once the tumorsuppressor genes have been inactivated, the cell becomesimmortal and DNA damage accumulates. This inevitablyleads to genetic instability and DNA mutations, which in timeresults in the creation of a cell that replicates uncontrollably,leading to cancer. The cancerous cells invade normal tissueseither through direct contact or spread to distant sites viametastasis. The growing tumor draws resources away fromimportant physiologic functions, replaces normal tissues andrestricts the function of vital tissues. Cancer eventuallybecomes a life-threatening situation.1
Cancer
Free Radical
Normal CellINITIATION
PROMOTION
PROGRESSION
DNA DamageDNA Repair
Initiated Cell
Proliferation
Proliferation
Proliferation
Apoptosis
Preneoplastic Cell State
Apoptosis
Neoplastic Cell State
Apoptosis
Initiation - the exposure of a cell to acarcinogen
Promotion - the uncontrolled cellular proliferation of cancer cells
Progression - the continuing growth andspread of cancer throughout the body
•••
Just like rusting metal, whichneeds to be exposed to water and
oxygen, cancer has severaldevelopmental stages:
Cancer is a serious health concern and aleading cause of death in developedcountries. In both the United States andCanada, one-in-four deaths areattributable to cancer - more than 1500deaths per day.2 In Canada, 38% ofwomen and 44% of men will eventuallydevelop cancer. Twenty-four percent ofCanadian women and 29% of Canadianmen will die of cancer. Cancer is theleading cause of premature death in NorthAmerica.3,4 (See Figure 2)
CausesOxidative stress and free radicals Oxidative stress is an important factor in thedevelopment of cancer. Oxygen free radicalsare produced 1) in the mitochondria duringnormal metabolism 2) in the atmosphere dueto pollution 3) by white blood cells in inflamedtissues and 4) by UV light.5
ADVANCES in orthomolecular research Volume 3, Issue 22
METABOLISM
UV LIGHT SMOKING
IONIZINGRADIATION
INFLAMMATION
WHITE BLOODCELL
DNA DAMAGEMICOCHONDRIAN
AIRPOLUTION
O2.- H2O2
.OH-
1O2
.OH-
1O2 .OH-
.OH-
O2.-
NO.
.OH-
O3 + UV(in air).-
.-
.
.
.
.
.
Figure 2: Leading Cancers in the US.Source: Jemal A, Murray T, Ward E, Samuels A, Tiwari RC, Ghafoor A, Feuer EJ, Thun MJ. Cancer statistics, 2005. CA CancerJ Clin. 2005 Jan-Feb;55(1):10-30.
Free radicals and DNA damage
O2·- Superoxide radical
·OH- Hydroxyl radicalROO· Peroxyl radical
H2O2 Hydrogen peroxide1O2 Singlet oxygen
NO· Nitric oxide
ONOO- PeroxynitriteHOCl Hypochlorous acid· Free electron
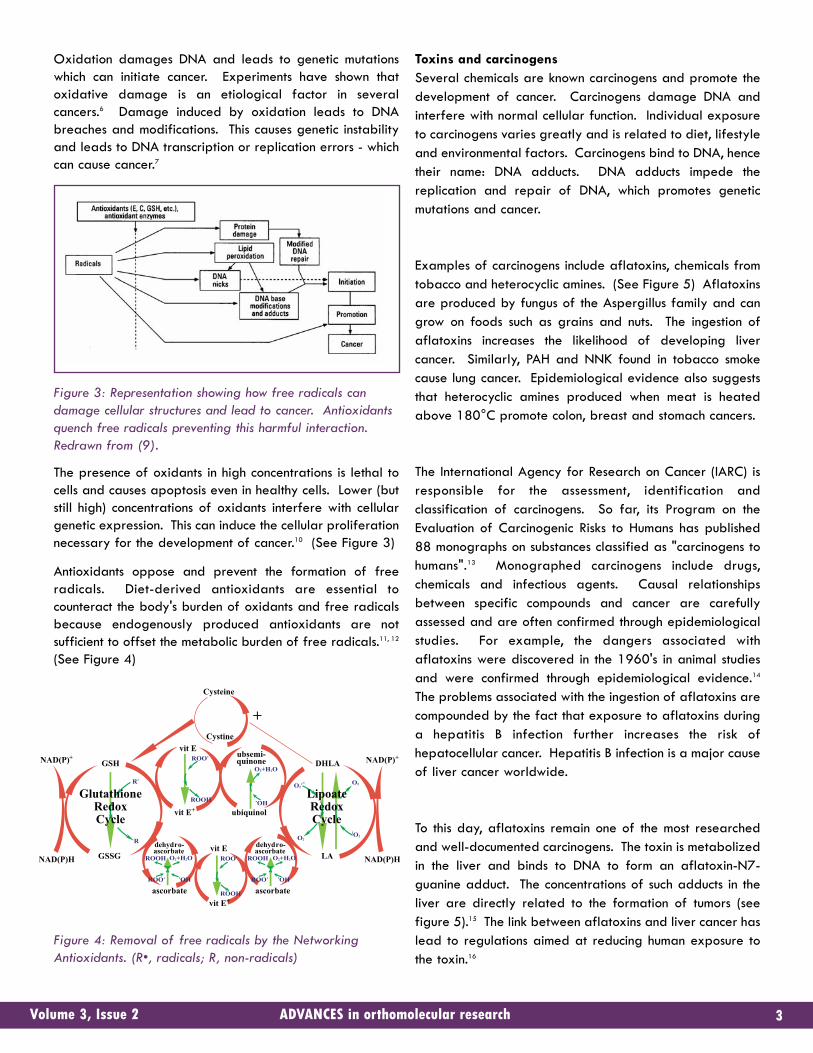
Oxidation damages DNA and leads to genetic mutationswhich can initiate cancer. Experiments have shown thatoxidative damage is an etiological factor in severalcancers.6 Damage induced by oxidation leads to DNAbreaches and modifications. This causes genetic instabilityand leads to DNA transcription or replication errors - whichcan cause cancer.7
Figure 3: Representation showing how free radicals candamage cellular structures and lead to cancer. Antioxidantsquench free radicals preventing this harmful interaction.Redrawn from (9).
The presence of oxidants in high concentrations is lethal tocells and causes apoptosis even in healthy cells. Lower (butstill high) concentrations of oxidants interfere with cellulargenetic expression. This can induce the cellular proliferationnecessary for the development of cancer.10 (See Figure 3)
Antioxidants oppose and prevent the formation of freeradicals. Diet-derived antioxidants are essential tocounteract the body's burden of oxidants and free radicalsbecause endogenously produced antioxidants are notsufficient to offset the metabolic burden of free radicals.11, 12
(See Figure 4)
Figure 4: Removal of free radicals by the NetworkingAntioxidants. (R•, radicals; R, non-radicals)
Toxins and carcinogensSeveral chemicals are known carcinogens and promote thedevelopment of cancer. Carcinogens damage DNA andinterfere with normal cellular function. Individual exposureto carcinogens varies greatly and is related to diet, lifestyleand environmental factors. Carcinogens bind to DNA, hencetheir name: DNA adducts. DNA adducts impede thereplication and repair of DNA, which promotes geneticmutations and cancer.
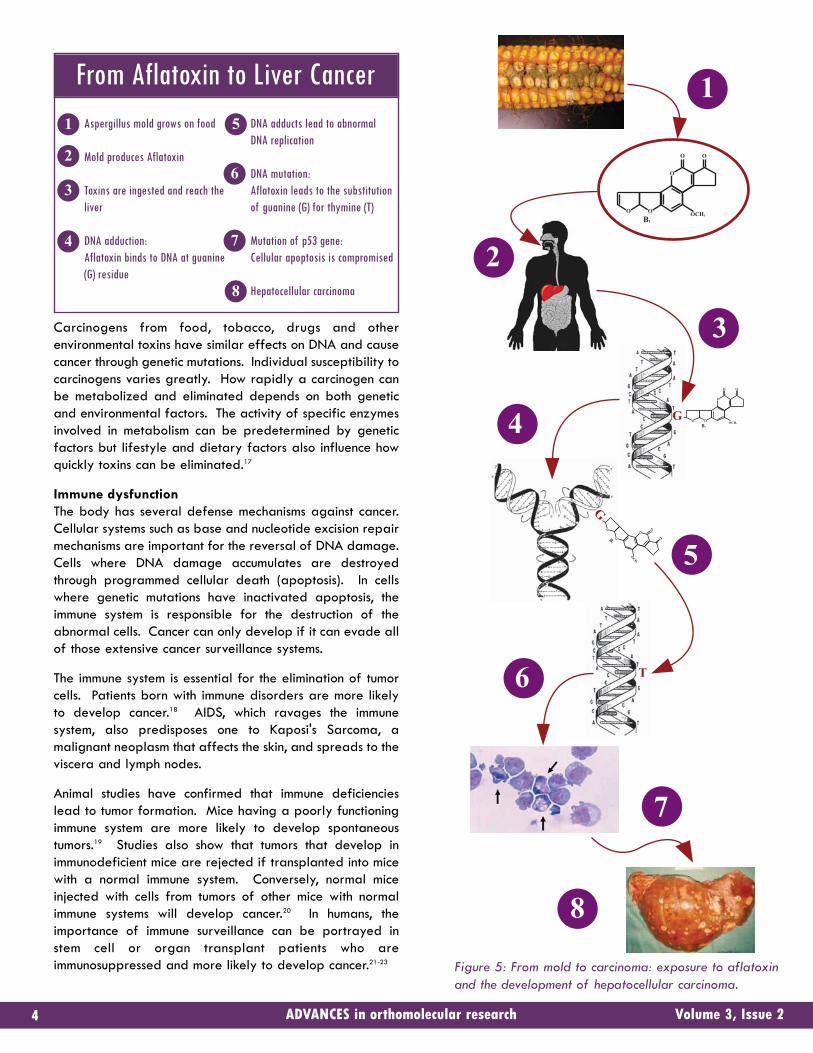
Examples of carcinogens include aflatoxins, chemicals fromtobacco and heterocyclic amines. (See Figure 5) Aflatoxinsare produced by fungus of the Aspergillus family and cangrow on foods such as grains and nuts. The ingestion ofaflatoxins increases the likelihood of developing livercancer. Similarly, PAH and NNK found in tobacco smokecause lung cancer. Epidemiological evidence also suggeststhat heterocyclic amines produced when meat is heatedabove 180°C promote colon, breast and stomach cancers.
The International Agency for Research on Cancer (IARC) isresponsible for the assessment, identification andclassification of carcinogens. So far, its Program on theEvaluation of Carcinogenic Risks to Humans has published88 monographs on substances classified as "carcinogens tohumans".13 Monographed carcinogens include drugs,chemicals and infectious agents. Causal relationshipsbetween specific compounds and cancer are carefullyassessed and are often confirmed through epidemiologicalstudies. For example, the dangers associated withaflatoxins were discovered in the 1960's in animal studiesand were confirmed through epidemiological evidence.14
The problems associated with the ingestion of aflatoxins arecompounded by the fact that exposure to aflatoxins duringa hepatitis B infection further increases the risk ofhepatocellular cancer. Hepatitis B infection is a major causeof liver cancer worldwide.
To this day, aflatoxins remain one of the most researchedand well-documented carcinogens. The toxin is metabolizedin the liver and binds to DNA to form an aflatoxin-N7-guanine adduct. The concentrations of such adducts in theliver are directly related to the formation of tumors (seefigure 5).15 The link between aflatoxins and liver cancer haslead to regulations aimed at reducing human exposure tothe toxin.16
3ADVANCES in orthomolecular researchVolume 3, Issue 2
GSH
GlutathioneRedoxCycle
LipoateRedoxCycle
GSSG
DHLA
LA
NAD(P)+
NAD(P)H
NAD(P)+
NAD(P)H
vit E
vit E+
ubsemi-quinone
ubiquinol
dehydro-ascorbate
ascorbate
dehydro-ascorbate
ascorbate
vit E
vit E+
Cysteine
Cystine
+
O2.-R.
R
ROO.
ROOH
ROO.
ROOH
ROO.
ROOHROO.
ROOH
O2+H2O
O2+H2O
O2
O2
1O2
.OH
.OH
O2+H2O
.OH
Carcinogens from food, tobacco, drugs and otherenvironmental toxins have similar effects on DNA and causecancer through genetic mutations. Individual susceptibility tocarcinogens varies greatly. How rapidly a carcinogen canbe metabolized and eliminated depends on both geneticand environmental factors. The activity of specific enzymesinvolved in metabolism can be predetermined by geneticfactors but lifestyle and dietary factors also influence howquickly toxins can be eliminated.17
Immune dysfunctionThe body has several defense mechanisms against cancer.Cellular systems such as base and nucleotide excision repairmechanisms are important for the reversal of DNA damage.Cells where DNA damage accumulates are destroyedthrough programmed cellular death (apoptosis). In cellswhere genetic mutations have inactivated apoptosis, theimmune system is responsible for the destruction of theabnormal cells. Cancer can only develop if it can evade allof those extensive cancer surveillance systems.
The immune system is essential for the elimination of tumorcells. Patients born with immune disorders are more likelyto develop cancer.18 AIDS, which ravages the immunesystem, also predisposes one to Kaposi's Sarcoma, amalignant neoplasm that affects the skin, and spreads to theviscera and lymph nodes.
Animal studies have confirmed that immune deficiencieslead to tumor formation. Mice having a poorly functioningimmune system are more likely to develop spontaneoustumors.19 Studies also show that tumors that develop inimmunodeficient mice are rejected if transplanted into micewith a normal immune system. Conversely, normal miceinjected with cells from tumors of other mice with normalimmune systems will develop cancer.20 In humans, theimportance of immune surveillance can be portrayed instem cell or organ transplant patients who areimmunosuppressed and more likely to develop cancer.21-23
O
O O
OCH3
B1
O O
O
O O
OCH3
B1
O OG
T
GO
O
O
OCH3
B1
O
O
3
2
1
4
5
6
7
8
Aspergillus mold grows on food
Mold produces Aflatoxin
Toxins are ingested and reach theliver
DNA adduction: Aflatoxin binds to DNA at guanine (G) residue
DNA adducts lead to abnormalDNA replication
DNA mutation: Aflatoxin leads to the substitution of guanine (G) for thymine (T)
Mutation of p53 gene:Cellular apoptosis is compromised
Hepatocellular carcinoma
1 5
2
6
3
74
8
From Aflatoxin to Liver Cancer
Figure 5: From mold to carcinoma: exposure to aflatoxinand the development of hepatocellular carcinoma.
ADVANCES in orthomolecular research Volume 3, Issue 24
Tumors release proinflammatory messengers, which attractsimmune cells to the area. This promotes the elimination ofcancer cells that had previously escaped the immune system- a process known as the adaptive immune response. Theadaptive immune system specializes in the elimination ofpathogenic challenges and is activated by non-specificimmune messengers.
Figure 6: Failure of tumor elimination.
The appearance of tumors that evade the immune system ispartly a consequence of immunoselection. Cancer cells aregenetically unstable which means that their characteristicsare changing rapidly. The immune system will selectivelytarget and destroy cells that can easily be recognized. Thisimplies that cancer cells, which cannot be identified, willsurvive and proliferate to form immune resistant tumors.
Genetic predispositionWe all have genetic polymorphisms. Polymorphisms arenatural genetic variations with a high enough prevalence atthe population level that they cannot be referred to asgenetic mutations. Polymorphisms may reduce the activityof specific enzymes and some polymorphisms reduce theactivity of cancer prevention mechanisms. Some individualsare born with genetic variations that make them more proneto developing cancer.24-27 The inactivation of tumor protein53 (also known as p53) is a good example of a geneticpolymorphism that predisposes to cancer. Individuals withgenetic variations affecting the p53 gene are moresusceptible to cancer because fewer mutations are requiredto shutdown apoptosis (several successive mutations are
needed to inactivate apoptosis). Studies have shown thatindividuals with polymorphisms affecting codon 72 (asection of DNA that codes for a specific amino acid) are 3.9times more likely to develop stomach cancer.28 Similarly,genetic variations affecting the immune system can weakenthe immunity, impede immunosurveillance and increase theincidence of cancer.
Chronic InflammationChronic inflammation can lead to the development ofcancer. Inflammation results from the activation of immunecells, mainly neutrophils and macrophages. When immunecells are activated, they release inflammatory mediators;and toxins, which include reactive oxygen species. Thepurpose of inflammation is the destruction of the offendingagent. Unfortunately, chronic inflammation leads tooxidative stress in surrounding cells. Oxidation promotescellular and DNA damage which predisposes one to geneticmutations and cancer.29 Examples of chronic inflammatoryconditions potentially leading to cancer include asbestosis,inflammatory bowel disease, Barrett's dysplasia andgastritis (see figure 7 on next page). This is why treatmentsaimed at the reduction of inflammation have been shown toprevent cancer.30
We regard cancer as fundamentally abhorrent, yet theprocess which leads to the faulty mutations behind cancer isalso responsible for the adaptive mutations which driveevolution. Although most mutations are detrimental, everyso often a new DNA mutation confers an advantage,enabling its carrier to produce more offspring to propagatethe new DNA sequence. Cancer may therefore neverdisappear and it may not be in our interest to irradicategenetic mutations. Genetic mutations that occur duringconception are, after all, nature's attempt to find a betterway...
References1 Fenton RG, Longo DL. Cell Biology of Cancer. Harrison's Principles of Internal Medicine15th Edition. McGraw-Hill. 20012 Jemal A, Murray T, Ward E, Samuels A, Tiwari RC, Ghafoor A, Feuer EJ, Thun MJ.Cancer statistics, 2005. CA Cancer J Clin. 2005 Jan-Feb;55(1):10-30.3 Canadian Cancer Society/National Cancer Institute of Canada: Canadian CancerStatistics 2006, Toronto, Canada, 20064 Jemal A, Murray T, Ward E, Samuels A, Tiwari RC, Ghafoor A, Feuer EJ, Thun MJ.Cancer statistics, 2005. CA Cancer J Clin. 2005 Jan-Feb;55(1):10-30.5 Valko M, Leibfritz D, Moncol J, Cronin MT, Mazur M, Telser J. Free radicals andantioxidants in normal physiological functions and human disease. Int J Biochem Cell Biol.2007 Apr;39(1):44-84. Epub 2006 Aug 4.6 Valko M, Rhodes CJ, Moncol J, Izakovic M, Mazur M. Free radicals, metals andantioxidants in oxidative stress-induced cancer. Chem Biol Interact. 2006 Mar10;160(1):1-40.7 Valko M, Leibfritz D, Moncol J, Cronin MT, Mazur M, Telser J. Free radicals andantioxidants in normal physiological functions and human disease. Int J Biochem Cell Biol.2007 Apr;39(1):44-84. Epub 2006 Aug 4.8 Pryor WA. Cigarette smoke radicals and the role of free radicals in chemicalcarcinogenicity. Environ Health Perspect. 1997 Jun;105 Suppl 4:875-82.9 Pryor WA. Cigarette smoke radicals and the role of free radicals in chemicalcarcinogenicity. Environ Health Perspect. 1997 Jun;105 Suppl 4:875-82.
5ADVANCES in orthomolecular researchVolume 3, Issue 2
12
T-Cell
T-Cell
Cancer Cells with Receptors Cancer Cells without Receptors
Immunoselection
Cancer cells that express the receptor needed toactivate T-cells are destroyed by the immune system. Cancer cells without these receptors survive andreplicate. This leads to the formation of a tumorthat cannot be attacked by the immune system - aprocess known as immunoselection.
1
2
10 Valko M, Leibfritz D, Moncol J, Cronin MT, Mazur M, Telser J. Free radicals andantioxidants in normal physiological functions and human disease. Int J Biochem Cell Biol.2007 Apr;39(1):44-84. Epub 2006 Aug 4.11 Valko M, Rhodes CJ, Moncol J, Izakovic M, Mazur M. Free radicals, metals andantioxidants in oxidative stress-induced cancer. Chem Biol Interact. 2006 Mar10;160(1):1-40.12 Fang YZ, Yang S, Wu G. Free radicals, antioxidants, and nutrition. Nutrition. 2002Oct;18(10):872-9.13 IARC Monographs on the Evaluation of Carcinogenic Risks to Humans. InternationalAgency for Research on Cancer. http://monographs.iarc.fr/14 Wogan GN, Hecht SS, Felton JS, Conney AH, Loeb LA. Environmental and chemicalcarcinogenesis. Semin Cancer Biol. 2004 Dec;14(6):473-86.15 Wogan GN, Hecht SS, Felton JS, Conney AH, Loeb LA. Environmental and chemicalcarcinogenesis. Semin Cancer Biol. 2004 Dec;14(6):473-86.16 FDA Regulatory Guidance for Toxins and Contaminants. National Grain and Feed Association.17 Wogan GN, Hecht SS, Felton JS, Conney AH, Loeb LA. Environmental and chemicalcarcinogenesis. Semin Cancer Biol. 2004 Dec;14(6):473-86.18 Hosokawa M. Combination of AHCC and Chemotherapy. Anti-Cancer Drugs. 9,343-350,1998.19 Shankaran V, Ikeda H, Bruce AT, White JM, Swanson PE, Old LJ, Schreiber RD.IFNgamma and lymphocytes prevent primary tumour development and shape tumourimmunogenicity. Nature. 2001 Apr 26;410(6832):1107-11.20 Shankaran V, Ikeda H, Bruce AT, White JM, Swanson PE, Old LJ, Schreiber RD.IFNgamma and lymphocytes prevent primary tumour development and shape tumourimmunogenicity. Nature. 2001 Apr 26;410(6832):1107-11.
21 Buell JF, Gross TG, Woodle ES. Malignancy after transplantation. Transplantation.2005 Oct 15;80(2 Suppl):S254-64.22 Trofe J, Beebe TM, Buell JF, Hanaway MJ, First MR, Alloway RR, Gross TG, WoodleES. Posttransplant malignancy. Prog Transplant. 2004 Sep;14(3):193-200.23 Penn I. Malignant melanoma in organ allograft recipients. Transplantation. 1996 Jan27;61(2):274-8.24 Nevanlinna H, Bartek J. The CHEK2 gene and inherited breast cancer susceptibility.Oncogene. 2006 Sep 25;25(43):5912-925 Mathew CG. Fanconi anaemia genes and susceptibility to cancer.Oncogene. 2006 Sep 25;25(43):5875-84.26 Rogowski W. Genetic screening by DNA technology: a systematic review of healtheconomic evidence.Int J Technol Assess Health Care. 2006 Summer;22(3):327-37.27 Liu WZ, Jin F, Zhang ZH, Wang SB. Role of detection of microsatellite instability inChinese with hereditary nonpolyposis colorectal cancer or ordinary hereditarycolorectal cancer. World J Gastroenterol. 2006 Aug 7;12(29):4745-9.28 Yi SY, Lee WJ. A p53 genetic polymorphism of gastric cancer: difference betweenearly gastric cancer and advanced gastric cancer. World J Gastroenterol. 2006 Oct28;12(40):6536-9.29 Ernst P. Review article: the role of inflammation in the pathogenesis of gastric cancer.Aliment Pharmacol Ther. 1999 Mar;13 Suppl 1:13-8.30 Grosch S, Maier TJ, Schiffmann S, Geisslinger G. Cyclooxygenase-2 (COX-2)-independent anticarcinogenic effects of selective COX-2 inhibitors. J Natl Cancer Inst.2006 Jun 7;98(11):736-47.
ADVANCES in orthomolecular research Volume 3, Issue 26
3
21
4
56
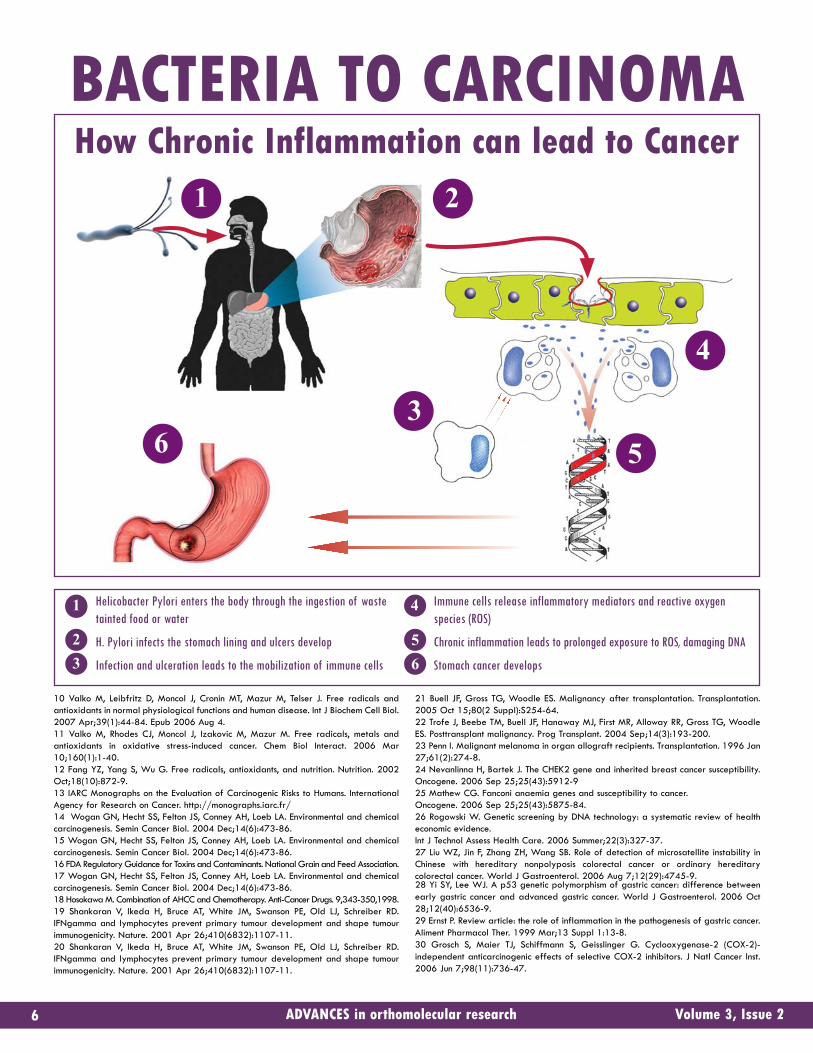
BACTERIA TO CARCINOMAHow Chronic Inflammation can lead to Cancer
11
2
3
4
5
6
Helicobacter Pylori enters the body through the ingestion of wastetainted food or water
H. Pylori infects the stomach lining and ulcers develop
Infection and ulceration leads to the mobilization of immune cells
Immune cells release inflammatory mediators and reactive oxygenspecies (ROS)
Chronic inflammation leads to prolonged exposure to ROS, damaging DNA
Stomach cancer develops
ADVANCES in orthomolecular research Volume 3, Issue 27
A Different ApproachIs a condition such as acute renal failure specifically adisease of the kidneys? Is pulmonary fibrosis specifically adisease of the lungs? Is cirrhosis specifically a disease ofthe liver?1 Perhaps the time is ripe to approach thesequestions from a broader perspective.
Enter AHCCAHCC, or Active Hexose Correlated Compound, is amonosaccharide, a simple sugar derived from the myceliumof a member of the basidiomycetes family of mushroomsknown as the Shiitake.2 The mushroom blend itself, which isin fact a hybrid, is developed in a pre-cultivation tank.3 Thebasidiomycetes mushroom colonies are then cultured in amain cultivation tank where they undergo a thoroughfermentation process that consists of advanced cultivation,enzymatic decomposition, sterilization, concentration andfinally freeze-drying.4 This is done in tanks as large as 15tons for as long as 45 days.5 This must be done under strictcontrols.6 The fermentation process breaks down nutrientsinto a form that is most easily assimilated by the body'sdigestive system.
The tangible end result is a product that has anexceptionally low molecular weight of 5,000 daltons, most
impressive when compared with the molecular weight ofmost mushroom extracts, which are measured in thehundreds of thousands of daltons.7 Arguably the mostactive nutrient in AHCC is acetylated α-glucan, acomponent known to enhance the immune system.8 However,in addition to merely breaking down nutrients, thecultivation and enzymatic decomposition segments of thefermentation process creates new nutrients.
The beneficial applications of AHCC are centered on it'sability to augment the immune system. However, it is alsorenowned for helping patients with HIV, hypertension,hypoglycemia and endocrine system modulation. It is evenknown to have cosmetic applications with respect toalopecia (hair loss).9 However, it is as a concurrenttreatment to chemotherapy that AHCC has carved out themost distinctive role for itself.
There are no fewer than 700 Japanese hospitals dispensingAHCC as part of various protocols.10 In addition, 15Japanese medical colleges and universities are conductingresearch with AHCC, not to mention additional researchbeing undertaken in China, South Korea, Thailand and theUnited States.11
Enter The Immune SystemThe immune system is composed mainly of white blood cells,and there are several sub-categories of white blood cellsthat seem to be exclusively designed by the body to directlyresist invasive threats. They are; macrophages, neutrophils,natural killer cells or NK cells, lymphokine activated killercells (LAK), cytotoxic lymphocytes and T-helper cells.12 Allsix of these sub-categories of white blood cells have atleast one specific function in common: they serve as thefront-line interceptors of the immune system. They circulatethroughout the body searching for any abnormal cells aswell as foreign substances, often referred to as antigens.13
These sub-types of white blood cells, also referred to asleukocytes, destroy the antigens at the point of contactbefore they have a chance to create any intracellulardisturbance. It is the differing specific mechanisms used bythese white blood cells to decimate the antigens thatdistinguish them best from each other.
Macrophages and neutrophils destroy any foreign bacteriathrough a process called "phagocytosis", which closelymatches its literal translation in Greek - cell eating.Macrophages and neutrophils literally engulf and digestany microbes perceived as a threat by the immune system.On the other hand, natural killer cells, lymphokine activatedkiller cells (LAK), and cytotoxic lymphocytes attach
themselves to the surface of the perceived micro-cellularthreat, and like reptilian predators inject their targets witha granule that causes a chemical reaction. That chemicalreaction leads to the destruction of the anomaly inquestion.14 T-helper cells exert much of their influence bymaintaining a favourable balance between two of theirmanifestations, namely T-helper cell type 1 cells (Th1) and Thelper cell type 2 cells (Th2).
It is absolutely critical to stress that the immune responsesystem is inherently dependent on its ability to recognize aforeign protein or bacteria as abnormal before it can directcountermeasures against it. While macrophages andnatural killer cells serve as the actual combatants againstany cellular abnormality, they require intracellularmessengers that would disseminate information betweencells in order to initiate and sustain the immune response.These intracellular couriers are a biologically active familyof proteins called cytokines.15 There are numerous types ofthese intracellular messengers, but the ones most directlypertinent to the immune response are: interferon(specifically gamma interferon); interleukin-2 (IL-2);interleukin-12 (IL-12); and tumor necrosis factor (TNF).16
There are no fewer than 700 Japanesehospitals dispensing AHCC as part of
various protocols.
How Does AHCC Work?AHCC exerts its influence on the immune system in a processthat directly involves all of the white blood cells touchedupon thus far. This process naturally encompassesbiochemical mechanisms that have multiple roles thatoverlap with one another, but if it were to be described ina step-by-step manner, it would likely resemble the tablebelow:
A great deal of emphasis has been placed on studyingAHCC’s numerous distinctive benefits, such as its overallenhancement of the immune system, its stimulating effect onthe different immune white blood cells such asmacrophages, NK cells and CTL cells, its equally stimulatingeffect on the different cytokines, and finally its improvementof theTh1/Th2 balance.17
The most common ground that scientists seem to haveisolated as the source for all these effects is that AHCC goesto work directly on the macrophage itself. It stimulates boththe activity of the macrophages as well as their numbers,perhaps even doubling them.18 This would of course lead tothe increased production of cytokines such as IL-12 and TNF(directly) in turn leading to the increased production of NK,LAK and CTL cells, not to mention more interferon(indirectly).19
8ADVANCES in orthomolecular researchVolume 3, Issue 2
This is the optimal method by which the immune system would respond to an antigen. The reality of the matter, of course, is thatwhat is optimal is often very far removed from what is standard. The purpose of AHCC is to make what is standard optimal.
1. An antigen enters the human bloodstream.
2. Imune cells begin to produce interferon in response.
3. Interferon binds to macrophages and triggers theiractivation.
4. Macrophages then produce interleukin-12 (IL-12)and tumor necrosis factor (TNF).
5. IL-12 and TNF both simultaneously stimulate the Thelper cells to manifest themselves into T helper celltype 1 cells (Th1) and T helper cell type 2 cells(Th2). The IL-12 also directly stimulates the activityand volume of natural killer (NK) cells, while at thesame time TNF exerts its inflammatory capabilitiesto influence the apoptosis of the antigen.
6. It is absolutely critical that the manifested Th1/Th2balance favours the production of Th1 cells as theyproduce interleukin-2 and more interferon. In sharp
contrast, Th2 cells produce cytokines that suppressthe immune response, such as IL-10, IL-6, and TGF-ß.
7. The empowered Th1 cells then proceed to increaselevels of IL-2 and interferon. The increased IL-2levels result in the direct stimulation of the activityand volume of cytotoxic lymphocytes (CTL) andlymphokine activated killer cells (LAK). Theincreased interferon will further enhance the activityof the macrophage, resulting in a "feedback loop"that will perpetually increase the production of IL-12, which in turn will increase the activities of theNK cells.
8. The result of the combined efforts of the LAK, CTLand NK cells will be the apoptosis of the originalinvading antigen.
OPTIMAL IMMUNE RESPONSE PROCESS
AHCC and the Symptoms ofCancer TreatmentCurrently, the standard options for cancer treatment arechemotherapy, radiation, and surgery. Chemotherapy isnotoriously aggressive in that it can cause loss of appetite,hair loss, bone marrow suppresssion and liver damage,severe vomiting, and anemia.20 Many of these symptomscan also be caused by radiation, and both treatments caninflict heavy damage on the patient's immune system. Theresult for the patient can be a dramatically reduced qualityof life, which can easily lead to (or include) depression.Surgery, for all of its power of quick resolution, is infamousfor draining its patients' recuperative abilities and veryoften causes unknown and unexpected complications of itsown. This too, can lead to a dramatically reduced qualityof life for patients.
A prospective cohort study with AHCC was performed fromFebruary 1, 1992 to December 31, 2001. A total of 269patients with hepatocellular carcinoma (HCC) were studied.113 of these patients were given AHCC following surgeryand the remainder was not, and no placebo was used.21
The period of time for which each patient was examinedwas from immediate post-surgery until either recurrence ordeath (from any cause). The survival rate of the AHCCgroup was 79 percent compared to 51 percent for thecontrol group.22 Furthermore, the recurrence rate among theAHCC group was 49 percent compared to 67 percent forthe control group.23 The conclusion of the researchers wasthat AHCC intake can improve the prognosis ofpostoperative hepatocellular carcinoma (HCC) patients.
The survival rate of the AHCC groupwas 79 percent compared to 51 percent
for the control group.
When the damaging effects of chemotherapy areexamined more closely, it becomes increasingly clear howAHCC can play an invaluable role. This is becausechemotherapy does not effectively distinguish betweenhealthy cells and tumors. AHCC, on the other hand,stimulates and reinforces the white blood cells and cytokineswhich attack only the tumors.24
In a large study involving 229 patients suffering fromgastrointestinal cancer and undergoing subsequentchemotherapy treatment, the efficacy of AHCC as achemotherapy support agent was put to the test.25 Thesepatients were being treated with a combination of 5-fluorouracil, CDDP, and other chemotherapy agents. 127 of
these patients were given AHCC while the remaining 102were not. The results were decisive: 27 months into thestudy, the survival rate was 66.7% for the AHCC group and35% for the control group. Among those patients afflictedwith colon cancer, the survival rate for the AHCC group was89.9% after 10.2 months of treatment as opposed to55.9% for the control group after the same amount oftime.26
The chemotherapy drug UFT was also combined with AHCCin a study to determine if the two could produce asynergistic effect. The study determined that AHCCcombined with UFT produced results on primary tumorgrowth and metastasis that UFT alone did not match.27
These results seemed to be mediated by the fact that theAHCC/UFT combination enhanced NK cell activity, where-as UFT alone suppressed it.28 This is most impressive since itimplies that AHCC's immune system-enhancing effects morethan compensate for UFT's suppressive ones.
AHCC in Combination withother Non-Toxic TherapyAHCC's capabilities as an unparalleled synergist to othertreatments is not limited to chemotherapy drugs. In fact,one animal study placed AHCC in combination withGenistein Combined Polysaccharide (GCP).29 GCP is a"functional food" derived from cultivated basidiomycetesand soybean isoflavones, and is reported to have tumorsuppressive capabilities.30 Although the tumor growth wasslowed in both the AHCC and the GCP groups, theAHCC/GCP combination had a more pronounced effect.31
AHCC and Quality of LifeQuality of life (QOL) parameters are a centerpiece ofAHCC supplementation. They have been examined heavilyin human studies with AHCC primarily because they have
ADVANCES in orthomolecular research Volume 3, Issue 29
10ADVANCES in orthomolecular researchVolume 3, Issue 2
such far-reaching implications. Not only do they improverecovery time and prevent recurrence, but they are alsowhat allow AHCC to be so widely applicable. Oneindicator of QOL is the patient's ability to perform dailyrudimentary tasks, and this was the exclusive indicator in astudy used to measure AHCC's effect on QOL among 38cancer patients who had not undergone surgery,chemotherapy, or radiation.32 It concluded that the QOLparameters were "significantly" improved after 6 months ofAHCC therapy.33 Another study included psychologicalstate and social interaction as indicators of QOL. Thisparticular study examined 28 cancer patients who
underwent AHCC treatment for 2 months, and it concludedthat all parameters of QOL had improved significantly.34
AHCC's effect on QOL makes it a worthwhile treatment forother conditions whose proliferation is dependent on themalfunction of the immune system. This would includeautoimmune diseases, inflammation, opportunistic infectionsand HIV. This is because the improvements in QOL aresimply the reflections of AHCC's effect on the immunesystem, and that effect is so fundamental that the list ofafflictions alleviated by its use continues to grow.
References1 Kenner D. AHCC: The Japanese Medicinal Mushroom Immune Enhancer. WoodlandPublishing.; ISBN: 1-58054-340-5: P. 82 Ibid. P. 63 Kosuna K. The Development and Application of Active Hexose CorrelatedCompound. Bio Industry 1993: 104 Kosuna K. Recent Progress of Research on AHCC; Active Hexose CorrelatedCompound. New Food Industry 1999; 41:17-235 Kenner D. AHCC: The Japanese Medicinal Mushroom Immune Enhancer. WoodlandPublishing.; ISBN: 1-58054-340-5: P. 66 AHCC Research Association. What Is AHCC? Summary Book. 1994 ; p.27 Kenner D. AHCC: The Japanese Medicinal Mushroom Immune Enhancer. WoodlandPublishing.; ISBN: 1-58054-340-5: P. 78 Ibid.9 AHCC Research Association. What Is AHCC? Summary Book. 1994 ; p.210 Kenner D. AHCC: The Japanese Medicinal Mushroom Immune Enhancer. WoodlandPublishing.; ISBN: 1-58054-340-5: P. 511 Ibid.12 Ibid. P. 1113 Ibid.14 Ibid. P.1215 Raffi Babakhanian. Cytokines, HIV and the Immune System: An overview of the roleof cell messengers in HIV infection. Aids Treatment Update. September 1995 16 Kosuna K, Recent Progress of Research on AHCC; Active Hemicellulose Compound.New Food Industry 1999;41:17-23.17 AHCC Research Association. Effect of AHCC on the Immune System. Summary Book.1994 ; p. 718 Kenner D. AHCC: The Japanese Medicinal Mushroom Immune Enhancer. WoodlandPublishing.; ISBN: 1-58054-340-5: P. 14
19 Kosuna K, Recent Progress of Research on AHCC; Active Hemicellulose Compound.New Food Industry 1999;41:17-23.20 Chemotherapy Effects. American Cancer Society, Inc. (c) 200521 Matsui Y., Uhara J., Satoi S., Kaibori M., Yamada H., Kitade H., Imamura A., TakaiS., Kawaguchi Y., Kwon A., Kamiyama Y. Improved Prognosis of PostoperativeHepatocellular Carcinoma Patients When Treated With Functional Foods: A ProspectiveCohort Study. Journal of Hepatology, vol. 37/1,pp 78-86, July 2002.22 Kenner D. AHCC: The Japanese Medicinal Mushroom Immune Enhancer. WoodlandPublishing.; ISBN: 1-58054-340-5: P. 1623 Ibid.24 Ibid. P. 1825 Kawaguchi Y, Teshima, Toyo H, Sugimoto N, Matsumiya M, Araki H, Komada N andKamiyama Y. Effect of AHCC on Digestive Cancer-Especially for Terminal Cancer. AHCCResearch Association 8th Symposium 2000.26 Ibid.27 Matsushita K., Kuramitsu Y., Ohiro Y., Obara M., Kobayashi M., Li Y., Hosokawa M.Combination Therapy of Active Hexose Correlated Compound Plus UFT SignificantlyReduces The Metastasis of Rat Mammary Adenocarcinoma. Anti-Cancer Drugs 1998,pp. 343-350. 28 Ibid.29 Sun B., Mukoda T., Miura T., Fujii H., Yuan L., White RD. Anti-tumor Effects of theCombination of Genistein Concentrated Polysaccharide (GCP) and Active HexoseCorrelated Compound (AHCC). Biotherapy 2001; 15(3): 379-382.30 Ibid.31 Ibid.32 Uno K., et al. Active Hexose Correlated Compound (AHCC) Improves ImmunologicalParameters And Performance Status of Patients with Solid Tumors. Biotherapy 200014(3) 303-309.33 Ibid.34 Iwamoto M. Effects of AHCC Administration on QOL in Cancer Patients. FightingAgainst Cancer. The 7th Symposium of AHCC Research Association, August 1999.
ADVANCES in orthomolecular research Volume 3, Issue 211
EEGGCCGGThe key to Green TeaIntroductionIt would not be an over statement to define Green tea asone of the world's first "functional foods". Historians claimits use dates back over 40 centuries to ancient China. Themyth of the Emperor Shen-Nung discovering the brewaccidentally in 2737 BC when tea leaves fell into a pot ofwater he was boiling remains a part of the folklore of thatnation. In any event, the earliest mention of green tea ispunctuated not by its soothing flavour but rather by itshealing powers, which have survived every type of scrutinyfrom antiquity to the present day. The modern citizens ofJapan boast one of the longest average lifespan in theworld, and there is a plethora of research to suggest thatgreen tea plays a significant role in that claim.
PharmacokineticMechanism of Action The active ingredients in the extract of green tea are calledcatechins. Catechins are polyphenolic compounds present inhigh concentrations in green tea and display a number ofantioxidant, anticarcinogenic, antiinflammatory,antiatherogenic, antimicrobial and thermogenic activities.
There are four main types of catechins occurring naturallyin green tea extract; epicatechin (EC), epigallocatechin(EGC), epicatechin gallate (ECG) and epigallocatechingallate (EGCG). EGCG is the largest and most potent ofthe catechins and comprises approximately 10%-50% ofthe total catechin content in most green tea extracts.
The antioxidant activity of green tea extract includes thescavenging of such reactive oxygen species as superoxide,hydroxyl and peroxyl radicals.1 It also inhibits lipidperoxidation, oxidation of low-density lipoproteins, and 2'-deoxyguanosine oxidation in DNA to 8-hydroxy-2' -deoxyguanosine.2 The anticarcinogenic activity of greentea catechins may be attributable to a number of differentmechanisms. The green tea catechins containing the gallategroup in their structure (EGCG, EGC and ECG) have allbeen found to induce apoptosis in numerous tumor cell lines.3
EGCG has also been shown to inhibit angiogenesis.4 EGCGand ECG have been demonstrated to restrict tyrosinephosphorylation of the receptor tyrosine kinase PDGFR-beta (platelet-derived growth factor receptor-beta) and itsdownstream signaling pathway, consequently inhibiting thetransformation of human glioblastoma cells.5 There is alsoevidence demonstrating that green tea catechins promotethe synthesis of hepatic phase II enzymes that are involvedin the detoxification of certain xenobiotics.
The Research Scientists have examined the medicinal properties of greentea catechins in their most elemental form - as ordinary,commonly available green tea beverages. In fact, one studythat observed 8,552 Japanese green tea drinkers aged 40and over from 1986 to 1996 concluded that there was asignificant inverse relationship between green teaconsumption and incidence of cancer.6 The greatest degreeof protection was among females consuming 10 or more cupsof green tea daily with each cup containing 150mg ofEGCG7 The researchers attributed the difference betweentheir degree of protection and that among males drinking anequal amount to the fact that a significantly higherpercentage of the males were smokers.8 Green tea has alsobeen reported to increase the tolerability of chemotherapydrugs, with one study indicating that green tea consumptioncan lower the cardiotoxicity of doxorubicin (Caelyx(r),Myocet(r)) without inhibiting its anti-tumor effects.9
The modern citizens of Japan boast one ofthe longest average lifespan in the world,
and there is a plethora of research tosuggest that green tea plays a significant
role in that claim.
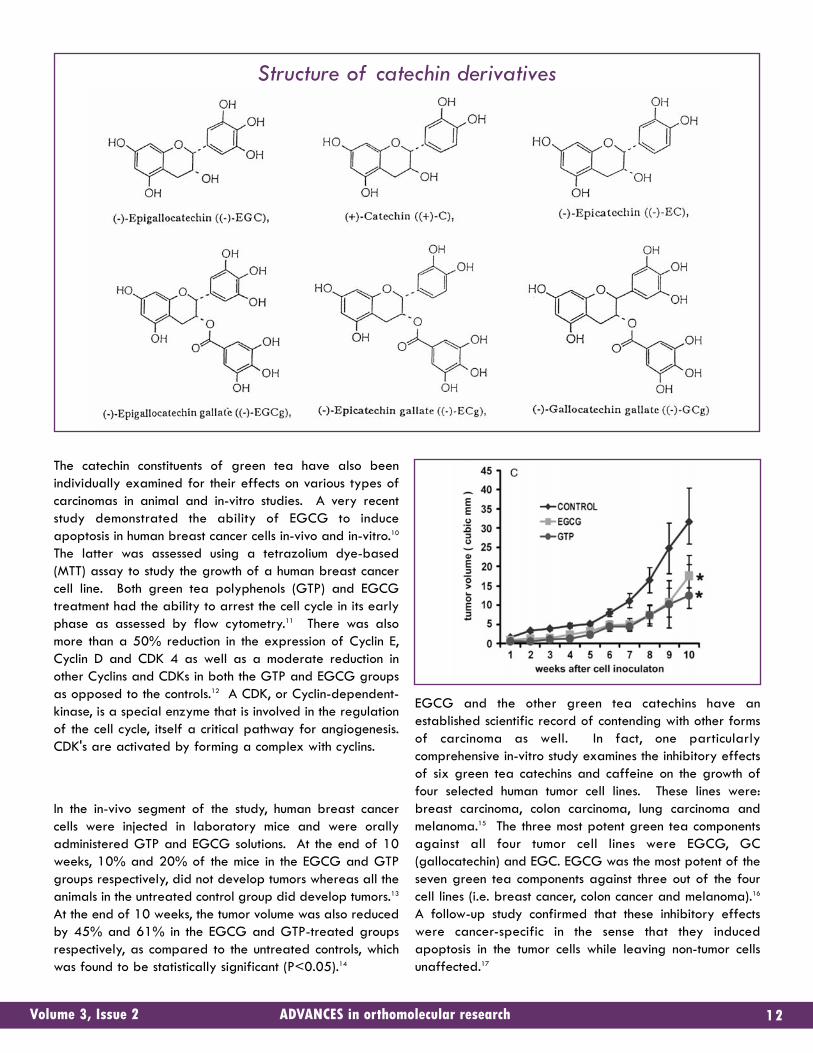
The catechin constituents of green tea have also beenindividually examined for their effects on various types ofcarcinomas in animal and in-vitro studies. A very recentstudy demonstrated the ability of EGCG to induceapoptosis in human breast cancer cells in-vivo and in-vitro.10
The latter was assessed using a tetrazolium dye-based(MTT) assay to study the growth of a human breast cancercell line. Both green tea polyphenols (GTP) and EGCGtreatment had the ability to arrest the cell cycle in its earlyphase as assessed by flow cytometry.11 There was alsomore than a 50% reduction in the expression of Cyclin E,Cyclin D and CDK 4 as well as a moderate reduction inother Cyclins and CDKs in both the GTP and EGCG groupsas opposed to the controls.12 A CDK, or Cyclin-dependent-kinase, is a special enzyme that is involved in the regulationof the cell cycle, itself a critical pathway for angiogenesis.CDK's are activated by forming a complex with cyclins.
In the in-vivo segment of the study, human breast cancercells were injected in laboratory mice and were orallyadministered GTP and EGCG solutions. At the end of 10weeks, 10% and 20% of the mice in the EGCG and GTPgroups respectively, did not develop tumors whereas all theanimals in the untreated control group did develop tumors.13
At the end of 10 weeks, the tumor volume was also reducedby 45% and 61% in the EGCG and GTP-treated groupsrespectively, as compared to the untreated controls, whichwas found to be statistically significant (P<0.05).14
EGCG and the other green tea catechins have anestablished scientific record of contending with other formsof carcinoma as well. In fact, one particularlycomprehensive in-vitro study examines the inhibitory effectsof six green tea catechins and caffeine on the growth offour selected human tumor cell lines. These lines were:breast carcinoma, colon carcinoma, lung carcinoma andmelanoma.15 The three most potent green tea componentsagainst all four tumor cell lines were EGCG, GC(gallocatechin) and EGC. EGCG was the most potent of theseven green tea components against three out of the fourcell lines (i.e. breast cancer, colon cancer and melanoma).16
A follow-up study confirmed that these inhibitory effectswere cancer-specific in the sense that they inducedapoptosis in the tumor cells while leaving non-tumor cellsunaffected.17
12ADVANCES in orthomolecular researchVolume 3, Issue 2
Structure of catechin derivatives
Another study examined EGCG's specific effect on humancolon carcinoma cells. This EGCG study bore many of thesame characteristics as the previous breast cancer study. Ittoo, involved an in-vitro and an in-vivo phase, the latterbeing conducted once again with laboratory mice beinginjected with human cancer cells, this time of the human coloncancer cell variation.18 The in-vivo segment of the studyrevealed that EGCG - in a dose-dependent fashion -decreased the expression of VEGF (Vascular EndothelialGrowth Factor), a critical factor in the process ofangiogenesis.19 Treatment with EGCG inhibited tumorgrowth by 58%, microvessel density by 30%, and tumor cellproliferation by 27% - while nearly doubling tumor cellapoptosis and tripling endothelial cell apoptosis.20
ConclusionThe study of the anticarcinogenic activity of green teacatechins in general and EGCG in particular is still ongoing.While EGCG and other green tea catechins are first andforemost antioxidants, it is clear that EGCG doesconsiderably more than simply scavenge free radicals. It istrue that there can be a great deal of overlap betweenantioxidant and antiinflammatory, antiatherogenic and evenanticarcinogenic mechanisms of action. However, EGCG hasalways provided evidence of its uniquely diffusecapabilities. These include its antimicrobial and antiviralactions, themselves supported by in-vitro evidence. Onesuch example of that evidence is a study that found thatvarious green tea catechins (including EGCG) inhibited theextracellular release of verotoxin from enterohemorrhagicEscherichia coli.21 The ability to induce thermogenesis isanother feature that helps to distinguish EGCG from otherantioxidants. One human study concluded that green teaextracts increased energy expenditure and fat utilization ina manner that goes beyond their caffeine content and is infact synergistic with that content. Compared with theplacebo, 90 mg of EGCG and 50 mg of caffeine produceda significant 4% increase in 24-hour energy expenditureand a significant decrease in 24-hour respiratory quotientin healthy men.22 Supplementation with 50 mg of caffeinealone did not produce significant thermogenic effects.23 (Arespiratory quotient is the ratio of the volume of carbondioxide expired to the volume of oxygen consumed).
This is testimony to the relative diversity of EGCG'sbiological actions, diversity that has led researchers tocombine EGCG with other natural substances in the hope ofproducing a synergistic combination - particularly withrespect to EGCG's anti-carcinogenic potential. One ofthese attempts has involved the ayurvedic herb curcumin,with some initially promising in-vitro results due to the
distinct mechanisms of action of each substance.24 However,more research is needed with this and other substances(including advanced lipid-based delivery systems) to fullymaximize the already-impressive potential of EGCG andother green tea catechins.
References1 Nakagawa K, Ninomiya M, Okubo T, et al. Tea catechin supplementation increasesantioxidant capacity and prevents phospholipid hydroperoxidation in plasma ofhumans. J Agric Food Chem. 1999; 47:3967-3973.2 Miura Y, Chiba T, Miura S, et al. Green tea polyphenols (flavan 3-ols) preventoxidative modification of low density lipoproteins: an ex vivo study in humans. J NutrBiochem. 2000; 11:216-222.3 Nakagawa H, et al. Generation of hydrogen peroxide primarily contributes to theinduction of Fe(II)-dependent apoptosis in Jurkat cells by (-)-epigallocatechin gallate.Carcinogenesis. 2004 Sep;25(9):1567-74. Epub 2004 Apr 16.4 Cao Y, Cao R. Angiogenesis inhibited by drinking tea. Nature. 1999; 398:381.5 Sachinidis A, Seul C, Seewald S, et al. Green tea compounds inhibit tyrosinephosphorylation of PDGF beta-receptor and transformation of A172 humanglioblastoma. FEBS Lett. 2000; 471:51-55.6 Fujiki H, Suganuma M, Imai K, Nakachi K. Green tea: cancer preventive beverageand/or drug. Cancer Lett. 2002 Dec 15; 188(1-2): 9-13.7 Ibid.8 Ibid.9 Hrelia S, et al. Nutritional interventions to counteract oxidative stress in cardiac cells.Ital J Biochem. 2004 Dec;53(4):157-63.10 Thangapazham RL, et al. Green tea polyphenols and its constituent epigallocatechingallate inhibits proliferation of human breast cancer cells in vitro and in vivo. CancerLett. 2006 Mar 3; [Epub ahead of print].11 Ibid.12 Ibid.13 Ibid.14 Ibid.15 Valcic S, et al. Inhibitory effect of six green tea catechins and caffeine on the growthof four selected human tumor cell lines. Anticancer Drugs. 1996 Jun;7(4):461-8.16 Ibid.17 Chen ZP et al. Green tea epigallocatechin gallate shows a pronounced growthinhibitory effect on cancerous cells but not on their normal counterparts. Cancer Lett.1998 Jul 17;129(2):173-9.18 Jung YD et al. EGCG, a major component of green tea, inhibits tumour growth byinhibiting VEGF induction in human colon carcinoma cells. Br J Cancer. 2001 Mar23;84(6):844-50.19 Ibid.20 Ibid.21 Sugita-Konishi Y, et al. Epigallocatechin gallate and gallocatechin gallate in greentea catechins inhibit extracellular release of Vero toxin from enterohemorrhagicEscherichia coli. O157:H7. Biochem Biophys Acta. 1999; 1472:42-50.22 Dulloo AG, Seydoux J, Girardier L, et al. Green tea and thermogenesis: interactionsbetween catechin-polyphenols, caffeine and sympathetic activity. Int J Obes RelatMetab Disord. 2000; 24:252-258. 23 Ibid.24 Khafif A, et al. Quantitation of chemopreventive synergism between (-)-epigallocatechin-3-gallate and curcumin in normal, premalignant and malignant humanoral epithelial cells. Carcinogenesis. 1998 Mar;19(3):419-24.
ADVANCES in orthomolecular research Volume 3, Issue 213
ADVANCES in orthomolecular research Volume 3, Issue 214
FFuu ccoo iiddaannfrom the ocean
to your cellsFar too many are reluctant to treat cancer naturally. This isunderstandable. Outrageous claims have been made in thepast with regards to nutritional supplements used for thosesuffering from cancer. Unfortunately, this has lead todistrust and skepticism. Although more research is needed,there is no doubt that nutrients can be powerful allies in thefight against cancer.
Nutrients can be used to prevent1,2 and treat3,4 neoplasia.Nutrients can also be used to support radiation andchemotherapy.5,6 It is also important to realize thatprescription medications are a leading cause of death inNorth America7 and that chemotherapy, although proveneffective for the treatment of cancer, is also a frequentcause of death in cancer patients.8 Nutritional strategiesthat can support the body while patients are undergoingchemotherapy or radiation treatments should not bediscounted.
Plants have long been used for their health benefits. Manyplant's first documented use dates back thousands of years.Seaweed has not only been used as a food source but alsoas a medicine for thousands of years. Fucoidans are oneimportant constituent of seaweed, first mentioned in themedical literature in 1970. Fucoidans are sulfatedpolysaccharides extracted from brown algae and containfucose, uronic acid and sulphate. Fucoidans are responsiblefor the characteristic slippery texture of seaweed.
If you only know algae as the dark stuff that is wrappedaround your raw fish at the sushi bar, you are missing out onone of the greatest health resources available to date.Humans and animals rely on their immune systems to combatdisease. Plants however do not have immune systems andmust produce chemicals that prevent and take care ofinfections and parasites - those chemicals are responsiblefor the medicinal properties of plants. Oceans contain mostof the living space on earth and their potential as sourcesof health-promoting nutrients remain largely unknown.9
Nonetheless, fucoidans have emerged from the sea andhave been the subject of over 600 medical papers.10
Research has shown that fucoidans possess potentantiproliferative properties,11 are effective antithromboticagents,12 reduce inflammation,13 and prevent tumor growthand metastasis.14
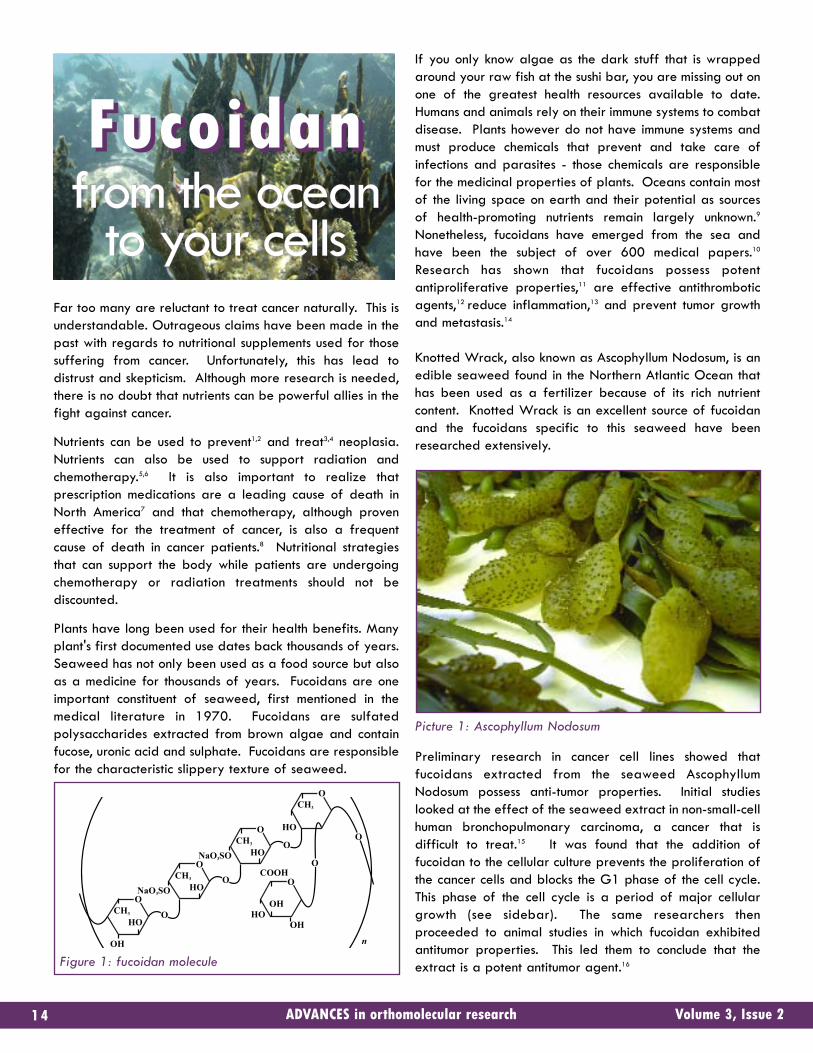
Knotted Wrack, also known as Ascophyllum Nodosum, is anedible seaweed found in the Northern Atlantic Ocean thathas been used as a fertilizer because of its rich nutrientcontent. Knotted Wrack is an excellent source of fucoidanand the fucoidans specific to this seaweed have beenresearched extensively.
Picture 1: Ascophyllum Nodosum
Preliminary research in cancer cell lines showed thatfucoidans extracted from the seaweed AscophyllumNodosum possess anti-tumor properties. Initial studieslooked at the effect of the seaweed extract in non-small-cellhuman bronchopulmonary carcinoma, a cancer that isdifficult to treat.15 It was found that the addition offucoidan to the cellular culture prevents the proliferation ofthe cancer cells and blocks the G1 phase of the cell cycle.This phase of the cell cycle is a period of major cellulargrowth (see sidebar). The same researchers thenproceeded to animal studies in which fucoidan exhibitedantitumor properties. This led them to conclude that theextract is a potent antitumor agent.16
NaO3SO
CH3
HO
OH
O
O
NaO3SO
CH3
HO
O
O
CH3
HO
O
O
CH3
O
O
O
O
HOOH
HO
n
OH
COOH
Figure 1: fucoidan molecule
15ADVANCES in orthomolecular researchVolume 3, Issue 2
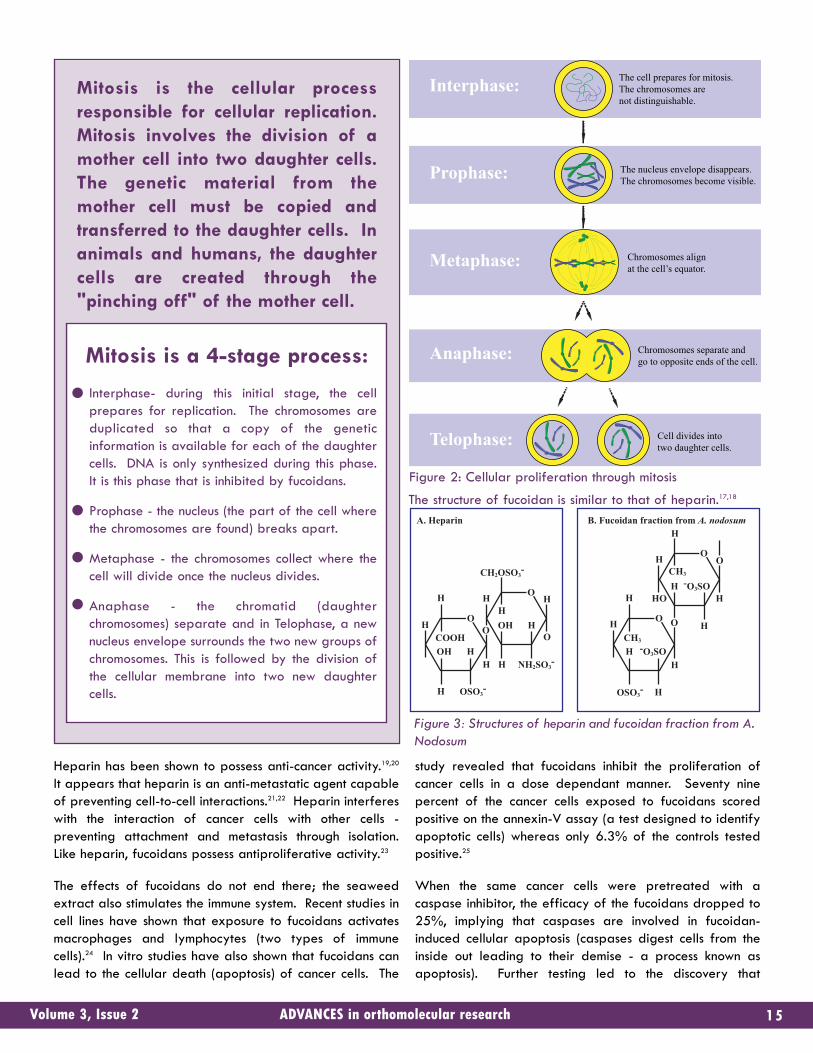
Interphase:
Prophase:
Metaphase:
Anaphase:
Telophase:
The cell prepares for mitosis. The chromosomes are not distinguishable.
The nucleus envelope disappears. The chromosomes become visible.
Chromosomes align at the cell’s equator.
Chromosomes separate and go to opposite ends of the cell.
Cell divides into two daughter cells.
A. Heparin
H
H
OHCOOH
HO
O
O
H
OSO3-
CH2OSO3-
H
OHH
H H
OH
NH2SO3-H
B. Fucoidan fraction from A. nodosum
H
H
-O3SOCH3
H O O
O
H
OSO3-
H
HCH3
H O
HHO-O3SO
H
H
Mitosis is the cellular processresponsible for cellular replication.Mitosis involves the division of amother cell into two daughter cells.The genetic material from themother cell must be copied andtransferred to the daughter cells. Inanimals and humans, the daughtercells are created through the"pinching off" of the mother cell.
Mitosis is a 4-stage process:
Interphase- during this initial stage, the cellprepares for replication. The chromosomes areduplicated so that a copy of the geneticinformation is available for each of the daughtercells. DNA is only synthesized during this phase.It is this phase that is inhibited by fucoidans.
Prophase - the nucleus (the part of the cell wherethe chromosomes are found) breaks apart.
Metaphase - the chromosomes collect where thecell will divide once the nucleus divides.
Anaphase - the chromatid (daughterchromosomes) separate and in Telophase, a newnucleus envelope surrounds the two new groups ofchromosomes. This is followed by the division ofthe cellular membrane into two new daughtercells.
Figure 2: Cellular proliferation through mitosis
Figure 3: Structures of heparin and fucoidan fraction from A.Nodosum
The structure of fucoidan is similar to that of heparin.17,18
Heparin has been shown to possess anti-cancer activity.19,20
It appears that heparin is an anti-metastatic agent capableof preventing cell-to-cell interactions.21,22 Heparin interfereswith the interaction of cancer cells with other cells -preventing attachment and metastasis through isolation.Like heparin, fucoidans possess antiproliferative activity.23
The effects of fucoidans do not end there; the seaweedextract also stimulates the immune system. Recent studies incell lines have shown that exposure to fucoidans activatesmacrophages and lymphocytes (two types of immunecells).24 In vitro studies have also shown that fucoidans canlead to the cellular death (apoptosis) of cancer cells. The
study revealed that fucoidans inhibit the proliferation ofcancer cells in a dose dependant manner. Seventy ninepercent of the cancer cells exposed to fucoidans scoredpositive on the annexin-V assay (a test designed to identifyapoptotic cells) whereas only 6.3% of the controls testedpositive.25
When the same cancer cells were pretreated with acaspase inhibitor, the efficacy of the fucoidans dropped to25%, implying that caspases are involved in fucoidan-induced cellular apoptosis (caspases digest cells from theinside out leading to their demise - a process known asapoptosis). Further testing led to the discovery that
•
•••
fucoidans influence cellular signaling and promoteapoptosis in cancer cells by down-regulating extracellularsignals such as GSK and ERK.26 These two cellular pathwayshave previously been linked to the initiation of apoptosis.27,28
Graph 1: Detection of apoptosis by annexin-V staining.Redrawn from (29)
The activity of fucoidans appears to be related to theirmolecular weight, charge and degree of sulfation.30 Forinstance, studies on low molecular weight fucoidans havedemonstrated that the molecule influences cellular processesimportant for angiogenesis, endothelial cell tube formationand cell migration. Low molecular weight fucoidans mayprove to be invaluable to patients with atherosclerosis andcardiovascular disease. Studies have also shown that lowmolecular weight fucoidans prevent cellular proliferation.31
Cellular proliferation is the increase in cell numberengendered through cellular division - a process that iscentral to cancer.
Meanwhile, other researchers have shown that fucoidanscan prevent angiogenesis by altering the binding of growthfactors to cellular receptors.32 This apparent dichotomy canbe explained by the molecular weight of the fucoidanfraction studied. Previous in vitro studies have shown that ahigh molecular weight hyluronan is antiangiogenic whereasthe smaller but otherwise similar hyaluronanoligosaccharides stimulate the formation of new bloodvessels.33 Such divergence may also apply to fucoidans,with low molecular weight fractions promoting angiogenesis
and larger molecules preventing it.34 Studies have alsodemonstrated that sulfated polysaccharides such asfucoidans prevent the metastasis of cancer cells. Thisactivity is attributable to an interference with cellularreceptors, which is mediated by fucoidans. This prevents thepassage of the cancerous cell through the capillary wall,thereby discouraging metastasis.35
Studies show that the ability of fucoidan to inhibit cellularproliferation is also dependant on the degree of sulfation -more sulfated fucoidans being more effective at preventingangiogenesis.36,37
Fucoidans possess several other health benefits, whichinclude the reduction of inflammation through theinactivation of the complement pathway and by inhibitingthe release of nitric oxide from macrophages.38,39 Fucoidansare also anticoagulants with antithrombotic activity,40,41 andcan modulate cellular adhesion and growth factor release.42
Epidemiological evidence speaks loudly to the healthbenefits associated with the consumption of seaweed. Thetraditional Japanese diet is comprised of roughly 10-25%seaweed.43 On the other hand, Western nations have avery low consumption of seaweed. Chronic disease rates innations consuming greater amounts of seaweed suggest abeneficial influence of seaweed on health. For example,breast cancer rates in Japan are 42.2 per 100,000 andrepresent roughly a third of the North American rate of125.9 per 100,000.44 Granted that several other factorsare important in explaining this difference, but given theweight of the scientific evidence supporting the value ofseaweed, there is little doubt that fucoidans and otherphytonutrients go a long way towards explaining thisdisparity.
References1 Waters, D.J., S. Shen, D.M. Cooley, et al. 2003. Effects of dietary Se supplementationon DNA damage and apoptosis in canine prostate. J. Natl. Cancer Inst. 95: 237-241.2 Flanagan JN, Young MV, Persons KS, Wang L, Mathieu JS, Whitlatch LW, Holick MF,Chen TC. Vitamin D metabolism in human prostate cells: implications for prostate cancerchemoprevention by vitamin D. Anticancer Res. 2006 Jul-Aug;26(4A):2567-72.3 Buletic Z, Soprano KJ, Soprano DR. Retinoid targets for the treatment of cancer. CritRev Eukaryot Gene Expr. 2006;16(3):193-210.4 Ferah Y, Ayse K, Mustafa C, Ugur S, Murat G, Lale AI. Possible therapeutic role ofvitamin D3 in aggressive fibromatosis. Jpn J Clin Oncol. 2004 Aug;34(8):472-5.5 Basu P, Biswas J, Mandal R, Choudhury P. Is interferon-alpha and retinoic acidcombination along with radiation superior to chemo-radiation in the treatment ofadvanced carcinoma of cervix? Indian J Cancer. 2006 Apr-Jun;43(2):54-9.6 Kassouf W, Highshaw R, Nelkin GM, Dinney CP, Kamat AM. Vitamins C and K3sensitize human urothelial tumors to gemcitabine. J Urol. 2006 Oct;176(4 Pt 1):1642-7.7 Lazarou J, Pomeranz BH, Corey PN. Incidence of adverse drug reactions inhospitalized patients: a meta-analysis of prospective studies. JAMA. 1998 Apr15;279(15):1200-5.8 Ohe Y, Yamamoto S, Suzuki K, Hojo F, Kakinuma R, Matsumoto T, Ohmatsu H, NishiwakiY. Risk factors of treatment-related death in chemotherapy and thoracic radiotherapyfor lung cancer. Eur J Cancer. 2001 Jan;37(1):54-63.
ADVANCES in orthomolecular research Volume 3, Issue 216
80
60
40
20
0
Ann
exin
pos
itive
cel
ls (%
)
Control Fucoidan Fucoidan+zVAD
9 Benchley P, Gradwohl J. Ocean Planet: Writings and Images of the Sea. Harry N.Abrams Inc10 Tanaka K, Sorai S. Hydrolysis of fucoidan by abalone liver alpha-L-fucosidase. FEBSLett. 1970 Jul 15;9(1):45-48.11 McCaffrey TA, Falcone DJ, Borth W, Brayton CF, Weksler BB. Fucoidan is a non-anticoagulant inhibitor of intimal hyperplasia. Biochem Biophys Res Commun. 1992 Apr30;184(2):773-81.12 Thorlacius H, Vollmar B, Seyfert UT, Vestweber D, Menger MD. The polysaccharidefucoidan inhibits microvascular thrombus formation independently from P- and L-selectinfunction in vivo. Eur J Clin Invest. 2000 Sep;30(9):804-10.13 Yang JW, Yoon SY, Oh SJ, Kim SK, Kang KW. Bifunctional effects of fucoidan on theexpression of inducible nitric oxide synthase. Biochem Biophys Res Commun. 2006 Jul21;346(1):345-50.14 Riou D, Colliec-Jouault S, Pinczon du Sel D, Bosch S, Siavoshian S, Le Bert V, TomasoniC, Sinquin C, Durand P, Roussakis C. Antitumor and antiproliferative effects of a fucanextracted from ascophyllum nodosum against a non-small-cell bronchopulmonarycarcinoma line. Anticancer Res. 1996 May-Jun;16(3A):1213-8.15 Riou D, Colliec-Jouault S, Pinczon du Sel D, Bosch S, Siavoshian S, Le Bert V, TomasoniC, Sinquin C, Durand P, Roussakis C. Antitumor and antiproliferative effects of a fucanextracted from ascophyllum nodosum against a non-small-cell bronchopulmonarycarcinoma line. Anticancer Res. 1996 May-Jun;16(3A):1213-8.16 Riou D, Colliec-Jouault S, Pinczon du Sel D, Bosch S, Siavoshian S, Le Bert V, TomasoniC, Sinquin C, Durand P, Roussakis C. Antitumor and antiproliferative effects of a fucanextracted from ascophyllum nodosum against a non-small-cell bronchopulmonarycarcinoma line. Anticancer Res. 1996 May-Jun;16(3A):1213-8.17 Logeart D, Prigent-Richard S, Jozefonvicz J, Letourneur D. Fucans, sulfatedpolysaccharides extracted from brown seaweeds, inhibit vascular smooth muscle cellproliferation. I. Comparison with heparin for antiproliferative activity, binding andinternalization. Eur J Cell Biol. 1997 Dec;74(4):376-84.18 Giraux JL, Matou S, Bros A, Tapon-Bretaudiere J, Letourneur D, Fischer AM.Modulation of human endothelial cell proliferation and migration by fucoidan andheparin. Eur J Cell Biol. 1998 Dec;77(4):352-9.19 Niers TM, Klerk CP, Dinisio M, Van Noorden CJ, Buller HR, Reitsma PH, Richel DJ.Mechanisms of heparin induced anti-cancer activity in experimental cancer models. CritRev Oncol Hematol. 2006 Oct 2820 Kragh M, Loechel F. Non-anti-coagulant heparins: a promising approach forprevention of tumor metastasis (review). Int J Oncol. 2005 Oct;27(4):1159-67.21 Kragh M, Loechel F. Non-anti-coagulant heparins: a promising approach forprevention of tumor metastasis (review). Int J Oncol. 2005 Oct;27(4):1159-67.22 Niers TM, Klerk CP, Dinisio M, Van Noorden CJ, Buller HR, Reitsma PH, Richel DJ.Mechanisms of heparin induced anti-cancer activity in experimental cancer models. CritRev Oncol Hematol. 2006 Oct 2823 Logeart D, Prigent-Richard S, Boisson-Vidal C, Chaubet F, Durand P, Jozefonvicz J,Letourneur D. Fucans, sulfated polysaccharides extracted from brown seaweeds, inhibitvascular smooth muscle cell proliferation. II. Degradation and molecular weight effect.Eur J Cell Biol. 1997 Dec;74(4):385-90.24 Choi EM, Kim AJ, Kim YO, Hwang JK. Immunomodulating activity of arabinogalactanand fucoidan in vitro. J Med Food. 2005 Winter;8(4):446-53.25 Aisa Y, Miyakawa Y, Nakazato T, Shibata H, Saito K, Ikeda Y, Kizaki M. Fucoidaninduces apoptosis of human HS-sultan cells accompanied by activation of caspase-3 anddown-regulation of ERK pathways. Am J Hematol. 2005 Jan;78(1):7-14.26 Aisa Y, Miyakawa Y, Nakazato T, Shibata H, Saito K, Ikeda Y, Kizaki M. Fucoidaninduces apoptosis of human HS-sultan cells accompanied by activation of caspase-3 anddown-regulation of ERK pathways. Am J Hematol. 2005 Jan;78(1):7-14.27 Song L, De Sarno P, Jope RS. Central role of glycogen synthase kinase-3beta inendoplasmic reticulum stress-induced caspase-3 activation. J Biol Chem. 2002 Nov22;277(47):44701-8.28 Loberg RD, Vesely E, Brosius FC 3rd. Enhanced glycogen synthase kinase-3betaactivity mediates hypoxia-induced apoptosis of vascular smooth muscle cells and isprevented by glucose transport and metabolism. J Biol Chem. 2002 Nov1;277(44):41667-73.29 Aisa Y, Miyakawa Y, Nakazato T, Shibata H, Saito K, Ikeda Y, Kizaki M. Fucoidaninduces apoptosis of human HS-sultan cells accompanied by activation of caspase-3 anddown-regulation of ERK pathways. Am J Hematol. 2005 Jan;78(1):7-14.30 Boisson-Vidal V, Zemani F, Caligiuri G, Galy-Fauroux, Colliec-Jouault S, Helley D,Fischer AM. Neoangiogenesis Induced by Progenitor Endothelial Cells: Effect ofFucoidan from Marine Algae. Cardiovascular & Hematological Agents in MedicinalChemistry, 2007, 5.31 Koyanagi S, Tanigawa N, Nakagawa H, Soeda S, Shimeno H. Oversulfation offucoidan enhances its anti-angiogenic and antitumor activities. Biochem Pharmacol.2003 Jan 15;65(2):173-9.32 Koyanagi S, Tanigawa N, Nakagawa H, Soeda S, Shimeno H. Oversulfation offucoidan enhances its anti-angiogenic and antitumor activities. Biochem Pharmacol.2003 Jan 15;65(2):173-9.
33 Rahmanian M, Pertoft H, Kanda S, Christofferson R, Claesson-Welsh L, Heldin P.Hyaluronan oligosaccharides induce tube formation of a brain endothelial cell line invitro. Exp Cell Res. 1997 Nov 25;237(1):223-30.34 Matou S, Helley D, Chabut D, Bros A, Fischer AM. Effect of fucoidan on fibroblastgrowth factor-2-induced angiogenesis in vitro. Thromb Res. 2002 May 15;106(4-5):213-21.35 Coombe DR, Parish CR, Ramshaw IA, Snowden JM. Analysis of the inhibition of tumourmetastasis by sulphated polysaccharides. Int J Cancer. 1987 Jan 15;39(1):82-8.36 Koyanagi S, Tanigawa N, Nakagawa H, Soeda S, Shimeno H. Oversulfation offucoidan enhances its anti-angiogenic and antitumor activities. Biochem Pharmacol.2003 Jan 15;65(2):173-9.37 Riou D, Colliec-Jouault S, Pinczon du Sel D, Bosch S, Siavoshian S, Le Bert V, TomasoniC, Sinquin C, Durand P, Roussakis C. Antitumor and antiproliferative effects of a fucanextracted from ascophyllum nodosum against a non-small-cell bronchopulmonarycarcinoma line. Anticancer Res. 1996 May-Jun;16(3A):1213-8. 38 Tissot B, Montdargent B, Chevolot L, Varenne A, Descroix S, Gareil P, Daniel R.Interaction of fucoidan with the proteins of the complement classical pathway. BiochimBiophys Acta. 2003 Sep 23;1651(1-2):5-16.39 Yang JW, Yoon SY, Oh SJ, Kim SK, Kang KW. Bifunctional effects of fucoidan on theexpression of inducible nitric oxide synthase. Biochem Biophys Res Commun. 2006 Jul21;346(1):345-50.40 Nardella A, Chaubet F, Boisson-Vidal C, Blondin C, Durand P, Jozefonvicz J.Anticoagulant low molecular weight fucans produced by radical process and ionexchange chromatography of high molecular weight fucans extracted from the brownseaweed Ascophyllum nodosum. Carbohydr Res. 1996 Aug 19;289:201-8.41 Marais MF, Joseleau JP. A fucoidan fraction from Ascophyllum nodosum. CarbohydrRes. 2001 Nov 8;336(2):155-9.42 Nardella A, Chaubet F, Boisson-Vidal C, Blondin C, Durand P, Jozefonvicz J.Anticoagulant low molecular weight fucans produced by radical process and ionexchange chromatography of high molecular weight fucans extracted from the brownseaweed Ascophyllum nodosum. Carbohydr Res. 1996 Aug 19;289:201-8.43 Skibola CF. The effect of Fucus vesiculosus, an edible brown seaweed, uponmenstrual cycle length and hormonal status in three pre-menopausal women: a casereport. BMC Complement Altern Med. 2004 Aug 4;4:10.44 Pisani P, Bray F, Parkin DM. Estimates of the world-wide prevalence of cancer for 25sites in the adult population. Int J Cancer. 2002 Jan 1;97(1):72-81.
17ADVANCES in orthomolecular researchVolume 3, Issue 2
SeMC stands alone as a200 microgram seleniumsupplement, distinguishedby the use of the bestselenium available: Se-methylselenocysteine.
SeMC is backed byresearch as being the mostpotent and least toxic formof selenium available.
SeMCSimply Selenium
ADVANCES in orthomolecular research Volume 3, Issue 218These statements have not been evaluated by the Food and Drug Administration. This product is not intended to diagnose, treat, cure, or prevent any disease.
Harness the power of green tea with ECGC MAX.
www.aor.ca
We have all heard of the health benefitsassociated with green tea. Unlike black tea,which is fermented, green tea undergoes littleprocessing which leaves the naturalantioxidants found in green tea intact.
EGCG MAX is a high-potency standardized extract ofgreen tea, high in epigallocatechin gallate (EgCG),believed to be the key phytonutrient in green tea,responsible for its health benefits.
Studies most consistently report health benefits in persons drinking ten cupsa day of high-EgCG sencha-style Japanese green tea; each cup ofthis tea contains 150 milligrams of EgCG.
The labels of most green tea extracts exaggerate thenumber of cups of tea represented in their capsules bycomparing the product to poor-quality teas. EGCGMAX allows you to more fully enjoy the healthyproperties of a sencha-rich lifestyle without consuminglarge volumes of tea.
EGCGMAX ™Green Tea perfected!
19ADVANCES in orthomolecular researchVolume 3, Issue 2
LL ii ggnnaannss Getting the Balance RightLignans are a relatively obscure sub-category ofphytonutrients that have recently been gaining an increasingamount of attentive interest from the scientific community.Phytonutrients themselves are broadly defined asbeneficial, naturally-occurring plant compounds, withphytoestrogens being one of the most significant types.True to their name, phytoestrogens mildly mimic the effectsof human estrogen. That being said, lignans are widelyrecognized as one of the two major categories ofphytoestrogens (the other being isoflavones). Lignans canbe found in trace amounts in certain plants, unrefined grainproducts, fruits, vegetables, and seeds - notably flax andsesame. One lignan in particular, namely the patentedHMRlignan(tm), is 7-hydroxymatairesinol, which is foundnaturally in the Norway Spruce (Picea abies), a species oftree native to the Scandinavian Peninsula.
Finland, where 7-hydroxymatairesinol was developed, is acenter of academic excellence for the study ofphytoestrogens. It was researchers at the prestigiousUniversity of Helsinki who established the relationshipbetween the lignan 7-hydroxymatairesinol and lowerincidences of breast cancer, prostate cancer andcardiovascular disease. Upon ingestion, 7-hydroxymatairesinol is directly converted into 'humanlignans', primarily enterolactone, which exerts a mild,estrogen-like activity. Put more succinctly, enterolactone isformed by intestinal bacteria from precursors in plant foods.The gentle, hormone-like action of enterolactone isbeneficial in menopausal and post-menopausal women aswell as middle-aged men due to its protection againstgender-related hormonally induced cancers (i.e. of thebreast and prostate) as well as its overall cardiovascularbenefits. 7-hydroxymatairesinol does not need to becleaved in the gastrointestinal tract before it can bemetabolized into the desired molecule enterolactone,effectively making 7-hydroxymatairesinol the world's firstand only direct enterolactone precursor.
Upon ingestion, 7-hydroxymatairesinol isdirectly converted into 'human lignans',
primarily enterolactone, which exerts a mild,estrogen-like activity
Enter Enterolactone Enterolactone is one of the most recent factors to be isolatedand identified for its direct association with cardiovascularhealth. In fact, large-scale human studies published in 2002and 2003 in both the United States and Finlandrespectively established the link between cardiovascularmortality rates and plasma enterolactone levels in both menand women. The US study, known as the FraminghamOffspring Study, was cross-sectional and highly extensive inits scope, involving 939 post-menopausal women.1 It foundthat the women with the lowest intake of lignans were threetimes more likely to experience some sort of cardiovascularcondition according to a test called the Metabolic SyndromeScore, designed in accordance with WHO (World HealthOrganization) criteria.2 As noted earlier, lignans are theprecursors to enterolactone and their intake increasesplasma enterolactone levels. The Finnish study examined1,889 middle-aged men over an average period of 12years and found "significant associations between elevatedserum enterolactone concentration and reduced risk ofcoronary heart disease and cardiovascular disease -related mortality".3
Cumulative coronary heart disease (CHD)-related mortality inmen according to quartiles of serum enterolactoneconcentration, adjusted for age and year of examination andof serum enterolactone measurement. Quartile 1 indicates aserum enterolactone concentration of 0.2 to 6.9 nmol/L;quartile 2, 7.0 to 13.7 nmol/L; quartile 3, 13.8 to 23.8nmol/L; and quartile 4, 23.9 to 88.7 nmol/L.)
The diets of the women in the Framingham offspring studyin fact included a variety of lignans and isoflavones,including: Secoisolariciresinol, Genistein, Daidzein,Formononetin, Matairesinol, Coumestrol, and Biochanin A.4
The variety of lignans and isoflavones in the diets of themen in the Finnish study were of course equally assorted.However, scientists eventually determined that matairesinol,in the form of 7-hydroxymatairesinol, is the most readilyconverted to enterolactone.
Antioxidant - Tip of theIcebergDue to the biphenolic (two-ringed) structure ofenterolactone (a feature shared by most antioxidants), itdemonstrates what can be defined as potent anti-oxidantcapabilities - thus contributing to its role in cardiovascularhealth. These capabilities were identified in a study wherelow serum enterolactone levels were directly associatedwith increased in-vivo lipid peroxidation.5 This is animportant discovery since lipid peroxidation is a cornerstonein the study of free radical generation, as lipids form thebackbone of cell membranes and their oxidativedegeneration precedes a free radical chain-reaction.
In fact, 7-hydroxymatairesinol has been shown to exhibitgreater free radical-scavenging capabilities than thestandard reference antioxidant compounds Trolox (a water-soluble form of vitamin E), butylated hydroxyanisol (BHA)and butylated hydroxytoluene (BHT). A highly detailedstudy examining the antioxidant properties of 7-hydroxymatairesinol in direct comparison with Trolox, BHAand BHT revealed some specifically interesting capabilitieson the part of 7-hydroxymatairesinol.6 Tests withlaboratory mice revealed that 7-hydroxymatairesinol was amore effective antioxidant than Trolox in all assays andmore effective than BHT or BHA in lipid peroxidation andsuperoxide scavenging assays.7 Enterolactone's antioxidantcapability may also encompass an anti-inflammatorycapacity as well.
Basic ChemoprotectivePharmacokineticsAn early study with laboratory mice indicated that 7-hydroxymatairesinol (or simply hydroxymatairesinol - andby extension enterolactone) mediates its chemopreventiveeffect through the Apc-beta-catenin pathway.8 Scientistsbased this hypothesis on the fact that hydroxymatairesinolnormalized beta-catenin levels in adenoma tissue in theaforementioned study.9 Beta-catenin is a central componentin the operation of cadherins, which are a class of proteinsthat ensure proper intracellular binding. The Apc (or theadenomatous polyposis coli gene - found in most colorectalcancer polyps) is important for the transduction of beta-catenin. This remains the most explicit hypothesis behindhydroxymatairesinol's mechanism of action.
ADVANCES in orthomolecular research Volume 3, Issue 220
ANTIOXIDANT ACTION OF 7-hydroxymatairesinol
Amounts of 7-hydroxymatairesinol or Trolox to elicit activity
ANTIOXIDANT FEATURE Trolox
Inhibition of lipid peroxidation (μmol/L)* 0.06 0.22
Inhibition of LDL oxidation (nmol/mg LDL)* 6.7 15.5
LDL incorporation (nmol/mg LDL)* 130 744
Superoxide anion scavenging (μmol/L)* 5.6 18.8
Peroxyl radical scavenging (ratio) 1 : 4 1 : 2
7-hydroxymatairesinol1
2
3
4
HORMONAL HEALTHBreastBreast cancer is widely considered by the medicalcommunity to be a hormone-regulated disease withestrogen known to play a disproportionately large role in itsdevelopment. Enterolactone inhibits estrogen by gentlybinding to the estrogen receptors, effectively serving as amild anti-estrogen in its own right.10 Furthermore,enterolactone stimulates the production of a naturalbiochemical called sex hormone-binding globulin (SHBG),which also binds to circulating estrogen, effectively loweringthe estrogen level available to the cancer cell and inhibitingits growth.11 Finally, there is evidence that enterolactonecompromises the very synthesis of estrogen itself byblocking aromatase, a key enzyme required for thesynthesis of estradiol (an important estrogenic hormone).12
This too, results in lower amounts of circulating estrogenavailable to any abnormal cells.
These chemopreventative effects in relation to anti-estrogenic activity were outlined in a study examining theinfluence of hydroxymatairesinol on uterine carcinogenesisamong laboratory rats. This study demonstrated, in a dose-dependent manner, that incidences of uterineadenocarcinoma among the study group animals were up to50% lower than those among the control group.13 The samestudy also revealed a delay in the start of persistent estrus(observed at eight months of age) among the 7-hydroxymatairesinol groups compared with the controlgroup.14
These observations have led to other studies examining 7-hydroxymatairesinol supplementation with regard to breastcancer itself. One such study at the National CancerResearch Institute of Italy in Genoa examined 258 womendiagnosed with the development of at least one breast cystand epidermal growth factor (EGF) concentration values,with 12 women developing breast cancer during the courseof the study.15 The researchers were trying to determine ifenterolactone accumulates in breast cyst fluid and whetherit correlates with the risk of breast cancer development.They found that while enterolactone does indeedaccumulate in cysts, it appears to significantly decrease therisk of breast cancer development among patients whosecysts have high EGF concentrations.16 These findings addeddepth to a previous study conducted in Finland at theNational Public Health Institute in Helsinki. This study,conducted among 194 breast cancer cases (68premenopausal and 126 postmenopausal) and 208community-based controls, examined the direct correlation
between serum enterolactone levels the risk of breastcancer.17 The researchers clearly determined that elevatedserum enterolactone levels were "significantly inverselyassociated with [the] risk of breast cancer".18
ProstateIn prostate health, an increasing body of evidence points tothe benefits of lignans in the maintenance of prostatic well-being, and suggests that enterolactone may directly inhibitthe growth and signaling of cancer cells. The first officialstudy to verify this took place in 2001 at Duke UniversityMedical Centre in Durham, North Carolina, USA, wherescientists examined enterolactone's effect on three humanprostate cancer cell lines (PC-3, DU-145 and LNCaP) in-vitro.19 They found that enterolactone was in the ratherunique position of having 'significantly inhibited the growthof all [3] cell lines' in comparison with the other compoundstested, namely enterodiol and genistein.20 Research has alsoindicated that enterolactone's specific anti-estrogenicactivities may reduce the growth of a hormone-dependentprostate via the 'significant decreases' in circulating levels ofprostate-specific antigen (PSA) and total cholesterol.21
A landmark in-vivo study took place in 2003 using purifiedlignans to determine their inhibitory effects on prostatecancer.22 Laboratory mice were injected subcutaneouslywith cancerous LNCaP cells and then fed either a controldiet or diets enriched with 7-hydroxymatairesinol.23 At theend of the nine-week study, the animals fed the 7-hydroxymatairesinol-enriched diets had tumor cellapoptosis rates that were four times higher than that of thecontrol group.24 Furthermore, the average weights of thetumors in the control group animals were between just undertwo-and-a-half to nearly three times greater than those ofthe study groups.25
Managing MenopauseThere are other areas where 7-hydroxymatairesinol canexert benefits as well. It must be remembered thatenterolactone serves as both a mild estrogen and anti-estrogen. This is of particular importance to themanagement of menopause, namely the several-yearperiod when estrogen levels are in flux, leading to acessation of menstruation. When estrogen levels decline,enterolactone exerts a weak estrogenic effect, mimickingthe presence of estrogen. When estrogen levels are toohigh, enterolactone occupies and blocks estrogen receptors,thereby smoothing the peaks and valleys.
21ADVANCES in orthomolecular researchVolume 3, Issue 2
In fact, a recent Dutch study conducted at the Julius Centerfor Health Sciences and Primary Care in Utrecht examinedhow dietary intake of two phytoestrogens - lignans andisoflavones - in the typical Western diet may affectcognitive function in postmenopausal women. The studyinvolved 394 healthy postmenopausal women who had notused hormonal replacement therapy since their lastmenstrual period.26 Their intake of phytoestrogens duringthe year prior to enrolment in the study was estimated by avalidated food frequency questionnaire.27 Cognitivefunction was assessed by a mini-mental state examination(MMSE), which involved questions and tasks associated withorientation, registration, attention, calculation, recall andlanguage.28 After adjustment for confounders, women whoconsumed higher levels of lignans performed better in theMMSE, whereas isoflavone intake appeared to have noeffect on cognitive function.29
Bone HealthThe aforementioned estrogen-stabilizing capability mayalso have implications for bone health, and indeed a 2002Korean study identified a link between enterolactone levelsand incidence of osteoporosis in post-menopausal women.30
The scientists concluded that Bone Marrow Density (BMD) ofthe lumbar spine (L2-L4), the femoral neck and Ward'striangle 'correlated positively with urinary enterolactone'among the 75 post-menopausal women (ages ranging from52-65 years) who participated in the study.31
In summation, 7-hydroxymatairesinol, which most readilyconverts to enterolactone in the human body, can accuratelybe described as a phytonutrient stabilizer of estrogen. Thiselemental definition underlies the complex biologicalmechanism of action by which 7-hydroxymatairesinol exertsits hormonal cascade. This cascade results in precisely thebiochemical changes required for optimal health.
References1 de Kleijn MJ, van der Schouw YT, Wilson PW, Grobbee DE, Jacques PF. Dietary intakeof phytoestrogens is associated with a favorable metabolic cardiovascular risk profile inpostmenopausal U.S.women: the Framingham study. J. Nutr. 2002 Feb;132(2):276-82.2 Ibid.3 Vanharanta M, Voutilainen S, Rissanen TH, Adlercreutz H, Salonen JT. Risk ofcardiovascular disease-related and all-cause death according to serum concentrationsof enterolactone: Kuopio Ischaemic Heart Disease Risk Factor Study. Arch Intern Med.2003 May 12;163(9):1099-104.4 de Kleijn MJ, van der Schouw YT, Wilson PW, Grobbee DE, Jacques PF. Dietary intakeof phytoestrogens is associated with a favorable metabolic cardiovascular risk profile inpostmenopausal U.S.women: the Framingham study. J. Nutr. 2002 Feb;132(2):276-82.5 Vanharanta M, Voutilainen S, Nurmi T, Kaikkonen J, Roberts LJ, Morrow JD, AdlercreutzH, Salonen JT. Association between low serum enterolactone and increased plasma F2-isoprostanes, a measure of lipid peroxidation. Atherosclerosis. 2002 Feb;160(2):465-9.6 Kangas L, Saarinen N, Mutanen M, Ahotupa M, Hirsinummi R, Unkila M, Perala M,Soininen P, Laatikainen R, Korte H, Santti R. Antioxidant and antitumor effects ofhydroxymatairesinol (HM-3000, HMR), a lignan isolated from the knots of spruce. Eur JCancer Prev. 2002 Aug;11 Suppl 2:S48-57.7 Ibid. 8 Oikannen SI, Pajari AM, Mutanen M. Chemopreventative activity of crudehydroxymatairesinol (HMR) extract in Apc(Min) mice [corrected]. Cancer Lett. 2000 Oct31;159(2):183-7.9 Ibid.10 Wang L-Q. Mammalian phytoestrogens: enterodiol and enterolactone. J ChromatogrB 777:289-309, 2002.11 Y. Mousavi and H. Adlercreutz. Genistein is an effective stimulator of sex hormone-binding globulin production in hepatocarcinoma human liver cancer cells and suppressesproliferation of these cells in culture. Steroids 58 (1993), p. 301.12 Saarinen NM, Houvinen R, Wärri A, Mäkelä SI, Valentín-Blasini L, Sjöholm R, ÄmmäläJ, Lehtilä R, Eckerman C, Collan YU, Santti RS. Enterolactone inhibits the growth of 7,12-dimethylbenz(a)anthracene-induced mammary carcinomas in the rat. Mol Cancer Ther1:869-876, 2002.13 Katsuda S, Yoshida M, Saarinen N, Smeds A, Nakae D, Santti R, Maekawa A.Chemopreventive effects of hydroxymatairesinol on uterine carcinogenesis in Donryurats. Exp Biol Med 2004;229(5):417-24.14 Ibid.15 Boccardo F, et al. Enterolactone in breast cyst fluid: correlation with EGF and breastcancer risk. Breast Cancer Res Treat. 2003 May;79(1):17-23.16 Ibid. 17 Pietinen P, et al. Serum enterolactone and risk of breast cancer: a case-control studyin eastern Finland. Cancer Epidemiol Biomarkers Prev. 2001 Apr;10(4):339-44. 18 Ibid.19 Lin X, Switzer BR, Denmark-Wahnefried W. Effect of mammalian lignans on thegrowth of prostate cancer cell lines. Anticancer Res. 2001 Nov-Dec;21(6A):3995-9.20 Ibid.21 Denmark-Wahnefried W. Pilot study to explore effects of low-fat, flaxseed-supplemented diet on proliferation of benign prostatic epithelium and prostate-specificantigen. Urology 2004 May;63(5):900-4.22 Bylund A, Saarinen N, Zhang JX, Bergh A, Widmark A, Johansson A, Lundin E,Adlercreutz H, Hallmans G, Stattin P, Makela S. Anticancer effects of a plant lignan 7-hydroxymatairesinol on a prostate cancer model in vivo. Experimental Biology andMedicine 230:217-223 (2005)23 Ibid.24 Ibid.25 Ibid.26 Franco OH, et al. Higher Dietary Intake of Lignans Is Associated with BetterCognitive Performance in Postmenopausal Women. J. Nutr. 135:1190-1195, May2005.27 Ibid.28 Ibid.29 Ibid.30 Kim MK, et al. Relationships of urinary phyto-oestrogen excretion to BMD inpostmenopausal women. Clinical Endocrinology (Oxf). 2002 Mar;56(3):321-8.31 Ibid.
ADVANCES in orthomolecular research Volume 3, Issue 222
ADVANCES in orthomolecular research Volume 3, Issue 223
Q I have cancer; can I combine nutraceuticaltherapies with chemotherapy and radiation?
A If you are considering nutrients as an adjunct toeither radiation or chemotherapy, you are in goodcompany. A recent study has shown that 61% of
cancer patients in a veteran administration hospital weretaking natural supplements. Of the supplements taken,multivitamins were the most common (80.3% of supplementsused), followed by minerals (40.6%) and herbs (24.8%).1
The vast majority of nutrients beneficial for healthyindividuals are also valuable for patients with chronicdiseases such as cancer. Given that malnutrition andcachexia (malnutrition associated with severe disease suchas cancer) are common problems in patients with cancer,supplementation can help maintain adequate nutrition. Incancer patients, nutrients can also be used to addressabnormal cellular growth and replication but must beselected based on the type of cancer and on the location ofthe neoplasm. Cancer is not a single illness but a variety ofdifferent diseases characterized by a diversity of locationsand cell types. While a nutrient may cause a specificcancer cell to die, it may have little effect on another cancerand may even help certain cancer cells to grow.
So how do you chose which nutrient is suitable for yourcondition? Consultation with an oncologist or health careprofessional who is able to advise you as to which nutrientsare suitable for your specific condition and ongoingtreatment is essential.
Having said that, there are some key principles to beconsidered by those using nutritional supplementation forcancer especially when used in conjunction withchemotherapy or radiation. The mechanism of action is oneof the most important factors to consider when developinga treatment strategy. Several different approaches can beused. Nutrients can enhance the immune system so that itcan identify and kill cancer cells more effectively.Supplements can also be used to promote adequate cellulardifferentiation and to induce the cellular death of cancercells. Antioxidants prevent DNA mutations and can be usedto shield the tissue surrounding tumor cells from negativeeffects while undergoing radiation treatment.
It is important to remember that antioxidants work togetherand recycle each other (read Recycle your Antioxidants).2
Once an antioxidant has quenched a free radical it itselfbecomes a weak oxidant. If other antioxidants are notpresent in sufficient amounts, the antioxidant cannot berecycled and it becomes a prooxidant.3 Supplementationwith mega doses of a single antioxidant can actuallyincrease lipid, protein and DNA oxidation.4 This explainswhy some studies have shown that food sources of a specificantioxidant reduce the risk of cancer while supplementationwith the same antioxidant has the opposite effect.
For example, a recent trial demonstrated that beta-carotene and alpha-tocopherol could actually cause moreharm than good when it comes to cancer patients andcancer survivors. The study looking at the effect of thevitamins in cancer patients showed that a-tocopherolsignificantly increases the incidence of second primarytumors and the recurrence of cancer.5 The beta-carotenesupplementation arm of the study was dropped for ethicalreasons because two large trials using beta-carotene werepublished in the interim; one demonstrated an increase inlung cancer incidence6 while the other showed no effect oncancer incidence.7
This should come as no surprise to readers of Advances (seeAdvances Volume 2* Issue 8 p.3-20). AOR has previouslyexplained the need to supplement with complete vitamin Eand complete beta-carotene. Studies have shown that thosewhose diets contain more beta-carotene are less likely todevelop cancer.8 Unfortunately, most beta-carotenesupplements (including the supplements used in theaforementioned trials) only contain the trans form of beta-carotene. On the other hand, food sources of beta-carotene contain both cis and trans beta-carotene. Thisneglect has significant implications - studies have shown thatthe synthetic beta-carotene (trans form) used in mostsupplements has lower antioxidant activity and can lead togenetic damage in human cells.9-12
Q&A
all-trans b-Carotene
9-cis b-Carotene
24ADVANCES in orthomolecular researchVolume 3, Issue 2
As far as alpha-tocopherol is concerned, AOR has beenproactive in educating consumers about the dangers ofsupplementation with incomplete vitamin E since 2001 (seeHolistic International Volume 1, * Issue 4, p.1-4).Unfortunately, research with alpha-tocopherol alonepersists and continues to reinforce the importance ofsupplementation with complete vitamin E.
Supplementation with a complete array of antioxidants isvery promising as demonstrated by a recent studyconducted by the Yale University School of Medicineshowing that a combination of antioxidants reduces the riskof cancer in smokers.13
ApoptosisCellular auto-destruction (apoptosis) is another importanttreatment avenue for cancer patients. Apoptosis is initiatedby internal or external triggers that lead to the release ofproteins known as caspases that destroy the cell by digestingit from the inside out. In 1988 scientists first discovered a linkbetween failed apoptosis and cancer when they determinedthat certain cancer cells produce an overabundance ofproteins that prevent apoptosis.14 Apoptosis is a complicatedcellular process but more research uncovered that the failureof the gene known as TP53 is involved in the proliferation ofcancer cells. The gene codes for the cellular antigen p53, atranscription factor that prevents the replication of cellscontaining damaged DNA, is a mechanism that is essential forthe suppression of cancer.15 If abnormal genetic mutationsinactivate the TP53 gene, normal apoptosis can no longeroccur. DNA damage then goes unchecked and the celleventually begins to replicate uncontrollably.
Cancer cells need to undergo several mutations and needvery specific characteristics before they can start to affectsurrounding tissues. Although there are hundreds of differentcancers, the majority of cancer cells are deficient in p53proteins. Cancers characterized by the loss of the p53protein function are more aggressive and are associated witha worse prognosis. Several nutrients and chemotherapeuticagents stimulate apoptosis in cancer cells. Such nutrients
include phosphatidylserine, sodium butyrate, pycnogenol,selenium and retinoic acid among others, and usually induceapoptosis through their influence on genetic expression.16-20
Metastasis and angiogenesis are also key to cancerprogression and proliferation. Cancer cells can proliferateand replicate uncontrollably, but it is their ability to spread tosurrounding and distant tissues that is most devastating to thehealth of the organism. Tumors have colossal nutrientrequirements due to their rapid growth and produce growthfactors that stimulate the formation of new blood vessels(angiogenesis) that are required to facilitate further growth.Supplements and drugs can specifically preclude cancergrowth by preventing the formation of new blood vessels andobstructing the migration of cancer cells. Good examplesinclude glycine, vitamin D3 and modified citrus pectin.21-23
When it comes to the combination of naturaltherapies with Western approaches, here is whatresearch has shown:
For those undergoing radiation therapyThe effects of radiation are mostly related to the productionof free radicals. Free radicals damage cellular DNA,eventually causing cellular death. This damage accumulatesand is inherited by the daughter cancer cells. Once enoughDNA damage accumulates in the cells, the cells becomeunviable and die.
This is not to say that free radicals are beneficial in cancerpatients. Free radicals damage all cells, not just cancer cells,but because cancer cells divide more rapidly, they are moresusceptible to DNA damage. However, one of the maindifficulties with radiation is that it is difficult to target cancercells specifically and the treatment ends up damaginghealthy cells in the surrounding tissues.24
The ability to spare healthy tissue from radiation inducedcellular damage is the reason behind the usefulness ofantioxidants for patients undergoing radiation therapy.25, 26
Protection inferred through supplementation with antioxidantsprotects tissues through which radiation must penetrate todestroy tumors. For instance, antioxidants protect the skin andallow for higher radiation doses and greater therapeuticgains.27 Animal studies have demonstrated that antioxidantshelp to promote normal wound healing in radiation treatedanimals - a significant benefit for any patient undergoingradiation after surgery.28-31 Studies have shown that animalstreated with herbal extracts had less radiation sickness andreduced mortality rates.32,33 Studies have also shown that zincsupplementation in patients with head and neck cancersprevents the development of dermatitis and mucositis, twocommon complications associated with radiation.34
ADVANCES in orthomolecular research Volume 3, Issue 225
With radiation, there is an underlying concern thatantioxidants may reduce the efficacy of the therapy byprotecting the cancerous cells from free radicals. However,research demonstrates that such assumptions do not hold uponce exposed to more scientific scrutiny. Recent test tubestudies showed that folic acid strongly inhibits cancer cellgrowth in conjunction with radiation.35 Although radiationsuccessfully targets abnormal cells, it also reduces the immuneresponse, which is essential for the prevention of furthercancerous growth and proliferation.36 Supplementation canalso be used to improve the nutrient status of patientsundergoing radiation treatments as shown in a study wherevitamin D supplementation improved carbohydratemetabolism in rats subjected to radiation.37
For chemotherapyChemotherapy utilizes substances that prevent the dividing ofrapidly growing cells or that induce the cellular death ofcancer cells (apoptosis). Unfortunately, mostchemotherapeutic drugs are unable to target cancer cellsspecifically and affect all rapidly dividing cells such as thecells responsible for hair growth and the cells that line thegastrointestinal tract. This is why chemotherapy can lead tohair loss and gastrointestinal distress. Another important sideeffect associated with chemotherapy relates to a reduction inthe production of platelets by the bone marrow. Thisreduction predisposes one to bleeding problems. For thisreason, patients undergoing chemotherapy should avoidsupplementation with any nutrient known to increase blood-clotting times.
Although there is good evidence showing that well-formulated antioxidant formulas help to prevent thedevelopment of cancer by preventing DNA damage,supplementation with high doses of antioxidants whileundergoing chemotherapy treatment is probably notadvisable until more research is available. According to theAmerican Cancer Society, unless advised by a doctor,supplementation while undergoing chemotherapy should belimited to a multivitamin and mineral formula. More extensivesupplementation can be resumed after treatmentcompletion.38
Supplementation during chemotherapy is possible and can bevery beneficial if properly conducted. As an example, newanimal research has shown that docosahexaenoic acid (DHA)prevents the vascularization of tumors and increases thesensitivity of cancer cells to chemotherapy.39-41 In patientsreceiving cyclophosphamide (a chemotherapeuticmedication), supplementation with lipoic acid normalizesblood lipid profiles which if left untreated can damage theheart and blood vessels.42
Some cancers respond to hormones, meaning that their growthis stimulated by the presence of specific hormones. Forinstance, breast cancer can be estrogen or progesteronepositive which signifies that the growth of the cancer isstimulated by estrogen or progesterone. Inhibiting the activityof those hormones can be used to prevent the hormonalstimulation of cancerous growth. Tamoxifen, for instance, is anestrogen receptor modulator and competes with estrogen forattachment on cell membranes. Several nutrients and plantextracts have weak estrogenic activity and bind to estrogenreceptors where their influence is far less than that ofestrogen. Such products include soy isoflavones, theconsumption of which reduces the risk of developing breastcancer. Furthermore, isoflavone consumption in breast cancersurvivors is safe and does not influence disease free orsurvival times.43 However, animal studies suggest that soyisoflavones are best avoided in patients with estrogenpositive breast cancers especially if they are undergoingtamoxifen therapy.44 Similarly, vitamin E acetate should beavoided in patients taking tamoxifen as a study has shownthat the vitamin reduces the efficacy of the chemotherapy.45,46
Nutrients can be used to reduce the side effects ofchemotherapy. Chemotherapy is detrimental to bones andpatients who have undergone chemo are significantly more atrisk for bone fractures. Hence the recent suggestion in themedical literature that lifestyle modifications such as vitaminD and calcium can be used to improve patient outcome.47
Cisplatin-based chemotherapeutics deplete magnesium andsupplementation is recommended in patients receiving thesedrugs.48 One of the most prescribed chemotherapies ispaclitaxel, a compound isolated from the bark of the Pacificyew tree, which is widely used for the treatment of cancer.Paclitaxel causes peripheral neuropathies in 60% of patients.New research shows that vitamin E supplementationsignificantly reduces the frequency of neuropathies in patientstaking paclitaxel.49 Glutamine is also beneficial for patientsundergoing chemotherapy and was shown to improve bothnutritional and immunological parameters in childrenundergoing chemotherapy.50
26ADVANCES in orthomolecular researchVolume 3, Issue 2
As an adjunct to surgeryIn any surgery, supplementation can accelerate recovery,sustain the immune system and help prevent infections.51,52 Forinstance, in cancer patients who underwent surgery, additionof EPA oil to their enteric tube feeding shortened theirhospital stay, lowered the incidence of complications, andprevented infections and sepsis.53
For cancer survivors Several nutrients promote immunocompetence and themaintenance of remission. Studies have once againdemonstrated that the right nutrients must be chosen. Anysupplement that can potentially increase growth hormonelevels is best avoided in cancer survivors. Fiber supplements,which would be expected to reduce the recurrence of coloncancer, were useless and possibly even detrimental to coloncancer survivors.54,55 This finding may simply be related to anabnormal gut microflora which may promote thedevelopment of cancer. Fiber is a food source for theintestinal microflora and in this case may allow thepathological bacteria to thrive, worsening the problem.Recent evidence that probiotics are useful for the preventionof cancers of the large bowel would support thishypothesis.56,57 Similarly, a large trial using N-acetylcysteine(NAC) and vitamin A in patients previously affected withhead or neck cancer showed the nutrients to be of nobenefit.58 Yet, in patients with ataxia telangiectasia (aneurodegenerative childhood disorder that often progressesto cancer), NAC reduces oxidative stress, increases lifespanand reduces the incidence of cancer.59 In test tube studiesusing cancer cell lines, the addition of NAC and vitamin C tothe growth medium reduces the expression of cancermarkers.60
Studies in patients that underwent surgery to remove non-small cell lung cancer tumors demonstrated that patientssupplementing their diets with natural supplements havesignificantly longer survival rates compared to those who donot take supplements.61,62 In patients with advanced cancer,vitamin C in the blood is often depleted and lower plasmalevels are associated with shorter survival times.63 Retinoicacid prevents the development of new tumors in patients with
head or neck cancers, with metastasis occurring in 24% of thepatients in the placebo group versus only 4% of the patientsreceiving retinoic acid.64
Still confused!If you are not sure what is indicated in your case, you need toconsider the mechanism of action. Unless you are undergoinga bone marrow transplant or are taking immunosuppressantmedications, immune stimulants will be beneficial. Anadequate immune response is essential for the prevention,management and remission of cancer.
Nutrients found in a multivitamin are also beneficial forcancer patients because deficiencies commonly develop andgastrointestinal problems commonly emerge. Mega dosesare more risky, especially when antioxidants are concerned.If a therapy is centered on inducing free radical damage incancer cells, antioxidants must be chosen carefully to insurethey do not reduce the efficacy of the treatment. Consultationwith a qualified health practitioner remains the best option inthose cases.
Nutrients capable of inducing genetic damage are alsobeneficial at all stages of cancer and can typically be usedwith radiation and chemotherapy. Unfortunately, suchnutrients often possess antioxidant potential and must be usedwith care.
Research relating to cancer and nutrition is still lacking,leaving us with an incomplete picture of the true potentialnutrients may hold when it comes to the prevention, treatmentand recovery from cancer. The complexity of the diseasetogether with the moderately successful treatments alreadyavailable makes it difficult to treat cancer patients withnutrients alone. Although the side effects associated withchemotherapy and radiation can be significant, suchtreatments have improved the prognosis of those affectedwith cancer. For example, if Terry Fox lived today, he wouldhave had an 80% chance of recovery and would not havelost his leg.65 Nonetheless, more research is constantlysurfacing and there is already significant evidence as to therole nutrients can play for those affected with cancer.
ADVANCES in orthomolecular research Volume 3, Issue 227
1 Lee AH, Ingraham SE, Kopp M, Foraida MI, Jazieh AR. The incidence of potentialinteractions between dietary supplements and prescription medications in cancer patientsat a Veterans Administration Hospital. Am J Clin Oncol. 2006 Apr;29(2):178-82.2 Barclay LR. The cooperative antioxidant role of glutathione with a lipid-soluble anda water-soluble antioxidant during peroxidation of liposomes initiated in the aqueousphase and in the lipid phase. J Biol Chem. 1988 Nov 5;263(31):16138-42.3 Wroblewski K. [Can the administration of large doses of vitamin C have a harmfuleffect?] Pol Merkur Lekarski. 2005 Oct;19(112):600-3.4 Hininger I, Waters R, Osman M, Garrel C, Fernholz K, Roussel AM, Anderson RA. Acuteprooxidant effects of vitamin C in EDTA chelation therapy and long-term antioxidantbenefits of therapy. Free Radic Biol Med. 2005 Jun 15;38(12):1565-70.5 Bairati I, Meyer F, Gelinas M, Fortin A, Nabid A, Brochet F, Mercier JP, Tetu B, HarelF, Masse B, Vigneault E, Vass S, del Vecchio P, Roy J. A randomized trial of antioxidantvitamins to prevent second primary cancers in head and neck cancer patients. J NatlCancer Inst. 2005 Apr 6;97(7):481-8.6 Omenn GS, Goodman GE, Thornquist MD, Balmes J, Cullen MR, Glass A, Keogh JP,Meyskens FL, Valanis B, Williams JH, Barnhart S, Hammar S. Effects of a combination ofbeta carotene and vitamin A on lung cancer and cardiovascular disease. N Engl J Med.1996 May 2;334(18):1150-5.7 Hennekens CH, Buring JE, Manson JE, Stampfer M, Rosner B, Cook NR, Belanger C,LaMotte F, Gaziano JM, Ridker PM, Willett W, Peto R. Lack of effect of long-termsupplementation with beta carotene on the incidence of malignant neoplasms andcardiovascular disease. N Engl J Med. 1996 May 2;334(18):1145-9.8 Van Poppel G,. Goldbohm RA. Epidemiologic evidence for beta-carotene and cancerprevention. Am J Clin Nutr. 1995 Dec;62(6 Suppl):1393S-1402S.9 Levin G, Mokady S. Antioxidant activity of 9-cis compared to all-trans beta-carotenein vitro. Free Radic Biol Med. 1994 Jul;17(1):77-82.10 Levin G, Yeshurun M, Mokady S. In vivo antiperoxidative effect of 9-cis beta-carotene compared with that of the all-trans isomer. Nutr Cancer. 1997;27(3):293-7.11 Ben-Amotz A, Levy Y. Bioavailability of a natural isomer mixture compared withsynthetic all-trans beta-carotene in human serum. Am J Clin Nutr. 1996 May;63(5):729-34.12 Xue KX, Wu JZ, Ma GJ, et al. Comparative studies on genotoxicity andantigenotoxicity of natural and synthetic beta-carotene stereoisomers. Mutat Res. 1998Oct 12;418(2-3):73-8.13 Wright ME, Mayne ST, Stolzenberg-Solomon RZ, Li Z, Pietinen P, Taylor PR, VirtamoJ, Albanes D. Development of a comprehensive dietary antioxidant index andapplication to lung cancer risk in a cohort of male smokers. Am J Epidemiol. 2004 Jul1;160(1):68-76.14 Vaux DL, Cory S, Adams JM. Bcl-2 gene promotes haemopoietic cell survival andcooperates with c-myc to immortalize pre-B cells. Nature. 1988 Sep29;335(6189):440-2.15 Tammemagi MC, McLaughlin JR, Mullen JB, Bull SB, Johnston MR, Tsao MS, CassonAG. A study of smoking, p53 tumor suppressor gene alterations and non-small cell lungcancer. Ann Epidemiol. 2000 Apr;10(3):176-85.16 Webb MS, Johnstone S, Morris TJ, Kennedy A, Gallagher R, Harasym N, Harasym T,Shew CR, Tardi P, Dragowska WH, Mayer LD, Bally MB. In vitro and in vivocharacterization of a combination chemotherapy formulation consisting of vinorelbineand phosphatidylserine. Eur J Pharm Biopharm. 2006 Oct 1717 Singh NP, Lai HC. Synergistic cytotoxicity of artemisinin and sodium butyrate onhuman cancer cells. Anticancer Res. 2005 Nov-Dec;25(6B):4325-31.18 Huang WW, Yang JS, Lin CF, Ho WJ, Lee MR. Pycnogenol induces differentiation andapoptosis in human promyeloid leukemia HL-60 cells. Leuk Res. 2005 Jun;29(6):685-92.19 Hiraoka K, Komiya S, Hamada T, Zenmyo M, Inoue A. Osteosarcoma cell apoptosisinduced by selenium. J Orthop Res. 2001 Sep;19(5):809-14.20 Hansen LA, Sigman CC, Andreola F, Ross SA, Kelloff GJ, De Luca LM. Retinoids inchemoprevention and differentiation therapy. Carcinogenesis. 2000 Jul;21(7):1271-9.21 Yamashina S, Ikejima K, Enomoto N, Takei Y, Sato N. Glycine as a therapeuticimmuno-nutrient for alcoholic liver disease. Alcohol Clin Exp Res. 2005 Nov;29(11Suppl):162S-5S.22 Nangia-Makker P, Hogan V, Honjo Y, Baccarini S, Tait L, Bresalier R, Raz A. Inhibitionof human cancer cell growth and metastasis in nude mice by oral intake of modifiedcitrus pectin. J Natl Cancer Inst. 2002 Dec 18;94(24):1854-62.23 Bao BY, Yao J, Lee YF. 1alpha, 25-dihydroxyvitamin D3 suppresses interleukin-8-mediated prostate cancer cell angiogenesis. Carcinogenesis. 2006 Sep;27(9):1883-93.24 Bucci MK, Bevan A, Roach M 3rd. Advances in radiation therapy: conventional to 3D,to IMRT, to 4D, and beyond. CA Cancer J Clin. 2005 Mar-Apr;55(2):117-34.25 Srinivasan M, Sudheer AR, Pillai KR, Kumar PR, Sudhakaran PR, Menon VP. Influenceof ferulic acid on gamma-radiation induced DNA damage, lipid peroxidation andantioxidant status in primary culture of isolated rat hepatocytes. Toxicology. 2006 Dec7;228(2-3):249-58.26 Srinivasan M, Rajendra Prasad N, Menon VP. Protective effect of curcumin ongamma-radiation induced DNA damage and lipid peroxidation in cultured humanlymphocytes. Mutat Res. 2006 Sep 12
27 Chandra Jagetia G, Rajanikant GK, Rao SK, Shrinath Baliga M. Alteration in theglutathione, glutathione peroxidase, superoxide dismutase and lipid peroxidation byascorbic acid in the skin of mice exposed to fractionated gamma radiation. Clin ChimActa. 2003 Jun;332(1-2):111-21.28 Jagetia GC, Rajanikant GK, Rao SK. Evaluation of the effect of ascorbic acidtreatment on wound healing in mice exposed to different doses of fractionated gammaradiation. Radiat Res. 2003 Mar;159(3):371-80.29 Jagetia GC, Rajanikant GK. Role of curcumin, a naturally occurring phenoliccompound of turmeric in accelerating the repair of excision wound, in mice whole-bodyexposed to various doses of gamma-radiation. J Surg Res. 2004 Jul;120(1):127-38.30 Jagetia GC, Rajanikant GK. Effect of curcumin on radiation-impaired healing ofexcisional wounds in mice. J Wound Care. 2004 Mar;13(3):107-9. 31 Jagetia GC, Rajanikant GK, Baliga MS, Rao KV, Kumar P. Augmentation of woundhealing by ascorbic acid treatment in mice exposed to gamma-radiation. Int J RadiatBiol. 2004 May;80(5):347-54.32 Jagetia GC, Venkatesh P, Baliga MS. Evaluation of the radioprotective effect of baelleaf (Aegle marmelos) extract in mice. Int J Radiat Biol. 2004 Apr;80(4):281-90.33 Jagetia GC, Venkatesh P, Baliga MS. Jagetia GC, Fruit extract of Aegle marmelosprotects mice against radiation-induced lethality. Integr Cancer Ther. 2004Dec;3(4):323-32.34 Lin LC, Que J, Lin LK, Lin FC. Zinc supplementation to improve mucositis and dermatitisin patients after radiotherapy for head-and-neck cancers: a double-blind, randomizedstudy. Int J Radiat Oncol Biol Phys. 2006 Jul 1;65(3):745-50.35 Delipetar-Grudl A, Getoff N. Radiation-induced sensitizing effect of folic acid(vitamin B11) and its synergistic action to mitomycin C: in vitro experiments andradiolysis. Oncol Res. 2004;14(11-12):559-66.36 Uh S, Lee SM, Kim HT, Chung Y, Kim YH, Park C, Huh SJ, Lee HB. The effect ofradiation therapy on immune function in patients with squamous cell lung carcinoma.Chest. 1994 Jan;105(1):132-7.37 Starikovich LS, Aragon GA, Vernikovska YI, Vigovska TV, Veliky MM. Effect of avitamin D3-based nutritional supplement ('Videchol') on carbohydrate metabolism ofrats following chronic low dose-rate irradiation. J Radiol Prot. 2001 Sep;21(3):269-76.38 American Cancer Society, Selecting Which Drugs to Use for ChemotherapyTreatments. 11/17/200639 Colas S, Maheo K, Denis F, Goupille C, Hoinard C, Champeroux P, Tranquart F,Bougnoux P. Sensitization by dietary docosahexaenoic acid of rat mammary carcinomato anthracycline: a role for tumor vascularization. Clin Cancer Res. 2006 Oct1;12(19):5879-86.40 Danbara N, Uehara N, Shikata N, Takada H, Hada T, Tsubura A. Dietary effects ofconjugated docosahexaenoic acid on N-methyl-N-nitrosourea-induced mammarycarcinogenesis in female Sprague-Dawley rats. Oncol Rep. 2004 Nov;12(5):1079-85.41 Pardini RS. Nutritional intervention with omega-3 fatty acids enhances tumorresponse to anti-neoplastic agents. Chem Biol Interact. 2006 Aug 25;162(2):89-105.42 Mythili Y, Sudharsan PT, Sudhahar V, Varalakshmi P. Protective effect of DL-alpha-lipoic acid on cyclophosphamide induced hyperlipidemic cardiomyopathy. Eur JPharmacol. 2006 Aug 14;543(1-3):92-6.43 Messina M, McCaskill-Stevens W, Lampe JW. Addressing the soy and breast cancerrelationship: review, commentary, and workshop proceedings. J Natl Cancer Inst. 2006Sep 20;98(18):1275-84.44 Hsieh CY, Santell RC, Haslam SZ, Helferich WG. Estrogenic effects of genistein onthe growth of estrogen receptor-positive human breast cancer (MCF-7) cells in vitro andin vivo. Cancer Res. 1998 Sep 1;58(17):3833-8.45 Peralta EA, Viegas ML, Louis S, Engle DL, Dunnington GL. Effect of vitamin E ontamoxifen-treated breast cancer cells. Surgery. 2006 Oct;140(4):607-1446 Ju YH, Doerge DR, Allred KF, Allred CD, Helferich WG. Dietary genistein negates theinhibitory effect of tamoxifen on growth of estrogen-dependent human breast cancer(MCF-7) cells implanted in athymic mice. Cancer Res. 2002 May 1;62(9):2474-7.47 Guise TA. Bone Loss and Fracture Risk Associated with Cancer Therapy. Oncologist.2006;11(10):1121-1131.48 Hodgkinson E, Neville-Webbe HL, Coleman RE. Magnesium depletion in patientsreceiving cisplatin-based chemotherapy. Clin Oncol (R Coll Radiol). 2006Nov;18(9):710-8.49 Argyriou AA, Chroni E, Koutras A, Iconomou G, Papapetropoulos S, PolychronopoulosP, Kalofonos HP. Preventing paclitaxel-induced peripheral neuropathy: a phase II trial ofvitamin E supplementation. J Pain Symptom Manage. 2006 Sep;32(3):237-44.50 Okur A, Ezgu FS, Tumer L, Cinasal G, Oguz A, Hasanoglu A, Karadeniz C. Effects oforal glutamine supplementation on children with solid tumors receiving chemotherapy.Pediatr Hematol Oncol. 2006 Jun;23(4):277-85.51 Ali S, Roberts PR. Nutrients with immune-modulating effects: what role should theyplay in the intensive care unit? Nutrients with immune-modulating effects: what roleshould they play in the intensive care unit?52 O'Flaherty L, Bouchier-Hayes DJ. Immunonutrition and surgical practice. Proc NutrSoc. 1999 Nov;58(4):831-7.
References
28ADVANCES in orthomolecular researchVolume 3, Issue 2
53 Elia M, Van Bokhorst-de van der Schueren MA, Garvey J, Goedhart A, Lundholm K,Nitenberg G, Stratton RJ. Enteral (oral or tube administration) nutritional support andeicosapentaenoic acid in patients with cancer: a systematic review. Int J Oncol. 2006Jan;28(1):5-23.54 Alberts DS, Martinez ME, Roe DJ, Guillen-Rodriguez JM, Marshall JR, van LeeuwenJB, Reid ME, Ritenbaugh C, Vargas PA, Bhattacharyya AB, Earnest DL, Sampliner RE.Lack of effect of a high-fiber cereal supplement on the recurrence of colorectaladenomas. Phoenix Colon Cancer Prevention Physicians' Network. N Engl J Med. 2000Apr 20;342(16):1156-6255 Bonithon-Kopp C, Kronborg O, Giacosa A, Rath U, Faivre J. Calcium and fibresupplementation in prevention of colorectal adenoma recurrence: a randomisedintervention trial. European Cancer Prevention Organisation Study Group. Lancet. 2000Oct 14;356(9238):1300-6.56 McGarr SE, Ridlon JM, Hylemon PB. Diet, anaerobic bacterial metabolism, and coloncancer: a review of the literature. J Clin Gastroenterol. 2005 Feb;39(2):98-109.57 Saikali J, Picard C, Freitas M, Holt P. Fermented milks, probiotic cultures, and coloncancer. Nutr Cancer. 2004;49(1):14-24.58 van Zandwijk N, Dalesio O, Pastorino U, de Vries N, van Tinteren H. EUROSCAN, arandomized trial of vitamin A and N-acetylcysteine in patients with head and neckcancer or lung cancer. For the EUropean Organization for Research and Treatment ofCancer Head and Neck and Lung Cancer Cooperative Groups. J Natl Cancer Inst. 2000Jun 21;92(12):977-86.
59 Reliene R, Schiestl RH. Antioxidant N-acetyl cysteine reduces incidence andmultiplicity of lymphoma in Atm deficient mice. DNA Repair (Amst). 2006 Jul13;5(7):852-9.60 Vanisree AJ, Shyamaladevi CS. The effect of N-acetylcysteine in combination withvitamin C on the activity of ornithine decarboxylase of lung carcinoma cells--In vitro. LifeSci. 2006 Jul 10;79(7):654-9.61 Jatoi A, Daly BD, Kramer G, Mason JB. A cross-sectional study of vitamin intake inpostoperative non-small cell lung cancer patients. J Surg Oncol. 1998 Aug;68(4):231-6.62 Jatoi A, Williams B, Nichols F, Marks R, Aubry MC, Wampfler J, Finke EE, Yang P. Isvoluntary vitamin and mineral supplementation associated with better outcome in non-small cell lung cancer patients? Results from the Mayo Clinic lung cancer cohort. LungCancer. 2005 Jul;49(1):77-84.63 Mayland CR, Bennett MI, Allan K. Vitamin C deficiency in cancer patients. PalliatMed. 2005 Jan;19(1):17-20.64 Hong WK, Lippman SM, Itri LM, Karp DD, Lee JS, Byers RM, Schantz SP, Kramer AM,Lotan R, Peters LJ, et al. Prevention of second primary tumors with isotretinoin insquamous-cell carcinoma of the head and neck. N Engl J Med. 1990 Sep20;323(12):795-801.65 Darrell Fox, Terry Fox Foundation, 2005 Apr. CBC News